-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
1/129
ECG RhythmInterpretation
LEVI ADRIANO SANTANA, RN
Bulacan State UniversityCollege of Nursing
Philippine Heart Association/ Philippine College of
Cardioloy
Certified BLS/ ACLS Provider
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
2/129
ECG Basics
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
3/129
Normal Impulse Conduction
Sinoatrial node
AV node
Bundle of His
Bundle Branches
Purkinje fibers
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
4/129
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
5/129
Impulse Conduction & the ECG
Sinoatrial node
AV node
Bundle of His
Bundle Branches
Purkinje fibers
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
6/129
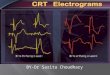
The PQRST
P wave - Atrial
depolarization
T wave - Ventricularrepolarization
QRS - Ventriculardepolarization
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
7/129
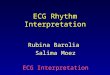
The PR Interval
Atrial depolarization
+
delay in AV junction(AV node/Bundle of His)
(delay allows time
for the atria tocontract before theventricles contract)
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
8/129
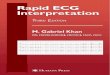
Pacemakers of the Heart
SA Node - Dominant pacemaker withan intrinsic rate of 60 -
100beats/minute.
AV Node - Back-up pacemaker withan intrinsic rate of 40 - 60
beats/minute. Ventricular cells - Back-up pacemaker
with an intrinsic rate of 20 - 45 bpm.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
9/129
The ECG Paper
Horizontally
One small box - 0.04 s
One large box - 0.20 s
Vertically
One large box - 0.5 mV
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
10/129
The ECG Paper (cont)
Every 3 seconds (15 large boxes) ismarked by a vertical
line.
This helps when calculating the heartrate.
3 sec 3 sec
l
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
11/129
How to Analyze aRhythm
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
12/129
Rhythm Analysis
Step 1: Calculate rate. Step 2: Determine regularity.
Step 3: Assess the P waves.
Step 4: Determine PR interval. Step 5: Determine QRS
duration.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
13/129
Step 1: Calculate Rate
Option 1 Count the # of R waves in a 6 second
rhythm strip, then multiply by 10.
Reminder: all rhythm strips in the
Modules are 6 seconds in length.
Interpretation?
9 x 10 = 90 bpm
3 sec 3 sec
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
14/129
Step 1: Calculate Rate
Option 2
Find a R wave that lands on a bold line.
Count the # of large boxes to the next Rwave. If the second R
wave is 1 largebox away the rate is 300, 2 boxes - 150,3 boxes -
100, 4 boxes - 75, etc. (cont)
R wave
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
15/129
Step 1: Calculate Rate
Option 2 (cont)
Memorize the sequence:
300 - 150 - 100 - 75 - 60 - 50
Interpretation?
300
150
100
75
60
50
Approx. 1 box less than
100 = 95 bpm
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
16/129
Step 2: Determine regularity
Look at the R-R distances (using a caliper
or markings on a pen or paper).
Regular (are they equidistant apart)?Occasionally irregular?
Regularly irregular?Irregularly irregular?
Interpretation?Regular
R R
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
17/129
Step 3: Assess the P waves
Are there P waves? Do the P waves all look alike?
Do the P waves occur at a regular
rate? Is there one P wave before each
QRS?Interpretation?Normal P waves with 1 P
wave for every QRS
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
18/129
Step 4: Determine PR interval
Normal: 0.12 - 0.20 seconds.(3 - 5 boxes)
Interpretation?0.12 seconds
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
19/129
Step 5: QRS duration
Normal: 0.04 - 0.12 seconds.(1 - 3 boxes)
Interpretation?
0.08 seconds
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
20/129
Rhythm Summary
Rate 90-95 bpm
Regularity regular
P waves normal
PR interval 0.12 s
QRS duration 0.08 s
Interpretation?
Normal Sinus Rhythm
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
21/129
Normal Sinus Rhythm
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
22/129
Normal Sinus Rhythm (NSR)
Etiology: the electrical impulse isformed in the SA node and
conductednormally.
This is the normal rhythm of the heart;other rhythms that do not
conduct viathe typical pathway are calledarrhythmias.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
23/129
NSR Parameters
Rate 60 - 100 bpm
Regularity regular P waves normal
PR interval 0.12 - 0.20 s
QRS duration 0.04 - 0.12 s
Any deviation from above is sinustachycardia, sinus bradycardia
or anarrhythmia
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
24/129
Arrhythmia Formation
Arrhythmias can arise from problemsin the:
Sinus node Atrial cells
AV junction
Ventricular cells
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
25/129
SA Node Problems
The SA Node can:
fire too slow
fire too fast
Sinus Bradycardia
Sinus Tachycardia
Sinus Tachycardia may be an appropriate
response to stress.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
26/129
Atrial Cell Problems
Atrial cells can:
fire occasionally
from a focus
fire continuouslydue to a loopingre-entrant circuit
Premature Atrial
Contractions (PACs)
Atrial Flutter
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
27/129
Teaching Moment
A re-entrantpathway occurswhen animpulse loopsand results
inself-
perpetuatingimpulseformation.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
28/129
Atrial Cell Problems
Atrial cells can also: fire continuously
from multiple fociorfire continuously
due to multiplemicro re-entrantwavelets
Atrial Fibrillation
Atrial Fibrillation
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
29/129
Teaching Moment
Multiple micro re-entrant wavelets
refers to wandering
small areas ofactivation whichgenerate fine chaotic
impulses. Collidingwavelets can, in turn,generate new foci
of
activation.
Atrial tissue
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
30/129
AV Junctional Problems
The AV junctioncan:
fire continuouslydue to a loopingre-entrant circuit
block impulsescoming from theSA Node
Paroxysmal
SupraventricularTachycardia
AV Junctional
Blocks
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
31/129
Ventricular Cell Problems
Ventricular cells can:
fire occasionallyfrom 1 or more
foci fire continuously
from multiple foci
fire continuouslydue to a looping
re-entrant circuit
Premature Ventricular
Contractions (PVCs)
Ventricular Fibrillation
VentricularTachycardia
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
32/129
Arrhythmias
Sinus Rhythms
Premature Beats
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
33/129
Rhythm #1
30 bpm Rate?
Regularity? regular
normal
0.10 s
P waves?
PR interval? 0.12 s
QRS duration?
Interpretation? Sinus Bradycardia
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
34/129
Sinus Bradycardia
Deviation from NSR- Rate < 60 bpm
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
35/129
Sinus Bradycardia
Etiology: SA node is depolarizingslower than normal, impulse
isconducted normally (i.e. normal PRand QRS interval).
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
36/129
Rhythm #2
130 bpm Rate?
Regularity? regular
normal
0.08 s
P waves?
PR interval? 0.16 s
QRS duration?
Interpretation? Sinus Tachycardia
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
37/129
Sinus Tachycardia
Deviation from NSR
- Rate > 100 bpm
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
38/129
Sinus Tachycardia
Etiology: SA node is depolarizingfaster than normal, impulse
isconducted normally.
Remember: sinus tachycardia is aresponse to physical or
psychologicalstress, not a primary arrhythmia.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
39/129
Premature Beats
Premature Atrial Contractions(PACs)
Premature VentricularContractions (PVCs)
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
40/129
Rhythm #3
70 bpm Rate? Regularity? occasionally irreg.
2/7 different contour
0.08 s
P waves?
PR interval? 0.14 s (except 2/7) QRS duration?
Interpretation? NSR with Premature Atrial
Contractions
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
41/129
Premature Atrial Contractions
Deviation from NSR These ectopic beats originate in the
atria (but not in the SA node),therefore the contour of the
P
wave, the PR interval, and thetiming are different than a
normallygenerated pulse from the SA node.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
42/129
Premature Atrial Contractions
Etiology: Excitation of an atrial cellforms an impulse that is
thenconducted normally through the AVnode and ventricles.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
43/129
Teaching Moment
When an impulse originatesanywhere in the atria (SA node,
atrial
cells, AV node, Bundle of His) andthen is conducted normally
throughthe ventricles, the QRS will be narrow(0.04 - 0.12 s).
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
44/129
Rhythm #4
60 bpm Rate?
Regularity? occasionally irreg.
none for 7th QRS
0.08 s (7th wide)
P waves?
PR interval? 0.14 s
QRS duration?
Interpretation? Sinus Rhythm with 1 PVC
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
45/129
PVCs
Deviation from NSR Ectopic beats originate in the ventricles
resulting in wide and bizarre QRScomplexes.
When there are more than 1 premature
beats and look alike, they are calleduniform. When they look
different, theyare called multiform.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
46/129
PVCs
Etiology: One or more ventricularcells are depolarizing and
theimpulses are abnormally conducting
through the ventricles.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
47/129
Teaching Moment
When an impulse originates in aventricle, conduction through
theventricles will be inefficient and the
QRS will be wide and bizarre.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
48/129
Ventricular Conduction
NormalSignal moves rapidlythrough the ventricles
AbnormalSignal moves slowlythrough the ventricles
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
49/129
Arrhythmias
Supraventricular Arrhythmias
Ventricular Arrhythmias
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
50/129
Rhythm #5
100 bpm Rate? Regularity? irregularly irregular
none
0.06 s
P waves?
PR interval? none
QRS duration?
Interpretation? Atrial Fibrillation
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
51/129
Atrial Fibrillation
Deviation from NSR
No organized atrial depolarization,
so no normal P waves (impulses arenot originating from the
sinusnode).
Atrial activity is chaotic (resulting inan irregularly irregular
rate).
Common, affects 2-4%, up to 5-
10% if > 80 years old
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
52/129
Atrial Fibrillation
Etiology: Recent theories suggestthat it is due to multiple
re-entrant
wavelets conducted between the R &L atria. Either way,
impulses areformed in a totally unpredictablefashion. The AV node
allows some ofthe impulses to pass through atvariable intervals (so
rhythm isirregularly irregular).
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
53/129
Rhythm #6
70 bpm Rate? Regularity? regular
flutter waves
0.06 s
P waves?
PR interval? none
QRS duration?
Interpretation? Atrial Flutter
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
54/129
Atrial Flutter
Deviation from NSR No P waves. Instead flutter waves
(note sawtooth pattern) areformed at a rate of 250 - 350
bpm.
Only some impulses conductthrough the AV node (usually
everyother impulse).
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
55/129
Atrial Flutter
Etiology: Reentrantpathway in the rightatrium with every2nd, 3rd
or 4thimpulse generating a
QRS (others areblocked in the AVnode as the
noderepolarizes).
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
56/129
Rhythm #7
74148 bpm Rate?
Regularity? Regular regular
Normal none
0.08 s
P waves?
PR interval? 0.16 s none QRS duration?
Interpretation? Paroxysmal Supraventricular
Tachycardia (PSVT)
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
57/129
PSVT
Deviation from NSR
The heart rate suddenly speeds up,often triggered by a PAC (not
seenhere) and the P waves are lost.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
58/129
PSVT
Etiology: There are several types of
PSVT but all originate above theventricles (therefore the QRS
isnarrow).
Most common: abnormal conductionin the AV node (reentrant
circuitlooping in the AV node).
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
59/129
Ventricular Arrhythmias
Ventricular Tachycardia
Ventricular Fibrillation
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
60/129
Rhythm #8
160 bpm Rate?
Regularity? regular
none
wide (> 0.12 sec)
P waves?
PR interval? none QRS duration?
Interpretation? Ventricular Tachycardia
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
61/129
Ventricular Tachycardia
Deviation from NSR
Impulse is originating in theventricles (no P waves, wide
QRS).
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
62/129
Ventricular Tachycardia
Etiology: There is a re-entrant
pathway looping in a ventricle (mostcommon cause).
Ventricular tachycardia cansometimes generate enough
cardiacoutput to produce a pulse; at othertimes no pulse can be
felt.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
63/129
Rhythm #9
none Rate?
Regularity? irregularly irreg.
none
wide, if recognizable
P waves?
PR interval? none QRS duration?
Interpretation? Ventricular Fibrillation
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
64/129
Ventricular Fibrillation
Deviation from NSR
Completely abnormal.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
65/129
Ventricular Fibrillation
Etiology: The ventricular cells areexcitable and depolarizing
randomly.
Rapid drop in cardiac output anddeath occurs if not quickly
reversed
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
66/129
Atrioventricular Nodal Blocks
1st Degree AV Block
2nd Degree AV Block, Type I
2nd Degree AV Block, Type II
3rd Degree AV Block
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
67/129
Rhythm #10
60 bpm Rate?
Regularity? regular
normal
0.08 s
P waves?
PR interval? 0.36 s QRS duration?
Interpretation? 1st Degree AV Block
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
68/129
1st Degree AV Block
Deviation from NSR
PR Interval > 0.20 s
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
69/129
1st Degree AV Block
Etiology: Prolonged conduction delayin the AV node or Bundle of
His.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
70/129
Rhythm #11
50 bpm Rate?
Regularity? regularly irregular
nl, but 4th no QRS
0.08 s
P waves?
PR interval? lengthens QRS duration?
Interpretation?2nd Degree AV Block, Type I
a.k.a. Weckebach or Mobitz I
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
71/129
2nd Degree AV Block, Type I
Deviation from NSR
PR interval progressively lengthens,then the impulse is
completelyblocked (P wave not followed by
QRS).
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
72/129
2nd Degree AV Block, Type I
Etiology: Each successive atrialimpulse encounters a longer
andlonger delay in the AV node until oneimpulse (usually the 3rd or
4th) fails
to make it through the AV node.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
73/129
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
74/129
2nd Degree AV Block, Type II
Deviation from NSR
Occasional P waves are completelyblocked (P wave not followed
byQRS).
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
75/129
2nd Degree AV Block, Type II
Etiology: Conduction is all or nothing
(no prolongation of PR interval);typically block occurs in the
Bundle ofHis.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
76/129
Rhythm #13
40 bpm Rate?
Regularity? regular
no relation to QRS
wide (> 0.12 s)
P waves?
PR interval? none QRS duration?
Interpretation?3rd Degree AV Block
a.k.a. Complete Heart Block
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
77/129
3rd Degree AV Block
Deviation from NSR
The P waves are completely blockedin the AV junction; QRS
complexesoriginate independently from below
the junction.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
78/129
3rd Degree AV Block
Etiology: There is complete block of
conduction in the AV junction, so theatria and ventricles form
impulsesindependently of each other. Without
impulses from the atria, the ventriclesown intrinsic pacemaker
kicks in ataround 30 - 45 beats/minute.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
79/129
Remember
When an impulse originates in aventricle, conduction through
theventricles will be inefficient and the
QRS will be wide and bizarre.
Diagnosing a Myocardial
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
80/129
Diagnosing a MyocardialInfarction
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
81/129
Diagnosing a MI
To diagnose a myocardial infarction youneed to go beyond looking
at a rhythmstrip and obtain a 12-Lead ECG.
Rhythm
Strip
12-Lead
ECG
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
82/129
RhythmStrip
12-Lead
ECG
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
83/129
The 12-Lead ECG
The 12-Lead ECG sees the heartfrom 12 different views.
Therefore, the 12-Lead ECG helpsyou see what is happening
indifferent portions of the heart.
The rhythm strip is only 1 ofthese 12 views.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
84/129
The 12-Leads
The 12-leads include:
3 Limb leads
(I, II, III)
3 Augmented leads(aVR, aVL, aVF)
6 Precordial leads(V1- V6)
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
85/129
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
86/129
Views of the Heart
Some leads geta good view ofthe:
Anterior portion
of the heart
Lateral portion
of the heart
Inferior portion
of the heart
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
87/129
ST Elevation
One way todiagnose anacute MI is to
look forelevation ofthe ST
segment.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
88/129
ST Elevation (cont)
Elevation of theST segment
(greater than 1small box) in 2leads isconsistent with
a myocardialinfarction.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
89/129
Anterior View of the Heart
The anterior portion of the heart isbest viewed using leads V1-
V4.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
90/129
Anterior Myocardial Infarction
If you see changes in leads V1 - V4that are consistent with
amyocardial infarction, you canconclude that it is an anterior
wallmyocardial infarction.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
91/129
Putting it all Together
Do you think this person is having amyocardial infarction. If
so, where?
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
92/129
InterpretationY thi i h i t
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
93/129
Yes, this person is having an acuteanterior wall myocardial
infarction.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
94/129
Other MI Locations
Now that you know where to look for ananterior wall myocardial
infarction letslook at how you would determine if the
MI involves the lateral wall or theinferior wall of the
heart.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
95/129
Other MI Locations
First, take a lookagain at thispicture of theheart.
Anterior portion
of the heart
Lateral portionof the heart
Inferior portion
of the heart
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
96/129
Other MI Locations
Second, remember that the 12-leads of the ECG lookat different
portions of the heart. The limb andaugmented leads see electrical
activity movinginferiorly (II, III and aVF), to the left (I, aVL)
and tothe right (aVR). Whereas, the precordial leads see
electrical activity in the posterior to anteriordirection.
Limb Leads Augmented Leads Precordial Leads
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
97/129
Other MI Locations
Now, using these 3 diagrams lets figurewhere to look for a
lateral wall and inferiorwall MI.
Limb Leads Augmented Leads Precordial Leads
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
98/129
Anterior MI
Remember the anterior portion of the heartis best viewed using
leads V1- V4.
Limb Leads Augmented Leads Precordial Leads
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
99/129
Lateral MI
So what leads do youthink the lateral portionof the heart is
bestviewed?
Limb Leads Augmented Leads Precordial Leads
Leads I, aVL, and V5- V6
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
100/129
Inferior MI
Now how about theinferior portion of theheart?
Limb Leads Augmented Leads Precordial Leads
Leads II, III and aVF
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
101/129
Putting it all Together
Now, where do you think this person ishaving a myocardial
infarction?
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
102/129
Inferior Wall MIThis is an inferior MI Note the ST
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
103/129
This is an inferior MI. Note the STelevation in leads II, III
and aVF.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
104/129
Putting it all Together
How about now?
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
105/129
Anterolateral MIThis persons MI involves both the anterior
wall
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
106/129
This persons MI involves both the anterior wall(V2-V4) and the
lateral wall (V5-V6, I, and aVL)!
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
107/129
ST Elevation and
Non-ST Elevation MIs
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
108/129
ST Elevation and non-ST Elevation MIs
When myocardial blood supply is abruptlyreduced or cut off to a
region of the heart,a sequence of injurious events occurbeginning
with ischemia (inadequate
tissue perfusion), followed by necrosis(infarction), and
eventual fibrosis(scarring) if the blood supply isn'trestored in an
appropriate period of time.
The ECG changes over time with each ofthese events
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
109/129
ECG Changes
Ways the ECG can change include:
Appearanceof pathologicQ-waves
T-waves
peaked flattened inverted
ST elevation &depression
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
110/129
ECG Changes & the Evolving MI
There are twodistinct patternsof ECG change
depending if theinfarction is:
ST Elevation(Transmural orQ-wave), or
Non-ST Elevation (Subendocardialor non-Q-wave)
Non-ST Elevation
ST Elevation
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
111/129
ST Elevation Infarction
ST depression, peaked T-waves, then T-wave inversion
The ECG changes seen with a ST elevation infarction are:
Before injury Normal ECG
ST elevation & appearance of
Q-waves
ST segments and T-waves return tonormal, but Q-waves persist
Ischemia
Infarction
Fibrosis
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
112/129
ST Elevation Infarction
Heres a diagram depicting an evolving infarction:
A. Normal ECG prior to MI
B. Ischemia from coronary artery
occlusion results in ST depression (notshown) and peaked
T-waves
C. Infarction from ongoing ischemiaresults in marked ST
elevation
D/E. Ongoing infarction with appearanceof pathologic Q-waves and
T-waveinversion
F. Fibrosis (months later) with persistentQ- waves, but normal
ST segment andT- waves
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
113/129
ST Elevation Infarction
Heres an ECG of an inferior MI:
Look at theinferior leads
(II, III, aVF).
Question:What ECGchanges doyou see?
ST elevationand Q-waves
Extra credit:What is therhythm? Atrial fibrillation (irregularly
irregular with narrow QRS)!
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
114/129
Non-ST Elevation Infarction
Heres an ECG of an inferior MI later in time:
Now what do you see in the inferior leads?
ST elevation, Q-waves and T-wave inversion
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
115/129
Non-ST Elevation Infarction
ST depression & T-waveinversion
The ECG changes seen with a non-ST elevation infarction are:
Before injury Normal ECG
ST depression & T-wave inversion
ST returns to baseline, but T-waveinversion persists
Ischemia
Infarction
Fibrosis
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
116/129
Non-ST Elevation Infarction
Heres an ECG of an evolving non-ST elevation MI:
Note the STdepressionand T-wave
inversion inleads V2-V6.
Question:What area of
the heart isinfarcting?
Anterolateral
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
117/129
Left Ventricular Hypertrophy
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
118/129
Left Ventricular Hypertrophy
Compare these two 12-lead ECGs. Whatstands out as different with
the second one?
Normal Left Ventricular Hypertrophy
Answer: The QRS complexes are very tall(increased voltage)
f l h
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
119/129
Left Ventricular Hypertrophy
Why is left ventricular hypertrophy characterized by tallQRS
complexes?
LVH ECHOcardiogramIncreased QRS voltage
As the heart muscle wall thickens there is an increase
inelectrical forces moving through the myocardium resulting
in increased QRS voltage.
f l h
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
120/129
Left Ventricular Hypertrophy
Criteria exists to diagnose LVH using a 12-lead ECG. For
example:
The R wave in V5 or V6 plus the S wave in V1 orV2 exceeds 35
mm.
However, for now, allyou need to know isthat the QRS
voltageincreases with LVH.
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
121/129
Bundle Branch Blocks
B dl B h Bl k
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
122/129
Bundle Branch Blocks
Turning our attention to bundle branchblocks
Remember normal
impulse conduction is
SA node
AV node
Bundle of His Bundle BranchesPurkinje fibers
N l I l C d ti
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
123/129
Normal Impulse Conduction
Sinoatrial node
AV node
Bundle of His
Bundle Branches
Purkinje fibers
B dl B h Bl k
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
124/129
Bundle Branch Blocks
So, depolarization ofthe Bundle Branchesand Purkinje fibersare
seen as the QRS
complex on the ECG.
Therefore, a conductionblock of the Bundle
Branches would bereflected as a change inthe QRS complex.
Right BBB
B dl B h Bl k
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
125/129
Bundle Branch Blocks
With Bundle Branch Blocks you will see two changeson the
ECG.
1. QRS complex widens(> 0.12 sec).
2. QRS morphology changes (varies depending on
ECG lead, and if it is a right vs. left bundle branchblock).
B dl B h Bl k
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
126/129
Bundle Branch Blocks
Why does the QRS complex widen?
When the conduction
pathway is blocked itwill take longer forthe electrical signalto
pass throughout
the ventricles.
Ri ht B dl B h Bl k
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
127/129
Right Bundle Branch Blocks
What QRS morphology is characteristic?
V1
For RBBB the wide QRS complex assumes aunique, virtually
diagnostic shape in those
leads overlying the right ventricle (V1 and V2).
Rabbit Ears
L ft B dl B h Bl k
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
128/129
Left Bundle Branch Blocks
What QRS morphology is characteristic?
For LBBB the wide QRS complex assumes acharacteristic change in
shape in those leads
opposite the left ventricle (right ventricularleads - V1 and
V2).
Broad,
deep Swaves
Normal
-
8/2/2019 BSU CON Basic-Advance ECG Interpretation 2012
129/129
END