Embed Size (px)
Citation preview

1
Breaking Tradition
Translating Evidence into Effective Learning In all programs, Jhpiego strives for optimal provision and experience of care, as well as safe and satisfied health care providers. To realize this goal, we ensure that health care providers have the capacity to deliver evidence-based care. Traditional training through extended, offsite, group-based workshops often fails to improve health care provider performance.1 Sustained improvements are better achieved through interactive techniques, simulated practice, immediate feedback, and ongoing learning opportunities delivered at appropriate doses and frequencies.2 This brief describes 10 key principles for effective, evidence-based learning, and highlights two examples of Jhpiego programs putting these principles into action.
Limitations of Offsite, Workshop-Based Training A systematic review of interventions to improve health care provider performance in low- and middle-income countries found that traditional one-time training interventions have limited effect.3 In traditional workshop-based training, health care providers leave their workplaces for learning that is often passive and lecture-based. Simulation or direct patient care may or may not be included. Training is often lengthy: obstetric and newborn care may be taught over 2 or 3 weeks, and HIV and infectious disease trainings can be 1 or 2 weeks long. To reduce offsite training time, learners may be asked to review materials in advance, which may not be practical for busy health care providers. Offsite workshops do not reach all health care providers in a given site, and learning may not occur in the context of broader quality improvement (QI) efforts that measure improvement in clinical performance.
Benefits of an Onsite, Learner-Focused Approach Jhpiego’s literature review on effective learning4 found that interactive, practice-heavy techniques (such as clinical simulation, case-based learning, hands-on practice with anatomic models, and immediate feedback on performance) improve learning outcomes. Onsite learning may be superior for skill acquisition, and various media can be used to deliver training efficiently. Learning sequenced over time is often preferable to one-time interventions. This literature review informed a set of 10 key principles for effective learning that translates into improved performance,5 as outlined on the next page. 1 Rowe AK, Rowe SY, Vujicic M, Ross-Degnan D, Chalker J, Holloway KA, Peters DH. 2009. Review of strategies to improve health care provider performance. In: Peters, DH, El-Saharty S, Siadet B, Janovsky K, Vujicic M, eds. Improving Health Service Delivery in Developing Countries: From Evidence to Action. Washington, DC: The World Bank, 101–126. 2 Bluestone J, Johnson P, Fullerton J, Carr C, Alderman J, BonTempo J. 2013. Effective in-service training design and delivery: evidence from an integrative literature review. Hum Resour Health 11:51. doi:10.1186/1478-4491-11-51. 3 Rowe AK, Rowe SY, Peters DH, Holloway KA, Chalker J, Ross-Degnan D. 2018. Effectiveness of strategies to improve health-care provider practices in low-income and middle–income countries: a systematic review. Lancet 6(11). doi:10.1016/S2214-109X(18)30398-X. 4 Bluestone et al. 2013 5 Bluestone et al. 2013

2

3
Effective Evidence-Based Learning in Action: Case Studies from Uganda and Ghana Two country programs illustrate how applying these principles led to improved performance.
Helping Mothers Survive, Uganda With funding from Laerdal Foundation for Acute Medicine, Jhpiego created the Helping Mothers Survive (HMS) suite of learning modules to update lifesaving skills of health care teams. HMS modules include onsite, hands-on activities using learning materials and job aids to reinforce health care provider behaviors. Through short, structured sessions led by a trained peer mentor at the facility, health care providers develop skills and improve their clinical decision-making, and then move on to additional clinical topics. Ongoing clinical updates and structured reinforcement spaced over time engage the entire health care team, extending learning’s reach beyond traditional training. In 2014, recognizing that postpartum hemorrhage (PPH) can occur simultaneously with newborn asphyxia, Jhpiego paired the HMS Bleeding after Birth6 module with Helping Babies Breathe (a comparable module to address birth asphyxia) in Uganda. The goal was to sustainably build the capacity of health care providers in 125 facilities to prevent and manage PPH and birth asphyxia, and to measure improvements in health care provision and outcomes. At each facility, the entire health care team received two 1-day onsite trainings—the first for PPH, and the second 2 months later for asphyxia.
6 Evans CL, Johnson P, Bazant E, Bhatnager N, Zgambo J, Khamis AR. 2014. Competency-based training “Helping Mothers Survive: Bleeding after Birth” for providers from central and remote facilities in three countries. Int J Gynaecol Obstet. 126(3):286–290.
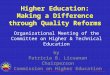
Kobusinge Lilian, a midwife, demonstrates the innovative learning material. Photo credit: Kate Holt/MCSP.

4
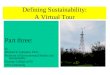
Results showed that combining onsite learning with a peer mentor to facilitate practice improved care immediately after the intervention and 6 months beyond (see Figure 1). Across all facilities, there was a 17% reduction in PPH, 47% reduction in retained placenta, 34% reduction in fresh stillbirth, and 62% reduction in early newborn death.7 Figure 1. Improved maternal health outcomes and reductions in newborn deaths and stillbirths, Uganda
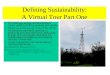
Accelerating Newborn Survival in Ghana In Ghana, Jhpiego developed a learning package and approach to improve knowledge and skills of maternal and newborn health care providers in 57 hospitals and polyclinics and in more than 50 primary health care facilities across four regions between 2013 and 2017. The learning included two 4-day interactive sessions, conducted onsite with teams of health care providers. The first session focused on normal labor and birth and the immediate postpartum period. The subsequent session, conducted a month later, concentrated on the management of complications. Learning included demonstrations, skills development with anatomic models and during clinical practice, case studies, and group work. Between learning sessions and for 11 months afterward, teams met weekly to practice on simulators with peer facilitators. In addition, regional master mentors provided onsite and mobile phone mentoring, and health care providers received SMS reminders and quizzes throughout the 1-year intervention. A rigorous quantitative and qualitative evaluation in 40 hospitals assessed health care providers’ knowledge and skill acquisition and retention after 1 year and documented the impact of learning on intrapartum stillbirth and newborn mortality within 24 hours of birth. As Figure 2 shows, across all sites and more than 100,000 deliveries, both intrapartum stillbirth and newborn death in the first 24 hours decreased by 50% and 54%, respectively.8 7 Evans CL, Bazant E, Atukunda I, Williams E, Niermeyer S, Hiner C, et al. 2018. Peer-assisted learning after onsite, low-dose, high-frequency training and practice on simulators to prevent and treat postpartum hemorrhage and neonatal asphyxia: a pragmatic trial in 12 districts in Uganda. PLoS One 13(12):e0207909. doi: 10.1371/journal.pone.0207909. 8 Gomez PP, Nelson AR, Asiedu A, Addo E, Agbodza D, Allen C, et al. 2018. Accelerating newborn survival in Ghana through a low-dose, high-frequency health worker training approach: a cluster randomized trial. BMC Pregnancy Childbirth 18(1):72. https://doi.org/10.1186/s12884-018-1705-5.
Figure 2. Reductions in newborn deaths and stillbirths, Ghana

5
A cost-effectiveness analysis9 determined that the approach (compared to the alternative of the status quo or “no training option”) cost $53 per disability-adjusted life year (DALY) averted. This is a highly cost-effective intervention in Ghana, where up to $1,480 is considered a feasible investment for averting one DALY (per the World Health Organization threshold value measure of country gross domestic product). In addition to this academic exercise, a practical costing analysis estimated that adapting and scaling up the approach at the district level would cost $506 per trainee. By comparison, an offsite basic emergency obstetric and newborn care training in Ghana costs an average of $901 per trainee—almost twice the cost of the new evidence-based approach. These savings enabled the Ghana Ministry of Health and Ghana Health Service to scale up this approach on their own path forward.
Additional Insights Together, results from Uganda and Ghana demonstrate the feasibility of successfully implementing evidence-based learning across a large number of facilities, health care providers, and deliveries. The two case studies provide additional insights for implementation in other countries: Design for the context. In both Uganda and Ghana, Jhpiego carefully studied the challenges, identified learning priorities, and then applied evidence-based learning principles to design the most appropriate intervention for the context. Although both projects used existing content, how they delivered the content was unique and impactful despite contextual challenges. Leverage existing capacity. In Uganda, existing district trainers led the onsite learning sessions; in Ghana, experienced health care providers were prepared as mentors to lead learning and provide follow-up support. In both countries, these individuals continued in these roles after the projects ended. Measure beyond numbers trained. Tracking “numbers trained” tells us nothing about improved performance or better quality of care for clients. We should aim to link learning interventions with impact and outcome measures to assess whether learning translates into meaningful change. Training alone will not improve quality of care. Training combined with QI efforts and coaching or supervision achieves a significantly greater effect than training alone.10 To be most effective, capacity-building of any type—including training—should be part of broader QI initiatives that assess and address gaps across the health system that are impacting performance.
9 Willcox M, Harrison H, Asiedu A, Nelson A, Gomez P, LeFevre A. 2017. Incremental cost and cost-effectiveness of low-dose, high-frequency training in basic emergency obstetric and newborn care as compared to status quo: part of a cluster randomized training intervention evaluation in Ghana. Global Health 13(1):88. doi: 10.1186/s12992-017-0313-x. 10 Rowe et al. 2018
Innovative models used onsite for demonstration and practice of new skills. Photo by: Kate Holt/MCSP.