Embed Size (px)
DESCRIPTION
Chen xin M.D., Pulmonary Medicine zhujiang hospital, southern medical university. C hronic O bstructive P ulmonary D isease. Introduction. - PowerPoint PPT Presentation
Citation preview

Chronic Obstructive
Pulmonary Disease
Chronic Obstructive
Pulmonary Disease
Chen xin M.D., Pulmonary Medicine
zhujiang hospital, southern medical university
Chen xin M.D., Pulmonary Medicine
zhujiang hospital, southern medical university

IntroductionIntroduction
• Chronic Obstructive Pulmonary Disease (COPD) is a major cause of chronic morbidity and mortality throughout the world. Many people suffer from this disease for years and die prematurely from it or its complications. COPD is the fourth leading cause of death in the world, and further increases in its prevalence and mortality can be predicted in the coming decades.
• Chronic Obstructive Pulmonary Disease (COPD) is a major cause of chronic morbidity and mortality throughout the world. Many people suffer from this disease for years and die prematurely from it or its complications. COPD is the fourth leading cause of death in the world, and further increases in its prevalence and mortality can be predicted in the coming decades.

DefinitionDefinition
• COPD is a preventable and treatable disease with some significant extrapulmonary effects that may contribute to the severity in individual patients.
• Its pulmonary component is characterized by airflow limitation that is not fully reversible.
• The airflow limitation is usually progressive and associated with the chronic inflammatory response of the lung to noxious particles or gases.
• acute exacerbations and It's complications influence the severity of the disease
• COPD is a preventable and treatable disease with some significant extrapulmonary effects that may contribute to the severity in individual patients.
• Its pulmonary component is characterized by airflow limitation that is not fully reversible.
• The airflow limitation is usually progressive and associated with the chronic inflammatory response of the lung to noxious particles or gases.
• acute exacerbations and It's complications influence the severity of the disease

DefinitionDefinition
• Airflow limitation• Not completely reversible• Progressive• Inflammation• “Bronchitis” & “Emphysema” no longer
in definition• The most common form of COPD is a
combination of chronic bronchitis and emphysema.
• Airflow limitation• Not completely reversible• Progressive• Inflammation• “Bronchitis” & “Emphysema” no longer
in definition• The most common form of COPD is a
combination of chronic bronchitis and emphysema.

Burden of COPDBurden of COPD
• COPD is a leading cause of morbidity and mortality worldwide and results in an economic and social burden that is both substantial and increasing.
• COPD prevalence, morbidity, and mortality vary across countries and across different groups within countries.
• The burden of COPD is projected to increase in the coming decades due to continued exposure to COPD risk factors and the changing age structure of the world’s population.
• COPD is a leading cause of morbidity and mortality worldwide and results in an economic and social burden that is both substantial and increasing.
• COPD prevalence, morbidity, and mortality vary across countries and across different groups within countries.
• The burden of COPD is projected to increase in the coming decades due to continued exposure to COPD risk factors and the changing age structure of the world’s population.

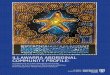
Percent Change in Age-Adjusted Death Rates, U.S.,
1965-1998
Percent Change in Age-Adjusted Death Rates, U.S.,
1965-1998
00
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
3.03.0
Proportion of 1965 Rate Proportion of 1965 Rate
–59%–59% –64%–64% –35%–35% +163%+163% –7%–7%
CoronaryHeart
Disease
CoronaryHeart
Disease
StrokeStroke Other CVDOther CVD COPDCOPD All OtherCauses
All OtherCauses

Of the six leading causes of death in the United States, only COPD has been increasing steadily since 1970
Source: Jemal A. et al. JAMA 2005

Disease Trajectory of a Patients with COPD
Disease Trajectory of a Patients with COPD
Symptoms
Exacerbations
Exacerbations
ExacerbationsDeterioration
End of Life

Risk FactorsRisk Factors
GenesExposure to particles• Tobacco smoke• Occupational dusts,
organic and inorganic• Indoor air pollution from
heating and cooking with biomass in poorly ventilated dwellings
• Outdoor air pollution
GenesExposure to particles• Tobacco smoke• Occupational dusts,
organic and inorganic• Indoor air pollution from
heating and cooking with biomass in poorly ventilated dwellings
• Outdoor air pollution
Lung growth and development
Oxidative stress
Gender
Age
Respiratory infections
Socioeconomic status
Nutrition
Comorbidities
Lung growth and development
Oxidative stress
Gender
Age
Respiratory infections
Socioeconomic status
Nutrition
Comorbidities

Risk FactorsRisk Factors
NutritionNutrition
InfectionsInfections
Socio-economic Socio-economic statusstatus
Aging PopulationsAging Populations

Pathology Pathology
• Pathological changes characteristic of COPD are found in the proximal airways, peripheral airways, lung parenchyma, and pulmonary vasculature. These changes include chronic inflammation, and structural changes resulting from repeated injury and repair.
• Inhaled cigarette smoke and other noxious particles cause lung inflammation, a normal response which appears to be amplified in patients who develop COPD.
• Pathological changes characteristic of COPD are found in the proximal airways, peripheral airways, lung parenchyma, and pulmonary vasculature. These changes include chronic inflammation, and structural changes resulting from repeated injury and repair.
• Inhaled cigarette smoke and other noxious particles cause lung inflammation, a normal response which appears to be amplified in patients who develop COPD.

• Lung inflammation is further amplified by oxidative stress and an excess of proteases in the lung.
• Lung inflammation is further amplified by oxidative stress and an excess of proteases in the lung.

LUNG INFLAMMATIONLUNG INFLAMMATION
COPD PATHOLOGYCOPD PATHOLOGY
OxidativeOxidativestressstress ProteinasesProteinases
Repair Repair mechanismsmechanisms
Anti-proteinasesAnti-proteinasesAnti-oxidantsAnti-oxidants
Host factorsAmplifying mechanisms
Cigarette smokeCigarette smokeBiomass particlesBiomass particles
ParticulatesParticulates
Source: Peter J. Barnes, MD
Pathogenesis of COPD

Cigarette smoke Cigarette smoke (and other irritants)(and other irritants)
PROTEASES PROTEASES Neutrophil elastaseNeutrophil elastaseCathepsinsCathepsinsMMPsMMPs
Alveolar wall destructionAlveolar wall destruction(Emphysema)(Emphysema)
Mucus hypersecretionMucus hypersecretion
CD8CD8+ +
lymphocytelymphocyte
Alveolar Alveolar macrophagemacrophage
EpithelialEpithelialcellscells
FibrosisFibrosis(Obstructive(Obstructivebronchiolitis)bronchiolitis)
FibroblastFibroblast
MonocyteMonocyteNeutrophilNeutrophil
Chemotactic factorsChemotactic factors
Inflammatory Cells Involved in COPD
Source: Peter J. Barnes, MD

Anti-proteases
SLPI 1-AT
Proteolysis
OO22--, H, H220022
OHOH.., ONOO, ONOO--
Mucus secretion
Plasma leak Bronchoconstriction
NF-NF-BB
IL-8IL-8
NeutrophilNeutrophilrecruitmentrecruitment
TNF-TNF-
IsoprostanesIsoprostanes
↓ ↓ HDAC2HDAC2
↑↑InflammationInflammationSteroidSteroid
resistanceresistance
Macrophage NeutrophilOxidative Stress in COPD
Source: Peter J. Barnes, MD

Mucus gland hyperplasia
Goblet cellhyperplasia
Mucus hypersecretion Neutrophils in sputum
Squamous metaplasia of epithelium
↑ Macrophages
No basement membrane thickening
Little increase in airway smooth muscle
↑ CD8+ lymphocytes
Changes in Large Airways of COPD Patients
Changes in Large Airways of COPD Patients
Source: Peter J. Barnes, MD

Disrupted alveolar attachments
Inflammatory exudate in lumen
Peribronchial fibrosisLymphoid follicle
Thickened wall with inflammatory cells- macrophages, CD8+ cells, fibroblasts
Changes in Small Airways in COPD Patients
Source: Peter J. Barnes, MD

Alveolar wall destruction
Loss of elasticity
Destruction of pulmonarycapillary bed
↑ Inflammatory cells macrophages, CD8+ lymphocytes
Source: Peter J. Barnes, MD
Changes in Lung Parenchyma in COPD

Endothelial dysfunction
Intimal hyperplasia
Smooth muscle hyperplasia
↑ Inflammatory cells (macrophages, CD8+ lymphocytes)
Changes in Pulmonary Arteries in COPD Patients
Source: Peter J. Barnes, MD

YYYYYY
Mast cellMast cell
CD4+ cellCD4+ cell(Th2)(Th2)
EosinophilEosinophil
AllergensAllergens
Ep cellsEp cells
ASTHMAASTHMA
BronchoconstrictionBronchoconstrictionAHRAHR
Alv macrophageAlv macrophage Ep cellsEp cells
CD8+ cellCD8+ cell(Tc1)(Tc1)
NeutrophilNeutrophil
Cigarette smokeCigarette smoke
Small airway narrowingSmall airway narrowingAlveolar destructionAlveolar destruction
COPDCOPD
Reversible IrreversibleAirflow LimitationAirflow Limitation
Source: Peter J. Barnes, MD

Chronic hypoxiaChronic hypoxia
Pulmonary vasoconstrictionPulmonary vasoconstriction
MuscularizationMuscularization
Intimal Intimal hyperplasiahyperplasia
FibrosisFibrosis
ObliterationObliteration
Pulmonary hypertensionPulmonary hypertension
Cor pulmonaleCor pulmonale
Death
EdemaEdema
Pulmonary Hypertension in COPD
Source: Peter J. Barnes, MD

NormalNormalInspiration
Expiration
alveolar attachments
Mild/moderateMild/moderateCOPD COPD
loss of elasticity
Severe Severe COPD COPD
loss of alveolar attachments
closure
small small airwayairway
Dyspnea↓ Exercise capacity
Air trappingAir trappingHyperinflationHyperinflation
↓ ↓ HealthHealthstatusstatus
Air Trapping in COPD
Source: Peter J. Barnes, MD

Macrophages
TNF- IL-8 IL-6
Bacteria Viruses Non-infective Pollutants
Epithelial cells
Oxidative stressOxidative stress
Neutrophils
Inflammation in COPD Exacerbations
Source: Peter J. Barnes, MD

Chronic bronchitisChronic bronchitis
• Chronic bronchitis is an inflammation and eventual scarring of the lining of the bronchial tubes.
• Symptoms of chronic bronchitis include chronic cough, increased mucus, frequent clearing of the throat and shortness of breath.
• Chronic bronchitis is an inflammation and eventual scarring of the lining of the bronchial tubes.
• Symptoms of chronic bronchitis include chronic cough, increased mucus, frequent clearing of the throat and shortness of breath.

EmphysemaEmphysema
Emphysema causes irreversible lung damage. The walls between the air sacs within the lungs lose their ability to stretch and recoil. They become weakened and break. Elasticity of the lung tissue is lost, causing air to be trapped in the air sacs and impairing the exchange of oxygen and carbon dioxide. Also, the support of the airways is lost, allowing for obstruction of airflow.
Emphysema causes irreversible lung damage. The walls between the air sacs within the lungs lose their ability to stretch and recoil. They become weakened and break. Elasticity of the lung tissue is lost, causing air to be trapped in the air sacs and impairing the exchange of oxygen and carbon dioxide. Also, the support of the airways is lost, allowing for obstruction of airflow.

EmphysemaEmphysema
• Symptoms of emphysema include cough, shortness of breath and a limited excercise tolerance. Diagnosis is made by pulmonary function tests, along with the patient’s history, examination and other tests.
• Symptoms of emphysema include cough, shortness of breath and a limited excercise tolerance. Diagnosis is made by pulmonary function tests, along with the patient’s history, examination and other tests.


COPD 病理学特点COPD 病理学特点
气道炎症
粘膜纤毛功能障碍
气道阻塞
气道结构改变
平滑肌收缩增加胆碱能释放 支气管高反应性 ?
弹性收缩降低
增加炎症细胞数量 / 活性- 中性粒细胞 ,- 巨噬细胞 ,- CD8+ 淋巴细胞提高 IL-8, TNF, LTB4
蛋白酶 / 抗蛋白酶失衡粘膜水肿
肺泡破坏上皮增生 腺体过度增大杯状细胞变形气道纤维化
粘液过度分泌粘液粘性增加减少纤毛转运粘膜损伤

PathophysiologyPathophysiology
• Increased mucus production and reduced mucociliary clearance - cough and sputum production
• Loss of elastic recoil - airway collapse
• Increase smooth muscle tone• Pulmonary hyperinflation• Gas exchange abnormalities -
hypoxemia and/or hypercapnia
• Increased mucus production and reduced mucociliary clearance - cough and sputum production
• Loss of elastic recoil - airway collapse
• Increase smooth muscle tone• Pulmonary hyperinflation• Gas exchange abnormalities -
hypoxemia and/or hypercapnia

Chronic bronchitis Emphysema
asthma
COPDCOPD


GOALS of COPD MANAGEMENTUPDATED 2011
GOALS of COPD MANAGEMENTUPDATED 2011
• Relieve symptoms • Prevent disease progression• Improve exercise tolerance• Improve health status• Prevent and treat complications• Prevent and treat exacerbations• Reduce mortality
• Relieve symptoms • Prevent disease progression• Improve exercise tolerance• Improve health status• Prevent and treat complications• Prevent and treat exacerbations• Reduce mortality

Four Components of COPD Management
Four Components of COPD Management
1. Assess and monitor disease 2. Reduce risk factors3. Manage stable COPD
I. EducationII. Pharmacologic/Non-
pharmacologic
4. Manage exacerbationsI. Diagnosis and Assessment of
SeverityII. Home/Hospital Management
1. Assess and monitor disease 2. Reduce risk factors3. Manage stable COPD
I. EducationII. Pharmacologic/Non-
pharmacologic
4. Manage exacerbationsI. Diagnosis and Assessment of
SeverityII. Home/Hospital Management

Assess and Monitor COPD: Key Points
Assess and Monitor COPD: Key Points
•A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease.•The diagnosis should be confirmed by spirometry. A post-bronchodilator FEV1/FVC < 0.70 confirms the presence of airflow limitation that is not fully reversible.•Comorbidities are common in COPD and should be actively identified.
•A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease.•The diagnosis should be confirmed by spirometry. A post-bronchodilator FEV1/FVC < 0.70 confirms the presence of airflow limitation that is not fully reversible.•Comorbidities are common in COPD and should be actively identified.

Diagnosis of COPDDiagnosis of COPD
SYMPTOMScoughcoughsputumsputum
shortness of breathshortness of breath
EXPOSURE TO RISKFACTORS tobaccotobacco
occupationoccupationindoor/outdoor pollutionindoor/outdoor pollution
clinical diagnosisclinical diagnosis
è
SPIROMETRY
diagnosis

Key Indicators for COPD Diagnosis
Key Indicators for COPD Diagnosis
Chronic cough Present intermittently or every day often present throughout the day; seldom only nocturnal
Chronic sputum production Present for many years, worst in winters. Initially mucoid – becomes purulent with exacerbation
Dyspnoea that is Progressive (worsens over time)Persistent (present every day)Worse on exerciseWorse during respiratory infections
Acute bronchitis Repeated episodes
History of exposure to risk factors Tobacco smoke (including beedi) occupational dusts and chemical smoke from home cooking and heating fuel

Physical signsPhysical signs
• Large barrel shaped chest (hyperinflation)
• Prominent accessory respiratory muscles in neck and use of accessory muscle in respiration
• Low, flat diaphragm• Diminished breath
sound
• Large barrel shaped chest (hyperinflation)
• Prominent accessory respiratory muscles in neck and use of accessory muscle in respiration
• Low, flat diaphragm• Diminished breath
sound

SpirometrySpirometry
• Diagnosis
• Assessing severity
• Assessing
prognosis
• Monitoring
progression
• Diagnosis
• Assessing severity
• Assessing
prognosis
• Monitoring
progression

SpirometrySpirometry
• FEV1 – Forced expired volume in the first second
• FVC – Total volume of air that can be exhaled from maximal inhalation to maximal exhalation
• FEV1/FVC% - The ratio of FEV1 to FVC, expressed as a percentage.
• FEV1 – Forced expired volume in the first second
• FVC – Total volume of air that can be exhaled from maximal inhalation to maximal exhalation
• FEV1/FVC% - The ratio of FEV1 to FVC, expressed as a percentage.

Flow Normal obstruction
restrictions Mixed
RVTLCVolum
Flow-volume curveFlow-volume curve

Chest X-raysChest X-rays
Emphysema Hyperinflation Flattened
diaphragms Decreased
vascular markings
Chronic Bronchitis Usually normal
Emphysema Hyperinflation Flattened
diaphragms Decreased
vascular markings
Chronic Bronchitis Usually normal

Flatdiaphragm
IncreasedRetrosternal
air
Hyper-inflated
Chest X-raysChest X-rays

Assess and Monitor COPD:
Spirometry GOLD 2006
Assess and Monitor COPD:
Spirometry GOLD 2006
• Spirometry should be performed after the administration of an adequate dose of a short-acting inhaled bronchodilator to minimize variability.
• A post-bronchodilator FEV1/FVC < 0.70 confirms the presence of airflow limitation that is not fully reversible.
• Where possible, values should be compared to age-related normal values to avoid overdiagnosis of COPD in the elderly.
• Spirometry should be performed after the administration of an adequate dose of a short-acting inhaled bronchodilator to minimize variability.
• A post-bronchodilator FEV1/FVC < 0.70 confirms the presence of airflow limitation that is not fully reversible.
• Where possible, values should be compared to age-related normal values to avoid overdiagnosis of COPD in the elderly.

COPD classification based on spirometry GOLD 2006
COPD classification based on spirometry GOLD 2006
Severity Postbronchodilator FEV1/FVC
Postbronchodilator FEV1% predicted
Mild COPD <0.7 >80
Moderate COPD
<0.7 50-80
Severe COPD <0.7 30-50
Very severe COPD
<0.7 <30
SPIROMETRY is not to substitute for clinical judgment in the evaluation of the severity of
disease in individual patients.

Assess and Monitor COPD:
GOLD 2011
Assess and Monitor COPD:
GOLD 2011
• Clinical symptoms • Spirometry• risk of acute exacerbations • complications
Global strategy for the diagnosis, management, and prevention of chronic
obstructive pulmonary disease Revised 2011
• Clinical symptoms • Spirometry• risk of acute exacerbations • complications
Global strategy for the diagnosis, management, and prevention of chronic
obstructive pulmonary disease Revised 2011

Assess and Monitor COPD: Clinical symptoms
Assess and Monitor COPD: Clinical symptoms
• COPD assessment test (CAT) including eight common clinical problem, to
evaluate the health damage of patients with COPD
• modified british medical research council (mMRC)
Having a good correlation with health condition and can predict the future risk of death
• COPD assessment test (CAT) including eight common clinical problem, to
evaluate the health damage of patients with COPD
• modified british medical research council (mMRC)
Having a good correlation with health condition and can predict the future risk of death

mMRC
CAT
mMRC
CAT

Assess and Monitor COPD: risk of acute exacerbations
Assess and Monitor COPD: risk of acute exacerbations
History of acute exacerbations : the number of acute exacerbations is more than 2
times in the last year
Spirometry: FEV1 < 50 % Pred as a high risk index
History of acute exacerbations : the number of acute exacerbations is more than 2
times in the last year
Spirometry: FEV1 < 50 % Pred as a high risk index

Comprehensive Assessment
Comprehensive Assessment
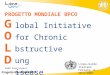
Risk 4 Risk(GOLD) 3 ≥ 2 (AE) 2 1 1 0 mMRC 0-1 mMRC 2+ CAT< 10 CAT> 10+
symptoms ( mMRC or CAT )
Risk 4 Risk(GOLD) 3 ≥ 2 (AE) 2 1 1 0 mMRC 0-1 mMRC 2+ CAT< 10 CAT> 10+
symptoms ( mMRC or CAT )
C D
A BA:Fewer symptoms, lower risk B: more symptoms, lower riskC: Fewer symptoms,higher riskD: more symptoms, higher risk

Arterial Blood Gas (ABGs)Arterial Blood Gas (ABGs)
• An ABG is done from a sample drawn from one of your arteries. The blood is then analyzed by a special machine, which records the amount of carbon dioxide (waste gas) and oxygen in your blood. One of the uses of this test is to determine whether or not you need any extra oxygen.
• An ABG is done from a sample drawn from one of your arteries. The blood is then analyzed by a special machine, which records the amount of carbon dioxide (waste gas) and oxygen in your blood. One of the uses of this test is to determine whether or not you need any extra oxygen.

Parameters and Predictions
Parameters and Predictions
Parameter Normal Values
Predictions
Arterial PO2 95 mmHg decrease
Arterial PCO2 40 mmHg increases
Aterial pH approx. 7.4 decreases
Arterial HCO3-content
22-26 mEq/L increases
Total Arterial O2 content
20 ml/dL decrease

Differential Diagnosis: Differential Diagnosis: COPD and AsthmaCOPD and Asthma
Differential Diagnosis: Differential Diagnosis: COPD and AsthmaCOPD and Asthma
COPD ASTHMA
Onset in mid-life
Symptoms slowly progressive
Long smoking history
Dyspnea during exercise
Largely irreversible airflow limitation
Onset early in life (often childhood)
Symptoms vary from day to day
Symptoms at night/early morning
Allergy, rhinitis, and/or eczema also present
Family history of asthma
Largely reversible airflow limitation

COPD and Co-Morbidities
COPD and Co-Morbidities
COPD patients are at increased risk for: • Myocardial infarction, angina
• Osteoporosis
• Respiratory infection
• Depression
• Diabetes
• Lung cancer
COPD patients are at increased risk for: • Myocardial infarction, angina
• Osteoporosis
• Respiratory infection
• Depression
• Diabetes
• Lung cancer

COPD and Co-Morbidities
COPD and Co-Morbidities
COPD has significant extrapulmonary
(systemic) effects including:
• Weight loss
• Nutritional abnormalities
• Skeletal muscle dysfunction
COPD has significant extrapulmonary
(systemic) effects including:
• Weight loss
• Nutritional abnormalities
• Skeletal muscle dysfunction

Management of Stable COPD
Reduce Risk Factors: Key Points
Management of Stable COPD
Reduce Risk Factors: Key Points
• Reduction of total personal exposure to tobacco smoke, occupational dusts and chemicals, and indoor and outdoor air pollutants are important goals to prevent the onset and progression of COPD.
• Smoking cessation is the single most effective — and cost effective — intervention in most people to reduce the risk of developing COPD and stop its progression.
• Reduction of total personal exposure to tobacco smoke, occupational dusts and chemicals, and indoor and outdoor air pollutants are important goals to prevent the onset and progression of COPD.
• Smoking cessation is the single most effective — and cost effective — intervention in most people to reduce the risk of developing COPD and stop its progression.

• Reducing the risk from indoor and outdoor air pollution is feasible and requires a combination of public policy and protective steps taken by individual patients.
• Reduction of exposure to smoke from biomass fuel, particularly among women and children, is a crucial goal to reduce the prevalence of COPD worldwide.
• Reducing the risk from indoor and outdoor air pollution is feasible and requires a combination of public policy and protective steps taken by individual patients.
• Reduction of exposure to smoke from biomass fuel, particularly among women and children, is a crucial goal to reduce the prevalence of COPD worldwide.

Management of Stable COPD
Manage Stable COPD: Key Points
Management of Stable COPD
Manage Stable COPD: Key Points
• Bronchodilator medications are central to the symptomatic management of COPD. They are given on an as-needed basis or on a regular basis to prevent or reduce symptoms and exacerbations.
• The principal bronchodilator treatments are ß2-agonists, anticholinergics, and methylxanthines used singly or in combination.
• Regular treatment with long-acting bronchodilators is more effective and convenient than treatment with short-acting bronchodilators.
• Bronchodilator medications are central to the symptomatic management of COPD. They are given on an as-needed basis or on a regular basis to prevent or reduce symptoms and exacerbations.
• The principal bronchodilator treatments are ß2-agonists, anticholinergics, and methylxanthines used singly or in combination.
• Regular treatment with long-acting bronchodilators is more effective and convenient than treatment with short-acting bronchodilators.

Management of Stable COPDPharmacotherapy: Bronchodilators
Management of Stable COPDPharmacotherapy: Bronchodilators
• Bronchodilator medications are central to the symptomatic management of COPD .They are given on an as-needed basis or on a regular basis to prevent or reduce symptoms and exacerbations.
• The principal bronchodilator treatments are ß2-agonists, anticholinergics, and methylxanthines used singly or in combination.
• Regular treatment with long-acting bronchodilators is more effective and convenient than treatment with short-acting bronchodilators.
• Bronchodilator medications are central to the symptomatic management of COPD .They are given on an as-needed basis or on a regular basis to prevent or reduce symptoms and exacerbations.
• The principal bronchodilator treatments are ß2-agonists, anticholinergics, and methylxanthines used singly or in combination.
• Regular treatment with long-acting bronchodilators is more effective and convenient than treatment with short-acting bronchodilators.


Algorithm for the management of COPD
Algorithm for the management of COPD
Short acting bronchodilator – as required
Tiotropium
Tiotropium+LABA
Long acting beta agonist
LABA + tiotropium
Add-Inhaled steroids-Theophylline
Mild
Severe
ass
ess
wit
h s
ym
pto
ms
and
spir
om
etr
y

Management of Stable COPD
Pharmacotherapy: Glucocorticosteroids
The addition of regular treatment with inhaled
glucocorticosteroids to bronchodilator treatment is appropriate for symptomatic COPD patients with an FEV1 < 50% predicted (Stage III: Severe COPD and Stage IV: Very Severe COPD) and repeated exacerbations.
An inhaled glucocorticosteroid combined with a long-acting ß2-agonist is more effective than the individual components .

Pharmacotherapy for Stable COPD
Pharmacotherapy for Stable COPD
Bronchodilators• Short-acting 2-
agonist – Salbutamol
• Long-acting 2-agonist - Salmeterol and Formoterol
• Anticholinergics – Ipratropium, Tiiotropium
• Methylxanthines - Theophylline
Bronchodilators• Short-acting 2-
agonist – Salbutamol
• Long-acting 2-agonist - Salmeterol and Formoterol
• Anticholinergics – Ipratropium, Tiiotropium
• Methylxanthines - Theophylline
Steroids
• Oral – Prednisolone
• Inhaled - Fluticasone, Budesonide
Steroids
• Oral – Prednisolone
• Inhaled - Fluticasone, Budesonide

Management of Stable COPD
Pharmacotherapy: Vaccines
In COPD patients influenza vaccines can reduce serious illness.
Pneumococcal polysaccharide vaccine is recommended for COPD patients 65 years and older and for COPD patients younger than age 65 with an FEV1 < 40% predicted.

Management of Stable COPD All Stages of Disease SeverityAll Stages of Disease SeverityManagement of Stable COPD All Stages of Disease SeverityAll Stages of Disease Severity
• Avoidance of risk factorsAvoidance of risk factors• - smoking cessation- smoking cessation• - reduction of indoor pollution- reduction of indoor pollution• - reduction of occupational - reduction of occupational
exposureexposure• Influenza vaccinationInfluenza vaccination
• Avoidance of risk factorsAvoidance of risk factors• - smoking cessation- smoking cessation• - reduction of indoor pollution- reduction of indoor pollution• - reduction of occupational - reduction of occupational
exposureexposure• Influenza vaccinationInfluenza vaccination

IV: Very Severe III: Severe II: Moderate I: Mild
Therapy at Each Stage of COPD (GOLD2006)
FEV1/FVC < 70%
FEV1 > 80% predicted
FEV1/FVC < 70%
50% < FEV1 < 80% predicted
FEV1/FVC < 70%
30% < FEV1 < 50% predicted
FEV1/FVC < 70%
FEV1 < 30% predicted
or FEV1 < 50% predicted plus chronic respiratory failure
Add regular treatment with one or more long-acting bronchodilators (when needed); Add rehabilitation
Add inhaled glucocorticosteroids if repeated exacerbations
Active reduction of risk factor(s); influenza vaccinationAdd short-acting bronchodilator (when needed)
Add long term oxygen if chronic respiratory failure. Consider surgical treatments

Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease
Revised 2011 Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease
Revised 2011
P First chonice
Second chonice Alternative chonice
A SABA /SAMA prn
LAMA/LABA orSAMA & SABA
Theophylline
B LABA / LAMA LAMA & LABA SABA & /orSAMA ; Theophylline
C ICS/LABA or LAMA
LAMA & LABA PDE-4 inhibitors ; SABA & /orSAMA ; Theophylline
D ICS/LABA or LAMA
ICS & LAMA ICS/LABA & LAMA ; ICS/LABA & PDE-4 inhibitors LAMA & LABA ; LAMA & PDE-4 inhibitors
Carbocisteine ; SABA & /orSAMA ; Theophylline
Therapy at Each Stage of COPD (GOLD2011)
Therapy at Each Stage of COPD (GOLD2011)

The Future of COPD :Phenotypes
The Future of COPD :Phenotypes
• Clinical Manifestations Age, smoking history, sex,
ethnicity
• Physiological Manifestations• Radiologic Characterization• frequent COPD Exacerbations• Systemic Inflammation
• Clinical Manifestations Age, smoking history, sex,
ethnicity
• Physiological Manifestations• Radiologic Characterization• frequent COPD Exacerbations• Systemic Inflammation

68
Management of Stable COPD
Other Pharmacologic Treatments
Antibiotics: Only used to treat infectious exacerbations of COPD
Antioxidant agents: No effect of n-acetylcysteine on frequency of exacerbations, except in patients not treated with inhaled glucocorticosteroids
Mucolytic agents, Antitussives, Vasodilators: Not recommended in stable COPD

69
Management of Stable COPD
Non-Pharmacologic Treatments
Rehabilitation: All COPD patients benefit from exercise training programs, improving with respect to both exercise tolerance and symptoms of dyspnea and fatigue.
Oxygen Therapy: The long-term administration of oxygen (> 15 hours per day) to patients with chronic respiratory failure has been shown to increase survival.

70
Management COPD Exacerbations
Key Points
An exacerbation of COPD is defined as:
“An acute event in the course of the disease characterized by a change in the patient’s baseline dyspnea, cough, and/or sputum that is beyond normal day-to-day variations, is acute in onset, and may warrant a change in regular medication in a patient with underlying COPD.”

71
Management COPD Exacerbations
Key Points
The most common causes of an exacerbation are infection of the tracheobronchial tree
and air pollution, but the cause of about one-third of severe exacerbations cannot be identified .
Patients experiencing COPD exacerbations with clinical signs of airway infection (e.g., increased sputum purulence) may benefit from antibiotic treatment .

72
Manage COPD Exacerbations
Key Points
Inhaled bronchodilators
(particularly inhaled ß2-agonists
with or without anticholinergics)
and oral glucocortico- steroids
are effective treatments for
exacerbations of COPD.

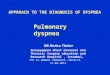
Manage COPD Exacerbation
cause and mechanism Manage COPD Exacerbation
cause and mechanism
Wedzicha JA. Lancet 2007 ; 370 : 786-796 Antonio Anzueto. Proc Am Thorac Soc 2007 ; 4 : 554–564 Wedzicha JA. Lancet 2007 ; 370 : 786-796 Antonio Anzueto. Proc Am Thorac Soc 2007 ; 4 : 554–564
VirusesBacteria
Aerial pollution
COPD airway inflammation is, the more serious, pathological physiology change is, the more evident. leading to a symptom aggravating, so patients much to seek for medical help, usually diagnosed of acute exacerbation
Cardiovascular Co-Morbidities Dynamic hyperinflation
The deterioration of airway inflammation
Symptoms of AECOPD
Expiratory Airflow limitation
Bronchial inflammationHydroncus, mucous
Systemic inflammation
COPD airway inflammation COPD airway inflammation

Management COPD Exacerbations
Key Points
Noninvasive mechanical ventilation in exacerbations improves respiratory acidosis, increases pH, decreases the need for endotracheal intubation, and reduces PaCO2, respiratory rate, severity of breathlessness, the length of hospital stay, and mortality.
Medications and education to help prevent future exacerbations should be considered as part of follow-up, as exacerbations affect the quality of life and prognosis of patients with COPD.

75
Global Strategy for Diagnosis, Management and Prevention of COPD: Summary
COPD is increasing in prevalence in many countries of the world.
COPD is treatable and preventable.
The GOLD program offers a strategy to identify patients and to treat them according to the best medications available.

76
COPD can be prevented by avoidance of risk factors, the most notable being tobacco smoke.
Patients with COPD have multiple other conditions (comorbidities) that must be taken into consideration.
GOLD has developed a global network to raise awareness of COPD and disseminate information on diagnosis and treatment.
Global Strategy for Diagnosis, Management and Prevention of COPD:
Summary