Embed Size (px)
Citation preview
P G S . T S C A O P H I P H O N G
Ca lâm sàng liệt dây 3
2017
Ca 1: Liệt dây 3 toàn bộ, mắt đỏ, sụp mi và đau cấp (Acute Painful Ptosis, Complete Ophthalmoplegia with a Red Eye)
Bệnh sử bn nữ 55t, nhập viện vì đau đầu 4 ngày trước đó,
đau giảm bớt nhưng còn sưng phù mắt phải sau 1 ngày nhập
viện, bn xuất hiện nhìn đôi than tê vùng mặt bên phải
Khám thị lực mắt phải giảm, đồng tử dãn, liệt hoàn toàn dây 3 phải, bn sụp
mi mắt lồi 7mm, có âm thổi mắt phải
Khám mắt bình thường, nhãn áp mắt phải 26mmHg, trái 18mmHg, đáy
mắt bình thường
1. Hướng chẩn đoán?
2. Các xét nghiện cần thiết?
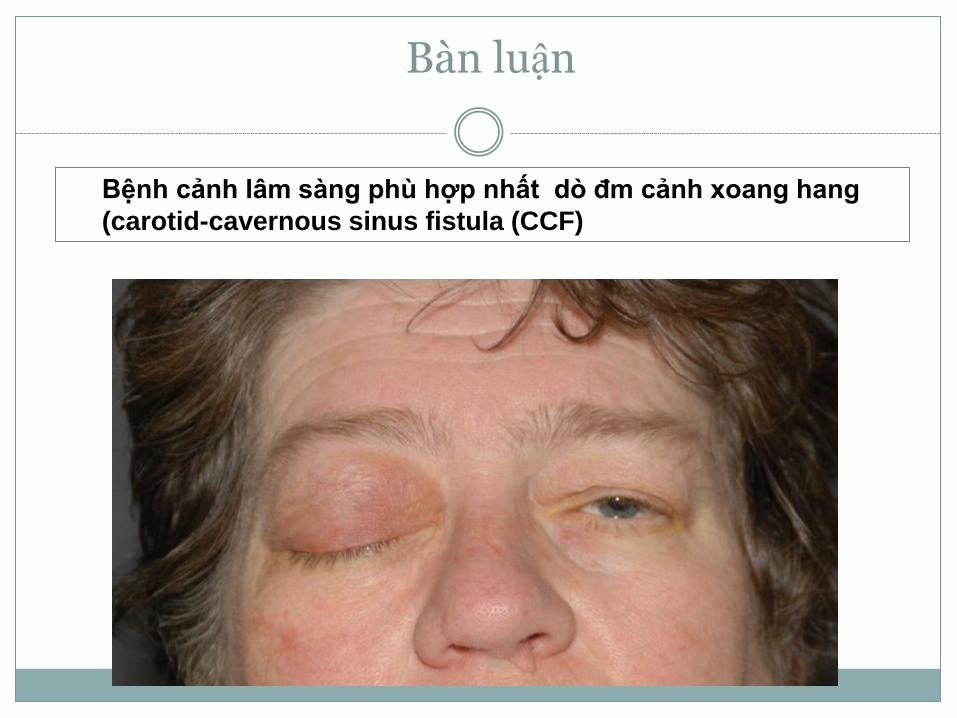
Bàn luận
Bệnh cảnh lâm sàng phù hợp nhất dò đm cảnh xoang hang
(carotid-cavernous sinus fistula (CCF)
CCFs có thể phân loại
1. Căn nguyên
(e.g. traumatic versus spontaneous)
2. Tốc độ dòng máu chảy
(e.g. high versus low flow),
3. Giải phẫu
(e.g. direct versus dural; internal carotid artery versus external
carotid artery supply versus both).
• Trực tiếp CCFs: 70% - 90% tất cả CCFs. Bất cứ tuổi
nào cả nam và nữ
• Trực tiếp CCF do rách thành đm cảnh trong đoạn
xoang hang
• Direct CCFs thường gặp chấn thương đầu
(especially motor vehicle accidents, fights, and falls)
• Tổn thương có thể rất nặng hay chỉ nhẹ (quite trivial).
• Một số ít direct CCFs do vỡ pre-existing aneurysm của
cavernous segment of the internal carotid artery.
• Direct CCFs có thể iatrogenic, xảy ra sau nhiều
diagnostic và therapeutic procedures
(e.g. carotid endarterectomy, cranial and percutaneous retro-
Gasserian procedure for the trigeminal neuralgia, transphenoidal
surgery, or maxillofacial surgeries).

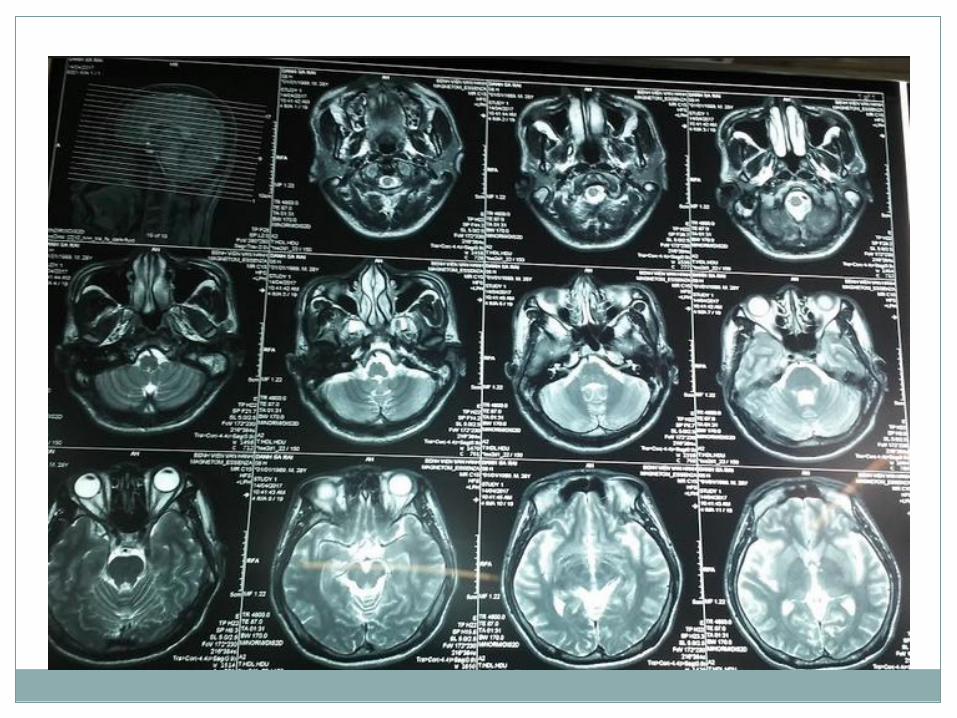
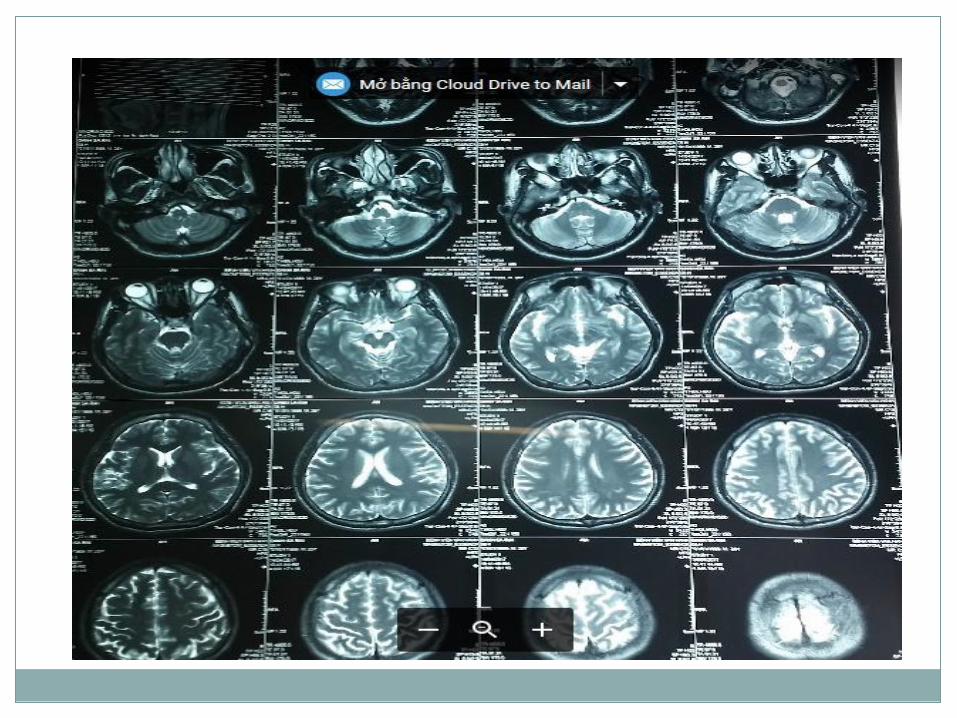
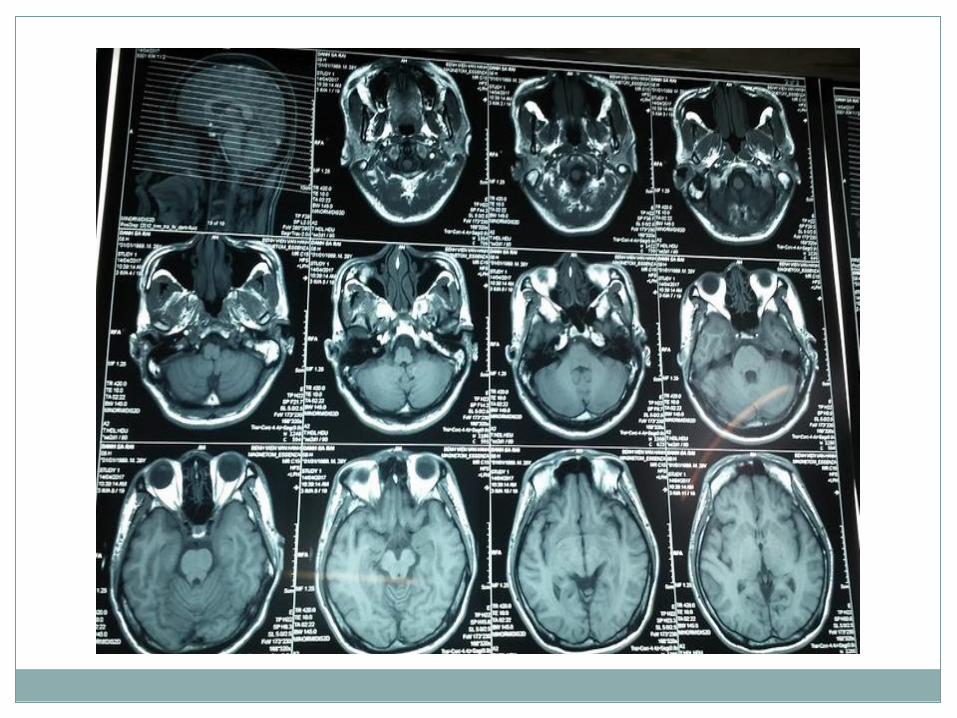
Brain MRI axial T1 without contrast cho thấy right proptosis (small
arrow) và enlarged flow void bên trong right cavernous sinus (large arrow).
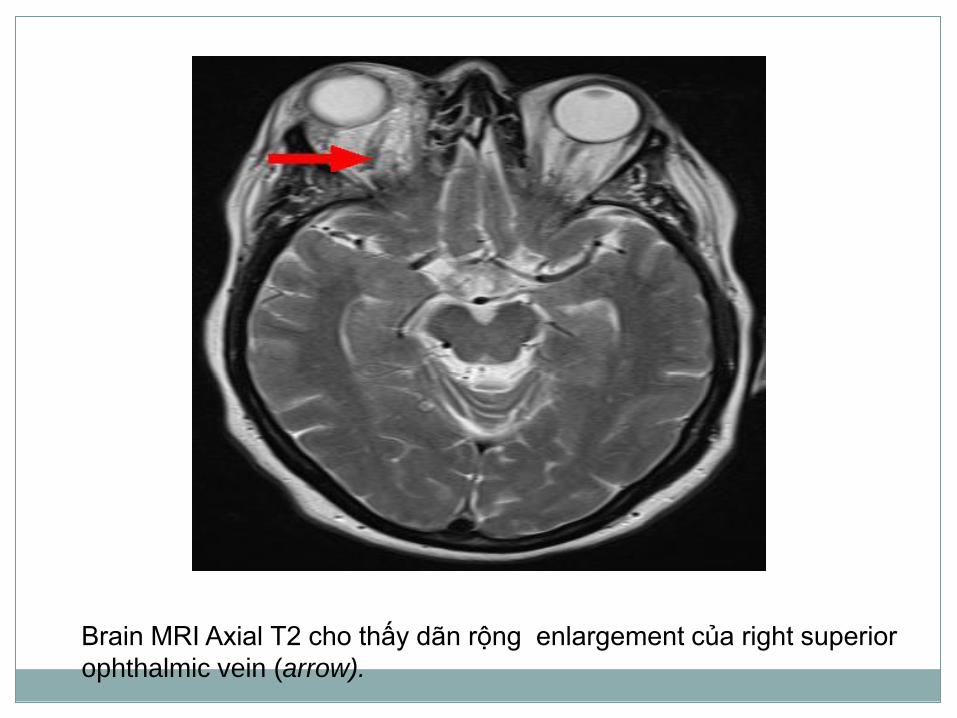
Brain MRI Axial T2 cho thấy dãn rộng enlargement của right superior
ophthalmic vein (arrow).
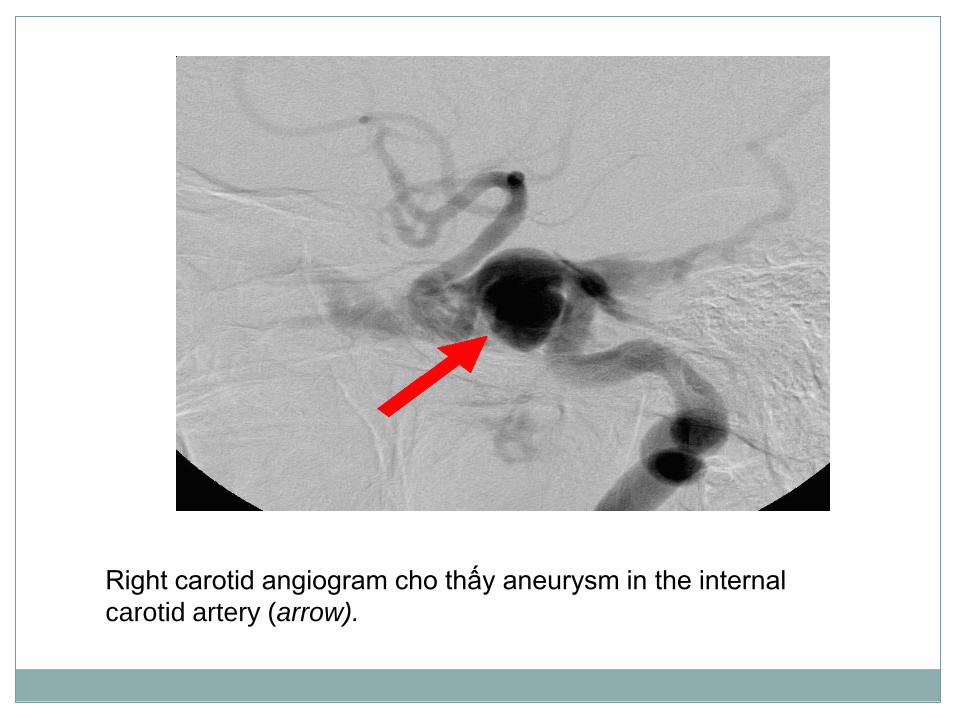
Right carotid angiogram cho thấy aneurysm in the internal
carotid artery (arrow).
• Đôi khi bn than phiền facial pain vùng phân bố dây V1 và
đôi khi dây V2
• Đôi bn giảm corneal sensation, decreased facial
sensation, hay cả 2, liên hệ ischemia hay compression
ophthalmic hay nhánh hàm trên dây V trong xoang hang
(maxillary divisions).
• Glaucoma xảy ra 30% to 50% ca, và hầu hết tăng
intraocular pressure là do increased episcleral venous
pressure hay orbital congestion
1. Direct CCF sẽ nghi ngờ bất cứ bn nào đột ngột
chemosis, proptosis, và red eye.
2. Nếu không có tiền sử chấn thương, có thể xem xét
ruptured cavernous aneurysm
Ca 2: liệt dây 3 toàn bộ, mắt đỏ, sụp mi và không đau mãn tính
(Chronic Painless Ptosis, Complete Ophthalmoplegia with a
Red Eye)
Bn nam 69 tuổi có tiền sử đỏ mắt trái trong 12 tuần trước đó,
bn khám và chẩn đoán viêm kết mạc được điều trị kháng sinh,
kháng histamin và steroid nhưng không khỏi. BN xấu hơn ,
nhìn đôi khi nhìn lên, nghe tiếng gió rít( whooshing ) trong tai.
Bn không tiền sử chấn thương, bướu cổ hay hút thuốc lá.
Thị lực 2 mắt tốt , không RAPD hay anisocoria, bn sụp mi mắt
trái, phù nhẹ mi mắt, tăng nhãn áp mắt trái 28mmHg
1. Chẩn đoán nguyên nhân?
2. Test chẩn đoán?
• Bn chronic “red eye” không đáp ứng nhiều topical
therapies, BS mắt tổng quát phải xem xét danh sách
nguyên nhân gây mắt đỏ khác(typical “red eye” list)
• Trong bn này có triệu chứng (e.g. diplopia, ptosis, and
proptosis), lâm sàng khu trú vấn đề di chuyển từ anterior
segment đến orbit.
• Dấu hiệu lâm sàng để phân biệt ở đây là: “arterialization”
của conjunctival và episcleral vessels, với classic dilated
và tortuous vessels extending to and from the limbus.
• Lâm sàng trên nghĩ đến nhiều nhất CCF.
• Hình ảnh khác biệt direct and high flow versus
indirect and slow flow fistula
• Orbital ultrasound có thể cho thấy dilated superior
ophthalmic vein and arterialization of flow có thể đạt được
qua orbital Doppler flow studies.
• CT scan or MR scan đặc biệt cho thấy dilated superior
ophthalmic vein và có thể enlargement hay flow voids
trong cavernous sinus.
.
Ca lâm sàng
• Cranial MRI/MRA : dilated left superior ophthalmic vein
with arterialized flow.
• Không có clinical or radiographic evidence cortical
venous drainage.
• Bn tếp tục xấu hơn và được thực hiện DSA xác định
indirect CCF với internal carotid artery feeders và tiếp
theo endovascular closure của fistula.
• Subjective bruit hết ngay sau procedure và 2 tháng sau
ptosis, lid edema, proptosis, ophthalmoplegia, và red
eye hoàn toàn hết
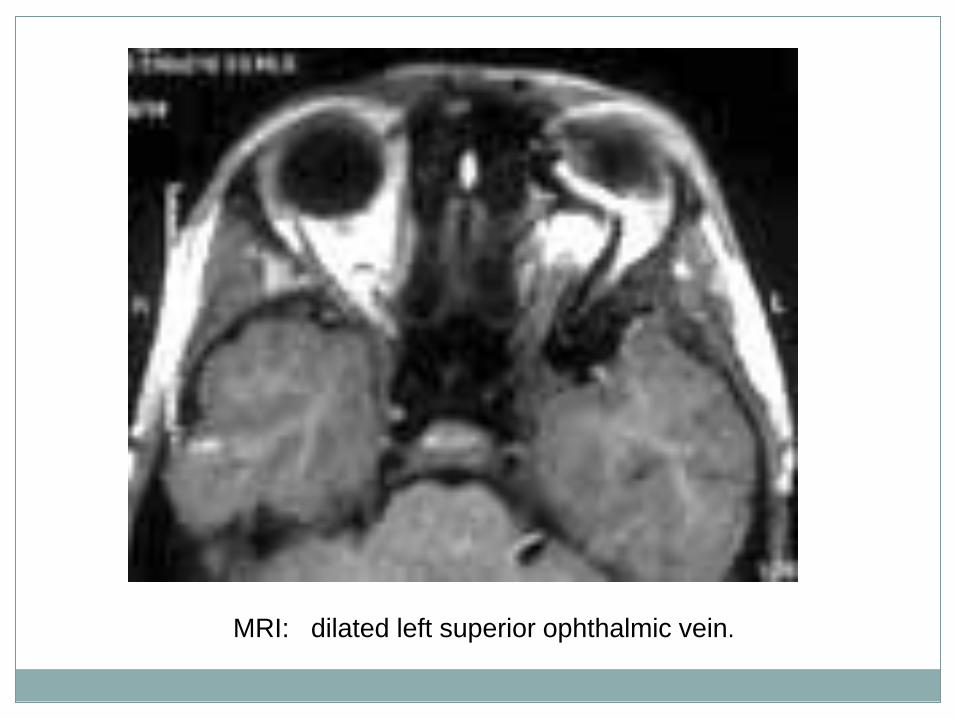
MRI: dilated left superior ophthalmic vein.
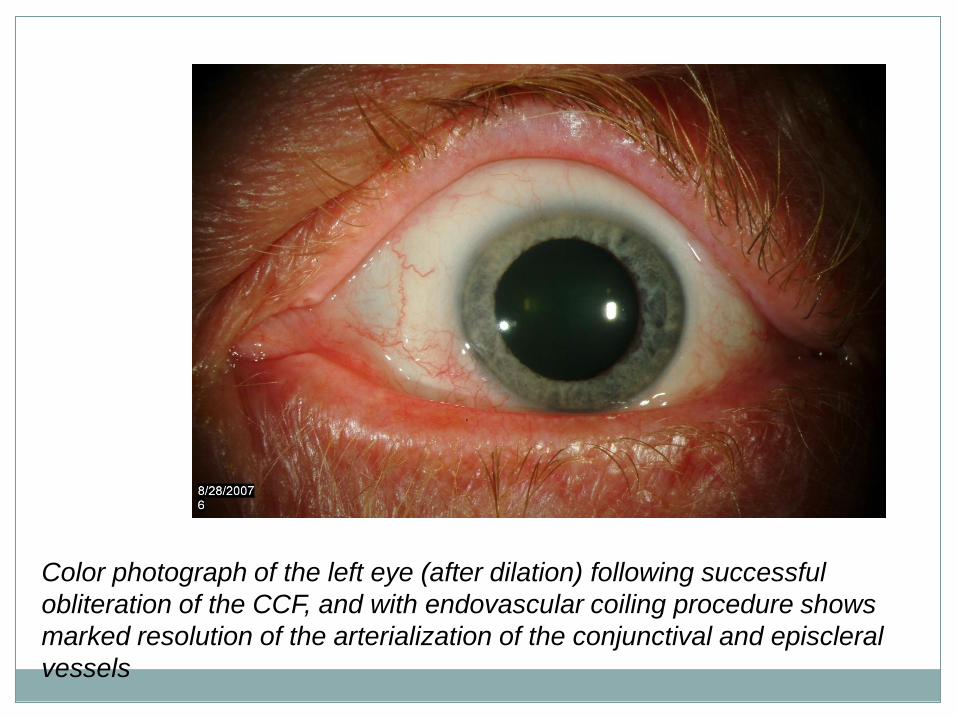
Color photograph of the left eye (after dilation) following successful
obliteration of the CCF, and with endovascular coiling procedure shows
marked resolution of the arterialization of the conjunctival and episcleral
vessels
Ca 3: liệt dây 3 đồng tử bình thường cấp
(Acute Pupil Spared Third Nerve Palsy)
• BN nam 66 tuổi nhập cấp cứu, bn đau đầu vài ngày trước.
• BN sụp mi mắt phải, nhìn đôi khi thức dậy vào buổi sáng
• Tiền sử diabetes mellitus kiểm soát bằng thể dục và ăn
kiêng, hypertension điều trị Lasix và hypercholesterolemia
điều trị statin. Tiền sử gia đình không ghi nhận bất thường
Thăm khám
• Thị lực , thị trường bình thường
• Pupillary bình thường không anisocoria hay RAPD.
• Liệt vân nhãn chung phải
• Slit lamp: posterior chamber intraocular lens bilaterally: bình
thường. Intraocular pressure 14 mm Hg.
• Funduscopic: bình thường 2 mắt
Chẩn đoán ?
Họ tên BN: nam, 28 tuổi.
Nghề nghiệp: làm rẫy ( trồng mãng cầu).
Địa chỉ: Tây Ninh
Thuận tay (P)
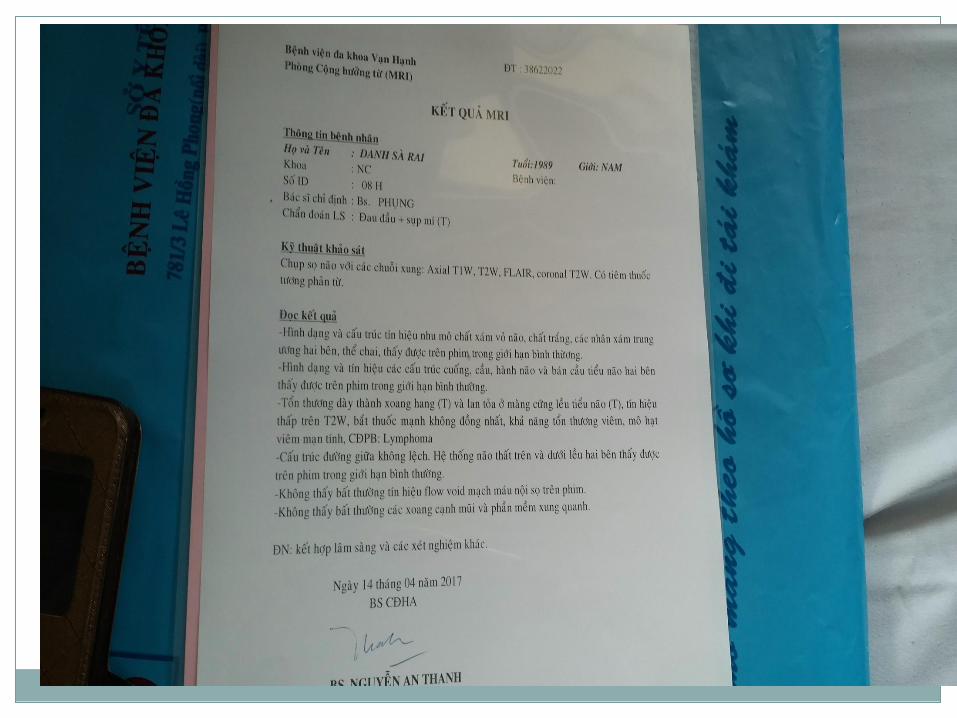
Nhập viện ngày 14/04/2017 vì đau đầu + sụp mi (T)
Ca lâm sàng liệt dây 3 đồng tử bình thường
BN cảm thấy đau ½ đầu bên trái, đau ở vùng trán ( trên ổ
mắt )+ vùng thái dương (T), không đau sau ổ mắt, không
đau tăng khi cử động mắt, đau từng cơn, có đáp ứng với
thuốc giảm đau, thường đau buổi trưa và chiều (11g, 17g).
Kèm theo sụp nhẹ mi mắt (T), và nhìn đôi khi nhìn bằng 2
mắt ( khi che từng mắt thì nhìn bình thường). Sụp mi và
nhìn đôi không dao động trong ngày.
BN có đi khám BS tư được chẩn đoán theo dõi Migrain (T).
Mắt trái mộng thịt, BN được điều trị: Flunarizin 5mg +
piracetam 800ng + magne B6 + Sanlein 0.1% nhỏ mắt.
Nhưng không giảm, BN đau đầu nhiều hơn, sụp mi (T) ngày
càng rõ nên nhập viện BV 115.
Tiền căn
Cách đây 2 năm từng bị sụp mi (P) + giới hạn vận
nhãn toàn bộ mắt (P). Tuy nhiên, không rõ chẩn đoán
và điều trị gì. Điều trị 3 tháng thì hết.
BN tỉnh, tiếp xúc tốt
Sinh hiệu:
M 68l/p, NT 18l/p, T 37°C, HA 100/70mmHg
CN 60 kg, CC 1,6m, BMI 23.4 kg/m2
Thăm khám thần kinh
Đồng tử: 3mm, đều 2 bên.
RAPD bình thường
Sụp mi (T), mắt (T) mở bằng ½ mắt (P)
Mắt (P): mi mắt mở lớn bình thường
Không giới hạn vận nhãn các hướng.
Dấu hiệu Simpson, Cogan: âm tính
Thao tác Gorelick: âm tính
Không lồi mắt.
Không rung giật nhãn cầu
Tóm tắt bệnh án
BN nam 28 tuổi, nhập viện vì đau đầu
Bệnh 1/2 tháng, với các triệu chứng:
TCCN:
Đau ½ đầu (T), vùng trán + thái dương (T), không đau trong
ổ mắt, không đau tăng khi cử động mắt
Sụp mi (T) + nhìn đôi khi nhìn 2 mắt (không dao động trong
ngày)
TCTT:
Sụp mi (T)
3. Tiền căn: cách đây 2 năm từng sụp mi (P) + giới hạn vận
nhãn toàn bộ mắt (P).
Vấn đề bàn luận
1. Liệt dây III không hoàn toàn, không ảnh hưởng
đồng tử (nhìn đôi, sụp mi)+ đau vùng hốc mắt
2. Tiền căn liệt III phải cách 2 năm (hồi phục)
Chẩn đoán nghĩ đến nhiều nhất ?
Các bước chẩn đoán tiếp theo ?
Các bước điều trị tiếp theo
Giải phẫu học dây III
Third cranial nerve
+ levator muscle of the eyelid
+ four extraocular muscles: medial rectus, superior rectus,
inferior rectus, and inferior oblique. (muscles adduct, depress, and elevate the eye).
Superior oblique muscle: cranial nerve IV
Lateral rectus muscle: cranial nerve VI.
Third cranial nerve constricts the pupil:
Parasympathetic fibers:
+ smooth muscle ciliary body
+ sphincter iris.
Nucleus: midbrain consists several subnuclei
innervate the individual extraocular muscles, the eyelids,
and the pupils.
Subnucleus, except the superior rectus subnucleus,
supplies the ipsilateral muscle.
Superior rectus subnucleus innervates the contralateral
superior rectus muscle
Levator subnucleus is a single central caudate nucleus
and innervates both levator palpebrae superioris muscles
(which control the eyelids)
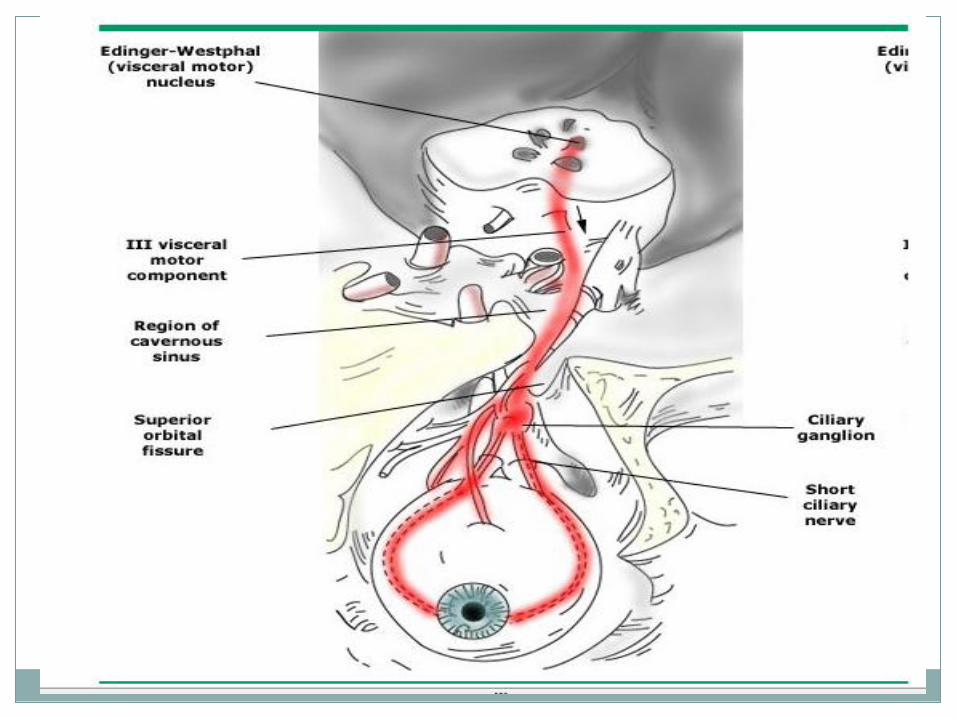
Parasympathetic pupil nucleus (Edinger-Westphal
nuclei) controls pupil constriction
Third nerve fascicle leaves the nucleus and passes
ventrally near important structures in the midbrain (eg, red
nucleus, corticospinal tract).
Third nerve then enters the subarachnoid space,
Passes into the lateral wall of the cavernous sinus,
Divides into superior and inferior branches as it enters the
superior orbital fissure in the orbit to innervate the extraocular
muscles
Superior division of the third nerve supplies the
levator palpebrae and the superior rectus,
Inferior division supplies the medial and inferior
rectus muscles, the inferior oblique, and the pupillary
sphincter.
In partial lesions, the pupil may be of normal size and
normally reactive (no internal dysfunction),
Dilated and poorly reactive (partial internal dysfunction),
Dilated and non-reactive to light and near stimulus
(complete internal dysfunction).
Tổng quan liệt dây III(TNP)
Phân loại:
• Third nerve palsy (TNP): chia 2 nhóm
+ non-isolated: không đơn độc
+ isolated TNP: liệt dây 3 đơn độc
• The isolated TNP were defined as TNP without
associated neurologic findings (e.g. headache, other
cranial neuropathies).
(bn có bằng chưng nhược cơ(myasthenia gravis) (e.g. variability,
fatigue Cogan’s lid twitch sign, enhancement of ptosis) không bao
gồm trong nhóm isolated TNP)
Phân loại: sáu nhóm TNP
Type 1: Non-isolated (nhóm không đơn độc)
TNP xem như non-isolated khi có triệu chứng sau:
1. Orbital disease (e.g. chemosis, proptosis, lid swelling, injection,
and positive forced ductions)
2. Bằng chứng myasthenia gravis (e.g. fatiguability of the motility defect,
Cogan’s lid twitch sign, orbicularis oculi weakness)
3. Liệt nhiều dây sọ (including bilateral TNP) hay radiculopathy
4. Dấu thân não (e.g. hemiplegia, cerebellar signs, other cranial nerve
deficits)
5. Systemic, infectious, or inflammatory risk factors for TNP (e.g.history of
previous malignancy, giant cell arteritis, collagen vacular disease)
6. Đau đầu nặng
Type 2: Traumatic TNP
Liệt đơn thuần một bên TNP, được xác định tạm thời liên hê tiền sử
chấn thương đầu và không tiến triển, không bao gồm chấn thương
đầu nhẹ
Type 3: Congenital TNP
Bn sinh ra có isolated TNP hay ghi nhận có TNP trong 3 tháng đầu.
Type 4: mắc phải, không chấn thương isolated TNP
• Type 4A: TNP with a normal pupillary sphincter with
completely palsied extraocular muscles (liệt toàn bộ vận nhãn
chung với đồng tử bình thường)
Acute Pupil Spared Third Nerve Palsy
• Type 4B: TNP with normal pupillary sphincter and
incomplete palsied extraocular muscles (liệt một phần vận nhãn
chung với đồng tử bình thường)
• Type 4C: TNP with subnormal pupillary sphincter
dysfunction and partial or complete extraocular muscle palsies (liệt một phần hay toàn bộ vận nhãn chung với đồng tử bất thường)
Type 5: Progressive or unresolved TNP (tiến triển )
+ Bn với TNP xấu hơn sau giai đoạn cấp (trên 2 tuần)
hay thêm dấu thần kin mới.
+ Bn không hết TNP sau 12-16 tuần xem như không hồi
phục(unresolved)
Type 6: TNP with signs of aberrant regeneration
(tái sinh lạc chổ)
Bàn về hướng xử trí
• Liệt dây 3 không đơn độc (Non-isolated TNP)
+ neuroimaging: chú ý khu vực phối hợp triệu chứng thần kinh (chẩn
đoán định khu)
+ thường chọn magnetic resonance (MR) imaging with and without
gadolinium enhancement
+ CT scanning : chọn đầu tiên trong bn chấn thương đầu hay bệnh lý
mạch máu cấp(infarction or hemorrhage).
+ nếu có dấu màng não thực hiện chọc dò DNT
• Bn liệt dây 3 mắc phải, đơn độc không chấn thương
Acquired, nontraumatic isolated TNP: sang thương bất cứ đâu
từ bó(fascicle) đến hốc mắt(orbit)
+ TNP cơ vòng đồng tử bình thường và liệt hoàn toàn cơ vận nhãn
ngoài: hầu hết không bao giờ intracranial aneurysms.
+ Loại TNP này nguyên nhân thường gặp: ischemia, đặc biệt liên hệ
diabetes mellitus.
+ Ischemic TNP có thể xảy ra với giant cell arteritis và systemic
lupus erythematosus.
• Pupil-sparing TNP:
+ đã được báo cáo với sildenafil citrate (Viagra)
+ cocaine.
• Nguy cơ ischemic oculomotor nerve palsies :
+ diabetes,
+ left ventricular hypertrophy,
+ elevated hematocrit.
+ Obesity,
+ hypertension,
+ smoking are also probable risk factors

• Ischemic lesions of the oculomotor nerve often spare the pupil because
the lesion is confined to the core of the nerve and does not affect
peripherally situated pupillomotor fibers.
• The pupil may, however, be involved in diabetic oculomotor palsies and
diabetes may even cause a superior branch palsy of the oculomotor
nerve.
• Pupil sparing has been documented in 62–86% of TNP due to
ischemia.
• Patients who have oculomotor nerve palsies with anisocoria of greater
than 2.0 mm are considered outliers for the diagnosis of ischemia.
• Bn liệt không hoàn toàn dây 3, không ảnh hưởng
đồng tử đòi hỏi MRI não để loại trừ tổn thương
choáng chổ(mass)
• Liên hệ đồng tử không chẩn đoán do chèn ép phình mạch, đến 38%
liên quan đồng tử được đề nghị do thiếu máu
• Bn liệt dây 3 không ảnh hưởng đồng tử(“relative pupil sparing” TNP)
chụp MRI loại trừ có thể chèn ép
• CT scan nếu nghi ngờ subarachnoid hemorrhage và chỉ định mạch
não đồ
• In another report of 24 patients with relative pupil-sparing TNP:
+ 10 had nerve infarction,
+ eight had parasellar tumors,
+ two had intracavernous carotid aneurysms,
+ one had leptomenigeal carcinomatosis
+ one had Tolosa-Hunt syndrome,
+ one had oculomotor neurilemmoma,
+ and one had primary ocular neuromyotonia.
• Others have reported
+ internal carotid, posterior communicating and basilar artery aneurysms in
isolated TNP with relative pupillary sparing.
• Cerebral angiography may still be warranted if MR imaging is negative.
• Because up to 38% of patients with ischemic third nerve palsies have
pupillary dysfunction
• Liệt toàn bộ dây 3 trong và ngoài(Complete external and
internal third nerve palsies) xảy ra đơn độc thường do
chèn ép hay thâm nhiễm màng não(compressive lesions
or meningeal infiltration).
• Dãn và mất px đồng tử xảy ra trên 71% bn do phình mạch
chèn ép và TNP.
• Aneurysms tổn thương đồng tử 96% trong TNP và chừa
lại 4% đồng tử chỉ trong liệt dây 3 không toàn bộ
Isolated complete or partial internal dysfunction (pupil
dilated) with completely normal external function of
the third nerve and no ptosis
HƯỚNG DẪN
Liệt đơn độc hoàn toàn hay 1 phần chức năng
trong(đồng tử dãn) và chức năng ngoài dây III
hoàn toàn bình thường và không sụp mi
(1)
• Nguy cơ aneurysm trong trường hợp này rất ít và
chẩn đoán hình ảnh có thể không đòi hỏi
• Lâm sàng tìm kiếm chẩn đoán căn nguyên khác rối
loạn chức năng đồng tử đơn độc.
(e.g. tonic pupil, pharmacologic, sphincter damage).
Partial external dysfunction TNP without internal dysfunction
Liệt chức năng ngoài một phần
không rối loạn chức năng trong (đồng tử hoàn toàn bình thường)
(2)
• Nguy cơ aneurysm trong bn partial TNP thì trung bình
(trên 30% ca).
• Bn rõ myasthenia gravis không đòi hỏi đánh giá thêm
aneurysm
• Căn nguyên khác non-aneurysmal :
+ neoplastic,
+ demyelinating,
+ infiltrative,
+ ischemic etiologies (có thể gây partial TNP without pupil involvement và đòi hỏi neuroimaging)
• Nếu TNP do aneurysm, TNP thường tiến triển theo thời
gian, TNP hoàn toàn và ảnh hưởng đồng tử
• BN theo dõi diển tiến lâm sàng và liên quan đồng tử trong tuần lể
đầu tiên
• Nếu MRI, MRA và CT sọ âm tính và nguy cơ chụp mạch máu cao
(e.g. elderly, severe cardiovascular disease, abnormal serum
creatinine), theo dõi là hợp lý và tìm kiếm thay đổi căn nguyên cho
partial external dysfunction TNP (e.g. myasthenia gravis).
• Bs lâm sàng vẫn xem xét angiography trong ca này nếu nguy cơ
aneurysm cao hơn nguy cơ chụp mạch máu (technically inadequate
MRA, progression to complete TNP, pupil involvement).
• Nếu bn partial TNP có dấu hiệu meningeal irritation, hay
liệt dây sọ khác hay diffuse meningeal involvement (e.g.
radiculopathies), chọc dò DNT khảo sát nhiễm trùng,
viêm nhiễm hay neoplastic meningitis.
• Trong ca nghi ngờ subarachnoid hemorrhage, CT scan
tiếp theo cerebral angiography
Complete external dysfunction with completely normal internal function TNP
Liệt dây III rối loạn chức năng ngoài hoàn
toàn với chức năng trong bình thường
(đồng tử bình thường)
(3)
• Nguy cơ rất thấp aneurysm và theo dõi bệnh lý mạch máu
• Đồng tử tái khám trong tuần lễ đầu tiên.
• Bn phát triển liên hệ đồng tử sẽ đánh giá theo khuyến cáo
pupil-involving TNP.
• Vasculopathic risk factors, đặc biệt diabetes mellitus,
hypertension và tăng increased cholesterol, sẽ theo dõi và
kiểm soát
• Bn trên 55 tuổi, đặc biệt có triệu chứng giant cell arteritis
(e.g. headache, jaw or tongue claudication, polymyalgia
rheumatica symptoms), xác định sedimentation rate.
Temporal artery biopsy thực hiện nếu VS tăng hay hiện
diện triệu chứng hệ thống
• Nếu bn không có vasculopathic risk factors, hay nếu
không cải thiện sau 4-12 tuần hay nếu có phát triển sự
tái sinh lạc chổ (aberrant regeneration develop), thực
hiện MRI, MRA hay CT
• Đánh giá myasthenia gravis thực hiện bn xem xét không
đau, liệt dây III không ảnh hưởng đồng tử, không lồi mắt
(painless, non-proptotic, pupil spared ophthalmoplegia)
Partial external dysfunction with partial internal dysfunction TNP
Liệt dây 3 với rối loạn chức năng
ngoài và trong một phần
(4)
• Hợp lý chẩn đoán hình ảnh MRI, MRA, CT não đầu tiên.
• Nếu kết quả âm tính, theo dõi tiến triển bệnh nhân hay
rối loạn chức năng trong hoàn toàn
.
• Nguy cơ cho aneurysm trong tình huống này vẫn chưa
loại chắc chắn(ngay cả MRI/MRA âm tinh). Lâm sàng
xem xét chụp mạch máu(DSA) nếu nguy cơ phình mạch
cao hơn nguy cơ angiography.
Complete external dysfunction with partial internal dysfunction TNP
Liệt dây 3 với rối loạn chức năng
ngoài hoàn toàn và rối loạn chức
năng trong một phần
(5)
• Nguy cơ aneurysm cho complete external dysfunction
with partial internal dysfunction (partial pupil or “relative
pupil sparing”) vẫn còn chưa biết nhưng có thể thấp
hơn partial external dysfunction hay không có partial
internal dysfunction.
• Nguy cơ aneurysm trong tình huống này ( ngay cả
negative MRI/MRA or CTA) không chắc chắn loại bỏ.
Lâm sàng xem xét chụp mạch máu(DSA) nếu thấy
nguy cơ phình mạch cao hơn nguy cơ angiography.
Isolated complete internal dysfunction with partial or complete external dysfunction TNP
Liệt dây 3 đơn độc rối loạn chức năng trong toàn
bộ và một phần hay toàn bộ chức năng ngoài
(6)
• Trường hợp nguy cơ cao nhất cho aneurysm (86% -
100% aneurysmal TNP pupil involvement). Thực hiện
MRI, MRA hay CTA đầu, ngay cả âm tính khuyến cáo
mạnh catheter angiography(DSA)
Any patient with TNP and signs of subarachnoid hemorrhage
Liệt dây 3 và dấu hiệu
xuất huyết dưới nhện
(7)
• Sự hiện diện SAH (on unenhanced CT scan or LP) là
cần thiết để bàn về complete hay incomplete TNP cũng
như áp dụng “rule of the pupil” moot.(tranh luận quy tắc
đồng tử)
• Thường CT scan đầu tiên (xem xét lumbar puncture)
bn TNP và dấu hiệu SAH.
• Hình ảnh SAH (e.g. severe headache, meningismus,
altered consciousness) có thể nhầm intracranial
etiologies khác như: pituitary apoplexy và hầu hết sẽ
CT trước khi xem xét angiography
• Bn SAH trên CT scan có thể catheter angiography.
• Bn không catheter angiogram (e.g. morbidly obese and
unable to be placed on the angiography table) có thể
cranial CT and CTA alone trước khi can thiệp
• Trong ca SAH khác , special MR imaging parameters,
bao gồm: FLAIR MRI và MRA có thể ích lợi. Catheter
angiography sẽ xem xét mạnh ngay cả nếu đánh giá
SAH (e.g. CT, LP) âm tính.
Patients who cannot undergo MRI or MRA
Bn không làm được MRI hay MRA (8)
• CT và CTA có thể xem xét chọn lọc nếu MRA không thực
hiện được hay chống chỉ định (e.g. obesity, claustrophobia,
pacemaker). Mặc dù CTA có một vài thuận lợi trên MRA
(especially if the location of the aneurysm is known),
• (superior quality of MRI has compared to CT in evaluating the entire
course of the third nerve makes the combination of MRI/MRA superior to
CT/CTA as the screening study for TNP)
• Không đầy đủ bằng chứng xác định kết hợp MRI và CTA
trên MRI/MRA trong bn TNP
Ca lâm sàng
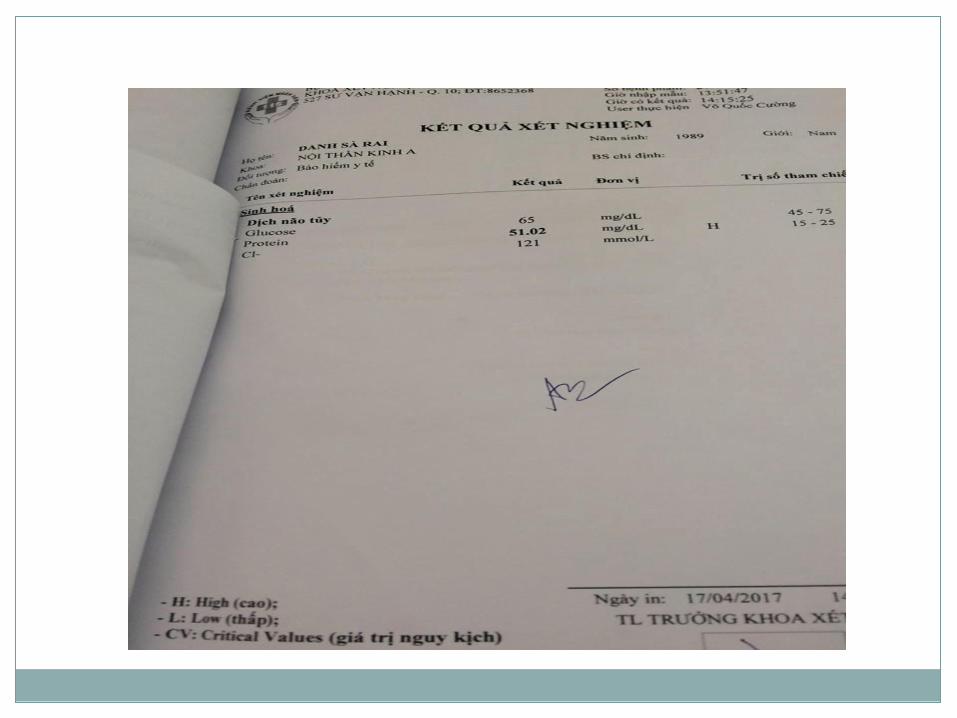
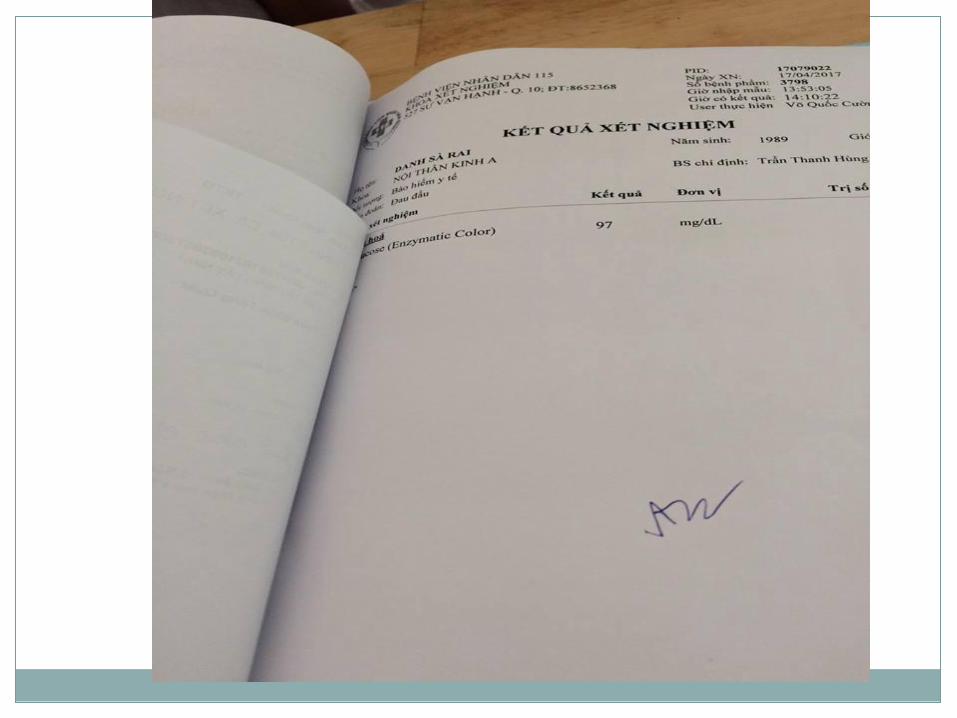
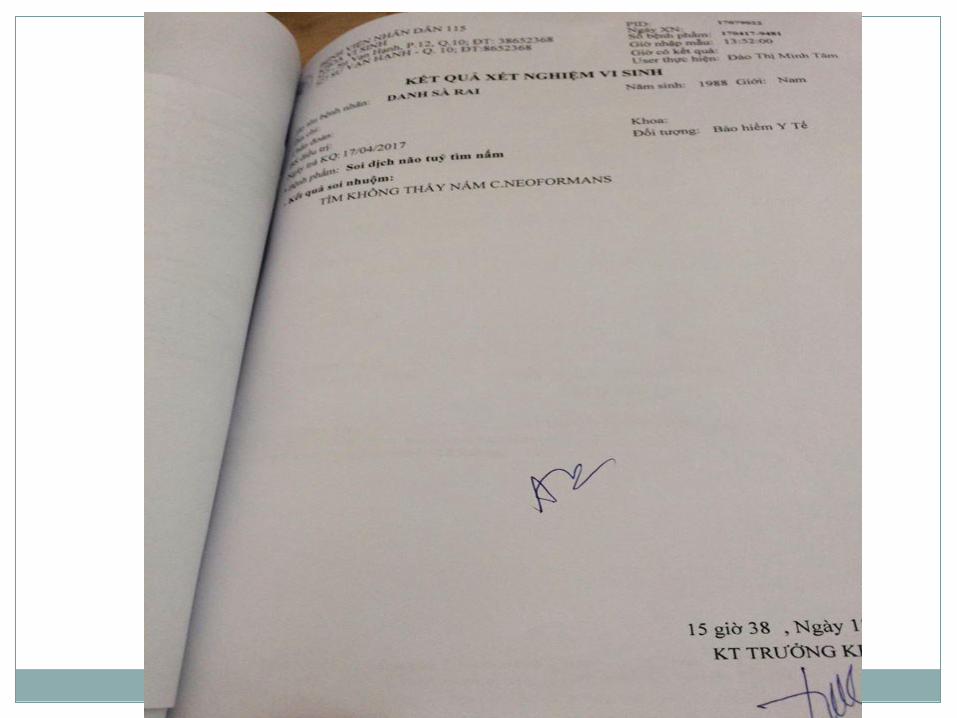
BN đau đầu+ sụp mi+nhìn đôi, đồng tử bình thường
Chẩn đoán:
+ Liệt dây 3 không đơn độc, rối loạn chức năng ngoài
không hoàn toàn với chức năng trong bình thường. Khả
năng liệt dây 3 do phình mạch khoảng 30%
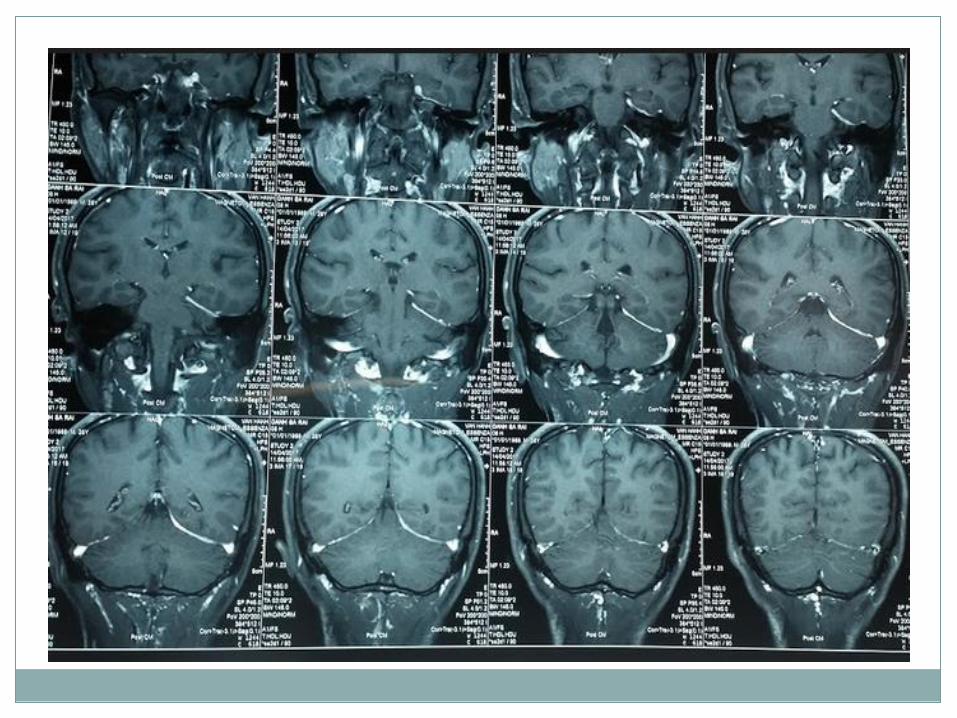
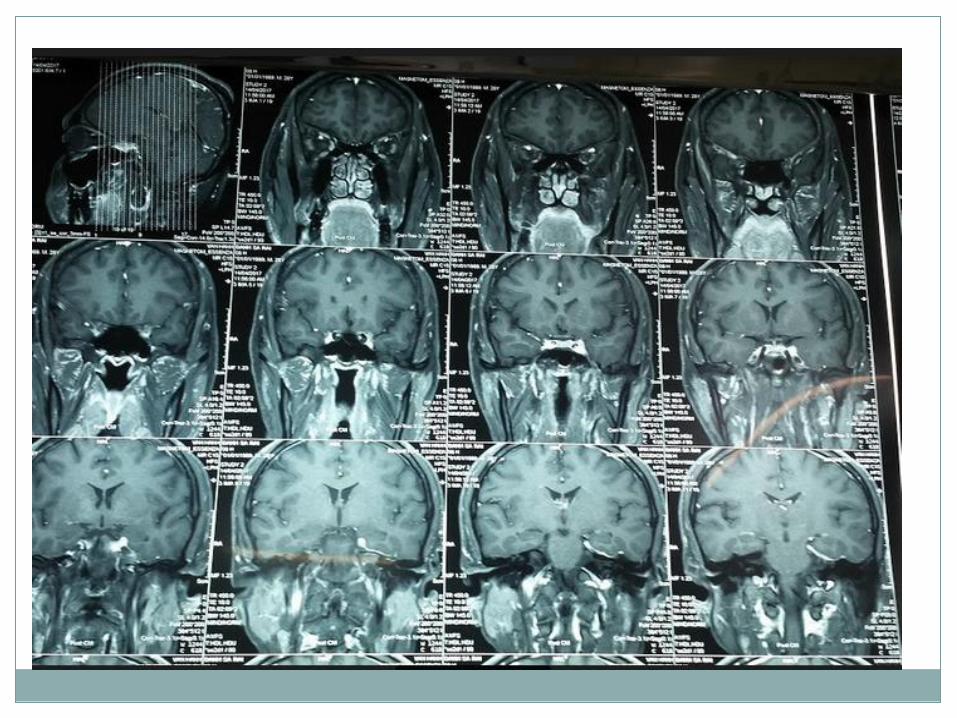
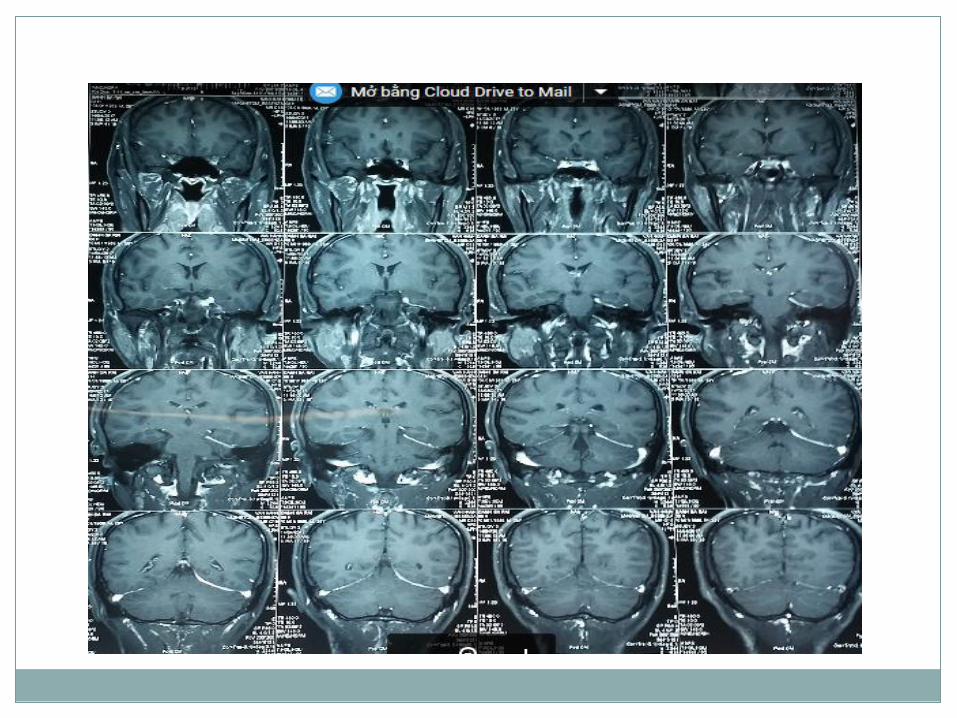
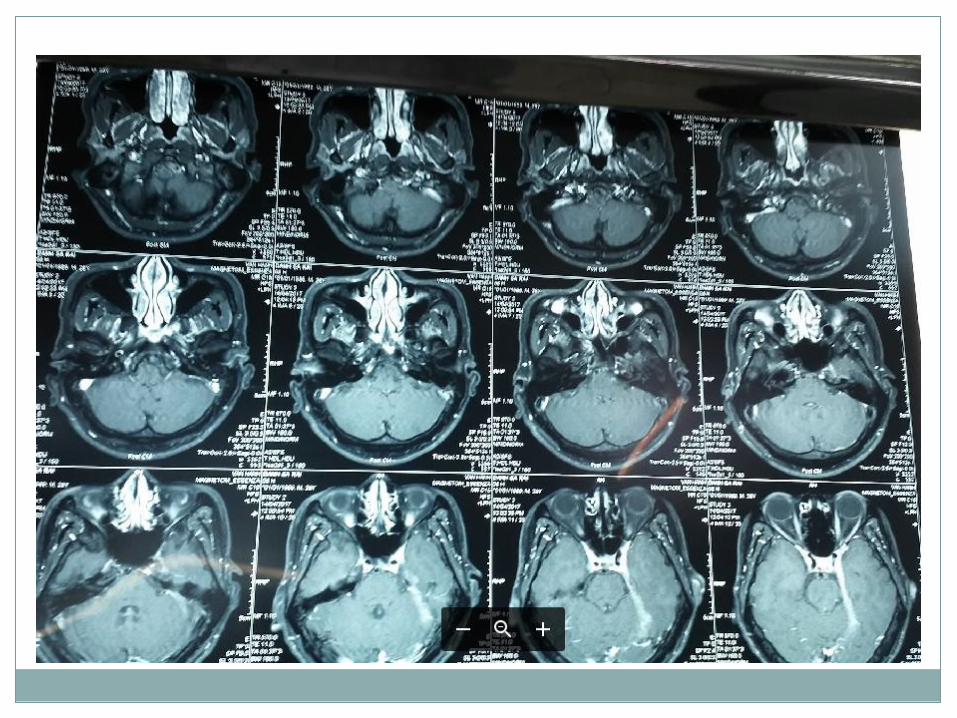
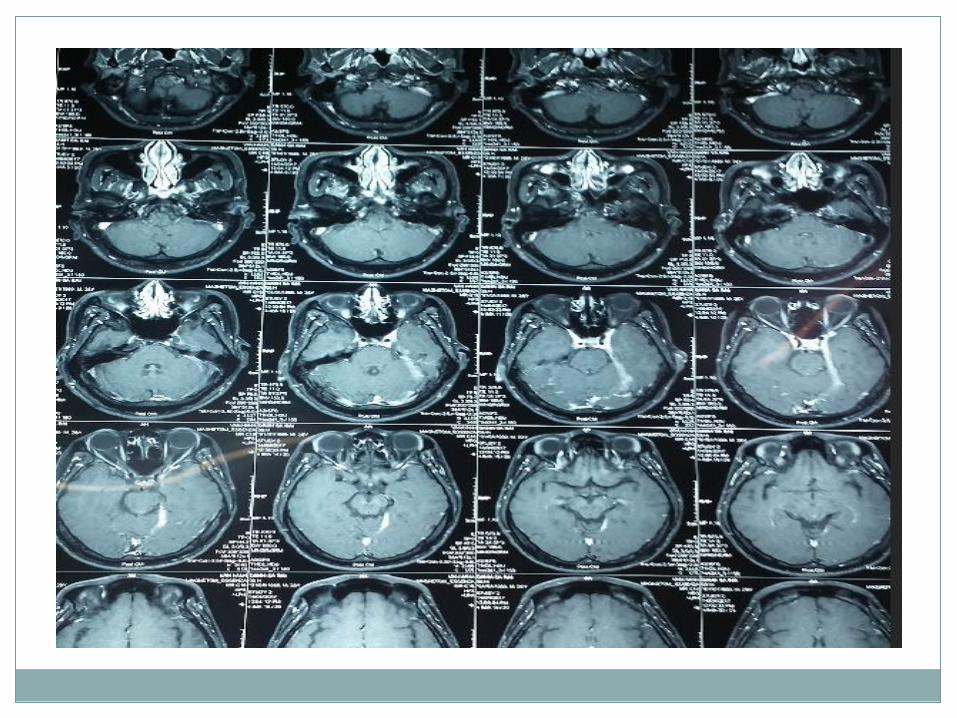
+ MRI tổn thương dày thành bên xoang hang trái, lan tỏa
màng cứng lều tiểu não, tín hiệu thấp trên T2W và bắt
gado mạnh không đồng nhất: viêm mô hạt mạn tính. Chẩn
đoán phân biệt lymphoma
Liệt dây 3(t) do viêm mô hạt mạn
tính thành xoang hang (t)
Điều trị:
BN này được điều trị solumedrol 40mg x 2 (TMC). Sau
1 ngày, BN hết hẳn đau đầu + hết sụp mi. (đáp ứng tốt
corticoids)
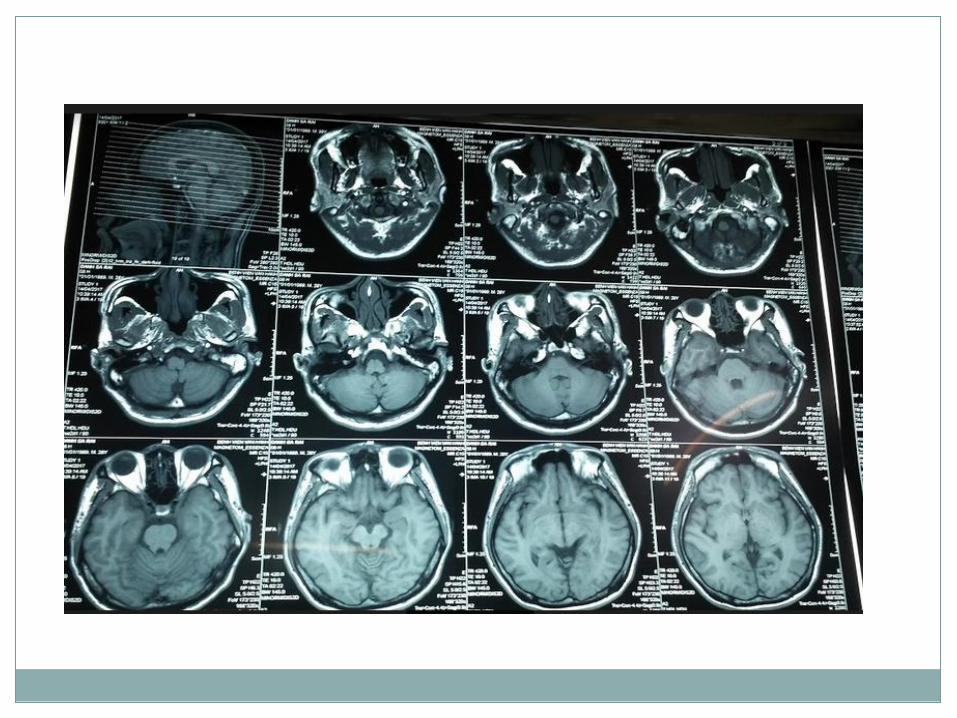
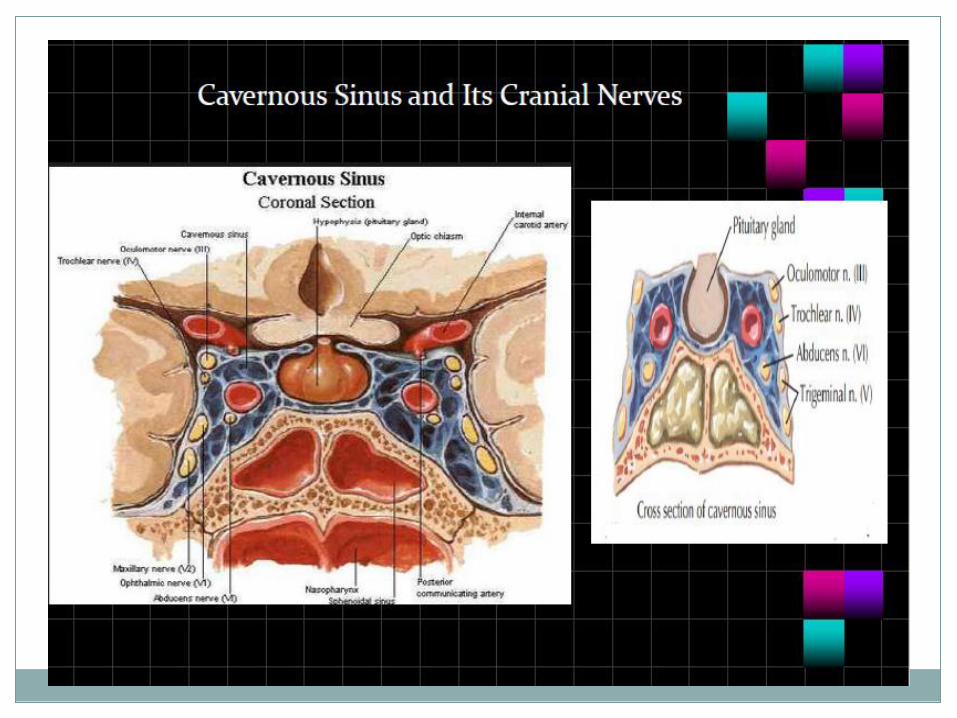
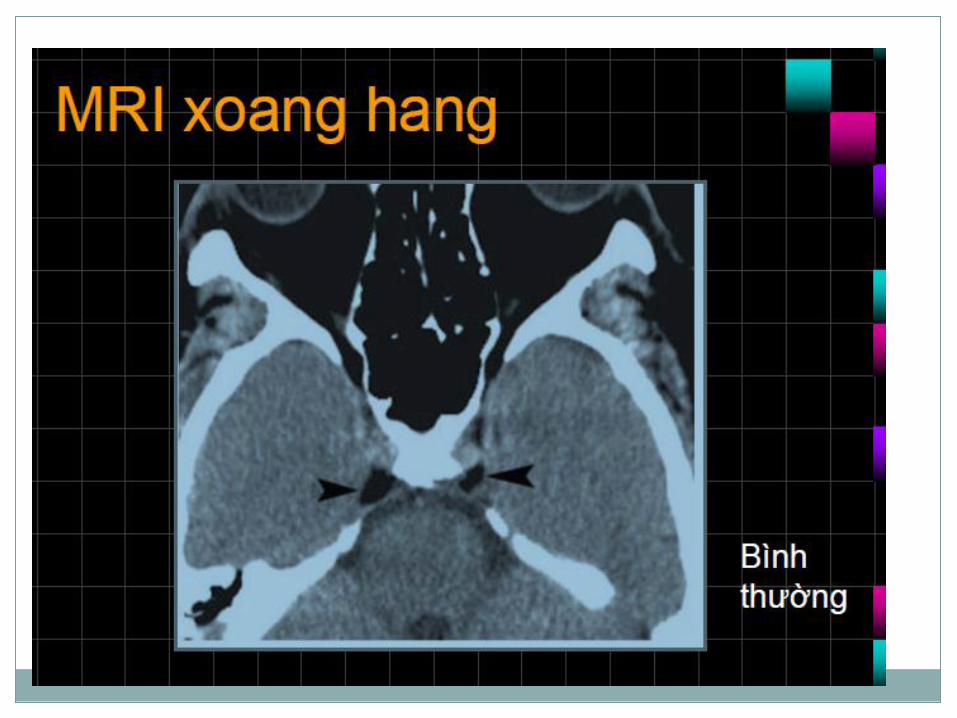
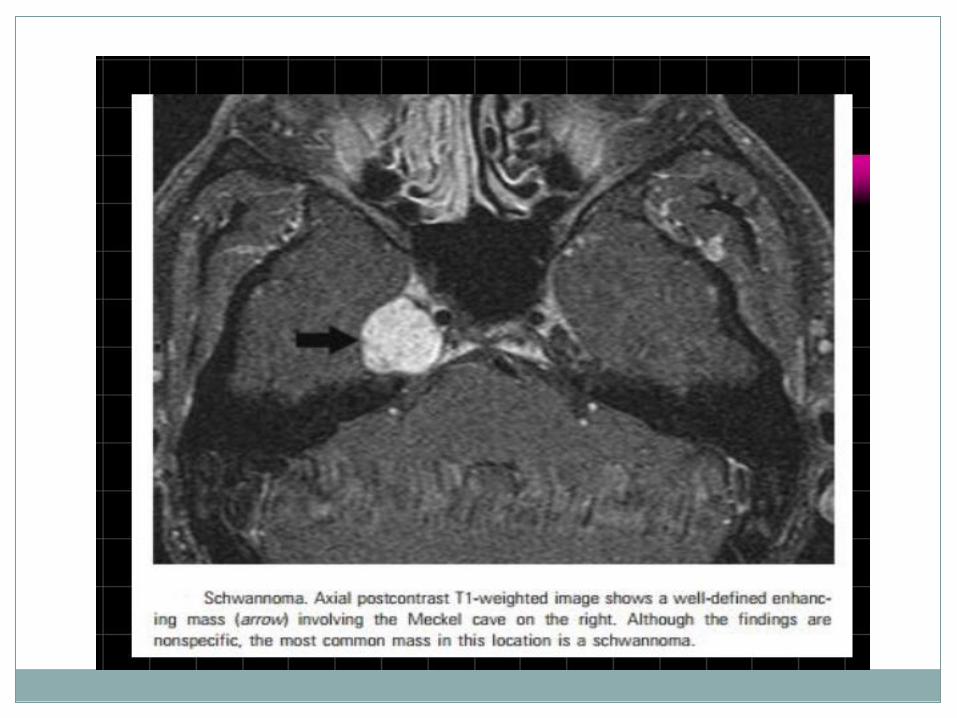
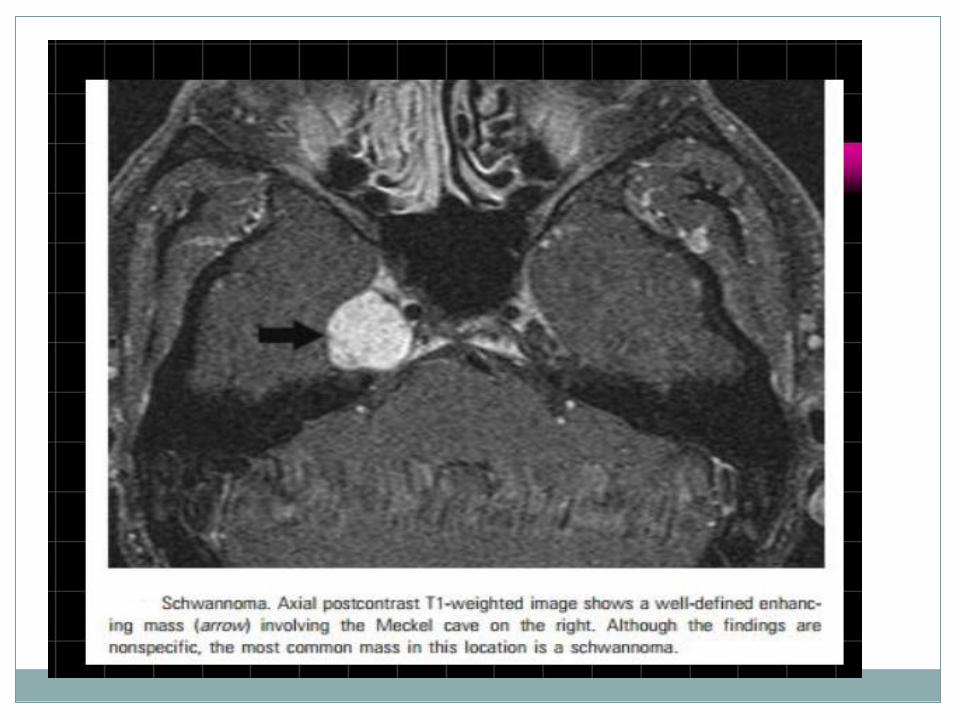
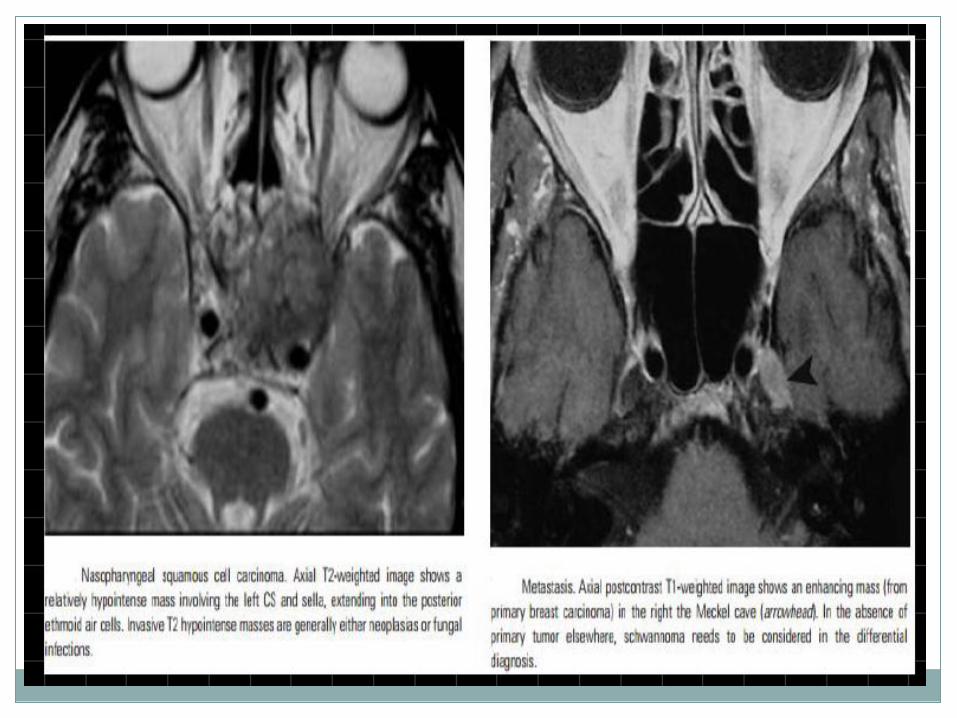
Hình ảnh xoang hang
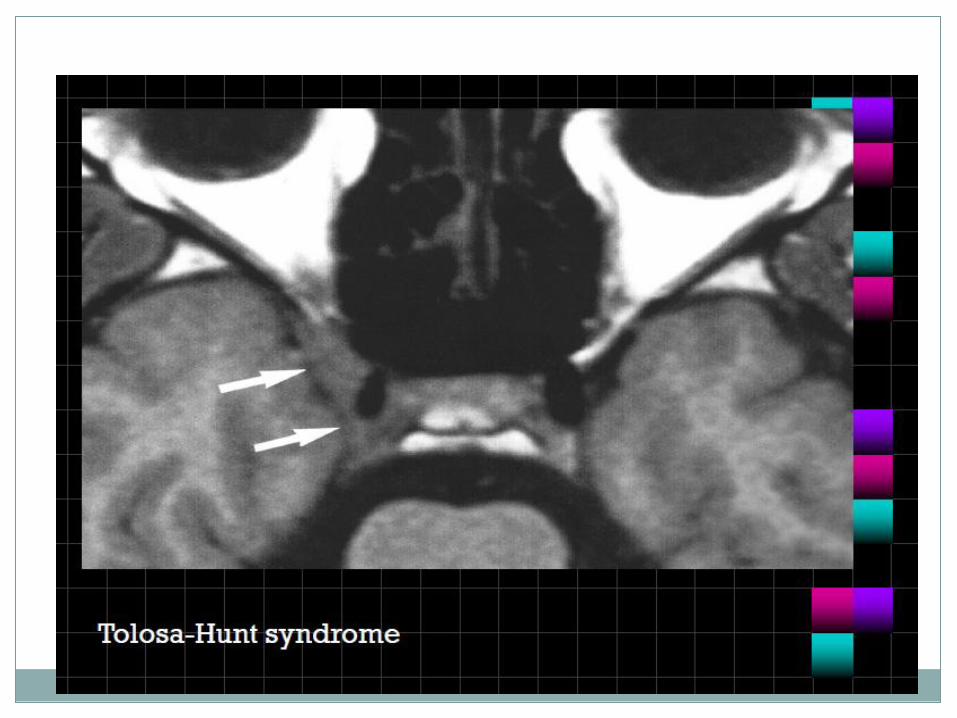
Tolosa-Hunt syndrome
Clinically it refers to the presence of a painful
ophthalmoplegia secondary to surrounding cavernous
sinus inflammation.
Tolosa-Hunt syndrome is essentially a clinical
diagnosis of exclusion
Definition
Episodic orbital pain associated with paralysis of
one or more of the CN III, IV, VI due to
granulomatous inflammation of the cavernous sinus
Presentation:
Pain behind the eye followed by painful ophthalmoplegia
CN III,IV, VI palsy leading to diplopia
Unilateral 95% of time
Natural history:
Benign condition but permanent neurological deficits
can occur, relapses occur in at least 50% of patients
and often requiring immunosuppressive therapy
May resolve spontaneously if left untreated
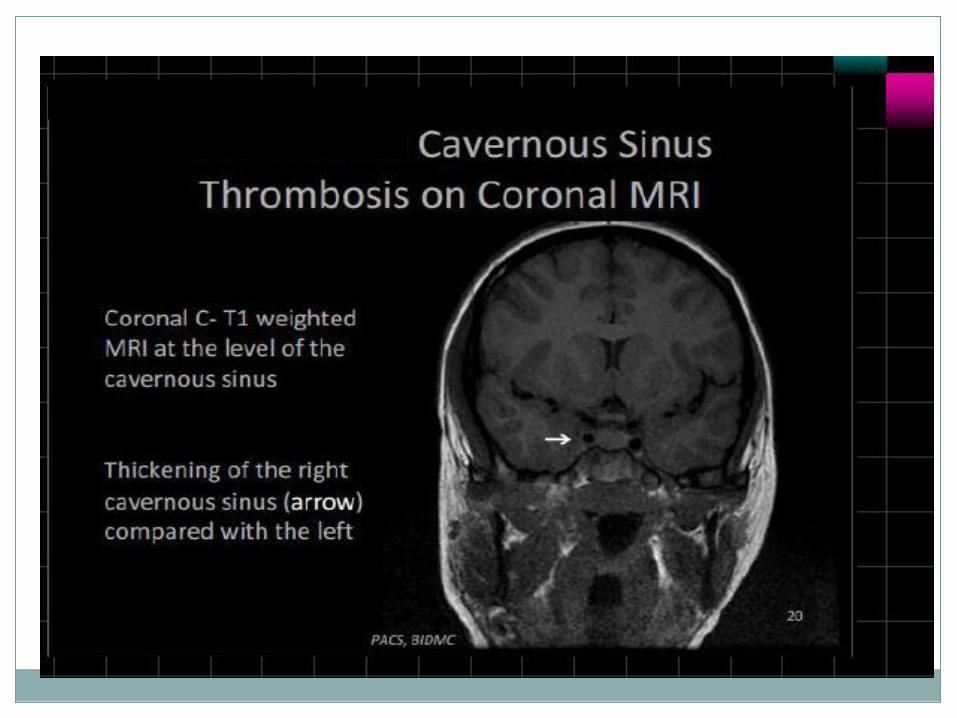
CT
May show asymmetrical enlargement in the region
of the cavernous sinus on the affected side +/-
contrast enhancement
The secondary criteria are internal carotid artery
narrowing, extension towards the superior orbital
fissure and orbital apex.
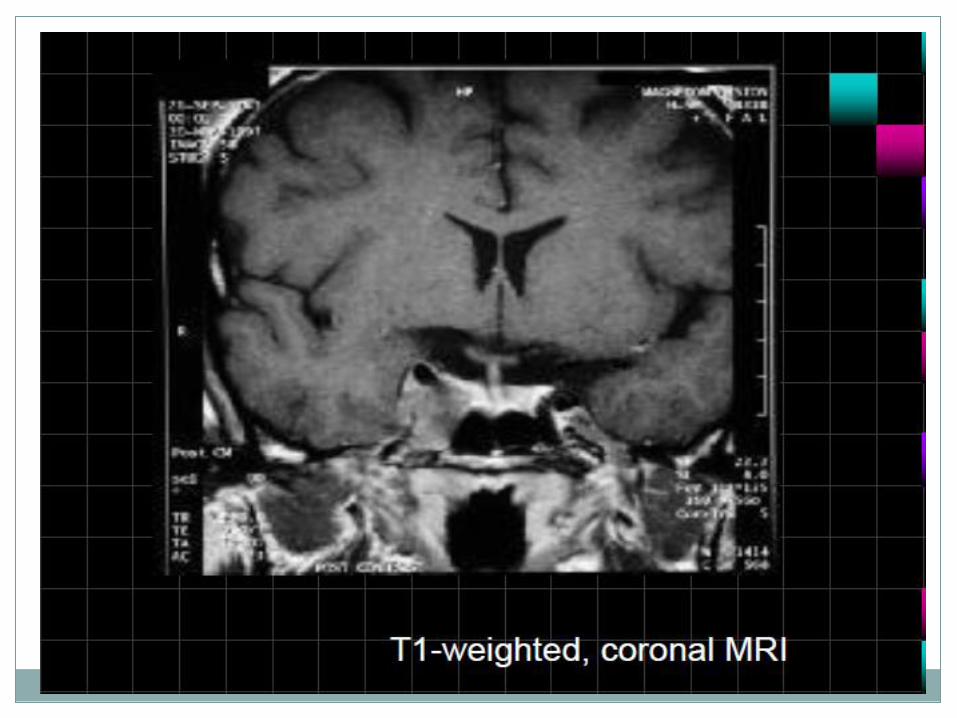
MRI
May show evidence of inflammatory changes in the
region of the anterior cavernous sinus, superior orbital
fissure +/- orbital apex.
Signal characteristics are nonspecific (clinical scenario
essential to diagnosis) but may include:
1. T1: involved region is isointense to hyperintense
compared with muscle
2. T2: involved area is hyperintense
3. T1 C+ (Gd): may show contrast enhancement during
active phase with resolution of enhancement following
treatment
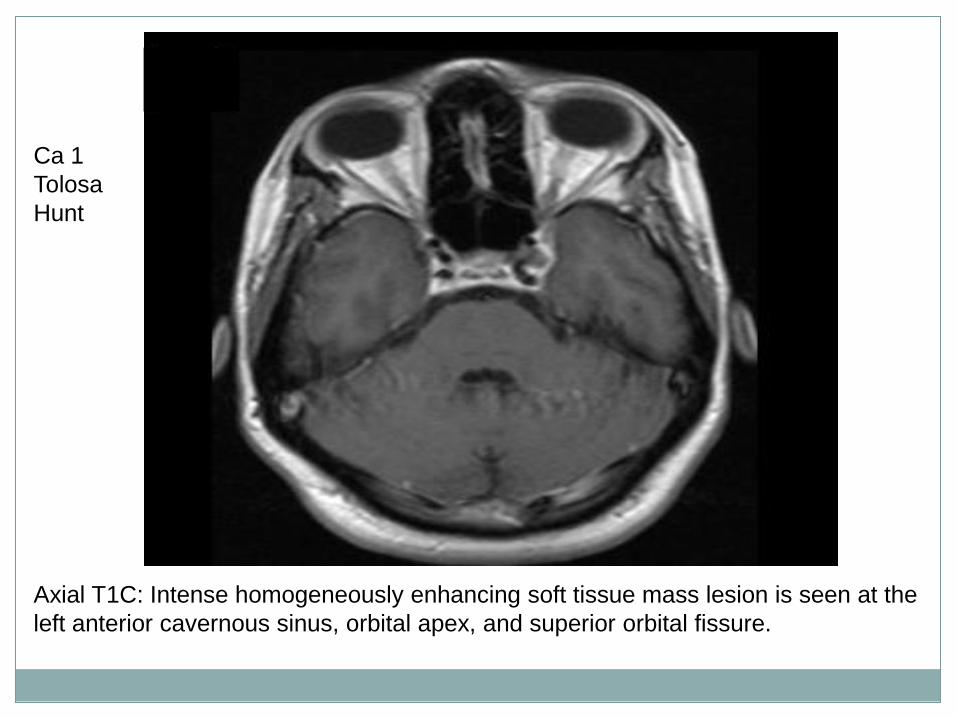
Axial T1C: Intense homogeneously enhancing soft tissue mass lesion is seen at the
left anterior cavernous sinus, orbital apex, and superior orbital fissure.
Ca 1
Tolosa
Hunt
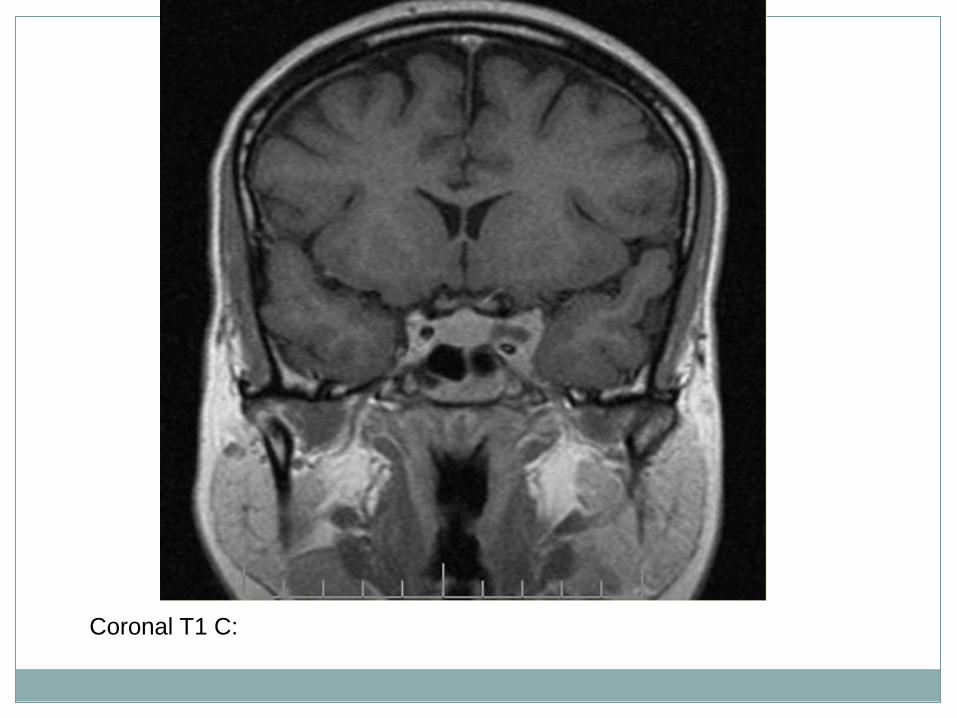
Coronal T1 C:
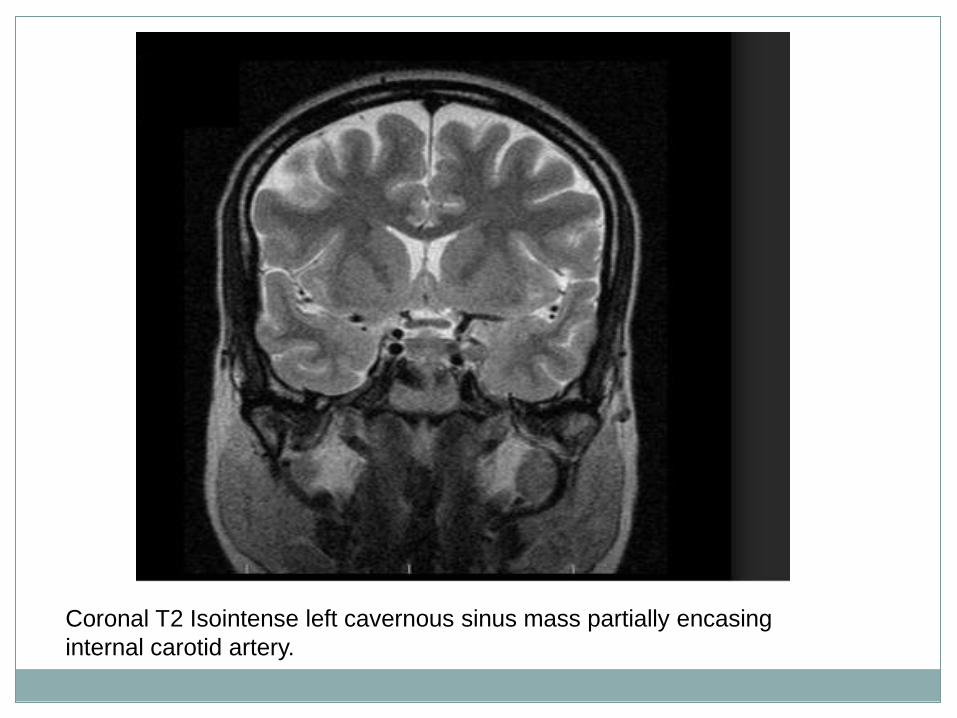
Coronal T2 Isointense left cavernous sinus mass partially encasing
internal carotid artery.

Ca 2 Tolosa Hunt
Câu hỏi ???