Embed Size (px)
Citation preview

AMSRJ 2015 Volume 2, Number 148
BRIEFRE
PORT
S
Hereditary Hemorrhagic Telangiectasia (HHT)is a disease defined by abnormal endothelial celldevelopment thatmanifests as cutaneous telang-iectasias, recurrent epistaxis, and visceral organarteriovenous malformations. This report’s ob-jective is to exhibit a unique presentation of anuncommon disease within the pediatric popula-tion. It also provides excellent educational valuethrough prioritizing the investigation of alterna-tive diagnoses in a pediatric patient who devel-ops a brain abscess without any known risk fac-tors. Herein we report the case of a previouslyhealthy 17-year-old female who developed sud-den aphasia and a newonset tonic-clonic seizureafter 3 days of headache and shortness of breath.She had a past medical history of migraines andrecurrent epistaxis. Imaging confirmed a ring-enhancing lesion in her frontal lobe, which sug-gested a brain abscess. She was treated with in-travenous antibiotics and steroids. Her neuro-logical symptoms subsided and she was dis-
charged home. Continuedwork-up revealed nu-merous arteriovenous malformations, whichlikely contributed to her brain abscess, and shewas diagnosed with HHT. HHT should be sus-pected in pediatric patients who develop brainabscesswithout anyother risk factors.Addition-ally, new onset neurological symptoms in pedi-atric patients should be investigated promptlywith head imaging. Timely identification andinitiation of therapy is crucial due to the highmorbidity and mortality associated with brainabscess, especially in HHT patients.
A 17-year-old female was transported to theemergency department after suffering from asudden episode of inability to speak followed bya single seizure episode at school. While in herclassroom, she reported a difficulty “findingwords” and stood up in panic from her desk. Sheapproached the teacher to ask permission toleave the room. Unable to speak, she began towrite on a sheet of paper, but her writing soonbecame incoherent to both the teacher and toherself.Her teacher senther to thenurse’soffice,where she suffered a new-onset generalized ton-ic-clonic seizure and the emergency medical
Brain Abscess as a Manifestation of HereditaryHemorrhagic Telangiectasia in a Pediatric Patient
¹University of South Florida College of Medicine, Tampa, FL²Children’s Hospital at Lehigh Valley Health Network, Allentown, PA
Jose M. Soto, BS¹; Tibisay Villalobos, MD²
Corresponding Author: Jose M. Soto, BS, University of SouthFlorida College of Medicine, 12901 Bruce B Downs Blvd,Tampa, FL 33612.Email: [email protected] authors claim no conflicts of interest or disclosures.AMSRJ 2015; 2(1):48-53http://dx.doi.org/10.15422/amsrj.2015.05.005
ABSTRACT
CASE PRESENTATION

AMSRJ 2015 Volume 2, Number 1 49
service (EMS) was called. This seizure lasted afew minutes and resolved by the time the EMSarrived. During the seizure, she also suffered anepisode of epistaxis. She was able to communi-cate on arrival to the ED, although with somedifficulty, and stated that she had a 3-day historyof headaches and shortness of breath. She alsoreported a history of headaches since the age oftwelve. She stated her headaches usually beginwithanauraof “shimmeringprismsandconesoflights.” The pain is typically unilateral and ac-etaminophen provides some relief. Theseheadacheswere sometimes associatedwith nau-sea and mild photophobia. They typically re-solvedwith sleep. Over the last three days, how-ever, the headaches had worsened, and ibupro-fen became ineffective. She denied any recenthead trauma.
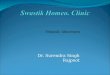
Her vital signs included a blood pressure of120/73 mmHg, heart rate of 117 beats/minute,respiratory rate of 16 breaths/minute, tempera-ture of 99.6° Fahrenheit. On exam, she appearedanxious and in mild distress. Her cranial nervesII-XII were grossly intact, and her pupils wereequally round and reactive to light. Dried bloodwas found in both of her nostrils; there was noactive bleeding. There were no meningeal signsduring her neck exam. Her cardiovascular, pul-monary, and abdominal exams were all withinnormal limits. Her neurological exam was alsogrossly normal with a Glasgow Coma Scalescore of 15, but she continued having difficulty“finding words.” A complete blood count withdifferential was drawn: hemoglobin was 14.8 g/dL, hematocrit was 45.7%, white blood cellswere 14.8 cells/mcL (71% neutrophils, 18%lymphocytes, 6% monocytes, 5% eosinophils),and platelets were 245,000/mcL. A computedtomography (CT) scan of her head without con-trast (Figure 1) showed an area of abnormallylow density in the left frontal lobe that was sug-gestive of vasogenic edema as the grey-whitematter differentiation was maintained and theedema primarily involved the white matter. No
evidence of intracranial hemorrhage was found.While air or maturing hematomas may alsocause low density on CT scans, these were ruledout due to the lack of a history of head trauma.Given the history of rapid onset neurologicsymptoms and the elevated white blood cellcount, as well as imaging that suggested an areaof edemawithout obvious intracranial bleeding,a brain abscess was suspected. Therefore, shewas admitted to the pediatric intensive care unitand started on empiric intravenous antibiotictherapy with ceftriaxone, metronidazole, andvancomycin as well as levetiracetam for seizureprophylaxis.
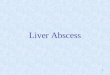
Amagnetic resonance imaging (MRI) scanwithand without contrast (Figures 2 and 3) con-firmed an area of vasogenic edema surroundinga ring-enhancing lesion in the left frontal lobe.Themidline shift seenon the earlierCTscanwasalso evident on theseMRI images. Although thedifferential diagnosis for ring-enhancing lesionsincludes glioblastoma multiforme, brain metas-tasis, infarct, contusion, and neurocysticerosis,
Figure 1. Initial CT scan taken at presentation to the hospital showing anarea suggestive of vasogenic edema in the left frontal lobe (arrow) andmild midline shift.
BRIEFREPO
RTSBRAIN ABSCESS

AMSRJ 2015 Volume 2, Number 150
thesewere ruled out due to history and age of thepatient. A follow up magnetic resonance an-giogram (MRA) of the head (Figure 4) demon-strated mass effect of the lesion on the medialcerebral artery branches on the left side, butthere was no evidence of aneurysms, arteriove-nous malformations, or major vessel occlusion.These findings were also consistent with a brainabscess.
The patient continued to have headaches and sixdays after admission, she became increasinglyconfused and developed right upper extremityweakness in addition to left facial drooping. A
Figure 2.T1-weighted coronalMRIwith contrast demonstratinga left sided ring-enhancing lesion (arrow) surrounded byvasogenic edema and also a midline shift.
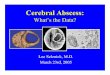
Figure 3. T2-weighted transverse MRI with contrast thathighlights the area of vasogenic edema (arrow) and also furtherdemonstrates the midline shift seen in previous images.
Figure 4. Coronal MRA of the head showing mass effect of thelesion on the branches of the left middle cerebral artery (arrow).
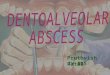
Figure 5. Repeat coronal MRI with the blue arrow pointing tothe original lesion and the red arrow pointing to the new lesion.
BRAIN ABSCESSBR
IEFRE
PORT
S

AMSRJ 2015 Volume 2, Number 1 51
repeat MRI (Figure 5) demonstrated a new areaof enhancement and diffusion restriction infero-laterally to the original lesion as well as in-creased vasogenic edema. The following day,she underwent a CT-guided biopsy of the origi-nal lesion with cultures. The tissue culture grewMicrococcus luteus/lylae. After the procedure,IV dexamethasone was added to her antibioticsto reduce brain tissue swelling. She continuedthis treatment regime for two additional weeksas her neurological symptoms began to subside.The patient was then discharged home for theremaining five weeks of IV antibiotics. Duringthis time frame, her facial palsy resolved and sheregained strength in her right upper extremity.Her headaches also improved.
During her admission, itwas discovered that shehad a past medical history significant for mi-graine headaches since the age of twelve andrecurrent episodes of epistaxis. It was also re-vealed that her mother had hereditary hemor-rhagic telangiectasia (HHT). There was a highlevel of suspicion for HHT due to family historyand recent events, so studies of the chest tosearch for pulmonary arteriovenous malforma-tions (PAVMs) aswell as a transcranialDopplerstudywere performed. Numerous PAVMswerefound in the patient’s left upper lobe aswell as inher right middle lobe (Figure 6). The transcra-nial Doppler study with agitated saline alsodemonstrated an arteriovenous shunt in themid-dle cerebral artery. The patient met 3 of the 4diagnostic Curacao criteria for HHT¹ (Table 1)and it was concluded that her undiagnosedHHThad predisposed her to this brain abscess.
The patient completed her IV antibiotic courseand followupMRIstudiesdemonstrated that thebrain abscess had resolved. The majority of thePAVMs seen on arteriogram have since beenobliterated.
Figure 6. Pulmonary arteriogram demonstrating a dominantarteriovenous malformation in the inferior aspect of the upperlobe (arrow) along with numerous smaller malformations.
Curacao Criteria for HHT
1. Recurrent Epistaxis
2. Telangiectasias
3. Visceral Manifestations
4. Affected 1st degree relative
3-4 criteria met: definitive HHT
2 criteria met: suspected HHT
1 criteria met: unlikely to be HHT
!Table 1. Curacao Criteria for the diagnosis of HHT
BRIEFREPO
RTSBRAIN ABSCESS

AMSRJ 2015 Volume 2, Number 152
Epidemiology and Pathophysiology
HHT is an autosomal dominant inherited disor-der that affects 1 in 10,000 people with no pref-erence for either sex.² It is most common in theCaucasianpopulation and is 97%penetrant.²Al-most 30%of patients do not have a family histo-ry of the disease.² The genes affected by thisdisorder both code for Transforming GrowthFactor-β receptors: ENG on chromosome9q34.1andACVRL-1 (activinAreceptor type II-like 1) on chromosome 12q13.13.³ These genesare crucial in the development of vascular en-dothelial cells during angiogenesis and eithermutation will manifest in the same manner.
Clinical Manifestations
The syndrome is defined by telangiectasias, ordilated post-capillary venules, of the skin, mu-cousmembranes and internal organs.Cutaneoustelangiectasias typically occur on the face,hands, and lips. When telangiectasias occur inthe nasal mucosa, they may cause spontaneousrecurrent epistaxis which is the first symptomformore than 90%of patients.4,5 More than 50%of patients with HHT will manifest with thissymptom before the age of twenty.¹ The bleed-ing can be so severe that 10-30%of patients willrequire blood transfusions over the course oftheir lifetime. In roughly 40% of patients, thegastrointestinal system is involved and can alsobe the source of significant blood loss.3,6
The diagnostic Curacao criteria¹ (Table 1) re-quire three of the following four findings: recur-rent epistaxis, cutaneous telangiectasias, viscer-al organ involvement (i.e., arteriovenous mal-formations thatmay bleed) and an affected first-degree relative. Few patients, however, mani-fest enough signs and symptoms within the firstthree decades of life to meet the criteria, and
therefore, it is recommended that asymptomaticchildren of HHT patients be geneticallyscreened for the disease.¹
Neurological manifestations
In a healthypatient, the lung capillary beds func-tion to filter the blood before it is pumped to thebrain, but pulmonary vascular malformations(PAVMs) found in HHT patients compromisethis protection system.7 Large PAVMs can re-sult in paradoxical micro-emboli entering cere-bral circulation and subsequent ischemic braininjury (i.e., stroke). Abscess formation can becaused by direct seeding of pathogenic bacteriainto the brain parenchyma or secondarily afteran anoxic brain injury creates an environmentsuitable for bacteria growth. About 1% of HHTpatients can develop cerebral abscess or septicmeningitis, which is significantly higher thanthe general population.7 For the reasons notedabove, PAVMs are a significant source of mor-bidity and mortality in HHT patients7 and theycan also lead to high-output cardiac failure inlater life.²
Brain abscesses are usually of poly-microbialorigin; only the slow growing members of theMicrococcusgenuswere isolated in this case be-cause empiric antimicrobial therapy had alreadybegun by the time of the biopsy.8, 9 It is importantto note that brain abscesses do not commonlypresent with the typical cardinal signs of infec-tion: fever, leukocytosis, or positive blood cul-tures.10
The neurological symptoms of brain abscessesare due in large part to the mass effect of thelesion on surrounding structures. Consequently,the symptoms can include a wide spectrum ofneurologic symptoms such as aphasia, seizures,and headaches depending on the location of thelesion. HHT patients can also develop cerebralvascular malformations (CAVMs), which canmanifest as various neurological symptoms.Approximately one-quarter of HHT patients
DISCUSSION
BRAIN ABSCESSBR
IEFRE
PORT
S

AMSRJ 2015 Volume 2, Number 1 53
will have a CAVM in their lifetime and there isa 0.5% bleeding risk per year.¹ The treatment ofchoice for arteriovenousmalformations remainsembolization of the feeding blood vessels.11
•The differential diagnosis for a pediatricpatient without any known risk factors whodevelops a brain abscess should includeHHT.
•Brain abscesses are typically poly-micro-bial in nature and do not present with theusual signsof infection, suchas fever, leuko-cytosis, or positive blood cultures.
1. Faughnan ME, Palda VA, Garcia-Tsao G, et al. Internationalguidelines for the diagnosis and management of hereditaryhaemorrhagic telangiectasia. Journal of medical genetics. 2011;48(2):73-87.
2. Daroff R, ed. Bradley's Neurology in Clinical Practice. 6th ed.Philadelphia, PA: W.B. Saunders; 2012.
3. Mark Feldman LF, Lawrence Brandt, eds. Sleisenger and Fordtran'sgastrointestinal and liver disease: pathophysiology, diagnosis,management. Philadelphia, PA: Saunders Elsevier; 2010.
4. Sadick H, Sadick M, Gotte K, et al. Hereditary hemorrhagictelangiectasia: an update on clinical manifestations and diagnosticmeasures. Wiener klinische Wochenschrift. 2006;118(3-4):72-80.
5. Murtagh B, Fulgham JR. 23-year-old woman with increasingfrequency ofmigraine headaches.MayoClinic proceedings. 2002;77(10):1105-8.
6.ChenCW, JaoSW,WuCC, et al. Red spots on the hands and red bloodin the stools. Lancet. 2008;371(9619):1190.
7. Moradi M, Adeli M. Brain abscess as the first manifestation ofpulmonary arteriovenous malformation: A case report. Advancedbiomedical research. 2014;3:28.
8. Frazier JL, Ahn ES, Jallo GI. Management of brain abscesses inchildren. Neurosurgical focus. 2008;24(6):E8.
9.SelladuraiBM,SivakumaranS,AiyarS, et al. Intracranial suppurationcaused by Micrococcus luteus. British journal of neurosurgery.1993;7(2):205-7.
10. Dong SL, Reynolds SF, Steiner IP. Brain abscess in patients withhereditary hemorrhagic telangiectasia: case report and literaturereview. The Journal of emergency medicine. 2001;20(3):247-51.
11. Meek ME, Meek JC, Beheshti MV. Management of pulmonaryarteriovenous malformations. Seminars in interventional radiology.2011;28(1):24-31.
REFERENCES
LEARNING POINTS
BRIEFREPO
RTSBRAIN ABSCESS