Embed Size (px)
Citation preview

7/20/2015
1
Calcium and Phosphate
Myles Wolf, MD, MMSc
The “Players”
ORGANS:
•Parathyroid
•Bone
•Gut
•Kidney
HORMONES:
•Parathyroid Hormone (PTH)
•(PTH-related Peptide)
•Calcidiol (25-OH-D3)
•Calcitriol (1,25-OH-D3)
•Fibroblast Growth Factor-23
•Klotho
2
Calcium
•Needed for skeleton
•Excitable tissues
•Action potentials
•Cardiac and muscle contractility
3
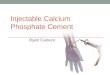
Calcium balance
4Goltzman D. Endotext
GI absorption: ~20%
Renal reabsorption: ~98%
FeCa: ~2%

7/20/2015
2
Intestinal absorption of calcium
5Bikle, D. Endotext
Transporters are highly dependent
on 1,25D
Tubular handling of calcium: TAL
6Unikowski B. http://alexandria.healthlibrary.ca
Inhibitors: furosemide, activation of CaSR
Tubular handling of calcium: DCT
7
Unikowski B. http://alexandria.healthlibrary.ca
Phosphate
•Phospholipid bilayers
•Cell signaling
•Glycolysis
•ATP
•DNA, RNA synthesis
•Unloading O2 (2,3-BPG)
8

7/20/2015
3
Phosphate Balance
Hruska KA et al. Kidney International (2008) 74, 148–157
Renal reabsorption: ~85-90%
FeP: ~10-15%
Serum P=40 mg/l; GFR 150L/d
800 mg/6000 mg = 13%
GI absorption: ~67%
9
Intestinal Phosphate Absorption
• Linear absorption, nonsaturable function of intake
• Approximately 60-75% of intake
• Primarily in small intestine
• 1,25(OH)2D3 stimulates absorption via NaPi2b
• Most phosphate absorption vitamin D independent
via paracellular transport
10
Prie D et al. Kidney International (2009) 75, 882-889.
Renal Phosphate Handling: Proximal Tubule
Apical
Basolateral
11
Main sodium-phosphate co-transporters
• Gut: NPT2b
− Active transport of phosphate
− Less important than passive phosphate transport
− Human deletion has no phosphate phenotype
• Kidney: NPT2a, NPT2c
− In PCT
− NPT2a mutations: Fanconi syndrome
− NPT2c mutations: HHRH syndrome
− Relative roles vary in mammalian species
12

7/20/2015
4
PTH
• Primarily regulates: ionized calcium
• Main stimulus: hypocalcemia
• Main effects: raise serum calcium
− Stimulates bone resorption
− Stimulates 1,25D production (CYP27B1)
− Inhibits CYP24
− Inhibits calciuria
− Stimulates phosphaturia
• Hyperphosphatemia stimulates parathyroid gland hyperplasia
13
1,25-dihydroxyvitamin D
• Primarily regulates: gut mineral absorption
• Main stimulus: PTH
• Main inhibitor: FGF23
• Main effects:
− Augment gut calcium absorption
− Augment gut phosphate absorption
− Feedback inhibition to suppress PTH
− Stimulates FGF23
− Stimulates 24-hydroxylase
14
Vitamin D synthesis and hydroxylases
15Bikle, D. Endotext
Vitamin D Stores and PTH
PT
H (
pg
/ml)
25 (OH) D (ng/ml)
inflection•N = 1,536 menopausal women on
osteoporosis Rx
•18% had D levels <20
•Inverse association between D
and PTH
RISK FACTORS for D deficiency: older age, non-white race, obesity, low exercise,
low education, insufficient supplementation, certain medications, lack of
discussion with MD about vit DHolick et al, J Clin Endocrinol Metab. 2005; 90: 3215-24. 16

7/20/2015
5
Prevalence of Secondary Hyperparathyroidism by Vitamin D Stores
% w
ith
PT
H >
40
pg
/ml
25 (OH) D (ng/ml)
Holick et al, J Clin Endocrinol Metab. 2005; 90: 3215-24. 17
FGF23
• Primarily regulates: ???
• Main stimulus: 1,25D and high dietary phosphate
• Main effects: lower serum phosphate
− Stimulates phosphaturia
− Inhibits 1,25D production (CYP27B1)
− Stimulates CYP24
− Inhibits PTH
• Direct effects on bone: ???
18
Classic Physiological Actions of FGF23
Wolf M, J Am Soc Nephrol 2010; Wolf M, Kidney Int 2012; Rodriguez-Ortiz ME, JASN 2012
+_
_+
Phosphaturia
+
+
Dietary phosphate
intake+
–?
CaP+?
+?
_+
1,25D
FGF23
PTH
19
FGF23 in normal physiology
• 29 healthy males subjected to
low phosphate diet with
phosphate binder, followed by
phosphate loading
• FGF-23 decreased with low
phosphate and increased with
phosphate load
20Ferrari, J Clin Endocrinol Metab, 2004
Pi
inta
ke
FG
F2
3Tm
Pi/
GF
R

7/20/2015
6
Wolf, J Am Soc Nephrol 2010 21
Illustrative Case Studies: CKD
• Features:
− Low 1,25D
− Variable 25D
− High PTH
− High FGF23
− Low klotho expression
− Low normal calcium
− High normal phosphate
22
23
Calcitriol Deficiency and SHPT in CKD
*Abnormal PTH based on Kidney Disease Outcomes Quality Initiative (K/DOQI) Clinical Practice
Guidelines for Bone Metabolism and Disease in CKD. 2003.Kates et al. Am J Kidney Dis. 1997;30:809-813; Martinez et al. Am J Kidney Dis. 1997;29:496-502; Martinez et al. Nephrol Dial
Transplant. 1996;11(suppl 3):22-28; St. John et al. Nephron. 1992;61:422-427.
GFR (mL/min/1.73 m2)
50
40
30
20
10
0105 95 7585 65 45 35 1555 25
1,25D
Lower range
of 1,25D
10
20
30
40
50
60
70
80
90
100
Pa
tie
nts
Wit
h E
lev
ate
d P
TH
(%
)*
CKD Stage 2 Stage 3
Ca
lcit
rio
l
1,2
5(O
H) 2
D3
(pg
/mL)
Stage 4●●●●
●●●●
●●●●
●●●●
●●●●
●●●●●●●●
●●●●●●●●
●●●●
●●●●
23
FGF23 by CKD stage in CRIC
350
400
300
200
150
50
0
FG
F23,
RU
/ml
105
161
256
145
76
154
96
239
174
388
110
249
All < 30 30 – 44 ≥ 45
100
250
Estimated glomerular filtration rate, ml/min/1.73m2
Isakova et al. Kidney Int 2011
N = 1649
P = 3.5
N = 1472
P = 3.7
N = 752
P = 4.1
N = 3879
P = 3.7
24

7/20/2015
7
FGF23 and PTH in CRIC
25
0
10
20
30
40
50
60
70
80
90
100
<20 20-29 30-39 40-49 50-59 60-69 ≥70
% o
fP
op
ula
tio
n
Estimated glomerular filtration rate, ml/min/1.73 m2
Hyperphosphatemia, serum phosphate ≥ 4.6 mg/dl
Secondary hyperparathyroidism, PTH ≥ 65 pg/ml
FGF23 excess, FGF23 ≥ 100 RU/ml
Isakova et al. Kidney Int 2011
Disordered Mineral Metabolism in Rat CKD
Hasegawa et al. Kidney Int 2010 26
Effects of Anti-FGF23 Antibodies
Normalize 1,25DIncreased serum P
Hasegawa et al. Kidney Int 2010 27
Normal PTH range
1. Increased FGF23 is the earliest alteration in mineral
metabolism in CKD
Cascade of disordered mineral metabolism in CKD
An
aly
te c
on
cen
tra
tio
n
>10,000
1000
90
60
30
40
>90 75 60 45 30 15 0 3 6 >12
GFR (mL/min/1.73 m2)
Time post-transplant (months)
1,25D
(pg/mL)
cFGF23
(RU/mL)
12 3
4
Dialysis
Wolf M. J Am Soc Nephrol 2010
PTH
(pg/mL)
P
(mg/dL)
Normal P range
2. Gradually increasing FGF23 levels cause early decline in 1,25D levels
3. This frees PTH from feedback inhibition, leading to secondary
hyperparathyroidism
4. All these changes occur long before increases in serum P
levels are evident
28

7/20/2015
8
FGF23 and mortality in incident ESRD
Gutierrez et al N Engl J Med 2008 29
FGF23 and mortality in CKD 2-4:266 events, 20.3/1000 person-years
30
Cu
mu
lati
ve
in
cid
en
ce
of
de
ath
, %
Years of follow up
0 1 2 3 4 5
0
10
20
FGF23 Quartile 1: 1.0; Referent
FGF23 Quartile 2: 1.3; 0.8–2.2
FGF23 Quartile 3: 2.0; 1.2–3.3
FGF23 Quartile 4: 3.0; 1.8–5.1
Isakova et al. JAMA 2011.
FGF23-Induced Hypertrophy of NRVM:FGFR-dependent but klotho independent
31
klotho
GAPDH
GAPDH
FGFR1
FGFR4
FGFR2
FGFR3
L CM BlH
Br K CM BlH
10010 25
FGF2
FGF23
Controlng/mL
Faul, Amaral, Oskuei et al. J Clin Invest. 2011.
Blocking FGFRs prevents LVH in uremic rats
32Faul, Amaral, Oskuei et al. J Clin Invest. 2011.
Sham 5/6 nephrectomy5/6 nephrectomy+
PD173074
0
50
100
150
200
250
Sh
am
5/6
5/6
+ P
D
SBP
0
200
400
600
800
1000
1200
1400
1600
Sh
am
5/6
5/6
+ P
D
FGF23

7/20/2015
9
Anti-FGF23 Ab: Increased calcification & mortality
33Shalhoub V, J Clin Invest 2012
Disordered phosphate homeostasis and cardiovascular disease in CKD
34Scialla J, Wolf M. Nat Rev Nephrol 2014
Illustrative monogenic case studies 1
• Biochemical phenotype:
− Rickets
− Hypophosphatemia
− Normal serum calcium
− Low FGF23
− Normal PTH
− Hypercalciuria
− High 1,25D
• Where is the primary lesion?
35
Hereditary hypophosphatemic rickets with hypercalciuria (HHRH)
• Key finding: Hypophosphatemia that is not FGF23 or PTH
mediated
• Primary defect: NaPi2c deficiency
• Phosphate wasting � rickets
• FGF23 suppression � 1,25D activation
• Hypercalciuria
• NaPi2a deficiency was recently described in humans for
the first time (Magen D, N Engl J Med 2010)
36

7/20/2015
10
Illustrative monogenic case studies 2
• Biochemical phenotype:
− Ectopic calcification
− Hyperphosphatemia
− Normal serum calcium
− Low intact FGF23
− Low PTH
− Hypercalciuria
− High 1,25D
• Where is the primary lesion?
37
Tumoral calcinosis: FGF23 deficiency
• Key finding: hyperphosphatemia with low FGF23 and low
PTH
• Absence of biologically active FGF23 or FGF23 action due
to klotho deficiency � elevated 1,25D
• Positive calcium balance + defective phosphate excretion
= calcifications
• Elevated 1,25D and calcium absorption suppress PTH and
permit hyperphosphatemia
38
Illustrative monogenic case studies 3
• Biochemical phenotype:
− Hypercalcemia
− Normal serum phosphate
− High-normal PTH
− Hypocalciuria
− High 1,25D
• Where is the primary lesion?
39
Familial hypocalciuric hypercalcemia (FHH)
• Key finding: hypercalcemia with non-suppressed PTH = primary
hyperparathyroidism
• Inactivating mutation of calcium sensing receptor
− Persistent PTH production despite hypercalcemia
− Upward reset of calcium set point
− PTH induces hypercalcemia
− Activation of TAL and DCT calcium transport by partially
inactive calcium sensing receptor
• Boards claim to fame:
− Looks like primary hyperparathyroidism on serum
− Don’t resect FHH
− Urine calcium differentiates
40

7/20/2015
11
Illustrative monogenic case studies 4
• Biochemical phenotype:
− Hypocalcemia
− Hyperphosphatemia
− Low PTH
− Hypercalciuria
− Low 1,25D
• Where is the primary lesion?
41
Autosomal dominant hypoparathyroidism
• Key finding: Hypocalcemia + low PTH = hypoparathyroidism
• Activating mutation of calcium sensing receptor
• Mirror image disease of FHH
− Absent PTH production despite hypocalcemia
− Downward reset of calcium set point
− Lack of PTH induces hypocalcemia
− Lack of PTH (and likely inappropriately low FGF23)
contribute to hyperphosphatemia
− Reduced TAL and DCT calcium transport by activated
calcium sensing receptor leads to calcium dumping,
hypercalciuria
42
Illustrative monogenic case studies: 5
• Biochemical phenotype:
− Hypocalcemia
− Hypophosphatemia
− High PTH
− Normal 25D
− Undetectable 1,25D
• Where is the primary lesion?
43
Vitamin D-dependent rickets type 1
• Key finding: hypocalcemia + hypophosphatemia with
secondary hyperparathyoridsm = defective vitamin D signaling
• 1-alpha hydroxylase deficiency (autosomal rec)
• Lack of 1,25D � hypocalcemia� secondary hyperpara and
hypophosphatemia
• Vitamin D-dependent rickets type 2 = VDR deficiency
− Difference is 1,25D level and response to 1,25D therapy
• FGF23 should be very low in type 1 and 2
• Vitamin D resistant rickets = primary FGF23 excess (XLH, ADHR,
TIO)
44

7/20/2015
12
Questions
45