Embed Size (px)
Citation preview

Vol. 6. 1021-1027, December 1997 Cancer Epidemiologj�, Biomarkers & Prevention /021
Calcium and Colorectal Epithelial Cell Proliferation in
Ulcerative l
Roberd M. Bostick,2 Mark Boldt, Mohamed Darif,James R. Wood, Paula Oven,, and John D. Potter
Department of Public Health Sciences-Epidemiology, The Bowman Gray
School of Medicine, Wake Forest University, Winston-Salem, North Carolina
27157 IR. M. B.]; Digestive Healthcare, PA, Minneapolis, Minnesota 55404
EM. B., J. R. W.]; Division of Biostatistics, School of Public Health, University
of Minnesota, Minneapolis, Minnesota 55455 [M. DI; Abbott-Northwestem
Hospital, Minneapolis, Minnesota [P. 0.]; and Fred Hutchinson Cancer
Research Center, Seattle, Washington 98104 [J. D. P.]
Abstract
In persons at higher risk for colon cancer (e.g., those
with sporadic adenoma or ulcerative colitis), compared tothose at lower risk, colonic epithelial cell proliferation
kinetics are altered. We have shown previously thatcalcium supplementation appears to normalize thedistribution of proliferating cells without affecting theproliferation rate in the colorectal mucosa of sporadicadenoma patients. In a pilot randomized, double-blind,placebo-controlled, clinical trial conducted concurrentlywith our previously published sporadic adenoma trial, wetested whether calcium supplementation can alsomodulate cell proliferation kinetics in patients withulcerative colitis. Ulcerative colitis patients (n = 31) wererandomized to placebo or 2.0 g of supplemental calcium
daily. Colorectal epithelial cell proliferation was
determined by immunohistochemical detection ofproliferating cell nuclear antigen labeling of cells in “non-prep” rectal biopsies taken at randomization and after 2months treatment. All biopsies were scored by onereviewer. Differences in mean follow-up minus baselinelabeling index (LI; the proportion of colon cryptepithelial cells that were labeled) and in the 0h
(proportion of labeled cells that were in the upper 40%
of the crypts) were compared with analysis of covariance.Pill-taking adherence was 97%. Biopsy-scoring reliabilitywas high (r 0.89). The pooled baseline LI and 0h were6.3% and 5.6%, respectively. The LI in the calciumgroup decreased by 0.3% (proportionately, 3%) morethan in the placebo group (P 0.91). Similarly, the 0h inthe calcium group decreased by 0.5% (proportionately,10%) more than in the placebo group (P = 0.85). This
Received 5/8/97; revised 8/27/97; accepted 8/28/97.
The costs of publication of this article were defrayed in part by the payment of
page charges. This article must therefore be hereby marked advertisement in
accordance with 18 U.S.C. Section 1734 solely to indicate this fact.I This study was supported in part by USPHS Biomedical Research Support Grant
507 RR 055448 (Division of Research Resources) and by PHS Grant POICA-
50305 (National Cancer Institute), NIH, Department of Health and Human
Services.
2 To whom requests for reprints should be addressed, at Department of PublicHealth Sciences-Epidemiology, The Bowman Gray School of Medicine, Wake
Forest University, Medical Center Boulevard, Winston-Salem, NC 27157.
pilot study does not suggest that 2.0 g of calcium ascalcium carbonate daily can substantially normalizeeither the rate or distribution of proliferating cells over a2-month period in the colon crypts of patients withulcerative colitis; a more definitive answer to the questionof whether calcium may be effective would require astudy with a larger sample size and/or other study designmodifications.
Introduction
Coborectal cancer is the second most common cause of cancerdeaths in the United States (1). Persons with ulcerative colitis,
especially those with pancobitis, are at increased risk of devel-
oping colon cancer (2). Dietary calcium supplementation hasbeen consistently found to reduce colon cancer occurrence in
experiments in animals (3-9), and the epidemiobogical litera-ture, although inconsistent, on balance provides additional sup-
port for the hypothesis that higher calcium consumption mayreduce colon cancer incidence in humans (10).
It has been hypothesized that calcium may reduce the risk
of colon cancer by normalizing cobonic crypt cell proliferationkinetics (1 1). Several studies (12-26) have reported that, com-
pared to patients at low risk for colon cancer, patients withcolon cancer (12-21) and patients in every category known to
be at higher risk for colon cancer [those with a history ofsporadic adenoma (12-15, 17-21), familial polyposis (16, 22),
or ulcerative colitis (12, 23, 24); those with a family history ofcolon cancer (16, 17, 25); and the elderly (13, 26)], on average,
exhibit in their normal-appearing mucosa both an increasedcobonic epithebiab cell proliferation rate and an extension of the
colon crypt proliferative zone from the lower (basal) 60% of thecrypt to include the upper (buminal) 40% of the crypt. In
patients with previous colon cancer or sporadic adenomas,these changes also predict adenoma recurrence (27, 28). Inbarge bowel tumors in humans, an upward shift in the prolif-
erative zone is found in colon cancers and adenomas but not in
hyperplastic pobyps (29). As reviewed elsewhere (30-32), pro-biferative changes in histologically normal-appearing mucosa
have been shown to be a consequence of both cancer-initiatingand cancer-promoting agents: proliferative changes both pre-
cede and accompany cobonic neoplasms in rodents given chem-icab carcinogens, and a high fat diet produces proliferativechanges in both rodents and humans. Evidence from animalexperiments and preliminary evidence from human studies
strongly suggest that these two proliferation abnormalities, i.e.,
hyperproliferation and upward shift of the proliferation zone,
are reversible biomarkers or precursors for colon neoplasia(30-33). In humans, the two proliferation abnormalities appearto be independent variables (19, 34), and rectal biopsy findings
on both measures reflect those throughout the colon (21 , 35).Calcium administration was found to ameliorate the pro-
liferative changes in rodents (36-38). Several (39-43), but notall (32, 44), small preliminary clinical trials suggested similar
on July 16, 2018. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1022 Calcium Trial in Ulcerative Colitis Patients
effects in humans. More recently, there have been three larger
controlled trials in humans with sporadic adenoma (45-47). Afull-scale (n = 193) trial in sporadic adenoma patients con-ducted by our group concurrently with the present study found
a large, statistically significant, normalizing effect on the pro-liferative zone (45); however, a second full-scale trial (47) didnot, and the third trial (46) did not address this measurement.
Possible mechanisms of action of calcium in normalizing cob-
rectal epithebial cell proliferation and reducing the risk of coloncancer include the binding of calcium with bile acids (thoughtto be promoters of colonic neoplastic change) to form inert
soaps (1 1) and the direct induction by calcium of terminal
differentiation of the cobonic epithebial cells (30-33).There have been no reported randomized clinical trials to
assess the efficacy of higher calcium consumption in normal-izing cell proliferation kinetics in humans with ulcerative co-
litis. To address this need, we conducted a randomized, double-
blind, placebo-controlled clinical trial (n = 31) to determinewhether calcium supplementation will reduce the coborectal
epithelial cell proliferation rate and normalize the distribution
of proliferating cells within colorectal crypts (i.e., shift the zoneof proliferation from one that includes the entire crypt to one
that is confined to the lower 60%, or normal proliferative zone,
of the crypt) in patients with ulcerative colitis.
Materials and Methods
This study was approved by the Committee on Use of HumanSubjects in Research of the University of Minnesota. Writteninformed consent was obtained from each study participant.
Participant Population. Participants were recruited from the
patient population attending a private practice gastroenterobogygroup that performs approximately 60% of all cobonoscopies in
the Minneapolis-St. Paul area. To be eligible for the study,subjects must have been 2 1-74 years of age, in general goodhealth, and capable of informed consent. They must have had a
history of pathology-confirmed ulcerative colitis with diseaseinvolvement that included the rectum; had no contraindications
to calcium supplementation or rectal biopsy procedures; and
had no medical conditions, habits, or medication usage thatwould otherwise interfere with the study as described below.
Specific exclusions included: a history of ever havingtoxic megacolon or other life-threatening complication of ub-cerative colitis, hospitalization for treatment of ulcerative co-litis within the previous 2 years, Crohn’s disease, calcium
supplement use, vegetarian diet, major diet change within theprevious 6 months, supplemental daily intake of vitamin D
greater than 400 IU or vitamin A greater than 10,000 IU,regular antacid use, bile acid-binding resin use, long-term tet-
racycline or indomethacin use, inability to refrain from aspirinuse for 10 days, history of bleeding disorder or current use of
anticoagulant medication, history of endocarditis or artificialheart valve, lithium therapy, current use of thiazide diuretics inamounts greater than the equivalent of 50 mg of hydrochbo-
rothiazide daily, immunosuppression, childbearing potential,renal insufficiency, kidney stones within the previous 20 years,hyper- or hypoparathyroidism, hypo- or hyperthyroidism not
under control, abnormal serum calcium or creatinine levels ateligibility visit, familial polyposis or Gardner syndrome, intes-
tinal malabsorption syndromes, active liver or pancreatic dis-ease, gastrectomy, bowel resection, enema or laxative depend-ence, active peptic ulcer disease, active malignancy other thannonmelanoma skin cancer, cardiovascular or pulmonary disease
that moderately or severely limited activity, narcotic or alcohol
dependence, nondeliberate weight loss of � 10% in the previous
3 months, and less than 80% compliance to a medicationregimen in a 4-week placebo run-in trial.
Clinical Trial Protocol. All age-eligible practice patients whohad been diagnosed with ulcerative colitis were identified as
potential study participants. All patients passing initial chartscreening for eligibility were sent an introductory letter, fob-bowed by a brief telephone interview. Potential participantswere then scheduled for an eligibility visit, at which time theywere interviewed, completed questionnaires, and provided a
blood sample. Their diet was assessed with a semiquantitativefood frequency questionnaire (48). Medical and pathology
records were reviewed. Those eligible entered a 4-week pla-cebo run-in trial. Only participants without significant per-
ceived side effects and who had taken at least 80% of theirtablets were eligible for randomization. Compliance for therun-in was assessed by questionnaire, interview, and pill count.Eligible participants then received their baseline biopsy and, ifstill willing to continue, were randomized (stratified by sex to
ensure balance by sex between treatment groups) to one of two
groups. All involved in the trial, including study personnel,endoscopists, study participants, and laboratory personnel were
blinded to treatment category.Participants (n = 31) were randomly assigned to the two
treatment groups: a placebo-control group (n = 14) and a 2.0 g(n 17) elemental calcium supplementation group. The pla-cebo was free of calcium, magnesium, vitamin D, or chelatingagents. As with our calcium and colorectal epithelial cell pro-liferation in sporadic adenoma patients trial (45), the calcium
tablets were calcium carbonate tablets (OsCal; at the time of thestudy, from Marion Merrill Dow, Inc., Kansas City, MO; nowfrom SmithKiine Beecham, Pittsburg, PA) taken twice dailywith meals (i.e., 5.0 g of calcium carbonate daily). Placebo and
calcium tablets were identical in size, appearance, and taste.The treatment period was 2 months. At the single fob-
bow-up visit 2 months after randomization (baseline), pill-
taking adherence was assessed by questionnaire, interview, andpill count. Participants were instructed to remain on their usualdiet during the study. Factors hypothesized to be related to
colon cell proliferation were assessed at baseline, and severalwere reassessed at the follow-up (final) visit.
Rectal biopsies were taken from study participants at ran-dom assignment to their treatment groups (baseline) and againat 2 months after onset of treatment (follow-up). The rectalbiopsy procedure was performed without the participant first
taking a laxative, enema, or other bowel-cleansing preparation.Three biopsies that appeared grossly adequate were taken fromnormal-appearing mucosa of the rectum 10 cm above the level
of the anus.
Laboratory Protocol. The laboratory protocol is described inmore detail elsewhere (45). Briefly, the biopsies were stretchedout flat, lumen side up, on bibulous paper; fixed in 70%ethanol; processed in a tissue processor; embedded in a paraffin
block; cut with a microtome so that crypts were longitudinallysectioned from base to lumen (section bevels were 3 p�m thickand taken 50 p.m apart); and mounted on microscope slides. Tolabel proliferating cells, slides were then subjected to immu-
nohistochemical analysis for PCNA3 as summarized: slideswere deparaffinized; rinsed; received a blocking agent, 5%
normal horse serum (diluted in PBS; Vector Laboratories,
Burbingame, CA), followed by PC-b clone PCNA antibody
3 The abbreviations used are: PCNA, proliferating cell nuclear antigen; LI,
labeling index; BrdUrd, 5-bromodeoxyuridine.
on July 16, 2018. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

CancerEpidemiology, Biomarkers & Prevention 1023
(diluted 1:200 with PBS; Oncogene Science, Cambridge, MA);
rinsed; received the secondary antibody, rabbit antimouse IgG
(diluted 1 :200 with PBS; DAKO Corp., Carpinteria, CA);rinsed; received the endogenous peroxide blocker, 0.3% H2O2;
rinsed; received the tertiary agent, avidin-biotin complex (Vec-tor Standard Kit at half strength); rinsed; developed by immer-
sion with the chromogen 3,3’-diaminobenzidine (Sigma Chem-ical Co., St. Louis, MO), in a 1 mg/mb solution with 0.003%
H2O2; rinsed; counterstained with Harris’s hematoxybin; dehy-drated; and coversbipped.
The BrdUrd uptake immunohistochemical method of iden-
tifying S-phase cells and measuring cell proliferation, as de-scribed elsewhere (45), was also used; however, the labeling
failure rate using this method in the ulcerative colitis patients inthe present study was 100% (compared to 15% in our concur-
rently studied sporadic adenoma patients; Ref. 45).
Protocol for Scoring Colon Crypt Sections on Slide. Thebiopsy scoring protocol is described in more detail elsewhere
(45). Briefly, colon crypts longitudinally sectioned from base to
lumen were analyzed. The total number of cells and number oflabeled cells for each crypt scored were counted, and the cell
count position of each PCNA-babeled cell within a crypt was
recorded. A scorabbe crypt was defined as an intact crypt
extending from the muscubaris to the lumen. Only whole crypts
were counted. Countable cells were defined as crypt cells in linein a single column of nuclei that extended from base to lumen.
An unlabeled cell was defined as a cell with a blue nucleus. Aweakly labeled cell (a cell in late G, or early G2) was defined
as a cell with a nucleus that was light brown in color (1-2 �
intensity). A strongly labeled cell (a cell in S-phase) was
defined as a cell with a nucleus that was dark brown in color(3-4k intensity). These cells tended to stand out prominently
on the slides. The slide reader began with the first PCNA-
stained slide on the participant. The slide was oriented in a
standardized fashion, and the section levels on the slides wereviewed in sequence using light microscopy. Scoring was begun
at the first complete crypt found. The reader moved through asection level from left to right until a scorable crypt waslocated. Crypts were always counted under X400 magnifica-
tion. During counting, a number was entered into a computer
data entry program that permitted analysis of the cell countposition and other characteristics of each cell. Each cell was
identified as an unlabeled cell, a weakly labeled cell, or astrongly labeled cell. The crypt base center cell was also iden-
tified. The goal was to score a minimum of 10 crypts.The number of labeled cells in the crypt was determined
by direct count of all labeled cells in the crypt. The position or
height of a labeled cell was assigned by cell count number from
the center cell of the crypt base.One slide reader scored slides throughout the study. Slides
from a 10% sample of biopsies scored by the reader wereresubmitted in a blinded manner to be reread to determine
intrarater reliability.
Statistical Analysis. Treatment groups were assessed for com-
parability of characteristics at baseline and at final follow-up by
x2 test for categorical variables and by analysis of covariancefor continuous variables; sex was included as a covariate.
Reader reliability was analyzed using intraclass correlation
coefficients.The overall cell proliferation rate, the LI, was calculated
for each biopsy by dividing the total number of labeled cellscounted (LC) by the total number of cells counted (TC) from allscored crypts from the biopsy and multiplying by 100% (100%x LCTTC; Ref. 18). Crypts were subdivided horizontally by cell
count height into five equal-sized compartments (18). A meas-
ure of the distribution of proliferating cells in the crypt, the
proportion of proliferating cells that were in the upper (luminal)
40% of the crypt (#{248}h)’ was calculated on each biopsy bydividing the number of labeled cells counted in the upper 40%of the crypt (LC4_5) by the total number oflabebed cells counted
(LC) and multiplying by 100% (#{248}h= 100% X LC4_5/LC; Ref.16). Each of these measures was calculated separately using
both the 3-4k labeled cells (strongly labeled cells) as thelabeled cells and the l-4� labeled cells (all labeled cells) as the
labeled cells.Mean coborectal epithelial cell proliferation parameters
were calculated for each treatment group at baseline and at the
2-month follow-up. Changes in proliferation parameters over
time were computed within each treatment group as person-
specific follow-up minus baseline differences, and then meanchanges were calculated and compared using analysis of co-variance (with sex as a covariate). Analyses were performed on
both the raw data and on the data transformed to improvenormality as described previously (45). However, because theresults of the analyses did not differ substantially, for simplic-ity, only the analyses on the raw data are presented herein.
In addition, the baseline cell proliferation data from both
treatment groups were combined and compared with those fromthe sporadic adenoma patients accrued during the same time
period in our concurrently conducted calcium and colorectalepithelial cell proliferation trial (45). Mean age- and sex-adjusted cell proliferation values were computed and comparedusing analysis of covariance.
Results
All patients were white, none had a history of having anadenoma, and none had a history of a first-degree relative withcolon cancer. Treatment groups did not differ significantly on
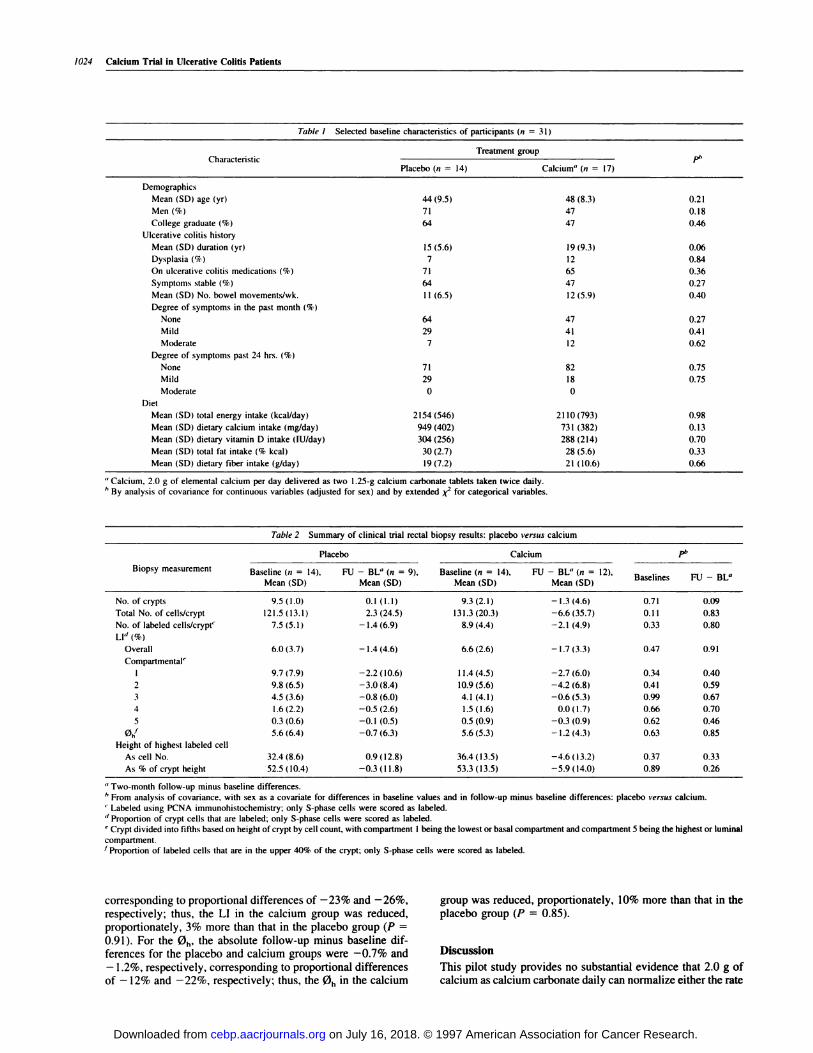
any other characteristics measured at baseline (for examples,see Table 1) or at the end of the study.
Biopsies that were scorable were obtained on 28 partici-
pants at baseline and 24 at 2 months; scorable biopsies wereobtained at both baseline and 2 months on 21 participants. A
total of 85% of biopsies had one or more scorable crypts andadequate labeling, and 84% had eight or more scorable crypts
and adequate labeling. Treatment groups did not differ signif-icantly at baseline on the mean number of crypts scored perparticipant, on crypt characteristics, or on cell proliferation
characteristics (Table 2). As shown in Table 3, levels of cellproliferation in the ulcerative colitis patients were higher thanthose found in the adenoma patients in our concurrent trial in
adenoma patients. The S-phase and all-labeled cell measure-ment alternatives for each proliferative parameter were highly
correlated, and analyses using either closely mirrored the other.
Consequently, for succinctness, only the more traditionallyreported S-phase measures are presented hereafter.
Adherence to visit attendance was 100%. The mean pro-
portion of pills taken in each group was 97%, and over 92% ofall participants in each group took �80% of their pills. Therewere no treatment or biopsy complications. Intrareader reliabil-
ity (intraclass correlation coefficient) for biopsy slide scoring
was 0.89.Analyses of clinical trial biopsy results by treatment group
are summarized in Table 2. There were no substantial or sta-tistically significant differences in follow-up minus baselinedifferences between the two treatment groups. For the LI, theabsolute follow-up minus baseline differences for the placeboand calcium groups were - 1.4% and - 1.7%, respectively,
on July 16, 2018. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
1024 Calcium Trial in Ulcerative Colitis Patients
Table 1 Selected baseline characteristics of participants (n 31)
Treatment groupCharacteristic
Placebo (n = 14) Calcium” (n = 17)Pb
Demographics
Mean (SD) age (yr) 44 (9.5) 48 (8.3) 0.21
Men (%) 71 47 0.18
College graduate (%) 64 47 0.46
Ulcerative colitis history
Mean (SD) duration (yr) 15 (5.6) 19 (9.3) 0.06
Dysplasia (%) 7 12 0.84
On ulcerative colitis medications (%) 71 65 0.36
Symptoms stable (%) 64 47 0.27
Mean (SD) No. bowel movements/wk. 1 1 (6.5) 12 (5.9) 0.40
Degree of symptoms in the pa.st month (%)
None 64 47 0.27
Mild 29 41 0.41
Moderate 7 1 2 0.62
Degree of symptoms past 24 hrs. (%)
None 71 82 0.75
Mild 29 18 0.75
Moderate 0 0
Diet
Mean (SD) total energy intake (kcal/day) 2154 (546) 21 10 (793) 0.98
Mean (SD) dietary calcium intake (mg/day) 949 (402) 731 (382) 0.13
Mean (SD) dietary vitamin D intake (lU/day) 304 (256) 288 (214) 0.70
Mean (SD) total fat intake (% kcal) 30 (2.7) 28 (5.6) 0.33
Mean (SD) dietary fiber intake (g/day) 19 (7.2) 21 (10.6) 0.66
“ Calcium, 2.0 g of elemental calcium per day delivered as two 1 .25-g calcium carbonate tablets taken twice daily.
I, By analysis of covariance for continuous variables (adjusted for sex) and by extended � for categorical variables.
Table 2 Summary of clinical trial rectal biopsy results: placebo versus calcium
Placebo Calcium Pb
B F � � BL�
ase ifl�S -
Biopsy measurement Baseline (n = 14), Hi - BL” (n = 9), Baseline (n = 14), FU - BL” (n = 12),
Mean (SD) Mean (SD) Mean (SD) Mean (SD)
No. ofcrypts 9.5(1.0) 0.1 (1.1) 9.3(2.1) -1.3(4.6) 0.71 0.09
Total No. of cells/crypt 121.5 (13.1) 2.3 (24.5) 131.3 (20.3) -6.6 (35.7) 0.1 1 0.83
No. of labeled cells/cryp( 7.5 (5. 1 ) - 1 .4 (6.9) 8.9 (4.4) - 2. 1 (4.9) 0.33 0.80
LI” (%)
Overall 6.0 (3.7) - 1.4 (4.6) 6.6(2.6) - 1.7 (3.3) 0.47 0.91
Compartmental�
I 9.7 (7.9) -2.2 (10.6) 1 1.4 (4.5) -2.7 (6.0) 0.34 0.40
2 9.8 (6.5) -3.0 (8.4) 10.9 (5.6) -4.2 (6.8) 0.41 0.59
3 4.5 (3.6) -0.8 (6.0) 4.1 (4.1) -0.6 (5.3) 0.99 0.67
4 1.6 (2.2) -0.5 (2.6) 1.5 (1.6) 0.0 (1.7) 0.66 0.70
5 0.3 (0.6) -0.1 (0.5) 0.5 (0.9) -0.3 (0.9) 0.62 0.46
0h� 5.6 (6.4) -0.7 (6.3) 5.6 (5.3) - I .2 (4.3) 0.63 0.85
Height of highest labeled cell
As cell No. 32.4(8.6) 0.9(12.8) 36.4(13.5) -4.6(13.2) 0.37 0.33
As % of crypt height 52.5 (10.4) -0.3 (1 1.8) 53.3 (13.5) -5.9 (14.0) 0.89 0.26
“ Two-month follow-up minus baseline differences.h From analysis of covariance, with sex as a covariate for differences in baseline values and in follow-up minus baseline differences: placebo versus calcium.
C Labeled using PCNA immunohistochemistry; only S-phase cells were scored as labeled.
d Proportion of crypt cells that are labeled; only S-phase cells were scored a.s labeled.
� Crypt divided into fifths based on height of crypt by cell count, with compartment 1 being the lowest or basal compartment and compartment 5 being the highest or luminal
compartment.
I Proportion of labeled cells that are in the upper 40% of the crypt; only S-phase cells were scored as labeled.
corresponding to proportional differences of -23% and -26%, group was reduced, proportionately, 10% more than that in the
respectively; thus, the LI in the calcium group was reduced, placebo group (P = 0.85).proportionately, 3% more than that in the placebo group (P
0.91). For the 0h’ the absolute follow-up minus baseline dif- �ferences for the placebo and calcium groups were -0.7% and D1SCU5S1on
- 1.2%, respectively, corresponding to proportional differences This pilot study provides no substantial evidence that 2.0 g ofof - 12% and -22%, respectively; thus, the 0h in the calcium calcium as calcium carbonate daily can normalize either the rate
on July 16, 2018. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 1025
Table 3 Comparison of ag e-, sex-adjusted colorectal epith dial cell p roliferation measurements in ulcerative colitis versus sporadic aden oma patients
Biopsy measurementSporadic adenoma (n =
M� (SE)
1 19) Ulcerative colitis (n = 28)
Mean (SE)
Proportional
difference” (%)
Pb
S-phase LI’ (%)
All-labeled cell LI” (%)
S-phase #{248}he(%)
All-labeled cell #{248}h1(’�’)
4.3 (0.3)
16.1 (0.8)
5.6 (0.6)
10.1 (0.8)
6.7 (0.6)
31.1 (2.8)
7.8 (1.5)
12.0 (1.9)
56
93
39
19
<0.0001
<0.0001
0.21
<0.0001
“ 100% x � - � cotiu,’Uacienoma) similarly for 0h�
b From analysis of covariance; adjusted for age and sex.
C Proportion of crypt cells that are labeled; only S-phase cells were scored as labeled.
d Proportion of crypt cells that are labeled; all labeled cells were scored as labeled.
e Proportion of labeled cells that are in upper 40% of the crypt; only S-phase cells were scored as labeled.
I Proportion of labeled cells that are in the upper 40% of the crypt; all labeled cells were scored as labeled.
or distribution of proliferating cells in the colon crypts of
patients with ulcerative colitis over a 2-month treatment period.However, it must be emphasized that the sample size was small
and the statistical power limited; thus, the findings may be due
to chance. Other possible reasons for our findings include that
(a) calcium may indeed have no substantial effect on colon cellproliferation in ulcerative colitis patients, because the colon
carcinogenic processes in ulcerative colitis patients differ fromthose in sporadic adenoma patients in ways that involve or do
not involve calcium, and (b) in contrast to our findings foradenoma patients, the calcium dose or duration may have been
insufficient for efficacy. Given the suggestion of a 3% propor-tionalby greater drop in the LI and the 10% proportionately
greater drop in the 0h’ as well as the caveats about sample sizeand chance and calcium dose and duration, the possibility that
calcium may beneficially contribute to a mubtifactorial ap-proach to normalizing coborectal epithelial cell proliferationand reducing the risk of colon cancer in ulcerative colitis
patients cannot be excluded.If the true possible treatment effects were the sizes esti-
mated by this pilot study, a sample size of 718 per treatment
group would have been required to detect the difference in theLI at P � 0.05, and 368 per group would have been required todetect the difference in the 0h#{149} To detect perhaps more mean-ingful proportional differences of 20% in the LI and #{216}�,,the
sample sizes would have needed to be 40 and 89 per group,respectively.
Other findings from this study include: (a) both the LI and
0h in ulcerative colitis patients are, on average, higher thanthose in sporadic adenoma patients; (b) investigating coborectal
epithelial cell proliferation in ulcerative colitis patients in gen-erab, and in clinical trials and using PCNA in particular, isfeasible; (c) the BrdUrd method for labeling proliferating colon
crypt cells in ulcerative colitis is ineffective when used in the
usual manner (the cause of this is unknown); and (d) theinadequate biopsy rate in the present study was 15% (compared
to 5% in our sporadic adenoma patients; Ref. 45), a factor thatshould be considered in deciding on sample sizes for colorectal
epithelial cell proliferation studies in ulcerative colitis patients.The present study has several strengths and limitations.
The most obvious limitation is, as pointed out above, the smallsample size and the consequent increased robe for chance in thelikelihood of detecting (or not detecting) a treatment effect. Thesmall sample size also precluded subgroup analyses. Another
limitation, common to nearby all coborectal epithebial cell pro-liferation trials, is that the only site sampled was the rectum;
thus, treatment effects higher in the colon cannot be ruled out.This is potentially important, because the physiology of the
colon and rectum and the epidemiology of colon and rectalcancer differ (2). The strengths of the study are that it is, to our
knowledge, the first clinical trial of calcium and coborectal
epithelial cell proliferation in ulcerative colitis patients; thehigh bevel of protocol adherence; the strict quality control and
consequent high level of biopsy-scoring reliability; and, per-haps most importantly, the randomized, controlled design.
There have been no previous reports of trials of calciumand coborectab epithelial cell proliferation; however, as re-viewed extensively elsewhere (49), there have been 14 previous
such trials in patients without inflammatory bowel disease whowere at increased risk for colon cancer (32, 39-47, 50-53).The results of these studies are inconsistent with one another:
the majority of the uncontrolled trials found mostly large de-
creases in the LI and 0h’ the small controlled trials yieldedmixed results, and the full-scale controlled trials found small(not statistically significant) proportional decreases in the LI of
about 3%. The full-scale trial in sporadic adenoma patientsconducted by our group concurrently with the present study
found a statistically significant proportional decrease of 100%
in the 0h (45), but a second full-scale trial (47), a trial withmore methodological problems (49), did not.
There have been no previous reports of comparisons be-
tween coborectal epithelial cell proliferation in ulcerative colitis
patients and sporadic adenoma patients, but three small studies(12, 23, 24) compared ulcerative colitis patients with normalpatients. All three studies used tritiated thymidine uptake and
microautoradiography as the S-phase cell labeling method, re-ported the LI but not the 0h’ and did not report biopsy-scoringreliability. One study compared eight normal subjects to four
patients with ulcerative colitis and found a 173% proportion-
ately higher LI in the ulcerative colitis patients (9.5% versus
25.9%; SE and P not given; Ref. 24). A second study comparedfour normal subjects with nine ulcerative colitis patients and
found a 3% proportionately lower LI in the ulcerative colitis
patients (1 1.1% versus 11.4%; SE and P not given; Ref. 23).The third study compared eight normal subjects with seven
ulcerative colitis patients and found a statistically significant168% proportionately higher LI in the ulcerative colitis patients
(9.5% versus 25.5%; SE 1 . 1 and 1 .8, respectively; Ref. 12).Taken altogether, the results of the present and past studiessuggest that, on average, ulcerative colitis patients may have
higher levels of colorectal epithelial cell proliferation than do
normal or sporadic adenoma patients.In summary, the sample size in this preliminary study does
not allow a definitive answer to the question of whether calcium
can reduce coborectab epithelial cell proliferation in ulcerativecolitis patients; therefore, although the results suggest that
calcium may have a modest effect, conservatively, they cannot
be considered to support the hypothesis. This study suggeststhat ulcerative colitis patients have higher levels of coborectab
epitheliab cell proliferation than do sporadic adenoma patients;
on July 16, 2018. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1026 Calcium Trial in Ulcerative Colitis Patients
confirms the feasibility of colorectal epithelial cell proliferationtrials in ulcerative colitis patients; and points out the futility of
using BrdUrd labeling in ulcerative colitis patients, the feasi-
bility of using PCNA labeling in these patients, the need toconsider a biopsy inadequacy rate of approximately 15%, andthe importance of randomization and control groups in chemo-
prevention trials of colorectal epithelial cell proliferation or
other cancer-related end points.
Acknowledgments
We thank Colleen Forster for help with developmental work to adapt the PCNA
labeling technique for large-scale studies; Patricia Winkels for advice and work
on biopsy procurement and initial handling methods: Bryan Randall for devel-
opment of the computer software necessary to score biopsy slides processed by
the PCNA technique: and the physicians of Digestive Healthcare, PA for advice
and work on biopsy procurement methods and implementing epidemiological
studies at the university-private community interface that measure colorectal
epithelial cell proliferation.
References
I . Boring, C. C., Squires, T. S., Tong. 1., and Montgomery, S. Cancer statistics,
1994. CA Cancer J. Clin., 44: 7-26, 1994.
2. Potter, J. D.. Slattcry. M. L., Bostick, R. M., and Gapstur, S. M. Colon cancer:
a review of the epidemiology. Epidemiol. Rev., 15: 499-545, 1993.
3. Appleton. G. V. N.. Davies, P. W., Bristol, J. B., and Williamson, R. C. N.
Inhibition of intestinal carcinogenesis by dietary supplementation with calcium.
Br. J. Surg.. 74: 523-525. 1987.
4. Pence, B. C., and Buddingh, F. Inhibition of dietary fat-promoted colon
carcinogenesis in rats by supplemental calcium or vitamin D3. Carcinogenesis
(Lond.), 9: 187-190, 1988.
5. Behling, A. R., Kaup, S. M., Choquette, L. L., and Greger, J. L. Lipid
absorption and intestinal tumour incidence in rats fed on varying levels of calcium
and butterfat. Br. J. Nutr.. 64: 505-513, 1990.
6. Wargovich, M. J.. Allnutt, D., Palmer, C., Anaya, P., and Stephens, L. C.
Inhibition of the promotional phase of azoxymethane-induced colon carcinogen-
esis in the F344 rat by calcium lactate: effect of simulating two human nutrient
density levels. Cancer Lett., 53: 17-25, 1990.
7. McSherry, C. K., Cohen, B. I., Bokkenhcuser, V. D., Mosbach, E. H., Winter,
J., Matoba, N.. and Scholes, J. Effects of calcium and bile acid feeding on colon
tumors in the rat. Cancer Res., 49: 6039-6043, 1989.
8. Sitrin, M. D., Halline. A. G., Abrahams, C., and Brasitus, T. A. Dietary
calcium and vitamin D modulate 1.2-dimethylhydrazine-induced colonic carci-
nogenesis in the rat. Cancer Res., 51: 5608-5613, 1991.
9. Kaskare, M. R., Clark, T. D., and Glauert, H. P. Effect of dietary calcium on
colon carcinogencsis induced by a single injection of 1,2-dimethylhydrazine in
rats. J. Nutr., 121: 568-577. 1991.
10. Bostick, R. M.. Potter, J. D., Sellers, T. A.. McKenzie, D. R., Kushi, L. H.,
and Folsom, A. R. Relation of calcium, vitamin D, and dairy food intake to
incidence of colon cancer among older women. Am. J. Epidemiol., 137: 1302-
1317, 1993.
I I . Newmark, H. L., Wargovich, M. J., and Bruce, W. R. Colon cancer and
dietary fat, phosphate and calcium: a hypothesis. J. NatI. Cancer Inst., 72:
1323-1325. 1984.
I 2. Bleiberg, H., Buyse, M., and Galand, P. Cell kinetic indicators of premalig-
nant stages of colorectal cancer. Cancer (Phila.), 56: 124-129, 1985.
13. Paganelli, G. M., Santucci, R., Biasco, G.. Miglioli, M., and Barbara, L.Effect of sex and age on rectal cell renewal in humans. Cancer Leti., 53: 1 17-121,
I 990.
14. Paganelli. G. M., Biasco, G., Santucci, R., Brandi, G., Lalli, A. A., Miglioli,
M., and Barbara, L. Rectal cell proliferation and colorectal cancer risk level inpatients with nonfamilial adenomatous polyps of the large bowel. Cancer (Phila.),
68: 2451-2454, 1991.
IS. Ponz de Leon, M., Roncucci, L., Di Donato, P., Tassi, L., Smerieri, 0.,
Grazia, M., Malagoli. A. G., Dc Maria, D., Antonioli, A., Chahin, N., Perini, M.,
Rigo, G.. Barberini, G., Manenti, A., Biasco, G., and Barbara, L Pattem ofepithclial cell proliferation in colorectal mucosa of normal subjects and of patients
with adenomatous polyps or cancer of the large bowel. Cancer Rca., 48: 412 1-
4126, 1988.
16. Lipkin. M., Blattner, W. E., Fraumeni, J. F., Lynch, H. T., Deschner, E., andWinawer, S. Tritiated thymidine (#{248}p’#{248}h) labeling distribution as a marker for
hereditary predisposition to colon cancer. Cancer Res., 43: 1899-1904, 1983.
17. Lipkin, M., Uehara, K., Winawer, S., Sanchez, A., Bauer, C., Phillips, R.,
Lynch, H. T., Blaitner, W. A., and Fraumeni, J. F., Jr. Seventh-Day Adventist
vegetarians have quiescent proliferative activity in colonic mucosa. Cancer Left.,
26: 139-144, 1985.
18. Lipkin, M., Enker, W. E., and Eilers, G. A. M. Tritiated-thymidine labeling
of rectal epithelial cells in “non-prep” biopsies of individuals at increased risk for
colonic neoplasia. Cancer Leu., 37: 155-161, 1987.
19. Risio, M., Lipkin, M., Candelaresi, G., Bertone, A., Coverlizza, S., and
Rossini, F. Correlations between rectal mucosa cell proliferation and the clinical
and pathological features of nonfamilial neoplasia of the large intestine. Cancer
Res., 5!: 1917-1921, 1991.
20. Stadler, J., Yeung, K. S., Furrer, R., Marcon, N., Himal, H. S., and Bruce,W. R. Proliferative activity of rectal mucosa and soluble fecal bile acids in
patients with normal colons and in patients with colonic polyps or cancer. Cancer
Lets., 38: 315-320, 1988.
21 . Terpstra, 0. T., Strautenstein, M. V., Dees, J., and Eilers, 0. A. M. Abnormal
pattem of cell proliferation in the entire mucosa of patients with colon adenomaor cancer. Gastroenterology, 92: 704-708, 1987.
22. Deschner, E. E., Lewis, D. M., and Lipkin, M. In vitro study of human rectal
epithelial cells. I. Atypical zone of H3 thymidine incorporation in mucosa of
multiple polyposis. J. Clin. Invest., 42: 1922-1928, 1963.
23. Biasco, G., Lipkin, M., Minarini, A., Higgins, P., Miglioli, M., and Barbara,
L. Proliferative and antigenic properties of rectal cells in patients with chronic
ulcerative colitis. Cancer Rca., 44: 5450-5454, 1984.
24. Bleiberg, H., Mainguet, P., Galand, P., Chretien, J., and Dupont-Mairesse, N.
Cell renewal in the human rectum: in vitro autoradiographic study on active
ulcerative colitis. Gastroenterology, 58: 851-855, 1970.
25. Genies, H., Gillin, J. S., Zimbalist, E., Urmacher, C., Lipkin, M., and
Winawer, S. J. Expansion of the epithelial proliferative compartment and fre-
quency of adenomatous polyps in the colon correlate with the strength of familyhistory of colorectal cancer. Cancer Res., 53: 279-282, 1993.
26. Roncucci, L., Ponz de Leon, M., Scalmati, A., Malgoli, G., Pratissoli, S.,
Perini, M., and Chahin, N. J. The influence of age on colonic epithelial cellproliferation. Cancer (Phila.), 48: 235-245, 1988.
27. Anti, M., Marra, G., Armelao, F., Percesepe, A., Ficarelli, R., Ricciuto,
G. M., Valenti, A., Rapaccini, G. L., Dc Vitis, I., D’Agnostino, G., Brighi, S., and
Vecchio, F. M. Rectal epithelial cell proliferation pattems as predictors of
adenomatous colorectal polyp recurrence. Gut, 34: 525-530, 1993.
28. Scalmati, A., Roncucci, L., Ghidini, G., Biasco, G., and Ponz de Leon, M.Epithelial cell kinetics in the remaining colorectal mucosa after surgery for cancer
of the large bowel. Cancer Res., 50: 7937-7941, 1990.
29. Risio, M., Coverlizza, M., Ferrari, A., Candelaresi, G., and Rossini, F.
Immunohistochemical study of epithelial cell proliferation in hyperplastic polyps.
adenomas, and adenocarcinomas of the large bowel. Gastroenterology, 94: 899-
906, 1988.
30. Newmark, H. L., and Lipkin, M. Calcium, vitamin D, and colon cancer.
Cancer Res., 52 (Suppl.): 2067s-2070s. 1992.
31. Wargovich, M. J., and Baer, A. R. Basic and clinical investigations of dietary
calcium in the prevention of colorectal cancer. Prey. Med., /8: 672-679, 1989.
32. Bostick, R. M., Potter, J. D., Fosdick, L., Grambsch, P., Lamps, J. W., Wood,
J. R., Louis, T. A., Ganz, R., and Grandits, 0. A. Calcium and colorectal epithelial
cell proliferation: a preliminary randomized, double-blinded, placebo-controlled
clinical trial. J. NatI. Cancer Inst., 85: 132-141, 1993.
33. Rozen, P. An evaluation of rectal epithelial proliferation measurement as
biomarker of risk for colorectal neoplasia and response in intervention studies.
Eur. J. Cancer Prey., I: 215-224, 1992.
34. Grambsch, P. M., Randall, B. L., Bostick, R. M., Potter, J. D., and Louis,
T. A. Modeling the labeling index distribution: an application of functional dataanalysis. J. Am. Stat. Assoc., 90: 813-821, 1995.
35. Potten, C. S., Kellett, M., Roberts, S. A., Rew, D. A., and Wilson, G. D.
Measurement of in vivo proliferation in human colorectal mucosa using bromode-
oxyuridine. Gut, 33: 71-81, 1992.
36. Wargovich, M. J., Eng, V. W. S., and Newmark, H. Calcium inhibits the
damaging and compensatory proliferative effects of fatty acids on mouse colonepithelium. Cancer Lett., 23: 253-258, 1984.
37. Bird, R. P., Schneider, R., Stamp, D., and Bruce, W. R. Effect of dietary
calcium and cholic acid on the proliferative indices of murine colonic epithelium.
Carcinogenesis (Land.), 7: 657-661, 1986.
38. Wargovich, M. J., Eng, W. W. S., Newmark, H. L., and Bruce, W. R. Calcium
ameliorates the toxic effect of deoxycholic acid on colonic epithelium. Carcino-
genesis (Lond.), 4: 1205-1207, 1983.
39. Lipkin, M., and Newmark, H. Effect of added dietary calcium on colonic
epithelial cell proliferation in subjects at high risk for familial colonic cancer.
N. EngI. J. Med., 313: 1381-1384, 1985.
on July 16, 2018. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 1027
40. Buset, M., Lipkin, M., Winawer, S., Swaroop, S., and Friedman, E. Inhibition
of human colonic epithelial cell proliferation in vivo and in vitro by calcium.
Cancer Res., 46: 5426-5430, 1986.
41. Rozen, P., Fireman, A., Fine, N., Wax, Y., and Ron, E. Oral calcium
suppresses increased rectal epithelial proliferation of persons at risk of colorectal
cancer. Gut, 30: 650-655, 1989.
42. Lipkin, M., Friedman, E., Winawer, S. J., and Newmark, H. Colonic epithe-
hal cell proliferation in responders and non-responders to supplemental dietary
calcium. Cancer Res., 49: 248-254, 1989.
43. Wargovich, M. J., Isbell, G., Shabot, M., Winn, R., Lanza, F., Hochman, L.,
Larson, E., Lynch, P., Roubein, L., and Levin, B. Calcium supplementation
decreases rectal epithelial cell proliferation in subjects with sporadic adenoma.
Gastroenterology, 103: 92-97, 1992.
44. Gregoire, R., Stern, H. S., Yeung, K. S., Stadler, J., Langley, S., Furrer, R.,
and Bruce, W. R. Effect of calcium supplementation on mucosal cell proliferationin high risk patients for colon cancer. Gut, 30: 376-382, 1989.
45. Bostick, R. M., Fosdick, L., Wood, J. R., Grambsch, P., Grandits, G. A.,
Lillemoc, T. J., Louis, T. A., and Potter, J. D. Calcium and colorectal epithelial
cell proliferation in sporadic adenoma patients: a randomized, double-blinded,
placebo-controlled clinical trial. J. Nail. Cancer Inst., 87: 1307-1315, 1995.
46. Armitage, N. C., Rooney, P. 5., Gifford, K-A., Clarke, P. A., and Hardcastle,
J. D. The effect of calcium supplements on rectal mucosal proliferation. Br. J.
Cancer, 71: 186-190, 1995.
47. Baron, J. A., Tosteson, T. D., Wargovich, M. J., Sandler, R., Mandel, J.,
Bond, J., Haile, R., Summers, R., van Stolk, R., Rothsstein, R., and Weiss, J.
Calcium supplementation and rectal mucosal proliferation: a randomized con-
trolled trial. J. NatI. Cancer Inst., 87: 1303-1307, 1995.
48. Willett, W. C., Sampson, L., Browne, M. L., Stampfer, M. J., Rosner, B.,Hennekens, C. H., and Speizer, F. E. The use of a self-administered questionnaire
to assess diet four years in the past. Am. J. Epidemiol., 127: 188-199, 1988.
49. Bostick, R. M. Human studies of calcium supplementation and colorectal
epithelial cell proliferation. Cancer Epidemiol. Biomarkers Prey., 6: 971-980,
1997.
50. O’Sullivan, K. R., Mathias, P. M., Beaffie, S., and O’Morain, C. Effect of oral
calcium supplementation on colonic crypt cell proliferation in patients with
adenomatous polyps of the large bowel. Eur. J. Gastroenterol. Hepatol., 5: 85-89,
1993.
51. Stem, H. S., Gregoire, R. C., Kashtan, H., Stadler, J., and Bruce, R. W.
Long-term effects of dietary calcium on risk markers for colon cancer in patients
with familial polyposis. Surgery (St. Louis), 108: 528-533, 1990.
52. Barsoum, G. H., Hendrickse, C., Winslet, M. C., Youngs, D., Donovan, I. A.,
Neoptolemos, J. P., and Keighley, M. R. B. Reduction of mucosal crypt cell
proliferation in patients with colorectal adenomatous polyps by dietary calcium
supplementation. Br. J. Surg., 79: 581-583, 1992.
53. Cats, A., Kleibeuder, J. H., van der Meer, R., Kuipers, F., Sluiter, W. J.,
Hardonk, M. J., Oremus, E. T. H. G. J., Mulder, N. H., and de Vries, E. G. E.
Randomized, double-blinded, placebo-controlled intervention study with supple-
mental calcium in families with hereditary nonpolyposis colorectal cancer. J. Natl.
Cancer Inst., 87: 598-603, 1995.
on July 16, 2018. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1997;6:1021-1027. Cancer Epidemiol Biomarkers Prev R M Bostick, M Boldt, M Darif, et al. colitis.Calcium and colorectal epithelial cell proliferation in ulcerative
Updated version
http://cebp.aacrjournals.org/content/6/12/1021
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/6/12/1021To request permission to re-use all or part of this article, use this link
on July 16, 2018. © 1997 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from





























