Embed Size (px)
Citation preview

Burden of Care Analysis of Various Infant Orthopedic Protocols for Improvement of Nasolabial Aesthetics in Patients with Complete Unilateral Cleft Lip and Palate
by
Emily Singer D.D.S.
A thesis submitted in conformity with the requirements for the degree of Master of Science (Orthodontics), Graduate Department of
Dentistry, University of Toronto
© Copyright by Emily Singer 2012

ii
Abstract
Burden of Care Analysis of Various Infant Orthopedic Protocols for
Improvement of Nasolabial Aesthetics in Patients with Complete
Unilateral Cleft Lip and Palate
Emily Singer
Master of Science Degree, 2012
Discipline of Orthodontics, Faculty of Dentistry, University of Toronto
Toronto, Ontario, Canada
The purpose of this study was to evaluate the burden of care (BOC) of two presurgical
infant orthopedic (PSIO) protocols used for complete unilateral cleft lip and palate
(CUCLP), and to compare aesthetic outcomes with centres not utilizing PSIO. Four
samples were collected. Two from the same centre that underwent either traditional
infant orthopedics (TIO) or nasoalveolar molding (NAM) and two from centres not
employing PSIO. BOC data were collected for the PSIO groups and photos at age 5
were collected for ratings of nasolabial aesthetics. The BOC of NAM was found to be
significantly greater than IO for number of visits (9.9 vs. 6.6, (p<0.001)) and days
wearing the appliance (127 vs. 112, (p<0.05)). Significant differences in aesthetic
ratings were noted amongst the three centres but not between the NAM and TIO

iii
groups. Overall, an increased burden of NAM over TIO was detected, without an
observable aesthetic improvement.

iv
Acknowledgments
I would like to express my gratitude to the following people for their dedication and
support during this investigation:
Dr. John Daskalogiannakis, University of Toronto, Faculty of Dentistry, Department of
Graduate Orthodontics; thank you for your encouragement, guidance and patience over
the past three years. It was an absolute pleasure to work with you and to be included in
your Americleft family.
Dr. Bryan Tompson, University of Toronto, Faculty of Dentistry, Department of Graduate
Orthodontics; thank you for your guidance and support throughout this research project
and over the past three years in the Orthodontics program – I really appreciated it.
Dr. Christopher Forrest, SickKids Hospital, Toronto, Ontario; thank you for taking the
time out of your busy schedule to serve on my committee. Your expertise and guidance
were invaluable and very much appreciated.
Dr. Ross E. Long Jr, Chief of Orthodontics and Director of Research, Lancaster Cleft
Palate Clinic, Lancaster, PA; thank you for making me feel so welcome among the
Americleft clan and for all your help with this project. You really went above and
beyond!
The Americleft Group; thank you all for your advice and encouragement and for taking
the time to meet in Columbus to rate photo after photo after photo… I couldn’t have
done it without all of you!
The staff in the Orthodontic, Media Services and Health Records Departments at
SickKids Hospital, Toronto, Ontario; thank you for all your help in pouring through
records to collect my sample and letting me “set up shop” in your space.

v
Table of Contents
Abstract……………………………………………………..…………………………….. ii
Acknowledgements…………………………………………………………….………… iv
List of Figures…………………………………………………………………………….. vii
List of Tables…………………………………….……………………………………….. viii
List of Appendices………………………………………………..……………………… ix
Introduction, Definitions and Statement of the Problem……………………………. 1
Review of the Literature……………………………………….………………………… 4
1. Embryogenesis of Cleft Lip and Palate…………………………………….. 4
2. Classification of Cleft Lip and Palate……………………………………….. 7
3. Nasolabial Morphology in Infants with Unrepaired CLP…………………. 8
4. Primary Surgical Repair of CUCLP…………………………………………. 9
5. Methods of Assessment of the Cleft-Related Facial Deformity………… 11
6. Development of Presurgical Infant Orthopedics………………………….. 16
7. PSIO for Improvement of Nasolabial Aesthetics in CUCLP……………. 19
8. Outcome Assessment: The Americleft Project…………………………… 25
9. Burden of Care in CLP Treatment…………………………………………. 29
Objectives of the Study…………………………………………………………………. 34
Hypotheses………………………………………………………………………………. 35
Samples and Methods………………………………………………………………….. 36
1. Samples………………………………………………………………………. 36
a. Inclusion/Exclusion Criteria…………………..…………………….. 37
b. Descriptive Data/Sample Sizes…………………..……………….. 38
2. Methods……………………………………………………………………… 41
a. Burden of Care………………………………………………………. 41
b. Nasolabial Aesthetics Assessment……………………………….. 42
c. Americleft “Q-Sort” Modification of Asher-McDade Method……. 45
Results……………………………………………………………………………………. 49

vi
Discussion………………………………………………………………………………... 58
Conclusions………………………………………………………………………………. 67
Clinical Significance & Future Directions……………………………………………… 68
References………………………………………………………………………………. 69
Appendices……………………………………………………………………………….. 81

vii
List of Figures
Figure 1: Schematic diagrams of the development of the lip and palate... 6
Figure 2: Illustrative drawings of types of CLP……………………………… 7
Figure 3: Nasolabial morphology in patients with unrepaired CUCLP……. 8
Figure 4: Example of coded slide used for rating…………………………… 45
Figure 5: Means and standard errors for the number of visits for appliance fabrication and adjustment…………………………………………. 50
Figure 6: Means and standard errors for the number of days each appliance was worn…………………………………………………………………… 50
Figure 7: Frequency of each raw score from 1 to 5 for each sample for the category VB……………………………………………………………………… 52
Figure 8: Frequency of each raw score from 1 to 5 for each sample for the category NLF……………………………………………………………………. 52
Figure 9: Frequency of each raw score from 1 to 5 for each sample for the category NLP……………………………………………………………………. 53
Figure 10: Mean nasolabial aesthetic scores for each individual category and for the cumulative scores in each sample…………………………………. 55

viii
List of Tables
Table 1: Sample Demographics…………………………………………….. 40
Table 2: Means, standard deviations and ranges for the number of visits for
appliance fabrication and adjustment……………………………. 49
Table 3: Means, standard deviations and ranges for the number of days each
appliance was worn………………………………………………… 49
Table 4: Mean weighted kappa values (and ranges) for the intra-rater and inter-
rater reliability assessments……………………………………….. 51
Table 5: Summary of the chi square analysis of the percent distribution in scores
for the category “vermilion border”………………………………… 53
Table 6: Summary of the chi square analysis of the percent distribution in scores
for the category “nasolabial frontal”……………………………….. 54
Table 7: Summary of the chi square analysis of the percent distribution in scores
for the category “nasolabial profile”...……………………………… 54
Table 8: Median values of nasolabial aesthetics ratings using the modified Asher-
McDade method……………………………………………………… 57

ix
List of Appendices
Appendix 1: Abbreviations/Acronyms…………………………………… 81
Appendix 2: Sample Demographics & BOC Data………………………. 82
Appendix 3: Statistical Analysis - Weighted Kappa Scores……………. 88
Appendix 4: Statistical Analysis – Kruskal-Wallis and Chi-square Tests 91

1
Introduction, Definitions and Statement of the
Problem
Restoration of acceptable form and function in a patient with complete unilateral cleft lip
and palate (CUCLP) involves the multidisciplinary management of deformities involving
the upper lip, nasal tissues, alveolar process, palate, and developing dentition. In the
absence of proper early management, severe facial deformity and functional
disturbance of developing teeth may ensue.
Orthodontists and cleft surgeons have worked collaboratively for decades to develop
techniques to help align both the bony and soft tissue structures of the segments of the
cleft prior to surgery. These techniques have ranged from simple lip taping to more
complex passive or active acrylic appliances aimed at repositioning the alveolar
segments and reducing the width and severity of the cleft (McNeil, 1950; Hotz, 1976),
and are collectively known as presurgical infant orthopedic treatment (PSIO).
In the early 90’s, Grayson and his colleagues introduced a type of PSIO procedure
combining an orthodontic intraoral device with a nasal stent, that they termed
nasoalveolar molding (NAM). The claimed advantage of NAM over more traditional
methods of PSIO is that it takes advantage of the malleability of immature nasal
cartilage and its ability to maintain a permanent correction of its form, thereby enabling
the surgeon to achieve a more anatomical and aesthetic repair of the alveolar process,
lip and nose (Grayson and Cutting, 1993).

2
NAM was introduced into the infant management protocol at Toronto’s SickKids
Hospital approximately ten years ago. Previously, this centre performed PSIO by
means of an active/passive intraoral acrylic appliance usually combined with extraoral
“outriggers” to aid in retention of the appliance. This served to mold the alveolar process
and reduce the width of the cleft deformity prior to surgery. For the purposes of this
thesis, the technique of presurgical molding used prior to the introduction of NAM at
SickKids Hospital will be termed traditional infant orthopedics (TIO).
Presurgical infant orthopedics (PSIO) will be used as a generic term encompassing any
type of presurgical manipulation of the cleft segments, alveolar or otherwise, that
includes both traditional infant orthopedics (TIO) and nasoalveolar molding (NAM)
techniques.
The benefit of NAM therapy is a controversial topic in the treatment of patients with
UCLP. Advocates of the technique claim that its use significantly enhances the ability of
the interdisciplinary team to achieve superior nasolabial aesthetics by improving nasal
symmetry, and also allows for easier surgery (Maull et al., 1999; Singh et al. 2007,
Barillas et al. 2009). Skeptics of both Grayson’s NAM technique and PSIO in general,
comment on the potential inhibition of future maxillary growth and the added expense
and burden (Ross, 1987; Pope et al., 2005; Prahl et al. 2006; Long, 2011).
The current burden of care and economic cost of multidisciplinary treatment for CUCLP
patients is estimated to be significant, weighing heavily on the families of these patients,
hospital personnel and, often, scarce government resources. For any treatment option,
the benefits and burden must be analyzed and evaluated so that available funds and

3
caregivers’ time may be efficiently allocated. To date, few studies have been published
that have examined the burden of care of various CLP treatment protocols. None of
these have examined the relationship between the burden of NAM over TIO and the
proposed improvement in nasolabial aesthetics.

4
Review of the Literature
1. Embryogenesis of Cleft Lip and Palate
Development of the human craniofacial region is a complex process during which
seemingly minor deviations in the precise timing of key events may result in significant
facial malformations. Knowledge of the embryologic processes involved in normal
craniofacial development is essential to appreciate the complexity of, and to plan
treatment for, the resultant anomalies.
Genetic, molecular, and cellular processes must be spatially and temporally regulated to
culminate in the proper three dimensional patterning and sculpting of the human face.
The starting constituent for the majority of skeletal and connective tissues in the face is
a pluripotent population of transient migratory cells known as cranial neural crest cells
(Cordero et al., 2011). Following embryo gastrulation in the third week of development,
neural crest cells are specified at the border of the neural plate and the non-neural
ectoderm. During the process of neurulation, the borders of the neural plate, the neural
folds, converge at the dorsal midline to form the neural tube. Neural crest cells from the
roof plate of the neural tube then undergo an epithelial to mesenchymal transition and
begin to migrate through the periphery where they differentiate into varied cell types.
These neural crest cells contribute largely to the formation of the mesenchyme of the
craniofacial complex (Kirschner and LaRossa, 2000).
By combination with the mesoderm, the neural crest cells aid in establishing the five
facial primordia including the frontonasal prominence and the paired maxillary and
mandibular prominences, that will later contribute to the formation of the lips, nose and

5
palate (Moore, 1982; Melnick, 1990). By the end of the fourth week, bilateral swellings,
the nasal placodes, develop on the lower part of the frontonasal prominence. The
medial and lateral nasal prominences develop as peripheral thickenings of the
mesenchymal tissue of the nasal placodes, producing two central depressions, the
nasal pits (Ten Cate, 1998). Failure of the nose to develop completely is associated
with failure of the nasal placodes to develop.
Between the fourth and eighth weeks, the paired medial nasal prominences fuse with
each other, with the paired lateral nasal prominences, and with cells in the maxillary
prominences. Successful fusion of the medial nasal and maxillary prominences is
essential for continuity of the upper lip and primary palate. Failure of fusion of one or
both medial nasal and maxillary prominences results in unilateral or bilateral cleft lip,
respectively.
As the face nears the completion of the “developmental critical period”, from
approximately the end of the sixth to the eighth intrauterine week, the lateral palatine
processes grow out from the walls of the still common oronasal cavity. Growth of these
paired processes is initially medial, but continues inferolaterally to lie on either side of
the developing tongue. Nearing the eighth week, palatal shelf elevation begins while
the tongue is depressed downward and forward. Once in contact, epithelial cells of the
palatal shelves degenerate by programmed cell death uniting the paired processes in a
process known as fusion. Once fusion of the shelves of the secondary palate occurs,
the mesenchymal cells differentiate and become osteogenic cells contributing to the
bony development of the premaxillary, maxillary and palatine portions of the palate

6
(Berkowitz, 2006). Cleft palate results from the failure of fusion of these paired lateral
palatine processes as a result of a defect in any of the three major stages of palatal
formation – palatal shelf outgrowth, elevation, or fusion (Kaartinen et al., 1995).
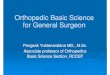
Figure 1. Schematic diagrams of the development of the lip and palate in humans. a. The developing frontonasal prominence, paired maxillary processes and paired mandibular processes surround the primitive oral cavity by the fourth week of development. b. By the fifth week, the nasal pits have formed, leading to the formation of the paired medial and lateral nasal processes. c. The medial nasal processes have merged with the maxillary processes to form the upper lip and primary palate by the end of the sixth week. The lateral nasal processes form the nasal alae and the mandibular processes fuse to form the mandible d. During the sixth week, the secondary palate develops as bilateral outgrowths from the maxillary processes, which grow vertically down the side of the tongue. e. Subsequently, the palatal shelves elevate to a horizontal position above the tongue, contact one another and commence fusion. f. Fusion of the palatal shelves ultimately divides the oronasal space into separate oral and nasal cavities. (Adapted from Dixon et al., 2011)

7
2. Classification of Cleft Lip and Palate
Numerous methods have been proposed for the classification and recording of CLP
deformities. None, however, have been universally accepted due to limitations
including inadequate descriptions of the deformities of the cleft in some classification
systems and unnecessarily onerous complexities of more sophisticated methods (Liu et
al., 2007). A simplified approach focuses on the distinction between clefts involving the
lip, palate or a combination thereof, with reference to the extent of the cleft (complete or
incomplete); between unilaterally or bilaterally occurring anomalies; and between those
occurring in conjunction with or in the absence of an associated syndrome.
Nonsyndromic CUCLP may therefore be defined as a continuous cleft extending from
the nasal sill through the upper lip and alveolar process on one side up to the incisive
foramen and posteriorly from the incisive foramen to include both the hard and soft
palates, in the absence of a concomitant syndrome. (Figure 2d)
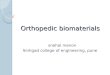
Figure 2. Illustrative drawings of types of CL&P. a and e show unilateral and bilateral clefts of the soft palate; b, c and d show degrees of unilateral cleft lip and palate; f, g and h show degrees of bilateral cleft lip and palate. (Adapted from Dixon et al. 2011)

8
3. Nasolabial Morphology in Infants with Unrepaired CUCLP
Bilateral dysmorphology of the nasolabial region is often demonstrated in patients with
CUCLP. The nasolabial region is largely asymmetric with deviation towards the non-
cleft side as aberrant muscle insertions and tongue protrusion cause the non-cleft side
of the maxilla to deviate and rotate away from the cleft. The perioral musculature
overpowers the inadequately supported bone and pulls the nose and nasal septum to
the non-cleft side, yet the alar base on the side of the cleft remains in about the same
position. As a result, the cleft side nostril becomes abnormally stretched and flattened
(Ross, 2002). These abnormal muscle insertions lead to displacement of the non-cleft
side tissues vertically, laterally and anteriorly, with lateral and vertical displacement of
the cleft side. The columella on the cleft side is shortened significantly, as compared
with the non-cleft side and is oriented obliquely, with its base deviated toward the non-
cleft side, away from the midline. The alar bases are asymmetric, with the cleft side alar
base displaced inferiorly and posteriorly (Lo, 2006).
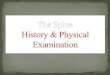
Figure 3. Typical nasolabial morphology in patients with unrepaired CUCLP (Adapted from http://dentistry.ouhsc.edu/os_cleft-craniofacial.php)

9
4. Primary Surgical Repair of CUCLP
Primary cheilorhinoplasty, surgical repair of the lip and nasal deformity, involves
reconstruction of the musculoaponeurotic complex of the cleft to place the muscles in
their proper anatomic and physiologic orientation through careful identification,
dissection, and mobilization of the paranasal and labial tissues. The cleft repair is
essentially a muscle repair to enhance the establishment of a normal nasolabial
complex. Accurate repositioning of the lower alar cartilages (Thomas, 2009) and the
orbicularis oris muscles (Farmand, 2002) during the primary lip repair is thought to aid in
establishing a normal nasal shape.
Chinese physicians, as early as the fourth century AD, were the first to describe a
technique to repair the cleft lip by simple excision of the cleft margins and suturing of
the opposing segments (Wong and Wu, 1932). While some form of this technique was
utilized by most surgeons until the early 19th century, it was later abandoned because it
led to the formation of a vertical scar that invariably resulted in an unaesthetic
shortening of the lip. In 1844, Germanicus Mirault devised a method to circumvent this
problem by introducing a triangular flap that was brought from the lateral side into a gap
created by a horizontal incision on the medial side. This not only eliminated the linear
scar by adding extra tissue to help lengthen the lip, but it also helped to recreate a
nostril floor (Bhattacharya et al., 2009). The triangular flap repair was later modified by
Tennison (Tennison, 1952) and by Randall (1959), who described the geometry of the
technique; and, today, the Tennison-Randall triangular flap repair is still utilized by
several cleft centres worldwide.

10
Along with the Tennison-Randall repair, the Millard rotation-advancement repair has
become part of the mainstay of primary CLP surgery and is thought to be a reliable and
versatile method for repair of the unilateral cleft lip deformity (Millard, 1976; Skyes,
2001). This technique allows for an anatomic lip repair and tip rhinoplasty while
camouflaging the scars in the nasal creases and newly formed philtral border (Kirschner
and LaRossa, 2000; Skyes, 2001; Arosarena, 2007).
Despite advancements in surgical techniques and attempts to reestablish normal
anatomy both immediately post surgically and during early growth, repair of a CUCLP
rarely produces ideal facial aesthetics. While satisfactory functional results can be
achieved after primary repair in the majority of patients with unilateral clefts,
morphologic results tend to be less ideal (Bilswatch et al., 2009). Patients generally
demonstrate some degree of deformation of the upper lip and nose with variable nasal
asymmetry, scarring of the philtral area, or an uneven vermillion border. The resultant
craniofacial impairments may have significant negative psychological consequences,
ranging from low self-esteem to the risk of social rejection (Tobiasen 1987, Broder and
Strauss, 1989; Fudalej et al., 2009).

11
5. Methods of Assessment of the Cleft-Related Facial Deformity
The ultimate objective of all CLP treatment modalities is to restore acceptable form and
function and to minimize the visible stigmata of the cleft related facial deformity.
Assessment of the appearance of the repaired deformity is a crucial component in
quality of life outcome measures in this patient population. Although international ratings
of attractiveness of individuals without clefts have been explored, a conclusive definition
of attractiveness in terms of facial features has not been agreed upon in the literature.
The measurement of facial aesthetics continues to be a complex and subjective process
that is dependent on a number of variables (Patzer, 1984; Al-Omari et al., 2005).
A review of the literature by Al-Omari et al. in 2005 identified the stimulus media,
scoring systems, characteristics of the raters and regions of interest most commonly
used in assessment of the appearance of the cleft-related facial deformity.
Stimulus Media
Stimulus media for the assessment of the cleft related deformity can be categorized into
direct clinical assessment of live subjects or facial casts, two- or three-dimensional
media or a comparative combination of clinical assessment with two- or three-
dimensional media.
For the assessment of live subjects or facial casts, both quantitative and qualitative
means have been employed. A number of studies have utilized anthropometry to
quantitatively analyze the extent of the abnormal morphology and degree of
disproportion and asymmetry of the repaired nasolabial region using direct linear and

12
proportional measurements (Lindsey and Farkas, 1972; Farkas et al. 1993). Friede et
al. (1980) measured angular, linear and surface measurements of plaster casts of the
midfacial regions of patients with clefts to evaluate various surgical techniques.
Qualitative visual evaluation of live subjects and clinical photographs was utilized by
Assuncao (1992), who employed a subjective “V.L.S.” classification system of the labial
deformity by the assessment of three components: the vermillion border, the lip and the
scar.
Qualitative and quantitative assessments of two-dimensional media, i.e. clinical
photographs and video recordings, are, by far, the most frequently used methods for
rating the cleft-related deformity. Subjective assessments of black and white
photographs (Glass et al., 1981), colour photographs (Asher-McDade et al. 1991;
Eliason et al. 1991; Roberts-Harry et al, 1991; Brattström et al. 1992; Mercado et al.
2011), projected colour transparancies (Tobiasen et al. 1991; Cussons et al., 1993;
Feragen et al., 1999; Al-Omari et al. 2003; Johnson and Sandy, 2003), and on-screen
digital photographs (Becker et al. 1998) have all been employed, as have quantitative
objective measures of various features of the nasolabial complex (Kohout et al., 1998;
Heller et al. 2011). Acceptable reliability and reproducibility from ratings of standardized
facial photographs (Asher-McDade et al., 1991) and direct measurements of on-screen
digital images (Becker et al., 1998) have been demonstrated. Several studies have also
shown good intra- and inter-examiner reliability scores between judgements of facial
appearance made from live stimuli and those from colour photographs (Becker et al.
1998; Johnson and Sandy, 2003; Al-Omari et al. 2003). While video recording has
been used to assess both the form and function of patients with cleft lip and palate

13
(Morrant and Shaw, 1996; Frey et al., 1999; Russell et al., 2000, 2001), a large range in
the reliability of ratings of video recordings has been observed (Morrant and Shaw,
1996) and attempts at digitizing soft tissue outlines from video imaging have not been
shown consistently to be valid or reproducible (Benson and Richmond, 1997).
Three-dimensional imaging techniques to assess the cleft deformity have included laser
scanning (Foong et al., 1999; Duffy et al. 2000), computer-aided tomography (CT)
(Fisher et al., 1999, Miyamoto et al. 2012), three-dimensional morphoanalysis (Ras et
al. 1994) and stereophotogrammetry (Al-Omari et al. 2003; Krimmel et al., 2006;
Nakamura et al., 2010; Sander et al., 2011). While the reliability and accuracy of 3-D
assessment media is promising, limitations including radiation exposure of CT imaging,
cooperation of young patients during prolonged image acquisition periods and limited
access to equipment across centres have prohibited widespread use, especially in
multicentre outcome studies.
Scoring Systems
Scoring methods to measure facial attractiveness have included ordinal scales based
on distinct categories of classification, rankings in order from best to worst for the
chosen features, or the use of visual analogue scales. The possibility of systematic bias
is recognized considering that raters may differ in their interpretation of a scoring
system. Several suggestions to overcome this limitation have been proposed. The use
of objective standards in conjunction with qualitative assessments, such as the
distribution of a written set of criteria for each index category, has been advocated
(Vegter and Hage, 2001; Johnson and Sandy, 2003). A visual yardstick to supplement

14
the Asher-McDade rating system (Asher-McDade et al., 1991), based on a set of
photographs that demonstrated the highest agreement among observers in the study,
has recently been published to facilitate the use of this commonly used 5 point ordinal
scale (Kuijpers-Jagtman et al., 2009).
Raters
In addition to the stimulus media and scoring systems selected, the composition of the
group of raters has been shown to have a large impact on the outcome of any study
assessing facial appearance. Researchers have attempted to determine whether
clinicians, patients, and laypersons agree in their perception of acceptable facial
attractiveness in patients with CLP. Studies comparing ratings of professionals and
laypersons have revealed inconsistent results, with some showing good agreement
(Coghlan et al. 1987; Cussons et al., 1993; Roberts-Harry and Stephens, 1991), and
others demonstrating discrepancies between expert and nonexpert groups (Eliason et
al., 1991). While some studies show that professionals tended to be more critical in
their assessments (Eliason et al. 1991), a recent study evaluating the relation between
professional and lay ratings of nasolabial appearance in CUCLP showed that the
professionals consistently gave higher scores for nasolabial appearance than did the lay
panel. In the same investigation, a self-assessment of nasolabial appearance by the
patients did not correlate with the judgement of either the lay or professional panels.
(Mani et al., 2010). Despite the inconsistent results regarding which group provides the
most reliable and clinically relevant outcome measure, most studies have concluded

15
that increasing the number of assessors should minimize interexaminer bias and
improve reliability (Asher-McDade et al., 1991).
Region of Interest
Since the ultimate aesthetic goals of a restored cleft deformity are to improve social
acceptance and reduce the visible stigmata associated with the malformation, many
studies have advocated assessment of the global facial appearance for ratings of
attractiveness, as would be perceived in social interactions (Tobiasen et al., 1991; Al-
Omari et al. 1993; Johnson and Sandy, 2003). Conversely, it has been demonstrated
that judgement of the cleft area is likely to be affected by surrounding features of the
face (Asher-McDade et al., 1991; Tobiasen and Hiebert, 1993) which may confound the
aesthetic assessments of various interventions or surgical techniques. Both Asher-
McDade et al. (1991) and Tobiasen et al. (1991) were able to demonstrate high
correlations between full-face ratings and ratings of the nasolabial area and photos
cropped just below the eyes, respectively, and both advocate using views that only
depict the nasolabial region for unbiased rating assessments.

16
6. Development of Presurgical Infant Orthopedics
Successful management of the functional and aesthetic demands of CLP repair requires
precise manipulation of the soft and hard tissues of the lip, nose and alveolus. It has
been theorized that favourable alignment of the alveolar segments of the cleft prior to
primary cheilorhinoplasty using non-surgical techniques can provide a foundation upon
which the results of primary lip and nasal surgery can be built.
Presurgical infant orthopedics has been employed in the treatment of CLP patients for
centuries. Early techniques included retraction of the protruding premaxilla using
elastics in patients with BCLP; facial binding to narrow the cleft and prevent postsurgical
dehiscence; the use of a bonnet and strapping to stabilize the premaxilla after surgical
retraction; or the passing of a silver wire through the two ends of the cleft followed by
progressive tightening to approximate the alveolar segments before lip repair (Grayson
and Shetye, 2009).
The modern school of infant orthopedic treatment was introduced by McNeil who used a
series of intraoral appliances to actively mold the alveolar segments into the desired
position presurgically (McNeil, 1950). The cleft is thereby narrowed and additional soft
and hard tissue is available for surgical repair (Ross and Johnston,1972). Hotz later
described the use of a passive orthopedic appliance to slowly align the cleft segments
(Hotz, 1969). Continued wear of the appliance prevented the tongue from entering the
cleft, allowing the palatal shelves to grow medially. The appliance is a compound
soft/hard acrylic resin which obturates the full extent of the cleft down to the tip of the
uvula, normalizing tongue posture and swallowing. Manipulation of the appliance

17
permits the deviated maxillary segments to lengthen and spontaneously assume a more
normal position. The results of the “growth-guidance” effect of the appliance are
uprighting the deviated greater segment and narrowing of the cleft (Hotz and Gnoinski
1976, Hotz et al. 1978). The McNeil and Hotz appliances, or various modifications
thereof, are still utilized by several CLP centres today.
In 1975, Georgiade and Latham introduced a pin-retained active appliance for patients
with BCLP to simultaneously retract the premaxilla and expand the posterior segments
over a period of several days (Georgiade and Latham, 1975). Similarly, the Latham
dentomaxillary alignment (DMA) appliance for UCLP advances and expands the lesser
segment of the unilateral cleft and retracts the greater segment posteromedially by daily
activation for 3 to 4 weeks (Latham, 1980). The use of the Latham appliance has been
controversial. Evidence has been accumulating that the pin-retained DMA appliance
may have detrimental effects on dental arch relationships and facial growth (Ross,
1987; Brattström et al., 1991; Chan et al., 2003; Berkowitz et al., 2004).
Motivated by research on the plasticity of neonatal auricular cartilage (Matsuo et al.
1984), Grayson and Cutting proposed that active molding and repositioning of the nasal
cartilages in patients with CLP may take advantage of the temporary plasticity of the
nasal cartilage of the newborn infant, thought to arise from high levels of hyaluronic acid
circulating for weeks after birth (Grayson et al. 1993, Cutting et al. 1998, Grayson et al.
1999). The technique, known as nasoalveolar molding (NAM), combines presurgical
alveolar molding with nasal molding through the incorporation of an acrylic nasal stent
to the labial vestibular flange of a conventional intraoral molding appliance. The nasal

18
stent and intraoral component are adjusted gradually, usually at weekly intervals over a
three-to-four -month period, to achieve nasal and alveolar symmetry, nasal tip projection
and contact of the cleft alveolar segments just prior to primary repair. According to
Grayson, presurgical reduction in the soft tissue and cartilaginous deformities allows for
repair under minimal tension, optimizing conditions for scar formation and improving
nasal symmetry in the long term (Grayson and Cutting, 2001).
The inclusion of PSIO of any kind in primary infant management is variable across CLP
centres. Proponents advocate its employment to facilitate surgical repair, improve
feeding, guide growth of the developing maxilla and provide psychological benefit to the
parents. Adversaries quote the potential inhibition of future maxillary growth and the
unnecessary added expense and burden of care for minimal, if any, long-term benefit
(Ross, 1987; Prahl et al. 2006).

19
7. PSIO for Improvement of Nasolabial Aesthetics in CUCLP
Despite its long standing history in CLP treatment and a recent resurgence with the
advent of NAM, the inclusion of PSIO in infant management protocols for patients with
CUCLP is still highly controversial. Alleged benefits of orthopedic appliances include
facilitation of feeding, guidance of growth, development of the maxillary segments,
normalization of tongue function, facilitation of surgery, better speech, and a positive
psychological effect on the parents (Prahl-Andersen, 2000).
In addition, it has been suggested that proper presurgical alignment of the cleft
segments with an intraoral appliance will provide a foundation upon which the results of
surgery can be built, allowing for a more esthetic repair under minimal tension (Grayson
et al., 1999). The incorporation of the nasal stent in the NAM appliance further aims to
improve nasolabial aesthetics by shaping and remodeling the nasal cartilages before
primary cheilorhinoplasty. The NAM technique is aimed at elevating the wing and tip of
the nose to improve nasal tip projection, expanding the nasal mucosal lining and
straightening the columella that has deviated towards the noncleft side. The result is
thought to be a more symmetric nose in the long term, with improved rounding of the
nostril on the cleft side and reduced alar flattening (Grayson and Cutting, 2001; Jaeger
et al., 2006; Shetye, 2010) .
The proposed benefits of PSIO, in general, and NAM, in particular, on improvement of
nasolabial aesthetics in patients with CUCLP have been examined in a number of
studies with conflicting results.

20
Traditional IO (infant orthopedics), generally involving an active or passive intraoral
appliance without the incorporation of a nasal stent, is thought by some to improve
facial appearance in unilateral cleft patients by facilitating lip surgery and stimulating a
favourable direction of maxillary growth (Graf-Pinthus and Bettex, 1974; Hotz and
Gnoinski, 1976). Others have refuted this claim, suggesting that similar effects could be
obtained with lip surgery alone (Ross, 1987; Asher-McDade et al., 1992; Winters and
Hurwitz, 1995).
To address the uncertainty surrounding the effects of IO, a prospective randomized
controlled trial (RCT), the Dutchcleft study, was conducted in three CLP centres in the
Netherlands (Prahl et al., 2006). The aim was to investigate the effect of IO using a
passive intraoral appliance in children with CUCLP. Early results showed that IO had a
temporary effect on maxillary arch dimensions, which did not last beyond surgical soft
palate closure (Prahl et al., 2001; Bongaarts et al., 2006). Results of aesthetic ratings in
the first two years of life using visual analogue scales and reference scores to assess
facial appearance showed no effect of IO on facial appearance in this study (Prahl et al.,
2006).
A later study by the same group evaluated the facial appearance at ages 4 and 6 in a
randomized clinical trial involving two of the three original Dutchcleft centres. Twenty-
seven patients were treated with a passive appliance until the time of soft palate closure
and 27 were treated with surgical repair alone. Twenty-six observers, 16 professionals
with experience in cleft care and 10 laypersons, were asked to evaluate photographs
(full facial photos and cropped photos of the nasolabial region alone) relative to a

21
reference photo of “average” CLP appearance. The results showed that while IO had a
positive effect on the full facial appearance of children with UCLP at the age of 4 years,
by the age of 6, only professionals saw a positive effect of IO which was limited to the
cropped nasolabial photographs. The authors concluded that the results at age 6, and
thus the influence of IO, were insignificant for patients with UCLP since they deal with
laypersons in their day to day lives (Bongaarts et al., 2008).
In another multicentre outcome assessment study, the Americleft group of researchers
examined nasolabial aesthetic outcomes of four centres each employing different early
management protocols. The subjects, totaling 124 patients across the four centres,
presented with repaired, nonsyndromic complete unilateral cleft lip and palate and were
between the ages of 5 and 12 years. Preorthodontic frontal and profile patient images
were scanned and cropped to show the nose and upper lip, and were evaluated by five
examiners using the rating system reported by Asher-McDade et al. (1991). No
statistically significant differences among centres were detected for either total aesthetic
scores or for any of the individual aesthetic components. Overall fair-to-good nasolabial
aesthetic results were achieved by all four North American centres despite using
different early treatment protocols (Mercado et al., 2011).
The past decade has seen a renaissance in the use of PSIO in CLP treatment with the
introduction and popularization of NAM. While early results showing immediate
postoperative improvements in nasal form following NAM were promising, a number of
studies have demonstrated variable degrees of relapse in the postoperative period (Liou
et al., 2004; Pai et al., 2005). As a result, a number of researchers have attempted to

22
address the controversy surrounding the long-term improvement in nasolabial
aesthetics proposed by Grayson and other advocates of the NAM technique.
In a systematic review by Uzel and Alparslan (2011), the authors aimed to assess the
scientific evidence on the efficiency of presurgical infant orthopedic appliances in
patients with cleft lip and palate and to address the controversy regarding whether these
appliances have any long-term advantages with respect to treatment outcomes. Two
literature surveys from five electronic databases were performed with a one-month
interval to identify RCTs and controlled clinical trials (CCTs), where the controls had no
PSIO. Studies with a follow up period of a minimum of six years were included in the
review with the exception of the outcome measures of feeding and motherhood
satisfaction, which are considered most important in the first year of life. Of the 319
articles retrieved in the literature surveys, 12 qualified for final analysis based on the
inclusion criteria. Eight RCTs and four CCTs were available on eight treatment
outcomes: motherhood satisfaction, feeding, speech, nasolabial appearance, occlusion,
facial growth, maxillary arch dimensions and nasal symmetry. In terms of appliance
design, one study was retrieved on the NAM approach (Barillas et al., 2009), active
appliances were evaluated in two articles (Chan et al., 2003; Masarei et al., 2007) and
passive appliances in eight (Ross and MacNamera, 1994; Konst et al., 2003; Bongaarts
et al., 2004; Prahl et al., 2005, 2008; Bongaarts et al., 2006; Bongaarts et al., 2008;
Bongaarts et al., 2009). No RCTs were identified that addressed either active PSIO or
NAM appliances and eight CCTs assessing NAM were excluded due to a lack of
appropriate controls or insufficient follow up periods.

23
Based on the results of the study, the authors concluded that PSIO appliances have no
long-term positive effects on seven of the eight studied treatment outcomes in patients
with CUCLP, with the exception being an improvement in nasal symmetry with NAM.
Barillas et al. (2009) demonstrated, based on measurements of stone cast models in
nine year old patients, greater symmetry in the lower lateral and septal cartilages of the
nose in a NAM group (n=15) than a surgery-alone sample (n=10). The authors called
for more RCTs to be conducted to have quality evidence regarding the effects of PSIO,
in general, and stated specifically that “the encouraging results surrounding the effect of
nasolaveolar molding appliances on nasal symmetry have to be supported by future
randomized controlled trials”.
Since it is suggested that the main difference of NAM from traditional IO is the
reshaping of the nasal cartilage and aesthetic benefits in terms of nasal tip and alar
symmetry (Grayson et al., 1999; Maull et al., 1999; Grayson et al., 2001; Suri and
Tompson, 2004; Singh et al., 2005), most studies demonstrating benefits of NAM have
focused on the assessment of nasal symmetry, alone, as the outcome measure
(Grayson et al. 1999, 2001, Maull et al. 1999; Liou et al. 2004, Barillas et al., 2009).
Given that the entire nasolabial region is an important component of facial aesthetics,
the authors highlighted that future RCTs should take into consideration the entire
nasolabial appearance, as well as nasal symmetry, when assessing NAM treatment.
No studies were identified in this review demonstrating a positive effect of PSIO, of any
kind, on nasolabial aesthetics as a whole.

24
To address the association between nasolabial symmetry and aesthetics in children
with CUCLP, Fudalej et al. (2012) examined frontal and worm’s-eye view photographs
of 60 consecutively treated children with CUCLP and 44 children without clefts. Eleven
nasal and labial measurements were made on both sides of the patient (cleft/non cleft
or right/left) and a coefficient of asymmetry (CA) was calculated for each measurement.
The Asher-McDade method (Asher-McDade et al., 1991) was used to evaluate
nasolabial appearance as a whole. Correlation and regression analysis were used to
identify an association between aesthetics and CA, sex, and the presence of CUCLP.
Ten measurements in the cleft group and two in the control group differed significantly
between the cleft and non-cleft, or right and left, sides, respectively. The significantly
higher values of 9 of 11 measurements with respect to their coefficients of asymmetry in
the children with CUCLP indicated that they had more asymmetrical nasolabial areas
than children without clefts. However, when comparing the CA and the results of the
ratings of overall nasolabial appearance, the regression analysis showed that nasolabial
aesthetics and nasolabial symmetry seem to be only weakly associated in patients with
CUCLP. Nasolabial symmetry is just one of the many variables contributing to overall
aesthetics in these patients.

25
8. Outcome Assessment: The Americleft Project
With the vast array of management protocols and surgical treatment techniques for the
correction of CLP referenced in the literature, little reliable information is available for
clinicians to make rational evidence-based decisions on the most efficient and effective
interventions for these patients (Semb and Shaw, 1998). As an example, in a survey of
201 European cleft centres, 194 different surgical protocols were reported for the
primary correction of CUCLP alone (Shaw et al., 2001).
Much of the evidence supporting these varied treatment modalities are the result of
retrospective, unblinded, uncontrolled, non-randomized, single-centre studies or
anecdotal case series. While randomized controlled trials (RCTs) provide the best
opportunity to evaluate the effectiveness of various treatment options, the expense, time
considerations, sample size limitations and ethical concerns inherent in conducting
these trials make it impossible to rely on them alone. Intercentre collaboration offers
significant advantages by providing insight into the processes and outcomes of
treatment of comparable services at other centres, the establishment of future directions
and the exchange of clearly successful practices (Long, 2011).
The landmark Eurocleft Study, conducted by the orthodontists from 6 major European
cleft-craniofacial centres clearly established the value of intercentre collaboration in
carrying out well controlled retrospective assessments of various treatment
interventions for CLP and led to a number of RCTs of surgical and orthopedic
interventions for primary infant management (Asher-McDade et al., 1992; Mars et al.,

26
1992; Mølsted et al. 1992; Shaw et al. 1992a; Shaw et al. 1992b; Prahl et al. 2001;
Prahl et al. 2003; Prahl et al. 2006; Prahl et al., 2008; Bongaarts et al., 2009).
As an initiative of a task force established by the American Cleft Palate-Craniofacial
Association in 2006, the Americleft project was started to promote collaboration
between North American cleft-craniofacial centres for the purpose of comparing
treatment outcomes. The goal is to identify best practices and allow for evidence-based
decision making in cleft-craniofacial care. Since its establishment, the Americleft
Project has carried out mixed-dentition comparisons of treatment outcomes from
diverse infant management protocols used by eight North American centres with
samples of both UCLP and BCLP patients. The outcome measures included dental
arch relationship ratings of dental casts, skeletal and soft-tissue morphology
assessments of lateral cephalometric radiographs and ratings of nasolabial appearance
of cropped frontal and lateral facial photographs (Daskalogiannakis et al., 2011;
Hathaway et al., 2011; Long et al., 2011; Mercado et al., 2011; Russell et al. 2011).
A number of key findings of particular interest to the orthodontist involved in CLP care
were elucidated from the Americleft study. First, in infant management protocols, the
inclusion of passive PSIO to improve the alignment of the maxillary segments before
primary cleft repair produced no measurable benefits in terms of dental arch
relationship, skeletal morphology or nasolabial aesthetics in the mixed dentition age
patient. The three Americleft centres that did employ PSIO were found to produce
outcomes that were on average either not significantly different, or worse, than the

27
centre that used only primary lip and palate surgery and no PSIO. These findings
corroborated those of both the Eurocleft intercentre study and the Dutchcleft RCT.
Second, the use of NAM as part of the infant management protocol of CUCLP was
evaluated and was shown to produce no measurable improvement in mixed dentition
dental arch relationships or skeletal morphologies. There was some evidence to
suggest that the average nasolabial appearance of the patients from the centre that
utilized NAM was significantly better than that of the patients from the Americleft centre
that did not utilize PSIO or secondary revision surgeries. Conversely, outcomes were
rated as comparable for the centre that employed NAM and those centres that used
secondary revision surgeries to achieve similar outcomes. The final decision as to “best
practice” for improvement of nasolabial appearance for techniques that produce similar
outcomes is thought to rely on a comparison of the burden, cost and risk of care of the
various interventions.
A third finding of the Americleft Project was that the inclusion of primary bonegrafting
was associated with significantly less favourable dental arch relationships and skeletal
morphologies in the mixed dentition in both UCLP and BCLP. Significantly more dental
and skeletal Class III relationships were identified in patients from the Americleft centre
that routinely performed primary bonegrafting as part of its management protocol.
Again, similar findings were noted in the previous Eurocleft intercentre comparison.
The growing body of data gained from these intercentre outcome comparisons, and
those of Eurocleft, should help guide both current treatment decisions and the direction

28
of future studies and further allow clinicians to identify best practices in cleft palate
orthodontic and surgical care (Long, 2011).

29
9. Burden of Care in CLP Treatment
While attempts are being made to improve the evidence regarding treatment
interventions for patients with CLP, information on the quality of life, healthcare use and
costs to affected individuals and their families is lacking. Understanding the effects of
treatment on the well-being of these patients and their caregivers and identifying
healthcare needs is critical for implementing changes in healthcare practices and
policies to improve health outcomes and reduce any unnecessary burden of CLP care
at the individual, family and societal levels (Wehby and Cassell, 2010).
Cost analyses are an objective means of estimating the benefits of primary prevention;
allocating resources for research; assessing expenditures associated with secondary
conditions; and evaluating treatment methodologies among affected children.
Estimates of treatment cost vary by geographic distribution, the type of cleft and
whether funding is via private insurance policies or public health sources.
A 1988 cohort study estimated the lifetime cost associated with CLP treatment to be
approximately $101,000 per each new case in the U.S. (CDC, 1995). Snowden et al.
(2003) used data from four national and two state data systems to estimate the costs of
medically treated craniofacial conditions and reported an estimated annual cost of
$11,350 per case of a congenital craniofacial anomaly including CLP. In 2009, Boulet et
al. reported an annual mean cost difference between children aged 0 through 10 years
with an orofacial cleft and those without of $13,405, with expenditure for a child with an
orofacial cleft approximately eight times higher than for a child the same age without an
orofacial cleft.

30
Data regarding the economic burden and cost effectiveness of infant orthopedics in the
management protocol of CLP are limited. A three-centre RCT was initiated by the
Dutchcleft group to evaluate the cost-effectiveness of IO for improving speech in
patients with CUCLP. Though limited sample sizes were used, the IO group obtained a
statistically significant higher rating of speech quality, compared with the non-IO group,
with minimal financial investment necessary to obtain the improvement. The authors
thereby concluded that from the perspective of speech development, the cost-
effectiveness of IO over non-IO seemed acceptable at that point in time (Konst et al.,
2004). In a similar study, the short-term cost effectiveness of PSIO by means of a
passive Hotz-type appliance was evaluated based on: (1) The time taken for the
surgical lip closure procedure and (2) Medical and non-medical costs until surgical lip
closure at 18 weeks of age. The durations of the surgical lip closure procedures did not
differ significantly (57.2 minutes for the PSIO sample and 56.4 minutes for non-PSIO
sample). The mean medical cost for PSIO treatment was $852 while the non-PSIO
treatment group had a significantly different mean medical cost of $304. Mean travel
costs and indirect nonmedical costs (time off work, etc.) were US$128 and US$231 for
PSIO and US$79 and US$130 for non-PSIO, respectively (Severens et al., 1998).
With respect to the cost effectiveness of NAM, Pfeifer et al. (2002) compared the
financial cost of two different treatment approaches for the correction of CUCLP. In this
study, the records of all patients (n = 30) with UCLP treated by a single surgeon in a
three-year period were examined retrospectively. Group 1 patients (n = 14) were
treated by lip repair, primary nasal repair, and secondary alveolar bone graft prior to
eruption of permanent dentition, while patients in Group 2 (n = 16) were treated by

31
NAM, gingivoperiosteoplasty (GPP), lip repair, and primary nasal repair. The average
cost of treatment for a patient treated by lip repair, primary nasal repair, and secondary
alveolar bone graft prior to eruption of the permanent dentition was calculated to be
$22,744. Of the 16 patients treated by NAM, GPP, lip repair, and primary nasal repair,
the cost was $19,475, with only six patients requiring secondary alveolar bone grafts in
the mixed dentition. Thus, the authors argued that the average cost savings of NAM and
GPP, compared with alveolar bone graft, is $2999, resulting from the decreased number
of patients who require secondary bone grafting. One of the drawbacks of this study is
that the determination of the adequacy of available bone at the cleft site, which affects
the decision as to whether or not a patient is deemed to require a bone graft, relies on a
subjective assessment. Unfortunately, at this time there are no universally accepted
guidelines in the evaluation of the success of an alveolar bone graft (or GPP)
procedure.
The authors did note that a criticism of GPP in the cleft-craniofacial literature is the
potential for impairment of maxillary growth. As a counterpoint, they provide evidence
to suggest that their technique of GPP will not impede maxillary growth as it
necessitates dissection only in the margins of the alveolar cleft after successful
presurgical alignment of the cleft alveolar segments with NAM. The patients in these
studies; however, had not yet completed their pubertal growth spurt to allow for final
assessment of maxillary growth (Wood et al. 1997; Lukash et al., 1998; Lee et al.,
2004). If a significant number of these patients ultimately would require maxillary
advancement surgery, the cost advantage of GPP may be lost. Alternatively, the
proposed advantage of NAM is its improvement of the cleft nasal deformity and a

32
potential reduction in the number of patients that would require secondary revision
surgery to achieve optimal nasolabial aesthetics. If further investigation showed that the
number of cleft nasal revisions is lower in the group treated by NAM and GPP, the total
cost savings of treatment could be even greater than reported (Pfeifer et al., 2002).
Beyond the economic burden, cost of care for patients with CLP can be quantified with
respect to treatment duration and number of appointments. The data related to the
orthodontic burden of care for infant orthopedics, in general, and NAM, in particular, are
limited at this time.
The results of the original Eurocleft study revealed mean ranges of orthodontic
treatment between 3.3 to 8.5 years, and attendance from 49 to 94 appointments for
patients with CUCLP. For infant orthopedics alone, treatment duration ranged from 0 to
15 months of treatment and 0 to 17 orthodontic visits, depending on the infant
management protocol (Semb et al., 2005). In another study attempting to evaluate the
outcome of NAM on nasal symmetry and intraoral dimensions in a sample of 12 patients
with UCLP, the length of NAM therapy was reported to be, on average, 110 days.
Surgical correction of patients with UCLP who underwent NAM was delayed to 3.6
months of age as compared to the standard timing of lip repair of 70 days of age at that
centre (Ezzat et al., 2007). Sicho et al. (2011) reported from data derived from three
CLP centres, that the mean number of clinic visits over an 18-month study period for
patients receiving NAM, for all types of clefts, was significantly greater than for non-
NAM subjects (14 vs. 3.14, respectively).

33
Over the past decade, NAM, a relatively new technique in cleft care, has continued to
grow in popularity. Of the 207 US teams listed in the 2007-2008 ACPA Membership,
Sischo et al. (2011) were able to identify at least 43 (21%) that offered NAM. Advocates
of the technique insist that it provides nasolabial aesthetic outcomes that could not be
achieved with traditional infant orthopedics or surgery alone, whereas opponents argue
that NAM places an extra emotional burden on the family system, which already must
adapt to having a newborn with a malformation (Pope et al., 2005; Sischo et al., 2011).
The emerging evidence and enthusiasm surrounding the short term benefits of NAM
“needs to be weighed against the increased burden of care due to the multiple number
of clinic visits necessary to adjust the appliance during the first year of life. Long-term
outcomes assessing the growth of the midface and both nasal and lip esthetics will be
necessary to determine the benefits of presurgical orthopedics and nasal molding”
(Wyszynski, 2002).

34
Objectives of the Study
To identify and quantify the increased burden of orthodontic care, defined as the
number of orthodontic visits and the total number of days utilizing the appliance,
of NAM over TIO for patients with nonsyndromic CUCLP at SickKids Hospital
To compare nasolabial aesthetic outcomes of various presurgical infant
orthopedic protocols for patients with nonsyndromic CUCLP both at SickKids as
well as from centres that do not utilize PSIO

35
Hypotheses
Hypothesis 1 (H1): Significant differences exist in the burden of orthodontic care when
it involves NAM as compared to TIO for the treatment of patients with nonsyndromic
CUCLP.
Null Hypothesis 1(H01): There exists no difference in the burden of orthodontic care
when it involves NAM as compared to TIO for the treatment of patients with
nonsyndromic CUCLP.
Hypothesis 2 (H2): Significant differences exist in the nasolabial aesthetics of patients
who have received NAM, compared to those who were treated with TIO or surgery
alone, for the initial repair of nonsyndromic CUCLP.
Null Hypothesis 2(H02): There exist no differences in the nasolabial aesthetics of
patients who have received NAM, compared to those who were treated with TIO or
surgery alone, for the initial repair of nonsyndromic CUCLP.

36
Samples and Methods
1. Samples
The subjects for the burden of care analysis of the various PSIO protocols utilized at
SickKids were obtained from a retrospective chart review of consecutively treated
patients at this centre with appliance insertion dates between January 1995 and
September 2005. Two separate samples were compiled. One sample underwent TIO
as part of the former standard protocol at SickKids (prior to 2001), and the second one
received the current protocol, in which NAM has replaced the previously utilized
appliance designs. The year 2005 was selected as the end point of the experimental
period to ensure the presence of photographic records at age 5 in the latter sample of
patients at the time of record evaluation (Fall 2010).
For the assessment of nasolabial aesthetics, retrospective samples from two other
centres that do not utilize PSIO were evaluated, in addition to the two samples
mentioned above. The two other samples were obtained from the Lancaster Cleft
Palate Clinic, Lancaster, PA and the Oslo Cleft Lip and Palate Centre, Oslo, Norway.
As per the original Americleft participants’ agreement, the centre of origin of each
sample will remain anonymous in the presentation of the results.
Approval for the use of the clinical records and standardized cropped photographs were
obtained from the respective Research Ethics Board of each participating centre prior to
initiating the investigation.

37
A. Inclusion/Exclusion Criteria
1. Only Caucasian patients were included in the investigation to avoid bias introduced
by racial variations in craniofacial form.
2. All subjects had been previously diagnosed with a nonsyndromic CUCLP. Any
patients with co-existing associated anomalies or syndromes were excluded.
3. All primary interventions with respect to the cleft, including orthodontic treatment for
PSIO and cleft related surgical procedures, were performed at the institution of
record and complete records of all procedures were available.
4. Subjects where appliance use was discontinued or deemed unsuccessful and
terminated prematurely as recorded in the chart by the treating orthodontist were
excluded (e.g. poor compliance by parent, inability of patient to tolerate appliance).
5. Subjects who underwent lip or nasal revision surgeries during the experimental
period, defined from birth until the date at which assessed photographs were taken,
were excluded.
6. Subjects who underwent any orthodontic intervention including fixed or removable
appliances, headgear or face-mask therapy prior to the date of acquisition of the
photos were excluded.
7. Photographs of subjects at age 4-6 yrs were available for standardization and
assessment. These photographs included standard frontal photographs for all
subjects, and, when available, cleft-side profile photographs. If the cleft-side

38
photograph was unavailable, the noncleft-side photograph was used and rated to
facilitate blinding and uniformity in rating; however, the ratings of the profile view of
the noncleft side were excluded from the analysis of the data.
8. Any subjects with photographs deemed by the primary investigator or by the
consensus of the raters to be of insufficient quality to be reliably rated were
excluded.
B. Descriptive Data/Sample Sizes
The following descriptive data were recorded for each subject included in the
investigation (Appendix 2):
1. Gender
2. Side of cleft
3. Date of insertion of appliance used for PSIO (where applicable)
4. Name of orthodontist responsible for PSIO (where applicable)
5. Date of primary cheilorhinoplasty
6. Name of surgeon who performed primary cheilorhinoplasty
7. Age when photographs were taken to be used in ratings of nasolabial aesthetics
The first sample (referred to as "Centre 1") consisted of 40 individuals of which 23
(57.5%) were male and 17 (42.5%) were female. The cleft was located on the left side

39
in 30 (75%) of subjects and on the right in 10 (25%) of subjects. No PSIO was utilized
and surgical repair was performed by 4 different surgeons. Photographs used for
ratings were taken at a mean age of 5.7 yrs with 31 cleft-side photos available for
standardization.
The second sample (referred to as "Centre 2") consisted of 38 individuals, of which 23
(60.5%) were male and 15 (39.5%) were female. The cleft was located on the left side
in 22 (57.9%) of the subjects and on the right side in 16 (42.1%). No PSIO was utilized
and surgical repair of the cleft was performed by the same surgeon for all subjects.
Photographs used for ratings were taken at a mean age of 5.1 yrs. Sixteen subjects
had cleft-side photographs available for standardization.
The third sample (referred to as "Centre 3(TIO)”) consisted of 38 individuals, of which
23 (60.5%) were male and 15 (39.5%) were female. The cleft was located on the left
side in 26 (68.4%) of the subjects and on the right side in 12 (32.6%). The appliance
treatment was delivered by 10 different orthodontists, with 5 different surgeons
performing the primary surgical repair. Photographs used for ratings were taken at a
mean age of 5.7 years. All subjects had cleft-side photographs available for
standardization.
The fourth sample (referred to as "Centre 3 (NAM)”) consisted of 33 individuals, of
which 25 (75.7%) were male and 8 (24.3%) were female. The cleft was located on the
left side in 21 subjects (63.6%) and on the right side in 11 (36.4%). Overall, 7 different
orthodontists were involved in delivering the NAM appliance treatment and 3 different
surgeons performed the primary repairs on this sample. Photographs used for rating of

40
nasolabial aesthetics in this sample were taken at a mean of 5.7 years of age. All
subjects had cleft-side photographs available for assessment.
The demographic characteristics of the four samples included in the investigation are
depicted in Table 1.
Sample N Cleft L/R M/F Ratio Mean Age Photos
(Range)
Centre 1 40 30/10 23/17 5.7 yrs
(4.5 -6.8 yrs)
Centre 2 38 22/16 23/15 5.1 yrs
(4.9 – 6.0 yrs)
Centre 3 (TIO) 38 26/12 23/15 5.7 yrs
(4.6-6.9 yrs)
Centre 3 (NAM) 33 21/12 25/8 5.7 yrs
(5.0-6.7 yrs)
Totals: 149 99/50 94/55 5.55 yrs
(4.5 – 6.9 yrs)
TABLE 1: Sample Demographics

41
2. Methods
A. Burden of Care
For each of the two samples from SickKids the orthodontic and surgical records were
obtained and the following information was recorded for evaluation of the burden of care
of each PSIO technique: date of appliance insertion, number of scheduled visits for
appliance monitoring or adjustment, number of emergency visits related to appliance (to
rule out extreme outliers due to multiple emergency visits), total number of visits related
to appliance, date of primary cheilorhinoplasty, date of any additional surgical
procedures and the names of the treating orthodontists and surgeons.
Using this data, the burden of orthodontic care of PSIO was calculated by determining
the total number of days utilizing the appliance and the total number of visits required
for appliance fabrication and adjustment. To calculate the number of days utilizing the
appliance, the span between the date the appliance was inserted and the date of the
primary cheilorhinoplasty was calculated. When counting the total number of visits
required for use of the appliance, appointment one was noted as the appointment
during which the impression for appliance fabrication was taken. All subsequent visits
for clinical monitoring or adjustment of the appliance were counted (including
emergency visits) up to the date of surgical repair.
The mean number of visits for appliance fabrication and adjustment and the mean
number of days utilizing the appliance between the two groups were compared using
independent t-tests (Microsoft Office Excel, 2007).
B. Nasolabial Aesthetics Assessment

42
No universally accepted standard rating method to assess facial aesthetics in CLP
exists at this time. However, a method that has become quite popular in recent history
is an index developed by Asher-McDade et al. (1991), specifically aimed at assessment
of treatment outcomes in subjects from different treatment centres. This index has been
used in similar investigations including the Eurocleft study (Asher-McDade et al., 1992;
Brattström et al., 2005), the CSAG study (Williams et al., 2001), and the Americleft
study (Mercado et al., 2011).
The Asher-McDade method utilizes a five-point ordinal scale in which four features of
the nose and lip including nasolabial profile, nasal symmetry, nasal form and vermillion
border are assessed separately and as a whole by a panel of judges (1 = very good
appearance, 2 = good appearance, 3 = fair appearance, 4 = poor appearance and 5 =
very poor appearance).
The method requires standardization and cropping of facial photographs to display only
the nasolabial region in order to reduce the influence of the surrounding facial features,
since it has been shown that judges are influenced by general facial attractiveness.
In this study, for each of the four samples, standard orthodontic frontal and profile
photographs were obtained as close to age 5 as possible, within an acceptable range of
4-6 years of age as long as the subject had not yet undergone any lip or nasal revision
surgeries or orthodontic treatment, as outlined in the exclusion criteria. This age was
selected as it provided the longest follow-up period possible within the confines of this
study during which the only intervention for subjects that might affect nasolabial
aesthetics would include PSIO (if applicable) and the primary repairs of the lip and

43
palate. Lip and nasal revision surgeries and orthodontic treatment both, undoubtedly,
could have an effect on nasolabial aesthetics. These procedures are often initiated
around the time of eruption of the permanent incisor teeth, or prior to the subject
entering elementary school for psychosocial reasons, both occurring around 6-7 years
of age.
The photographs from the two SickKids samples were available in either digital or
photographic slide format depending on the year of photo acquisition. Photographic
slides were scanned at the highest possible resolution and converted to digital images.
The Oslo and Lancaster sample photographs were digitized by scanning photographs
taken with a standard 35mm film camera and forwarded using a powerpoint document
and USB flash drive, respectively. Photos were scanned and saved as JPEG images
with at least a 1400dpi resolution, in accordance with the recommendations in the
Americleft Study Guide.
All images were imported into Adobe Photoshop 6.0 and saved in JPEG format for
preparation by the primary investigator as outlined below.
i. Frontal Images:
The images were oriented with the interpupillary line parallel to the floor to
correct for posturing errors.
The photos were cropped with a trapezoidal outline to expose only the
nasolabial area including the inner canthi region, nasal bridge, nostrils,
alar regions, philtrum and upper lip.

44
ii. Profile Images*:
The photos were cropped to create an outline extending superiorly from
glabella, anteriorly to a point just past the nasal tip, inferiorly to stomion
and angled posterior with a line from glabella tangent to the medial aspect
of the eye to intersect the inferior line passing through stomion.
The backgrounds of the profile images, that varied by centre, were
replaced with a uniform background colour to blind for centre identification.
* To ensure uniformity and standardization of the images for ratings, all profile views
were displayed as right-sided profiles to conform with conventional North American
orthodontic record assessments. In the case where the cleft-side photograph was
available but the cleft occurred on the left, the photograph was flipped so that the cleft
would appear as a right-sided view. If the cleft-side photograph was unavailable, the
unaffected right side image was still cropped and rated by the examiners to ensure
blinding during rating, as examiners may have known which orthodontic records are
standard at each centre. The ratings of unaffected side profiles were not used in the
analysis of the data.
After cropping, each subject’s frontal and profile photographs were inserted into a
powerpoint slide. The master list of subject research numbers from all samples was
randomized and subsequently an unidentifiable case number was assigned to each
slide (subject) to be used for rating. An example of a coded slide is depicted below
(Figure 4).

45
FIGURE 4. Example of coded slide used for rating of nasolabial aesthetics
The complete set of 149 photographs was rated by six orthodontists with experience in
treating subjects with cleft lip and palate, and one orthodontic resident. Two complete
sets of ratings were performed on separate days. Inter- and intra-rater reliabilities were
calculated using weighted kappa statistics.
C. Americleft “Q-Sort” Modification of Asher-McDade Method
Despite the recent popularity of the Asher-McDade method for analysis of nasolabial
appearance in patients with cleft lip and palate, when the same group that rated the
photographs used in the present study utilized the method in a previous study (Mercado
et al., 2011), the inter-rater reliabilities were found to be only moderate-to-good while
the intra-rater reliabilities were found to be good-to-very good. It was felt that the
previous format, in which ratings were completed using a powerpoint presentation
attended by the entire group at the same time provided limited period for viewing and
rating of each slide, potentially allowing for internal creep by the examiner as later

46
subjects might be rated more favourably or harshly than earlier subjects with similar
outcomes after viewing more of the subjects in the sample. For example, an early rated
subject may have been awarded a score of “5” by a particular rater. As the rater
progressed with rating of more and more photographs from the sample, several other
patients judged to have an even poorer appearance than this early patient, could only
be given the same minimum score of “5”. Should the rater be allowed to re-rate the
sample after viewing the entire sample set, his/her internal calibration could be altered
to the point of awarding a higher score to this early seen subject on a subsequent
rating. While, in theory, appropriate calibration of the examiners prior to rating should
minimize this effect, this was viewed by the collective group of raters to be a flaw in the
original method and a limitation in attempting to apply objective measurements to a
subjective assessment of nasolabial appearance.
Since the purpose of the ratings in the context of this and other intercentre collaborative
studies is to have a reliable assessment of the relative differences between samples, a
modification of the Asher-McDade method that might better allow for relative
assessment was proposed and utilized for the ratings in this particular study. The
modification, known as the Q-sort method, was originally proposed in 1953 by
Stephenson and has been used in the orthodontic literature in the assessment of smile
aesthetics (Schabel et al. 2009). The Q-sort method uses a progressive forced choice
narrowing of the sample to create a quasi-normal distribution for rating subjects on an
aesthetic scale from least to most pleasing.

47
In this study the Q-sort method was employed by printing the powerpoint slides onto
standard 4 x 6 inch index cards and laminating them for distribution of a set of photos to
each rater. The raters were then given as much time as needed to divide and re-
arrange the cards into five piles based on the standard Asher-McDade five-point scale
described above. When the rater was satisfied with his or her ratings, the case
numbers corresponding to each pile were recorded on a standard data form and
entered into an Excel spreadsheet (Microsoft Office, 2007). This distribution was
repeated for each variable investigated. Since this method is more time-consuming
than the standard Asher-McDade method, it was collectively decided for the purpose of
this study to group the categories “nasal form” and “nasal symmetry” into a single
category termed “nasolabial frontal”.
In addition, to aid in inter-rater reliability, the raters were given a visual yardstick and a
written outline of the criteria for each number in the five-point scale. The visual
yardstick was an 8.5 x 11 inch laminated print-out of four to five examples of what
constitutes a “1”, “2”, “3”, etc. for each of the three variables. The yardstick was derived
from the examples given in the original Asher-McDade study and by selecting
photographs that were rated uniformly by all raters during a previous study (Mercado et
al., 2011) involving the same group of raters utilizing this rating method. A calibration
session was performed prior to initiation of the ratings to ensure uniform agreement
among raters on the validity of the yardstick. Any photograph in which there was
disagreement among the raters was eliminated from the yardstick.

48
An assessment of the differences in the inter-rater and intra-rater reliabilities using the
Q-sort over the standard Asher-McDade method is currently underway, but is yet
unpublished.
Ratings of the nasolabial aesthetic assessments were compared using a Kruskal Wallis
one-way analysis of variance test with pairwise comparisons to identify significant
differences among samples for each individual aesthetic variable as well as the total
overall score. Chi-square analyses were also performed to test for significant
differences in the distribution of scores for each variable within each sample. All tests
were performed using the Minitab 16 Statistical Software program (Minitab Inc., 2010).

49
Results
1. Burden of Care of NAM vs. TIO
The results of the burden of care analysis for the number of visits required for appliance
fabrication and adjustment and the number of days each appliance was worn for the
NAM and TIO groups are displayed in Tables 2 & 3 and Figures 5 & 6, respectively.
Statistically significant differences between the two groups were detected for both
variables using two-tailed, independent t-tests (p<0.001; p<0.05).
Mean SD Range
NAM 9.94* 2.60 5-16
TIO 6.58 1.35 4-10
Table 2. Means, standard deviations and ranges for the number of visits for appliance
fabrication and adjustment for the NAM and TIO groups (*p<0.001)
Mean SD Range
NAM 127.51* 32.46 79-233
TIO 112.18 31.92 72-197
Table 3. Means, standard deviations and ranges for the number of days each appliance
was worn for the NAM and TIO groups (*p<0.05)

50
Figure 5. Means and standard errors for the number of visits for appliance fabrication
and adjustment (p< 0.001)
Figure 6. Means and standard errors for the number of days each appliance was worn
(p<0.05)
9.9
6.6
0
2
4
6
8
10
12
NAM TIO
# o
f V
isit
s
127.5
112.2
0
20
40
60
80
100
120
140
NAM TIO
# o
f D
ays

51
2. Nasolabial Aesthetic Ratings
Intra- and Inter-rater Reliabilities
Table 4 summarizes the weighted kappa values for the evaluation of intra- and inter-
examiner reliabilities for the three categories of nasolabial aesthetic ratings averaged
among seven raters.
Intra-rater Inter-rater
Vermillion Border 0.785 (0.704-0.855) 0.629 (0.588-0.668)
Nasolabial Frontal 0.744 (0.621-0.901) 0.549 (0.495-0.607)
Nasolabial Profile 0.711 (0.569-0.822) 0.517 (0.408-0.570)
Table 4. Mean weighted kappa values (and ranges) for the intra-rater and inter-rater
reliability assessments among seven raters for the three categories of nasolabial
aesthetics.
Overall substantial intra-rater agreement was observed for all three variables. The inter-
rater reliability was found to be moderate (nasolabial frontal and nasolabial profile) to
substantial (vermillion border) across the seven raters (Landis and Koch,1977).
Nasolabial Aesthetics Scores
The frequency distributions of each raw score from 1 to 5 in each sample are shown in
Figures7, 8 & 9 for the various categories of nasolabial aesthetics.

52
Figure 7. Frequency of each raw score from 1 to 5 for each sample for the category VB
(vermillion border)
Figure 8. Frequency of each raw score from 1 to 5 for each sample for the category
NLF (nasolabial frontal)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
CTR 1 CTR 2 CTR 3 (TIO) CTR 3 (NAM)
1
2
3
4
5
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
CTR1 CTR2 CTR3 (TIO) CTR3 (NAM)
1
2
3
4
5

53
Figure 9. Frequency of each raw score from 1 to 5 for each sample for the category
NLP (nasolabial profile)
A chi square analysis was performed to identify any significant differences in the
percent distribution of scores between the groups for each category. Tables 5, 6 & 7
summarize the results of the chi square tests.
Score 1 vs 2 1 vs 3 (TIO) 1 vs 3 (NAM) 2 vs 3 (TIO) 2 vs 3 (NAM) 3 (TIO) vs 3 (NAM)
1 nsd nsd * nsd * nsd
2 * * * nsd nsd nsd
3 nsd * nsd nsd nsd *
4 nsd * * * * nsd
5 * * * nsd nsd nsd
Table 5. Summary of the chi square analysis of the percent distribution in scores for the
category “vermilion border” (nsd = no significant difference)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
CTR 1 CTR 2 CTR 3 (TIO) CTR 3 (NAM)
1
2
3
4
5

54
Score 1 vs 2 1 vs 3 (TIO) 1 vs 3 (NAM) 2 vs 3 (TIO) 2 vs 3 (NAM) 3 (TIO) vs 3 (NAM)
1 * nsd nsd * nsd nsd
2 * nsd nsd * * nsd
3 nsd nsd nsd nsd nsd nsd
4 * nsd nsd * * nsd
5 * nsd * * nsd *
Table 6. Summary of the chi square analysis of the percent distribution in scores for the
category “nasolabial frontal” (nsd = no significant difference)
Score 1 vs 2 1 vs 3 (TIO) 1 vs 3 (NAM) 2 vs 3 (TIO) 2 vs 3 (NAM) 3 (TIO) vs 3 (NAM)
1 nsd nsd * nsd nsd *
2 nsd nsd nsd nsd nsd nsd
3 * nsd nsd nsd nsd nsd
4 nsd nsd * nsd nsd nsd
5 * nsd nsd * * nsd
Table 7. Summary of the chi square analysis of the percent distribution in scores for the
category “nasolabial profile” (nsd = no significant difference)

55
The mean scores across all four samples for each individual category along with the
mean cumulative total scores are depicted in Figure 10.
Figure 10. Mean nasolabial aesthetic scores for each individual category and for the
cumulative scores in each sample
A Kruskal-Wallis test was conducted to evaluate differences among the four samples in
the scores for the nasolabial aesthetic ratings. The test revealed statistically significant
differences between the samples in the categories “vermillion border” and “nasolabial
frontal” (p < 0.001; p= 0.002), as well as in the cumulative scores for overall nasolabial
aesthetics (p = 0.007). No significant differences were detected between samples for
the category “nasolabial profile” (p > 0.05). Follow-up tests were conducted to evaluate
pairwise differences among the four samples, controlling for Type I error across tests
using the Bonferroni correction.
0
0.5
1
1.5
2
2.5
3
3.5
4
Vermilion Border Nasolabial Frontal Nasolabial Profile Cumulative Score
Centre 1
Centre 2
Centre 3 (TIO)
Center 3 (NAM)

56
Within the category “vermillion border”, pairwise comparisons revealed significant
differences between Centre 1 and the TIO sample from Centre 3 (p=0.003) and
between Centre 1 and NAM sample from Centre 3 (p<0.001), with both samples from
Centre 3 exhibiting superior nasolabial aesthetic scores.
Within the category “nasolabial frontal”, significant differences were detected between
Centres 1 and 2 (p<0.001) with Centre 2 exhibiting the greater (less favourable) score
and between Centres 2 and Centre 3 (TIO) with the TIO sample demonstrating superior
ratings.
When the three categories were averaged to determine an overall cumulative score,
statistically significant differences were revealed between Centre 2 and the TIO sample
from Centre 3 (p <0.001) with the TIO group exhibiting improved overall aesthetics.

57
The median values for each sample across the aesthetic categories and the results of
the Kruskal Wallis multiple and pairwise comparisons are summarized in Table 8.
Vermillion
Border
Nasolabial
Frontal
Nasolabial
Profile
Cumulative
Score
Centre 1 3.39a,b 2.93c 2.71 3.00
Centre 2 3.07 3.36c,d 2.82 3.21e
Centre 3 (TIO) 2.79a 2.82d 2.86 2.82e
Centre 3 (NAM) 2.36b 3.00 3.07 2.86
Kruskal-Wallis
(Multiple
Comparisons)
p < 0.001 p = 0.002 p > 0.05 p = 0.007
Table 8. Median values of nasolabial aesthetics ratings using the modified Asher-
McDade method. [Pairwise comparison significant differences: a (p = 0.003); b, c, d, e
(p < 0.001)]

58
Discussion
A number of publications reporting immediate postsurgical improvements in nasal
symmetry following NAM therapy (Grayson et al. 1999, 2001, Maull et al. 1999; Liou et
al. 2004) have led advocates of the technique to call for a “paradigm shift” in infant CLP
management from more traditional methods of PSIO (Grayson and Maull, 2004).
However, as has previously been stated, the mounting evidence and enthusiasm
surrounding short-term benefits of NAM must be balanced against the increased burden
of care due to the multiple clinic visits and treatment costs necessary to institute such
care. Even more importantly, long-term outcome assessment is necessary before the
various proposed benefits of presurgical orthopedics and nasal molding can be claimed
(Wyszynski, 2002; Long, 2011).
In this study, a significant increase in the burden of orthodontic care of NAM over TIO
was identified, both with respect to the number of days in treatment and the number of
appointments required to implement care. However, no significant differences in the
nasolabial aesthetic outcomes of these subjects could be identified by orthodontists with
experience in cleft care. In short, with respect to nasolabial aesthetics, an increased
burden of care was identified when using NAM over TIO, without a measurable
associated benefit.
Interestingly, when comparing these two groups of subjects who underwent PSIO
during infancy to two groups of subjects from centres that performed surgical repair of
the cleft without PSIO, significant differences in scores for the categories of vermillion

59
border, nasolabial frontal and overall nasolabial aesthetics were elucidated. The
analysis demonstrated more favourable outcomes in the groups of subjects that
underwent either TIO or NAM. This finding is inconsistent with previous studies in
which centres with the highest intensity of early treatment achieved the lowest rankings
for eventual outcome (Shaw et al., 2005). Moreover, an RCT designed to assess this
very topic failed to show an effect of traditional infant orthopedics on facial appearance
in the long term (Prahl et al. 2006).
Results of retrospective multicentre investigations must always be interpreted with
caution as “a fundamental limitation of intercenter comparisons is that they cannot
distinguish between the influence of different individual elements of a center's protocol
on its outcomes nor between its protocols and the influence of the personnel who
deliver that protocol.” (Shaw et al., 2005)
In this study, the assessment of nasolabial aesthetics is performed at the age of 5 and
not later, in an attempt to minimize the compounded effect of every individual procedure
or component of the protocol, a concern that would have been greater, the later the age
of the subjects at the time of evaluation. By rating photographs taken at approximately
age five and excluding subjects that had undergone any additional treatment beyond
primary lip and palate repair and PSIO, if applicable, this study attempted to focus on
the influence of a single variable, the employment of either TIO or NAM.
The influence of additional variables, such as genetic variability, the type of surgical
repair and the personnel delivering the protocol, were the obvious limitations of this
investigation. The WHO (2004) referred to the confounding effect of discrepancies in

60
surgical skill and technique as proficiency bias, stating that it confounds any attempt at
comparisons of outcomes, except within randomized trials. Within the four samples in
this study, primary repair was performed by anywhere between one and five surgeons
with varying surgical experience and methods of repair. While the NAM and TIO
samples were treated by a number of the same surgeons, the distribution was not
uniform between the two groups. This proficiency bias makes it impossible to draw
definitive conclusions regarding whether any observed differences in aesthetic
outcomes truly reflect the influence of the PSIO procedure or are merely a reflection of
the technical skills of different operators within and across samples.
Another challenge in performing intercentre collaborative studies, or even intracentre
studies in centres serving modern urban communities that are ethnically and racially
diverse, is the enormous heterogeneity in the original cleft deformity and underlying
craniofacial form that exists among subjects. Even in children born with the same type
of cleft and treated by identical procedures, outcomes can differ considerably due to the
great genetic variability observed in individuals born with CLP (Mølsted, 1999). An
attempt was made to minimize this heterogeneity to the extent possible, by limiting the
inclusion in this investigation to subjects with non-syndromic CUCLP patients of
Caucasian background.
In its original articles, the Eurocleft group stated that ideal sample sizes for
assessments of cephalometric soft- and hard-tissue measurements and for ratings of
dental arch relationships using the Goslon yardstick, should comprise between 30 and
40 subjects per sample. No recommendations were given for ideal sample sizes for

61
assessment of nasolabial appearance (Shaw et al., 1992). When the same group
conducted its own intercentre assessments of nasolabial appearance, sample sizes of
fewer than 20 subjects in most groups were used with large variability in sample sizes
among centres, due to inadequate available records (Asher-McDade et al., 1992).
When the Americleft group examined the nasolabial appearance of subjects from four
centres, sample sizes were increased slightly (ranging between 21 to 37 subjects per
centre), but with the largest group of 37 subjects limited to just 6 profile images of the
affected side for ratings of profile aesthetics (Mercado et al., 2011). These reduced
sample sizes are indicative of the difficulties encountered in investigations of this type,
mainly owing to the inadequacies of record keeping.
To address the issue of sample size determination in the assessment of the aesthetic
outcomes of cleft lip repair, Power and Matic (2012) conducted a study to determine the
ideal sample size required to critically analyze consecutive unilateral cleft lip repairs and
to determine the number of consecutive cases that represent average outcomes.
Consecutive pre-operative and two-year post-operative photographs of CUCLP subjects
were randomized and evaluated by craniofacial surgeons. Results showed that
calculations for 10 consecutive cases demonstrated wide 95% confidence intervals,
spanning two points on the post-operative grading scales, however the confidence
intervals narrowed within one qualitative grade (±0.30) and one point (±0.50) on the ten-
point scale when a sample size increased to 27 consecutive cases. The authors
concluded that increasing numbers of consecutive cases (n>27) are increasingly
representative of average results.

62
In the present investigation, sample sizes between 33 and 40 subjects were obtained
from each centre; however, similar to Mercado et al. (2011), several profile images of
the nonaffected side had to be excluded in the final analysis from the two centres not
employing PSIO. The residual samples sizes of 16 and 31 subjects for profile
assessments in these two groups were still equal to or greater than previous studies of
this nature. It should be noted that while statistically significant differences were
observed between centres that did and did not employ PSIO for the categories
vermillion border and nasolabial frontal, no significant differences were detected
between samples for the nasolabial profile category. The inability to detect significant
differences for this variable may reflect that, in fact, no differences in aesthetic
outcomes exist, or, may simply be the result of reduced power from decreasing sample
sizes.
Aesthetic outcome assessments inevitably carry a high degree of subjectivity.
Moreover, the use of still photographic images has many limitations (Tobiasen, 1988;
Asher-McDade et al., 1992; Morrant and Shaw, 1996). While results of studies using 3-
dimensional assessments are becoming rapidly available and may represent the future
of cleft deformity analysis, digital 2-dimensional photographs are still the most widely
available, economical and accessible clinical records for use in intercentre collaborative
studies. Recognizing the inherent limitations, the Asher-McDade method has been
shown to be reliable and reproducible and has been used in similar multicentre
assessments of nasolabial aesthetics in the past; it was therefore selected for use in
this study (Brattström et al., 2005; Williams et al., 2001; Mercado et al., 2011).

63
A criticism of this method is that it does not take into account more characteristics of the
repaired lip, such as the scar, contour of the philtrum and the white roll. Evaluation of
this kind of detail requires images of high resolution under standardized lighting and
precise patient positioning, a virtual impossibility in a retrospective intercentre
comparison. In this study, some images were scanned from printed photos, others from
slides and others were obtained directly from digital cameras with high resolution.
While variations in image quality can be overcome in the gross evaluation of the
continuity of the vermillion border, shape of the nose, and profile using the Asher-
McDade method, evaluation of the upper lip in greater objective detail would require live
subjects or highly standardized images at the same resolution (Mercado et al., 2011).
A further criticism of the method used to assess nasolabial appearance in this study is
that it did not include a worm’s-eye view photograph that is thought, by some, to be the
best angle to assess nostril symmetry and deviations in nasal form. Conversely,
although the worm’s-eye view may, in fact, be the best angle to assess symmetry of the
nostrils from a professional point of view, this angle is rarely shown in social
circumstances and may be an unrealistic measure of attainment of the ultimate goal of
cleft surgery, that being the reduction of visible social stigmata (Kuijpers-Jagtman et al.,
2009). Regardless, the worm’s eye view, like the affected-side profile view, was not
consistently available from the centres in this study. A consideration for future research
endeavors is the creation of a method for standardized record taking, both with respect
to image quality and to which views should be included in a standard photographic
series.

64
With respect to the reliability of the method for rating nasolabial aesthetics, an overall
substantial intrarater reliability was achieved (mean 0.747), while moderate interrater
reliabilities were observed (mean 0.565). While these results are similar to previous
studies employing this rating method (Asher-McDade et al. 1992; Williams et al. 2001;
Brattström et al. 2005; Mercado et al. 2011), ideally more standardized, objective
assessment methods should be developed to improve the reliability and accuracy of the
evaluation of nasolabial aesthetic outcomes in this patient population.
In the first part of this study, comparisons were made between the burden of orthodontic
care of two groups of subjects at the same centre treated during different time periods
with two types of PSIO, TIO or NAM. For the purposes of calculation in this study the
time of initial lip repair was taken as the endpoint of PSIO treatment. Since these
samples were drawn from two different time periods, it is important to note that
variations in surgical wait times may have confounded the difference in the results
between the two groups. While this centre's patient population has been steadily
increasing with time, available operating room time has been slowly decreasing. This
could mean that the more recent sample may have had to endure a longer wait for a
surgical date for cheilorhinoplasty. It is conceptually possible that PSIO treatment
objectives for a specific patient can be met, but because a surgical date is not
immediately available, the orthodontist might elect to continue to see the patient on a
maintenance basis, thereby artificially inflating the calculated burden of care. A recent
prospective study was conducted to determine the duration of wait times for surgery for
children and youth at Canadian pediatric academic health institutions and to determine
the percentage of patients receiving surgery after a predetermined acceptable target

65
waiting period. Overall, 27% of pediatric patients from across Canada received their
surgery beyond their standardized target waiting period. Dentistry, ophthalmology,
plastic surgery for cleft lip and palate and cancer surgery showed the highest
percentages of surgeries completed past target (Wright and Menaker, 2011). Due to
the retrospective nature of this study, data on patients’ wait times for surgery after
completion of PSIO could not be obtained, as this type of information was not recorded
in the orthodontic or surgical records. Any assumptions made about the potential
confounding effect of surgical wait times on the results are merely speculative.
While prolonged surgical wait times may have resulted in the overestimation of the
burden of care in one or both samples, the magnitude of the burden of either sample
may have been underestimated by cancelled or missed appointments. Again, as a
result of the retrospective nature of this study, it was only possible to record the number
of appointments actually attended by the subject, rather than scheduled by the
practitioner. Patient burnout is a well-documented phenomenon in the literature of
organizational behaviour and industrial psychology. Orthodontics is known to be a
dental specialty in which long-term patient cooperation and attendance at appointments
is a major factor influencing treatment success (Brezniak and Ben-Ya’ir, 1989). It has
been shown that patients with CLP may be considered at a particular risk of burnout
and poor attendance with clinic appointments as a result of considerable demands on
the family to attend an extraordinary number of outpatient appointments, and because
many multidisciplinary cleft lip and palate clinics are regional, necessitating
considerable travel (Rivkin et al., 2000; Rodd et al., 2007). It is likely that as the burden
of care and demand on parents’ schedules increase, appointment failure rates may

66
follow. Failure to schedule or keep appointments may account for why, despite being
statistically significant, the magnitude of the difference in the number of appointments
between the TIO and NAM groups was minimal (mean of 3.3 visits) and smaller than
one might expect knowing the suggested protocol for each technique.
Finally, while in this study no benefit was found to justify the added burden when
comparing NAM and TIO, it is important to realize that these findings addressed only
one aspect of the burden against one of the proposed benefits of the technique. It has
been suggested that in addition to long term improvements in aesthetics, NAM therapy
facilitates and shortens the primary surgical repair and reduces the number of surgical
revisions performed to correct excessive scar tissue and nasal and labial deformities
(Maull et al.,1999; Grayson and Shetye, 2009). These additional claimed advantages of
NAM could not be assessed by the present investigation. Future prospective studies
should assess these variables to allow for a more comprehensive comparison of the
overall burden of care with each intervention.

67
Conclusions
Under the conditions of this investigation the following conclusions can be drawn:
1. Significant differences exist in the burden of orthodontic care when it involves NAM
as compared to TIO for the treatment of patients with non-syndromic CUCLP, with NAM
patients requiring more appointments and a greater number of days wearing the
appliance.
2. No significant differences exist in the nasolabial aesthetics of patients who have
received NAM as compared to TIO for the initial repair of non-syndromic CUCLP at age
4-6 years.
3. Significant differences exist in the nasolabial aesthetics between centres that utilize
PSIO and those that do not, with centres not employing PSIO demonstrating poorer
nasolabial aesthetics across several categories.

68
Clinical Significance & Future Directions
It is incumbent upon health care professionals providing any treatment for a patient to
perform a risk- and cost-benefit analysis of any intervention to enable them to make
sound, scientific, evidence-based decisions regarding patient care. The burden of CLP
treatment to the individual patients, their families and the health care system is known to
be quite significant. Streamlining treatment protocols and eliminating unnecessary
procedures should be a focus of every CLP centre when evaluating existing protocols
for potential modifications.
The present investigation was conducted with the hope to shed light on the increased
burden imposed on patients undergoing NAM over traditional IO in the absence of
noticeable benefits with respect to nasolabial aesthetics. Furthermore, studies like this
one, along with similar intercentre investigations, like the Eurocleft and Americleft
projects, should alert the CLP community to the concern regarding the lack of standards
in recording and reporting outcomes, and the absence of quality evidence upon which
centres can base their current protocols. It is hoped that results obtained from
retrospective, cross-sectional comparisons such as this one can be used to design
future RCTs to objectively assess outcomes of interventions for patients with CLP more
objectively, so that clinicians may maximize treatment benefits while minimizing burden.

69
References
Al-Omari I, Millett DT, Ayoub A, Bock M, Ray A, Dunaway D, et al. An appraisal of three methods of rating facial deformity in patients with repaired complete unilateral cleft lip and palate. Cleft Palate Craniofac J. 2003 Sep;40(5):530-7.
Al-Omari I, Millett DT, Ayoub AF. Methods of assessment of cleft-related facial deformity: a review. Cleft Palate Craniofac J. 2005 Mar;42(2):145-56.
Arosarena OA. Cleft lip and palate. Otolaryngol Clin North Am. 2007 Feb;40(1):27,60, vi.
Asher-McDade C, Brattström V, Dahl E, McWilliam J, Mølsted K, Plint DA, et al. A six-center international study of treatment outcome in patients with clefts of the lip and palate: Part 4. Assessment of nasolabial appearance. Cleft Palate Craniofac J. 1992 Sep;29(5):409-12.
Asher-McDade C, Roberts C, Shaw WC, Gallager C. Development of a method for rating nasolabial appearance in patients with clefts of the lip and palate. Cleft Palate Craniofac J. 1991 Oct;28(4):385,90; discussion 390-1.
Assuncao AG. The V.L.S. classification for secondary deformities in the unilateral cleft lip: clinical application. Br J Plast Surg. 1992 May-Jun;45(4):293-6.
Barillas I, Dec W, Warren SM, Cutting CB, Grayson BH. Nasoalveolar molding improves long-term nasal symmetry in complete unilateral cleft lip-cleft palate patients. Plast Reconstr Surg. 2009 Mar;123(3):1002-6.
Becker M, Svensson H, Jacobsson S. Clinical examination compared with morphometry of digital photographs for evaluation of repaired cleft lips. Scand J Plast Reconstr Surg Hand Surg. 1998 Sep;32(3):301-6.
Benson PE, Richmond S. A critical appraisal of measurement of the soft tissue outline using photographs and video. Eur J Orthod. 1997 Aug;19(4):397-409.
Berkowitz S. Cleft Lip and Palate. 2nd ed. Spring Publishing Group; 2006.
Berkowitz S, Mejia M, Bystrik A. A comparison of the effects of the Latham-Millard procedure with those of a conservative treatment approach for dental occlusion and facial aesthetics in unilateral and bilateral complete cleft lip and palate: part I. Dental occlusion. Plast Reconstr Surg. 2004 Jan;113(1):1-18.
Bhattacharya S, Khanna V, Kohli R. Cleft lip: The historical perspective. Indian J Plast Surg. 2009 Oct;42 Suppl:S4-8.
Bilwatsch S, Kramer M, Haeusler G, Schuster M, Wurm J, Vairaktaris E, et al. Nasolabial symmetry following Tennison-Randall lip repair: a three-dimensional

70
approach in 10-year-old patients with unilateral clefts of lip, alveolus and palate. J Craniomaxillofac Surg. 2006 Jul;34(5):253-62.
Bongaarts CA, Kuijpers-Jagtman AM, van 't Hof MA, Prahl-Andersen B. The effect of infant orthopedics on the occlusion of the deciduous dentition in children with complete unilateral cleft lip and palate (Dutchcleft). Cleft Palate Craniofac J. 2004 Nov;41(6):633-41.
Bongaarts CA, Prahl-Andersen B, Bronkhorst EM, Prahl C, Ongkosuwito EM, Borstlap WA, et al. Infant orthopedics and facial growth in complete unilateral cleft lip and palate until six years of age (Dutchcleft). Cleft Palate Craniofac J. 2009 Nov;46(6):654-63.
Bongaarts CA, Prahl-Andersen B, Bronkhorst EM, Spauwen PH, Mulder JW, Vaandrager JM, et al. Effect of infant orthopedics on facial appearance of toddlers with complete unilateral cleft lip and palate (Dutchcleft). Cleft Palate Craniofac J. 2008 Jul;45(4):407-13.
Bongaarts CA, van 't Hof MA, Prahl-Andersen B, Dirks IV, Kuijpers-Jagtman AM. Infant orthopedics has no effect on maxillary arch dimensions in the deciduous dentition of children with complete unilateral cleft lip and palate (Dutchcleft). Cleft Palate Craniofac J. 2006 Nov;43(6):665-72.
Boulet SL, Grosse SD, Honein MA, Correa-Villasenor A. Children with orofacial clefts: health-care use and costs among a privately insured population. Public Health Rep. 2009 May-Jun;124(3):447-53.
Brattström V, McWilliam J, Larson O, Semb G. Craniofacial development in children with unilateral clefts of the lip, alveolus, and palate treated according to four different regimes. I. Maxillary development. Scand J Plast Reconstr Surg Hand Surg. 1991;25(3):259-67.
Brattström V, McWilliam J, Semb G, Larson O. Craniofacial development in children with unilateral clefts of the lip, alveolus, and palate treated according to four different regimes. II. Mandibular and vertical development. Scand J Plast Reconstr Surg Hand Surg. 1992;26(1):55-63.
Brattström V, Mølsted K, Prahl-Andersen B, Semb G, Shaw WC. The Eurocleft study: intercenter study of treatment outcome in patients with complete cleft lip and palate. Part 2: craniofacial form and nasolabial appearance. Cleft Palate Craniofac J. 2005 Jan;42(1):69-77.
Brezniak N, Ben-Ya'ir S. Patient burnout - behaviour of young adults undergoing orthodontic treatment. Stress Med. 1989;5:183-187.
Centers for Disease Control and Prevention (CDC). Economic costs of birth defects and cerebral palsy--United States, 1992. MMWR Morb Mortal Wkly Rep. 1995 Sep 22;44(37):694-9.

71
Chan KT, Hayes C, Shusterman S, Mulliken JB, Will LA. The effects of active infant orthopedics on occlusal relationships in unilateral complete cleft lip and palate. Cleft Palate Craniofac J. 2003 Sep;40(5):511-7.
Coghlan BA, Matthews B, Pigott RW. A computer-based method of measuring facial asymmetry. Results from an assessment of the repair of cleft lip deformities. Br J Plast Surg. 1987 Jul;40(4):371-6.
Cordero DR, Brugmann S, Chu Y, Bajpai R, Jame M, Helms JA. Cranial neural crest cells on the move: their roles in craniofacial development. Am J Med Genet A. 2011 Feb;155A(2):270-9.
Cussons PD, Murison MS, Fernandez AE, Pigott RW. A panel based assessment of early versus no nasal correction of the cleft lip nose. Br J Plast Surg. 1993 Jan;46(1):7-12.
Cutting C, Grayson B, Brecht L, Santiago P, Wood R, Kwon S. Presurgical columellar elongation and primary retrograde nasal reconstruction in one-stage bilateral cleft lip and nose repair. Plast Reconstr Surg. 1998 Mar;101(3):630-9.
Daskalogiannakis J, Mercado A, Russell K, Hathaway R, Dugas G, Long RE,Jr, et al. The Americleft study: an inter-center study of treatment outcomes for patients with unilateral cleft lip and palate part 3. Analysis of craniofacial form. Cleft Palate Craniofac J. 2011 May;48(3):252-8.
Dixon M, Marazita M, Beaty T, Murray J. Cleft lip and palate: understanding genetic and environmental influences. Nature Reviews Genetics. 2011;12:167-178.
Duffy S, Noar JH, Evans RD, Sanders R. Three-dimensional analysis of the child cleft face. Cleft Palate Craniofac J. 2000 Mar;37(2):137-44.
Eliason MJ, Hardin MA, Olin WH. Factors that influence ratings of facial appearance for children with cleft lip and palate. Cleft Palate Craniofac J. 1991 Apr;28(2):190,3;193-4.
Ezzat CF, Chavarria C, Teichgraeber JF, Chen JW, Stratmann RG, Gateno J, et al. Presurgical nasoalveolar molding therapy for the treatment of unilateral cleft lip and palate: a preliminary study. Cleft Palate Craniofac J. 2007 Jan;44(1):8-12.
Farkas LG, Hajnis K, Posnick JC. Anthropometric and anthroposcopic findings of the nasal and facial region in cleft patients before and after primary lip and palate repair. Cleft Palate Craniofac J. 1993 Jan;30(1):1-12.
Farmand M. Lip repair techniques and their influence on the nose. Facial Plast Surg. 2002 Aug;18(3):155-64.
Feragen KJ, Semb G, Magnussen S. Asymmetry of left versus right unilateral cleft impairments: an experimental study of face perception. Cleft Palate Craniofac J. 1999 Nov;36(6):527-32.

72
Fisher DM, Lo LJ, Chen YR, Noordhoff MS. Three-dimensional computed tomographic analysis of the primary nasal deformity in 3-month-old infants with complete unilateral cleft lip and palate. Plast Reconstr Surg. 1999 Jun;103(7):1826-34.
Foong KW, Sandham A, Ong SH, Wong CW, Wang Y, Kassim A. Surface laser scanning of the cleft palate deformity--validation of the method. Ann Acad Med Singapore. 1999 Sep;28(5):642-9.
Frey M, Giovanoli P, Gerber H, Slameczka M, Stussi E. Three-dimensional video analysis of facial movements: a new method to assess the quantity and quality of the smile. Plast Reconstr Surg. 1999 Dec;104(7):2032-9.
Friede H, Lilja J, Johanson B. Lip-nose morphology and symmetry in unilateral celft lip and palate patients following a two-stage lip closure. Scand J Plast Reconstr Surg. 1980;14(1):55-64.
Fudalej P, Katsaros C, Hozyasz K, Borstlap WA, Kuijpers-Jagtman AM. Nasolabial symmetry and aesthetics in children with complete unilateral cleft lip and palate. Br J Oral Maxillofac Surg. 2012 Jan 13 (Epub ahead of print).
Georgiade NG, Latham RA. Maxillary arch alignment in the bilateral cleft lip and palate infant, using pinned coaxial screw appliance. Plast Reconstr Surg. 1975 Jul;56(1):52-60.
Glass L, Starr CD, Stewart RE, Hodge SE. Indentikit Model II--a potential tool for judging cosmetic appearance. Cleft Palate J. 1981 Apr;18(2):147-51.
Graf-Pinthus B, Bettex M. Long-term observation following presurgical orthopedic treatment in complete clefts of the lip and palate. Cleft Palate J. 1974 Jul;11(0):253-60.
Grayson BH, Cutting C, Wood R. Preoperative columella lengthening in bilateral cleft lip and palate. Plast Reconstr Surg. 1993 Dec;92(7):1422-3.
Grayson BH, Cutting CB. Presurgical nasoalveolar orthopedic molding in primary correction of the nose, lip, and alveolus of infants born with unilateral and bilateral clefts. Cleft Palate Craniofac J. 2001 May;38(3):193-8.
Grayson BH, Maull D. Nasoalveolar molding for infants born with clefts of the lip, alveolus, and palate. Clin Plast Surg. 2004 Apr;31(2):149,58, vii.
Grayson BH, Santiago PE, Brecht LE, Cutting CB. Presurgical nasoalveolar molding in infants with cleft lip and palate. Cleft Palate Craniofac J. 1999 Nov;36(6):486-98.
Grayson BH, Shetye PR. Presurgical nasoalveolar moulding treatment in cleft lip and palate patients. Indian J Plast Surg. 2009 Oct;42 Suppl:S56-61.
Hathaway R, Daskalogiannakis J, Mercado A, Russell K, Long RE,Jr, Cohen M, et al. The Americleft study: an inter-center study of treatment outcomes for patients with

73
unilateral cleft lip and palate part 2. Dental arch relationships. Cleft Palate Craniofac J. 2011 May;48(3):244-51.
Heller M, Schmidt M, Mueller CK, Thorwarth M, Schultze-Mosgau S. Clinical-anthropometric and aesthetic analysis of nose and lip in unilateral cleft lip and palate patients. Cleft Palate Craniofac J. 2011 Jul;48(4):388-93.
Hotz M, Gnoinski W. Comprehensive care of cleft lip and palate children at Zurich university: a preliminary report. Am J Orthod. 1976 Nov;70(5):481-504.
Hotz M, Gnoinski W. The determining role of gnatho-orthopedics in modern treatment of cleft lip-palate (surgical-orthopedic coordinated technique). Mondo Ortod. 1976 Oct-Nov;18(5):25-41.
Hotz MM. Pre- and early postoperative growth-guidance in cleft lip and palate cases by maxillary orthopedics (an alternative procedure to primary bone-grafting). Cleft Palate J. 1969 Oct;6:368-72.
Hotz MM, Gnoinski WM, Nussbaumer H, Kistler E. Early maxillary orthopedics in CLP cases: guidelines for surgery. Cleft Palate J. 1978 Oct;15(4):405-11.
Jaeger M, Braga-Silva J, Gehlen D, Sato Y, Zuker R, Fisher D. Correction of the alveolar gap and nostril deformity by presurgical passive orthodontia in the unilateral cleft lip. Ann Plast Surg. 2007 Nov;59(5):489-94.
Johnson N, Sandy J. An aesthetic index for evaluation of cleft repair. Eur J Orthod. 2003 Jun;25(3):243-9.
Kaartinen V, Voncken JW, Shuler C, Warburton D, Bu D, Heisterkamp N, et al. Abnormal lung development and cleft palate in mice lacking TGF-beta 3 indicates defects of epithelial-mesenchymal interaction. Nat Genet. 1995 Dec;11(4):415-21.
Kirschner RE, LaRossa D. Cleft lip and palate. Otolaryngol Clin North Am. 2000 Dec;33(6):1191,215, v-vi.
Kohout MP, Aljaro LM, Farkas LG, Mulliken JB. Photogrammetric comparison of two methods for synchronous repair of bilateral cleft lip and nasal deformity. Plast Reconstr Surg. 1998 Oct;102(5):1339-49.
Konst EM, Prahl C, Weersink-Braks H, De Boo T, Prahl-Andersen B, Kuijpers-Jagtman AM, et al. Cost-effectiveness of infant orthopedic treatment regarding speech in patients with complete unilateral cleft lip and palate: a randomized three-center trial in the Netherlands (Dutchcleft). Cleft Palate Craniofac J. 2004 Jan;41(1):71-7.
Konst EM, Rietveld T, Peters HF, Kuijpers-Jagtman AM. Language skills of young children with unilateral cleft lip and palate following infant orthopedics: a randomized clinical trial. Cleft Palate Craniofac J. 2003 Jul;40(4):356-62.

74
Krimmel M, Kluba S, Bacher M, Dietz K, Reinert S. Digital surface photogrammetry for anthropometric analysis of the cleft infant face. Cleft Palate Craniofac J. 2006 May;43(3):350-5.
Kuijpers-Jagtman AM, Nollet PJ, Semb G, Bronkhorst EM, Shaw WC, Katsaros C. Reference photographs for nasolabial appearance rating in unilateral cleft lip and palate. J Craniofac Surg. 2009 Sep;20 Suppl 2:1683-6.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977 Mar;33(1):159-74.
Latham RA. Orthopedic advancement of the cleft maxillary segment: a preliminary report. Cleft Palate J. 1980 Jul;17(3):227-33.
Lee CT, Grayson BH, Cutting CB, Brecht LE, Lin WY. Prepubertal midface growth in unilateral cleft lip and palate following alveolar molding and gingivoperiosteoplasty. Cleft Palate Craniofac J. 2004 Jul;41(4):375-80.
Lindsay WK, Farkas LG. The use of anthropometry in assessing the cleft-lip nose. Plast Reconstr Surg. 1972 Mar;49(3):286-93.
Liou EJ, Subramanian M, Chen PK, Huang CS. The progressive changes of nasal symmetry and growth after nasoalveolar molding: a three-year follow-up study. Plast Reconstr Surg. 2004 Sep 15;114(4):858-64.
Liu Q, Yang ML, Li ZJ, Bai XF, Wang XK, Lu L, et al. A simple and precise classification for cleft lip and palate: a five-digit numerical recording system. Cleft Palate Craniofac J. 2007 Sep;44(5):465-8.
Lo LJ. Primary correction of the unilateral cleft lip nasal deformity: achieving the excellence. Chang Gung Med J. 2006 May-Jun;29(3):262-7.
Long RE,Jr. The Americleft Project: Comparing Treatment Outcomes for Cleft Lip and Palate to Identify Evidence-Based Best Practices of Importance to the Orthodontist. 2011.
Long RE,Jr, Hathaway R, Daskalogiannakis J, Mercado A, Russell K, Cohen M, et al. The Americleft study: an inter-center study of treatment outcomes for patients with unilateral cleft lip and palate part 1. Principles and study design. Cleft Palate Craniofac J. 2011 May;48(3):239-43.
Lukash FN, Schwartz M, Grauer S, Tuminelli F. Dynamic cleft maxillary orthopedics and periosteoplasty: benefit or detriment? Ann Plast Surg. 1998 Apr;40(4): 326-7.
Mani MR, Semb G, Andlin-Sobocki A. Nasolabial appearance in adults with repaired unilateral cleft lip and palate: Relation between professional and lay rating and patients' satisfaction. J Plast Surg Hand Surg. 2010 Nov;44(4-5):191-8.

75
Mars M, Asher-McDade C, Brattström V, Dahl E, McWilliam J, Mølsted K, et al. A six-center international study of treatment outcome in patients with clefts of the lip and palate: Part 3. Dental arch relationships. Cleft Palate Craniofac J. 1992 Sep;29(5):405-8.
Masarei AG, Wade A, Mars M, Sommerlad BC, Sell D. A randomized control trial investigating the effect of presurgical orthopedics on feeding in infants with cleft lip and/or palate. Cleft Palate Craniofac J. 2007 Mar;44(2):182-93.
Maull DJ, Grayson BH, Cutting CB, Brecht LL, Bookstein FL, Khorrambadi D, et al. Long-term effects of nasoalveolar molding on three-dimensional nasal shape in unilateral clefts. Cleft Palate Craniofac J. 1999 Sep;36(5):391-7.
McNeil C. Orthodontic procedures in the treatment of congenital cleft palate. Dent Records. 1950;70:126-132.
Melnick M. Cleft lip and cleft palate. Etiology and pathogenesis. In: Kernahan DA, Rosenstein SW, Dado DV, editor. Cleft Lip and Palate. A System of Management. Baltimore: Williams & Wilkins.; 1990. p.3.
Mercado A, Russell K, Hathaway R, Daskalogiannakis J, Sadek H, Long RE,Jr, et al. The Americleft study: an inter-center study of treatment outcomes for patients with unilateral cleft lip and palate part 4. Nasolabial aesthetics. Cleft Palate Craniofac J. 2011 May;48(3):259-64.
Millard DJ. Cleft Craft: The Evolution of Its Surgery. Vol 1 ed. Boston: Little Brown; 1976.
Miyamoto J, Miyamoto S, Nagasao T, Nakajima T, Kishi K. Anthropometric evaluation of bilateral cleft lip nose with cone beam computed tomography in early childhood: Estimation of nasal tip collapse. J Plast Reconstr Aesthet Surg. 2012 Feb;65(2):169-74.
Mølsted K. Treatment outcome in cleft lip and palate: issues and perspectives. Crit Rev Oral Biol Med. 1999;10(2):225-39.
Mølsted K, Asher-McDade C, Brattström V, Dahl E, Mars M, McWilliam J, et al. A six-center international study of treatment outcome in patients with clefts of the lip and palate: Part 2. Craniofacial form and soft tissue profile. Cleft Palate Craniofac J. 1992 Sep;29(5):398-404.
Moore KL. The Developing Human. WB Saunders Co, editor. Philadelphia; 1982.
Morrant DG, Shaw WC. Use of standardized video recordings to assess cleft surgery outcome. Cleft Palate Craniofac J. 1996 Mar;33(2):134-42.
Nakamura N, Okawachi T, Nishihara K, Hirahara N, Nozoe E. Surgical technique for secondary correction of unilateral cleft lip-nose deformity: clinical and 3-dimensional

76
observations of preoperative and postoperative nasal forms. J Oral Maxillofac Surg. 2010 Sep;68(9):2248-57.
Pai BC, Ko EW, Huang CS, Liou EJ. Symmetry of the nose after presurgical nasoalveolar molding in infants with unilateral cleft lip and palate: a preliminary study. Cleft Palate Craniofac J. 2005 Nov;42(6):658-63.
Patzer G. The Physical Attractiveness Phenomena. New York: Plenum Press; 1984.
Pfeifer TM, Grayson BH, Cutting CB. Nasoalveolar molding and gingivoperiosteoplasty versus alveolar bone graft: an outcome analysis of costs in the treatment of unilateral cleft alveolus. Cleft Palate Craniofac J. 2002 Jan;39(1):26-9.
Pope AW, Tillman K, Snyder HT. Parenting stress in infancy and psychosocial adjustment in toddlerhood: a longitudinal study of children with craniofacial anomalies. Cleft Palate Craniofac J. 2005 Sep;42(5):556-9.
Power SM, Matic DB. Critical Analysis of Consecutive Unilateral Cleft Lip Repairs: Determining Ideal Sample Size. Cleft Palate Craniofac J. 2012 Mar 19 (Epub ahead of print).
Prahl C, Kuijpers-Jagtman AM, Van 't Hof MA, Prahl-Andersen B. Infant orthopedics in UCLP: effect on feeding, weight, and length: a randomized clinical trial (Dutchcleft). Cleft Palate Craniofac J. 2005 Mar;42(2):171-7.
Prahl C, Kuijpers-Jagtman AM, Van 't Hof MA, Prahl-Andersen B. A randomized prospective clinical trial of the effect of infant orthopedics in unilateral cleft lip and palate: prevention of collapse of the alveolar segments (Dutchcleft). Cleft Palate Craniofac J. 2003 Jul;40(4):337-42.
Prahl C, Kuijpers-Jagtman AM, van't Hof MA, Prahl-Andersen B. A randomised prospective clinical trial into the effect of infant orthopaedics on maxillary arch dimensions in unilateral cleft lip and palate (Dutchcleft). Eur J Oral Sci. 2001 Oct;109(5):297-305.
Prahl C, Prahl-Andersen B, van 't Hof MA, Kuijpers-Jagtman AM. Infant orthopedics and facial appearance: a randomized clinical trial (Dutchcleft). Cleft Palate Craniofac J. 2006 Nov;43(6):659-64.
Prahl C, Prahl-Andersen B, Van't Hof MA, Kuijpers-Jagtman AM. Presurgical orthopedics and satisfaction in motherhood: a randomized clinical trial (Dutchcleft). Cleft Palate Craniofac J. 2008 May;45(3):284-8.
Prahl-Andersen B. Dental treatment of predental and infant patients with clefts and craniofacial anomalies. Cleft Palate Craniofac J. 2000 Nov;37(6):528-32.
Randall P. A triangular flap operation for the primary repair of unilateral clefts of the lip. Plastic and reconstructive surgery.1959; 23:331-347.

77
Ras F, Habets LL, van Ginkel FC, Prahl-Andersen B. Three-dimensional evaluation of facial asymmetry in cleft lip and palate. Cleft Palate Craniofac J. 1994 Mar;31(2):116-21.
Rivkin CJ, Keith O, Crawford PJ, Hathorn IS. Dental care for the patient with a cleft lip and palate. Part 2: The mixed dentition stage through to adolescence and young adulthood. Br Dent J. 2000 Feb 12;188(3):131-4.
Roberts-Harry D, Stephens CD. Panel perception of facial attractiveness. Br J Orthod. 1991 May;18(2):152-3.
Rodd HD, Clark EL, Stern MR, Baker SR. Failed attendances at hospital dental clinics among young patients with cleft lip and palate. Cleft Palate Craniofac J. 2007 Jan;44(1):92-4.
Ross R. Midfacial and mandibular dysmorphology and growth in facial clefting: clinical implications. In: Mooney M SM, editor. Understanding craniofacial anomalies: the etiopathogenesis of craniosynostoses and facial clefting. Toronto: Wiley-Liss Inc.
Ross R, Johnston M. Cleft Lip and Palate. Baltimore: Williams and Wilkins; 1972.
Ross RB. Treatment variables affecting facial growth in complete unilateral cleft lip and palate. Cleft Palate J. 1987 Jan;24(1):5-77.
Ross RB, MacNamera MC. Effect of presurgical infant orthopedics on facial esthetics in complete bilateral cleft lip and palate. Cleft Palate Craniofac J. 1994 Jan;31(1):68-73.
Russell K, Long RE,Jr, Hathaway R, Daskalogiannakis J, Mercado A, Cohen M, et al. The Americleft study: an inter-center study of treatment outcomes for patients with unilateral cleft lip and palate part 5. General discussion and conclusions. Cleft Palate Craniofac J. 2011 May;48(3):265-70.
Russell KA, Waldman SD, Lee JM. Video-imaging assessment of nasal morphology in individuals with complete unilateral cleft lip and palate. Cleft Palate Craniofac J. 2000 Nov;37(6):542-50.
Russell KA, Waldman SD, Tompson B, Lee JM. Nasal morphology and shape parameters as predictors of nasal esthetics in individuals with complete unilateral cleft lip and palate. Cleft Palate Craniofac J. 2001 Sep;38(5):476-85.
Sander M, Daskalogiannakis J, Tompson B, Forrest C. Effect of alveolar bone grafting on nasal morphology, symmetry, and nostril shape of patients with unilateral cleft lip and palate. Cleft Palate Craniofac J. 2011 Jan;48(1):20-7.
Schabel BJ, McNamara JA,Jr, Franchi L, Baccetti T. Q-sort assessment vs visual analog scale in the evaluation of smile esthetics. Am J Orthod Dentofacial Orthop. 2009 Apr;135(4 Suppl):S61-71.

78
Semb G, Brattström V, Mølsted K, Prahl-Andersen B, Shaw WC. The Eurocleft study: intercenter study of treatment outcome in patients with complete cleft lip and palate. Part 1: introduction and treatment experience. Cleft Palate Craniofac J. 2005 Jan;42(1):64-8.
Semb G, Shaw WC. Facial growth after different methods of surgical intervention in patients with cleft lip and palate. Acta Odontol Scand. 1998 Dec;56(6):352-5.
Severens JL, Prahl C, Kuijpers-Jagtman AM, Prahl-Andersen B. Short-term cost-effectiveness analysis of presurgical orthopedic treatment in children with complete unilateral cleft lip and palate. Cleft Palate Craniofac J. 1998 May;35(3):222-6.
Shaw WC, Asher-McDade C, Brattström V, Dahl E, McWilliam J, Mølsted K, et al. A six-center international study of treatment outcome in patients with clefts of the lip and palate: Part 1. Principles and study design. Cleft Palate Craniofac J. 1992 Sep;29(5):393-7.
Shaw WC, Dahl E, Asher-McDade C, Brattström V, Mars M, McWilliam J, et al. A six-center international study of treatment outcome in patients with clefts of the lip and palate: Part 5. General discussion and conclusions. Cleft Palate Craniofac J. 1992 Sep;29(5):413-8.
Shaw WC, Semb G, Nelson P, Brattström V, Mølsted K, Prahl-Andersen B, et al. The Eurocleft project 1996-2000: overview. J Craniomaxillofac Surg. 2001 Jun;29(3):131,40; discussion 141-2.
Shetye PR. Presurgical infant orthopedics. J Craniofac Surg. 2012 Jan;23(1):210-1.
Singh GD, Levy-Bercowski D, Santiago PE. Three-dimensional nasal changes following nasoalveolar molding in patients with unilateral cleft lip and palate: geometric morphometrics. Cleft Palate Craniofac J. 2005 Jul;42(4):403-9.
Sischo L, Chan JW, Stein M, Smith C, van Aalst JA, Broder HL. Nasoalveolar Molding: Prevalence of Cleft Centers Offering NAM and Who Seeks It. Cleft Palate Craniofac J. 2011 Jul 8 (Epub).
Skyes J. Management of the cleft lip deformity. Facial Plastic Surgery Clinics of North America. 2001;9(1):37-50.
Smith K. University of Oklahoma College of Dentistry Cleft Craniofacial Fellowship. http://dentistry.ouhsc.edu/os_cleft-craniofacial.php.; 2012(04/11).
Snowden CB, Miller TR, Jensen AF, Lawrence BA. Costs of medically treated craniofacial conditions. Public Health Rep. 2003 Jan-Feb;118(1):10-7.
Stephenson W. The study of behaviour. Chicago: University of Chicago Press. 1953.

79
Suri S, Tompson BD. A modified muscle-activated maxillary orthopedic appliance for presurgical nasoalveolar molding in infants with unilateral cleft lip and palate. Cleft Palate Craniofac J. 2004 May;41(3):225-9.
Ten Cate A. Oral Histology: Development, Structure and Function. 5th ed. St. Louis: Mosby-Year Book, Inc; 1998.
Tennison CW. The repair of the unilateral cleft lip by the stencil method. Plast Reconstr Surg (1946). 1952 Feb;9(2):115-20.
Thomas C. Primary rhinoplasty by open approach with repair of unilateral complete cleft lip. J Craniofac Surg. 2009 Sep;20 Suppl 2:1711-4.
Tobiasen JM. Social judgments of facial deformity. Cleft Palate J. 1987 Oct;24(4):323-7.
Tobiasen JM, Hiebert JM. Reliability of esthetic ratings of cleft impairment. Cleft Palate J. 1988 Jul;25(3):313-7.
Tobiasen JM, Hiebert JM, Boraz RA. Development of scales of severity of facial cleft impairment. Cleft Palate Craniofac J. 1991 Oct;28(4):419-24.
Uzel A, Alparslan ZN. Long-term effects of presurgical infant orthopedics in patients with cleft lip and palate: a systematic review. Cleft Palate Craniofac J. 2011 Sep;48(5):587-95.
Vegter F, Hage JJ. Facial anthropometry in cleft patients: a historical appraisal. Cleft Palate Craniofac J. 2001 Nov;38(6):577-81.
Wehby GL, Cassell CH. The impact of orofacial clefts on quality of life and healthcare use and costs. Oral Dis. 2010 Jan;16(1):3-10.
Williams AC, Bearn D, Mildinhall S, Murphy T, Sell D, Shaw WC, et al. Cleft lip and palate care in the United Kingdom--the Clinical Standards Advisory Group (CSAG) Study. Part 2: dentofacial outcomes and patient satisfaction. Cleft Palate Craniofac J. 2001 Jan;38(1):24-9.
Winters JC, Hurwitz DJ. Presurgical orthopedics in the surgical management of unilateral cleft lip and palate. Plast Reconstr Surg. 1995 Apr;95(4):755-64.
Wong K, Wu L. History of Chinese Medicine. Tientsin: Tientsin Press; 1932.
Wood RJ, Grayson BH, Cutting CB. Gingivoperiosteoplasty and midfacial growth. Cleft Palate Craniofac J. 1997 Jan;34(1):17-20.
World Health Organization. Global strategies to reduce the health care burden of craniofacial anomalies: report of WHO meetings on international collaborative research on craniofacial anomalies. Cleft Palate Craniofac J. 2004 May;41(3):238-43.

80
Wright JG, Menaker RJ, Canadian Paediatric Surgical Wait Times Study Group. Waiting for children's surgery in Canada: the Canadian Paediatric Surgical Wait Times project. CMAJ. 2011 Jun 14;183(9):E559-64.
Wyszynski D. Cleft Lip and Palate: From Origin to Treatment. New York: Oxford University Press; 2002.

81
Appendix 1: Abbreviations/Acronyms
ACPA: American Cleft Palate Craniofacial Association
BCLP: Bilateral Cleft Lip and Palate
CA: Coefficient of Asymmetry
CCT: Controlled Clinical Trial
CDC: Centre for Disease Control
CLP: Cleft Lip and Palate
CSAG: Clinical Standards Advisory Group
CT: Computed Tomography
CUCLP: Complete Unilateral Cleft Lip and Palate
DMA: Dentomaxillary Alignment Appliance
GPP: Gingivoperiosteoplasty
IO: Infant Orthopedics
JPEG: Joint Photographic Experts Group
NAM: Nasoalveolar Molding
PSIO: Presurgical Infant Orthopedics
RCT: Randomized Controlled Trial
TIO: Traditional Infant Orthopedics
UCLP: Unilateral Cleft Lip and Palate
US: United States
USB: Universal Serial Bus Drive
WHO: World Health Organization

82
Appendix 2: Sample Demographics & BOC Data
Centre 1
Research Number
Sex Cleft Side Surgeon Code Age at Photo (yrs)
Non Cleft Side Photos
1 F L 2 4.82 Y 2 F L 3 5.01 3 M R 2 4.45 4 F R 3 5.09 Y 5 M L 3 5.1 6 M L 2 5.03 8 F R 2 6.01 Y 9 F L 2 4.39 Y
10 M L 2 5.05 11 F L 2 6.01 12 M R 2 6.07 13 M L 3 6.03 14 M L 2 4.92 Y 15 M L 2 6.03 17 F L 2 6.83 18 F R 2 6.23 19 M L 2 6.18 Y 20 F L 2 6.22 21 F L 3 5.26 23 F L 3 6.01 Y 24 M L 2 6.01 25 M L 2 6.04 Y 26 M L 2 4.76 27 M R 2 5.87 Y 28 M R 3 6.01 29 F L 2 6.05 30 M L 2 4.01 31 M L 4 6.08 32 M R 6 6.2 33 M L 2 5.66 34 F R 6 5.99 35 M L 6 6.33 36 M L 2 6.05 37 F L 2 6.06 38 F L 2 6.06 39 M L 2 6.02 40 M L 3 6.15 41 F L 6 5.96 43 M L 6 5.99 44 F R 6 6.02

83
Centre 2
Research Number
Sex Cleft Side Surgeon Code
Age at Photo (yrs)
Non Cleft Side Photos
1-1-1 M R 1 5.02
1-1-2 M R 1 5.00
1-1-4 F L 1 5.01 Y
1-1-5 F L 1 5.01 Y
1-1-6 M L 1 5.00 Y
1-1-8 M R 1 5.02 Y
1-1-10 F L 1 4.96 Y
1-1-12 M L 1 4.97 Y
1-1-13 F R 1 5.01
1-1-14 M L 1 5.29 Y
1-1-16 F L 1 4.99 Y
1-1-19 F R 1 5.13
1-1-21 F R 1 4.98
1-1-23 M L 1 5.00 Y
1-1-24 M L 1 4.99
1-1-27 M L 1 5.00 Y
1-1-28 M L 1 5.01 Y
1-1-29 F R 1 5.01
1-1-31 F R 1 5.00
1-1-33 M L 1 5.97 Y
1-1-34 M R 1 5.98
1-1-35 M L 1 5.01 Y
1-1-36 F L 1 5.00 Y
1-1-38 F L 1 5.00 Y
1-1-40 M R 1 5.01
1-1-41 M R 1 5.05
1-1-42 F L 1 5.01 Y
1-1-44 M R 1 5.02
1-1-45 M R 1 5.91
1-1-46 F R 1 5.02
1-1-47 F R 1 5.01
1-1-48 M L 1 5.07 Y
1-1-50 M L 1 5.01 Y
1-1-51 F L 1 4.95 Y
1-1-52 M L 1 4.98 Y
1-1-53 M R 1 6.01
1-1-54 M L 1 4.97 Y
1-1-56 M L 1 5.01 Y

84
Centre 3 (TIO)
Research Number
Sex Side of cleft
Appliance Insertion
Date
# of Scheduled
Visits
# of Emerg Visits
Total Visits
Age at Photo (yrs)
Ortho Code
Surgeon Code
Date of Lip
Repair
U1 M L Jan 12/99 4 0 4 6.12 1 1 Apr 12/99
U3 F R June 5/00 4 0 4 6.01 2 2 Oct 4/00
U4 M L July 31/00 5 0 5 4.91 3 2 Jan 24/01
U5 M L Aug 20/99 6 0 6 6.42 4 2 Dec 8/99
U6 M R Apr 8/99 6 0 6 5.97 4 1 Sep 27/99
U8 F L Feb 1/01 7 0 7 6.78 3 2 Aug 17/01
U9 M L Mar 30/99 8 0 8 5.89 5 1 Nov 22/99
U10 F R March 18/99
7 0 7 5.79 5 2 Jun 21/99
U11 F L Jan 17/00 6 1 7 5.12 2 3 May 10/00
U12 M R Feb 29/00 6 0 6 5.36 2 3 May 17/00
U13 F L Aug 1/00 9 0 9 4.6 3 2 Dec 5/00
U15 M L Sep 25/97 7 0 7 5.45 6 3 Jan 7/98
U16 F L Jan 8/98 6 0 6 4.96 6 3 Mar 20/98
U17 M L Dec 4/97 8 0 8 6.05 4 2 Apr 1/98
U19 F L Dec 18/97 7 0 7 5.26 6 1 Mar 23/98
U21 F L Aug 13/97 5 0 5 5.11 6 2 Nov 18/97
U22 M R Jan 8/98 6 0 6 5.52 6 4 Mar 27/98
U23 F L June8/98 6 1 7 4.77 6 4 Sep 23/98
U26 F R Oct 29/98 5 0 5 5.61 5 2 Mar 3/99
U28 M L Apr 6/00 7 0 7 6.06 2 3 June 21/00
U30 F L May 6/98 6 0 6 6.88 7 4 Aug 5/98
U32 F L Sept 25/97 6 2 8 5.05 5 5 Dec 10/97
U33 M R Sept 2/97 6 0 6 6.19 5 1 Mar 9/08
U38 F L Feb 24/97 6 1 7 5.21 8 1 May

85
14/97
U40 F L July 10/96 6 0 6 5.97 4 2 Oct 2/96
U43 M L Apr 9/96 7 0 7 6.58 9 1 Jul 22/96
U44 M L Feb 26/96 7 1 8 5.74 4 2 Jun 5/96
U45 M L Dec 22/95 7 1 8 5.94 9 1 Apr 22/96
U46 M R Sep 7/95 7 0 7 6.83 9 1 Feb 26/96
U47 M R Sep 5/95 7 0 7 5.53 9 1 Jan 8/96
U48 M L Sep 7/95 9 0 9 5.54 9 1 Jan 29/96
U51 M R Mar 27/97 7 0 7 5.06 4 2 Aug 11/97
U54 F L Oct 2/96 7 0 7 5.32 4 2 Jan 22/97
U56 M R May 6/96 8 1 9 5.51 9 1 Sep 23/96
U58 M R Jan 16/96 9 1 10 5.63 9 1 Jun 24/96
U59 M L Feb 21/95 7 0 7 6.13 9 1 July 26/95
U60 M L Jan 26/94 6 0 6 5.05 10 1 May 16/94
U61 M L Jan 11/95 4 0 4 5.55 10 1 Mar 27/95

86
Centre 4 (NAM)
Research Number
Sex Side of
Cleft
Appliance Insertion
Date
# of Scheduled
Visits
# of Emerg Visits
Total Visits
Age at Photo (yrs)
Ortho Code
Surgeon Code
Date of Lip Repair
U1 M L July 9/02 9 0 9 5.5 1 1 Oct 31/02
U2 M L Dec 19/02 7 0 7 5.99 2 2 Apr 23/03
U4 M R Apr 15/04 11 0 11 5.52 2 2 Sep 29/04
U7 M R Jan 14/03 5 0 5 6.95 3 3 May 2/03
U8 F R Jan 30/03 8 0 8 5.39 2 2 May 7/03
U11 M R July 15/02 10 1 11 5.44 1 1 Nov 11/02
U12 M L Mar 28/02 15 1 16 6.24 3 2 Aug 2/02
U14 M R Apr 16/03 7 0 7 5.97 3 2 Aug 14/03
U18 M L Aug 15/02 8 0 8 6.15 1 2 Nov 27/02
U19 M L Sept 22/05 11 1 12 4.96 4 1 March 13/06
U20 M R Dec 9/04 13 0 13 5.17 5 2 June 22/05
U21 M R Sept 5/02 9 0 9 6.1 1 2 Jan 15/03
U22 M L Apr 16/03 5 0 5 5.31 3 2 July 18/03
U23 F L Apr 1/02 9 0 9 6.54 2 2 July 23/02
U24 M R Sept 18/03 10 0 10 5.24 2 2 Feb 18/04
U25 F L July 14/04 12 0 12 5.67 3 1 Nov 22/04
U26 M L Sept 19/02 8 0 8 5.56 2 2 Jan 8/03
U27 F L Nov 17/04 14 0 14 5.27 3 2 Apr 6/05
U28 F R Mar 17/03 10 0 10 6.27 6 2 Aug 14/03
U29 M R Nov 20/02 8 0 8 5.45 3 2 Feb 26/03
U31 M L Aug 21/03 11 0 11 6.73 2 2 Dec 3/03
U32 M L Dec 23/03 15 0 15 4.38 2 2 June 18/04
U34 M L Apr 8/04 9 0 9 5.59 2 2 Sep 15/04
U35 M L Jan 22/04 9 0 9 5.28 2 2 Jun 2/04
U37 M R Mar 4/03 10 0 10 5.43 6 2 July 16/03
U38 M L Dec 11/02 14 0 14 5.18 3 2 Mar 7/03
U39 M L Jan 30/01 10 0 10 6.09 7 1 May 14/01
U41 M R May 24/01 12 0 12 5.57 2 2 Oct 19/01
U43 F L Apr 12/01 11 0 11 5.45 7 2 Aug 16/01
U47 F L Apr 19/01 8 0 8 5.3 7 1 Aug 3/01
U50 M L Mar7/01 8 0 8 6.3 3 2 May 25/01

87
U51 F L Nov 2/00 10 0 10 5.4 7 2 Feb 14/01
U53 M L Sept 20/01 9 0 9 6.5 2 2 Jan 15/02

88
Appendix 3: Statistical Analysis - Weighted Kappa
Scores
Vermilion Border Rating 1- 7 raters
GS RH AM RL AS JD KR Overall
GS 0.855 0.67 0.658 0.694 0.593 0.596 0.688 RH 0.67 0.807 0.607 0.676 0.595 0.555 0.712 AM 0.658 0.607 0.761 0.61 0.513 0.522 0.602 RL 0.694 0.676 0.61 0.815 0.695 0.577 0.649 AS 0.593 0.595 0.513 0.695 0.839 0.488 0.642 JD 0.596 0.555 0.522 0.577 0.488 0.716 0.57 KR 0.688 0.712 0.602 0.649 0.642 0.57 0.704
0.650 0.636 0.585 0.650 0.591 0.551 0.644 0.615
0.785
Vermilion Border Rating 2- 7 raters
GS RH AM RL AS JD KR Overall
GS 0.855 0.665 0.7 0.714 0.654 0.627 0.653 RH 0.665 0.807 0.685 0.712 0.554 0.663 0.642 AM 0.7 0.685 0.761 0.644 0.585 0.658 0.638 RL 0.714 0.712 0.644 0.815 0.711 0.682 0.646 AS 0.654 0.554 0.585 0.711 0.839 0.588 0.574 JD 0.627 0.663 0.658 0.682 0.588 0.716 0.531 KR 0.653 0.642 0.638 0.646 0.574 0.531 0.704
0.669 0.654 0.652 0.685 0.611 0.625 0.614 0.644
0.785

89
Nasolabial Frontal Rating 1 – 7 raters
GS RH AM RL AS JD KR Overall
GS 0.901 0.527 0.489 0.617 0.545 0.452 0.52 RH 0.527 0.694 0.553 0.672 0.62 0.435 0.618 AM 0.489 0.553 0.621 0.545 0.446 0.43 0.59 RL 0.617 0.672 0.545 0.77 0.65 0.482 0.62
AS 0.545 0.62 0.446 0.65 0.849 0.484 0.642 JD 0.452 0.435 0.43 0.482 0.484 0.654 0.446 KR 0.52 0.618 0.59 0.62 0.642 0.446 0.718 AVG 0.525 0.571 0.509 0.598 0.565 0.455 0.573 0.542
0.744
Nasolabial Frontal Rating 2 – 7
raters
GS RH AM RL AS JD KR Overall
GS 0.901 0.514 0.552 0.685 0.545 0.452 0.52 RH 0.514 0.694 0.486 0.551 0.616 0.496 0.564 AM 0.552 0.486 0.621 0.528 0.338 0.532 0.596 RL 0.685 0.551 0.528 0.77 0.681 0.601 0.651 AS 0.545 0.616 0.338 0.681 0.849 0.591 0.623 JD 0.452 0.496 0.532 0.601 0.591 0.654 0.54 KR 0.52 0.564 0.596 0.651 0.623 0.54 0.718 AVG 0.545 0.538 0.505 0.616 0.566 0.535 0.582 0.555
0.744

90
Nasolabial Profile Rating 1 - 7 Raters
GS RH AM RL AS JD KR Overall
GS 0.817 0.424 0.604 0.673 0.514 0.453 0.594 RH 0.424 0.609 0.487 0.383 0.412 0.271 0.465 AM 0.604 0.487 0.675 0.566 0.523 0.347 0.604 RL 0.673 0.383 0.566 0.812 0.649 0.572 0.683 AS 0.514 0.412 0.523 0.649 0.822 0.604 0.716 JD 0.453 0.271 0.347 0.572 0.604 0.674 0.534 KR 0.594 0.465 0.604 0.683 0.716 0.534 0.569 AVG 0.544 0.407 0.522 0.588 0.570 0.464 0.599 0.528
0.711
Nasolabial Profile Rating 2 - 7 raters
GS RH AM RL AS JD KR Overall
GS 0.817 0.445 0.52 0.637 0.487 0.38 0.485 RH 0.445 0.609 0.418 0.275 0.434 0.356 0.411 AM 0.52 0.418 0.675 0.564 0.58 0.421 0.514 RL 0.637 0.394 0.564 0.812 0.654 0.653 0.643 AS 0.487 0.434 0.58 0.4 0.822 0.672 0.596 JD 0.38 0.356 0.421 0.653 0.672 0.674 0.56 KR 0.485 0.411 0.514 0.643 0.596 0.56 0.569 AVG 0.492 0.410 0.503 0.529 0.571 0.507 0.535 0.507
0.711

91
Appendix 4: Statistical Analysis – Kruskal-Wallis and
Chi-square Tests
KRUSKAL-WALLIS ANALYSIS
VERMILION BORDER
————— 12/29/2011 10:55:05 AM ————————————————————
Welcome to Minitab, press F1 for help.
————— 1/9/2012 10:54:17 AM ————————————————————
Welcome to Minitab, press F1 for help.
Retrieving project from file: 'E:\EMILY\AMERICLEFT OSU\MINITAB VB.MPJExecuting from
file: H:\Latest Macros\macros\KrusMC.Mac
Macro is running ... please wait
Kruskal-Wallis: Multiple Comparisons
Kruskal-Wallis Test on the data
Group N Median Ave Rank Z
Ctr 1 40 3.393 94.9 3.42
Ctr 2 38 3.071 80.4 0.89

92
Ctr 3 38 2.786 66.0 -1.49
Ctr 4 33 2.357 55.0 -3.02
Overall 149 75.0
H = 17.85 DF = 3 P = 0.000
H = 17.87 DF = 3 P = 0.000 (adjusted for ties)
Kruskal-Wallis: All Pairwise Comparisons
----------------------------------------
Comparisons: 6
Ties: 101
Family Alpha: 0.05
Bonferroni Individual Alpha: 0.008
Bonferroni Z-value (2-sided): 2.638
----------------------------------------
Standardized Absolute Mean Rank Differences
|Rbar(i)-Rbar(j)| / Stdev
Rows: Group i = 1,...,n
Columns: Group j = 1,...,n
1. Table of Z-values
Ctr 1 0.00000 * * *
Ctr 2 1.49159 0.00000 * *

93
Ctr 3 2.95728 1.44725 0.00000 *
Ctr 4 3.93512 2.46911 1.07375 0
----------------------------------------------------------
Adjusted for Ties in the Data
1. Table of Z-values
Ctr 1 0.00000 * * *
Ctr 2 1.49236 0.00000 * *
Ctr 3 2.95881 1.44800 0.00000 *
Ctr 4 3.93715 2.47038 1.07430 0
2. Table of P-values
Ctr 1 1.00000 * * *
Ctr 2 0.13560 1.00000 * *
Ctr 3 0.00309 0.14762 1.00000 *
Ctr 4 0.00008 0.01350 0.28269 1
----------------------------------------------------------
Sign Confidence Intervals controlled at a family error rate of 0.05
Desired Confidence: 93.789

94
Sign confidence interval for median
Confidence
Achieved Interval
N Median Confidence Lower Upper Position
Ctr 1 40 3.393 0.9193 3.000 3.714 15
0.9379 2.958 3.757 NLI
0.9615 2.857 3.857 14
Ctr 2 38 3.071 0.9270 2.643 3.500 14
0.9379 2.631 3.500 NLI
0.9664 2.571 3.500 13
Ctr 3 38 2.786 0.9270 2.429 3.000 14
0.9379 2.405 3.012 NLI
0.9664 2.286 3.071 13
Ctr 4 33 2.357 0.9199 2.071 2.643 12
0.9379 2.054 2.696 NLI
0.9649 2.000 2.857 11
Kruskal-Wallis: Conclusions
The following groups showed significant differences (adjusted for ties):
Groups Z vs. Critical value P-value
Ctr 1 vs. Ctr 4 3.93715 >= 2.638 0.0001
Ctr 1 vs. Ctr 3 2.95881 >= 2.638 0.0031

95
NASOLABIAL FRONTAL
————— 1/9/2012 11:00:40 AM ————————————————————
Welcome to Minitab, press F1 for help.
Executing from file: H:\Latest Macros\macros\KrusMC.Mac
Macro is running ... please wait
Kruskal-Wallis: Multiple Comparisons
Kruskal-Wallis Test on the data
Group N Median Ave Rank Z
Ctr 1 40 2.929 64.8 -1.74
Ctr 2 38 3.357 97.5 3.72
Ctr 3 38 2.821 63.1 -1.97
Ctr 4 33 3.000 75.1 0.02
Overall 149 75.0
H = 15.39 DF = 3 P = 0.002
H = 15.41 DF = 3 P = 0.002 (adjusted for ties)
Kruskal-Wallis: All Pairwise Comparisons
----------------------------------------

96
Comparisons: 6
Ties: 103
Family Alpha: 0.05
Bonferroni Individual Alpha: 0.008
Bonferroni Z-value (2-sided): 2.638
----------------------------------------
Standardized Absolute Mean Rank Differences
|Rbar(i)-Rbar(j)| / Stdev
Rows: Group i = 1,...,n
Columns: Group j = 1,...,n
1. Table of Z-values
Ctr 1 0.00000 * * *
Ctr 2 3.33568 0.00000 * *
Ctr 3 0.17712 3.46861 0.00000 *
Ctr 4 1.01204 2.17541 1.16884 0
----------------------------------------------------------
Adjusted for Ties in the Data
1. Table of Z-values
Ctr 1 0.00000 * * *

97
Ctr 2 3.33780 0.00000 * *
Ctr 3 0.17723 3.47082 0.00000 *
Ctr 4 1.01269 2.17680 1.16958 0
2. Table of P-values
Ctr 1 1.00000 * * *
Ctr 2 0.00084 1.00000 * *
Ctr 3 0.85933 0.00052 1.00000 *
Ctr 4 0.31121 0.02950 0.24217 1
----------------------------------------------------------
Sign Confidence Intervals controlled at a family error rate of 0.05
Desired Confidence: 93.789
Sign confidence interval for median
Confidence
Achieved Interval
N Median Confidence Lower Upper Position
Ctr 1 40 2.929 0.9193 2.714 3.000 15
0.9379 2.693 3.021 NLI
0.9615 2.643 3.071 14
Ctr 2 38 3.357 0.9270 3.214 3.786 14

98
0.9379 3.191 3.797 NLI
0.9664 3.071 3.857 13
Ctr 3 38 2.821 0.9270 2.571 3.286 14
0.9379 2.560 3.286 NLI
0.9664 2.500 3.286 13
Ctr 4 33 3.000 0.9199 2.714 3.286 12
0.9379 2.714 3.304 NLI
0.9649 2.714 3.357 11
Kruskal-Wallis: Conclusions
The following groups showed significant differences (adjusted for ties):
Groups Z vs. Critical value P-value
Ctr 2 vs. Ctr 3 3.47082 >= 2.638 0.0005
Ctr 1 vs. Ctr 2 3.33780 >= 2.638 0.0008

99
NASOLABIAL PROFILE
————— 1/9/2012 11:07:28 AM ————————————————————
Kruskal-Wallis: Multiple Comparisons
Kruskal-Wallis Test on the data
Group N Median Ave Rank Z
Ctr 1 31 2.714 52.4 -1.35
Ctr 2 16 2.821 61.4 0.24
Ctr 3 38 2.857 55.8 -0.81
Ctr 4 33 3.071 69.5 1.98
Overall 118 59.5
H = 4.67 DF = 3 P = 0.198
H = 4.68 DF = 3 P = 0.197 (adjusted for ties)
Kruskal-Wallis: All Pairwise Comparisons
----------------------------------------
Comparisons: 6
Ties: 74
Family Alpha: 0.05
Bonferroni Individual Alpha: 0.008
Bonferroni Z-value (2-sided): 2.638

100
----------------------------------------
Standardized Absolute Mean Rank Differences
|Rbar(i)-Rbar(j)| / Stdev
Rows: Group i = 1,...,n
Columns: Group j = 1,...,n
1. Table of Z-values
Ctr 1 0.00000 * * *
Ctr 2 0.86101 0.000000 * *
Ctr 3 0.41450 0.552732 0.00000 *
Ctr 4 2.00374 0.775140 1.68466 0
----------------------------------------------------------
Adjusted for Ties in the Data
1. Table of Z-values
Ctr 1 0.00000 * * *
Ctr 2 0.86161 0.000000 * *
Ctr 3 0.41479 0.553117 0.00000 *
Ctr 4 2.00513 0.775680 1.68584 0
2. Table of P-values

101
Ctr 1 1.00000 * * *
Ctr 2 0.38890 1.00000 * *
Ctr 3 0.67829 0.58018 1.00000 *
Ctr 4 0.04495 0.43794 0.09183 1
----------------------------------------------------------
Sign Confidence Intervals controlled at a family error rate of 0.05
Desired Confidence: 93.789
Sign confidence interval for median
Confidence
Achieved Interval
N Median Confidence Lower Upper Position
Ctr 1 31 2.714 0.9292 2.500 3.071 11
0.9379 2.492 3.071 NLI
0.9706 2.429 3.071 10
Ctr 2 16 2.821 0.9232 2.357 4.143 5
0.9379 2.319 4.158 NLI
0.9787 2.000 4.286 4
Ctr 3 38 2.857 0.9270 2.500 3.143 14
0.9379 2.500 3.143 NLI
0.9664 2.500 3.143 13
Ctr 4 33 3.071 0.9199 2.786 3.500 12

102
0.9379 2.786 3.518 NLI
0.9649 2.786 3.571 11
Kruskal-Wallis: Conclusions
There were no significant group differences (adjusted for ties).

103
CUMULATIVE SCORES
————— 4/6/2012 2:46:17 PM ————————————————————
Welcome to Minitab, press F1 for helpExecuting from file: H:\Latest
Macros\macros\KrusMC.Mac
Macro is running ... please wait
Kruskal-Wallis: Multiple Comparisons
Kruskal-Wallis Test on the data
Group N Median Ave Rank Z
Ctr 1 111 3.000 213.7 0.53
Ctr 2 92 3.214 241.1 2.95
Ctr 3 114 2.821 184.0 -2.55
Ctr 4 99 2.857 200.5 -0.76
Overall 416 208.5
H = 12.13 DF = 3 P = 0.007
H = 12.14 DF = 3 P = 0.007 (adjusted for ties)
Kruskal-Wallis: All Pairwise Comparisons
----------------------------------------
Comparisons: 6
Ties: 361

104
Family Alpha: 0.05
Bonferroni Individual Alpha: 0.008
Bonferroni Z-value (2-sided): 2.638
----------------------------------------
Standardized Absolute Mean Rank Differences
|Rbar(i)-Rbar(j)| / Stdev
Rows: Group i = 1,...,n
Columns: Group j = 1,...,n
1. Table of Z-values
Ctr 1 0.00000 * * *
Ctr 2 1.61670 0.00000 * *
Ctr 3 1.84992 3.38655 0.000000 *
Ctr 4 0.79282 2.33088 0.997815 0
----------------------------------------------------------
Adjusted for Ties in the Data
1. Table of Z-values
Ctr 1 0.00000 * * *
Ctr 2 1.61733 0.00000 * *
Ctr 3 1.85064 3.38787 0.000000 *
Ctr 4 0.79313 2.33179 0.998205 0

105
2. Table of P-values
Ctr 1 1.00000 * * *
Ctr 2 0.10581 1.00000 * *
Ctr 3 0.06422 0.00070 1.00000 *
Ctr 4 0.42770 0.01971 0.31818 1
----------------------------------------------------------
Sign Confidence Intervals controlled at a family error rate of 0.05
Desired Confidence: 93.789
Sign confidence interval for median
Confidence
Achieved Interval
N Median Confidence Lower Upper Position
Ctr 1 111 3.000 0.9125 2.857 3.071 47
0.9379 2.857 3.129 NLI
0.9423 2.857 3.143 46
Ctr 2 92 3.214 0.9237 3.000 3.357 38
0.9379 3.000 3.386 NLI
0.9524 3.000 3.429 37
Ctr 3 114 2.821 0.9248 2.643 2.929 48

106
0.9379 2.613 2.958 NLI
0.9508 2.571 3.000 47
Ctr 4 99 2.857 0.9296 2.643 3.071 41
0.9379 2.643 3.071 NLI
0.9556 2.643 3.071 40
Kruskal-Wallis: Conclusions
The following groups showed significant differences (adjusted for ties):
Groups Z vs. Critical value P-value
Ctr 2 vs. Ctr 3 3.38787 >= 2.638 0.0007

107
CHI SQUARE ANALYSIS
————— 1/6/2012 4:41:02 PM ————————————————————
Welcome to Minitab, press F1 for help.
Tabulated statistics: Center, Rating
Using frequencies in Responses
Rows: Center Columns: Rating
1 2 3 4 5 All
CTR 1 44 99 205 62 24 434
10.14 22.81 47.24 14.29 5.53 100.00
CTR 2 23 58 59 42 42 224
10.27 25.89 26.34 18.75 18.75 100.00
CTR 3 56 133 204 115 24 532
10.53 25.00 38.35 21.62 4.51 100.00
CTR 4 17 93 183 134 33 460
3.70 20.22 39.78 29.13 7.17 100.00
All 140 383 651 353 123 1650
8.48 23.21 39.45 21.39 7.45 100.00

108
Cell Contents: Count
% of Row
Pearson Chi-Square = 107.711, DF = 12, P-Value = 0.000
Likelihood Ratio Chi-Square = 101.567, DF = 12, P-Value = 0.000
————— 1/11/2012 11:55:36 AM ————————————————————
Welcome to Minitab, press F1 for help.
Retrieving project from file: 'R:\RESEARCH PROJECTS\CLEFT PALATE
CLINIC\CENTER SCORES.MPJ'
Descriptive Statistics: Responses
Variable Center Sum
Responses CTR 1 434.0
CTR 2 224.00
CTR 3 532.0
CTR 4 460.0
Executing from file: C:\Documents and Settings\mahorst\My
Documents\macros\MULTPROP.MAC
Results for: Worksheet 2

109
Multiple Comparisons for Proportions
Ho: There is not a significant difference between Proportions
H1: There is a significant difference between Proportions
Row Compare Diff SE q q(.05) Conclusion
1 CTR 1 Rating 3 vs CTR 4 Rating 1 32.1846 1.35481 23.7558 5.01 Significant
Difference
2 CTR 1 Rating 3 vs CTR 3 Rating 5 31.0391 1.30959 23.7013 5.01 Significant
Difference
3 CTR 1 Rating 3 vs CTR 1 Rating 5 29.6908 1.37435 21.6035 5.01 Significant
Difference
4 CTR 1 Rating 3 vs CTR 4 Rating 5 27.7803 1.35481 20.5049 5.01 Significant
Difference
5 CTR 1 Rating 3 vs CTR 1 Rating 1 24.7655 1.37435 18.0198 5.01 Significant
Difference
6 CTR 1 Rating 3 vs CTR 2 Rating 1 24.5643 1.66501 14.7533 5.01 Significant
Difference
7 CTR 1 Rating 3 vs CTR 3 Rating 1 24.4179 1.30959 18.6455 5.01 Significant
Difference
8 CTR 1 Rating 3 vs CTR 1 Rating 4 21.1440 1.37435 15.3847 5.01 Significant
Difference
9 CTR 1 Rating 3 vs CTR 2 Rating 4 17.6583 1.66501 10.6055 5.01 Significant
Difference
10 CTR 1 Rating 3 vs CTR 2 Rating 5 17.6583 1.66501 10.6055 5.01 Significant
Difference
11 CTR 1 Rating 3 vs CTR 4 Rating 2 16.6522 1.35481 12.2912 5.01 Significant
Difference
12 CTR 1 Rating 3 vs CTR 3 Rating 4 15.6756 1.30959 11.9698 5.01 Significant
Difference
13 CTR 1 Rating 3 vs CTR 1 Rating 2 14.8467 1.37435 10.8027 5.01 Significant
Difference
14 CTR 1 Rating 3 vs CTR 3 Rating 2 13.3876 1.30959 10.2228 5.01 Significant
Difference
15 CTR 1 Rating 3 vs CTR 2 Rating 2 12.7615 1.66501 7.6645 5.01 Significant
Difference

110
16 CTR 1 Rating 3 vs CTR 2 Rating 3 12.4720 1.66501 7.4907 5.01 Significant
Difference
17 CTR 1 Rating 3 vs CTR 4 Rating 4 10.7251 1.35481 7.9163 5.01 Significant
Difference
18 CTR 1 Rating 3 vs CTR 3 Rating 3 5.1451 1.30959 3.9288 5.01 No
Difference
19 CTR 1 Rating 3 vs CTR 4 Rating 3 4.3013 1.35481 3.1748 5.01 No
Difference
20 CTR 4 Rating 3 vs CTR 4 Rating 1 27.8833 1.33499 20.8865 5.01 Significant
Difference
21 CTR 4 Rating 3 vs CTR 3 Rating 5 26.7377 1.28907 20.7419 5.01 Significant
Difference
22 CTR 4 Rating 3 vs CTR 1 Rating 5 25.3894 1.35481 18.7402 5.01 Significant
Difference
23 CTR 4 Rating 3 vs CTR 4 Rating 5 23.4790 1.33499 17.5874 5.01 Significant
Difference
24 CTR 4 Rating 3 vs CTR 1 Rating 1 20.4642 1.35481 15.1048 5.01 Significant
Difference
25 CTR 4 Rating 3 vs CTR 2 Rating 1 20.2630 1.64892 12.2887 5.01 Significant
Difference
26 CTR 4 Rating 3 vs CTR 3 Rating 1 20.1166 1.28907 15.6055 5.01 Significant
Difference
27 CTR 4 Rating 3 vs CTR 1 Rating 4 16.8427 1.35481 12.4317 5.01 Significant
Difference
28 CTR 4 Rating 3 vs CTR 2 Rating 4 13.3570 1.64892 8.1004 5.01 Significant
Difference
29 CTR 4 Rating 3 vs CTR 2 Rating 5 13.3570 1.64892 8.1004 5.01 Significant
Difference
30 CTR 4 Rating 3 vs CTR 4 Rating 2 12.3509 1.33499 9.2517 5.01 Significant
Difference
31 CTR 4 Rating 3 vs CTR 3 Rating 4 11.3742 1.28907 8.8236 5.01 Significant
Difference
32 CTR 4 Rating 3 vs CTR 1 Rating 2 10.5453 1.35481 7.7836 5.01 Significant
Difference
33 CTR 4 Rating 3 vs CTR 3 Rating 2 9.0863 1.28907 7.0487 5.01 Significant
Difference
34 CTR 4 Rating 3 vs CTR 2 Rating 2 8.4602 1.64892 5.1308 5.01 Significant
Difference
35 CTR 4 Rating 3 vs CTR 2 Rating 3 8.1707 1.64892 4.9552 5.01 No
Difference

111
36 CTR 4 Rating 3 vs CTR 4 Rating 4 6.4238 1.33499 4.8119 5.01 No
Difference
37 CTR 4 Rating 3 vs CTR 3 Rating 3 0.8437 1.28907 0.6545 5.01 No
Difference
38 CTR 3 Rating 3 vs CTR 4 Rating 1 27.0395 1.28907 20.9760 5.01 Significant
Difference
39 CTR 3 Rating 3 vs CTR 3 Rating 5 25.8940 1.24146 20.8577 5.01 Significant
Difference
40 CTR 3 Rating 3 vs CTR 1 Rating 5 24.5457 1.30959 18.7430 5.01 Significant
Difference
41 CTR 3 Rating 3 vs CTR 4 Rating 5 22.6353 1.28907 17.5594 5.01 Significant
Difference
42 CTR 3 Rating 3 vs CTR 1 Rating 1 19.6205 1.30959 14.9821 5.01 Significant
Difference
43 CTR 3 Rating 3 vs CTR 2 Rating 1 19.4193 1.61197 12.0469 5.01 Significant
Difference
44 CTR 3 Rating 3 vs CTR 3 Rating 1 19.2729 1.24146 15.5244 5.01 Significant
Difference
45 CTR 3 Rating 3 vs CTR 1 Rating 4 15.9989 1.30959 12.2167 5.01 Significant
Difference
46 CTR 3 Rating 3 vs CTR 2 Rating 4 12.5132 1.61197 7.7627 5.01 Significant
Difference
47 CTR 3 Rating 3 vs CTR 2 Rating 5 12.5132 1.61197 7.7627 5.01 Significant
Difference
48 CTR 3 Rating 3 vs CTR 4 Rating 2 11.5071 1.28907 8.9267 5.01 Significant
Difference
49 CTR 3 Rating 3 vs CTR 3 Rating 4 10.5305 1.24146 8.4823 5.01 Significant
Difference
50 CTR 3 Rating 3 vs CTR 1 Rating 2 9.7016 1.30959 7.4081 5.01 Significant
Difference
51 CTR 3 Rating 3 vs CTR 3 Rating 2 8.2426 1.24146 6.6394 5.01 Significant
Difference
52 CTR 3 Rating 3 vs CTR 2 Rating 2 7.6165 1.61197 4.7249 5.01 No
Difference
53 CTR 3 Rating 3 vs CTR 2 Rating 3 7.3270 1.61197 4.5453 5.01 No
Difference
54 CTR 3 Rating 3 vs CTR 4 Rating 4 5.5801 1.28907 4.3287 5.01 No
Difference
55 CTR 4 Rating 4 vs CTR 4 Rating 1 21.4595 1.33499 16.0747 5.01 Significant
Difference

112
56 CTR 4 Rating 4 vs CTR 3 Rating 5 20.3139 1.28907 15.7586 5.01 Significant
Difference
57 CTR 4 Rating 4 vs CTR 1 Rating 5 18.9656 1.35481 13.9987 5.01 Significant
Difference
58 CTR 4 Rating 4 vs CTR 4 Rating 5 17.0552 1.33499 12.7756 5.01 Significant
Difference
59 CTR 4 Rating 4 vs CTR 1 Rating 1 14.0404 1.35481 10.3634 5.01 Significant
Difference
60 CTR 4 Rating 4 vs CTR 2 Rating 1 13.8392 1.64892 8.3929 5.01 Significant
Difference
61 CTR 4 Rating 4 vs CTR 3 Rating 1 13.6928 1.28907 10.6222 5.01 Significant
Difference
62 CTR 4 Rating 4 vs CTR 1 Rating 4 10.4189 1.35481 7.6903 5.01 Significant
Difference
63 CTR 4 Rating 4 vs CTR 2 Rating 4 6.9332 1.64892 4.2047 5.01 No
Difference
64 CTR 4 Rating 4 vs CTR 2 Rating 5 6.9332 1.64892 4.2047 5.01 No
Difference
65 CTR 4 Rating 4 vs CTR 4 Rating 2 5.9271 1.33499 4.4398 5.01 No
Difference
66 CTR 4 Rating 4 vs CTR 3 Rating 4 4.9504 1.28907 3.8403 5.01 No
Difference
67 CTR 4 Rating 4 vs CTR 1 Rating 2 4.1215 1.35481 3.0422 5.01 No
Difference
68 CTR 4 Rating 4 vs CTR 3 Rating 2 2.6625 1.28907 2.0655 5.01 No
Difference
69 CTR 4 Rating 4 vs CTR 2 Rating 2 2.0364 1.64892 1.2350 5.01 No
Difference
70 CTR 4 Rating 4 vs CTR 2 Rating 3 1.7469 1.64892 1.0594 5.01 No
Difference
71 CTR 2 Rating 3 vs CTR 4 Rating 1 19.7126 1.64892 11.9548 5.01 Significant
Difference
72 CTR 2 Rating 3 vs CTR 3 Rating 5 18.5670 1.61197 11.5182 5.01 Significant
Difference
73 CTR 2 Rating 3 vs CTR 1 Rating 5 17.2187 1.66501 10.3415 5.01 Significant
Difference
74 CTR 2 Rating 3 vs CTR 4 Rating 5 15.3083 1.64892 9.2838 5.01 Significant
Difference
75 CTR 2 Rating 3 vs CTR 1 Rating 1 12.2935 1.66501 7.3834 5.01 Significant
Difference

113
76 CTR 2 Rating 3 vs CTR 2 Rating 1 12.0923 1.91198 6.3245 5.01 Significant
Difference
77 CTR 2 Rating 3 vs CTR 3 Rating 1 11.9459 1.61197 7.4107 5.01 Significant
Difference
78 CTR 2 Rating 3 vs CTR 1 Rating 4 8.6720 1.66501 5.2083 5.01 Significant
Difference
79 CTR 2 Rating 3 vs CTR 2 Rating 4 5.1862 1.91198 2.7125 5.01 No
Difference
80 CTR 2 Rating 3 vs CTR 2 Rating 5 5.1862 1.91198 2.7125 5.01 No
Difference
81 CTR 2 Rating 3 vs CTR 4 Rating 2 4.1802 1.64892 2.5351 5.01 No
Difference
82 CTR 2 Rating 3 vs CTR 3 Rating 4 3.2035 1.61197 1.9873 5.01 No
Difference
83 CTR 2 Rating 3 vs CTR 1 Rating 2 2.3746 1.66501 1.4262 5.01 No
Difference
84 CTR 2 Rating 3 vs CTR 3 Rating 2 0.9156 1.61197 0.5680 5.01 No
Difference
85 CTR 2 Rating 3 vs CTR 2 Rating 2 0.2895 1.91198 0.1514 5.01 No
Difference
86 CTR 2 Rating 2 vs CTR 4 Rating 1 19.4231 1.64892 11.7793 5.01 Significant
Difference
87 CTR 2 Rating 2 vs CTR 3 Rating 5 18.2775 1.61197 11.3386 5.01 Significant
Difference
88 CTR 2 Rating 2 vs CTR 1 Rating 5 16.9292 1.66501 10.1676 5.01 Significant
Difference
89 CTR 2 Rating 2 vs CTR 4 Rating 5 15.0188 1.64892 9.1083 5.01 Significant
Difference
90 CTR 2 Rating 2 vs CTR 1 Rating 1 12.0040 1.66501 7.2096 5.01 Significant
Difference
91 CTR 2 Rating 2 vs CTR 2 Rating 1 11.8028 1.91198 6.1731 5.01 Significant
Difference
92 CTR 2 Rating 2 vs CTR 3 Rating 1 11.6564 1.61197 7.2312 5.01 Significant
Difference
93 CTR 2 Rating 2 vs CTR 1 Rating 4 8.3825 1.66501 5.0345 5.01 Significant
Difference
94 CTR 2 Rating 2 vs CTR 2 Rating 4 4.8968 1.91198 2.5611 5.01 No
Difference
95 CTR 2 Rating 2 vs CTR 2 Rating 5 4.8968 1.91198 2.5611 5.01 No
Difference

114
96 CTR 2 Rating 2 vs CTR 4 Rating 2 3.8907 1.64892 2.3595 5.01 No
Difference
97 CTR 2 Rating 2 vs CTR 3 Rating 4 2.9140 1.61197 1.8077 5.01 No
Difference
98 CTR 2 Rating 2 vs CTR 1 Rating 2 2.0851 1.66501 1.2523 5.01 No
Difference
99 CTR 2 Rating 2 vs CTR 3 Rating 2 0.6261 1.61197 0.3884 5.01 No
Difference
100 CTR 3 Rating 2 vs CTR 4 Rating 1 18.7970 1.28907 14.5818 5.01 Significant
Difference
101 CTR 3 Rating 2 vs CTR 3 Rating 5 17.6514 1.24146 14.2183 5.01 Significant
Difference
102 CTR 3 Rating 2 vs CTR 1 Rating 5 16.3031 1.30959 12.4490 5.01 Significant
Difference
103 CTR 3 Rating 2 vs CTR 4 Rating 5 14.3927 1.28907 11.1652 5.01 Significant
Difference
104 CTR 3 Rating 2 vs CTR 1 Rating 1 11.3779 1.30959 8.6881 5.01 Significant
Difference
105 CTR 3 Rating 2 vs CTR 2 Rating 1 11.1767 1.61197 6.9336 5.01 Significant
Difference
106 CTR 3 Rating 2 vs CTR 3 Rating 1 11.0303 1.24146 8.8850 5.01 Significant
Difference
107 CTR 3 Rating 2 vs CTR 1 Rating 4 7.7564 1.30959 5.9227 5.01 Significant
Difference
108 CTR 3 Rating 2 vs CTR 2 Rating 4 4.2706 1.61197 2.6493 5.01 No
Difference
109 CTR 3 Rating 2 vs CTR 2 Rating 5 4.2706 1.61197 2.6493 5.01 No
Difference
110 CTR 3 Rating 2 vs CTR 4 Rating 2 3.2646 1.28907 2.5325 5.01 No
Difference
111 CTR 3 Rating 2 vs CTR 3 Rating 4 2.2879 1.24146 1.8429 5.01 No
Difference
112 CTR 3 Rating 2 vs CTR 1 Rating 2 1.4590 1.30959 1.1141 5.01 No
Difference
113 CTR 1 Rating 2 vs CTR 4 Rating 1 17.3379 1.35481 12.7973 5.01 Significant
Difference
114 CTR 1 Rating 2 vs CTR 3 Rating 5 16.1924 1.30959 12.3645 5.01 Significant
Difference
115 CTR 1 Rating 2 vs CTR 1 Rating 5 14.8441 1.37435 10.8008 5.01 Significant
Difference

115
116 CTR 1 Rating 2 vs CTR 4 Rating 5 12.9337 1.35481 9.5465 5.01 Significant
Difference
117 CTR 1 Rating 2 vs CTR 1 Rating 1 9.9189 1.37435 7.2171 5.01 Significant
Difference
118 CTR 1 Rating 2 vs CTR 2 Rating 1 9.7177 1.66501 5.8364 5.01 Significant
Difference
119 CTR 1 Rating 2 vs CTR 3 Rating 1 9.5713 1.30959 7.3086 5.01 Significant
Difference
120 CTR 1 Rating 2 vs CTR 1 Rating 4 6.2973 1.37435 4.5820 5.01 No
Difference
121 CTR 1 Rating 2 vs CTR 2 Rating 4 2.8116 1.66501 1.6887 5.01 No
Difference
122 CTR 1 Rating 2 vs CTR 2 Rating 5 2.8116 1.66501 1.6887 5.01 No
Difference
123 CTR 1 Rating 2 vs CTR 4 Rating 2 1.8055 1.35481 1.3327 5.01 No
Difference
124 CTR 1 Rating 2 vs CTR 3 Rating 4 0.8289 1.30959 0.6329 5.01 No
Difference
125 CTR 3 Rating 4 vs CTR 4 Rating 1 16.5091 1.28907 12.8069 5.01 Significant
Difference
126 CTR 3 Rating 4 vs CTR 3 Rating 5 15.3635 1.24146 12.3754 5.01 Significant
Difference
127 CTR 3 Rating 4 vs CTR 1 Rating 5 14.0152 1.30959 10.7020 5.01 Significant
Difference
128 CTR 3 Rating 4 vs CTR 4 Rating 5 12.1048 1.28907 9.3903 5.01 Significant
Difference
129 CTR 3 Rating 4 vs CTR 1 Rating 1 9.0900 1.30959 6.9411 5.01 Significant
Difference
130 CTR 3 Rating 4 vs CTR 2 Rating 1 8.8888 1.61197 5.5142 5.01 Significant
Difference
131 CTR 3 Rating 4 vs CTR 3 Rating 1 8.7424 1.24146 7.0420 5.01 Significant
Difference
132 CTR 3 Rating 4 vs CTR 1 Rating 4 5.4684 1.30959 4.1757 5.01 No
Difference
133 CTR 3 Rating 4 vs CTR 2 Rating 4 1.9827 1.61197 1.2300 5.01 No
Difference
134 CTR 3 Rating 4 vs CTR 2 Rating 5 1.9827 1.61197 1.2300 5.01 No
Difference
135 CTR 3 Rating 4 vs CTR 4 Rating 2 0.9767 1.28907 0.7576 5.01 No
Difference

116
136 CTR 4 Rating 2 vs CTR 4 Rating 1 15.5324 1.33499 11.6349 5.01 Significant
Difference
137 CTR 4 Rating 2 vs CTR 3 Rating 5 14.3869 1.28907 11.1606 5.01 Significant
Difference
138 CTR 4 Rating 2 vs CTR 1 Rating 5 13.0385 1.35481 9.6239 5.01 Significant
Difference
139 CTR 4 Rating 2 vs CTR 4 Rating 5 11.1281 1.33499 8.3357 5.01 Significant
Difference
140 CTR 4 Rating 2 vs CTR 1 Rating 1 8.1133 1.35481 5.9885 5.01 Significant
Difference
141 CTR 4 Rating 2 vs CTR 2 Rating 1 7.9121 1.64892 4.7984 5.01 No
Difference
142 CTR 4 Rating 2 vs CTR 3 Rating 1 7.7657 1.28907 6.0243 5.01 Significant
Difference
143 CTR 4 Rating 2 vs CTR 1 Rating 4 4.4918 1.35481 3.3154 5.01 No
Difference
144 CTR 4 Rating 2 vs CTR 2 Rating 4 1.0061 1.64892 0.6101 5.01 No
Difference
145 CTR 4 Rating 2 vs CTR 2 Rating 5 1.0061 1.64892 0.6101 5.01 No
Difference
146 CTR 2 Rating 5 vs CTR 4 Rating 1 14.5263 1.64892 8.8096 5.01 Significant
Difference
147 CTR 2 Rating 5 vs CTR 3 Rating 5 13.3808 1.61197 8.3009 5.01 Significant
Difference
148 CTR 2 Rating 5 vs CTR 1 Rating 5 12.0325 1.66501 7.2267 5.01 Significant
Difference
149 CTR 2 Rating 5 vs CTR 4 Rating 5 10.1221 1.64892 6.1386 5.01 Significant
Difference
150 CTR 2 Rating 5 vs CTR 1 Rating 1 7.1072 1.66501 4.2686 5.01 No
Difference
151 CTR 2 Rating 5 vs CTR 2 Rating 1 6.9060 1.91198 3.6120 5.01 No
Difference
152 CTR 2 Rating 5 vs CTR 3 Rating 1 6.7597 1.61197 4.1934 5.01 No
Difference
153 CTR 2 Rating 5 vs CTR 1 Rating 4 3.4857 1.66501 2.0935 5.01 No
Difference
154 CTR 2 Rating 5 vs CTR 2 Rating 4 0.0000 1.91198 0.0000 5.01 No
Difference
155 CTR 2 Rating 4 vs CTR 4 Rating 1 14.5263 1.64892 8.8096 5.01 Significant
Difference

117
156 CTR 2 Rating 4 vs CTR 3 Rating 5 13.3808 1.61197 8.3009 5.01 Significant
Difference
157 CTR 2 Rating 4 vs CTR 1 Rating 5 12.0325 1.66501 7.2267 5.01 Significant
Difference
158 CTR 2 Rating 4 vs CTR 4 Rating 5 10.1221 1.64892 6.1386 5.01 Significant
Difference
159 CTR 2 Rating 4 vs CTR 1 Rating 1 7.1072 1.66501 4.2686 5.01 No
Difference
160 CTR 2 Rating 4 vs CTR 2 Rating 1 6.9060 1.91198 3.6120 5.01 No
Difference
161 CTR 2 Rating 4 vs CTR 3 Rating 1 6.7597 1.61197 4.1934 5.01 No
Difference
162 CTR 2 Rating 4 vs CTR 1 Rating 4 3.4857 1.66501 2.0935 5.01 No
Difference
163 CTR 1 Rating 4 vs CTR 4 Rating 1 11.0406 1.35481 8.1492 5.01 Significant
Difference
164 CTR 1 Rating 4 vs CTR 3 Rating 5 9.8951 1.30959 7.5559 5.01 Significant
Difference
165 CTR 1 Rating 4 vs CTR 1 Rating 5 8.5468 1.37435 6.2188 5.01 Significant
Difference
166 CTR 1 Rating 4 vs CTR 4 Rating 5 6.6363 1.35481 4.8984 5.01 No
Difference
167 CTR 1 Rating 4 vs CTR 1 Rating 1 3.6215 1.37435 2.6351 5.01 No
Difference
168 CTR 1 Rating 4 vs CTR 2 Rating 1 3.4203 1.66501 2.0542 5.01 No
Difference
169 CTR 1 Rating 4 vs CTR 3 Rating 1 3.2740 1.30959 2.5000 5.01 No
Difference
170 CTR 3 Rating 1 vs CTR 4 Rating 1 7.7667 1.28907 6.0250 5.01 Significant
Difference
171 CTR 3 Rating 1 vs CTR 3 Rating 5 6.6211 1.24146 5.3333 5.01 Significant
Difference
172 CTR 3 Rating 1 vs CTR 1 Rating 5 5.2728 1.30959 4.0263 5.01 No
Difference
173 CTR 3 Rating 1 vs CTR 4 Rating 5 3.3624 1.28907 2.6084 5.01 No
Difference
174 CTR 3 Rating 1 vs CTR 1 Rating 1 0.3476 1.30959 0.2654 5.01 No
Difference
175 CTR 3 Rating 1 vs CTR 2 Rating 1 0.1464 1.61197 0.0908 5.01 No
Difference

118
176 CTR 2 Rating 1 vs CTR 4 Rating 1 7.6203 1.64892 4.6214 5.01 No
Difference
177 CTR 2 Rating 1 vs CTR 3 Rating 5 6.4747 1.61197 4.0167 5.01 No
Difference
178 CTR 2 Rating 1 vs CTR 1 Rating 5 5.1264 1.66501 3.0789 5.01 No
Difference
179 CTR 2 Rating 1 vs CTR 4 Rating 5 3.2160 1.64892 1.9504 5.01 No
Difference
180 CTR 2 Rating 1 vs CTR 1 Rating 1 0.2012 1.66501 0.1208 5.01 No
Difference
181 CTR 1 Rating 1 vs CTR 4 Rating 1 7.4191 1.35481 5.4761 5.01 Significant
Difference
182 CTR 1 Rating 1 vs CTR 3 Rating 5 6.2735 1.30959 4.7905 5.01 No
Difference
183 CTR 1 Rating 1 vs CTR 1 Rating 5 4.9252 1.37435 3.5837 5.01 No
Difference
184 CTR 1 Rating 1 vs CTR 4 Rating 5 3.0148 1.35481 2.2253 5.01 No
Difference
185 CTR 4 Rating 5 vs CTR 4 Rating 1 4.4043 1.33499 3.2991 5.01 No
Difference
186 CTR 4 Rating 5 vs CTR 3 Rating 5 3.2587 1.28907 2.5280 5.01 No
Difference
187 CTR 4 Rating 5 vs CTR 1 Rating 5 1.9104 1.35481 1.4101 5.01 No
Difference
188 CTR 1 Rating 5 vs CTR 4 Rating 1 2.4939 1.35481 1.8407 5.01 No
Difference
189 CTR 1 Rating 5 vs CTR 3 Rating 5 1.3483 1.30959 1.0296 5.01 No
Difference
190 CTR 3 Rating 5 vs CTR 4 Rating 1 1.1455 1.28907 0.8887 5.01 No
Difference
Reference: Biostatistical Analysis, 4th Edition, Jerrold Zar, 1999, p564.
————— 4/26/2012 1:52:08 PM ————————————————————

119
Welcome to Minitab, press F1 for help.
Retrieving project from file: 'E:\EMILY\AMERICLEFT OSU\CENTER SCORES FOR
CHI TEST.MPJ'
————— 1/11/2012 2:15:48 PM ————————————————————
Welcome to Minitab, press F1 for help.
Executing from file: H:\Latest Macros\macros\MULTPROP.MAC
Multiple Comparisons for Proportions
Ho: There is not a significant difference between Proportions
H1: There is a significant difference between Proportions
Row Compare Diff SE q q(.05) Conclusion
1 CTR 1 Rating 3 vs CTR 3 Rating 5 32.9511 1.22586 26.8800 5.01 Significant
Difference
2 CTR 1 Rating 3 vs CTR 2 Rating 1 32.0048 1.22586 26.1081 5.01 Significant
Difference
3 CTR 1 Rating 3 vs CTR 1 Rating 5 31.6992 1.21005 26.1965 5.01 Significant
Difference
4 CTR 1 Rating 3 vs CTR 4 Rating 1 28.8711 1.27254 22.6878 5.01 Significant
Difference
5 CTR 1 Rating 3 vs CTR 2 Rating 2 25.2640 1.22586 20.6092 5.01 Significant
Difference
6 CTR 1 Rating 3 vs CTR 4 Rating 5 24.8073 1.27254 19.4944 5.01 Significant
Difference
7 CTR 1 Rating 3 vs CTR 1 Rating 1 24.4558 1.21005 20.2105 5.01 Significant
Difference
8 CTR 1 Rating 3 vs CTR 3 Rating 1 23.7946 1.22586 19.4106 5.01 Significant
Difference

120
9 CTR 1 Rating 3 vs CTR 2 Rating 5 21.4357 1.22586 17.4863 5.01 Significant
Difference
10 CTR 1 Rating 3 vs CTR 4 Rating 2 16.2046 1.27254 12.7341 5.01 Significant
Difference
11 CTR 1 Rating 3 vs CTR 1 Rating 4 15.8400 1.21005 13.0904 5.01 Significant
Difference
12 CTR 1 Rating 3 vs CTR 1 Rating 2 14.7086 1.21005 12.1553 5.01 Significant
Difference
13 CTR 1 Rating 3 vs CTR 4 Rating 4 14.6749 1.27254 11.5320 5.01 Significant
Difference
14 CTR 1 Rating 3 vs CTR 3 Rating 2 12.7859 1.22586 10.4302 5.01 Significant
Difference
15 CTR 1 Rating 3 vs CTR 2 Rating 4 8.0003 1.22586 6.5263 5.01 Significant
Difference
16 CTR 1 Rating 3 vs CTR 3 Rating 3 1.8683 1.22586 1.5240 5.01 No
Difference
17 CTR 1 Rating 3 vs CTR 3 Rating 4 1.8683 1.22586 1.5240 5.01 No
Difference
18 CTR 1 Rating 3 vs CTR 2 Rating 3 1.2166 1.22586 0.9925 5.01 No
Difference
19 CTR 1 Rating 3 vs CTR 4 Rating 3 0.6676 1.27254 0.5246 5.01 No
Difference
20 CTR 4 Rating 3 vs CTR 3 Rating 5 32.2835 1.28758 25.0731 5.01 Significant
Difference
21 CTR 4 Rating 3 vs CTR 2 Rating 1 31.3372 1.28758 24.3381 5.01 Significant
Difference
22 CTR 4 Rating 3 vs CTR 1 Rating 5 31.0316 1.27254 24.3855 5.01 Significant
Difference
23 CTR 4 Rating 3 vs CTR 4 Rating 1 28.2035 1.33210 21.1722 5.01 Significant
Difference
24 CTR 4 Rating 3 vs CTR 2 Rating 2 24.5964 1.28758 19.1028 5.01 Significant
Difference
25 CTR 4 Rating 3 vs CTR 4 Rating 5 24.1397 1.33210 18.1216 5.01 Significant
Difference
26 CTR 4 Rating 3 vs CTR 1 Rating 1 23.7882 1.27254 18.6935 5.01 Significant
Difference
27 CTR 4 Rating 3 vs CTR 3 Rating 1 23.1270 1.28758 17.9617 5.01 Significant
Difference
28 CTR 4 Rating 3 vs CTR 2 Rating 5 20.7681 1.28758 16.1296 5.01 Significant
Difference

121
29 CTR 4 Rating 3 vs CTR 4 Rating 2 15.5370 1.33210 11.6635 5.01 Significant
Difference
30 CTR 4 Rating 3 vs CTR 1 Rating 4 15.1724 1.27254 11.9230 5.01 Significant
Difference
31 CTR 4 Rating 3 vs CTR 1 Rating 2 14.0410 1.27254 11.0339 5.01 Significant
Difference
32 CTR 4 Rating 3 vs CTR 4 Rating 4 14.0073 1.33210 10.5152 5.01 Significant
Difference
33 CTR 4 Rating 3 vs CTR 3 Rating 2 12.1183 1.28758 9.4117 5.01 Significant
Difference
34 CTR 4 Rating 3 vs CTR 2 Rating 4 7.3328 1.28758 5.6950 5.01 Significant
Difference
35 CTR 4 Rating 3 vs CTR 3 Rating 3 1.2007 1.28758 0.9325 5.01 No
Difference
36 CTR 4 Rating 3 vs CTR 3 Rating 4 1.2007 1.28758 0.9325 5.01 No
Difference
37 CTR 4 Rating 3 vs CTR 2 Rating 3 0.5490 1.28758 0.4264 5.01 No
Difference
38 CTR 2 Rating 3 vs CTR 3 Rating 5 31.7345 1.24146 25.5622 5.01 Significant
Difference
39 CTR 2 Rating 3 vs CTR 2 Rating 1 30.7881 1.24146 24.8000 5.01 Significant
Difference
40 CTR 2 Rating 3 vs CTR 1 Rating 5 30.4825 1.22586 24.8663 5.01 Significant
Difference
41 CTR 2 Rating 3 vs CTR 4 Rating 1 27.6545 1.28758 21.4779 5.01 Significant
Difference
42 CTR 2 Rating 3 vs CTR 2 Rating 2 24.0474 1.24146 19.3702 5.01 Significant
Difference
43 CTR 2 Rating 3 vs CTR 4 Rating 5 23.5907 1.28758 18.3218 5.01 Significant
Difference
44 CTR 2 Rating 3 vs CTR 1 Rating 1 23.2392 1.22586 18.9575 5.01 Significant
Difference
45 CTR 2 Rating 3 vs CTR 3 Rating 1 22.5780 1.24146 18.1867 5.01 Significant
Difference
46 CTR 2 Rating 3 vs CTR 2 Rating 5 20.2191 1.24146 16.2866 5.01 Significant
Difference
47 CTR 2 Rating 3 vs CTR 4 Rating 2 14.9880 1.28758 11.6405 5.01 Significant
Difference
48 CTR 2 Rating 3 vs CTR 1 Rating 4 14.6234 1.22586 11.9291 5.01 Significant
Difference

122
49 CTR 2 Rating 3 vs CTR 1 Rating 2 13.4920 1.22586 11.0062 5.01 Significant
Difference
50 CTR 2 Rating 3 vs CTR 4 Rating 4 13.4583 1.28758 10.4524 5.01 Significant
Difference
51 CTR 2 Rating 3 vs CTR 3 Rating 2 11.5693 1.24146 9.3191 5.01 Significant
Difference
52 CTR 2 Rating 3 vs CTR 2 Rating 4 6.7837 1.24146 5.4643 5.01 Significant
Difference
53 CTR 2 Rating 3 vs CTR 3 Rating 3 0.6517 1.24146 0.5249 5.01 No
Difference
54 CTR 2 Rating 3 vs CTR 3 Rating 4 0.6517 1.24146 0.5249 5.01 No
Difference
55 CTR 3 Rating 4 vs CTR 3 Rating 5 31.0828 1.24146 25.0373 5.01 Significant
Difference
56 CTR 3 Rating 4 vs CTR 2 Rating 1 30.1365 1.24146 24.2751 5.01 Significant
Difference
57 CTR 3 Rating 4 vs CTR 1 Rating 5 29.8309 1.22586 24.3347 5.01 Significant
Difference
58 CTR 3 Rating 4 vs CTR 4 Rating 1 27.0028 1.28758 20.9718 5.01 Significant
Difference
59 CTR 3 Rating 4 vs CTR 2 Rating 2 23.3957 1.24146 18.8453 5.01 Significant
Difference
60 CTR 3 Rating 4 vs CTR 4 Rating 5 22.9391 1.28758 17.8157 5.01 Significant
Difference
61 CTR 3 Rating 4 vs CTR 1 Rating 1 22.5875 1.22586 18.4259 5.01 Significant
Difference
62 CTR 3 Rating 4 vs CTR 3 Rating 1 21.9264 1.24146 17.6618 5.01 Significant
Difference
63 CTR 3 Rating 4 vs CTR 2 Rating 5 19.5674 1.24146 15.7617 5.01 Significant
Difference
64 CTR 3 Rating 4 vs CTR 4 Rating 2 14.3363 1.28758 11.1343 5.01 Significant
Difference
65 CTR 3 Rating 4 vs CTR 1 Rating 4 13.9718 1.22586 11.3976 5.01 Significant
Difference
66 CTR 3 Rating 4 vs CTR 1 Rating 2 12.8403 1.22586 10.4746 5.01 Significant
Difference
67 CTR 3 Rating 4 vs CTR 4 Rating 4 12.8066 1.28758 9.9463 5.01 Significant
Difference
68 CTR 3 Rating 4 vs CTR 3 Rating 2 10.9176 1.24146 8.7942 5.01 Significant
Difference

123
69 CTR 3 Rating 4 vs CTR 2 Rating 4 6.1321 1.24146 4.9394 5.01 No
Difference
70 CTR 3 Rating 4 vs CTR 3 Rating 3 0.0000 1.24146 0.0000 5.01 No
Difference
71 CTR 3 Rating 3 vs CTR 3 Rating 5 31.0828 1.24146 25.0373 5.01 Significant
Difference
72 CTR 3 Rating 3 vs CTR 2 Rating 1 30.1365 1.24146 24.2751 5.01 Significant
Difference
73 CTR 3 Rating 3 vs CTR 1 Rating 5 29.8309 1.22586 24.3347 5.01 Significant
Difference
74 CTR 3 Rating 3 vs CTR 4 Rating 1 27.0028 1.28758 20.9718 5.01 Significant
Difference
75 CTR 3 Rating 3 vs CTR 2 Rating 2 23.3957 1.24146 18.8453 5.01 Significant
Difference
76 CTR 3 Rating 3 vs CTR 4 Rating 5 22.9391 1.28758 17.8157 5.01 Significant
Difference
77 CTR 3 Rating 3 vs CTR 1 Rating 1 22.5875 1.22586 18.4259 5.01 Significant
Difference
78 CTR 3 Rating 3 vs CTR 3 Rating 1 21.9264 1.24146 17.6618 5.01 Significant
Difference
79 CTR 3 Rating 3 vs CTR 2 Rating 5 19.5674 1.24146 15.7617 5.01 Significant
Difference
80 CTR 3 Rating 3 vs CTR 4 Rating 2 14.3363 1.28758 11.1343 5.01 Significant
Difference
81 CTR 3 Rating 3 vs CTR 1 Rating 4 13.9718 1.22586 11.3976 5.01 Significant
Difference
82 CTR 3 Rating 3 vs CTR 1 Rating 2 12.8403 1.22586 10.4746 5.01 Significant
Difference
83 CTR 3 Rating 3 vs CTR 4 Rating 4 12.8066 1.28758 9.9463 5.01 Significant
Difference
84 CTR 3 Rating 3 vs CTR 3 Rating 2 10.9176 1.24146 8.7942 5.01 Significant
Difference
85 CTR 3 Rating 3 vs CTR 2 Rating 4 6.1321 1.24146 4.9394 5.01 No
Difference
86 CTR 2 Rating 4 vs CTR 3 Rating 5 24.9507 1.24146 20.0979 5.01 Significant
Difference
87 CTR 2 Rating 4 vs CTR 2 Rating 1 24.0044 1.24146 19.3356 5.01 Significant
Difference
88 CTR 2 Rating 4 vs CTR 1 Rating 5 23.6988 1.22586 19.3324 5.01 Significant
Difference

124
89 CTR 2 Rating 4 vs CTR 4 Rating 1 20.8707 1.28758 16.2093 5.01 Significant
Difference
90 CTR 2 Rating 4 vs CTR 2 Rating 2 17.2636 1.24146 13.9059 5.01 Significant
Difference
91 CTR 2 Rating 4 vs CTR 4 Rating 5 16.8070 1.28758 13.0532 5.01 Significant
Difference
92 CTR 2 Rating 4 vs CTR 1 Rating 1 16.4554 1.22586 13.4236 5.01 Significant
Difference
93 CTR 2 Rating 4 vs CTR 3 Rating 1 15.7943 1.24146 12.7223 5.01 Significant
Difference
94 CTR 2 Rating 4 vs CTR 2 Rating 5 13.4354 1.24146 10.8222 5.01 Significant
Difference
95 CTR 2 Rating 4 vs CTR 4 Rating 2 8.2042 1.28758 6.3718 5.01 Significant
Difference
96 CTR 2 Rating 4 vs CTR 1 Rating 4 7.8397 1.22586 6.3953 5.01 Significant
Difference
97 CTR 2 Rating 4 vs CTR 1 Rating 2 6.7083 1.22586 5.4723 5.01 Significant
Difference
98 CTR 2 Rating 4 vs CTR 4 Rating 4 6.6746 1.28758 5.1838 5.01 Significant
Difference
99 CTR 2 Rating 4 vs CTR 3 Rating 2 4.7855 1.24146 3.8548 5.01 No
Difference
100 CTR 3 Rating 2 vs CTR 3 Rating 5 20.1652 1.24146 16.2431 5.01 Significant
Difference
101 CTR 3 Rating 2 vs CTR 2 Rating 1 19.2189 1.24146 15.4809 5.01 Significant
Difference
102 CTR 3 Rating 2 vs CTR 1 Rating 5 18.9133 1.22586 15.4286 5.01 Significant
Difference
103 CTR 3 Rating 2 vs CTR 4 Rating 1 16.0852 1.28758 12.4926 5.01 Significant
Difference
104 CTR 3 Rating 2 vs CTR 2 Rating 2 12.4781 1.24146 10.0511 5.01 Significant
Difference
105 CTR 3 Rating 2 vs CTR 4 Rating 5 12.0214 1.28758 9.3365 5.01 Significant
Difference
106 CTR 3 Rating 2 vs CTR 1 Rating 1 11.6699 1.22586 9.5198 5.01 Significant
Difference
107 CTR 3 Rating 2 vs CTR 3 Rating 1 11.0087 1.24146 8.8676 5.01 Significant
Difference
108 CTR 3 Rating 2 vs CTR 2 Rating 5 8.6498 1.24146 6.9675 5.01 Significant
Difference

125
109 CTR 3 Rating 2 vs CTR 4 Rating 2 3.4187 1.28758 2.6551 5.01 No
Difference
110 CTR 3 Rating 2 vs CTR 1 Rating 4 3.0541 1.22586 2.4914 5.01 No
Difference
111 CTR 3 Rating 2 vs CTR 1 Rating 2 1.9227 1.22586 1.5685 5.01 No
Difference
112 CTR 3 Rating 2 vs CTR 4 Rating 4 1.8890 1.28758 1.4671 5.01 No
Difference
113 CTR 4 Rating 4 vs CTR 3 Rating 5 18.2762 1.28758 14.1942 5.01 Significant
Difference
114 CTR 4 Rating 4 vs CTR 2 Rating 1 17.3298 1.28758 13.4593 5.01 Significant
Difference
115 CTR 4 Rating 4 vs CTR 1 Rating 5 17.0242 1.27254 13.3782 5.01 Significant
Difference
116 CTR 4 Rating 4 vs CTR 4 Rating 1 14.1962 1.33210 10.6570 5.01 Significant
Difference
117 CTR 4 Rating 4 vs CTR 2 Rating 2 10.5891 1.28758 8.2240 5.01 Significant
Difference
118 CTR 4 Rating 4 vs CTR 4 Rating 5 10.1324 1.33210 7.6064 5.01 Significant
Difference
119 CTR 4 Rating 4 vs CTR 1 Rating 1 9.7809 1.27254 7.6861 5.01 Significant
Difference
120 CTR 4 Rating 4 vs CTR 3 Rating 1 9.1197 1.28758 7.0828 5.01 Significant
Difference
121 CTR 4 Rating 4 vs CTR 2 Rating 5 6.7608 1.28758 5.2508 5.01 Significant
Difference
122 CTR 4 Rating 4 vs CTR 4 Rating 2 1.5297 1.33210 1.1483 5.01 No
Difference
123 CTR 4 Rating 4 vs CTR 1 Rating 4 1.1651 1.27254 0.9156 5.01 No
Difference
124 CTR 4 Rating 4 vs CTR 1 Rating 2 0.0337 1.27254 0.0265 5.01 No
Difference
125 CTR 1 Rating 2 vs CTR 3 Rating 5 18.2425 1.22586 14.8814 5.01 Significant
Difference
126 CTR 1 Rating 2 vs CTR 2 Rating 1 17.2961 1.22586 14.1094 5.01 Significant
Difference
127 CTR 1 Rating 2 vs CTR 1 Rating 5 16.9905 1.21005 14.0412 5.01 Significant
Difference
128 CTR 1 Rating 2 vs CTR 4 Rating 1 14.1625 1.27254 11.1293 5.01 Significant
Difference

126
129 CTR 1 Rating 2 vs CTR 2 Rating 2 10.5554 1.22586 8.6106 5.01 Significant
Difference
130 CTR 1 Rating 2 vs CTR 4 Rating 5 10.0987 1.27254 7.9359 5.01 Significant
Difference
131 CTR 1 Rating 2 vs CTR 1 Rating 1 9.7472 1.21005 8.0552 5.01 Significant
Difference
132 CTR 1 Rating 2 vs CTR 3 Rating 1 9.0860 1.22586 7.4120 5.01 Significant
Difference
133 CTR 1 Rating 2 vs CTR 2 Rating 5 6.7271 1.22586 5.4877 5.01 Significant
Difference
134 CTR 1 Rating 2 vs CTR 4 Rating 2 1.4960 1.27254 1.1756 5.01 No
Difference
135 CTR 1 Rating 2 vs CTR 1 Rating 4 1.1314 1.21005 0.9350 5.01 No
Difference
136 CTR 1 Rating 4 vs CTR 3 Rating 5 17.1110 1.22586 13.9584 5.01 Significant
Difference
137 CTR 1 Rating 4 vs CTR 2 Rating 1 16.1647 1.22586 13.1865 5.01 Significant
Difference
138 CTR 1 Rating 4 vs CTR 1 Rating 5 15.8591 1.21005 13.1061 5.01 Significant
Difference
139 CTR 1 Rating 4 vs CTR 4 Rating 1 13.0310 1.27254 10.2402 5.01 Significant
Difference
140 CTR 1 Rating 4 vs CTR 2 Rating 2 9.4239 1.22586 7.6876 5.01 Significant
Difference
141 CTR 1 Rating 4 vs CTR 4 Rating 5 8.9673 1.27254 7.0468 5.01 Significant
Difference
142 CTR 1 Rating 4 vs CTR 1 Rating 1 8.6158 1.21005 7.1201 5.01 Significant
Difference
143 CTR 1 Rating 4 vs CTR 3 Rating 1 7.9546 1.22586 6.4890 5.01 Significant
Difference
144 CTR 1 Rating 4 vs CTR 2 Rating 5 5.5957 1.22586 4.5647 5.01 No
Difference
145 CTR 1 Rating 4 vs CTR 4 Rating 2 0.3645 1.27254 0.2865 5.01 No
Difference
146 CTR 4 Rating 2 vs CTR 3 Rating 5 16.7465 1.28758 13.0062 5.01 Significant
Difference
147 CTR 4 Rating 2 vs CTR 2 Rating 1 15.8002 1.28758 12.2712 5.01 Significant
Difference
148 CTR 4 Rating 2 vs CTR 1 Rating 5 15.4946 1.27254 12.1761 5.01 Significant
Difference

127
149 CTR 4 Rating 2 vs CTR 4 Rating 1 12.6665 1.33210 9.5087 5.01 Significant
Difference
150 CTR 4 Rating 2 vs CTR 2 Rating 2 9.0594 1.28758 7.0360 5.01 Significant
Difference
151 CTR 4 Rating 2 vs CTR 4 Rating 5 8.6028 1.33210 6.4580 5.01 Significant
Difference
152 CTR 4 Rating 2 vs CTR 1 Rating 1 8.2512 1.27254 6.4840 5.01 Significant
Difference
153 CTR 4 Rating 2 vs CTR 3 Rating 1 7.5900 1.28758 5.8948 5.01 Significant
Difference
154 CTR 4 Rating 2 vs CTR 2 Rating 5 5.2311 1.28758 4.0628 5.01 No
Difference
155 CTR 2 Rating 5 vs CTR 3 Rating 5 11.5154 1.24146 9.2757 5.01 Significant
Difference
156 CTR 2 Rating 5 vs CTR 2 Rating 1 10.5690 1.24146 8.5134 5.01 Significant
Difference
157 CTR 2 Rating 5 vs CTR 1 Rating 5 10.2634 1.22586 8.3725 5.01 Significant
Difference
158 CTR 2 Rating 5 vs CTR 4 Rating 1 7.4354 1.28758 5.7747 5.01 Significant
Difference
159 CTR 2 Rating 5 vs CTR 2 Rating 2 3.8282 1.24146 3.0837 5.01 No
Difference
160 CTR 2 Rating 5 vs CTR 4 Rating 5 3.3716 1.28758 2.6186 5.01 No
Difference
161 CTR 2 Rating 5 vs CTR 1 Rating 1 3.0201 1.22586 2.4636 5.01 No
Difference
162 CTR 2 Rating 5 vs CTR 3 Rating 1 2.3589 1.24146 1.9001 5.01 No
Difference
163 CTR 3 Rating 1 vs CTR 3 Rating 5 9.1565 1.24146 7.3756 5.01 Significant
Difference
164 CTR 3 Rating 1 vs CTR 2 Rating 1 8.2101 1.24146 6.6133 5.01 Significant
Difference
165 CTR 3 Rating 1 vs CTR 1 Rating 5 7.9045 1.22586 6.4482 5.01 Significant
Difference
166 CTR 3 Rating 1 vs CTR 4 Rating 1 5.0765 1.28758 3.9426 5.01 No
Difference
167 CTR 3 Rating 1 vs CTR 2 Rating 2 1.4693 1.24146 1.1836 5.01 No
Difference
168 CTR 3 Rating 1 vs CTR 4 Rating 5 1.0127 1.28758 0.7865 5.01 No
Difference

128
169 CTR 3 Rating 1 vs CTR 1 Rating 1 0.6612 1.22586 0.5394 5.01 No
Difference
170 CTR 1 Rating 1 vs CTR 3 Rating 5 8.4953 1.22586 6.9301 5.01 Significant
Difference
171 CTR 1 Rating 1 vs CTR 2 Rating 1 7.5490 1.22586 6.1581 5.01 Significant
Difference
172 CTR 1 Rating 1 vs CTR 1 Rating 5 7.2434 1.21005 5.9860 5.01 Significant
Difference
173 CTR 1 Rating 1 vs CTR 4 Rating 1 4.4153 1.27254 3.4697 5.01 No
Difference
174 CTR 1 Rating 1 vs CTR 2 Rating 2 0.8082 1.22586 0.6593 5.01 No
Difference
175 CTR 1 Rating 1 vs CTR 4 Rating 5 0.3515 1.27254 0.2763 5.01 No
Difference
176 CTR 4 Rating 5 vs CTR 3 Rating 5 8.1437 1.28758 6.3249 5.01 Significant
Difference
177 CTR 4 Rating 5 vs CTR 2 Rating 1 7.1974 1.28758 5.5899 5.01 Significant
Difference
178 CTR 4 Rating 5 vs CTR 1 Rating 5 6.8918 1.27254 5.4158 5.01 Significant
Difference
179 CTR 4 Rating 5 vs CTR 4 Rating 1 4.0637 1.33210 3.0506 5.01 No
Difference
180 CTR 4 Rating 5 vs CTR 2 Rating 2 0.4566 1.28758 0.3546 5.01 No
Difference
181 CTR 2 Rating 2 vs CTR 3 Rating 5 7.6871 1.24146 6.1920 5.01 Significant
Difference
182 CTR 2 Rating 2 vs CTR 2 Rating 1 6.7408 1.24146 5.4297 5.01 Significant
Difference
183 CTR 2 Rating 2 vs CTR 1 Rating 5 6.4352 1.22586 5.2495 5.01 Significant
Difference
184 CTR 2 Rating 2 vs CTR 4 Rating 1 3.6071 1.28758 2.8015 5.01 No
Difference
185 CTR 4 Rating 1 vs CTR 3 Rating 5 4.0800 1.28758 3.1687 5.01 No
Difference
186 CTR 4 Rating 1 vs CTR 2 Rating 1 3.1337 1.28758 2.4338 5.01 No
Difference
187 CTR 4 Rating 1 vs CTR 1 Rating 5 2.8281 1.27254 2.2224 5.01 No
Difference
188 CTR 1 Rating 5 vs CTR 3 Rating 5 1.2519 1.22586 1.0213 5.01 No
Difference

129
189 CTR 1 Rating 5 vs CTR 2 Rating 1 0.3056 1.22586 0.2493 5.01 No
Difference
190 CTR 2 Rating 1 vs CTR 3 Rating 5 0.9463 1.24146 0.7623 5.01 No
Difference
Reference: Biostatistical Analysis, 4th Edition, Jerrold Zar, 1999, p564.