Embed Size (px)
Citation preview
THE NEUROPATHOLOGICAL ASPECTS OF THROMBOCYTICACROANGIOTHROMBOSIS
A CLINICO-ANATOMICAL STUDY OF GENERALIZED PLATELET THROMBOSISBY
RAYMOND D. ADAMSDepartment of Neurology, Harvard Medical School, and the Neurological Unit, Boston City Hospital
JAN CAMNMERMEYERDepartment of Neurology, Harvard Medical School, and the Neurological Unit, Boston City Hospital,
Rockefeller Foundation Fellow
AND
PATRICK J. FITZGERALDMallory Institute ofPathology, Boston City Hospital(RECEIVED FOR PUBLICATION, DECEMBER 27, 1947)
During the past two years we have been able tostudy the neuropathological changes in fourpatients in whom the principal symptomatologywas fever, purpura, thrombocytopenia, and anemia.In each instance the onset of symptoms was acute,the course of the illness rapidly progressive, andthe termination fatal in a few days to weeks. Theoutstanding morphological finding was an increasedcellularity and thrombosis of arterioles and capil-laries in many organs, including the brain, by whatare presumed to be agglutinated masses of platelets.In this respect it differs from the better knownthrombocytopenic purpura of Werlhof and, as faras we know, from other diseases.
In our cases and in all of those which havehitherto been reported (see Table), neurologicalsymptoms such as muscular weakness, hemiplegia,convulsions, drowsiness, confusion, stupor, or comabecame manifest at some time, usually in the laterstages of the illness. For this reason, and alsobecause the neuropathological changes in a seriesof cases have not been described-in detail, it wasdeemed advisable to bring this unusual syndrome tothe attention of neurologists and neuropathologists.
This disease entity, if it be such, was first describedin 1925 by Moschowitz. He had examined theorgans of an adolescent girl who had succumbedto an acute febrile illness with joint pains, anwmia,petechial hlmorrhages in the skin, left hemiplegia,coma, and death within two weeks. In many ofthe capillaries and arterioles of the heart, liver,kidneys, and spleen there were thrombi of the
"hyalin " type. Unfortunately a platelet countwas not done. The brain was not examined.
In 1936 Baehr and others summarized thefindings in four similar cases, each characterizedby fever, progressive anaemia, mild icterus, andpurpura. There were leucocytosis, reticulocytosis,and marked thrombocytopenia. Neurologicalsymptoms consisting of convulsions, hemiplegia,delirium, or coma were present in three of thefour cases. Necropsy revealed diffuse arteriolar andcapillary thrombosis. The thrombotic material wasbelieved to be composed of platelets.
Since the paper by Baehr and others nine othercases (Gitlow and Goldmark, 1939; Altschule,1942; Bernheim, 1943; Trobaugh and others,1946; Engel and others, 1947; Fitzgerald andothers, 1947) have been reported, bringing the totalto fourteen. All have shown platelet thrombi inthe arterioles and capillaries, anemia and thrombo-cytopenia. All have ended fatally within a few daysto weeks. Four of the fourteen cases have beenadult males and the rest adult fenjales. The brainwa s examined in eight of these cases. Grossly theon ly changes were a few petechial hemorrhages,an d these were not denronstrable in all the cases.Be rnheim was the first to report the brain lesionsin detail. In additicn to platelet thrombi she notedsm all fcci of isclanlic necrosis. Engel and othersha ve descrited vascular Aard parenchymal lesions in
-a further case which differed frcm others in that theill ness lasted three rrcnths, cccurring in two phasesse rarated by an inteiNal of three weeks. However,
27
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
28 RAYMOND D. ADAMS, JAN CAMMERMEYER AND PATRICK J. FITZGERALD
some of the symptomatology in the first stagesmay have been due to a verrucous endocarditiswith brain embolism.The present communication summarizes the
neuropathological findings in four cases which havebeen examined at the Mallory Institute of Pathologyand the Neuropathology Laboratory of BostonCity Hospital. One of our cases was reported byTrobaugh and others in 1946, and three otherswere described along with a general review of thesubject in the paper of Fitzgerald and others in1947.
Summary of CasesCase 1. (Case II of Fitzgerald and others, 1947).
-The patient was a 24-year-old negress who was broughtto the hospital because ofdeepening coma oftwelve hours'duration. She had -had many illnesses during theprevious three years. In 1942 she had had gonorrheeaand toxemia of pregnancy, and was delivered of a full-term stillborn infant. In 1945 she had an incompletemiscarriage. In the fall of 1945 she developed a skinrash after being given sulphonamide prophylacticallyduring the extraction of abscessed teeth. In 1946 shewas hospitalized for chest and joint pains and urticariawhich were diagnosed- as rheumatic fever. The urticariacontinued intermittently and was being treated withbenadryl when she first complained of faintness, suffoca-tion, nausea, hbmatemesis, epistaxis, and menorrhagiaabout one week before admission. In the followingdays she became very weak and stuporous, and then,a few hours before entry, comatose.
Physical examination upon final admission showed a
poorly nourished woman whose blood pressure was
98 rnm. Hg systolic and 76 diastolic, pulse 90, respiration30, and temperature 970 F. There was a macular rashover the skin of the chest, abdomen, back, and thighs.The pupils were equal in size but reacted sluggishly tolight. The knee jerks were absent and the other tendonreflexes were one plus and equal. There were no otherabnormal neurological signs.The red cell count was 2.74 million per c.mm. of
blood, hemoglobin 7 g. and white blood cells 14,900with 50 per cent. neutrophilic leucocytes, 46 per cent.lymphocytes, and 4 per cent. monocytes. The ictericindex was 25. The blood sugar, non-protein nitrogen,and chloride values were normal. The CO2 combiningpower was 35 vol. per cent. The cerebrospinal fluidwas normal.The patient remained in coma and died six hours
after entry to the hospital, about a week or less afterthe onset of acute symptoms.ANATOMICAL DIAGNosIs.-There were arteriolar,
capillary, and venular thrombi with minimal endothelialproliferation in the oesophagus, lungs, heart, liver,pncreas, spleen, kidneys, ovaries, uterus, vagina, lymphnodes, bone marrow, and brain; focal necroses of themyocardium, pancreas, and brain; multi-nucleatedgiant cells in the lung capillaries; extramedullarymyelopoiesis of the spleen; hyperplasia of the vertebralmarrow; petechii and ecchymoses of the heart and
kidney; healed pleuritis of the left apex; and spleno-megaly.NEUROPATHOLOGICAL FINDINGs.-The brain was of
normal size and configuration. There were no grosslesions in the cerebrum or brain stem.
Microscopic examination disclosed both vascular andparenchymatous changes in the cerebrum and brain stemas well as other changes of lesser significance.The leptomeninges were thickened by an increased
amount of relatively acellular collagenous connectivetissue which in some places, particularly near the bottomof the sulci, contained small numbers of lymphocytes.The meningeal arteries and veins were normal.There was an increased number of glia-ells in the
marginal layer of the cerebral cortex, most marked inthe sulci. They consisted of small clusters of astrocytenuclei, some with visible perikaryon (amceboid cells),and scattered, elongated, microglial cells with irregularbipolar processes.
In all the parts of the cerebral cortex which wereexamined, that is, the hippocampus, premotor, sensori-motor, temporal, parietal, and occipital lobes, and inthe caudate nucleus, putamen, thalamus, and substantiainnominata, there was an increased cellularity of thearterioles, capillaries, and possibly small veins andthrombi of amorphous material partially or completelyfilling the lumen of many of these vessels. The adven-titial cells of the aforementioned vessels were pale andswollen, and small granules of pigment, appearingyellowish in thionine-stained sections (probably " lipo-fuscin ") could be seen in their cytoplasm. The endo-thelial cells of these vessels were increased in numberand in size. Not infrequently the proliferating endo-thelial cells crowded concentrically into the lumen orextended diagonally or transversely across it. Thethrombotic material which filled many of the vesselswas finely granular and sometimes mixed with a fewred corpuscles and white blood cells. In thionine stainsthe thrombotic mass was greyish and contained someminute chromatin particles and in hfimatoxylin andeosin stains it had a pink colour. One or two mastcells lay outside the adventitia of some vessels (Fig. 5 B).
In the tissue adjacent to many of the affected vesselsin a small zone approximately 100 microns in size thenerve cells were pale with loss of Nissl substance andnuclear chromatin. In some of these minute fociseveral pleomorphic microglial cells * were found. Insections stained for myelin by Loyez technique there wasno demonstrable change in the myelinated fibres. A fewpetechial hiemorrhages of well-preserved red corpuscleswere also present in the cerebral cortex.No significant changes could be demonstrated in
the cerebellum or in sympathetic ganglia. The medulla,pons, and midbrain were not available for microscopicexamination.The arteries and veins, though occasionally surrounded
by a few lymphocytes, macrophages with " lipofuscin '-pigment and mast cells, showed no endothelial reactionor thrombi.
* We are referring, by this term, to microglial cells which areenlarged and have visible cytoplasm and processes and elongated orirregular nuclei.
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
THROMBOCYTIC ACROANGIOTHROMBOSIS
NEURO-ANATOMICAL FINDINGS.-Multiple small vesselswith endothelial reaction and thrombi; a fewpetechial hemorrhages; multiple small foci of peri-vascular necrosis, some with microglia reaction; hyper-plasia of glia-cells in the first cortical layer; fibroticthickening of leptomeninges.COMMENT.-The neuropathological changes which
could be related to the acute disease process were thecellular proliferation in the walls of the arterioles andcapillaries, the thrombi, the multiple small foci of nerve-cell alteration, and the scattered petechial hkmorrhages.The age of the glia-cell reaction in the marginal layerof cerebral cortex was difficult to judge. Unquestionablysome of these glial changes and certainly the fibroticthickening of the meninges were much older than thedisease process under consideration.The vascular and parenchymal lesions in the brain
were of the same type as those in many of the otherorgans but differed from those in the heart by being lesshlemorrhagic. Some of the cerebral changes may havebeen several days, possibly a week old, which was soonafter the time of the onset of the hxmorrhagic diathesis;but most ofthem seemed to be more recent, correspondingmore nearly to the development of stupor and coma.Case 2 (Reported by Trobaugh and others, 1946).
The patient was a 24-year-old white man who had beenwell until two weeks before admission when he developeda cold with fever, prostration, and cough. His conditionimproved slightly in the next ten days, and on theeleventh day he felt generally ill and noticed hkmaturia.Severe vomiting of several hours' duration precededentry to the hospital. i
At the time of arrival to the hospital his temperaturewas 1010 F., blood pressure was 120 mm. Hg systolicand 70 diastolic, and the pulse was rapid. He wasrestless and stuporous. His skin was pale and slightlyjaundiced, with petechie over the abdomen, lower legs,and in the mouth and conjunctiva!. There were noother abnormal physical findings.The hlmoglobin was 36 per cent., red cell count 2-18
million per c.mm. of blood, white blood cells 9,200.The differential count of white blood cells was 37 percent. segmented neutrophilic leucocytes and 17 per cent.band forms, 23 per cent. lymphocytes, 17 per cent.monocytes, 4 per cent. eosinophils, 2 per cent. basophils,and 1 per cent. blast forms. Reticulocytes made up10 per cent. of the red blood cells. The osmotic fragilitytest gave normal results and there were no cold agglu-tinins. Platelets were markedly reduced in stainedsmears' of the blood. The icteric index was 20.The patient became more deeply confused and restless
and died on the third day in the hospital, the seventeenthday of the illness or six days after the onset of thehemorrhagic diathesis.ANATOMICAL DIAGNOSIS.-There were widespread
arteriolar and capillary thromboses in the heart'(myo-cardium), liver, pancreas, kidneys, adrenal cortex(mostly glomerular zone), ileum, and duodenum(mucosa), lymph nodes, bone marrow, and brain; smallfoci of necrosis, both anoemic and hlmorrhagic, in themyocardium, adrenal cortex (fasciculate zone) and
pancreas; petechial hemorrhages in the heart (epi-cardium, myocardium, and endocardium), lungs, andintestinal mucosa; multinucleated giant cells in thelung capillaries; heemolytic icterus as evidenced bymoderate hemosiderosis of the liver and spleen and byhyperactive bone marrow; and bronchopneumonia.NEUROPATHOLOGICAL FINDINGS.-NO gross abnor-
malities of the brain were detected.In microscopic sections of the cerebral cortex the
leptomeninges appeared thickened owing to an increasedamount of connective tissue. A few lymphocytes andan occasional neutrophilic leucocyte were seen in the pia.One small flat subarachnoid haemorrhage of well-preserved red corpuscles was present. Some of thesubarachnoid arteries were filled with blood cells, andin many of them minute granules of red colour inaniline-blue-stained sections were found on the endo-thelial surface and between the red corpuscles within thevessel lumen. In one medium-sized artery the endo-thelial cells were larger and more numerous than usual.No thrombi could be found.
In the marginal layer of the cerebral cortex, especiallynear the bottom of the sulci, there were clusters ofastrocyte nuclei and single hypertrophied astrocytes withvisible cytoplasm and pleomorphic microglial cells.Throughout the cerebral cortex arterioles and capil-
laries of pronounced cellularity were noted. Theendothelial cells were increased in number and had i.pale, indented nucleus and a basophilic or even meta-chromatic cytoplasm in thionine-stained sections. Thesecells were arranged circularly or they protruded into thelumen, in some places appearing almost to occlude it.Smaller, more elongated cells with darker nuclei werefound outside the endothelial cells. An occasionalmitotic' figure could be seen in an endothelial cell. Therewere a few lymphocytes and an occasional unidentifiedmononuclear cell or neutrophilic leucocyte in the wall ofthe vessel or its perivascular space. The externaldiameter of these vessels was larger than normal. Thelumen of many vessels was partly or completely filledwith a granular amorphous material similar to that inCase 1.
There were only slight parenchymal changes consistingof a small zone around the most severely affected vesselswhere the nerve cells were pale, that is, loss of Nisslsubstance and pale nuclei, or, less often, had disappeared.In some of these foci microglial cells had increased innumber and were pleomorphic. A few small hlmor-rhages were found in the cerebral cortex.
These vascular and parenchymatous changes werepresent in all parts of the cerebral cortex, being mostconspicuous in layers II, III, and IV. Similar vascularlesions were seen in the medulla, and in fact the tissuedamage was much more pronounced here than in thecortex. These medullary lesions took the form of smallfoci of necrosis and hemorrhage in which there wereclumps of swollen astrocytes and pleomorphic microglialcells. Such-lesions were situated in the lateral part ofthe magno-cellular reticular formation and nucleus ofBurdach (Fig. 5A). In addition to the focal lesions,all the nuclei appeared to contain a few scattered swollenastrocytes and microglial cells.
29
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
30 RAYMOND D. ADAMS, JAN CAMMERMEYER AND PATRICK J. FITZGERALD
NEURO-ANATOMICAL FINDINGS.-There were multiplesmall vessels with endothelial proliferation and thrombi;a few petechial hemorrhages in the cerebral cortex andsubarachnoid space; endothelial reaction in onemedium-sized leptomeningeal artery; infiltration ofleptomeninges by a few lymphocytes and an occasionalneutrophilic leucocyte; multiple small foci of necrosisin the cerebral cortex and in the nuclei of the medullasome, particularly in the medulla, with glia-cell reaction;and diffuse glia-cell proliferation in the medulla andfirst cortical layer.COMMENT.-In this case it was concluded that the
alteration of the walls of the arterioles and capillaries,the thrombi, the perivascular tissue changes, and thepetechial hemorrhages were the underlying pathologyof the disease under consideration. The significance ofmeningeal fibrosis and glia-cell reaction in the marginallayer of cerebral cortex and in some parts of the medullacould not be determined.The vascular lesions in the brain were exactly like
those in other organs. Many of the parenchymatouschanges were of such a character as to be adjudged abouta week old. Presumably the vessels in all the differentorgans had been involved at about the time of, or slightlybefore, the haemorrhagic tendency became manifest.The vascular changes in the brain were apparentlyslightly older and somewhat more advanced in this casethan in Case 1,
Case 3 (Case I of Fitzgerald and others, 1947).-Thepatient was a 34-year-old white male who had been welluntil three weeks before admission, when he firstexperienced slight nausea and severe epigastric pain.He continued to work for the next three weeks untilweakness, fatigue, anorexia, and constipation necessitatedentry into the hospital for examination. In the past thepatient had had an obscure abdominal disorder forwhich he took bismuth and aluminium hydroxide.There was no history of exposure to other drugs or toxicagents or of allergy.The patient was restless and apprehensive. His
temperature, pulse, respiration, and blood pressure werewithin normal limits. The skin was pale and dry.There were numerous recent retinal haemorrhages. Theremainder of the examination was not remarkable.The red cell count was 2-14 million per c.mm. of
blood, and the hmemoglobin was 42 per cent.; the whitecell count was 13,700, with 60 per cent. neutrophilicleucocytes, 10 per cent. band forms, 1 per cent. juvenileforms, 1 per cent. myelocytes, 27 per cent. lymphocytes,and 1 per cent. monocytes. The platelet count was88,000; the clotting time was 3 minutes, and the bleedingtime 11-5 minutes. The prothrombin time was con-siderably prolonged in comparison to a normal control.The osmotic fragility of the red corpuscles was normal.The icteric index was 13.
His temperature varied from 99 to 1020 F. but wasnormal after the sixth hospital day. The patient wasvery restless and often confused. He complained ofdizziness. On the twelfth hospital day he becamecomatose and died a few hours later, twelve days afterthe exacerbation of the disease and five weeks from theonset of his illness.
ANATOMICAL DIAGNosIs.-There was diffuse arteriolar,capillary, and venular thrombosis with. endothelialproliferation in the heart, lungs, liver, spleen, adrenals,gastrointestinal tract, kidneys, prostate, testicles, lymphnodes, bone marrow, brain, and spinal cord; petechialhemorrhages and ecchymoses in the skin, pericardium,myocardium, lungs, peritoneum, small intestines, andbrain; multiple foci of necrosis in the myocardium andbrain; multinucleated giant cells in the capillaries ofthe lung; cardiomegalv, hepatomegaly, and spleno-megaly; hyperplasia of the bone marrow; tracheo-bronchitis and bronchopneumonia; atelectasis; andinterstitial cell hyperplasia of the testicles.NEUROPATHOLOGICAL FINDINGs.-The only gross
abnormality in the brain was the presence of petechialhemorrhages. They were fifteen to twenty in numberand could be seen on the cut surface of the cerebralcortex, lenticular nucleus, thalamus, superior colliculi,pontine nuclei, and cerebellar cortex.
In microscopic sections the leptomeninges werenormal except for a few scattered lymphocytes and anoccasional neutrophilic leucocyte. The large arteriesshowed slight reduplication of the internal elastic laminaand irregular basophilic staining of parts of the media.In the walls of some middle-sized arteries there wereirregular "calcified " bodies situated chiefly in themedia and sometimes in the intima and adventitia.
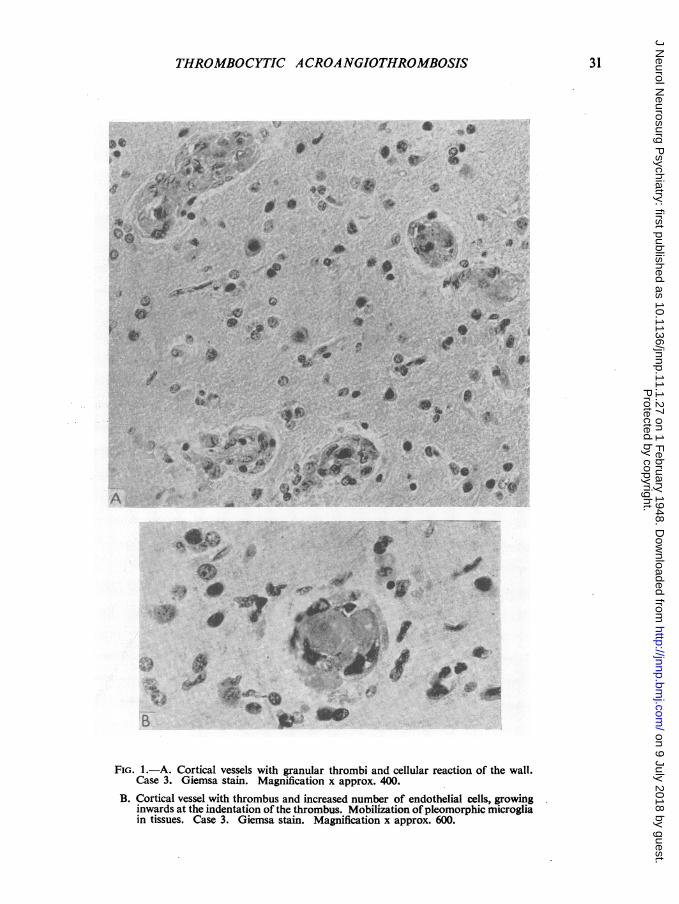
In some parts of the grey matter there was cellularproliferation and partial or complete thrombosis ofmost of the arterioles and capillaries (Fig. 1 A and B).The endothelial cells were increased in number, hadpale and enlarged nuclei which protruded into the lumenand encircled or invaded thrombi of granular character(Fig. 2 c). The cytoplasm of some of these cells wasquite basophilic and contained small dark granules.No definite mitotic figures were found. In a few vesselsthe cellular reaction was not accompanied by throm-bosis. In some of the vessels, stained for reticulum,silver-impregnated fibrils often ending in bulbs werefound between the intimal and adventitial cells of the,vessel wall (Fig., 2 A and B). In van Gieson-stainedsections a slight trace of reddish colour but no fullydeveloped fuchsinophilia of the intercellular fibrilscould be seen. In the choroid plexus were some vesselswith a pronounced cellular reaction nearly completelyobliterating the lumen (Fig. 5 c).
Parenchymatous lesions were found in the cortexof the frontal, parietal, temporal lobes and the thalamus,midbrain, pons, and medulla but they varied greatlyin different regions. In the cerebral cortex the vesselswith reactive changes were surrounded by a zone inwhich nerve cells were poorly stained. The nerve-cellalteration was more pronounced in the sensori-motorcortex, where in some foci these cells had completelydisappeared or were shrunken, homogeneous, and pale,with a darkly stained nucleus. Many swollen astrocytenuclei and pleomorphic microglial cells were found insome of these foci. There were also several collectionsof extravasated red corpuscles. In the marginal layerof the cortex, small clusters of naked astrocyte ntucleiand scattered " ameboid " astrocytes were found.The most severe lesions were in the superior colliculi
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
THROMBOCYTIC ACROANGIOTHROMBOSIS
--
* c.4'%1 *41* 'j - s /
o.). S
a.s
eE:Alk
.* j.,r.!"OA
r6:
tpk'r
v-e
A :'
4|*a.* 4*
. .*di
16 i .H9M..
S ta
'Sd.1%w_
.10+.
0* 0
.4*
'4:-
,.g.;,.
_*.w~~~ .u.vO~~~~~~~~jr Os"00a;^f_-0
4''>v̂ . _
t*
0
4'
*#|
1. lk
0~~~~~~~~~~~~~~~~~...Z 'F
'Qe+ {
B
.4.4' 4.4 lt
',* ,w R*s X~dM
AP.
X.
k A~,O
w4J,
FIG. 1.-A. Cortical vessels with granular thrombi and cellular reaction of the wall.Case 3. Giemsa stain. Magnification x approx. 400.
B. Cortical vessel with thrombus and increased number of endothelial cells, growinginwards at the indentation of the thrombus. Mobilization ofpleomorphic microgliain tissues. Case 3. Giemsa stain. Magnification x approx. 600.
A
31
*^cr- t
I
4 Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
32 RAYMOND D. ADAMS, JAN CAMMERMEYER AND PATRICK J. FITZGERALD
4
Nh-
"Wt o7$
.g. .... .....
\ > .\... ..
*e,xhR :1
.:-.s..w.,.ii.t. at .., ,
5N1:E 0 ''
B_ '''
* .,. w,....... . F.:
:. * .+. ti
*:|E!' i._.,.,,Z1%
:w_~~~~~~~~
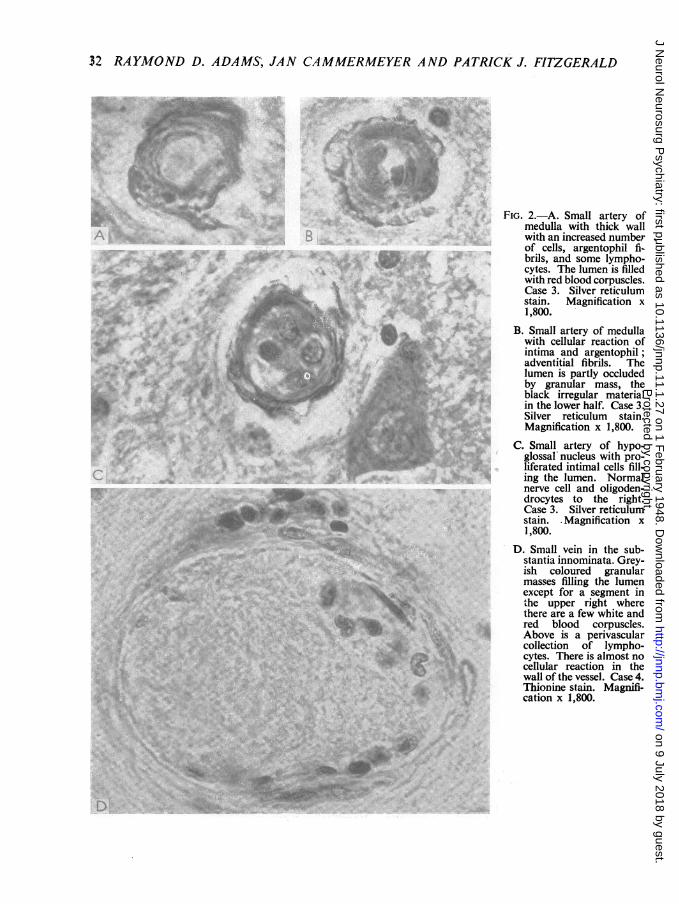
FIG. 2.-A. Small artery ofmedulla with thick wallwith an increased numberof cells, argentophil fi-brils, and some lympho-cytes. The lumen is filledwith red blood corpuscles.Case 3. Silver reticulumstain. Magnification x1,800.
B. Small artery of medullawith cellular reaction ofintima and argentophil;adventitial fibrils. Thelumen is partly occludedby granular mass, theblack irregular materialin the lower half. Case 3.Silver reticulum stain.Magnification x 1,800.
C. Small artery of hypo-glossal nucleus with pro-liferated intimal cells fill-ing the lumen. Normalnerve cell and oligoden-drocytes to the right.Case 3. Silver reticulumstain. Magnification x1,800.
0. Small vein in the sub-stantia innominata. Grey-ish coloured granularmasses filling the lumenexcept for a segment inthe upper right wherethere are a few white andred blood corpuscles.Above is a perivascularcollection of lympho-cytes. There is almost nocellular reaction in thewall of the vessel. Case 4.Thionine stain. Magnifi-cation x 1,800.
v
.h Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
33THROMBOCYTIC ACROANGIOTHROMBOSISa ..,-
a'a
to *i.(I1A
94
I.0 t
4)c
.;*
a
a t
f I *
A I4
I..Ii-v i
.4*3h 1'
^,i.c:
tf4w
\js 4#S
I
r..x
A :
a Aw
el;;j at
F I
* A (;aA
4
* t
Si~~~~~~~2
# / X ) ~~~~~~~~~'
f~~F.-# 4
X ts sSW~~~~~~~-~
r
Lt t ( A'"S~~~~~~~~t 4.4iA
:l-*
4 44
- t
* - .4
w W *.
4iI
a ..
.*t " %
40
3
.0
9$
*7
4-, 4
*.1
a4%.
I-4i
.4I I-m 0*XX .}t .~~~~~~~~~~~~
-~ ~ ~ ~ -
-' 1. *' g '
* 39 A^
t1 ,_ r
v ~ ~~~V
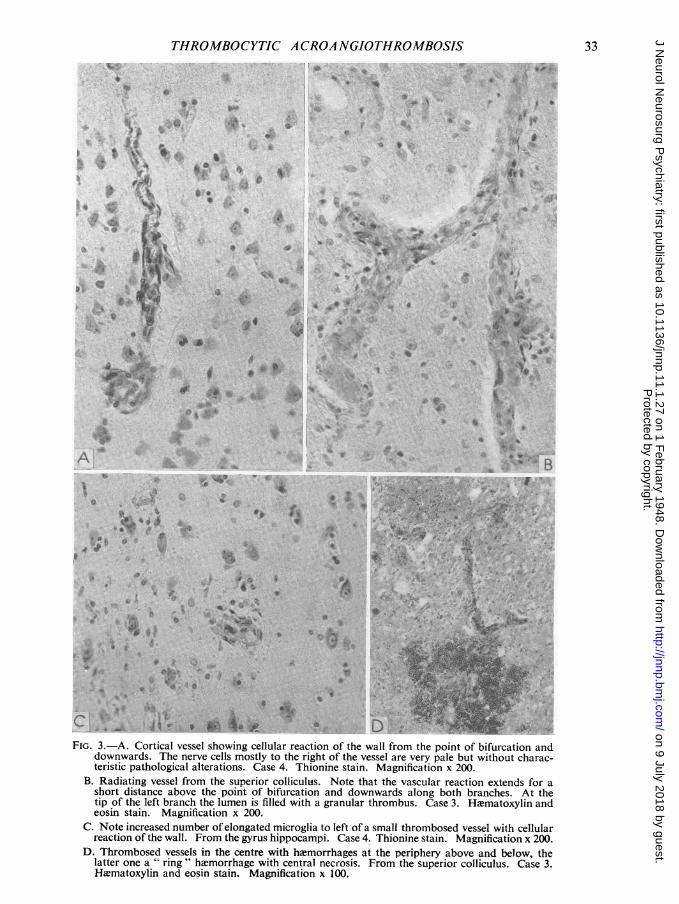
.4+° D -FIG. 3.-A. Cortical vessel showing cellular reaction of the wall from the point of bifurcation and
downwards. The nerve cells mostly to the right of the vessel are very pale but without charac-teristic pathological alterations. Case 4. Thionine stain. Magnification x 200.
B. Radiating vesse'l from the superior colliculus. Note that the vascular reaction extends for ashort distance above the point of bifurcation and downwards along both branches. At thetip of the left branch the lumen is filled with a granular thrombus. Case 3. HWmatoxylin andeosin stain. Magnification x 200.
C. Note increased number ofelongated microglia to left of a small thrombosed vessel with cellularreaction of the wall. From the gyrus hippocampi. Case 4. Thionine stain. Magnification x 200.
D. Thrombosed vessels in the centre with hemorrhages at the periphery above and below, thelatter one a " ring" hemorrhage with central necrosis. From the superior colliculus. Case 3.H1ematoxylin and eosin stain. Magnification x 100.
A
*Y 7sS
r~~~~~it.e-d *~~f
r'- ,
_.
i /%
.F.
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
34 RAYMOND D. ADAMS, JAN CAMMERMEYER AND PATRICK J. FITZGERALD
a.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~#'f
)ia;|0' > t'> '1, t
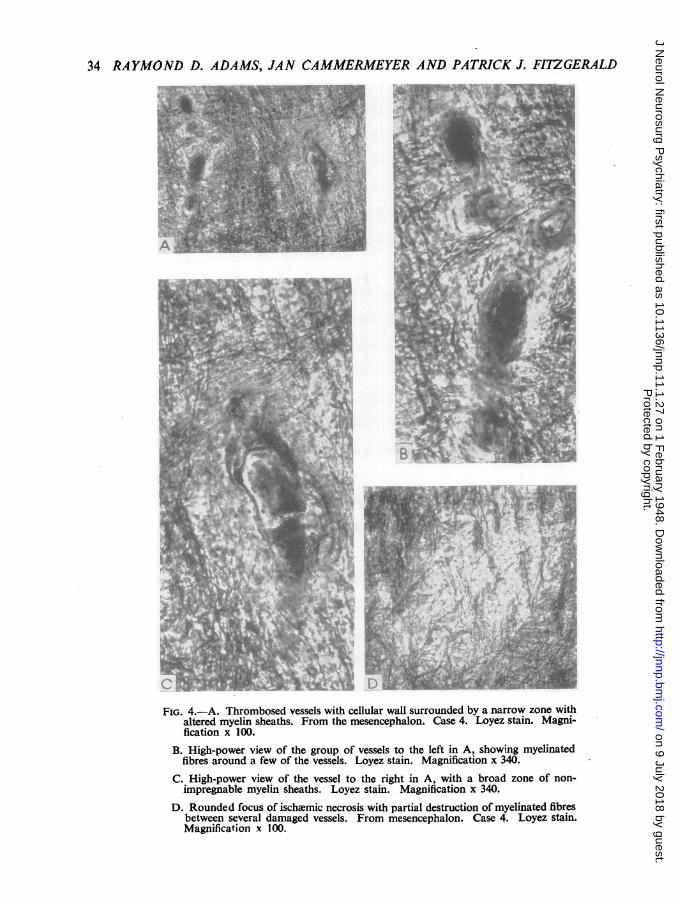
FIG. 4.-A. Thrombosed vessels with cellular wall surrounded by a narrow zone withaltered myelin sheaths. From the mesencephalon. Case 4. Loyez stain. Magni-fication x 100.
B. High-power view of the group of vessels to the left in A, showing myelinatedfibres around a few of the vessels. Loyez stain. Magnification x 340.
C. High-power view of the vessel to the right in A, with a broad zone of non-impregnable myelin sheaths. Loyez stain. Magnification x 340.
D. Rounded focus of ischaemic necrosis with partial destruction of myelinated fibresbetween several damaged vessels. From mesencephalon. Case 4. Loyez stain.Magnification x 100.
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
THROMBOCYTIC A CRO.4 NGJOTHROMBOSIS
I*% -t -.~:
A,'n. o '
w .*
_
N -
rtO;-
I
'tt
e-It
VP
*i
4-
.. I
a
t~~~~fa ~
*.
a."~~~ ~ ~ ~ ~~~~~~~~.
:. C'.. @,
...s*:
S.d,w...'4
* .'0
?~ ~ %j
4Xd**
st
*~ ~ ~fi au-* S
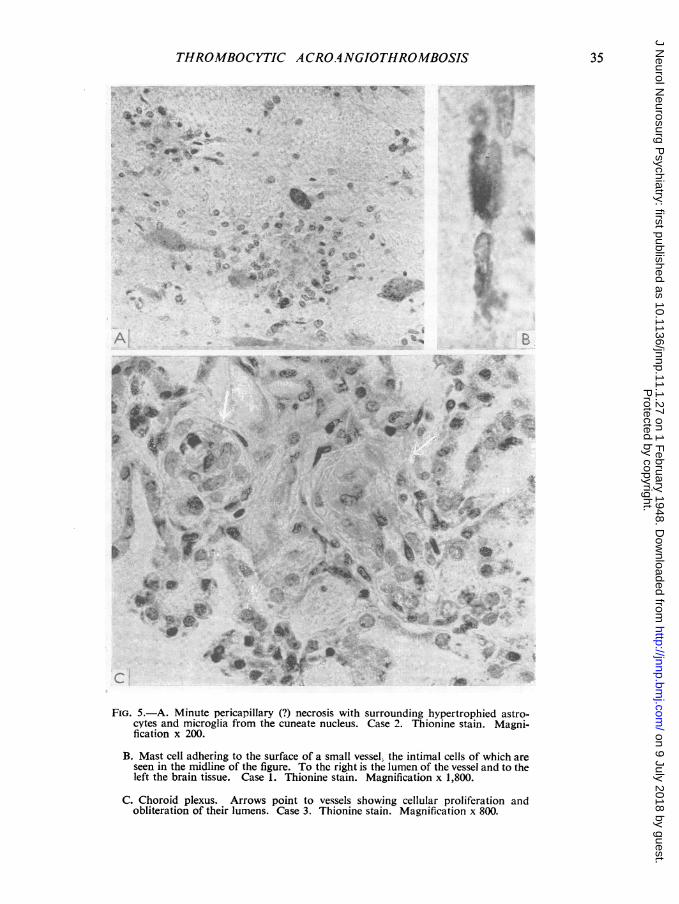
FIG. 5.-A. Minute pericapillary (?) necrosis with surrounding hypertrophied astro-
cytes and microglia from the cuneate nucleus. Case 2. Thionine stain. Magni-fication x 200.
B. Mast cell adhering to the surface of a small vessel, the intimal cells of which are
seen in the midline of the figure. To the right is the lumen of the vessel and to theleft the brain tissue. Case 1. Thionine stain. Magnification x 1,800.
C. Choroid plexus. Arrows point to vessels showing cellular proliferation andobliteration of their lumens. Case 3. Thionine stain. Magnification x 800.
*L
R
35
j.5..
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
36 RAYMOND D. ADAMS, JAN CAMMERMEYER AND PATRICK J. FITZGERALD
and tegmentum of the midbrain. The vessels passingfrom the surface of the colliculi towards the aqueductwere conspicuous on account of their cellularity andthe thrombi. One of them, an arteriole which was cutin longitudinal section, contained a thrombus in oneportion on either side of which were normally colouredred corpuscles (Fig. 3 B). Swollen astrocytes andpleomorphic microglial cells were present in the tissueadjacent to the thrombus. There were several freshperivascular and " ring " hmemorrhages (Fig. 3 D), andin some few places microglial cells were filled withhemosiderin. There was quite extensive nerve-celldestruction in these areas.
In the pons and medulla practically all the nucleishowed vascular changes, focal nerve cell loss, andclumps of astrocytes and pleomorphic microglial cells.Similar changes were found in the upper part of thecervical spinal cord and at the level of the decussationof the pyramidal tracts.NEURO-ANATOMICAL FINDINGS.-There were multiple
small vessels with endothelial proliferation; cellularendothelial reaction and thrombi; multiple smallperivascular foci of altered nerve cells; multiple small,recent and older hiemorrhages, especially in the colliculi;and diffuse glia-cell reaction in the first cortical layer.COMMENT.-The vascular and parenchymatous lesions
were of the same type as in Cases 1 and 2 but wereconsiderably older as judged by the increase in reticularconnective tissue and in one lesion many microglialphagocytes containing hmemosiderin. The latter repre-sents a reaction to hmemorrhage that was probablyten to twelve days old and correlates well with theclinical exacerbation which occurred at that time.
Case 4 (Case III of Fitzgerald and others, 1947).-The patient was a 28-year-old white man who had hadrheumatic fever at the age of 12 years and had beenrejected by the army in 1941 because of cardiac murmurs.Since 1943 he had been subject to frequent attacks ofprecordial pain, palpitation, and occasionally faintingspells. In February, 1947, five weeks before admissionto the hospital, he began to have mild pains in bothknees; there was no redness or swelling of these joints.Four weeks later he had fever and chills, cough, andback pain. A dull, generalized headache began shortlyafterwards. Sulphadiazene was given two days beforeentry to the hospital. On the following day he vomitedclotted blood, had a severe epistaxis, and voided urineof red colour. A rash appeared over the face and neck.Once before the patient had taken sulphadiazene
without untoward reaction. He had not been exposedto other toxic drugs, such as benzene, inorganic solvents,or fava beans.EXAMINATIQN.-The temperature was 990 F., the pulse
88, the respiration 20, and the blood pressure 114 mm.Hg systolic and 76 diastolic. The patient was lethargic,but when aroused responded appropriately to questions.There were petechial hemorrhages in the skin over theface, and in the oral mucous membranes and conjunc-tiwe. The cervical, axillary, and inguinal lymph nodeswere slightly enlarged. The heart was of normal sizeand the rhythm was regular but there were apical systolic
and diastolic murmurs and an aortic systolic murmur.The liver and spleen were not palpable. No abnormalneurological signs were present.
LABORATORY DATA.-The urine was normal. Thehemoglobin was 7 g., the red cell count 2-3 millionper 100 c.mm. of blood, the white cell count 11,650with 86 per cent. neutrophils, 11 per cent. lymphocytes,and 3 per cent. monocytes. The hematocrit was 17.The bleeding and clotting times were normal. Theplatelets numbered less than 50,000. The blood culturewas negative. The electrocardiogram was normal.
COURSE IN HOSPITAL.-The patient remained drowsyuntil the fourth hospital day, when he was seized withseveral generalized convulsions during which the headand eyes turned to the left. He was confused forseveral hours after the seizures, and during this timehis temperature rose to 1030 F. Penicillin was givenin a dosage of 100,000 units every three hours. On theeighth hospital day he went into status epilepticus whichcould be controlled only by large doses of paraldehyde,given intramuscularly. Following this the patientremained comatose. No other abnormal neurologicalfindings were noted. His cerebrospinal fluid was undera pressure of 110 mm., was clear and colourless, andcontained no cells and a protein of only 26 mg. He wastransfused with whole blood several times and his redcell count rose to 3 5 million. However, the comapersisted and he died on the twelfth day in hospital,or thirteen days after the first symptoms of hemorrhagicdiathesis.ANATOMICAL DLAGNOSIS.-There were multiple thrombi
in the arterioles, capillaries, and venules in the heart,kidney, bone marrow, and brain; petechial hxemorrhagesin the heart and brain; multiple foci of necrosis in theheart and brain; multinucleated giant cells in thecapillaries of the lung; hyperplasia of the bone marrow;and diffuse myocardial fibrosis of moderate degree.NEUROPATHOLOGICAL FINDINGS.-Three or four pete-
chial hemorrhages were visible on the surface of thecerebral and cerebellar hemispheres, and about 20more in the form of discrete round heemorrhages,1 to 2 mm. in diameter, were seen in the cortex, basalganglia, and substantia nigra when the formalin-fixedbrain was sectioned.There were moderate numbers of astrocytes with
visible cytoplasm and elongated microglial cells in themarginal layers of the cerebral cortex. Arterioles,capillaries, and possibly small veins were exceedinglycellular and were in some places filled with red corpusclesand white blood cells and in others occluded by homo-geneous or slightly granular masses.The cells in the vessel walls had an elongated, thin
cytoplasmic body and were arranged concentricallyaround the lumen. The most centrally placed cells hadlarge multiformed nuclei and more abundant cytoplasm.Both the endothelial and adventitial cells appeared tohave undergone hyperplasia. Sometimes the thrombushad retracted from the vessel wall, and the detachedsurface was covered by a thin basophilic process of anendothelial cell. In places where an arteriole was
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
THROMBOCYTIC ACROANGIOTHROMBOSIS
fortuitously cut in longitudinal section the mural cellu-larity and thrombosis could be traced past a bifurcationof the vessel into capillaries for a short distance (Fig. 3 A).Basophilic granules were seen in the cytoplasm ofsome cells of the vessel wall. An occasional mitoticfigure was found. A few lymphocytes, mononuclearcells, and neutrophilic leucocytes had infiltrated the wallor the perivascular space of the affected vessels.Some of the nerve cells and glia-cell nuclei immediately
adjacent to the affected vessels were pale or in someplaces the neurones had disappeared. There were afew swollen astrocyte nuclei in some of these foci,and in one of them many pleomorphic microglial cellsas well (Fig. 3 c). In rare instances damaged bloodvessels were surrounded by " ring " hlmorrhages. Thenerve cells were preserved in Sommer's sector ofAmmon's horn.A Loyez-stained section from the mesencephalon
demonstrated the loss of a few myelinated fibres nextto the most severely damaged vessels (Fig. 4 A, B,and c).The vascular lesions were quite pronounced in the
putamen and less so in the globus pallidus, thalamus,caudate nucleus, paraventricular hypothalamic nucleus,and substantia innominata (Fig. 2 D), in the substantianigra, the abducens, inferior olivary, and magnocellularpart of the lateral reticular nuclei, and the superiorcerebellar peduncle and dentate nucleus. In the brainstem there was a slight diffuse increase in astrocytesand microglial cells and also several minute foci ofswollen astrocytes and pleomorphic microglial cells.In the walls of many of the arteries in the pallidumthere was a deposition of basophilic material; some ofthese vessels also showed cellular hyperplasia andthrombosis. In one focus in the dorsal part of thesuperior cerebellar peduncle all the vessels were damagedin a quite large area (Fig. 4 A, B, c), and the interveningnerve and glia cells were shrunken and pyknotic, whilethe myelinated fibres were damaged (Fig. 4 D).
In the choroid plexus of the lateral ventricles therewere a few arterioles or small arteries which showed 'aslight but definitegllular hyperplasia. At the base ofthe brain a few meningeal arteries showed a slightproliferation of endothelial cells but no other changes.The subependymal glia had multiplied focally near thefourth ventricle, the aqueduct of Sylvius, and the lateralventricle.NEURO-ANATOMICAL FiNDINGs-There were multiple
small vessels with endothelial -proliferation and plateletthrombi; multiple small perivascular foci of partial orcomplete necrosis in the cerebral cortex and brain stem;several old foci of isch.emic necrosis in the cerebralcortex; diffuse glia-cell hyperplasia in first corticallayer, subependymal zone, and brain-stem nuclei; anda few petechial haemorrhages.CoMMENT.-All the damaged vessels in the brain did
not show the same degree of reaction; some of themexhibited only a markedly increased cellularity, andothers were partly or completely occluded by thrombiwithout any cellular reaction. In comparison to themyocardial lesions there was in the brain a more pro-nounced cellular. reaction and considerably fewer
F
hemorrhages. Some of the lesions in the brain weremild and acute, whereas others, in which a definite gliatreaction was demonstrable, must have been of one ortwo weeks' duration. Presumably these older lesionscoincided approximately with the progression of symp-toms thirteen days before the patient's death.
DiscussionSymptomatology.-Although subject to consider-
able variation, the clinical picture of this disease,as formulated from all of the published cases,tended to follow a recognizable pattern. Usuallyit presented three main features: the signs ofh"emorrhagic disease, severe anmmia, and neuro-logical symptoms.Both sexes were affected, female more often than
male. The disease was somewhat more commonin adolescents and young adults and occurred inboth white and coloured races.Some of the patients had enjoyed excellent health
before the onset, whereas others had suffered fromrheumatic fever, urticaria, or a recent upper respira-tory infection. Several of them had rather vagueprodromal symptoms, such as nausea and vomiting,weakness, malaise, and abdominal pain. Whenfirst seen the patients were, as a rule, quite paleand complaining of weakness, lassitude, vague painsin their joints, abdomen, or in other parts, or feverand chills. Usually small haemorrhages in the formof purpura, epistaxis, hiematemesis, hematuria, ormenorrhagia had already occurred. Quite soon thebleeding became more profuse, and fever, if notalready present, appeared. Neurological symptomsmost often developed at this stage of the diseasebut were occasionally present from the onset. Forthe most part they were cerebral in nature andconsisted of confusion, coma, motor paralysis, andconvulsions.The onset of symptoms was usually acute and
the course progressive with a fatal termination infrom one to eight weeks.The blood presented the appearance ofmoderately
severe anaemia with red corpuscles ranging from1-0 to 2-74 million per 100 c.mm. of blood. Thehaemoglobin was low, usually giving a colour indexof about 1X0. The white cell count was normal orelevated, with a neutrophilic leucocytosis. Instained films there was anisocytosis, polychromato-philia, and reticulocytosis. Occasionally a fewnucleated red cells and myelocytes were present.Platelets were reduced in number, usually below50,000. The Rumpel-Leede sign was present.Bleeding time was often prolonged; over 30 minutesin some cases; and, although clotting was usuallynot delayed, the coagulum retracted poorly. Ery-throcyte fragility was normal. The icteric indexranged from 8 to 25 and the quantitative Van den
37
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
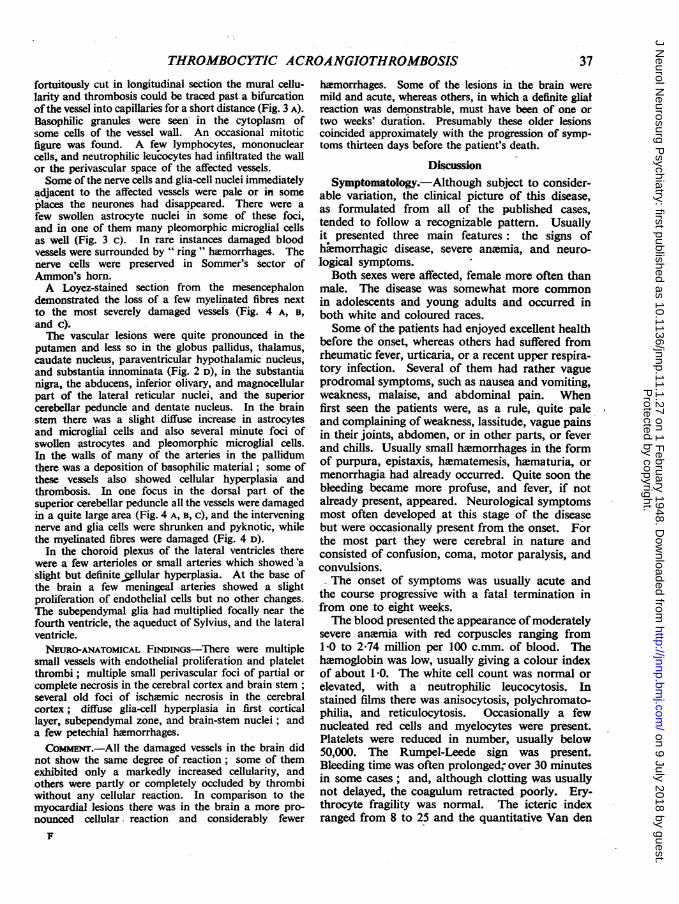
38 RAYMOND D. ADAMS, JAN CAMMEPMEYER AND -PATRICK J. FIZGERALD
SUMMARY OF CLIICAL FINDGS IN TH 13 REPoRTD CASES WIT THROMBOCYTIC ACROANGIOTHROMBOSI
Sex T T TotalCase and Age General clinical findings Neurological findings duration
colour |_ of illnass
1. Moschowitz,1925
2. Baehr,Klemperer,Schifrin, 1936
3. Baehr,Klemperer,Schifrin, 1936
4. Baehr,Klemperer,Schifn, 1936
5. Baehr,Klemperer,Schifrin, 1936
6. Gitlow andGoldmark,
1939
7. Altshule, 1942
8. Bernheim, 1943
9. Trobaugh,Markowitz,Davison, andCrowley, 1946
10. Carter, 1947
11. Engel,Schemker, andHumphrey,
1947
12. Fitzgerald,Auerbach, andFrame, 1947
13. Fitzgerald,Auerbach, andFrame 1947
14. Fitzgerald,Auerbach, andFrame, 1947
Weakness and joint pains andpallor, petechii, (?) jaundice
Listlessness, hematuria, pallorand skin purpura, retinalhimorrhages, splenomegaly
Weakness aqd pallor, icterusand petechial skin htemor-rhages
Urticaria, purpura, retinalhimorrhages, nausea andvomiting
Upper respiratory infection, pur-pura, icterus, retinal hemor-rhages
Upper respiratory infection, pur-pura, enlargement of spleenand liver
Malaise, pallor, hepatomegaly,and splenomegaly
Weakness, dermatitis, pallor,purpura
Upper respiratory. infection,icterus, and purpura
None
Sore throat, fever, malaise,purpura, hematuria, menor-rhagia, vomiting, ECGchanges; improved.
5 weeks later: recurrence ofsystemic and hiemorrhagicsymptoms
Nausea, vomiting, abdominalpain, pallor, purpura
Urticaria, faintness, epistaxis,hamatemesis, menorrhagia,pallor, hepatomegaly
Rheumatic fever, precordialpain, syncope, joint pains,chills and fever, epistaxis,hmmatemesis, hamaturia,pallor and purpura
Left hemiparesisKemig sign
None
Headache, convulsions
Delirium and stupor
Right hemiparesis,coma
Right hemiparesis,coma
Confusion, left facialweakness, delirium
Left facial weakness,hemianwtthesia,con-vulsions
Restlessness, stupor,coma
Confusion, aphasia,unequal tendon re-flexes, right Babinski,coma
Blurred vision, head-ache, delirium
Coma, deviation ofhead and eyes toright, left hemipare-sis, right facial weak-ness, flaccid para-plegia
Restlessness,confusion, and coma
Stupor, coma
Status epilepticus,confusion, coma
14 days
7 weeks
2 months
9 days
2 weeks
18 days
13 days
2 weeks
15 days
12 days
50 days
7 days
5 weeks
I week
2 weeks
F,W
F,W
F,W
F,W
F,W
F,W
F,W
F,W
M,W
M,C
F,C.
M,W_
F,C
M,W
16
9.5
18
22
48
18
50
33
24
66
15
24
27
28
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from

THROMBOCYTIC ACROANGIOTHROMBOSIS
Bergh analyses from 0 5 to 2;5 mg. The cerebro-spinal fluid was normal in the three cases in whichit was examined.As shown in the Table, twelve of the thirteen cases
had neurological symptoms at some stage of thedisease. Some alteration in the state of conscious-ness was most frequent. This was variously desig-nated in the records as irrationality, restlessness,confusion, delirium, stupor, or coma. It usuallybegan with confusion and progressed terminally tocoma. The latter was a sign therefore of graveprognostic import; once coma set in, death alwaysfollowed within a few days.Motor paralysis was observed in seven of the
fourteen cases. The paralysis was not complete inany of them. In five of the seven there was ahemiparesis with involvement of face, arm, and leg,and diminished tendon and abdominal reflexes anda Babinski sign on the side of the weakness. Inthree cases a facial weakness was present, but fromthe meagre descriptions in the records one couldnot decide whether it was due to involvement of thefacial nucleus or nerve or to a supranuclear lesion..
Seizures occurred in three cases. They weregeneralized in each instance, and in one case wenton to status epilepticus which undoubtedly con-tributed to death. Focal or unilateral convulsionswere not observed, which is rather surprising inview of the focal character of certain other neuro-logical findings.
Less frequent findings were a left hemianmsthesiaand deviation of the head and eyes to right as inBernheim's case (1943); the latter finding was alsopresent in the case of Engel and others (1947).In the case reported by Carter (1947) there wasagrammatism, acoustic and verbal agnosia, andideokinetic apraxia, but inasmuch as the patientwas both confused and aphasic the validity of someof these interpretations of the mental state nmightbe questioned.Evidence of spinal cord or possibly peripheral
nerve damage was observed in only three cases.The second of Fitzgerald's cases had nuchal rigidityand absent knee jerks, the case of Engel and othershad a flaccid paraplegia, and in Carter's case therewere at times hypoactive knee jerks, absent anklejerks, diminished pain and touch sensation in thelegs, and diminished temperature sensation in allfour extremities but no motor weakness. As statedabove, Carter's patient was confused and aphasicand some of the signs were probably notdependable.
Central Nervous System Lesions.-In the presentmaterial the outstanding neuropathological changeswere (a) cellular hyperplasia, endothelial and
probably adventitial, of arterioles, capillaries, andvenules; (b) thrombi of agglutinated platelets inarterioles, capillaries, and venules of cerebral cortex,basal ganglia, and brain-stem nuclei; (c) foci ofnerve cell damage and in places glial proliferation;(d) petechial himorrhages.The character of the vascular change has already
been described in the case summaries. An excessivecellularity of the arterioles, capillaries, and venulesand an increase in their total diameter were themost noticeable findings in himatoxylin-eosin andthionine stains (Fig. 1 A). It was not alwayspossible to be sure of the exact identity of thesecells. Those nearest the lumen had rather pale,indented nuclei and moderate amounts of basophiliccytoplasm and were abnormally oriented to thevessel, some encircling and narrowing the lumenand others traversing the lumen and dividing it.In Cases 2 and 4 a few mitotic figures were found.The outer cells in the vessel wall were more elongated,had more heavily chromatinized nuclei and, inCase 1, granules of lipofuscin in their cytoplasm.Occasionally a few lymphocytes, a neutrophilicleucocyte, or an unidentified mononuclear cell wereinterspersed between these cells. In silver stainsfor reticular connective tissue there was in somevessels a slight increase in argentophilic fibrilseither separating the proliferating cells or extendingoutward from the adventitia. In van Gieson stainssome of these fibres were faintly fuchsinophilic.All stages of vascular changes could be demonstratedin each individual case (Fig. 2 A, B, and c).The arterioles, capillaries, and venules were
occluded by thrombi which on differential stainingappeared to be masses of agglutinated platelets.In the phosphotungstic acid haematoxylin stain thethrombi were a pale brown and no fibroglia werepresent. Weigert's stain for fibrin coloured thethrombi a dull grey, and in this and the phospho-tungstic acid haematoxylin stain only an occasionalbluish strand of fibrin was present. With Mallory'saniline blue stain the thrombi were a lavendercolour and no fibrillar elements could be seen.In reticulum stains no argentophilic fibrils wereseen within the thrombi. In Giemsa stain (Wol-bach's modification) the thrombi were pale grey toblue. The earlier lesions stained a dark blue, olderones a greyish-blue, and no red colour was apparentin either. In the normal vessels between redcorpuscles and leucocytes fine granules of aboutthe size of normal platelets also stained a bluishcolour. The van Gieson stain gave a pink colourto the thrombi, whereas the red blood corpuscleswere yellow. No bacteria or inclusion bodiescould be seen. HWmoglobin stains showed thethrombi to be a red or brownish-red in contrast
39
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
40 RAYMOND D. ADAMS, JAN CAMMERMEYER AND PATRICK J. FITZGERALD
to the olive green or green of the red blood cor-
puscles.. From these studies it was concluded thatthe thrombi were composed of agglutinated plateletsand not of erythrocytes, leucocytes, fibrin, heemo-siderin, or hvmoglobin. The failure ofthe plateletsto appear as reddish bodies with bluish granules inthe Giemsa stain does not disprove this possibility.Platelets often disintegrate so rapidly in post-mortemmaterial that they cannot be identified by specificstains.The blood vessels which were involved in this
pathological process were the arterioles, capillaries,and possibly venules of the grey matter. In sectionswhere the vessels could be followed for a distancein longitudinal section both the cellular reactionand the thromboses were restricted to a portion ofthe vessel extending for a short distance into thebranching capillaries. In the cases of longerduration there was a tendency for larger veins tobecome thrombosed.
Cases 1 and 2 presented the "earliest" reactionand Cases 3 and 4 the " oldest" changes (seepage 41). In the latter cases, however, it was
possible to find vascular lesions of all different ages,indicating that the process had continued over theentire period of the illness. In Cases 2 and 4 one
or two small arteries in the leptomeninges had beeninvolved.Damage to parenchyma, although present in
every case, was slight. Alteration of some of thenerve cells in small foci around the thrombosedvessels was the usual finding. Even in the oldestlesions the change in the neurones was not com-
mensurate with longstanding vascular occlusion(Fig. 3 A). The nerve cells had seldom undergonecomplete disintegration: they were usually faintlystained, with a pale bluish cytoplasm and nucleus.In some foci there were a few enlarged astrocytesand elongated or pleomorphic microglial cells. ByLoyez myelin stains and Gros-Bielschowsky axiscylinder stain it has not been possible to demonstrateany massive destruction of myelinated fibres or axiscylinders next to the altered blood vessels, but therewas some demyelination (Fig. 4 A, B, C). In thebrain stem there were a few larger foci with necrosisof nervous tissue and a more marked glial reaction(Fig. 4 D, and Fig. 5 A).
Pe4echial hvmorrhages were found in all ourfour cases. They were easily visible to the nakedeye in Case 4, and mistaken for congested bloodvessels in Cases 2 and 3. In Cases 2 and 4 they weremore numerous in the midbrain than elsewhere.They ranged in size from a fraction of a mm. to 2-0mm., and at most numbered 25 or 30 in all*.
* An exception was the case of Alen, in which a large brainhamorrhage was the cause of death.
Unlike some other types of brain purpura they werefor the most part confined to the cortical grey matter,basal ganglia, and brain stem. Only a few wereseen in white matter. In microscopic sections thehemorrhages were discrete and of two types,-perivascular, and ring-shaped around a necroticcentre. Usually they were in close relationship todamaged vessels. Sometimes an altered vessel orcluster of histiocytes were situated in the centre of aring haemorrhage. In older lesions there was awell-marked proliferation of pleomorphic microglialcells amongst which pale red corpuscles and swollenastrocytes were visible. Microglial phagocytescontaining himosiderin pigment were noted inCase 3. Wherever the reaction of glial cells wasintense, evidences of hamorrhage could usuallybe found.
In the case in which the neurological symptomswere of briefest duration there were mast cells inthe adventitia of the walls of damaged vessels(Fig. 5 B). This finding was of interest when viewedin the light of the recent discovery of Jorpes and,others (1937), Holmgren (1940), and Sylven (1945),that the mast cell contains and secretes heparin.Conceivably they constituted in our case a reactionof the organism to thrombosis of small vessels.In the other three cases some of the outer cells inthe vessel wall had a " basophilic," metachromatic,or slightly hyperchromatic cytoplasm in thioninerstained sections but no true mast cells were present.The exact nature and purpose of these cells couldnot be ascertained.The distribution of the vascular and the paren-
chymal lesions were fairly uniform in each of thefour cases. For the most part they occurred ingrey matter and not the white. In the cerebralcortex the second to fourth layers were affectedmore than the others. Changes of the same typewere found in the grey matter of the caudate andlenticular nuclei, the thalamus, hypothalamus, andsubthalamus and nuclear structures of the midbrain,pons, and medulla and to a lesser degree the greymatter of the cerebellum. Definite vascular abnor-malities were found in the vessels of the choroidplexus in two cases (Fig. 5 c) and questionably insubarachnoid, vessels of two cases.
It was difficult to determine the age of the vascularchanges because, as this is a new type of pathologicreaction, one dare not use as a standard of com-parison the general pathological concepts of tissuereaction to injury. From a study of. our materialand previously published cases we have, beenimpressed by the fact that all lesions were in aboutthe same stages of development and were ofrelatively uniform character. Even in those casesin which the disease had been present for the longest
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
THROMBOCYTIC ACROANGIOTHROMBOSIS
period of time, the vascular changes in the brain,as well as other organs, did not appear to be muchmore advanced than in the cases of shortest dura-tion. However, within rather narrow limits slightindividual differences between cases could bedetected. As judged by the degree of glial reactionto parenchymal damage and the proliferation ofcells in the vessel wall our Cases 1 and 2 presenteda somewhat earlier reaction than Cases 3 and 4.In all of these cases the brain lesions seemed tocorrelate best with symptoms of the terminal phasesof the disease, that is, with the acute onset of thehemorrhagic diathesis or the exacerbation of theillness.The significance of the fibrotic thickening of the
meninges, and the gliosis in the marginal layer ofcerebral cortex, in the inferior olivary nuclei, andsometimes in other nuclear structures is doubtful.These changes are not specific and were of suchcharacter as to have preceded the acute illness underconsideration.
A:tiology and Pathogenesis.-The cause of thisdisease is as yet unknown. Moschowitz was ofthe opinion that the thrombi were of the hyalinetype and made up ofcompact masses oferythrocytes.Baehr and his associates formulated the hypothesisthat the disease was the result of sensitization of thevascular endothelium with secondary plateletthrombosis, and of lthrombopenia due to thewithdrawal of platelets from the circulation. Theypointed out the resemblance between the vascularlesions in this disease and those which occurred inthe veins in the Schwartzman phenomenon. Thefact that two of our cases (1 and 4) had had allergicmanifestations, as did the case of Engel and others,gives some support to this hypothesis. Appertainingto the matter of sensitivity it is of interest that threeof 'the thirteen reported cases have had urticaria.The absence of inflammatory exudate, bacteria,
or inclusion bodies rules out most infectious agents.The possibility of a bacterial or other toxin actingon the endothelium cannot be as readily dismissed.On the experimental side Kielanowski and Selzer(1937) have demonstrated platelet thrombosis inthe vessels of rabbits after the intradermal injectionof B. coli culture filtrate. This reaction was,however, accompanied by infiltration of neutro-philic leucocytes in the vessel wall, which occurred-only in slight degree in our Cases 2, 3, and 4. Alsoit has been shown by Dameshek and Miller (1946)that the injection of colloidal particles into animalswill produce agglutination of platelets and severethrombopenia.We agree with Baehr and his associates and with
subsequent writers on this subject, that the thrombi
are probably composed of platelets. This con-clusion is arrived at partly by the exclusion byspecial stains of other blood elements in the thrombiand not by the positive staining of platelets, whichis very- difficult in post-mortem material.The relation of the thrombi to ftie vascular
proliferation could not be settled with finality. Inevery case there were many cellular vessels whichwere not thrombosed and also thrombosed vesselswithout cellular hyperplasia. From available evi-dence we find it impossible to decide whetherthrombosis or endothelial proliferation is theprimary event.
Relation of Neurological Symptoms to BrainLesions.-Our four cases did not have the kind ofneurological symptoms that lend themselves toexact clinico-anatomical correlation. The con-fusion, stupor, coma, and convulsions were indicativeof a widespread disorder of the cerebral cortexand basal ganglia and could be related to thewidespread vascular damage in these parts of thebrain. In those cases showing perivascular necrosisand hemorrhage in the nuclei of the brain stemthere had been no symptoms pointing to damage ofthese structures. In all probability the lesions werein these cases too small and widely scattered to causefocal neurological symptoms. Perhaps in thosecases previously reported in which aphasia, hemi-paresis, facial weakness, etc., had occurred there wasunusually severe affection of the blood vessels inone region so as to produce a much lArger focus ofischaemic necrosis similar to that in the tegmentumof the midbrain in our Case 4. In neither our .casenor that of Bernheim in which generalized convul-sions occurred was it possible to find the " pseudo-laminar degeneration" of cortex -which has beenobserved in some cases of epilepsy.
Differentiation as a Disease Entity.-From theclinical point of view thrombocytic acroangio-thrombosis must be distinguished from idiopathicthrombocytopenic purpura, other acute diseases inwhich there is a hemorrhagic tendency, and diffusevascular disease, particularly disseminated lupuserythematosus, subacute bacterial endocarditis, andacute hemorrhagic encephalitis.We have studied the pathological material from
six cases of idiopathic thrombocytopenic purpura,some of which had been presented by Nickersonand Sunderland (1937) and were unable to find anyvascular hyperplasia or thrombosis of the type whichoccurs in thrombocytic acroangiothrombosis. Themarked anmmia so often seen in the platelet throm-bosis cases is not usually found in Werlhof's syn-drome. Also, there are important clinical differ-ences inasmuch as frequency ofsymptoms ofcerebral
41
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
42 RAYMOND D. ADAMS, JAN CAMMERMEYER AND PATRICK J. JGERALD
disorder in Werlhof's syndrome is much lower,estimated at about 15 per cent., and when presentare almost always related to hiamorrhage into thebrain and spinal cord or the meninges (Weisfuse;see footnote page 40).The pathological findings in " allergic" purpura
and in disseminated vascular disease, that is,post-exanthematous encephalomyelitis, disseminatedlupus erythematosus, and periarteritis nodosa, differfrom those of the disease under consideration inregard to the brain. In our cases oflupus erythema-tosus the most striking brain lesions were embolicand were secondary to Libman-Sachs type ofverrucous endocarditis. In many respects theyresembled the focal necroses in Engels and others'case. Furthermore the subarachnoid arteries were
occluded, whereas in thrombocytic acroangio-thrombosis the small vessels in the grey matter were
exclusively involved. In our cases of lupuserythematosus fibrinoid necrosis of connectivetissue and vascular thrombosis or hyperplasia ofendothelial cells were not present in the brain. Theclose relationship of platelet thrombosis and lupuserythematosus and rheumatic fever cannot be denied,but until more is known of the aetiology of thesediseases they must be separated.On morphological grounds alone the occurrence
of petechial hzmorrhages in the brain requires thatone consider such diseases as pericapillary encepha-lorrhagia (acute haemorrhagic encephalitis or hemor-rhagic leucoencephalitis), post-exanthematousencephalomyelitis, fat embolism, and other varietiesof brain purpura. So little is known about acutehamorrhagic encephalitis that it is difficult toconstruct a clear concept of its clinical and patho-logical features. Some cases have apparentfy beenthe result of the administration of arsenic or someother compound, whereas others have occurredin the course of a virus pneumonia, influenza, or
without known antecedents. The outstandingclinical symptoms have been stupor, coma, andconvulsions. The cerebrospinal fluid has beennormal. At autopsy myriads of petechial haemor-rhages were widely disseminated through thecerebral white matter and to a lesser extent in thewhite matter of the brain stem. Unlike thrombo-cytic acroangiothrombosis there have been noh.emorrhages in the skin or other organs, anxmia,or thrombopenia, and the vascular lesions of thebrain are dissimilar. Other types of brain purpuraand post-exanthematous encephalomyelitis can bereadily distinguished by histopathological examina-tion.
It should be pointed out that one of the uniqueand distinctive pathological features of thrombo-cytic acroangiothrombosis is -the occurrence of
prominent vascular lesions with only slight paren-chymal lesions. The discrepancy between themarked vascular reaction and the slight parenchymalchange was quite remarkable. By comparison thedegree of tissue damage was much less than incerebral fat embolism where vessels of similar sizemay be occluded. The most likely explanations ofthis discrepancy are that platelet thrombosisoccurred slowly, so that adequate collateral circula-tion could be established; and that the occlusionwas in many vessels incomplete. Undoubtedlymany of the thrombi formed shortly before deathso that there was insufficient time for tissue necrosisto become manifest.
Since the real cause and pathogenesis of plateletthrombosis are unknown, one of us (P.F.) hassuggested the descriptive term thrombocytic acro-angiothrombosis. " This term designates the loca-tion of the lesion (acro-terminal, angio-vessel),states the nature of the process (thrombosis-plugingof a blood vessel by clot), and identifies the chiefconstituents of the thrombus (thrombocytes orplatelets)" (Fitzgerald and others, 1947).
SummaryThe neurological and neuropathological findings
in four cases of thrombocytic acroangiothrombosisare presented. This is a rare disease of unknownEetiology which begins acutely, runs a rapidlyprogressive course, and usually causes death in afew days or weeks. The leading clinical featureswere fever, purpura, anemia, thrombopenia, andsymptoms of cerebral disorder such as muscularweakness, hemiplegia, convulsions, confusion,stupor, and coma. The cerebrospinal fliid wasnormal. The most important pathological changeswere a striking increase in cellularity of the walls ofarterioles and capillaries and thrombi of platelets.These vascular abnormalities were quite pronouncedin the brain of each of the four cases, and weresometimes associated with multiple small foci ofparenchymal necrosis and petechial heemorrhages.The neurological data of fourteen reported cases
are summarized.Clinically the disease must be distinguished from
idiopathic thrombopenic purpura, disseminatedlupus erythematosus, subacute bacterial endo-carditis, and rickettsial diseases. This usually ispossible by taking into consideration the totalclinical picture and the laboratory data. Thediagnosis of the disease can probably be establishedby bone-marrow biopsy in which platelet thrombiand vascular hyperplasia can often be seen. Thebrain lesions are believed to represent a uniquepicture unlike any other neuropathological type ofreaction to disease.
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from
THROMBOCYTIC ACROANGIOTHROMBO.IS
REFERENCESAllen, A. C. Personal Communication.Altschule, M. D. (1942). New Engl. J. Med., 227,477.Baehr, G., Klemperer, P., and Schifrin, A. (1936).
Trans. Ass. Amer. Phys., 51, 43.Bemheim, A. I. (1943). J. Mt. Sinai Hosp., 10, 287.Carter, J. R. (1947). Amer. J. med. Sci., 213, 585.'Dameshek, W., and Miller, E. B. (1946). Blood, 1, 27.Engel, G. L., Scheinker, I. M., and Humphrey, D. C.
(1947). Ann. intern. Med., 26, 919.Fitzgerald, P. J., Auerbach, O., and Frame, E. (1947).In the press.
Gitlow, S., and Goldmark, C. (1939). Ann. intern. Med.,13, 1046.
Holmgren, Hj. (1940). Z. mikr. -anat. Forsc., 47, 489.Jorpes, E., Holmgren, Hj., and Wilander, 0. (1937).
Ibid., 42, 279.Kielanowski, T., and Selzer, A., Quot. from G. Schwartz-man, (1937). " Phenomenon of Local Tissue Reac-tivity." Paul B. Hoeber. New York.
Moschowitz, E. (1925). Arch. intern. Med., 36, 89.Nickerson, D. A., and Sunderland, D. A. (1937). Amer.
J. Path., 13, 463.Sylven, D. (1945). Acta radiol., Suppl., 59, 99.Trobaugh, F. E., Markowitz, M., Davidson, C. S., and
Crowley, W. F. (1946). Arch. Path., 41, 327.Weisfuse, L. Personal Communication.
43
Protected by copyright.
on 9 July 2018 by guest.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.11.1.27 on 1 F
ebruary 1948. Dow
nloaded from





















![Vegetative postencephalitic syndromes - JNNP’s ambition ...jnnp.bmj.com/content/jnnp/s1-7/27/248.full.pdf · SENSORIMOTOR NEUROLOGY. [143] Tumours ofthe frontal lobe ... scrupulosity,](https://img.pdfslide.net/doc/110x75/5ada19d77f8b9a137f8cff6b/vegetative-postencephalitic-syndromes-jnnps-ambition-jnnpbmjcomcontentjnnps1-727248fullpdfsensorimotor.jpg)







