Embed Size (px)
Citation preview

lable at ScienceDirect
DERMATOLOGICA SINICA 29 (2011) 94e97
Contents lists avai
Dermatologica Sinica
journal homepage: http: / /www.derm-sinica.com
CASE REPORT
Bullous pemphigoid in a chronic renal allograft rejection patient: a case reportand review of the literature
Tse-Yuan Liaw 1, Shang-Jyh Hwang 2, Daw-Yang Hwang 2, Gwo-Shing Chen 1,*
1Department of Dermatology, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan2Division of Nephrology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
a r t i c l e i n f o
Article history:Received: Aug 16, 2010Revised: Sep 29, 2010Accepted: Dec 20, 2010
Keywords:Bullous pemphigoidChronic rejectionRenal allograft transplantation
* Corresponding author. Department of DermaUniversity Hospital, 100 Tzyou 1st Road, Kaohsiung 8
E-mail address: [email protected] (G.-S. Chen
1027-8117/$ e see front matter Copyright � 2011, Tadoi:10.1016/j.dsi.2011.07.004
a b s t r a c t
Bullous pemphigoid (BP) is an autoimmune blistering disorder of the skin. Various provocative factorshave been proposed. However, BP in renal transplantation patients has scarcely been reported. Herein,we report the case of a 27-year-old man who received cadaveric renal transplantation 10 years agopresenting with bullous eruption during chronic renal allograft rejection phase, with the renal allograftbeing the possible trigger stimulus for BP development in our case. Bullous lesions were soon controlledby oral corticosteroids and did not recur after removal of the graft. The pathogenesis and management ofsuch patients will also be reviewed along with the case report.
Copyright � 2011, Taiwanese Dermatological Association.Published by Elsevier Taiwan LLC. All rights reserved.
Introduction
Bullous pemphigoid (BP) is an acquired autoimmune blisteringdermatosis with clinical features of chronic, recurrent subepi-dermal bulla formation. Various provocative factors, includingcancers, drugs, physical stimuli, and immune abnormalities, havebeen proposed.1,2 However, BP in renal transplantation patients israre.We report a case of chronic renal allograft rejection presentingwith BP and discuss the pathogenesis and management.
Case report
A 27-year-old man had end-stage renal failure because of long-term Chinese herbal medication use and received left nephrec-tomy with ambulatory peritoneal dialysis from 1997 to 1999. Hethen received cadaveric renal transplantation in Mainland China inDecember 1999. However, progressive deterioration of renal func-tion was noted thereafter despite the use of immunosuppressants,which included prednisolone, mycophenolate mofetil, sirolimus,and tacrolimus. Renal allograft biopsy showed chronic rejectionchange. He then received hemodialysis regularly and furosemidetreatment for controlling fluid overload. Other significant medicalhistory included hypertension under oral medication control. One
tology, Kaohsiung Medical07, Taiwan.).
iwanese Dermatological Associatio
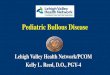
month before the beginning of bullous eruption, hematuria alongwith generalized pruritus and tiny erythematous papules andvesicles were noted during the tapering of oral prednisolone(2.5 mg/d) and tacrolimus (2 mg/d). Subsequently, large tensebullae progressively emerged over his trunk and four limbs withoozing erosive wounds (Figure 1), and he was admitted to ourdermatology ward for further treatment.
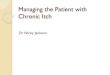
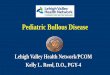
At admission, serum creatinine was 6.94 mg/dL with blood ureanitrogen of 21.8 mg/dL. Complete blood count and differentialcount showed marked eosinophilia (eosinophil count, 13.4%)without leukocytosis. Liver function tests, general serumbiochemical tests, electrolytes, stool routine, chest X-ray were allnormal. A skin biopsy was performed on the patient’s right forearmfor histology and direct immunofluorescence study, which showeda subepidermal blister with many eosinophils in the superficialdermis (Figures 2A and 2B) and linear immunoglobulin G (IgG) andcomplement component 3 deposition along the dermoepidermaljunction (Figures 3A and 3B), respectively. However, indirectimmunofluorescence study result was negative. Immunohisto-chemical staining with Type IV collagen showed that Type IVcollagen was localized to the blister base (Figure 2C). According tothe clinical pictures, pathology findings, immunofluorescencestudy, and Type IV collagen immunohistochemical staining, BPwas diagnosed. Oral prednisolone (30 mg/d) was administeredfor controlling the disease activity. Bullous lesions soon resolvedafter treatment without formation of new blisters. Hematuriadisappeared once corticosteroids were administered. Itchingimproved dramatically as well.
n. Published by Elsevier Taiwan LLC. All rights reserved.

Figure 1 Close view of patient’s left forearm showing tense bullae. Some bullae wereruptured leaving oozing erosive wounds.
T.-Y. Liaw et al. / Dermatologica Sinica 29 (2011) 94e97 95
After discharge, oral prednisolone was gradually tapered. Beforethe onset of bullous eruption, a cauliflower-like lesionwas noted onthe neck of his bladder from cystoscopy examination during thesurvey for hematuria. After improvement of skin lesions, the rightkidney, allograft, and bladder tumor were removed. Histopathologyof the renal graft was compatible with chronic rejection. Directimmunofluorescence study of the renal allograft showed faint and
Figure 2 (A) Low-power view of subepidermal bulla with conspicuous infiltration of eosinop(A) showing numerous eosinophils near the dermoepidermal junction (hematoxylin and eosIV collagen was localized to the blister base (100�).
barely detectable IgG deposition. No bullous eruption recurred inthe subsequent 8 months after graft nephrectomy and discontin-uation of both systemic corticosteroids and immunosuppressants.The patient is now under regular hemodialysis.
Discussion
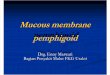
BP is a chronic autoimmune subepidermal blistering dermatosismediated by autoantibodies against antigens located in the base-ment membrane zone. BP in renal transplantation patients is rare,and only six cases have been described in the published liter-ature.3e8 A summary of previously reported cases and ours is givenin Table 1. Almost all the reported patients had chronic renal allo-graft rejection, with BP responding partially to systemic cortico-steroid treatment.3e7 Skin lesions in two cases cleared afterremoval of the graft.3,6 These observations suggested to us thatrenal allograft may play an important role in the pathogenesis of BP.
In our case, generalized itching and bullous eruption occurredconcomitantly with hematuria and during the tapering of immu-nosuppressants for renal allograft rejection, resolving simulta-neously after systemic corticosteroid treatment. BP did not recurafter graft nephrectomy, supporting the supposition that renalallograft participates in the pathogenesis of BP. Moreover, duringthe tapering of immunosuppressants, graft rejection triggered anoverwhelming response to allograft antigens with formation ofautoantibodies. Administration of corticosteroids helped to alle-viate the rejection as well as the autoimmune process, and webelieve that further graft nephrectomy helped to eliminate thesource of autoantibody induction.
hils near the dermoepidermal junction (hematoxylin and eosin, 40�). (B) Close view ofin, 200�). (C) Immunohistochemical staining with Type IV collagen revealed that Type

Figure 3 Direct immunofluorescence study. (A) Linear IgG deposition along the basement membrane zone (100�). (B) Linear complement component 3 deposition along thebasement membrane zone (100�).
T.-Y. Liaw et al. / Dermatologica Sinica 29 (2011) 94e9796
The immune mechanism producing bullous eruption duringrenal graft rejection is not fully understood so far. One theory is denovo autoantibody formation, which, in renal allografts, may resultfrom chronic allogeneic stimuli.9 Immune cross-reactivity betweenthe glomerular and epidermal basement membrane (one possibleantigen being identified as the alpha 5 chain of Type IV collagen)10
has been suggested in some of the reported cases of BP in associ-ation with graft rejection,11e15 explaining the possible associationbetween BP and hematuria in our patient.
We also observed a different direct immunofluorescence resultin the renal allograft compared with other case reports, with faintand barely detectable IgG deposition, which may be a result of end-stage graft damage with minimal antigens left in the allograft.
Currently, both cellular and humoral immunities are believed toplay an important role in the development of chronic renal allograftrejection.16e19 In experimental models for chronic renal allograftrejection, antibodies against glomerular basement membraneantigens have been found, including the heparan sulfate
Table 1 Published case reports of bullous pemphigoid in renal transplant patients.
Reference, year Age (y)a/sex
Underlying disease Rejection
Feehally et al, 19823 10/F Chronic pyelonephritis,cytomegalovirusinfection after transplantation
Chronic (poo
Yamazaki et al, 19984 9/M Crescentic glomerulonephritis Chronic (pooMorelli and Weston,
1999515/F Hereditary cystinosis Chronic (poo
Tessari et al, 20026 47/F Mesangial glomerulonephritis Chronic (pooChen et al, 20097 52/M Chinese herbal nephropathy,
hepatitis B and CChronic (norgradual dete
Sofi et al, 20108 46/M Diabetic nephropathy, hypertension,hepatitis C, Type I diabetes mellitus
Acute (poorrejection)
The present case 27/M Chinese herbal nephropathy Chronic (poo
Some of the content was adapted from Chen et al., 2009.7a Age at diagnosis.b Duration from renal transplantation to onset of bullous pemphigoid.c The patient underwent renal transplantation twice.
F¼ female; HD¼ hemodialysis; M¼male; PD¼ peritoneal dialysis.
proteoglycan perlecan and collagen Types IV and VI.20,21 Cross-reactive autoantibodies against both renal allograft and skin anti-gens may explain the development of BP in a patient experiencingrenal allograft rejection.
BP has been reported to be associated with some medications.Sulfur-containing drugs, such as furosemide,22 commonly causedrug-induced BP, andmay act as hapten, altering the antigenicity ofthe basement membrane zone or attaching to cells and eliciting theformation of autoantibodies. Tacrolimus, a selective blocker for theexpression of the interleukin-2 gene, is believed to act on a keyelement of the immune system, possibly on the regulatory T cells,causing a decreased regulatory T-cell activity indirectly contrib-uting to the induction of autoantibodies. Because our patient hadbeen treated with both furosemide and tacrolimus for many years,it is less likely that BP was induced by drugs.
Systemic corticosteroids, plasmapheresis, monoclonal anti-body,23 intravenous immunoglobulin,24,25 and graft nephrectomyhave all been used in the treatment of BP patients with allograft
Intervalb (y) Treatment
r renal function with HD) 2 Corticosteroids and graft nephrectomy
r renal function with PD) 5 Corticosteroids and graft atrophyr renal function with HD) 3 (7 mo)c Corticosteroids
r renal function with HD) 15 Corticosteroids and graft nephrectomymal renal function withrioration)
13 Corticosteroids and plasmapheresisdied of sepsis
renal function when Unknown Corticosteroids
r renal function with HD) 10 Corticosteroids and graft nephrectomy

T.-Y. Liaw et al. / Dermatologica Sinica 29 (2011) 94e97 97
rejection. Because a unified therapeutic approach for these patientsis absent because of the rarity of cases and lack of experience ofmost clinicians, there is a need for the establishment of a stan-dardized treatment protocol for these patients.
In conclusion, we report a case of BP associated with chronicrenal allograft rejection in a young man with renal allograft, theprobable triggering factor for the development of the bullousdisease. Bullous eruption was easily controlled by systemiccorticosteroids and did not recur after graft nephrectomy duringa clinical follow-up of 8 months. For the treatment of BP patientswith chronic renal allograft rejection, in addition to the elimina-tion of all possible provocative factors, systemic corticosteroidswith graft nephrectomy can be considered as a therapeuticoption.
References
1. Nousari HC, Anhalt GJ. Pemphigus and bullous pemphigoid. Lancet1999;354:667e72.
2. Vassileva S. Drug-induced pemphigoid: bullous and cicatricial. Clin Dermatol1998;16:379e87.
3. Feehally J, Reilly DT, Walls J, Wood RF. An antibody-mediated bullous skineruption caused by chronic renal allograft rejection. Transplantation1982;34:295e6.
4. Yamazaki S, Yokozeki H, Katayama I, et al. Childhood bullous pemphigoidassociated with chronic renal allograft rejection. Br J Dermatol1998;138:547e8.
5. Morelli JG, Weston WL. Childhood immunobullous disease following a secondorgan transplant. Pediatr Dermatol 1999;16:205e7.
6. Tessari G, Barba A, Chieregato C, et al. Bullous eruption during chronic renalallograft rejection. Dermatology 2002;204:307e8.
7. Chen TJ, Lai PC, Yang LC, et al. Bullous pemphigoid in a renal transplantrecipient: a case report and review of the literature. Am J Clin Dermatol2009;10:197e200.
8. Sofi AA, Gottwald L, Bohman K, Kaw D. Bullous pemphigoid associated withacute renal allograft rejection. Transplantation 2010;89:368e9.
9. Aprile M, Halloran P, Haddad G, Robinette M. Autoantibody against fibroblastsin renal transplant recipients: analysis by 51Cr-release assays. Clin Exp Immunol1981;46:565e74.
10. Ghohestani RF, Hudson BG, Claudy A, Uitto J. The alpha 5 chain of type IVcollagen is the target of IgG autoantibodies in a novel autoimmune diseasewith subepidermal blisters and renal insufficiency. J Biol Chem2000;275:16002.
11. Davenport A, Verbov JL, Goldsmith HJ. Circulating anti-skin basementmembrane zone antibodies in a patient with Goodpasture’s syndrome. BrJ Dermatol 1987;117:125e7.
12. Plaisier E, Borradori L, Hellmark T, et al. Anti-glomerular basement membranenephritis and bullous pemphigoid caused by distinct anti-alpha 3(IV)NC1 andanti-BP180 antibodies in a patient with Crohn’s disease. Am J Kidney Dis2002;40:649e54.
13. Simon CA, Winkelmann RK. Bullous pemphigoid and glomerulonephritis:report of four cases. J Am Acad Dermatol 1986;14:456e63.
14. van Joost T, Muntendam J, Heule F, et al. Subepidermal bullous autoimmunedisease associated with immune nephritis: immunomorphologic studies. J AmAcad Dermatol 1986;14:214e20.
15. Singhal PC, Scharschmidt LA. Membranous nephropathy associated withprimary biliary cirrhosis and bullous pemphigoid. Ann Allergy 1985;55:484e5.
16. Joosten SA, van Kooten C. Non-HLA humoral immunity and chronic kidney-graft loss. Lancet 2005;365:1522e3.
17. Joosten SA, Sijpkens YW, van Kooten C, Paul LC. Chronic renal allograft rejec-tion: pathophysiologic considerations. Kidney Int 2005;68:1e13.
18. Porcheray F, DeVito J, Yeap BY, et al. Chronic humoral rejection of humankidney allografts associates with broad autoantibody responses. Trans-plantation 2010;89:1239e46.
19. Rowshani AT, Bemelman FJ, Lardy NM, Ten Berge IJ. Humoral immunity inrenal transplantation: clinical significance and therapeutic approach. ClinTransplant 2008;22:689e99.
20. Joosten SA, van Kooten C, Paul LC. Pathogenesis of chronic allograft rejection.Transpl Int 2003;16:137e45.
21. Joosten SA, van Dixhoorn MG, Borrias MC, et al. Antibody response againstperlecan and collagen types IV and VI in chronic renal allograft rejection in therat. Am J Pathol 2002;160:1301e10.
22. Koch CA, Mazzaferri EL, Larry JA, Fanning TS. Bullous pemphigoid after treat-ment with furosemide. Cutis 1996;58:340e4.
23. Szabolcs P, Reese M, Yancey KB, et al. Combination treatment of bullouspemphigoid with anti-CD20 and anti-CD25 antibodies in a patient with chronicgraft-versus-host disease. Bone Marrow Transplant 2002;30:327e9.
24. Harman KE, Black MM. High-dose intravenous immune globulin for thetreatment of autoimmune blistering diseases: an evaluation of its use in 14cases. Br J Dermatol 1999;140:865e74.
25. Ahmed AR. Intravenous immunoglobulin therapy for patients with bullouspemphigoid unresponsive to conventional immunosuppressive treatment.J Am Acad Dermatol 2001;45:825e35.