Embed Size (px)
Citation preview
CAMEROON ACADEMY OF SCIENCES
ACADEMIE DES SCIENCES DU CAMEROUN

CAMEROON ACADEMY OF SCIENCES
RECENT ADVANCES IN ONCHOCERCIASIS RESEARCH AND IMPLICATIONS FOR CONTROL
PRODUCED BY AN EXPERT COMMITTEE OF THE CAMEROON ACADEMY OF SCIENCES
Committee Members (Authors) Vincent N. TANYA, DVM, M.Sc., PhD, FCAS, FTWAS (Chair); Chief Research Officer, Institute of Agricultural Research for Development; Technical Adviser No1, Ministry of Scientific Research and Innovation, Yaoundé, Cameroon Samuel WANJI, Dr Habl; Associate Professor of Molecular Parasitology and Entomology, Department of Microbiology and Parasitology, Faculty of Science, University of Buea, Cameroon Joseph KAMGNO, MD, MPH, PhD, Senior Lecturer, Department of Public Health, Faculty of Medicine and Biomedical Sciences, University of Yaoundé I, Cameroon and Director of the Centre for Research on Filariasis and other Tropical Diseases, Yaoundé, Cameroon Daniel M. ACHUKWI, DVM, PhD, Chief Research Officer, Director of Scientific Research, Institute of Agricultural Research for Development, Yaoundé, Cameroon Peter Ayuk Ivo ENYONG, DEA, Doct. es Sc, Senior Research Fellow, Research Foundation in Tropical Diseases and Environment, Buea, Cameroon Study Staff of the CameroonAcademy of Sciences David Akuro Mbah, PhD, Executive Secretary
Vincent N. Tanya, PhD, Programme Officer
Thaddeus A. Ego, Administrative Assistant
December 2012
ii
Recent advances in onchocerciasis research and implications for control
Published by The Cameroon Academy of Sciences P.O. Box 1457 Yaoundé, Cameroon
Tel: (237)2223 9741; Fax: (237) 2222 9741 E-mail: [email protected]
Website: www.casciences.com
NOTICE
The project that is the subject of this study was supported by grant agreement n°IOM-5855-05-002 between the United States National Academy of Sciences and the Cameroon Academy of Sciences. International Standard Book Number 9956-26-38-x
Additional copies of this publication are available from the Cameroon Academy of Sciences, P.O. Box 1457 Yaoundé, Cameroon or http:www.casciences.com Cover pictures provided by Drs Achukwi and Kamgno Citation: CAS (2012). Recent Advances in Onchocerciasis Research and Implications for Control. Cameroon Academy of Sciences, Yaoundé, Cameroon.
All rights reserved © The Cameroon Academy of Sciences
iii
Recent advances in onchocerciasis research and implications for control
Table of Contents
Table of Contents ......................................................................................................................................................... iii
List of Figures ................................................................................................................................................................ v
Acronyms...................................................................................................................................................................... vi
Cameroon Academy of Sciences ................................................................................................................................ viii
Acknowledgements ..................................................................................................................................................... ix
Preface ........................................................................................................................................................................... x
Executive Summary ...................................................................................................................................................... xi
Resumé ....................................................................................................................................................................... xiv
Background information on onchocerciasis ................................................................................................................. 1
Introduction .............................................................................................................................................................. 1
Global magnitude...................................................................................................................................................... 1
Onchocerciasis in Cameroon ..................................................................................................................................... 2
Bio‐ecology of S. damnosum .................................................................................................................................... 3
Life cycle of Onchocerca volvulus ............................................................................................................................. 4
Pathology of onchocerciasis ..................................................................................................................................... 6
Socio‐economic implications of onchocerciasis ........................................................................................................ 8
Treatment and control of onchocerciasis................................................................................................................... 11
Introduction ................................................................................................................................................................ 11
Surgical treatment .................................................................................................................................................. 11
Vector control ......................................................................................................................................................... 11
Historical Background ........................................................................................................................................ 11
The phases of vector control in Africa ................................................................................................................ 12
Problems of vector control ................................................................................................................................. 15
Drug treatment ....................................................................................................................................................... 16
Ivermectin in the control of onchocerciasis ............................................................................................................ 16
Ivermectin family and chemical structure .............................................................................................................. 16
Effect of ivermectin on O. volvulus ......................................................................................................................... 17
Clinical trials with Ivermectin .................................................................................................................................. 17
African Programme for Onchocerciasis Control ..................................................................................................... 18
Effect of the drug on the transmission of onchocerciasis ....................................................................................... 19
Problems associated with the use of ivermectin for onchocerciasis control ......................................................... 20
APOC achievements ................................................................................................................................................ 24
APOC challenges ..................................................................................................................................................... 24
Onchocerciasis control strategies in Cameroon ......................................................................................................... 25
Introduction ............................................................................................................................................................ 25
Identification of priority populations to be treated in Cameroon .......................................................................... 25
Evolution of onchocerciasis control strategies in Cameroon .................................................................................. 26

iv
Recent advances in onchocerciasis research and implications for control
Early large scale distributions ............................................................................................................................ 26
Community‐based strategies ............................................................................................................................. 26
The advent of the African Programme for Onchocerciasis Control in Cameroon .................................................. 26
Difficulties related to onchocerciasis control in Cameroon .................................................................................... 27
Chemotherapy and immunology of onchocerciasis: insights from the bovine model ............................................. 29
Introduction ............................................................................................................................................................ 29
O. ochengi/cattle model for onchocerciasis research ............................................................................................ 29
O. ochengi and chemotherapeutic studies ............................................................................................................. 29
Chemotherapeutic studies with anthelmintics .................................................................................................. 29
Antibiotic therapy for onchocerciasis ................................................................................................................ 30
O. ochengi and immunological studies ................................................................................................................... 32
Putative immunity .............................................................................................................................................. 32
Zooprophylaxis ................................................................................................................................................... 33
Vaccination trials ................................................................................................................................................ 33
Antibiotic therapy for the control of onchocerciasis: current status and perspectives ........................................... 35
Introduction ............................................................................................................................................................ 35
A new opportunity for the treatment of onchocerciasis: the endosymbiont Wolbachia ....................................... 35
Anti‐Wolbachia treatment: current status ............................................................................................................. 36
Lessons from animal models .............................................................................................................................. 36
Anti‐Wolbachia therapy: from animal models to humans ................................................................................. 26
Anti‐Wolbachia as alternative treatment for onchocerciasis in areas of co‐endemicity with loiasis ................ 37
Scaling up the anti‐Wolbachia treatment: the community‐directed delivery approach ................................... 37
The way forward for the elimination of onchocerciasis ............................................................................................ 41
Vector Control ......................................................................................................................................................... 41
The improvement of Community Directed Treatment with Ivermectin ................................................................. 42
Anti‐Wolbachia treatment ...................................................................................................................................... 44
Vaccination ............................................................................................................................................................. 46
Sustainability and ownership of control programmes ............................................................................................ 46
References ................................................................................................................................................................... 49
Appendices.................................................................................................................................................................69
Statement of task .................................................................................................................................................... 70
Biographical sketch of committee members .......................................................................................................... 72

v
Recent advances in onchocerciasis research and implications for control
List of Figures
Figure 1. Distribution of onchocerciasis showing current status of global onchocerciasis control............................... 2
Figure 2. Rapid epidemiological mapping of onchocerciasis in Cameroon .................................................................. 3
Figure 3. Transmission cycle of Onchocerca volvulus, O.ochengi and O. ramachandrini .............................................. 5
Figure 4. Life cycle of O.volvulus ................................................................................................................................... 5
Figure 5. Chemical structure of ivermectin ................................................................................................................. 17
Figure 6. Sub‐conjunctival haemorrhage in a post ivermectin SAE case ..................................................................... 23
vi
Recent advances in onchocerciasis research and implications for control
Acronyms
ABRs Annual biting rates
APOC African Programme for Onchocerciais Control
ATPs Annual transmission potentials
CAS Cameroon Academy of Sciences
CDDs Community‐directed distributors
CDTI Community‐Directed Treatment with Ivermectin
CHC Chlorinated hydrocarbon
CRFilMT
DALYs
Centre for Research on Filariasis and other Tropical Diseases
Disability‐Adjusted Life‐Years
DDT Dichlorodiphenyltrichloroethane
DEC Diethylcarbamazine
EAC Expert Advisory Committee
FAO Food and Agriculture Organisation of the United Nations
GABA ϒ‐aminobutyric acid
GTZ Gesellshaft fur Technische Zusammenarbeit (German Technical Cooperation)
HKI Helen Keller International
IAMP Inter Academy Medical Panel
IAP Inter Academy Panel on International Issues
IEF International Eye Foundation
IMPM Institut de Recherches Médicales et d’Etudes de Plantes Médicinales
IRAD Institute de Recherche Agricole pour le Développement
IRD Institut de Recherche pour le Développement
IVM Ivermectin
JPC Joint Programme Committee
LCIF Lions Club International Foundation
MDD Mass Drug Distribution
MDP Mectizan Donation Programme
MEC Mectizan®Expert Committee
vii
Recent advances in onchocerciasis research and implications for control
NASAC Network of African Science Academies
NGDOs Non Governmental Development Organizations
NGOs Non Governmental Organizations
NOCP National Onchocerciasis Control Programme
NOTF National Onchocerciasis Task Force
OCCGE
OCP
Organisation de Coordination et de Coopération pour la Lutte contre les Grandes Endémies
Onchocerciasis Control Programme
ORSTOM Office de la Recherche Scientifique et Technique Outre‐Mer
PLERI Probable L. loa encephalopathies related to the treatment with Ivermectin
RAPLOA Rapid Epidemiological Assessment of Loiasis
RBF River Blindness Foundation
REA Rapid Epidemiological Assessment of Onchocerciasis
REMO Rapid Epidemiological Mapping of Onchocerciasis
ROD Reactive onchodermatitis
SAEs Severe Adverse Events
SSI Sight Savers International
TCC Technical Consultative Committee
TDR Special Programme for Research and Training in Tropical Diseases (TDR) of the WHO
TWAS Third World Academy of Sciences (the Academy of Sciences for the Developing World)
UNDP United Nations Development Programme
USAID United States Agency for International Development
USNAS United States National Academy of Sciences
WHO World Health Organisation

viii
Recent advances in onchocerciasis research and implications for control
Cameroon Academy of Sciences
The Cameroon Academy of Sciences (CAS) was formally recognized by declaration N° Reg. 00701/RDA/J06/BAPP of 29 May 1991 by the Cameroon Government in accordance with law N° 90/053 of 19 December 1990, regulating freedom of association. It is a non‐profit society of distinguished scholars engaged in promoting excellence and relevance in science and technology and providing advice to the government of Cameroon and other partners.
The vision of the Cameroon Academy of Sciences is to be the prime mover of science and technology, making scientific knowledge available to decision and policy makers with a view to influence investment priorities in science and technology, and promoting the use of science and innovation in the economic, social and cultural development of Cameroon. Consequently, the Academy produces robust forum and committee advisory documents as well as reports on priority problems that are delivered to policy and decision makers and the public. The independence, highly qualified membership, multidisciplinary composition and rigorous procedures for objective and unbiased analysis enable the Academy to effectively deliver credible advice.
In carrying out its work, the Academy collaborates with the various ministries of the Government of Cameroon, the United States National Academy of Sciences (USNAS), the Academy of Sciences for the Developing World (TWAS), Royal Society (UK), the Network of African Science Academies (NASAC), Inter Academy Panel on International Issues (IAP), Inter Academy Medical Panel (IAMP) and other international and national organizations. EXECUTIVE COMMITTEE OF CAS
President Prof. Samuel Domngang 1st Vice President Prof. Sammy Beban Chumbow 2nd Vice President Prof. Peter M. Ndumbe Executive Secretary Dr. David Akuro Mbah Assistant Executive Secretary Prof. Manguelle‐Dicom E. Treasurer/Programme Officer Dr. Vincent N. Tanya
DEANS OF CAS COLLEGES
College of Biological Sciences Prof. Daniel N. Lantum College of Mathematics and Physical Sciences Prof. Samuel Domngang College of Social Sciences Prof. Sammy Beban Chumbow
JOURNAL OF THE CAMEROON ACADEMY OF SCIENCES (JCAS)
Editor‐in‐Chief Prof. Vincent P. K. Titanji KEY ADMINISTRATIVE STAFF OF CAS
David Akuro Mbah, PhD, Executive Secretary E. Manguelle‐Dicom, PhD, Assistant Executive Secretary Vincent N. Tanya, PhD, Treasurer/Programme Officer Thaddeus A. Ego, Administrative Assistant
CONTACT INFORMATION
Cameroon Academy of Sciences P.O. BOX 1457 Yaoundé, Cameroon Telephone: +237 2223 9741 Fax: +237 2223 9741 Email: [email protected] Website: www.casciences.com
ix
Recent advances in onchocerciasis research and implications for control
Acknowledgements
The Cameroon Academy of Sciences (CAS) Expert Committee is appreciative of the contributions and efforts of all
those who helped in the realisation of this project. The Committee thanks the Members of the CAS Forum on
Public Health for choosing this subject and for their guidance and support through out the period of the study.
The Committee gratefully acknowledges the United States National Academy of Sciences (USNAS) for facilitating
financial support from Bill and Melinda Gates Foundation and for providing technical support for this work within
the framework of its African Science Academy Development Initiative (ASADI). Gratitude is conveyed to Dr. Patrick
Kelley, Ms Patricia Cuff, Mr. Jim Banihashemi and Ms Angela Mensah for making possible the collaboration
between the Cameroon Academy of Sciences and the USNAS. Dr. Kelly and Ms Cuff also provided guidance on
carrying out consensus studies.
We would like to thank Drs Marcelline Ntep and Benjamin Biholong of the National Onchocerciasis Control
Programme, Yaounde, Cameroon for providing information, input and assistance that facilitated the writing of this
report.
The review process for the study was overseen by Dr. David A. Mbah, Executive Secretary of the Cameroon
Academy of Sciences.
This report was reviewed independently by experts who were selected for their technical competence. They
provided candid and critical comments that greatly improved the quality of this report. The Committee would like
to thank the following for the review :
Bridget B. Kelly, MD, PhD, Senior Programme Officer, Board on Global Health, Institute of Medicine of the
National Academies, Washington, DC, USA;
Ben L. Makepeace, PhD, Senior Research Fellow, Department of Infection Biology, Institute of Infection
and Global health, University of Liverpool, Liverpool, England, UK;
Vincent P.K. Titanji, PhD, Professor of Biochemistry, Former Vice‐Chancellor of the University of Buea,
Cameroon;
Roger Moyo‐Somo, MD, PhD, Professor of Parasitology, Faculty of Medicine and Biomedical Sciences,
University of Yaoundé I, Cameroon.
Responsibility for the final content and quality of this report is totally that of the Expert Committee and CAS.

x
Recent advances in onchocerciasis research and implications for control
Preface
As part of its present strategic plan, the Cameroon Academy of Sciences (CAS) organises workshops and seminars
and carries out research and consensus studies in order to provide information for evidence‐based actions by
various stakeholders. It has so far organised several seminars and workshops either alone or in collaboration with
other partners.
In its meeting of 21 April 2011, the Academy’s Forum on Public Health decided to carry out its first consensus
study. From among several themes that were short‐listed during the meeting, it was decided that a consensus
study should be carried out on recent advances in onchocerciasis research and implications for control. The
members of the Forum felt that Cameroonian scientists, their partners (British, German, Ghanaian and French)
and others had done significant scientific research in recent years on onchocerciasis which could even be
described as ground breaking. They also believed that the studies had important implications for the control of the
disease in Cameroon. Unfortunately, this crucial scientific information is buried in different scientific journals and
is not readily available to stakeholders involved in treatment and control efforts in developing countries in general
and Cameroon in particular. Consequently, the Forum members asked the Academy to carry out a consensus
study. Accordingly, CAS in recognition of its advocacy role in giving visibility to Cameroonian research efforts and
that of its partners and other scientists, convened an expert panel to bring together the data on recent research
on onchocerciasis, analyse it and present sound advice and reasoning for reorientation of the current
onchocerciasis control strategies in Africa in general and in Cameroon in particular.
In view of all of the above, it is hoped that the report herein presented will provoke dialogue among stakeholders
and draw public attention.

xi
Recent advances in onchocerciasis research and implications for control
Executive Summary
The Cameroon Academy of Sciences convened an expert panel to bring together the data on recent research on
onchocerciasis, analyse it and present sound advice and reasoning for reorientation of the current onchocerciasis
control and research strategies in Cameroon in particular and the world in general.
Onchocerciasis is a parasitic disease caused by Onchocerca volvulus and transmitted via the bites of a black fly of
the genus Simulium. It is a debilitating dermal filariasis which is endemic mainly in tropical Africa and to a lesser
extent in Central and South America and the Arabian Peninsula particularly in Yemen. The clinical and socio‐
economic effects are most severe in sub‐Saharan Africa where it causes blindness and severe skin diseases.
Presently, onchocerciasis is recognised as the world’s second leading infectious cause of blindness. Figures on its
global magnitude cited in the literature are quite varied. The World Health Organization estimates that about 37
million people are currently infected with the parasite with about 99% of them living in sub‐Saharan Africa. Almost
1.5 million are visually impaired and about 500,000 are blind. A total of 90 million people are at risk of becoming
infected with the parasite.
Over the years, attempts to control the disease have been based on vector control and drugs. Despite more than
forty years of control in Africa, the disease is still a public health concern in many African countries, where the
prevalence in some foci is still very high. It is therefore important to seek for complementary strategies so that the
current control strategies can be improved.
Vector control
Early efforts to control onchocerciasis were based on treatment of water courses with insecticides to kill the larvae
of the Simulium vectors. This approach, used by the Onchocerciasis Control Programme (OCP) in West Africa
successfully reduced the burden of disease in the areas covered by the programme. This strategy can still be used
in combination with other approaches today. The two recent cases of vector elimination in Itwara (Uganda) and
Bioko Island (Equatorial Guinea) applied the OCP methodology with the help of the African Programme for
Onchocerciasis Control (APOC).
In view of the on‐going construction of new hydroelectric dams in Cameroon, the authorities of the projects should
already build into their operational activities, some black fly vector control components so as to be prepared to
handle any unforeseen S. damnosum population explosion after the construction. The main rivers of Cameroon
should also be the target of focal black fly control activities as they all contribute to the breeding of S. damnosum.
Furthermore, operational research is needed to improve monitoring and establish thresholds that determine when
and where vector control is needed. It is also necessary to evaluate the adverse environmental effects of the
insecticides used in any control operations.
Community‐Directed Treatment with Ivermectin
Ivermectin (Mectizan) donated by Merck & Co was introduced in 1987 for mass treatment of onchocerciasis.
APOC launched in 1996 the Community‐Directed Treatment with Ivermectin (CDTI) strategy. Ivermectin is

xii
Recent advances in onchocerciasis research and implications for control
microfilaricidal and its use successfully reduced the morbidity of onchocerciasis in various communities. It had
been hoped that CDTI would eliminate the disease by breaking transmission but this has not happened, probably
as a result of specific epidemiological, sociological and logistical factors that make elimination using ivermectin
alone unlikely in some areas.
The main limitation of ivermectin is that it has little effect on the adult worms that continue to produce
microfilariae and hence re‐treatment is required at intervals that experts in many on‐going programmes have not
definitely determined or agreed upon. A major obstacle for onchocerciasis control using ivermectin has been the
occurrence of post ivermectin severe adverse events in areas co‐endemic with loiasis.
In view of the above, we suggest that CDTI should be improved by the following:
• There is need for the research organisations in charge of medical research in Cameroon to investigate the
epidemiological, sociological and logistical factors that contribute to the maintenance of high levels of the
prevalence of onchocerciasis after more than 17 years of treatment with ivermectin using the CDTI
approach in areas where loaisis is absent.
• The National Onchocerciasis Control Programme should intensify communication to inform the population
on the benefits of treatment with ivermectin. Efforts should also be made to seek for permanent non
compliers in order to inform, educate and properly treat them.
• The strategy of the control programme in the Americas which is based on at least twice yearly treatment
and which has resulted in the near elimination of onchocerciasis in that area should be adopted in all
endemic foci in general and Cameroon in particular where the results of the epidemiological evaluation
are not as good as was expected. This should be accompanied by epidemiological surveillance to detect
and control disease resurgence. Therapeutic approaches to reduce the load of L. loa infections are also
necessary to increase ivermectin coverage. Hypoendemic areas should also be covered under the new
strategy of “Test and Treat” that is being developed.
To date, there is a lot of controversy regarding the emergence of resistance of O. volvulus to ivermectin. In
addition to the phenotypic suspicions of resistance, many studies have revealed that selection occurs in some
genes of the parasite. Despite these phenotypic and genotypic studies, the unequivocal proof of resistance is yet
to be established. Further studies are therefore needed to clarify this situation in order to preserve the benefits of
past and current onchocerciasis control programmes.
Antibiotic therapy of human onchocerciasis
The symbiosis of filarial nematodes and intracellular Wolbachia bacteria has been studied as a target for antibiotic
therapy of filariasis in cattle using O. ochengi. The results showed that doxycycline is macrofilaricidal. As a result of
the close phylogenetic relationship between O. volvulus and O. ochengi, antibiotic treatment may also be
macrofilaricidal in humans. Trials in humans have demonstrated that:
• antibiotic treatment of O. volvulus results in sterility and inhibits larval development and adult worm
viability;
• depletion of bacteria following treatment with doxycycline resulted in a complete and long‐term blockage
of embryogenesis;

xiii
Recent advances in onchocerciasis research and implications for control
• doxycycline also had macrofilaricidal effect on O. volvulus;
• the endosymbiont Wolbachia is absent from L. loa and this fact can be exploited for the administration of
antibiotherapy for the treatment of onchocerciasis in areas where L. loa is co‐endemic;
• the large scale administration of doxycycline for six weeks is feasible in co‐endemic villages of loiasis and
onchocerciasis using community directed approach with high therapeutic coverage and very high
compliance rates.
In view of the above results, we recommend as follows:
• The recently completed community‐directed intervention (CDI) trials using a 6‐week course of doxycycline
at 100 mg/day demonstrated that prolonged courses of treatment can be effectively delivered either
through individual or mass treatment using doxycycline. Consequently, doxycycline at this regimen could
be used for individual treatment and should be a reserve in cases of ivermectin resistance.
• Given that the cost of purchase and delivery of doxycycline for the six week treatment per patient is
relatively high for most onchocerciasis patients living in endemic communities, research efforts should be
maintained to develop shorter regimens of this drug. Lobbying should be made by governments and Non
Governmental Development Organisations for the reduction of the prices of this drug.
Vaccination
Vaccination can be a complementary tool for the present onchocerciasis control efforts as it can protect
vulnerable groups particularly children living in endemic areas against infection and reduce adult worm burden
and fecundity, thus reducing the pathological effects caused by the microfilariae. Many research groups have
identified a number of O. volvulus larval vaccine candidates. Trials with some of them have obtained proof‐of‐
principle of vaccination against L3 infection as it was shown that microfilarial loads reduced significantly in animal
models. Consequently, we recommend that donors should provide funding for research groups which have
identified promising vaccine candidates for the purpose of vaccine design, formulation and delivery.
Sustainability and ownership of control programmes
APOC’s mandate is expected to end in 2015. At that time, it will transfer full responsibility for onchocerciasis
control to national control programmes. Governments would be expected to provide adequate technological and
financial support for national control programmes to enable them take on the responsibilities that would be
transferred from APOC. The inability of national control programmes to sustain disease control efforts can have
important ramifications as disease resurgence can reverse the gains in public health produced by both OCP and
APOC over the years.
To create sustainable disease control efforts beyond APOC’s mandate, we urge National Programmes to develop
technical and technological competence that would enable them to function properly after the withdrawal of
APOC. We appeal to National Governments and donors not to abdicate their financial responsibility which is
needed to ensure that the substantial investments and progress made towards eliminating onchocerciasis in Africa
are sustained for the future.
xiv
Recent advances in onchocerciasis research and implications for control
Resumé
L’Académie des Sciences du Cameroun a réuni un panel d’experts afin de rassembler les données relatives aux
recherches récentes sur l'onchocercose, les analyser et prodiguer des conseils pratiques et judicieux aux fins de
donner une nouvelle orientation aux stratégies de lutte contre l’onchocercose au Cameroun en particulier et dans
le monde en général.
L’onchocercose est une maladie parasitaire causée par Onchocerca volvulus. Elle est transmise par les piqures
d’une mouche du genre Simulium. Il s’agit d’une filariose dermique débilitante, endémique surtout en Afrique
tropicale et dans une moindre mesure en Amérique Centrale et du Sud, ainsi que dans la Péninsule arabique et au
Yémen en particulier. Les effets cliniques et socio‐économiques sont plus néfastes en Afrique subsaharienne car
elle y entraîne la cécité et des dermatoses sévères. De nos jours, l’onchocercose est connue comme la deuxième
cause de cécité d’origine infectieuse dans le monde. Les statistiques relatives à son impact sont très variées. Les
estimations de l’Organisation Mondiale de la Santé font état de près de 37 millions de personnes infectées par le
parasite avec approximativement 99% vivant en Afrique subsaharienne. Près de 1,5 millions de personnes
souffrent de déficience visuelle et près de 500 000 sont aveugles. Un total de 90 millions de personnes est à risque
d’infection par le parasite.
Au cours des années écoulées, les tentatives relatives à la lutte contre la maladie ont été basées sur la lutte
antivectorielle et la chimiothérapie. Malgré plus de quarante années de lutte en Afrique, la maladie représente
toujours un problème de santé publique dans plusieurs pays, et la prévalence dans certains foyers reste très
élevée. Il est donc très important de rechercher des stratégies complémentaires afin d’améliorer la lutte contre
l’onchocercose.
Lutte antivectorielle
Les efforts de lutte contre l'onchocercose portaient plus sur le traitement des cours d’eaux à l’aide d’insecticides
afin d’éliminer la lave de la simulie. Cette approche utilisée par le Programme de Lutte contre l'Onchocercose en
Afrique de l’Ouest ou encore Onchocerciasis Control Program in West Africa (OCP) a considérablement réduit
l’endémicité de la maladie dans les zones couvertes par ce Programme. Cette lutte antivectorielle peut encore être
utilisée de nos jours en association avec d’autres approches. Les deux derniers cas d'éradication de l’agent vecteur
à Itwara (Ouganda) et sur l’Ile de Bioko (Guinée Equatoriale) ont appliqué la méthode du programme OCP avec
l’aide du Programme Africain de Lutte contre l'Onchocercose (APOC).
Compte tenu de la construction en cours de nouveaux barrages hydroélectriques au Cameroun, les responsables
des projets devraient déjà concevoir dans leurs activités opérationnelles, des plans de lutte contre les mouches
noires, vecteurs de la maladie, afin d’être prêts à gérer tout imprévu relatif à une croissance exponentielle de la
population de S. damnosum après la construction des barrages. Les principaux fleuves du Cameroun devraient
également être la cible des activités de lutte contre la mouche noire puisqu'ils contribuent tous à la reproduction du
vecteur. Aussi, une recherche opérationnelle s’avère nécessaire en vue de déterminer les seuils à partir desquelles
la lutte contre le vecteur s’impose. Par ailleurs, il est important d’inclure dans les projets de lutte antivectorielle,
une composante environnementale sur l’effet des larvicides sur la flore et la faune aquatique.
xv
Recent advances in onchocerciasis research and implications for control
Traitement par ivermectine sous directives communautaires
L’ivermectine (Mectizan) offert par Merck & Co, a été introduit en 1987 pour le traitement en masse de
l’onchocercose. L’APOC a mis sur pied en 1996, la stratégie de Traitement à l’Ivermectine sous Directives
Communautaires (TIDC). L’ivermectine est un microfilaricide puissant et son utilisation a réduit de façon
significative la morbidité de l’onchocercose dans différentes communautés. On espérait que l’ivermectine pouvait
éliminer la maladie en interrompant la transmission, mais tel n’est pas le cas. Ceci pourrait être dû aux facteurs
épidémiologiques, sociologiques et logistiques qui rendent difficile l’élimination de l’onchocercose à l’aide de
l’ivermectine uniquement dans certain foyers.
La principale limite de l’ivermectine réside dans le fait que ce médicament a un effet limité sur les vers adultes qui
continuent de produire les microfilaires, soulignant ainsi la nécessité de traitements biannuels une ou deux fois
par an. Un autre obstacle à la lutte contre l’onchocercose à l’aide de l’ivermectine reste la survenue des effets
secondaires graves dans des zones co‐endémiques avec la loase.
A la lumière de ce qui précède, nous suggérons que le TIDC soit amélioré en tenant compte des propositions
suivantes :
• Il est nécessaire que les structures de recherche dans le domaine de la santé au Cameroun mènent des
études sur les facteurs épidémiologiques, sociologiques et logistiques qui contribuent à maintenir des
prévalences élevées de l'onchocercose, après plus de 15 années de traitement à l'ivermectine.
• Le Programme National de Lutte contre l’Onchocercose doit intensifier la communication afin d’informer
la population sur les avantages du traitement à l’ivermectine. Des efforts doivent également être déployés
pour identifier les sujets qui restent en marge du traitement de façon permanente afin de les informer, les
éduquer et les traiter convenablement.
• La stratégie du programme de lutte dans les Amériques basée sur l’administration d’au moins deux doses
par an et qui a abouti à une élimination presque totale de l’onchocercose dans cette zone devrait être
adoptée dans toutes les zones où le programme a des difficultés à éliminer la maladie (les zones où les
prévalences restent élevées malgré plusieurs années de traitements, avec des niveaux de transmission très
élevés). Les approches thérapeutiques de réduction de la charge des infections de la filariose à L. loa sont
également nécessaires pour réduire le risque d’effets secondaires graves et ainsi accroître la couverture à
l'ivermectine. Les zones hypo, endémiques doivent être incluses dans le programme de traitement si l’on
veut réellement éliminer la maladie.
Jusqu’à nos jours, il y a beaucoup de controverse autour de l’émergence de la résistance de l’O. volvulus à
l’ivermectine. En plus des suspicions phénotypiques sur la résistance, des recherches ont prouvé qu’une sélection
intervient dans certains gènes du parasite. En dépit de ces études phénotypiques et génotypiques, la preuve de la
résistance n’est pas encore établie. D’autres recherches doivent donc être effectuées afin de clarifier cette situation
et préserver les acquis programmes de lutte contre l’onchocercose.
xvi
Recent advances in onchocerciasis research and implications for control
Thérapie à base d’antibiotiques pour le traitement de l’onchocercose chez l’homme
La symbiose entre les nématodes et la bactérie intracellulaire Wolbachia a été bien étudiée chez le bétail avec le
modèle O. ochengi. La bactérie Wolbachia est une cible pour le traitement de l’onchocercose à base
d’antibiotique. Les résultats ont montré que la doxycycline est macrofilaricide. Du fait qu’O. ochengi est proche
phylogénétiquement d’O. volvulus, le traitement à base d’antibiotiques peut être également macrofilaricide chez
les êtres humains. Des essais sur l'homme ont démontré que:
• Le traitement d’O. volvulus à base d’antibiotiques abouti à la stérilisation des vers, l’inhibition du
développement larvaire et la mort du ver adulte.
• La bactérie Wolbachia n’est pas en symbiose avec L. loa, et ce fait peut être exploité pour l’administration
de l’antibiothérapie dans le traitement de l’onchocercose dans des zones où le L. loa est co‐endémique.
• L’administration à grande échelle de doxycycline pendant six semaines est réalisable dans des villages co‐
endémiques pour la loase et l’onchocercose en utilisant le schéma de traitement sous Directives
communautaires.
Vu les résultats ci‐dessus, nous recommandons que:
• Les travaux de recherche continuent, pour la détermination des schémas thérapeutiques plus court et
utilisable en traitement de masse avec moins de difficultés.
• La doxycycline soit une alternative au cas où la résistance à l’ivermectine se confirme. Un lobbying
devraient être fait par les gouvernements des pays endémiques afin d’obtenir la doxycycline à des prix
raisonnable.
Vaccination
La vaccination peut être un outil complémentaire pour les efforts actuels de lutte contre l’onchocercose dans la
mesure où elle peut permettre de protéger les groupes vulnérables, et surtout les enfants vivant dans les zones
endémiques. Elle peut aussi permettre de réduire le nombre de vers adultes et la fécondité, réduisant ainsi les
effets pathologiques causés par les microfilaires. Plusieurs groupes de recherche ont identifié un certain nombre
de vaccins contre les stades larvaires d’O. volvulus. Des essais de certains d’entre eux ont démontré l’efficacité de
la vaccination contre l’infection par les larves L3. Dans le modèle animal, il a été démontré que la vaccination
entraîne une réduction significative des charges microfilarienne. Nous recommandons par conséquent aux
bailleurs et aux gouvernements de soutenir les groupes de recherche qui ont identifié les vaccins candidats les plus
prometteurs en vue de leur développement, leur formulation et leur utilisation dans la lutte contre l’onchocercose.
Viabilité et responsabilité des programmes de lutte
Le mandat du Programme Africain de Lutte contre l’Onchocercose s’achève en principe en 2015. Il transfèrera
alors toute la responsabilité de la lutte contre l’onchocercose aux programmes nationaux de lutte. Les
gouvernements devront alors apporter une assistance technique et financière adéquate aux programmes
nationaux de lutte afin de leur permettre de prendre les responsabilités qui leurs seront confiées par l’APOC.
L’incapacité des programmes nationaux à maintenir les efforts de lutte contre la maladie pourrait avoir des

xvii
Recent advances in onchocerciasis research and implications for control
conséquences importantes puisque la résurgence de la maladie peut anéantir les acquis obtenus par les
programmes OCP et APOC pendant des années.
Afin de maintenir des efforts de lutte durable contre la maladie après le mandat d’APOC, nous recommandons aux
programme nationaux d’assurer une bonne préparation (formations des expertises nationales dans la perspective
du retrait du programme APOC), et aux différents gouvernements et autres bailleurs de ne pas renoncer à leurs
responsabilités financières qui est nécessaire afin de s’assurer que les investissements substantiels et les progrès
réalisés dans le sens de l’élimination de l'onchocercose en Afrique perdurent.

1
Recent advances in onchocerciasis research and implications for control
Background information on onchocerciasis
Introduction
Onchocerciasis is a parasitic disease caused by Onchocerca volvulus and transmitted by the bites of a black fly of
the genus Simulium. It is a debilitating dermal filariasis which is endemic mainly in tropical Africa and to a lesser
extent in Central and South America and the Arabian Peninsula, particularly in Yemen (WHO, 1995a). The clinical
and socio‐economic effects are most severe in Guinea and Sudan savanna areas where it causes blindness in
exposed humans (Leveque, 1989).
In 1875, O’Neill working with patients from the Gold Coast (Ghana) who had “craw craw”, a skin manifestation,
established the link between microfilariae and “onchocerciasis”. However, it was Leuckart in 1893 who examined
nodules extracted from patients from Gold Coast and discovered that the nodules contained adult worms which he
then named Filarial volvulus. Independently of the work of Leuckart, Theobald (1903) examined black flies from
the Democratic Republic of Congo (DRC) and named them Simulium damnosum. In spite of all the above, the
relationship between the vector and the disease remained unknown until 1926 when Blacklock working in Sierra
Leone, demonstrated the development of microfilariae into infective larvae in S. damnosum (Blacklock, 1926 a,b).
The first clinical presentation of onchocerciasis, the ocular form of the disease, was described in Guatemala
(Robles, 1919).
Global magnitude
Presently, onchocerciasis is recognised as the world’s second leading infectious cause of blindness. Figures on its
global magnitude cited in the literature are quite varied. The World Health Organization estimates that about 37
million people are currently infected with the parasite, with about 99% of them in sub‐Saharan Africa. Almost 1.5
million are visually impaired and about 500,000 are blind. A total of 90 million people are at risk of becoming
infected with the parasite (APOC, 2005; Boatin and Richards, 2006; WHO, 2011). In hyperendemic areas in Africa,
about 15 to 40% of adults could be blind because of onchocerciasis. Before the launching of the control
programme, for example in Burkina Faso, it was estimated that 46% of males and 36% of females living in
onchocerciasis hyperendemic areas became blind before their death (Prost, 1986).
The disease is endemic in Africa, Latin America and Yemen. In sub–Saharan Africa, the African onchocercal belt
extends from Senegal in the west to Ethiopia in the east involving 30 countries and as far south as Angola and
Malawi (Figure 1). The disease is also called river blindness because the blood sucking blackfly (Simulium spp)
which transmits the disease breeds in fast flowing rivers and blindness is an important clinical manifestation. In
onchocerciasis, chronic skin (dermatitis) and eye lesions are also common. It is a major public health problem in
many tropical countries (WHO, 1995a). The initial infestation often occurs in childhood, and many of the affected
individuals remain asymptomatic for long periods. A positive association has been found between river blindness
and excess mortality in infected people, either blind or not (Pion et al., 2002; Little et al., 2004).
2
Recent advances in onchocerciasis research and implications for control
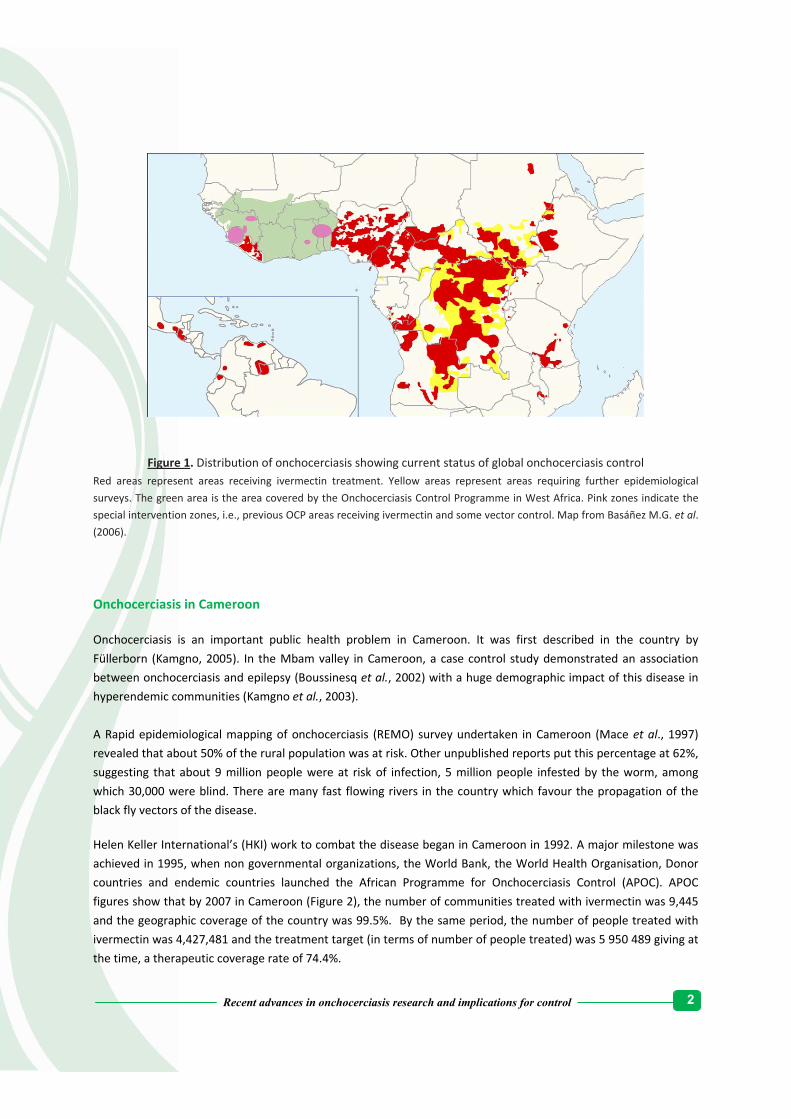
Figure 1. Distribution of onchocerciasis showing current status of global onchocerciasis control Red areas represent areas receiving ivermectin treatment. Yellow areas represent areas requiring further epidemiological
surveys. The green area is the area covered by the Onchocerciasis Control Programme in West Africa. Pink zones indicate the
special intervention zones, i.e., previous OCP areas receiving ivermectin and some vector control. Map from Basáñez M.G. et al.
(2006).
Onchocerciasis in Cameroon
Onchocerciasis is an important public health problem in Cameroon. It was first described in the country by
Füllerborn (Kamgno, 2005). In the Mbam valley in Cameroon, a case control study demonstrated an association
between onchocerciasis and epilepsy (Boussinesq et al., 2002) with a huge demographic impact of this disease in
hyperendemic communities (Kamgno et al., 2003).
A Rapid epidemiological mapping of onchocerciasis (REMO) survey undertaken in Cameroon (Mace et al., 1997)
revealed that about 50% of the rural population was at risk. Other unpublished reports put this percentage at 62%,
suggesting that about 9 million people were at risk of infection, 5 million people infested by the worm, among
which 30,000 were blind. There are many fast flowing rivers in the country which favour the propagation of the
black fly vectors of the disease.
Helen Keller International’s (HKI) work to combat the disease began in Cameroon in 1992. A major milestone was
achieved in 1995, when non governmental organizations, the World Bank, the World Health Organisation, Donor
countries and endemic countries launched the African Programme for Onchocerciasis Control (APOC). APOC
figures show that by 2007 in Cameroon (Figure 2), the number of communities treated with ivermectin was 9,445
and the geographic coverage of the country was 99.5%. By the same period, the number of people treated with
ivermectin was 4,427,481 and the treatment target (in terms of number of people treated) was 5 950 489 giving at
the time, a therapeutic coverage rate of 74.4%.
3
Recent advances in onchocerciasis research and implications for control
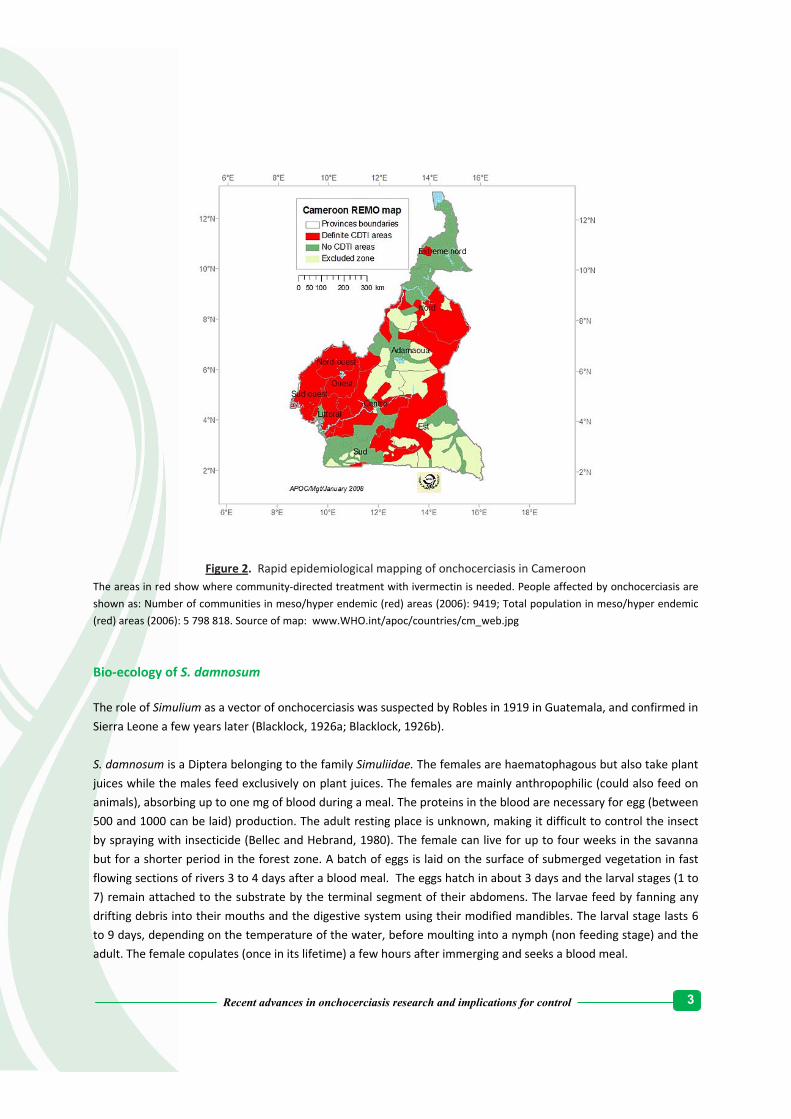
Figure 2. Rapid epidemiological mapping of onchocerciasis in Cameroon The areas in red show where community‐directed treatment with ivermectin is needed. People affected by onchocerciasis are
shown as: Number of communities in meso/hyper endemic (red) areas (2006): 9419; Total population in meso/hyper endemic
(red) areas (2006): 5 798 818. Source of map: www.WHO.int/apoc/countries/cm_web.jpg
Bio‐ecology of S. damnosum
The role of Simulium as a vector of onchocerciasis was suspected by Robles in 1919 in Guatemala, and confirmed in
Sierra Leone a few years later (Blacklock, 1926a; Blacklock, 1926b).
S. damnosum is a Diptera belonging to the family Simuliidae. The females are haematophagous but also take plant
juices while the males feed exclusively on plant juices. The females are mainly anthropophilic (could also feed on
animals), absorbing up to one mg of blood during a meal. The proteins in the blood are necessary for egg (between
500 and 1000 can be laid) production. The adult resting place is unknown, making it difficult to control the insect
by spraying with insecticide (Bellec and Hebrand, 1980). The female can live for up to four weeks in the savanna
but for a shorter period in the forest zone. A batch of eggs is laid on the surface of submerged vegetation in fast
flowing sections of rivers 3 to 4 days after a blood meal. The eggs hatch in about 3 days and the larval stages (1 to
7) remain attached to the substrate by the terminal segment of their abdomens. The larvae feed by fanning any
drifting debris into their mouths and the digestive system using their modified mandibles. The larval stage lasts 6
to 9 days, depending on the temperature of the water, before moulting into a nymph (non feeding stage) and the
adult. The female copulates (once in its lifetime) a few hours after immerging and seeks a blood meal.

4
Recent advances in onchocerciasis research and implications for control
Life cycle of Onchocerca volvulus
Onchocerca worms survive in their natural host for several years and the adult worm life span is generally
estimated to range from 10 to 15 years (Plaisier et al., 1991; Ottesen, 1995) despite ongoing cellular immune
responses and high titres of parasite‐specific IgG and IgE antibodies. There is some evidence that an active
modulation of the host’s immune system is one of the strategies permitting long‐term survival of the parasite
(Maizels et al., 1993). Throughout its life span, the adult fertilized female worm reproduces continuously, giving
birth to millions of microfilariae that are released per day and migrate to invade the skin and eyes. In the latter
case, they provoke ocular pathology resulting in blindness in humans. During feeding on the skin, the blood‐
sucking black fly vector Simulium damnosum (Philippon, 1977) ingests the skin dwelling microfilariae which
eventually develop into the third stage infective larvae (Figure 3). When the infective black fly bites a human being
again, the infective larvae from the head of the fly enter the wound and penetrate the tissues. In this definitive
host, these infective larvae moult (Figure 4) and develop to become immature adult worms enclosed in
collagenous, subcutaneous or deeper worm bundles as palpable nodules, where they develop to maturity.
Many Simulium species have been incriminated to a greater or lesser extent in the transmission of O. volvulus
(Crosskey, 1990), their relative vectorial capacities contributing to shape diverse transmission patterns in different
endemic areas. S. damnosum concurrently transmits both O. volvulus and animal Onchocerca species such as O.
ochengi. Under field conditions humans are exposed to such animal‐derived Onchocerca spp L3 (Figure 3) but they do
not develop in them. The larvae of these flies are aquatic dwellers and occur mainly in fast‐flowing water, requiring
a minimum flow of about 50 cm/s for survival. In Africa, the S. damnosum species complex, which includes
approximately 60 cytoforms, is responsible for more than 95 percent of onchocerciasis cases (Crosskey, 1990;
Crosskey and Howard, 2004). S. Neavei whose larvae are phoretic on crabs transmits the infection in East Africa. In
Latin America, S. ochraceum, S. exiguum, S. metallicum and S. guianense are the main vectors, respectively, in
Mexico and Guatemala, Colombia and Ecuador, northern Venezuela and southern Venezuela and Brazil (Bradley et
al., 2005; WHO, 2005).

5
Recent advances in onchocerciasis research and implications for control
Figure 3. Transmission cycle of Onchocerca volvulus, O.ochengi and O. ramachandrini Wharthogs are implicated in the life cycle of O.ramachandrini. Copied with permission from Renz and Wenk
(www.riverblindness.eu)
Figure 4. Life cycle of O.volvulus Copied and modified with permission from Renz and Wenk (www.riverblindness.eu)

6
Recent advances in onchocerciasis research and implications for control
Pathology of onchocerciasis
In endemic areas, the majority of O.volvulus‐infected persons develop a generalized form of the disease which is
characterized by varying microfilariae densities and numbers of adult parasites. Most often, this is accompanied by
a low degree of inflammatory processes in the skin. Generally there is a wide spectrum of ensuing pathological
events which represent the cumulative tissue and functional outcomes of a long‐standing interplay between the
host and parasite.The adult worms are enclosed in collagenous tissues where they form palpable nodules in the
skin.The nodules in humans typically range from the size of a pea to about 1‐4cm in diameter and may contain two
to four adult worms that can reach a length of 80 cm. In bovine O.ochengi, more than 12 adult male worms have
been detected living with one female worm in one nodule (Achukwi, unpublished data). The microfilariae can
survive 2 to 3 years.
After mating, the female worm releases around 1000 microfilariae larvae a day into the surrounding tissue. It is the
microfilarial stage of the parasite that causes the pathology of onchocerciasis, comprising a variety of
dermatological manifestations and eye lessions. Microfilariae concentrate in the dermis of the skin and the eyes
and most clinical pathology is seen at these two sites. The clinical spectrum may show:
i. apparently immune, clinically normal individuals;
ii. individuals who are infected yet asymptomatic;
iii. persons with eye or skin pathology.
Blindness is the most serious complication of onchocerciasis. It has been indicated that disease progression may be
influenced by factors such as an individual’s immune response (Ottesen, 1984) and the local incidence of
infestation (Bundy et al., 1991). In general, the relative importance of ocular and skin complications varies with the
parasite strain involved. Blindness tends to predominate in savannah areas and skin disease in forest areas.
Skin lesions
The skin manifestations of onchocerciasis are highly variable. Severe itching is fairly common. In endemic areas, a
small proportion of patients often described as clinically symptomatic patients, have severe dermatological lesions
that are usually confined to distinct areas of the body (Anderson et al., 1973; Buttner et al., 1982). The mechanism
underlying the propensity of some patients to develop an extremely debilitating dermatitis known as reactive
onchodermatitis (ROD) or sowda, has been a matter of controversy (Ali et al., 2003; Gallin et al., 1995; Mackenzie
et al., 1985; Murdoch et al., 1997). The factors that predispose patients to developing ROD are not clearly defined,
although it has been observed that there is an immunogenetic basis for the spectrum of cutaneous presentations
in onchocerciasis (Murdoch et al., 1997). Sowda occurs in a small proportion of patients who exhibit a hyperactive
form of onchocerciasis characterized by very low mf densities, only a few nodules with adult worms, pronounced
cellular and humoral immune responses and the ability to eliminate the microfilariae (Büttner et al., 1982; Lucius
et al., 1986; Brattig et al., 1987). The phenomenon of low microfilariae load is thought to result from an active
down regulation of parasite burdens by the host (Büttner and Racz 1983). A clinical classification of onchocercal
dermatitis defining six different patterns has been suggested by Murdoch et al. (1993) as follows:
i. Acute papular onchodermatitis – there is an early skin change characterised by widespread eczematous
rashes with multiple small pruritic papules which progress to vesicles and pustules. This form often
affects the face, the trunk and the extremities.

7
Recent advances in onchocerciasis research and implications for control
ii. Chronic papular onchodermatitis – this has a severely itching maculopapular rash containing scattered
flat‐topped papules and hyper pigmented macules, typically affecting the shoulders, the buttocks and
the extremities early in the infestation.
iii. Lichenified onchodermatitis – it consists of hyperkeratotic and hyper pigmented confluent plaques most
often affecting the lower extremities and associated with lymphadenopathy.
iv. Onchocercal depigmentation or leopard skin – has vitiligo‐like lesions with hypo pigmented patches
containing perifollicular spots of normally pigmented skin. Onchocercal depigmentation often affects
the shins in a symmetrical pattern and is rarely associated with pruritis and excoriations.
v. Onchocercal nodules – these are asymptomatic subcutaneous nodules of variable sizes located over bony
prominence and containing the adult worms. Other classic clinical pictures include lizard skins with
dry ichthyose‐like lesions with a mosaic pattern resembling the scales of a lizard.
vi. Hanging groin – characterised by folds of atrophic inelastic skin in the inguinal region associated with
lymphadenopathy.
In a population where onchodermatitis is endemic, the most common skin manifestation is chronic papular
onchodermatitis and followed by onchocercal depigmentation (Hagan, 1998).
Eye lesions
Ocular lesions can involve all eye tissues, ranging from punctuate and sclerosing keratitis (anterior segment) to
optic nerve atrophy (posterior segment). Onchocercal ocular disease covers a wide spectrum, ranging from mild
symptoms such as pruritis, redness, pain, photophobia, diffuse keratitis and blurring of vision to more severe
symptoms of corneal scarring, night blindness, intraocular inflammation, glaucoma, visual field loss and eventually,
blindness (Enk et al., 2003).
In untreated populations, the progressive nature of onchocercal ocular disease has been found to be responsible
for the existence of entire villages in which the older population was blind and only young people had functional
vision. This phenomenon was first observed in villages in proximity of rivers, the breeding site of the Simulium
black fly, hence, the name river blindness. Ocular lesions are usually bilateral and can affect various structures of
the anterior and posterior segments of the eye (Abiose, 1998). Anterior segment disease is related to the presence
of living or dead microfilariae in the eye. In the anterior chamber, the microfilariae can be seen with a slit lamp.
A number of studies have reported a reduced vitamin A status in individuals with onchocercal infections (Mustafa
et al., 1979; Zambou et al., 1999). An unpublished survey undertaken by the World Health Organization comparing
foci in West African savannah and the forest area of Cameroon showed that lesions caused by vitamin A deficiency
were more common in villages of the savannah areas with high Onchocerca parasite prevalence than in equivalent
forest zone villages, where dietary vitamin A was not limited. Posterior eye lesions such as retinitis,
choroidoretinitis and optic nerve damage are also more common in the savannah. In Côte d’Ivoire, Lagraulet
(1971) reported that individuals with onchocerciasis had lower serum vitamin A levels than comparative control
groups. These findings are controversial given that in other studies, vitamin A levels in skin or plasma were found
not to differ significantly between infected and uninfected people (Williams et al., 1985; Stürchler et al., 1987).

8
Recent advances in onchocerciasis research and implications for control
The pathogenesis of blindness is not clearly defined but it is thought that the immune reaction to the secreted
products or to the contents of dead microfilariae is important and possibly compounded by the induction of
autoimmunity to antigens of the eye. Dead microfilariae may cause severe anterior uveitis with formation of
synaechiae, cataract and glaucoma. Confluent opacities may obscure major portions of the cornea, ultimately
leading to a sclerosing keratitis with fibrovascular pannus and marked reduction of the visual functions. Posterior
segment disease manifests as atrophy of the retinal‐pigment epithelium and is associated with choroidoretinal
scarring and subretinal fibrosis (Newland et al., 1991). Optic neuritis followed by post neuritic optic atrophy may
also occur (Abiose et al., 1993).
It is thought that in chronic onchocercal infestations, a combination of both host‐ and parasite‐mediated processes
can synergize to control aberrant immune reactivity and damage to the host. This attenuation of the immune
response tends to limit the host´s capability to clear the infection (Maizels and Yazdanbakhsh, 2003; Bourke et al.,
2011).
The role of Wolbachia bacteria in pathology
Wolbachia bacteria living as symbionts of the major pathogenic filarial nematodes of humans, including O. volvulus
have during the last decade provided a breakthrough in our understanding of the pathogenesis of onchocerciasis
with dramatic implications for treatment and prevention programmes (Hoerauf et al., 2003a). Wolbachia bacteria
belong to the order Rickettsiales and are abundant in all development stages of filarial nematodes, including the
hypodermis and reproductive tissue of adult filariae.
Wolbachia species seem to have evolved as symbionts essential for worm development, survival, induction of
inflammatory disease pathogenesis and fertility of the nematode host.Their depletion results in disruption of
embryogenesis in the female worm (Bandi et al., 2001). Wolbachia‐bacterial endosymbionts also drive the
pathogenesis through the activation and regulation of host immunity (Taylor et al., 2010). Filarial and Wolbachia
antigens elicit the release of pro‐inflammatory and chemotactic cytokines by resident cells, which induce cellular
infiltration and amplification of the inflammatory response (Hise et al., 2004). It was in the bovine O.ochengi model
at the Veterinary Research Laboratory of the Institute of Agricultural Research for Development, Wakwa –
Ngaoundere in North Cameroon that it was first shown that the elimination of Wolbachia organisms led to adult
Onchocerca worm death (Langworthy et al., 2000). Thereafter, a series of field trials against onchocerciasis and
lymphatic filariasis have demonstrated that 4–8 week courses of the antibiotic doxycycline deplete the bacteria
and result in the long‐term sterility and most importantly death of adult worms (Hoerauf et al., 2001).
Socio‐economic implications of onchocerciasis
The blindness, dermatitis and chronic disability caused by onchocerciasis remain a huge socio‐economic
development impediment as the scarce labour force is weakened, the social life of several millions of people is
compromised and poverty is sustained in affected communities.
There are high mortalities of the blind victims of onchocerciasis, particulary among male patients (Prost, 1986;
Pion et al., 2002). High microfilarial loads have been reported to negatively affect the definitive host’s life
expectancy even in non blind patients (Little et al., 2004). Clinical manifestations such as epilepsy which may

9
Recent advances in onchocerciasis research and implications for control
possibly be due to heavy infestation (Boussinesq et al., 2002) may be partially responsible for excess mortality. In
most communities, epilepsy and onchodermatitis can lead to social stigmatization (Vlassoff et al., 2000).
Onchocerciasis is believed to be responsible for the annual loss of approximately one million disability‐adjusted
life‐years (DALYs). Visual impairment and blindness account for 40% of DALYs associated with onchocerciasis.
These are healthy life‐years lost due to disability and mortality, more than half of them due to skin disease
(Remme, 2004) which greatly reduces income‐generating capacity (Oladepo et al., 1997), incurs significant health
expenditures and exerts on a long‐term basis, a very high negative socio‐economic impact on the affected
populations and their land use (Evans 1995).
In sub Saharan Africa, blindness greatly diminishes agricultural production while increasing poverty and famine. In
West African valleys, onchocerciasis is known to prevent resettlement of arable lands (Hervouet and Prost, 1979).

10
Recent advances in onchocerciasis research and implications for control

11
Recent advances in onchocerciasis research and implications for control
Treatment and control of onchocerciasis
Introduction
A combination of several strategies has been used in the attempt to treat or control onchocerciasis. These include
surgical treatment, vector control, drugs and occasional mass therapy and vector control.
Surgical treatment
Denodulization through surgery has been used to prevent high rates of blindness and eye lesions as it removes
adult worms. The effect is however limited as the microfilariae remain in the body and can still be transmitted by
biting flies to other persons. It is also difficult to remove all the adult worms as some nodules are located deeply in
the tissues.
Vector control
Historical Background
Intensive work on the biology, bionomics and distribution of S. damnosum (Crosskey, 1958) and the development
of chlorinated hydrocarbons (CHC) increased the prospects of onchocerciasis control by attacking the vector. The
breakthrough came when it was shown that Dichlorodiphenyltrichloroethane (DDT), a CHC applied at very low
dosage directly into the river or stream was effective in killing Simulium larvae, thus paving the way for the
institution of vector control by larviciding. Effective vector control requires a good knowledge of the insect’s
biology and ecology. The insecticide of choice in the early days of vector control was DDT but it was replaced quite
appropriately by Temephos around 1972 as it was beginning to go out of favour due to its adverse effects on the
environment (Leveque, 1989).
Onchocerciasis vector control activities in Africa were executed in three phases. The first phase or pre‐Onchocerca
Control Programme (OCP) phase started with bush clearing activities (1932‐1944) and was followed by the use of
CHC insecticides, especially DDT (1944‐1972). The second phase or OCP phase was characterized by the use of
Temephos, an organophosphate and other larvicides (Phoxim, Pyraclofos, Permethrin, Etofenprox, Carbosulfan
and Bacillus thuringiensis H 14). The third phase or post OCP phase consisted of the introduction of focal vector
control by the African Programme for Onchocerciasis Control (APOC). In this last phase, vector control activities
were carried out using OCP guidelines and were put in place as a means to stop transmission of onchocerciasis in
some isolated foci.
In this section, we review the use of vector control in curbing black fly nuisance and the elimination of
onchocerciasis in some parts of Africa (Brown, 1962; McMahon, 1967; Davies, 1994; Walsh 1990) and discuss the
role it can play as a complement to the efforts of the African Programme for Onchocerciasis Control (APOC) in the
elimination of this disease in Cameroon and Africa.

12
Recent advances in onchocerciasis research and implications for control
The phases of vector control in Africa
The pre OCP phase (1932 – 1972)
Simulium vector control, prior to the OCP was largely experimental as there were no reference points to guide the
activities. It was characterized by environmental modifications such as bush clearing and larviciding with DDT to
control Simulium vectors. For example, bush clearing in the Kodera district in Kenya led to the eradication of S.
neavei from a small focus in Riana (Buckley, 1951). The same action in S. damnosum larval habitats around
Kinshasa did not produce the same results (Henry and Meredith, 1990). The successful demonstration of DDT as a
larvicide against Simulium larvae led to intensive pioneering experiments in Kenya and Uganda.
The control projects of this phase were largely localized schemes which lasted for short periods while others went
on for many years. Such control schemes were carried out in West and Central Africa in countries like Chad,
Cameroon, Nigeria, Benin, Burkina Faso, Côte d’Ivoire and Mali (Duke, 1964; Davies, 1968; Hitchen and Going,
1966; Walsh, 1970).
Successful vector control projects : Some of the control projects produced good results. In Benin, treatment of the
Yerpoo River which was infested with S. damnosum with 6 rounds of DDT at a dose of 1‐4 ppm/30 min greatly
reduced the population of adult flies. In Burkina Faso, treatment of the Black Volta and its tributaries with DDT
emulsion at the rate of 0.5ppm/30min from October 1962 to February 1963 at 10 day intervals reduced the
Simulium biting densities from 700 flies/man/week to 1 fly/man/week (McMahon, 1967). Small scale Simulium
vector control schemes using DDT were successfully conducted in Cameroon between 1956 and 1966 around Tiko,
Limbe and Edea to curb biting fly nuisance especially around the plantations of the Cameroon Development
Corporation (Duke 1964; Brown 1962;). In March 1978, Temephos at the dose of 0.05 – 0.10 ppm/10 min. was
used to successfully control S. squamosum nuisance at the Songloulou dam site in the forest zone. However,
resistance to Temephos was observed in June 1980 necessitating a larvicide rotation (Chlorphaxim replaced
Temephos) in 1985 (Hougard et al., 1992).
Control activities in Ghana from 1954 to 1955 achieved complete control of S. damnosum around the Kanyanbia,
Sisili, Kamba and the Black Volta Rivers. In 1959, DDT applied at 0.1 ppm/30 min. to the Black Volta and the Kamba
Rivers led to a complete control of S damnosum for 80 km. To reduce the level of nuisance at the Akosombo dam
site, several treatments with DDT (0.1 – 0.3 ppm/30 mins) were applied. Fly biting rates reduced at variable rates
between 1962 and 1963 until the reservoir was filled up inundating the breeding sites upstream (McMahon, 1967).
In Côte d’Ivoire, two S. damnosum control schemes (northern savanna area and forest zone in the south) were
executed between 1963 and 1970. Both of them were to protect two important agricultural communities from S.
damnosum nuisance (400 flies/man/day) in the rainy season. The Bagoe and the Bandama were treated at the rate
of 0.1 to 0.5 ppm/ 30 min. The results were good (McMahon, 1967). These projects were integrated into the OCP
as from 1975.
In Uganda control activities with DDT were able to eliminate the vector from three foci: the Bundongo forest in
1954, the Victoria Nile in 1973 and the Ruwenzori falls in 1976/77 (McMahon et al., 1958; Davies, 1994).
One of the most successful vector control projects was in Kenya where onchocerciasis was eradicated as a result of
the total elimination of the vector, S. neavei (Garnham and McMahon, 1947; Garnham and McMahon, 1981;

13
Recent advances in onchocerciasis research and implications for control
McMahon, 1967; McMahon et al., 1958). The developing stages of S. neavei in Kenya remained unknown until
McMahon in 1950, found the early stages of this fly to be breeding in phoretic association with the fresh water
crab (Potamonautes niloticus) in Kipsonoi River, near Kericho. The eradication of S. neavei and consequently
onchocerciasis from Kenya benefited from very favourable conditions, namely, a single vector, foci isolated from
one another and good follow‐up of activities. Three main foci: Mount Elgon, North Nyanza (Kakamega/Kaimosi)
and South Nyanza (Kisii, Kericho, Kodera, Riana) were identified. S. neavei was eradicated from the Riana sub‐focus
by bush clearing. This vector control method has never been repeated successfully anywhere else. All the other
foci were treated with DDT. The dosages varied from 1 to 2 ppm/ 30 min every 14 days, culminating in the demise
of onchocerciasis whose prevalence was up to 45% in some communities with 10% blind (McMahon et al., 1958).
The results of the Rapid Epidemiological Mapping of Onchocerciasis (REMO) indicate that Kenya, a country which
used to be hyperendemic for the disease is still free (Noma et al., 2002).
Unsuccesful vector control projects: Other vector control schemes were complete failures. For example, the Mayo
Kebi River scheme (1955 – 1959) in Chad was carried out in a 55km stretch between Tessoko and Mayo Ligam. The
treatment targeted both adults and larvae of S. sirbanum. Six applications of gamma‐BHC at 1‐2.5 ppm/30 min
were made at 3 different points on the ground. At the same time, 10 adulticide applications were made with 2%
lindane in gas oil emitted as aerosols from Bell helicopters. Both adults and larvae disappeared one week after
treatment but the flies returned in the rainy season of the same year. The failure of the project was attributed to
factors such as adult aestivation, insufficient dosing points and reinvasion from the untreated Mayo Wemba, a
tributary of the Benoue (Brown, 1962).
Other failed schemes include those carried out in Guinea Bisau (Davies, 1994) and in Nigeria around Kaduna,
Lokoja, Enugu, Niger River and Kainji dam which succeeded in reducing the Simulium populations but did not
reduce transmission as the infective rates (ranging from 0.7% to 2.95%) and the prevalence (88.04% in 1957 to
73.71% in 1960 ‐ 1966) of the disease remained high (Davies et al., 1978; Davies, 1968; Davies, 1994).
The OCP phase (1975‐2002)
The available information on the biology, bionomics and distribution of Simulium species and the existence of
ongoing small control schemes led to the convening of a meeting, sponsored by the United States Agency for
International Development (USAID), ‘Organisation de Coordination et de Coopération pour la Lutte contre les
Grandes Endémies’ (OCCGE) and WHO in Tunis in July 1968. The purpose of the meeting was to bring together
scientists to discuss the feasibility of onchocerciasis control. The meeting concluded that a large‐scale control
campaign rather than eradication was the solution. A programme was recommended involving 10‐15 years of
aerial larvicide spraying and simultaneous revamping of the health care systems of the endemic countries. The
area selected to start the trials was the Volta River Basin and extending into Senegal, Mali and Guinea. The
Onchocerciasis Control Programme (OCP) was thus born and after all technical, financial and administrative
arrangements were completed, it was launched in 1974 under the aegis of the WHO and it was operational from
1974 to 2002. Its mandate was to eliminate onchocerciasis as a disease of public health importance and as an
obstacle to socio‐economic development.
The basic strategy of OCP was to interrupt the transmission of O. volvulus by destroying the S. damnosum at its
larval stage by aerial application of selective insecticides in infested rivers so that adult onchocercal parasites could
eventually die out naturally in the human hosts (Hougard, 1993). The first aerial treatments began in 1974 and by
the end of 1977, a total of 654,000 sq. km, spread over seven countries (Burkina Faso, Mali, Niger, Cote d’Ivoire,
14
Recent advances in onchocerciasis research and implications for control
Benin, Ghana and Togo) was covered. As the operations were going on in the original programme area,
entomological observations revealed that reinvasion of the zone was compromising the control scheme. The OCP
was therefore extended to Western Mali, South Eastern Guinea, Northern Sierra Leone, Southern basins of Cote
d’Ivoire, Benin, Ghana and Togo. The insecticide selected for the operations was Temephos, an organo‐phosphate
which selectively kills the larvae of S. damnosum but is less toxic to non target fauna.
The overall authority for policy‐making, planning, programming, implementation and financing of OCP operations
was vested in the Joint Programme Committee (JPC), composed of representatives of the participating countries,
the donors and the sponsoring agencies.The Expert Advisory Committee (EAC), made up of 12 scientists, carried
out annual, independent evaluation of OCP operations and gave technical and scientific advice to the JPC and the
Programme Director. The Committee of Sponsoring Agencies (UNDP, FAO, WHO, World Bank) monitored the
Programme operations, considered management issues and reviewed the documentation for JPC.
Aerial treatment using helicopters and fixed wing small aircrafts was supplemented by ground larviciding where
appropriate. Rigorous monitoring methodologies were put in place for the follow up of both Simulium populations
and aquatic fauna during the entire life of the programme. In the course of OCP activities, it was observed that S.
damnosum developed resistance to Temephos and other larvicides (Phoxim, Pyraclofos, Permethrin, Etofenprox,
and Carbosulfan). This led to the introduction of larvicide rotation. This method was able to check the
development of larval resistance to an individual insecticide (WHO, 1987a, b).
The OCP also set the criteria for declaring a vector control programme a success as follows:
a) The “tolerable level of onchocerciasis infection” in a community: “The attainment and maintenance of all
persons living therein who were not infected with O. volvulus in the outset of the campaign, of a zero
incidence of the serious and irreversible ocular lesions resulting from onchocerciasis”.
b) An annual transmission potential (ATP) of 100 larvae was the maximum permissible transmission level.
c) The calculation of ATPs and annual biting rates (ABRs) was based on at least four catching days in a month
throughout the year.
In the same light, the Environmental Monitoring Group was set up with the responsibility of monitoring the
environmental impact of the large quantities of larvicides on the aquatic fauna. Specifically, it:
a) organized and evaluated the long‐term monitoring of the aquatic fauna;
b) assessed the level of toxicity of new products or formulations and approved or rejected their operational
use;
c) reviewed the nature and magnitude of the ecological problems connected with the programme and with
associated economic development projects proposed in areas freed from onchocerciasis in order to
identify the environmental and human ecological implications of such developments.
OCP achievements: The success of the OCP was outstanding and this led to the cessation of larviciding and the
eventual closure of the programme in 2002 (Yameogo, 2003). The OCP was the largest vector control scheme to be
attempted and it was born out of the experience gained from several pilot projects executed in Burkina Faso, Cote

15
Recent advances in onchocerciasis research and implications for control
d’Ivoire, Mali, Ghana, Benin and Togo (Walsh et al., 1979). The success of the OCP and the standards it set make it
stand out as the reference for all other Simulium control schemes in Africa.
It has been estimated that from 1974 to 2002, skin infection and eye lesions were prevented in 40 million people in
11 countries, 600,000 cases of blindness were prevented, 25 million hectares of abandoned arable land reclaimed
for settlement and agricultural production capable of feeding 17 million people annually. The economic rate of
return was calculated at 20% (Hodgkin et al., 2007).
The post OCP phase (2002 – today)
This phase of onchocerciasis control was characterized by vector control activities pioneered by APOC. In its effort
to control the disease in Africa, APOC included focal vector control in areas where the foci were shown to be so
isolated and there was no risk of re‐invasion of the foci by migratory black flies. Three such projects were identified
in Bioko Island in Equatorial Guinea (Traore et al., 2009), Itwara in Uganda (Kipp et al., 1992; Garms et al., 2009)
and Tukuyu in Tanzania (APOC, 2005). Whereas the vector was eliminated in the first two foci, the Tukuyu focus
suffered from re‐invasion problems and larviciding was suspended.
Problems of vector control
Despite the successes mentioned above, vector control as described in this section was also plagued by problems
such as resistance of the vector to larvicides, effect of the larvicides on non target organisms and reinvasion of
control areas by the vector.
Resistance of the vector to larvicides
This generally is a result of the development of genetic resistance to the organic compounds used in the control
process. Resistance involving two of the seven species of the S. damnosum complex namely, S. sanctipauli and S.
subrense was reported against the organophosphate, Temephos, in the OCP. This is thought to have developed
through selection of resistant individuals under long and intensive larvicide treatment spreading out through
dissemination. Generally, the development of resistance can be controlled by alternating the use of different
compounds. Unfortunately this approach can result in the development of resistance to multiple compounds as
was the case against chlophoxim and temephos along the tributaries of the Niger in Mali and the upper reaches of
the Sassandra River (Norgbey, 1997; Leveque, 1989).
Effect of the larvicides on non target organisms
The larvicides used in the vector control of onchocerciasis also had adverse environmental impacts. As a result of
studies carried out early in the course of larvicide applications, organochlorine insecticides were abandoned in
favour of organophosphates that were more readily biodegradable. Even the organophosphates have been shown
to have negative environmental impacts. For example, a routine spraying operation with Temephos using (0.05‐0.1
mg/l for 10 min) can produce a massive detachment of insect fauna, which is reflected by a rise in the drift, after a
15‐45 min period of latency. The mortality rate of drifting organisms has been shown to be very high. Generally,
temephos and other insecticides cause a reduction of about 30% of invertebrate fauna (Norgbey, 1997). There is
not much data on the effects of larvicides on aquatic flora. It has however, been suggested that aquatic plants can
16
Recent advances in onchocerciasis research and implications for control
break down into microscopic parts resulting in food scarcity and then reduction in fish populations following
spraying.
The results described above which had a strong impact on invertebrate organisms were for the first applications of
temephos and chlorphoxim. However, the results obtained after many years' treatment showed little long‐term
effect of the various larvicides on the non‐target fauna. The treated rivers had fairly strong resilience and a great
capacity for recovery (Leveque, 1989).
Reinvasion of control areas by the vector
Reinvasion by insect vectors following chemical control is a common phenomenon. It is often observed in Tse‐tse
fly control activities. It was a major problem in the OCP operations where flies were often carried by prevailing
winds from untreated zones close to OCP areas. The strategy employed in controlling the problem was to expand
the control area to cover the sources of departure of reinvading flies.
Drug treatment
There was no ideal drug for treating onchocerciasis before 1987. Two microfilaricides, diethylcarbamazine (DEC)
citrate and suramin were used until the 1970s when they became unpopular because of severe side effects. The
drug of choice recommended by the WHO is ivermectin (Mectizan®). Its antiparasitic properties were discovered in
1970, but it was in 1980 that clinical trials confirmed its efficiency against O. volvulus (Diallo et al., 1986; Lariviere
et al., 1989a,b,c; Greene et al., 1985a).
Control activities by APOC have been based largely on mass drug administration using ivermectin. Here we
described the role of ivermectin in the control of onchocerciasis in Africa.
Ivermectin in the control of onchocerciasis
Ivermectin family and chemical structure
The avermectins to which ivermectin belongs are macrocyclic lactones derived from the product of fermentation
of Streptomyces avermitilis. This germ was isolated from a soil sample collected near a golf course at Katawana in
Ito city, Shizuoka Prefecture in Japan. The avermectins were isolated by solvent extraction from the mycelia
solvent partition and column chromatography (Miller et al., 1979). This process of isolation was improved using
selected strains of S. avermitilis. A selective hydrogenation of avermectin B1 led to the synthesis of two molecules,
the 22, 23‐dihydroavermectin B1a (80%) and the 22, 23‐dihydroavermectin B1b (20%). The combination of these
two molecules constitutes ivermectin (Figure 5).
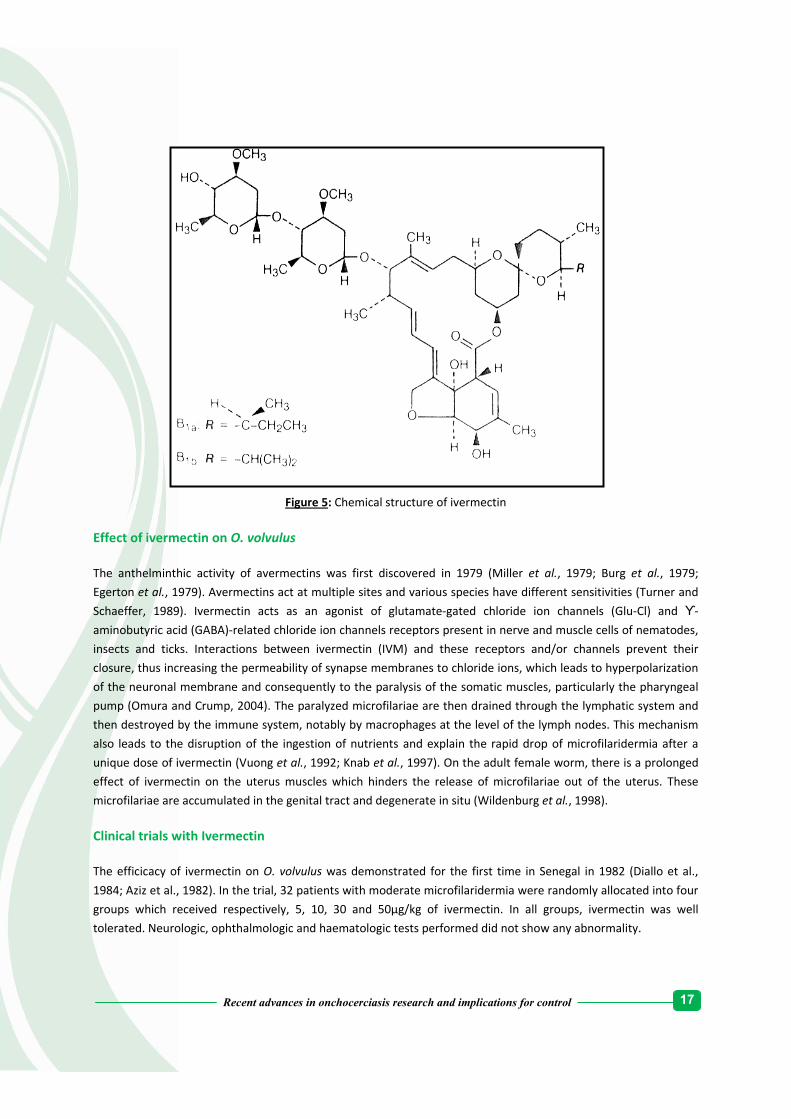
17
Recent advances in onchocerciasis research and implications for control
Figure 5: Chemical structure of ivermectin
Effect of ivermectin on O. volvulus
The anthelminthic activity of avermectins was first discovered in 1979 (Miller et al., 1979; Burg et al., 1979;
Egerton et al., 1979). Avermectins act at multiple sites and various species have different sensitivities (Turner and
Schaeffer, 1989). Ivermectin acts as an agonist of glutamate‐gated chloride ion channels (Glu‐Cl) and ϒ‐
aminobutyric acid (GABA)‐related chloride ion channels receptors present in nerve and muscle cells of nematodes,
insects and ticks. Interactions between ivermectin (IVM) and these receptors and/or channels prevent their
closure, thus increasing the permeability of synapse membranes to chloride ions, which leads to hyperpolarization
of the neuronal membrane and consequently to the paralysis of the somatic muscles, particularly the pharyngeal
pump (Omura and Crump, 2004). The paralyzed microfilariae are then drained through the lymphatic system and
then destroyed by the immune system, notably by macrophages at the level of the lymph nodes. This mechanism
also leads to the disruption of the ingestion of nutrients and explain the rapid drop of microfilaridermia after a
unique dose of ivermectin (Vuong et al., 1992; Knab et al., 1997). On the adult female worm, there is a prolonged
effect of ivermectin on the uterus muscles which hinders the release of microfilariae out of the uterus. These
microfilariae are accumulated in the genital tract and degenerate in situ (Wildenburg et al., 1998).
Clinical trials with Ivermectin
The efficicacy of ivermectin on O. volvulus was demonstrated for the first time in Senegal in 1982 (Diallo et al.,
1984; Aziz et al., 1982). In the trial, 32 patients with moderate microfilaridermia were randomly allocated into four
groups which received respectively, 5, 10, 30 and 50µg/kg of ivermectin. In all groups, ivermectin was well
tolerated. Neurologic, ophthalmologic and haematologic tests performed did not show any abnormality.

18
Recent advances in onchocerciasis research and implications for control
Phase two trials were conducted in Paris and in Ghana. In Paris, patients were treated with 150 and 200µg/kg. In
Ghana, patients were treated with 50, 100, 150 or 200µg/kg. The microfilaricidal effect was more important from
100µg/kg. Adverse events were described with the increase of the doses. These included swelling, Mazzoti
reactions, conjunctivitis with transitory blurred vision and the appearance of microfilariae in the anterior chamber
of the eye (Coulaud et al., 1983, 1984; Awadzi et al., 1995).
Phase three trials compared a unique dose of 200µg/kg of ivermectin to 7 to 8 days of Diethylcarbamazin in
Senegal (Diallo et al., 1986), Mali (Lariviere et al., 1985), Liberia (Albiez et al., 1988; Taylor et al., 1986; Greene et
al., 1985b) and Ghana (Awadzi et al., 1986). In general, these trials showed more pronounced effects of ivermectin
compared to DEC with less adverse events in ivermectin treated groups. The microfilaridermia remained low
(below 10%) during the year following the administration of a unique dose of ivermectin. An important
observation was the decrease of microfilariae in the anterior chamber of the eye. Another phase three trial with
larger sample sizes was carried out in Côte d’Ivoire, (Lariviere et al., 1989a,b,c), Ghana, (Dadzie et al., 1989; Awadzi
et al., 1989) Mali (Vingtain et al., 1988), Togo (Hussein et al., 1987) and Liberia (Taylor and Greene, 1989; Newland
et al., 1988; White et al., 1987). All the results of phase I, II and III indicated that ivermectin could be used for mass
treatment of onchocerciasis. The phase IV studies were then carried out with the objective of measuring the effect
of repeated treatments on microfilaridermia, the symptoms of onchocerciasis and the transmission of the disease.
African Programme for Onchocerciasis Control
In Africa, two key events marked onchorcerciasis control in 1987. In October of that year, ivermectin (Mectizan®),
which proved to be both well tolerated and efficient against O. volvulus microfilariae, was authorized for
commercialization for the treatment of human onchocerciasis in France. Soon after, Merck and Co., Inc took an
unprecedented decision to provide it free of charge as long as needed, to those who would ask for it to treat
onchocerciasis everywhere in the world. Merck took this decision, working in collaboration with renowned experts
in public health and parasitology, the World Health Organizaton and other agencies to combat the disease in the
endemic countries. This historic decision came nearly five years after the first human clinical trials in Dakar,
Senegal (Aziz et al., 1982). The Mectizan Donation Programme (MDP) was created the same year to coordinate the
activities related to the donation (Boussinesq et al., 1997). The drug donation facilitated the launching of the
African Programme for Onchocerciasis Control (APOC).
APOC objective and strategy
The objective of APOC was to control onchocerciasis as a public health problem from the 19 endemic countries
outside OCP area by establishing sustainable ivermectin‐based treatment projects in zones where onchocerciasis
was meso or hyperendemic.
The strategy was based on the Community‐Directed Treatment with Ivermectin (CDTI). This relied on the massive
participation of endemic communities. Members of these communities were invited to appoint people called
community‐directed distributors (CDDs), who were then trained by the local health officers and NGO. The CDDs’
tasks were to sensitize the population, carry out a census of the community members, distribute Mectizan®,
monitor treated individuals for SAEs and report them to the nearest health facilities. The CDDs worked under the
supervision of the local health staff (Homeida et al., 2002)..

19
Recent advances in onchocerciasis research and implications for control
The objectives of MDP are to supply Mectizan® to countries in need and to ensure an adequate use of drug as well
as the appropriate medical monitoring of adverse events. The MDP also put in place an expert committee
(Mectizan® Expert Committee, MEC) made up of independent scientists who provide technical support (MEC/TCC,
2004). This committee assess the quality of Mectizan® distribution projects submitted to MDP by endemic
countries, follow Mectizan® distribution process and seek to ensure the best possible use of the drug (Alleman et
al., 2006). This drug donation led to the involvement of Non Governmental Organizations in the control of
onchocerciasis. Between 1989 and 1994, Non Governmental Development Organizations (NGDOs) set up
ivermectin distribution programmes in several onchocerciasis foci in Africa. In 1991, an NGDOs coordination group
for onchocerciasis control was born in Geneva at the WHO headquarters. In 1995, building on the OCP experience,
many international organizations launched in partnership with endemic countries, donor countries and the NGOs
coordination, the African Programme for Onchocerciais Control (APOC). The programme was based on a
partnership involving various United Nations organizations, the governments of the participating countries,
endemic countries, NGOs, donor countries and the private sector (Merck & Co., Inc through the Mectizan®
Donation Programme). About thirty NGOs are presently involved in onchocerciais control in Africa. Some of them
are: Christoffel Blinden mission, Global 2000 River blindness Programme of The Carter Centre, Healthnet
International, Helen Keller International, Inter Church Medical Assistance, Lions Club International Foundation,
l’Organisation pour la Prévention de la Cécité and Sight Savers. In some countries, local NGOs take part in APOC
activities. Examples of these include Perspectives in Cameroon, Mission to Save the Helpless in Nigeria and
Christian Association of Liberia in Liberia (Cross, 2000). WHO is the programme executing agency, with the
headquarters in Ouagadougou, Burkina Faso. The financial agent is the World Bank, which set up a special fiduciary
fund where contributions from donors were paid to finance the programme activities. The Bank coordinated
actions from all the donors and mobilized funding for the programme.The endemic participating countries are
Angola, Burundi, Cameroon, Congo, Democratic Republic of Congo, Ethiopia, Equatorial Guinea, Liberia, Malawi,
Nigeria, Uganda, Central‐African Republic, Sudan, Tanzania and Chad.
Effect of the drug on the transmission of onchocerciasis
The use of ivermectin at the usual dose induces an important reduction of microfilaridermia. This reduction
persists for three to six months (Pion et al., 2011; Basanez et al., 2008) and has an impact on the number of
microfilariae that the vector can ingest during a blood meal. The impact of treatment on the transmission was
demonstrated for the first time in Liberia (Cupp et al., 1986). These authors compared the number of microfilariae
intake by Simulium from patients treated with ivermectin, DEC and placebo three weeks before. This intake was
significantly reduced in patients treated with ivermectin. In Ghana, two months after a unique dose of ivermectin,
it was shown that transmission indicators were reduced from 85 to 65% compared to the initial value (Remme et
al., 1989). In the Vina valley in Cameroon, after five years of annual treatment with ivermectin, the prevalence of
microfilaridermia in children aged 5 to 7 years old who had never been treated was reduced to 55.4%,
demonstrating a reduction in the transmission of onchocerciasis (Boussinesq et al., 1995).
Repeated treatments with ivermectin significantly contributed to the reduction of the impact of onchocerciasis in
more than 25 countries. In addition, the transmission of the disease has been interrupted in some foci in at least
10 countries and onchocerciasis is no longer seen in children in many formerly known endemic countries.
Consequently, ivermectin monotherapy for onchocerciasis control has grown tremendously, receiving funding,
technical and logistical support from international public health donors.
20
Recent advances in onchocerciasis research and implications for control
Problems associated with the use of ivermectin for onchocerciasis control
The control of onchocerciasis presently depends on mass drug distribution (MDD) using ivermectin. As at now, it is
the only drug that is being used for the mass treatment of onchocerciasis. It is given free of charge by Merck and
Co. for as long as needed.This and the use of vector control measures have been extremely effective in abating the
public health impact of onchocerciasis (Molyneux, 2005; Boatin et al., 1997). Unfortunately, there are many
problems with the use of ivermectin for onchocerciasis control. Some of these are described below:
Ivermectin is effective against the microfilariae that cause the severe manifestations of the disease. Its
main limitation is that it has little effect on the adult worms that continue to produce microfilariae and
hence re‐treatment is required at intervals that clinicians in many on‐going programmes have not
definitely determined or agreed upon. It reduces microfilariae load but does not interrupt transmission as
it is incapable of reducing the levels of infestation below those necessary to sustain transmission. At least
two treatments per year need to be continued for a long period of time. Pregnant women, breastfeeding
mothers and children below 5 years are also excluded in ivermectin treatment programmes.
There is mounting clinical and molecular evidence that resistance to ivermectin by O. volvulus is emerging
(Ardelli and Prichard, 2004; Awadzi et al., 2004a,b; Bourguinat et al., 2007; Osei‐Atweneboana et al.,
2007; Lustigman and McCarter, 2007; Canul‐Ku et al., 2011). The emergence of resistance to ivermectin
was first suggested in Ghana where sub‐optimal responses were reported in O. volvulus multi‐treated
populations (Awadzi et al., 2004a,b). Recently, it was noticed that the ability of ivermectin to suppress
microfilariae repopulation was reduced in some communities which had received mass treatment for 6 to
18 years (Osei‐Atweneboana et al., 2007, 2011). Besides these phenotypic suspicions of resistance, many
studies have revealed that selections are occurring in some genes of the parasite such as ABC transporters
(Ardelli and Prichard, 2004, 2007;Ardelli et al., 2006a), P‐glycoprotein (Ardelli et al., 2005, 2006b; Eng and
Prichard, 2005), β‐tubulin (Eng and Prichard, 2005; Eng et al., 2006; Bourguinat et al., 2006, 2007) and P‐
glycoprotein like protein (Bourguinat et al., 2008). In studies conducted in the Mbam valley, a
hyperendemic region for onchocerciasis in Cameroon, it was shown that the genetic selection induced by
ivermectin treatments was associated with a lower reproductive rate of the heterozygote female
parasites (Gardon et al., 2002).
Despite these phenotypic and genotypic studies, the unequivocal proof of resistance has yet to be established. It
was demonstrated that some confusing factors related the host immunological status (Ali et al., 2002; Babayan et
al., 2010), the drug compliance (Cabaret, 2010) and the population dynamics of the parasite (Pion et al., 2011) can
be implicated in drug failure, leading to an inaccurate conclusion of resistance.
Adverse events following treatment with ivermectin have been described, especially in patients
harbouring very high microfilarial loads. The pathogenesis of these post treatment adverse events is not
yet well described. These adverse events are categorised as follows:
• Minor and moderate adverse events
In the savanna regions, adverse events are minor or moderate. These adverse events occur after 24 to 48 hours
after treatment and consist of itching, fever, joint pain, muscle pain, headache, dizziness, general pain, oedema
and cutaneous eruption. The intensity of these adverse events depends on the intensity of infection (Whitworth et

21
Recent advances in onchocerciasis research and implications for control
al., 1991). More serious clinical adverse events (orthostatic hypotention) were described in West Africa (Awadzi,
2003; Chijioke and Okonkwo, 1992; Awadzi et al., 1989; De Sole et al., 1989a,b). The incidence of these adverse
events also depends on the prevalence of onchocerciasis and the regions. It has been reported to vary from 13 to
59.1% (Njoo et al., 1993; De Sole et al., 1989b; Kipp et al., 2003). The incidence of adverse events decreases
significantly with the years of treatments.
Immunological and pathological studies have demonstrated that minor and moderate adverse events after
treatment with ivermectin are due to inflammatory reactions associated with the destruction of microfilariae
(Wildenburg et al., 1994; Ackerman et al., 1990). It had been suggested that lipopolysaccharides (LPS) released by
endosymbiotic Wolbachia play a role in the pathogenesis of adverse events (Cross et al., 2001; Keiser et al., 2002).
It has now been shown that Wolbachia does not contain LPS and that the inflammation is driven by Wolbachia
lipoproteins (Turner et al., 2009) At the level of the eye, ivermectin provokes a transitory increase of the number
of microfilariae in the cornea, inducing a transitional blurred vision (Boussinesq, 2005). All these minor and
moderate adverse events regress spontaneously but some may need symptomatic treatment such as antalgic, anti‐
inflammatory or antihistaminic drugs.
• Severe adverse events in loaisis co‐endemic areas
The major obstacle in the control of onchocerciasis, particularly in Central Africa, is the occurrence of severe
adverse events (SAEs) after treatment with ivermectin in areas where onchocerciasis is co‐endemic with loaisis.
These post treatment reactions occur in patients harbouring high Loa loa microfilarial loads (> 8000 mf/ml)
(Boussinesq et al., 1998; Gardon et al., 1997). These adverse events are classified in two main categories, SAEs
without neurological signs and probable L. loa encephalopathies related to treatment with ivermectin.
o Adverse reactions without neurological signs
The first category corresponds to patients who do not present neurologic signs but their conditions necessitate
hospitalisation. Reactions in these patients start twelve to twenty‐four hours after treatment. Predominant
symptoms are severe headaches, fever, general pain, severe joint pains, anorexia, nausea, vomiting and diarrhoea.
These symptoms are so severe in some patients that they cannot stand up. In some patients, there are conjunctiva
and retinal haemorrhages (Fobi et al., 2000) while others develop kidney problems (Ducorps et al., 1995). The
duration of these reactions is variable. Hospitalisation is generally around 4 days but in some rare cases it has been
prolonged to two weeks. Patients with these reactions recovered without sequels. It is difficult to know if providing
prompt and proper medical care to patients with SAEs can avoid their worsening into neurological cases and
coma, but observations in some areas in Cameroon tend to confirm this hypothesis (Fokom Domgue, 2006).
Patients developing this first category of SAEs are those with 8000 mf/ml of L. loa and above.
o Probable L. loa encephalopathies related to the treatment with Ivermectin (PLERI)
PLERI are SAEs with neurological involvement occurring after treatment with ivermectin in patients with very high
microfilarial loads (> 30 000 mf/ml) ( Boussinesq et al., 1998; Gardon et al., 1997; Twum‐Danso, 2003a,b). To be
admitted as a PLERI patient, neurological symptoms should start within the week after the treatment of a healthy
individual. Four case definitions have been adopted for neurological post ivermectin SAEs (Twum‐Danso, 2003b):
22
Recent advances in onchocerciasis research and implications for control
Definite Case of Loa encephalopathy
- Encephalopathy in which brain tissue obtained by autopsy or by needle sampling has microscopic findings
consistent with L. loa encephalopathy (vasculopathy with evidence of L. loa microfilariae as a likely
aetiology);
- Onset of Central Nervous System (CNS) symptoms and signs within 7 days of treatment with ivermectin;
illness progressing to coma without remission.
Probable Case of Loa encephalopathy
- Encephalopathy (without seizures, usually with fever) in a person previously healthy and who has no
other underlying cause for encephalopathy;
- Onset of progressive CNS symptoms and signs within 7 days of treatment with ivermectin; illness
progressing to coma without remission;
- Peripheral blood L. loa > 10,000 mf/ml pre‐treatment or > 1,000 mf/ml within 1 month post‐treatment or
> 2700 mf/ml within 6 months of treatment; and/or L. loa microfilariae present in cerebrospinal fluid
(CSF) within 1 month post‐treatment.
Possible Case of Loa encephalopathy
- Encephalopathy (without seizures, usually with fever) in a person previously healthy and who has no
other underlying cause for encepahalopathy;
- Onset of progressive CNS symptoms and signs within 7 days of treatment with ivermectin; illness
progressing to coma without remission;
- Semi‐quantitative or non‐quantitative positive (i.e. +, ++, +++) L. loa microfilariae in peripheral blood
within 1 month post‐treatment.
Encephalopathy of other known aetiology
- Encephalopathy with sufficient clinical information to determine an etiology other than L. loa (e.g.
cerebral malaria)
Pathophysiology of post Ivermectin SAEs: Many hypotheses have been put forward to explain the
pathophysiology of post ivermectin SAEs. The first is the mechanical phenomenon due to the paralysis of an
important number of microfilariae in the blood stream following treatment with ivermectin. These microfilariae
are drained to the microcirculation, creating micro‐embolism and difficulty in the oxygenation of the brain and
other organs. The conjunctivae and retinal haemorrhage that occur at the level of the capillaries (Fig. 6) are in
favour of this hypothesis (Fobi et al., 2000). Another hypothesis is the passage of the microfilariae into the brain
parenchyma. The third hypothesis is the vasoconstriction of the capillaries following a complex formed by the L.
loa antigen and antibody following the death of microfilariae. The last hypothesis is the intravascular disseminated
coagulation. In some cases, it has been described as generalized haemorrhage in the brain, the kidney and the liver
(Kamgno et al., 2010).
It has also been suspected that strain variation may be responsible. Consequently, it has been hypothesized that
those who developed SAEs may be infected by a strain of Simian L. loa which has nocturnal periodicity. The
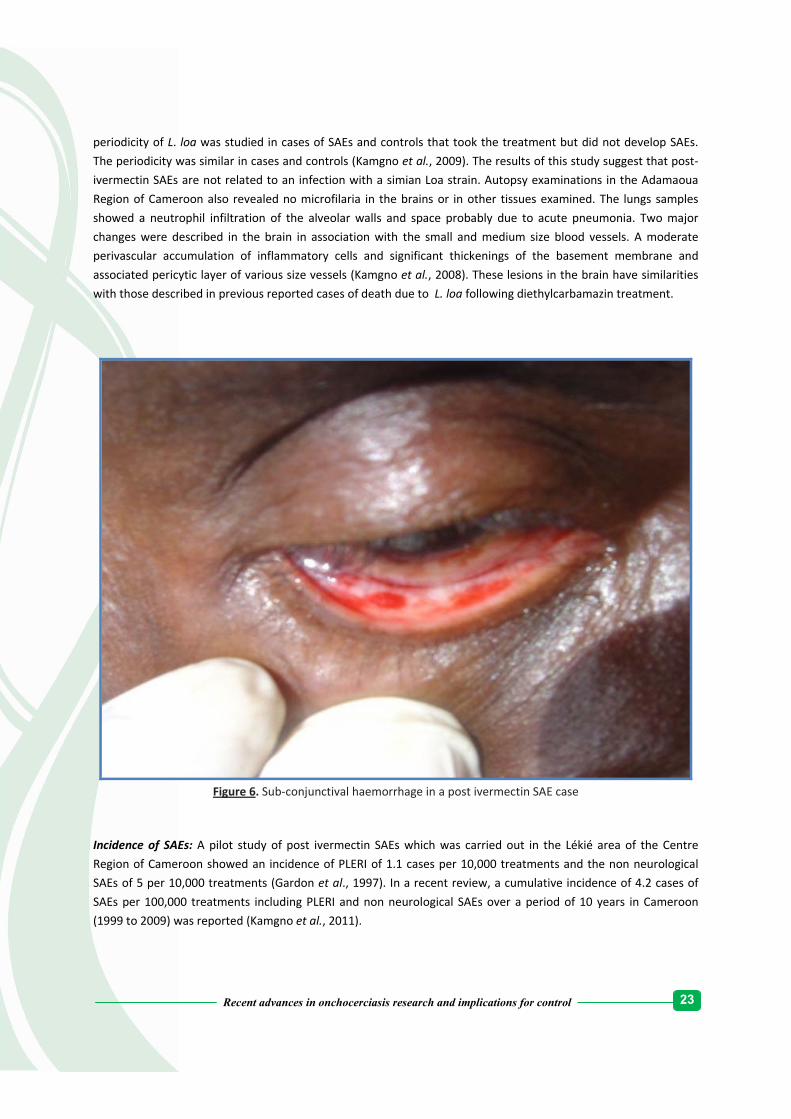
23
Recent advances in onchocerciasis research and implications for control
periodicity of L. loa was studied in cases of SAEs and controls that took the treatment but did not develop SAEs.
The periodicity was similar in cases and controls (Kamgno et al., 2009). The results of this study suggest that post‐
ivermectin SAEs are not related to an infection with a simian Loa strain. Autopsy examinations in the Adamaoua
Region of Cameroon also revealed no microfilaria in the brains or in other tissues examined. The lungs samples
showed a neutrophil infiltration of the alveolar walls and space probably due to acute pneumonia. Two major
changes were described in the brain in association with the small and medium size blood vessels. A moderate
perivascular accumulation of inflammatory cells and significant thickenings of the basement membrane and
associated pericytic layer of various size vessels (Kamgno et al., 2008). These lesions in the brain have similarities
with those described in previous reported cases of death due to L. loa following diethylcarbamazin treatment.
Figure 6. Sub‐conjunctival haemorrhage in a post ivermectin SAE case
Incidence of SAEs: A pilot study of post ivermectin SAEs which was carried out in the Lékié area of the Centre
Region of Cameroon showed an incidence of PLERI of 1.1 cases per 10,000 treatments and the non neurological
SAEs of 5 per 10,000 treatments (Gardon et al., 1997). In a recent review, a cumulative incidence of 4.2 cases of
SAEs per 100,000 treatments including PLERI and non neurological SAEs over a period of 10 years in Cameroon
(1999 to 2009) was reported (Kamgno et al., 2011).

24
Recent advances in onchocerciasis research and implications for control
In addition to all of the above, there can be acute accidental intoxication with ivermectin (7 – 8 mg/kg)
which is correlated with a clinical presentation showing vomiting, sedation and mydriasis. On the other
hand, doses of 120 mg/kg, ten times the normal adult dose for onchocerciasis treatment, was
administered to healthy subjects, without any toxicity (Guzzo et al., 2002).
There have been suggestions that ivermectine can cause teratogenic effects. However, studies have not
shown any such effects on animals treated with normal doses (Poul, 1988; Keisler et al., 1993). In
Cameroon and Liberia, a follow up of pregnant women who ignored their pregnancy status and took
ivermectin during mass treatment was conducted. No difference was found between children of
accidentally treated pregnant women and those of untreated ones (Chippaux et al., 1995; Pacque et al.,
1990).
APOC achievements
It was estimated in 2005 that 500,000 DALYs per year were averted, 177,000 communities were mobilized and a
workforce of 261,000 community distributors was trained and made available for other programmes. For the past
Quarter century (1987‐2012), over 800 million people have been treated with ivermectin for the control of
onchocerciasis in 16 countries. The economic rate of return was put at 17% and US$7 per DALY was averted
(Hodgkin et al., 2007). However, in assessing the benefits accrued through these control programmes, it is
important to also consider the number of deaths avoided in addition to the cost‐effectiveness of treatment and
the number of people prevented from becoming blind (Benton, 1998; Waters et al., 2004).
The sustained political commitment of national governments, bilateral donors, and NGDOs and the long‐term
support of onchocerciasis control coupled with the regional approach, the contribution of a diverse group of
stakeholders (Seketeli et al., 2002) and the emphasis on continued operational research contributed to a large
extent in the success levels attained by APOC.
APOC challenges
Despite the achievements of OCP and APOC, onchocerciasis has not been eradicated. Early hopes that mass
treatment with ivermectin would eradicate the disease by breaking transmission have not been realized
(Borsboom et al., 2003). Estimations based on REMO show that the mean infestation rate among countries
targeted by APOC is around 38%, with 87 million people at risk of infection (Hotez and Kamath, 2009). In 2005,
APOC estimated that in Africa, 37 million people carried O. volvulus and 90 million were at risk (APOC, 2005).
Wars and treatment complications linked to onchocerciasis and loasis co‐endemicity have been major
impediments to the expansion of APOC activities in Central Africa. In areas that are hyperendemic with L. loa,
ivermectin is contraindicated as there is a risk of (SAEs) following treatment in people who have a high
microfilaraemia of L. Loa. This can result in encephalopathy (Gardon et al., 1997; Boussinesq et al., 2006).
Furthermore, the difficult terrains in most of Africa, specific epidemiological conditions and socio‐economic
limitations have contributed in maintaining onchocerciasis in the continent. The movement of human populations
and frequent social and political upheavals in the African Region increases the risk of transmission and/or re‐
emergence of onchocerciasis.

25
Recent advances in onchocerciasis research and implications for control
Onchocerciasis control strategies in Cameroon
Introduction
Cameroon set up a national programme for onchocerciasis control in 1991. Its structure was a reflection of the
Cameroonian public health system. It has three levels: a central level made up of the central departments of the
Ministry of Public Health and the General and Central Hospitals, intermediary level made up of Regional
Delegations of Public Health and Regional Hospitals and a peripheral level comprising 189 Health Districts and
1689 Health Centres. The Health District is the basic implementation level of health programmes and projects and
hosts a district hospital. There are two dialogue structures whose members are elected by the populations at the
district level: the management Committee of the District and the District Health Committee. The health district
consists of several health areas, some of which may have Integrated Health Centres run by nurses. At the level of a
health area, there is a Health Committee and a Management Committee. These are dialogue structures
participating in the mobilization of the populations around health‐related projects and programmes.
The National Onchocerciasis Control Programme (NOCP) works under the aegis of the National Onchocerciasis Task
Force (NOTF) presided over by the Director of Disease Control of the Ministry of Public Health. The other members
of this group are: the persons in charge of health facilities in endemic areas, the representatives of the NGDOs
participating in onchocerciasis control in Cameroon, Lions Club International and members of research institutes
working on filariasis in Cameroon. In 2003, a loasis Technical Adviser in charge of the surveillance system of SAEs
events that occur after treatment with ivermectin was added to this organization and in 2005, the Centre for
Reearch on Filariasis and other Tropical Diseases (CRFilMT) was also added to it. The programme is run on a daily
basis by a Permanent Secretary who ensures its coordination.
Identification of priority populations to be treated in Cameroon
At the time of the NOCP initiation, very little data regarding onchorcerciasis endemicity were available in
Cameroon, even though the main foci were already known. As a result, a survey based on the Rapid
Epidemiological Assessment of Onchocerciasis (REA) and REMO principles was carried out in 1992 throughout the
entire Cameroonian territory (Ngoumou et al., 1994). These surveys led to the mapping of areas where
onchocerciasis was meso‐ or hyper‐endemic (that is where the nodule prevalence in men aged 20 or more is over
20%) in the country and priority areas where ivermectin should be distributed. This mapping was particularly
important in forest areas endemic for loasis where there is a risk of SAEs after treatment with ivermectin.
Consequently, it was essential to properly define onchocerciasis endemic areas in order to reduce the risk of
treated individuals developing post‐therapeutic SAEs, when the advantage associated with the treatment is not
well established. Therefore in these areas, REA was conducted to refine the distribution of onchocerciasis. Rapid
Epidemiological Assessment of Loiasis (RAPLOA) (Takougang et al., 2002; Wanji et al., 2005) and parasitological
surveys were also conducted to determine the level of endemicity of loiasis (Kamgno et al., 1997; Kamgno and
Boussinesq, 2001) and to put in place proper measures for the prevention and management of post ivermectin
SAEs) following the Technical Consultative Committee (TCC) and Mectizan Expert Committee (MEC)
recommendations. The results of these surveys as well as those achieved in the parasitological surveys (Kamgno et

26
Recent advances in onchocerciasis research and implications for control
al., 1997; Kamgno et al., 1998; Kamgno and Boussinesq, 2001) helped to determine the meso‐ and hyper‐endemic
areas eligible for CDTI as well as hypo‐endemic areas that are not CDTI‐ eligible in the whole country.
Evolution of onchocerciasis control strategies in Cameroon
Early large scale distributions
In 1987, ivermectin distribution focusing on a few thousand people was organized in the framework of phase IV
clinical drug trials. These studies were carried out in the Vina valley by ORSTOM team (currently called IRD) and in
the South West Province by a team from the Institute of Medical Research and Medicinal Plant Studies (IMPM)
(Boussinesq et al., 1993a,b; Somo et al., 1993a,b; Chippaux et al., 1999).
In 1989, the German Technical Cooperation, GTZ (Gesellshaft fur Technische Zusammenarbeit) launched the
ivermectin distribution programme in the Littoral province. Between 1992 and 1995, three NGDOs namely, the
River Blindness Foundation (RBF) (now the Carter Center), International Eye Foundation (IEF) and Helen Keller
International (HKI) signed agreements with the Ministry of Public Health to set up distribution programmes in
other provinces of Cameroon. Treatment strategies varied according to regions.
Community‐based strategies
In 1994, the NGDOs for onchocerciasis control gathered around Lions Club International Foundation (LCIF) to form
a coalition for onchocerciasis control in Cameroon. In 1995, the LCIF launched the “Sight First” project. Thereafter,
another NGDO, Sight Savers International (SSI), started a Mectizan® distribution programme in Nanga Eboko
district.
Ivermectin was distributed through two strategies described as “advanced strategy” (wherein nurses moved
around with their motor cycles from village to village to administer the drug) and “community‐based”. In the latter
case, community‐directed distributors (CDDs) appointed by the population distributed the tablets but the health
staff still had an important role to play in the process. They had to number the households, order Mectizan®,
determine the distribution period, monitor the adverse events and write up the distribution reports. Community
members helped the health staff and participated in the population mobilization. The distribution costs were still
very high and the geographic and therapeutic coverage rates were most often very low due to difficulties to reach
some communities.
The advent of the African Programme for Onchocerciasis Control in Cameroon
In 1996, APOC objectives and strategies were presented to Cameroonian authorities. The following year, a
convention covering the period from 1996 to 2001 was signed between the Ministry of Public Health and the
Directorate of APOC. The first distributions organized in the framework of APOC took place in 1999. The two
memoranda covering the period from 2001 to 2007 and the disengagement of APOC (2008‐2010) were signed in
2001. These conventions allowed different partners to submit requests for funding to APOC for CDTI projects
covering either a province of the country or a part of the province. These projects were funded up to 75 % by APOC
and the NGDO for the first year, and the remaining 25 % by Cameroon Government. APOC participation, which was
27
Recent advances in onchocerciasis research and implications for control
agreed to last 5 years, was supposed to decrease gradually while that of the government had to increase
progressively to ensure the sustainability of the programme. To date, 15 CDTI projects have been funded in
Cameroon that cover the ten regions of the country.
Difficulties related to onchocerciasis control in Cameroon
The difficulties associated with onchocerciasis control in Cameroon are: duration of treatment programmes, cost
recovery and SAEs.
i. Duration of treatment programmes
Mectizan® is a microfilaricide, with a limited effect on adult worms (Duke et al., 1991). It should be administered on
a repetitive basis each year. Mathematical simulations showed that, in order to be able to eliminate onchocerciasis
as a public health problem, 25 years of Mectizan® distribution would be necessary if programmes were able to
keep the therapeutic coverage rate at 65 %. According to previsions from developed models, if the interval
between treatments is six months rather than 12, then the duration of the programme might be halved (Winnen et
al., 2002), but this assertion is not true in all contexts.
ii. Cost recovery
The strategy for onchocerciasis control in Cameroon underwent, like the health system of the country, a number of
modifications since the NOCP was established. In 1991, when the NOCP was set up, cost recovery was a strong
principle of the Cameroon health system. As such, the NOCP adopted it. Mectizan® was received from MDP free of
charge but delivered to patients against a payment of CFA 100 (0.25 $). This cost recovery lasted until 1996 when
APOC was being established.
During the consultations with APOC officials, Cameroon expressed the wish to maintain the principle of cost
recovery despite APOC’s reticence, which dreaded its negative impact on the population’s compliance with
treatment. In this way, Cameroon unlike other countries adopted the CDTI strategy recommended by APOC but
with a particularity, the cost recovery. The CDDs received 25 F per treatment. Later on, under the pressure of
NGDOs and taking into account the fact that in some poor families, parents could afford their own drug but not
that of children, the treatment cost was reduced (10 F CFA) for children less than 15 years‐old. It was also decided
that treatment should be free of charge for poor people.
In 2002, due to a very low coverage, notably in areas where SAEs occurred, the government decided that
treatment should henceforth be free for everybody. When this decision was taken, the problem of the payment of
CDDs emerged. The Cameroon government therefore decided to pay them directly at the rate of 25 F CFA per
treated individual. This is the policy applied to date.
iii. Severe adverse events occurring after treatment with ivermectin
In Cameroon, adverse events occurring after treatment with ivermectin constitute an important obstacle
depending on the geographic areas. In areas where loasis is absent or where the prevalence and parasite load are
below 20%, adverse events are minor or moderate. On the contrary, in areas where onchocerciasis and loasis are
co‐endemic, SAEs may occur after treatment with ivermectin. These therapeutic accidents occur in people whose
parasitic loads of L. loa are very high (> 8000 mf/ml) (Gardon et al., 1997; Boussinesq et al., 1998).

28
Recent advances in onchocerciasis research and implications for control

29
Recent advances in onchocerciasis research and implications for control
Chemotherapy and immunology of onchocerciasis:
insights from the bovine model
Introduction
Research in onchocerciasis particularly that concerned with chemotherapy and immunity has been limited by the
lack of suitable animal models for O. volvulus since the parasite is very host restricted and naturally infects only
humans and gorillas. Of all animal models used to date, it is only in chimpanzees that the infection closely
resembles that in humans. This is, however, impractical for use on a large scale for research due to the cost, ethical
and conservation concerns (Copeman, 1979).
O. ochengi/cattle model for onchocerciasis research
As a result of the availability of cattle Onchocerca parasites from abattoir material and their generic relationship to
O. volvulus, bovine Onchocerca species have been extensively used in comparative studies. O. gibsoni has been
used in drug evaluation (Copeman, 1979). Unfortunately, the deep anatomical location of many bovine species
makes them unsuitable for many research studies as their viability can only be assessed on a single occasion at
post‐mortem of the host (Trees et al., 1998). This difficulty does not apply to O. ochengi.
The cattle O. ochengi forms nodules that closely resemble those formed by O. volvulus (Renz et al., 1995; Achukwi
et al., 2007). The adults of O. ochengi which are widely distributed in West Africa form multiple intradermal or
subcutaneous nodules that can be enumerated non‐invasively by palpation and sequential nodulectomies
undertaken easily to study the kinetics of the response of the macrofilariae to drugs. O. ochengi also shares some
characteristics in common with O. volvulus, such as a common arthropod vector, S. damnosum (Wahl et al., 1998)
and a very close phylogenetic relationship (Bain, 1981; Xie et al., 1994). Drug activity against microfilariae can be
evaluated by skin biopsies of the abdominal skin (Trees et al., 1998; 2000). These characteristics render the readily
accessible cattle O. ochengi a favourable model system for in vivo immunological and chemotherapeutic studies on
onchocerciasis that are not possible in humans.
A lot of studies have been carried out on this model. Published results of the studies have direct relevance to the
development of complementary therapy for river blindness given the difficulties of eliminating onchocerciasis with
ivermectin alone (Borsboom, 2003) and rising concerns about suspected resistance to this drug (Awadzi, 2004a;
Bourguinat et al., 2007).
O. ochengi and chemotherapeutic studies
Chemotherapeutic studies with anthelmintics
In the early 1990s, a team of researchers from the Veterinary Research Laboratory of IRAD Wakwa‐Ngaoundere

30
Recent advances in onchocerciasis research and implications for control
and partners from the University of Tubingen (Germany) and the Liverpool School of Tropical Medicine (UK)
started to evaluate various chemotherapeutic agents in cattle naturally infected with multiple O.ochengi nodules.
The studies were financed by the WHO‐MACROFIL Programme.
As a result of the close phylogenetic relationship between O. volvulus and O. ochengi, drug activity against both
parasites would be expected to be similar. In fact, drugs with known activities against O. volvulus, have established
the predictive value of O. ochengi in cattle. It has been shown that the effects of a number of anti‐filarial
anthelmintics, including ivermectin, suramin and melarsomine on O. ochengi are similar to those against O.
volvulus (Renz et al., 1995; Trees et al., 1998). Melarsomine had lethal effects on both microfilariae and adult
worms. Suramin only had partial effects on all worms.
Ivermectin, which was originally developed for veterinary use, has been integrated in onchocerciasis control
strategies despite the fact that there is a major stage‐related change in its efficacy against O. volvulus. Even at high
doses, it is lethal only to the L1 larvae and not to the adult worms. In adults, there is induction of some
degenerative changes in some worm tissues and the abrogation of embryogenesis but this is reversible (Kläger et
al., 1993). Its effect on the infective larvae (L3) and hence its prophylactic potential is uncertain. Tchakouté et al.
(1999) assessed the prophylactic potential of ivermectin against naturally transmitted O. ochengi in a controlled
prospective study in Wakwa‐Ngaoundere involving calves. Calves exposed to natural, fly transmitted challenge
were treated monthly with ivermectin at either 200 µg/kg or 500 µg/kg for 21 months. Infection was completely
prevented in 15 treated calves while 5 out 6 untreated controls became infected and had patent
microfilaridermias. The implication of this for humans is that strategic chemotherapy at times of maximal
transmission can be considered prophylactic as well as therapeutic against O. volvulus infection. However, for this
to be applied for mass human treatment, studies are needed to establish treatment intervals and doses required
to provide prophylaxis.
The efficacy of UMF‐078, a modified flubendazole was assessed in vivo in O. ochengi at two dosage rates by
Bronsvoort et al. (2008). Following treatment at 150 mg/kg intramuscular, nodule diameter, worm motility and
worm viability declined significantly. Embryogenesis was abrogated and death of all adult worms occurred by 24
weeks post treatment. These effects were less pronounced at 50 mg/kg intramuscular. Although no toxic signs
were observed in this trial, other studies have raised concerns regarding neuro‐ and genotoxicity with UMF‐078
(Trees et al., 1998; El‐Makawy et al., 2006).
Antibiotic therapy for onchocerciasis
The Cameroonian, British and German research group at IRAD Wakwa in North Cameroon through a chance
observation found that in an animal infected with over 100 O. ochengi nodules intended for a chemotherapeutic
trial, repeated treatment with oxytetracycline for an incidental skin infection of Dermatophilus congolensis led to
the resolution of all nodules. Also, all microfilariae were cleared from the skin of a similarly treated animal being
used for infective larvae production. In this latter case, there was subsequently no uptake of mf by feeding black
flies with a resultant zero infective larvae development in the black fly. These observations and increasing
knowledge of the existence of intracellular bacteria (Wolbachia) in filarial nematodes (Kozek and Marroquin, 1977;
Henkle‐Dührsen et al., 1998; Taylor and Hoerauf, 1999) encouraged the researchers to carry out a trial. They
demonstrated that treatment with oxytetracycline was macrofilaricidal. Embryogeneis was blocked in the female
worm, and existing microfilariae in the skin eventually disappeared as they were cleared by attrition when they

31
Recent advances in onchocerciasis research and implications for control
reached the end of their natural life span. The O. ochengi intradermal nodules were also resolved by nine months
post treatment in cattle treated intermittently for six months (Langworthy et al., 2000). Serial electron‐microscopic
examination showed that the macrofilaricididal effects were related to the elimination of intracellular bacterial
organisms. The sequential changes in the physical integrity of the organisms preceded the death of worms.
Contrary to long‐term intermittent treatment, short‐term intensive treatment that is given daily for 2 weeks
induces only transient and inconsequential effects on Wolbachia pipientis numbers and is not macrofilaricidal
(Gilbert et al., 2005).
Sequencing of a fragment of the 16s rRNA gene from the O. ochengi micro‐organisms showed them to be
Wolbachia organisms of the order Rickettsiales and were closely related to that of other Onchocerca species,
particularly O. volvulus (Bandi et al., 1998; Henkle‐Duhrsen et al., 1998).
The existence of Wolbachia as obligate intracellular bacteria in O. volvulus was first described by Kozek and
Marroquin (1977). Many filarial nematodes have a mutually dependent relationship with Wolbachia bacteria.
These endosymbionts are essential for worm development, fertility, survival and induction of inflammatory disease
pathogenesis. They are also required for successful early moulting as it has been demonstrated that the crucial
moulting step from L3 to L4 larvae is blocked by exposure of Wolbachia‐infected worms to tetracycline (Smith and
Rajan, 2000). They are Rickettsia‐like, matrilineally inherited and infect many species of invertebrates (Werren et
al., 1995; Stouthamer et al., 1999; Hise et al., 2004).
Implications for chemotherapy in humans
Wolbachia, like other Rickettsial bacteria, are susceptible to the tetracycline family of antibiotics (e.g. doxycycline),
azithromycin and rifampicin (Bandi et al., 1999 a, b; Townson et al., 2000). The existence of an almost identical
Wolbachia in O. volvulus suggests that anti‐Wolbachia treatment with these antibiotics may also be
macrofilaricidal. This can augment the success of long‐established mass treatment programmes by reducing side‐
effects that may result from the release of intact bacteria and Wolbachia products from dying nematodes (Cross et
al., 2001). Pre‐treatment targeting of Wolbachia may abrogate inflammatory responses and allow a wider range of
anti‐filarial drugs to be used (Hise et al., 2004). As a result of the fact that antibiotics do not affect the Wolbachia‐
negative L. loa which can provoke serious adverse reactions following ivermectin therapy, antibiotics can present
us a new strategy for onchocerca treatment in areas of co‐endemicity with L. loa.
The greatest obstacle to the use of antibiotic therapy in the control of onchocerciasis is the long duration of
treatment. Shorter treatment regimes are necessary if tetracyclines are to find their way into routine use against
onchocerciasis. Presently at IRAD Wakwa in North Cameroon, experiments in the proven cattle model on
chemotherapy of onchocerciasis which target Wolbachia endosymbionts of O. ochengi are being carried out with
the aim of developing optimum treatment regimes using existing drugs.
Mechanism of the macrofilaricididal action of antibiotics
Supporting evidence that the effect of the antibiotic is on the bacterial endosymbiont has been provided by studies
which showed that antibiotic treatment of Acanthocheilonema viteae and L. loa which do not contain Wolbachia
had no effect on the worm development or reproduction (Hoerauf et al., 1999; Brouqui et al., 2001). Further

32
Recent advances in onchocerciasis research and implications for control
evidence showing that antibiotics act indirectly by disrupting intracellular Wolbachia symbionts has been provided
in the review by Taylor et al. (2005).
Nfon et al. (2006) provided evidence with studies involving O. ochengi in cattle which suggest that worm killing in
onchocercomas is associated with a shift in the dominant granulocyte type surrounding the parasites, from
neutrophils to eosinophils. The presence of Wolbachia provokes neutrophil infiltration into the nodules. When
Wolbachia were eliminated following antibiotic treatment, few neutrophils were seen at sites where most bacteria
were killed. On the other hand, eosinophils which are adapted to killing worms were present in increased numbers
around worms and were observed degranulating on the filarial cuticle. These observations suggest that
accumulation of degranulating eosinophils over a prolonged period is a cause rather than an effect of parasite
death, and the macrofilaricidal mechanism of antibiotics may relate to facilitation of eosinophil infiltration around
worms by ablation of Wolbachia‐mediated neutrophilia.
It is still unclear whether the eosinophils are involved in parasite killing or if they are attracted secondarily to dying
worms. Hansen et al. (2010) tried to investigate this by giving adulticidal regimens of oxytetracycline or
melarsomine regimens to cattle infected with O. ochengi. Unlike oxytetracycline, melarsomine did not directly
affect Wolbachia viability. In the oxytetracycline group, eosinophil degranulation increased significantly and
nodular gene expression of bovine neutrophilic chemokines was lowest. Moreover, intense eosinophil
degranulation was initially associated with worm vitality, not degeneration. The data suggest that Wolbachia
confers longevity on O. ochengi through a defensive mutualism, which diverts a potentially lethal effector cell
response.
The bacterial depletion by antibiotics results in sterility of worms (through the blocking of female worm
development and embryogenesis), inhibition of larval development (by impairing microfilariae development into
L3 and interfering with moulting from L4 to adults) and inhibition of adult worm viability (Hoerauf et al., 2000a;
Casiraghi et al., 2002; Arumugam et al., 2008).
O. ochengi and immunological studies
As a result of the need for more control options for onchocerciasis, there has been growing interest in
investigating the existence of protective immunity in humans and its mechanisms, in identifying candidate vaccine
antigens and seeking evidence for prophylactic immunization. Again the O. ochengi cattle model has been an
appropriate tool for understanding the immunology of O. volvulus in humans as the biological and molecular
similarities between the two parasites and the ability to induce experimental O. ochengi infections in cattle have
made it possible to study the kinetics of immune responses to various antigens and challenge infections. This is
important for the possible development of vaccines.
Putative immunity
In endemic or hyperendemic areas, there are non‐infected individuals commonly referred to as endemic normals
or putatively immune (PI). The nature of this protective immunity has been difficult to examine in humans for
ethical reasons. Hence, Tchakoute et al. (2006) carried out a series of experiments with O. ochengi in cattle to
investigate the nature of functional immunity in onchocerciasis involving either exposure to natural field challenge

33
Recent advances in onchocerciasis research and implications for control
or experimental single‐pulse challenge. In an area endemic for O. ochengi, the authors demonstrated on the basis
of adult worm burdens that putative immunity also occurs in a subset within herds of infected cattle. The PI
animals were shown to be significantly less susceptible to heavy field challenge than age matched naïve controls.
Although they did not exhibit absolute refractoriness to O. ochengi infection, the burden of both adult parasites
and microfilariae in these animals was substantially lower than that in the controls and accumulated at a slower
rate.
Zooprophylaxis
It has been hypothesized that the predominant transmission of O. ochengi by S. damnosum in some areas of sub‐
Saharan Africa could lead to the protection of humans against onchocerciasis caused by O. volvulus. In order to
provide evidence for this, Achukwi et al. (2007) investigated whether exposure to O. volvulus could protect cattle
from O. ochengi. Gudali calves were vaccinated with live O. volvulus infective larvae and subsequently challenged
with O. ochengi infective larvae whilst raised in a fly‐proof house. The vaccinated‐challenged animals had 83–87%
less adult O. ochengi parasites than non‐vaccinated challenged animals. These findings support the idea of cross‐
protection (zooprophylaxis) due to inoculation of humans with O. ochengi infective larvae under natural
transmission conditions in endemic areas. In this experiment, no O.volvulus adult worms developed in the
vaccinated group. This is either due to their host specificity or the infective larvae were recognised and destroyed
by the cattle immune system before they could have a chance to grow to adult worms. The live O. volvulus‐
infective larvae most likely behaved like irradiation‐attenuated filarial larvae of other filariae parasites reported in
jird (Lucius et al., 1991).
O. volvulus and O. ochengi exhibit extensive antigenic cross‐reactivity as indicated by the serological recognition of
O. volvulus recombinant antigens by cattle infected with O. ochengi (Achukwi et al., 2004; Graham et al., 1999).
They can also generate cross‐protective responses both experimentally (Achukwi et al., 2007) and naturally (Wahl
et al., 1998a,b). Further evidence for all of this is provided by the fact that, molecular and biochemical comparisons
between O.volvulus and O.ochengi reveal almost identical antigenic and genomic profiles (Xie et al., 1994).
Vaccination trials
As a result of the fact that O. volvulus and O. ochengi have broad antigenic cross‐reactivity and generate cross‐
protective responses (Achukwi et al., 2004, 2007; Graham et al., 1999; Wahl et al., 1998a,b), the bovine O. ochengi
system was utilised to evaluate a recombinant vaccine in a field trial in a hyperendemic area of North Cameroon
(Makepeace et al., 2009). Naïve calves, reared in fly‐proof accommodation, were immunised with eight
recombinant antigens of O. ochengi, administered separately with either Freund’s adjuvant or alum. The selected
antigens were orthologues of O. volvulus recombinant proteins that had previously been shown to confer
protection against filarial larvae in rodent models and, in some cases, were recognised by serum antibodies from
putatively immune humans. The vaccine was highly immunogenic, eliciting a mixed IgG isotype response. Four
weeks after the final immunisation, vaccinated and adjuvant treated control calves were exposed to natural
parasite transmission by the black fly vectors in an area of Cameroon hyperendemic for O. ochengi. After 22
months, all the control animals had patent infections, compared with only 58% of vaccinated cattle. This study
shows that vaccination can reduce both the pathology and transmissibility of the infection and thus suggests that a
vaccine against microfilariae to prevent development of disease in humans may be achievable. Given that the
disease is associated with the microfilarial stage in onchocerciasis and that this stage is the key to transmission, an

34
Recent advances in onchocerciasis research and implications for control
anti‐microfilarial vaccine could be a very useful control option since it can abrogate transmission.
Tchakoute et al. (2006) also reported that vaccination with irradiated L3 of O. ochengi induced significant
protection against experimental challenge. Significantly lower worm burdens were observed in vaccinated animals
compared to controls after almost 2 years of continuous exposure to intense natural challenge from infected
Simulium. This is at variance with the failure of cattle to develop immunity after drug‐abbreviated infections. O.
volvulus‐infected humans treated with suramin, also became re‐infected after chemotherapy and developed
microfilariae loads at pre‐treatment levels (Duke, 1968). It seems that parasite death is an insufficient stimulus for
the induction of protective immunity. It has been suggested that immunity induced by irradiated L3 is mediated by
activated eosinophils (Bleiss et al., 2002; Le Goff et al., 2000; Abraham et al., 2004).

35
Recent advances in onchocerciasis research and implications for control
Antibiotic therapy for the control of onchocerciasis:
current status and perspectives
Introduction
The problems associated with the use of ivermectin for onchocerciasis control especially in the forest zones of the
Central African region where several cases of adverse reactions following ivermectin treatment were reported in
patients infected with L. loa (Chippaux et al., 1996; Gardon et al., 1997) have prompted a search for new filaricides
which could substitute ivermectin in areas of co‐endemicity and/or could be used to treat onchocerciasis without
affecting L. loa. In this regard, the discovery of Wolbachia endobacteria in some pathogenic human filarial
nematodes (Taylor et al., 1999; Taylor et al., 2005) but not L. loa (Büttner et al., 2003; McGarry et al., 2003)
presented an opportunity to take a novel approach to onchocerciasis treatment based on the use of antibiotics to
target the endobacteria (Hoerauf et al., 2001; Debrah et al., 2006). Such strategies have now been shown to be
effective in both the long‐term reduction of parasite loads and morbidity (Hoerauf et al., 2001). In animal studies,
it was observed that depletion of the Wolbachia using tetracycline not only had microfilaricidal effects but also led
to the sterility of female worms (Hoerauf et al. 1999) and the death of adult worms (Langworthy et al., 2000).
Similarly in humans, a 6‐week course of doxycycline treatment against O. volvulus depleted the bacteria, resulted
in a blockage of embryogenesis and killed the adult worms. These effects were reflected in sustained reductions in
skin microfilariae (Hoerauf et al., 2003a,b). These findings have demonstrated the superior pharmacological
efficacy of doxycycline for the treatment of onchocerciasis (Hoerauf, 2006). Macrofilaricides have a higher
potential for sustainable onchocerciasis control but this can only be guaranteed through high coverage and
compliance (Brieger et al., 2007). This is particularly important for a drug such as doxycyline that must be taken on
a daily basis for 6 weeks.
In this section, we describe:
• Antibiotic therapy in onchocerciasis by highlighting the scientific basis for the use of antibiotics;
• Treatment options with different antibiotics and how antibiotic therapy could substitute ivermectin in
problem areas where there are risks of SAEs and resistance by O. volvulus to ivermectin;
• The use of antibiotics for the treatment of onchocerciasis through the community directed approach.
A new opportunity for the treatment of onchocerciasis: the endosymbiont Wolbachia
The endosymbiont Wolbachia has generally been thought to be widespread in filarial nematodes, including the
major pathogenic filariae of humans such as Wuchereria bancrofti, Brugia malayi and O. volvulus (Casiraghi et al.,
2004). However, new evidence from a recent large‐scale survey indicates that the number of Wolbachia‐free
filarial species is greater than expected among filariae of mammals (Ferri et al., 2011). They belong to the order
Rickettsiales and are closely related to the genera Ehrlichia, Cowdria and Anaplasma. They are found in the body
wall (the hypodermis), in oocytes, in all embryonic stages and in microfilariae. Wolbachia spp in filariae seem to
have evolved as symbionts essential for the fertility of their nematode hosts and are transmitted transovarially to
the next worm generation like mitochondria.

36
Recent advances in onchocerciasis research and implications for control
Among the important filarial species investigated so far using PCR, only five species, the human filaria Loa loa, the
rodent filariae Acanthocheilonema viteae and Monanema martini, the deer filaria Onchocerca flexuosa and the
horse filaria Setaria equina appear to be free of symbionts. In filarial species positive for Wolbachia, all isolates
examined have been found to harbour this bacterium, showing identical or nearly identical gene sequences
throughout the geographical distribution of the worm (Bandi et al., 1998; Fenn et al., 2004). In addition, the
phylogeny of Wolbachia endosymbionts is congruent with the phylogeny of their host nematodes. The distribution
and phylogenetic patterns of Wolbachia in filarial nematodes indicate that the association is stable and specific
and suggests a long co‐evolutionary history (Bandi et al. 1998). This suggests co‐adaptation and reciprocal
dependence between filarial nematodes and their Wolbachia. These observations encouraged researchers to
hypothesize that antibiotic treatment against Wolbachia may be detrimental to the nematode. This has been
shown in animal studies on a variety of filarial species (Langworthy et al., 2000; Smith et al., 2000; Casiraghi et al.,
2002; Rao et al., 2002). Antibiotics have been used to deplete the endosymbionts from filariae and show the
mutualistic symbiosis between filarial Wolbachia and their hosts (Hansen et al., 2010). Depletion of Wolbachia
resulted in the disruption of embryogenesis in female worms.
Anti‐Wolbachia treatment: current status
Lessons from animal models
As shown above, several reports have described the effects of antibiotics on filarial nematodes in experimental
animal models. More importantly, members of the tetracycline family (oxytetracycline, doxycycline, minocycline)
have been found to be effective against filarial worms. The modes of action of these antibiotics are generally on
bacterial RNA polymerases, protein synthesis and other processes. They may affect similar pathways in both
worms and their Wolbachia.
In several nematode infections, the antibiotics have multiple effects on worm growth and development, worm
fertility (particularly female worm embryogenesis) and worm survival, with evidence suggesting that prolonged
treatment can be detrimental to worms (Bosshardt et al., 1993; McCall et al., 1999; Casiraghi et al., 2002).
Moreover, when microfilaraemic animals are treated, their microfilarial numbers in circulation are considerably
reduced (Hoerauf et al., 1999). In contrast, in animals infected with A. viteae worms that lack Wolbachia, similar
long‐term treatment had no effect on worm biology and development, suggesting that these bacteria play a very
important role in the growth and reproduction of the filarial worms that harbour them.
Combination studies using rifampicin and doxycycline in animal models have been found to have the potential to
achieve acceptable short‐term regimen plans (Townson et al., 1999, 2000, 2006; Specht et al. 2008). Interestingly,
in addition to anti‐Wolbachia properties, tetracyclines markedly affected the normal embryogenesis profiles by
causing damage and degeneration of intrauterine embryos. Polymerase chain reaction (PCR) assay also confirmed
the clearance of Wolbachia DNA after prolonged therapy (Volkmann et al. 2003; Kramer et al., 2003). The
reduction or clearance of bacterial specific hsp60 and Wolbachia surface protein (WSP) as determined by
immunohistochemical staining indicated the absence or clearance of Wolbachia in treated worms (Kramer, 2003).
Penicillin, gentamycin, the macrolides erythromycin and azithromycin, ciprofloxacin and chloramphenicol were
shown to be ineffective against Wolbachia in the L. sigmodontis model and consequently, did not display
antifilarial activity (Hoerauf et al., 2000).

37
Recent advances in onchocerciasis research and implications for control
Anti‐Wolbachia therapy: from animal models to humans
The availability of doxycycline has encouraged clinical investigators to test the hypothesis that elimination of
Wolbachia may be beneficial in reducing the human filarial infections. The fact that doxycycline is already
registered enabled a quick transition to phase IIa studies in human onchocerciasis, which have been carried out in
Ghana over the past ten years.
Patients were given doxycycline (100mg/day) for six weeks under daily supervision by a physician. The activity of
the drug against Wolbachia and adult worms was assessed from extirpated onchocercomas. Immunohistology with
antibodies to Wolbachia proteins was used to assess the presence or absence of Wolbachia and monitor changes
in embryogenesis. Nodules from patients not treated with doxycycline served as controls. Administration of
doxycycline led to depletion of Wolbachia followed by an interruption of embryogenesis in worms, which could be
observed for 18 months. In further trials using doxycycline at 200 mg/day for four or six weeks, interruption of
embryogenesis was observed for 24 months (Hoerauf et al., 2001). This was the longest period of sterility of
female worms ever achieved by an antifilarial drug without SAEs. Consistent with the blockage of embryogenesis,
after additional treatment with ivermectin, more than 90% of the patients who had received doxycycline showed
an absence of microfilaridermia after 18 months and the remaining patients showed very low numbers of
microfilariae. In contrast, patients treated with ivermectin alone showed an increase in microfilarial counts as early
as four months after administration of ivermectin.
Preliminary results with other doxycycline regimens indicate that 100 mg or 200 mg doxycycline per day for two
weeks does not eliminate the endobacteria or interrupt embryogenesis. When given at the dose of 200 mg/day for
four weeks, it gives the same efficacy as l00 mg for six weeks (Hoerauf et al., 2003a,b). In more recent studies, it
was demonstrated that doxycycline alone, given at 200 mg/day for 5 weeks could kill 60‐70% of adult worm
populations (Hoerauf et al., 2009).
Anti‐Wolbachia as alternative treatment for onchocerciasis in areas of co‐endemicity with loiasis
The first clinical trial with doxycycline in areas of co‐endemicity of onchocerciasis and loaisis was carried out in
forest villages of Cameroon (Wanji et al., 2009). The results confirmed previous findings that a dose of doxycycline
sufficient to deplete Wolbachia by 90% results in the death of adult worms. Histological and PCR analysis
confirmed that doxycycline treatment resulted in loss of Wolbachia from the adult parasites, with an extensive loss
of uterine contents reflecting a blockage of embryogenesis. Treatment with doxycycline alone is superior to
ivermectin in achieving sustained reductions in skin microfilariae. The trial indicates that doxycycline treatment is
well‐tolerated in O. volvulus patients co‐infected with low to moderate levels of L. loa. These findings support the
use of a doxycycline only regimen to treat onchocerciasis patients coinfected with L. loa.
Scaling up the anti‐Wolbachia treatment: the community‐directed delivery approach
The argument for mass treatment with doxycycline in areas of co‐endemicity with O.volvulus and L. loa relies
heavily on its selective toxicity for O. volvulus and the absence of adverse reactions due to lack of action on L. loa.
However, its acceptance as a complementary tool for mass treatment of onchocerciasis will very much depend on
the development of effective strategies for the treatment of target communities.

38
Recent advances in onchocerciasis research and implications for control
In view of the above, a study was designed in Cameroon to assess the feasibility of a large scale delivery of
doxycycline using the community‐directed approach for the treatment of onchocerciasis in areas of co‐endemicity
with loiasis, with the specific objective of determining the therapeutic coverage and the compliance rate and
identifying the side effects associated with the treatment (Wanji et al., 2009).
The study was carried out in communities in the Mbanga and Melong Health Districts in the Littoral Region of
Cameroon. These communities had never received mass treatment with ivermectin prior to the study. A cascade
mechanism involving advocacy meetings with all stakeholders (health system and community members) was used
to introduce the community‐directed delivery process to the population in the onchocerciasis/loiasis co‐endemic
areas. Community health implementers selected by community members were trained to deliver doxycycline and
to document the treatment coverage, compliance and side effects. This work was carried out under the
supervision of local officials of the Ministry of Public Health.
Of the 21,355 individuals identified, 17,519 were eligible for the treatment and 12,936 of these were treated with
doxycycline, giving a general therapeutic coverage of 60.6% and a therapeutic coverage per eligible population of
73.83%. Of the 12,936 individuals that started treatment in the study area, 12,612 completed the 6 weeks
treatment without missing a single treatment, giving a compliance rate of 97.5%.
Of the 371 people who had side effects recorded during the treatment, 270 (72.8%) had side effects that are well
known and associated with doxycycline intake. These included nausea (13.74%), mild diarrhoea (12.6%), vomiting
(13.7%), loss of appetite (1.1%), mild skin rash (5.9%), joint pains (7.4%), fever (4.1%), headache (6.2%), blurred
vision (2.2%) and feeling tired (9.2%). Apart from one patient who received anti‐inflammatory drugs to treat a
swollen arm, these side effects were generally mild and subsided without any intervention or interruption of
treatment.
The high therapeutic coverage achieved in this study is a prerequisite for the success of any disease control
programme. This augured well for encouraging a subsequent implementation of a large‐scale distribution of
doxycycline for the treatment of onchocerciasis in areas co‐endemic with L. loa.
Doxycycline combines the properties of being both a macro and microfilaricide on O. volvulus with 60 to 65% of
the female worms dying following a six week treatment (Hoerauf et al., 2009). It alo retards the development of O.
volvulus larvae in the vector as microfilariae depleted of Wolbachia endosymbiotic bacteria develop poorly in
Simulium spp (Albers et al., 2012).
Complying or conforming to treatment is absolutely necessary for effective treatments to have desired effects.
High compliance to treatment is dependent on the willingness and motivation of patients to follow the regimens
prescribed which is based on the information about the medication received by the patient, the complexity of the
regimen, the side effects and the benefits they may derive from the treatment (Khalid et al., 2009). In the
Cameroon study, 97.5% of the people who started treatment effectively completed it. This compliance was high
despite the long regimen of doxycycline. This is a good indicator that doxycycline can be used on a large scale for
the control of onchocerciasis using a community directed approach. The compliance rate did not vary with age or
sex of the treated population. This is an indication of good acceptability of the drug by all categories of individuals
in the community.
Several factors accounted for the high compliance rate achieved in the Cameroon study. The social awareness

39
Recent advances in onchocerciasis research and implications for control
campaigns during which the population was well informed on the process and the role they were expected to play
contributed much to its success. The fact that each partner in the CDI process adequately played his role was an
important factor for success. The awareness of the burden of onchocerciasis and its socio‐economic impacts on the
population was a motivating factor for community adherence and compliance to treatment. The fact that the drug
was delivered by community health implementers selected by community members guaranteed some trust and
was a great motivating factor for the population’s adherence and compliance. It is known that interventions
delivered by community health workers are more accepted by the population than those delivered using the
normal health system (Gyapong et al., 2000) and that it significantly improves the accessibility of the treatment
and treatment seeking behaviour of community members.
The fact that the drug was free was also an encouraging factor for the population to accept and adhere to the
treatment. The positive effects experienced by those who took the drug motivated others to request for their own
treatment.

40
Recent advances in onchocerciasis research and implications for control

41
Recent advances in onchocerciasis research and implications for control
The way forward for the elimination of onchocerciasis
The Onchocerciasis Control Programme (OCP) recognized the fact that stopping transmission could reduce the
chances of children born after the programme was initiated getting the disease but could not prevent the disease
from progressing in the adult population. Ivermectin treatment was therefore introduced to curb clinical
symptoms and halt the aggravation of ocular lesions. Chemotherapy was thus recognized as a good and less
expensive tool to control onchocerciasis and today the African Programme for the Onchocerciasis Control (APOC)
is using Community‐Directed Treatment with Ivermectin (CDTI) as its main strategy against this disease. Studies in
Mali and Senegal have established the proof‐of‐principle that onchocerciasis elimination with ivermectin
treatment is feasible in at least some endemic foci in Africa. The results have been instrumental for the current
evolution from onchocerciasis control to elimination in Africa (Traore et al., 2012). However, ivermectin has been
shown to be less effective in some communities in Ghana and transmission is still ongoing in northern Cameroon
after 17 years of ivermectin treatment (Katabarwa et al., 2011). The other problems associated with the use of
ivermectin in onchocerciasis control as listed in previous sections of this document have not disappeared.
Recently, APOC announced that it is now an elimination programme with a target date of 2025. For this to be
achieved and considering the problems identified above, it is necessary for its efforts to be accompanied by
various strategic options which should seek to be complementary. Here, we suggest some of these options.
Vector Control
The OCP which was a successful multilateral collaborative endeavour was originally based only on aerial larvicide
spraying. This approach successfully interrupted the transmission of O. volvulus in many areas. Therefore, vector
control could supplement other strategies where possible to accelerate the elimination of onchocerciasis.
Simulium control has been implemented in several areas of Cameroon as a focal activity. The on‐going
construction of new hydroelectric dams will bring human populations from all over Cameroon and beyond to settle
around these dams. This is good for the economy but has the potential of creating new health situations as the
workers come in with various transmissible diseases. The dam spillways may also constitute breeding sites for S.
damnosum, while the lakes will be breeding grounds for vectors of malaria and intermediate hosts of
schistosomiasis.
In view of the above, different control measures will need to be envisaged for various vector‐borne diseases. In the
case of onchocerciasis, vector management for black flies and drug treatment will have to be integrated for better
results. In this regard, the main rivers of Cameroon shall be targeted as they all contribute more or less to the
breeding of S. damnosum. In the savannah, where the transmission is seasonal, an S. damnosum control scheme
will go a long way to break the transmission cycle and hasten the demise of the disease. In the forest region where
transmission is perennial, the main river which is the Sanaga with its 4 dams (Edea, Song Loulou, Bamimdjin, and
Mbakaou) and soon Lom Pangal, is not new to black fly control. The Memvele dam is presently being built.
42
Recent advances in onchocerciasis research and implications for control
Recommendation 1: In view of the on‐going construction of new hydroelectric dams in Cameroon, the authorities
of the projects should already build into their operational activities, some black fly vector control components so as
to be prepared to handle any unforeseen S. damnosum population explosion after the construction. The main rivers
of Cameroon should also be the target of focal black fly control activities as they all contribute to the breeding of S.
damnosum.
A black fly control scheme as recommended above must include the following components:
1. Cartography – a good knowledge of the geography of the area with a trained team in place.
2. Hydrology – A team of hydro‐biologists with a detailed knowledge of the rivers and their seasonal
variations will monitor the larvicide treatment and its effect on the aquatic fauna.
3. Medical Entomologists – The entomologists have the duty of monitoring the black fly populations as
treatment progresses and to inform the technical team whether their work is going on well or not and to
raise an alarm in case it is not.
4. A technical team – a good technical knowledge of the treatment techniques will require persons trained
in the management of insecticides and equipment used, including aircrafts and helicopters.
Recommendation 2: Operational research is essential to improve monitoring and establish thresholds that
determine when and where vector control is needed. It is also needed to determine whether adult black flies can be
lured by attractants to insecticide treated screens as used in tsetse control, and whether insecticide treated over‐
garments or bands at the wrists and ankles could reduce the impact of the flies on field workers.
Recommendation 3: Capacity building is indispensable to increase local knowledge of vector ecology, sampling
procedures and control techniques.
The improvement of Community Directed Treatment with Ivermectin
Despite more than forty years of onchocerciasis control in Africa, the disease is still a public health concern in
many African countries. The success of OCP in West Africa led to a significant decrease of the burden of
onchocerciasis, but the disease is not yet eliminated. In APOC countries, the CDTI has improved significantly the
treatment and geographical coverage with ivermectin. The evaluation fifteen years or more after the launching of
CDTI has shown reductions in prevalence to less than 10% in some foci, and even less than 1% in some (Mas et al.,
2006; Traore et al., 2012). However, the prevalence in some other foci is still very high as shown by Katabarwa et
al. (2011) in North cameroon. It is important to understand why this is so. There may be specific epidemiological,
sociological and logistical factors that make elimination using ivermectin alone unlikely in some areas.
Recommendation 4: There is need for research organisations in charge of medical research in Cameroon to
investigate the epidemiological, sociological and logistical factors that contribute to the maintenance of high levels
of the prevalence of onchocerciasis after more than 17 years of treatment with ivermectin through the CDTI
approach in areas where loaisis is absent.
The fear of side effects in the forest communities in Cameroon where loaisis is co‐endemic has led to a reduction in
the ivermectin uptake with serious epidemiological consequences. In some surveys, it has been observed that in
43
Recent advances in onchocerciasis research and implications for control
some foci, some families had never taken Mectizan after five rounds of treatment. These families represented
about 15% of the total population. In some other areas, people who experience SAEs refuse to continue treatment.
These situations contribute to the maintenance of the transmission of the disease.
Recommendation 5: To improve the impact of treatment, the National Onchocerciasis Control Programme should
intensify communication to inform the population on the benefits of treatment with ivermectin. Efforts should also
be made to seek for permanent non compliers in order to inform, educate and properly treat them.
For CDTI in the field, the CDDs used to register the population of each village. This survey was important for the
calculation of the treatment coverage that could help in understanding the impact of the mass treatment. In the
last few years, this activity has not been taken seriously and has made it difficult to obtain accurate treatment
coverage.
Recommendation 6: To enable the collection of data which contribute to the understanding of the impact of mass
treatment, the village census should be done during CDTI field activities.
From the results of the ONCHSIM model (a microsimulation model for onchocerciasis transmission), developed by
Plaisier et al. (1990), we need more than 15 years to achieve elimination of onchocerciasis in endemic areas with
once a year treatment. With twice a year regiment, this time could be shortened by half (Winnen et al., 2002). This
could be more effective in curbing transmission since it has been shown in many studies that repopulation of
dermal microfilariae occurs as soon as four months after a single treatment with ivermectin.
Unlike the APOC strategy which used once a year treatment with ivermectin for a very long time, the treatment
frequency strategy in the Americas was established very early in the programme to be twice annually after it was
established that this would have an accelerating effect on stopping disease transmission (Cupp et al., 1992). The
MDA approach was offered at least twice each year to all eligible individuals living in all endemic communities with
the objective of reaching a minimum of 85% treatment coverage. As a result of these changes, the programme
objective in the Americas has changed from simply controlling onchocerciasis to that of completely eliminating
transmission of the disease by 2012 (Gustavsen et al., 2011).
Recommendation 7: The strategy of the control programme in the Americas which is based on at least twice yearly
treatment and which has resulted in the near elimination of onchocerciasis in that area should be adopted in all
endemic foci in general and Cameroon in particular where the results of the epidemiological evaluations are not as
good as was expected. This should be accompanied by epidemiological surveillance to detect and control disease
recurrence. Therapeutic approaches to reduce the load of L. loa infections are also necessary to increase ivermectin
coverage.
In the efforts to eliminate onchocerciasis, hypoendemic areas should not be forgotten. The present strategy
focuses on treating the meso and hyperendemic areas (with 20% and more prevalence of nodules). Areas with less
than 20% prevalence (hypoendemic areas) of nodules could constitute a reservoir of transmission, hence the
necessity for treating them. The treatment of these areas is now projected and in areas hypoendemic for
onchocerciasis and endemic for loaisis, a new strategy of “Test and Treat” is now under development.
Recommendation 8: The National Onchocerciasis Control Programme of Cameroon should adopt the new strategy
of “Test and Treat” that is being developed for hypoendemic areas.

44
Recent advances in onchocerciasis research and implications for control
To date, there is a lot of controversy regarding the emergence of resistance of O. volvulus to ivermectin. In
addition to the phenotypic suspicions of resistance, many studies have revealed that selection occurs in some
genes of the parasite. Despite these phenotypic and genotypic studies, the unequivocal proof of resistance is yet to
be established.
Recommendation 9: Further studies are needed to clarify the emergence of resistance of O. volvulus to ivermectin
in order to preserve the benefits of past and current onchocerciasis control programmes.
Anti‐Wolbachia treatment
The need for new drugs for onchocerciasis to achieve elimination of transmission cannot be over emphasised in
view of the many problems associated with the use of ivermectin for onchocerciasis control. The discovery of
Wolbachia endobacteria in some pathogenic human filarial nematodes (Taylor et al., 1999, 2005) but not L. loa
(Büttner et al., 2003; McGarry et al., 2003) gave an opportunity to study another approach to onchocerciasis
treatment based on the use of antibiotics to target the endobacteria. Results of human trials using doxycycline
(Hoerauf et al., 2001; Debrah et al., 2006; Wanji et al., 2009) have been very encouraging.
The argument for mass treatment with doxycycline in areas of co‐endemicity with O.volvulus and L. loa relies
heavily on its selective toxicity for O. volvulus and the absence of adverse reactions due to lack of action on L. loa.
However, its acceptance as a complementary tool for mass treatment of onchocerciasis will very much depend on
development of effective strategies for its delivery to the target communities.
The community‐directed intervention (CDI) trials using a 6‐week course of doxycycline challenges the notion that
prolonged courses of treatment cannot be effectively delivered through CDI (Wanji et al., 2009). The Cameroon
study showed that the intake of doxycycline on a large scale is accompanied by only mild side effects which are
generally well known to be associated with doxycycline intake. This can justify the use of this drug to treat
onchocerciasis in areas where O. volvulus and L. loa co‐exist. The high compliance rate recorded was a good
indicator that the mass administration of doxycycline for the treatment of onchocerciasis in areas of co‐endemicity
of loiasis can be a sustainable activity. RAPLOA which is a rapid diagnostic tool has been used to map areas of high
risk of encephalopathy to define restricted areas where these regimens could be deployed (Wanji et al., 2001,
2012). These areas are now well known. The regimes described above, can already be considered as suitable
treatment for individual cases of onchocerciasis in patients co‐infected with L. loa and the further development of
other anti‐Wolbachia regimens compatible with MDA could offer an alternative tool for the control on
onchocerciasis in Africa.
Recoomendation 10: Given that the recently completed community‐directed intervention using a 6‐week course of
doxycycline at a 100 mg/day demonstrated that prolonged courses of treatment can be effectively delivered either
through individual or mass treatment using doxycycline, we recommend the use of doxycycline in O. volvulus and L.
Loa co‐endemic areas and in cases of ivermectin resistance.
Mathematical simulations show that macrofilaricidal drugs have higher potentials of achieving elimination of
onchocerciasis and require less number of rounds of mass drug administration (Alley et al., 2001). It can therefore
be anticipated that with a general therapeutic coverage of 60% achieved with the community‐directed
administration of doxycycline, it may require less rounds of mass drug administration to bring the community
45
Recent advances in onchocerciasis research and implications for control
microfilarial load of O. volvulus below the threshold level of transmission in a given endemic area. Nevertheless, it
is necessary to develop a mathematical model based on data generated so far to determine the number of rounds
as well as the periodicity of mass administration of doxycycline for the control of onchocerciasis.
Recommendation 11: It is necessary for epidemiologists to develop a mathematical model to determine the
number of rounds as well as the periodicity of mass administration of doxycycline for the control of onchocerciasis.
For any health intervention to achieve its goal, the intervention must be cost effective. It should be affordable to
the health system and donors or community members. Policy and decision makers are increasingly requesting for
information on cost‐effectiveness to minimise cost of interventions and to efficiently allocate health resources.
Few studies have investigated the cost effectiveness of community based interventions. In a recent multi‐country
study on community‐directed interventions for major health problems in Africa involving eight research teams
from five African countries, it was demonstrated that community‐directed interventions are more cost‐effective
than conventional delivery systems for the integrated delivery of vitamin A, insecticide treated nets and anti‐
malarial drugs to communities. With lower implementation costs, the community directed approach achieved
higher coverage than the conventional delivery system at the health district and front line health facility levels. As
shown by Wanji et al. (2009), the community‐directed approach will be more cost effective for the delivery of
doxycycline than the conventional delivery system.
One important consideration for the large scale use of doxycycline for the treatment of onchocerciasis is the fact
that this drug is not presently made available free of charge as is the case with ivermectin. The cost (purchase and
delivery) of the six week treatment per patient is estimated at $ 2.5 (Wanji et al., 2009). Given the fact that most of
the onchocerciasis patients living in endemic communities have incomes below the poverty level, this estimated
cost may be a serious barrier to their accessibility to this therapy. It would therefore be necessary for the health
systems of endemic countries to subsidize the cost of doxycycline for the end users in the large scale treatment of
onchocerciasis where appropriate.
Recommendation 12: Given that the cost of purchase and delivery of doxycycline for the six week treatment per
patient is relatively high for most onchocerciasis patients living in endemic communities, it is necessary for the
health systems of endemic countries to subsidize the cost of the drug for the end users in the large scale treatment
of onchocerciasis where appropriate.
Currently the treatment and control of onchocerciasis rely on a single drug, ivermectin which is used in mass drug
administration (MDA) either annually or biannually or for individual every 3 to six months. It is effective at reducing
microfilarial loads but is only marginally effective against adult worms and so requires sustained delivery for more
than 15 to 17 years in order to interrupt transmission (Diawara et al. 2009; Taylor et al. 2010). Also, in areas of co‐
endemicity with loiasis, the MDA with ivermectin may have limited impact because of non compliance due to fear
of severe adverse reactions by the target population (Wanji et al; unpublished data). Recent investigations with
anti‐Wolbachial drugs have demonstrated the superior efficacy of anti‐Wolbachial drugs compared with existing
anti‐onchocercal drugs through permanent sterilization and macrofilaricidal activity against adult O. volvulus. It has
been reported that more than 97% of some 13000 people from villages where the infection is endemic started and
completed a six‐week doxycycline treatment regimen after community directed explanation and organisation and
3 to 4 years after treatment, the impact of doxycycline treatment is superior to ivermectin treatment in reducing

46
Recent advances in onchocerciasis research and implications for control
the microfilarial prevalence and intensity (Wanji et al., 2009; Tamarozzi et al. 2011). This is a major step towards
the large scale implementation of antibiotic therapy against onchocerciasis in areas of onchoecerciasis‐loiasis co‐
endemicity. This should likely speed up the elimination of onchoecrciasis in those areas.
Vaccination
It is clear that the goal of onchocerciasis eradication will not be achieved in the near future if the control strategy is
based only on vector control and ivermectin distribution. While the search for an efficient macrofilaricide remains
an attractive option today, this can be complemented with additional tools, such as vaccines that can protect
vulnerable groups particularly children living in endemic areas against infection and reduce adult worm burden and
fecundity, thus reducing the pathological effects caused by the microfilariae.
Several strategic approaches have been used to search for vaccine candidates. These include the search for target
antigens or molecules that will prevent the production of microfilariae by female worms so that severe pathology
and/or transmission of microfilariae to the black fly will be abrogated and those that could stop infection by
preventing the establishment of infective L3 larvae in the definitive host to become adult worms (i.e. prevents
worm development and patency). Other strategies have used filariae infective larvae attenuated by irradiation in
various animal models (Le Goff, 1997, 2000; Babayan et al., 2006; Tchakoute et al., 2006; Allen et al., 2008),
recombinant proteins (Makepeace et al., 2009) and live infective larvae of O. volvulus in cattle (Achukwi et al.,
2007).
Many research groups have identified a number of O.volvulus larval vaccine candidates. Trials with some of them
obtained proof‐of‐principle of vaccination against L3 infection as it was shown that microfilarial load reduced
significantly in animal models (Makepeace et al., 2009; Tchakoute et al., 2006).
Recoomendation 13: Donors should provide funding for research groups which have identified promising vaccine
candidates for the purpose of vaccine design, formulation and delivery.
Sustainability and ownership of control programmes
APOC’s mandate is expected to end in 2015. At that time, it will transfer full responsibility for onchocerciasis
control to various national control programmes. Governments would be expected to provide necessary financial
support. It is also hoped that non‐governmental development organizations will continue to play their critical role.
The overall goal is to establish country‐led programmes capable of eliminating onchocerciasis as a public health
problem in all endemic countries in Africa (2008).
However, the inability of national control programmes to sustain disease control efforts can have important
ramifications as disease resurgence can reverse the gains in public health produced by both OCP and APOC over
the years. The ability to create sustainable disease control efforts beyond APOC’s mandate will depend on the
ability of national governments to provide adequate technological and financial support for national control
programmes to enable them take on the responsibilities that would be transferred from APOC. Consequently, the
international community must ensure that national control programmes and governments have the management
and technical capacities, effective larvicides, microfilaricides, macrofilaricides and funds to continue control
efforts.

47
Recent advances in onchocerciasis research and implications for control
Recommendation 14: To create sustainable disease control efforts beyond APOC’s mandate, we urge National
Programmes to develop technical and technological competence that would enable them to function properly after
the withdrawal of APOC.
Recommendation 15: We appeal to National Governments and donors not to abdicate their financial responsibility
which is needed to ensure that the substantial investments and progress made towards eliminating onchocerciasis
in Africa are sustained for the future.

48
Recent advances in onchocerciasis research and implications for control

49
Recent advances in onchocerciasis research and implications for control
References
Abraham D., Leon O., Schnyder‐Candrian S., Wang C. C., Galioto A. M., Kerepesi L. A., Lee J. J. and Lustigman S.
(2004). Immunoglobulin E and eosinophil‐dependent protective immunity to larval Onchocerca volvulus in
mice immunized with irradiated larvae. Infect. Immun. 72: 810–817.
Abiose A. (1998). Onchocercal eye disease and the impact of Mectizan treatment. Ann. Trop. Med. Parasitol. 92
(Suppl 1): S11‐ S22.
Abiose A., Jones B.R., Cousens S.N., Murdoch I., Cassels‐Brown A., Babalola O.E., Alexander N.D., Nuhu I., Evans J.
and Ibrahim U.F. (1993). Reduction in incidence of optic nerve disease with annual ivermectin to control
onchocerciasis. Lancet 341:130–134.
Ackerman S. J., Kephart G. M., Francis H., Awadzi K., Gleich G. J. and Ottesen E. A.(1990). Eosinophil degranulation:
an immunologic determinant in the pathogenesis of the Mazzotti reaction in human onchocerciasis. J.
Immunol 144: 3961‐3969.
Achukwi M.D. Harnett W., Bradley J. and Renz A. (2004). Onchocerca ochengi acquisition in zebu Gudali cattle
exposed to natural transmission: parasite population dynamics and IgG antibody subclass responses to
Ov10/Ov11 recombinant antigens. Veterinary Parasitology 122:35‐49.
Achukwi M.D., Harnett W., Enyong P. and Renz A. (2007). Successful vaccination gainst Onchocerca ochengi
infestation in cattle using live Onchocerca volvulus infective larvae. Parasite Immunol 29: 113–116.
Albers A., Esum M.E., Tendongfor N., Enyong P., Wanji S., Hoerauf A. and Pfarr K. (2012).
Retarded Onchocerca volvulus L1 to L3 larval development in the Simulium damnosum vector after anti‐
wolbachial treatment of the human host. Parasite and Vectors 5:12
(http://www.parasitesandvectors.com/content/5/1/12).
Albiez E. J., Newland H. S., White A. T., Kaiser A., Greene B. M., Taylor H. R. and Buttner D.W. (1988).
Chemotherapy of onchocerciasis with high doses of diethylcarbamazine or a single dose of ivermectin:
microfilaria levels and side effects. Trop Med Parasitol 39: 19‐24.
Alleman M.M., Twum‐Danso N.A. and Thylefors B.I. (2006). The Mectizan Donation Program ‐ highlights from 2005.
Filaria J.5: 11.
Allen J.E., Adjei O., Bain O., Hoerauf A., Hoffmann W.H., Makepeace B.L., Schulz‐Key H., Tanya V.N., Trees A.J.,
Wanji S. and Taylor D.W. (2008). Of mice, cattle, and humans: the immunology and treatment of River
Blindness. PLoS Negl Trop Dis 2(4): e217. doi:10.1371/journal.pntd.0000217
Alley W.S., van Oortmarssen G.J., Boatin B.A., Nagelkerke N.J., Plaisier A.P., Remme J.H.,Lazdins J., Borsboom G.J.
and Habbema J.D. (2001). Macrofilaricides and onchocerciasis control: mathematical modeling of the
prospects for elimination. BMC Public Health 1: 12. Published online 2001 November 6.
doi: 10.1186/1471‐2458‐1‐12
50
Recent advances in onchocerciasis research and implications for control
Ali M.M., Baraka O.Z., Abdelrahman S.I., Sulaiman S.M., Williams J.F., Homeida M.M. and Mackenzie C.D. (2003).
Immune responses directed against microfilariae correlate with severity of clinical onchodermatitis and
treatment history. J. Infect. Dis. 187: 714–717.
Ali M.M., Mukhtar M.M., Baraka O.Z., Homeida M.M., Kheir M.M. and Mackenzie C.D. (2002). Immunocompetence
may be important in the effectiveness of Mectizan (ivermectin) in the treatment of human onchocerciasis.
Acta Trop. 84:49‐53.
Anderson J., Fuglsang H. and Al Zubaidy A. (1973). Onchocerciasis in Yemen with special reference to sowda.
Transactions of the Royal Society of Tropical Medicine and Hygiene. 67: 30‐31.
APOC (2005). Final communique of the 11th session of the Joint Action Forum (JAF) of APOC, Paris, France, 6–9
December 2005. Ouagadougou (Burkina Faso): APOC.
APOC (2008). African Programme for Onchocerciasis Control: sustainability and ownership.
www.WHO.int/apoc/sustainability/en.
Ardelli B. F., Guerriero S. B. and Prichard R. K. (2005). Genomic organization and effects of ivermectin selection on
Onchocerca volvulus P‐glycoprotein. Mol. Biochem. Parasitol.143: 58‐66.
Ardelli B. F., Guerriero S. B. and Prichard R. K. (2006a). Characterization of a half‐size ATP‐binding cassette
transporter gene which may be a useful marker for ivermectin selection in Onchocerca volvulus. Mol.
Biochem. Parasitol.145: 94‐100.
Ardelli B. F., Guerriero S. B. and Prichard R. K. (2006b). Ivermectin imposes selection pressure on P‐glycoprotein
from Onchocerca volvulus: linkage disequilibrium and genotype diversity. Parasitology 132: 375‐386.
Ardelli B. F. and Prichard R. K. (2004). Identification of variant ABC‐transporter genes among Onchocerca volvulus
collected from ivermectin‐treated and untreated patients in Ghana, West Africa. Ann. Trop. Med.
Parasitol. 98: 371‐384.
Ardelli B. F. and Prichard R. K. (2007). Reduced genetic variation of an Onchocerca volvulus ABC transporter gene
following treatment with ivermectin. Trans. R. Soc. Trop. Med. Hyg. 10: 1223‐1232.
Arumugam S., Pfarr K.M. and Hoerauf A. (2008). Infection of the intermediate mite host with Wolbachia‐depleted
Litomosoides sigmodontis microfilariae: impaired L1 to L3 development and subsequent sex‐ratio
distortion in adult worms. Int. J. Parasitol. 38: 981‐987.
Awadzi K. (2003). Clinical picture and outcome of serious adverse events in the treatment of onchocerciasis. Filaria
J. 2 Suppl 1: S6.
Awadzi K., Attah S.K., Addy E.T., Opoku N.O., Quartey B.T., Lazdins‐Helds J.K., Ahmed K., Boatin B.A., Boakye D.A.
and Edwards G. (2004a). Thirty‐month follow‐up of sub‐optimal responders to multiple treatments with
ivermectin, in two onchocerciasis‐endemic foci in Ghana. Ann. Trop. Med. Parasitol. 98: 359–370.
Awadzi K., Boakye D.A., Edwards G., Opoku N.O., Attah S.K., Osei‐Atweneboana M.Y., Lazdins‐Helds J.K., Ardrey
A.E., Addy E.T., Quartey B.T., Ahmed K., Boatin B.A. and Soumbey‐Alley E.W. (2004b). An investigation of
persistent microfilaridermias despite multiple treatments with ivermectin, in two onchocerciasis‐endemic
foci in Ghana. Ann. Trop. Med. Parasitol. 98: 231–249.
51
Recent advances in onchocerciasis research and implications for control
Awadzi K., Dadzie K.Y., Klager S. and Gilles H.M. (1989). The chemotherapy of onchocerciasis. XIII. Studies with
ivermectin in onchocerciasis patients in northern Ghana, a region with long lasting vector control. Trop.
Med. Parasitol. 40: 361‐366.
Awadzi K., Dadzie K.Y., Schulz‐Key H., Gilles H.M., Fulford A.J. and Aziz M.A. (1986). The chemotherapy of
onchocerciasis. XI. A double‐blind comparative study of ivermectin, diethylcarbamazine and placebo in
human onchocerciasis in northern Ghana. Ann. Trop. Med. Parasitol. 80: 433‐442.
Awadzi K., Hero M., Opoku N.O., Addy E.T., Buttner D.W. and Ginger C.D. (1995). The chemotherapyof
onchocerciasis XVIII. Aspects of treatment with suramin. Trop. Med. Parasitol. 46: 19‐26.
Aziz M.A., Diallo S., Diop I.M., Lariviere M. and Porta M. (1982). Efficacy and tolerance of Ivermectin in human
onchocerciasis. Lancet 2 (8291): 171‐173.
Babayan S.A., Attout T., Harris A., Taylor M.D., Le Goff L., Vuong P.N., Renia L., Allen J.E., and Bain O. (2006).
Vaccination against filarial nematodes with irradiated larvae provides long‐term protection against the
third larval stage but not against subsequent life cycle stages. Int J. Parasitol. 36: 903‐914.
Babayan S.A., Read A.F., Lawrence R.A., Bain O. and Allen J.E. (2010). Filarial parasites develop faster and
reproduce earlier in response to host immune effectors that determine filarial life expectancy. PLoS Biol.
8(10): e1000525.
Bain O. (1981). Le genre Onchocerca: hypothèses sur son évolution et clé dichotomique des espèces. Annales de
Parasitologie 56: 503‐526.
Bandi C., Slatko, B. E. and O'Neill S. L. (1999a). Wolbachia genomes and the many faces of symbiosis. Parasitol.
Today15: 428‐429.
Bandi C., Anderson T.J.C., Genchi C. and Blaxter M.L. (1998). Phylogeny of Wolbachia in filarial nematodes. Proc. R.
Soc. Lond. B 265: 2407 ‐ 2413.
Bandi C., McCall J.W., Genchi C., Corona S., Venco L., and Sacchi L. (1999b). Effects of tetracycline on the filarial
worms Brugia pahangi and Dirofilaria immitis and their bacterial endosymbionts Wolbachia. Int. J.
Parasitol.29: 357–364.
Bandi C., Trees A.J. and Brattig N.W. (2001). Wolbachia in filarial nematodes: evolutionary aspects and implications
for the pathogenesis and treatment of filarial diseases. Vet. Parasitol. 98:215‐ 38.
Basáñez M.G., Pion S.D., Boakes E., Filipe J.A., Churcher T.S. and Boussinesq M. (2008). Effect of single‐dose
ivermectin on Onchocerca volvulus: a systematic review and meta‐analysis. Lancet Infect. Dis.8: 310‐322.
Basáñez M.G., Pion S.D.S., Churcher T.S., Breitling L.P., Little M.P. and Boussinesq M. (2006). River blindness: a
success story under threat? PLoS Med. 3(9): e371.DOI:10.1371.
Bellec C. and Hebrand G. (1980). Les lieux de repos des adultes du complexe Simulium damnosum. 2. Etude de la
distribution spatio‐temporelle. Cahier Orstom sér Ent. méd. Et Parasitol. 18: 277 – 289.
Benton B. (1998). Economic impact of onchocerciasis control through the African Programme for Onchocerciasis
Control: An overview. Ann. Trop. Med. Parasitol. 92 (Suppl): S33–S39.
Blacklock D. B. (1926a). The developement of Onchocerca volvulus in Simulium damnosum. Ann. Trop. Med.
Parasitol.20: 1‐48.
52
Recent advances in onchocerciasis research and implications for control
Blacklock D.B. (1926b). The further developement of Onchocerca volvulus Leucart in Simulium damanosum
Theobald. Ann. Trop. Med. Parasitol. 20: 203‐218.
Bleiss W., Oberlander U., Hartmann S., Adam R., Marko A., Schonemeyer A. and Lucius R. (2002). Protective
immunity induced by irradiated third‐stage larvae of the filaria Acanthocheilonema viteae is directed
against challenge third‐stage larvae before molting. J. Parasitol. 88:264–270.
Boatin B., Molyneux D.H., Hougard J.M., Christensen O.W., Alley E.S., Yameogo L., Seketeli A. and Dadzie K.Y.
(1997). Patterns of epidemiology and control of onchocerciasis in West Africa. J. Helminthol. 71: 91–101.
Boatin B.A. and Richards F.O. (2006). Control of onchocerciasis. Adv. Parasitol. 61: 349–394.
Bosshardt S.C., McCall J.W., Coleman S.U., Jones K.L., Petit T.A. and Klei T.R. (1993). Prophylactic activity of
tetracycline against Brugia pahangi infection in jirds (Meriones unguiculatus). J. Parasitol. 79: 775‐777.
Borsboom G.J., Boatin B.A., Nagelkerke N.J., Agoua H., Akpoboua K.L., Alley E.W., BissanY., Renz A., Yameogo L.,
Remme J.H., Habbema J.D. (2003). Impact of ivermectin on onchocerciasis transmission: assessing the
empirical evidence that repeated ivermectin mass treatments may lead to elimination/eradication in
West Africa. Filaria Journal 2: 8.
Bourguinat C., Pion S.D., Kamgno J., Gardon J., Duke B.O., Boussinesq M. and Prichard R.K. (2007). Genetic
selection of low fertile Onchocerca volvulus by ivermectin treatment. PLoS Negl. Trop. Dis. 1: e72.
doi:10.1371/journal.pntd.0000076.
Bourguinat C., Pion S.D., Kamgno J., Gardon J., Gardon‐Wendel N., Duke B. O., PrichardR.K. and Boussinesq M.
(2006). Genetic polymorphism of the beta‐tubulin gene of Onchocerca volvulus in ivermectin naive
patients from Cameroon and its relationship with fertility of the worms. Parasitology 132: 255‐262.
Bourguinat C., Ardelli B. F., Pion S. D., Kamgno J., Gardon J., Duke B.O., Boussinesq M. And PrichardR. K. (2008). P‐
glycoprotein‐like protein, a possible genetic marker for ivermectin resistance selection in Onchocerca
volvulus. Mol. Biochem. Parasitol. 158: 101‐111.
Bourguinat C., Pion S.D., Kamgno J., Gardon J., Duke B.O., Boussinesq M. and Prichard R.K. (2007). Genetic
selection of low fertile Onchocerca volvulus by ivermectin treatment. PLoS Negl. Trop. Dis. 1: e72.
doi:10.1371/journal.pntd.0000076.
Bourke C. D., Maizels R. M. and Mutapi F. (2011). Acquired immune heterogeneity and its sources inhuman
helminth infection. Parasitology 138: 139–159.
Boussinesq M. (2005). Ivermectine. Med. Trop. 65: 69‐79.
Boussinesq M., Chippaux J.P., Ernould J. C., Quillevere D. and Prod'hon J. (1995). Effect of repeated treatments
with ivermectin on the incidence of onchocerciasis in northern Cameroon. Am. J. Trop. Med. Hyg. 53: 63‐
67.
Boussinesq M., Chippaux J.P., Ernould J.C., Prod'Hon J. and Quillevere D. (1993a). Parasitological efficacy of
repeated treatments with ivermectin in an onchocerciasis focus in north Cameroon. Bull. Soc. Pathol.
Exot.86: 112‐115.
53
Recent advances in onchocerciasis research and implications for control
Boussinesq M., Gardon J., Gardon‐Wendel N., Kamgno J., Ngoumou P. and Chippaux J.P. (1998). Three probable
cases of Loa loa encephalopathy following ivermectin treatment for onchocerciasis. Am. J. Trop. Med.
Hyg. 58: 461‐469.
Boussinesq M., Godin C. and Louis F.J. (1997). 10 years of mectizan donation. Med. Trop. 57: 345‐346.
Boussinesq M., Kamgno J., Pion S.D. and Gardon J (2006). What are the mechanisms associated with post‐
ivermectin serious adverse events? Trends Parasitol. 22: 244–246.
Boussinesq M., Pion S.D., Demanga N. and Kamgno J. (2002). Relationship between onchocerciasis and epilepsy: A
matched case‐control study in the Mbam Valley, Republic of Cameroon. Trans. R. Soc. Trop. Med. Hyg. 96:
537–541.
Boussinesq M., Prod'hon J., Chippaux J.P.and Quillevere D. (1993b). Long‐term effect of a single dose of ivermectin
on skin microfilarial density in an endemic onchocerciasis area of North Cameroon. Ann Soc Belg Med
Trop73: 189‐196.
Bradley J.E, Whitworth J.A.G. and Basanez M‐G (2005). Onchocerciasis. In: Cox F.E.G., Wakelin D., Gillespie S.H. and
Despommier D.D. (ed.) Parasitology, Topley and Wilson’s Microbiology and Microbial Infections. 10th
edition. London: Hodder Arnold. pp. 781–801.
Brattig N.W., Tischendorf F.W., Albiez E.J., Büttner D.W. and Berger J. (1987). Distribution pattern of peripheral
lymphocyte subsets in a localized and generalized form of onchocerciasis. Clin. Immunol. and
Immunopath.44:149–159.
Brieger W.R., Okeibunor J.C., Abiose A.O., Ndyomugyenyi R., Kisoka W., Wanji S., Elhassan E. and Amazigo U.V.
(2007). Feasibility of measuring compliance to annual ivermectin treatment in the African Programme for
Onchocerciasis Control. Tropical Medicine and International Health12: 260–268.
Bronsvoort B. M. deC., Makepeace B.L., Renz A., Tanya V.N., Fleckenstein L., Ekale D. and Trees A.J. (2008). UMF‐
078: A modified flubendazole with potent macrofilaricidal activity against Onchocerca ochengi in African
cattle. Parasites and Vector 1:18 doi:10.1186/1756‐3305‐1‐18.
Brouqui P., Fournier P.E. and Raoult D. (2001). Doxycycline and eradication of microfilaremia in patients with
loiasis. Emerg. Infect. Dis. 7: 604–605.
Brown A.W.A. (1962). A survey of Simulium control in Africa. Bull. Wld Hlth Org. 27:511‐527.
Buckley J.J.C. (1951). Studies on human onchocerciasis and Simulium in Nyanza province, Kenya. II The
disappearance of Simulium neavei from a bush‐cleared focus. J. Helm. 25: 213‐222.
Bundy D.A.P, Grenfell B.T. and Rajagoplan P.K. (1991). Immunoepidemiology of lymphatic filariasis: the relationship
between infection and disease. Immunology Today12: A71.
Burg R.W., Miller B.M., Backer E.E., Birnbaum J., Currie J.A., Harman R., Kong V.L., Monogham R.L.,Olson G., Putter
I., Tumac J.P., Wallick H., Stapley E.O., Oiwa R. and Omura S. (1979). The action of avermectin on
identified central neurons from Helix and its interaction with acetylcholine and gamma‐amminobutyric
acid response. Antimicrob. Agents Chemother. 15: 361‐367.
Büttner D.W. and Racz P. (1983). Macro‐and microfilariae in nodules from onchocerciasis patients in the Yemen
Arab Republic. Tropenmedizin und parasitologie 34: 113‐121.
54
Recent advances in onchocerciasis research and implications for control
Büttner D.W., von Laer G., Mannweiler E.and Büttner M. (1982). Clinical, parasitological and serological studies on
onchocerciasis in the Yemen Arab Republic. Tropenmedizin und Parasitologie 33: 201–212.
Büttner D.W., Wanji S., Bazzocchi C., Bain O. and Fischer P. (2003). Obligatory symbiotic W. pipientis endobacteria
are absent from Loa loa. Filaria J.2: 10.
Canul‐Ku H.L., Rodriguez‐Vivas R.I., Torres‐Acosta J.F.J., Aguilar‐Caballero A.J., Pérez‐Cogollo L.C. and Ojeda‐Chi
M.M. (2011). Prevalence of cattle herds with ivermectin resistant nematodes in the hot sub‐humid tropics
of Mexico. Vet. Parasitol. doi:10.1016/j.vetpar.2011.07.029.
Casiraghi M., Bain O., Guerrero R., Martin C., Pocacqua V., Gardner S.L., Franceschi A. and Bandi C. (2004).
Mapping the presence of Wolbachia pipientis on the phylogeny of filarial nematodes: evidence for
symbiont loss during evolution. Int. J. Parasitol. 34: 191‐203.
Casiraghi M., Mccall J.W., Simoncini L., Kramer L.H., Sacchi L., Genchi C., Werren J.H. and Bandi C. (2002).
Tetracycline treatment and sex‐ratio distortion: a role for Wolbachia in the moulting of filarial
nematodes? Int. J. Parasitol. 32: 1457‐1468.
Chijioke C.P. and Okonkwo P.O. (1992). Adverse events following mass ivermectin therapy for onchocerciasis.
Trans. R. Soc. Trop. Med. Hyg. 86: 284‐286.
Chippaux J.P., Boussinesq M., Fobi G., Lafleur C., Auduge A., Banos M.T., Ngosso A. and Prod'hon J. (1999). Effect of
repeated ivermectin treatments on ocular onchocerciasis: evaluation after six to eight doses. Ophthalmic
Epidemiol6: 229‐246.
Chippaux J.P., Boussinesq M., Gardon J., Gardon‐Wendel N. and Ernould J.C. (1996). Severe adverse reaction risks
during mass treatment with ivermectin in loiasis‐endemic areas. Parasitology Today 12: 448‐450.
Chippaux J.P., Gardon‐Wendel N., Ernould J.C. and Gardon J. (1995). Comparison between Various methods of
pregnancy screening during a large‐scale ivermectin treatment in Cameroon. Bull. Soc. Pathol. Exot. 88:
129‐133.
Copeman D. B. (1979). An evaluation of the Bovine‐Onchocerca gibsoni, O. gotturossa model as a tertiary screen
for drugs against O. volvulus in man. Tropical Medicine and Parasitology 30: 469‐474.
Coulaud J.P., Lariviere M., Aziz M. A., Gervais M. C., Gaxotte P., Deluol A. M. and Cenac J. (1984). Ivermectin in
onchocerciasis. Lancet 2(8401): 526‐527.
Coulaud J.P., Lariviere M., Gervais M.C., Gaxotte P., Aziz A., Deluol A.M. and Cenac J. (1983). Treatment of human
onchocerciasis with ivermectin. Bull. Soc. Pathol. Exot. Filiales 76: 681‐688.
Cross H.F., Haarbrink M., Egerton G., Yazdanbakhsh M. and Taylor M. J. (2001). Severe reactions to filarial
chemotherapy and release of Wolbachia endosymbionts into blood. Lancet 358(9296): 1873‐1875.
Crosskey R.W. (1958). First results in the control of Simulium damnosum, Theobald (Diptera, Simuliidae) in
Northern Nigeria. Bull. Entom. Res. 49: 715‐735.
Crosskey R.W. (1990). The natural history of blackflies. Chichester: John Wiley and Sons. p711.
Crosskey R.W. and Howard T.M. (2004). A revised taxonomic and geographical inventory of world blackflies
(Diptera: Simuliidae). London: The Natural History Museum. Available: http://www.nhm.ac.uk/research‐
curation/projects/blackflies.
55
Recent advances in onchocerciasis research and implications for control
Cupp E.W., Bernardo M.J., Kiszewski A.E., Collins R.C., Taylor H.R., Aziz M.A. and Greene B.M. (1986). The effects of
ivermectin on transmission of Onchocerca volvulus. Science 231: 740‐742.
Cupp E.W., Ochoa J.O., Collins R.C., Cupp M.S., Gonzales‐Peralta C., Castro J., Zea‐Flores G. (1992).The effects of
repetitive community wide ivermectin treatment on transmission of Onchocerca volvulus in Guatemala.
Am J Trop Med Hyg 47: 170‐180.
Dadzie K.Y., Awadzi K., Bird A.C. and Schulz‐Key H. (1989). Ophthalmological results from a Placebo controlled
comparative 3‐dose ivermectin study in the treatment of onchocerciasis. Trop. Med. Parasitol.40: 355‐
360.
Davies J.B. (1968). The Simulium control scheme at Abuja, Northern Nigeria and its effect on the prevalence of
onchocerciasis in the area. Bull. Wld Hlth Org., 39: 187‐207.
Davies J.B. (1994). Sixty Years of Onchocerciasis Control: A chronological summary with comments on eradication,
reinvasion and resistance. Annu. Rev. Entomol. 39. 23‐45.
Davies J.B., Le Berre R., Walsh J.F. and Cliff B. (1978). Onchocerciasis and Simulium control in the Volta River Basin.
Mosquito News 38: 466‐472.
Debrah A.Y., Mand S., Marfo–Debrekyei Y.M., Larbi J., Adjei O. and Hoerauf A. (2006). Assessment of microfilarial
loads in the skin of onchocerciasis patients after treatment with different regimens of doxycycline plus
ivermectin. Filaria J. 5:1.
De Sole G., Remme J., Awadzi K., Accorsi S., Alley E.S., Ba O., Dadzie K.Y., Giese J., Karam M. and Keita F.M. (1989).
Adverse reactions after large‐scale treatment of onchocerciasis with ivermectin: combined results from
eight community trials. Bull. World Health Organ. 67: 707‐719.
Diallo S., Aziz M.A., Lariviere M., Diallo J.S., Diop‐Mar I., N'Dir O., Badiane S., Py D., Schulz‐Key H., Gaxotte P. and
Victorius A. (1986). A double‐blind comparison of the efficacy and safety of ivermectin and
diethylcarbamazine in a placebo controlled study of Senegalese patients with onchocerciasis. Trans. R.
Soc. Trop. Med. Hyg.80: 927‐934.
Diallo S., Lariviere M., Diop Mar I., N'Dir O., N'Diaye R., Badiane S., Porta M. and Aziz M. (1984). Management in
Senegal of the first efficacy and tolerability studies of ivermectin (MK 933) in human onchocerciasis. Bull.
Soc. Pathol. Exot. Filiales 77: 196‐205.
Diawara L., Traoré M.O., Badji A., Bissan Y., Doumbia K., Goita S.F., Konaté L., Mounkoro K., Sarr M.D., Seck A.F.,
Toé L., Tourée S., and Remme J.H.F. (2009). Feasibility of onchocerciasis elimination with ivermectin
treatment in endemic foci in Africa: first evidence from studies in Mali and Senegal. PloS Negl. Trop. Dis. 3:
e497.
Duke B. O. (1968). Reinfections with Onchocerca volvulus in cured patients exposed to continuing transmission.
Bulletin of the World Health Organization 39:307–309.
Duke B.O.L. 1964‐1972. Annual Reports 1964 to 1972, Helminthiasis Research Unit, Kumba, Cameroon.
Duke B.O., Zea‐Flores G.and Munoz B. (1991). The embryogenesis of Onchocerca volvulus over the first year after a
single dose of ivermectin. Trop. Med. Parasitol.42: 175‐180.
56
Recent advances in onchocerciasis research and implications for control
Ducorps M., Gardon‐Wendel N., Ranque S., Ndong W., Boussinesq M., Gardon J., Schneider D. and Chippaux J.P.
(1995). Secondary effects of the treatment of hypermicrofilaremic loiasis using ivermectin. Bull. Soc.
Pathol. Exot.88: 105‐112.
Egerton J.R., Otslind D.A., Blair L.S., Eary D.H., Suhayda D., Cifelli S., Riek R.F. and Campbell W.C. (1979).
Avermectins, new family of potent anthelminthic agents: efficacy of B1a component. Antimicrob. Agents
Chemother. 15: 372‐378.
El‐Makawy A., Radwan H.A, Ghaly I.S. and El‐Raouf A.A. (2006). Genotoxical, teratological and biochemical effects
of anthelmintic drug oxfendazole maximum residue limit (MRL) in male and female mice. Reproduction,
Nutrition, Development 46: 139‐156.
Enk C.D., Anteby I., Abramson N., Amer R., Amit Y., Bergshtein‐Kronhaus T., Cohen E., Greenberg Z., Jonas F.,
Maayan S., Marva E., Strauss U. and Ben Ezra D. (2003). Onchocerciasis among Ethiopian immigrants in
Israel. Isr. Med. Assoc. J. 5: 485 ‐ 488.
Eng J.K., Blackhall W.J., Osei‐Atweneboana M.Y., Bourguinat C., Galazzo D., Beech R.N., UnnaschT.R., Awadzi K.,
Lubega G.W. and Prichard R.K. (2006). Ivermectin selection on beta‐tubulin: evidence in Onchocerca
volvulus and Haemonchus contortus. Mol. Biochem. Parasitol.150: 229‐235.
Eng J.K. and Prichard R.K. (2005). A comparison of genetic polymorphism in populations of Onchocerca volvulus
from untreated‐ and ivermectin‐treated patients. Mol. Biochem. Parasitol.142: 193‐202.
Evans T.G. (1995). Socioeconomic consequences of blinding onchocerciasis in West Africa. Bull. World Health
Organ. 73: 495–506.
Fenn K. and Blaxter M. (2004). Quantification of Wolbachia bacteria in Brugia malayi through the nematode life
cycle. Mol. Biochem.Parasitol. 137: 361‐364.
Ferri E., Bain O., Barbuto M., Martin C., Lo N., Uni S., Landmann F., Baccei S.G., Guerrero R., Lima S.S., Bandi C.,
Wanji S., Diagne M. and Casiraghi M. (2011). New insights into the evolution of Wolbachia infections in
filarial nematodes inferred from a large range of screened species. PLoS ONE 6(6): e20843.
doi:10.1371/journal.pone.0020843.
Fobi G., Gardon J., Santiago M., Ngangue D., Gardon‐Wendel N. and Boussinesq M. (2000). Ocular findings after
ivermectin treatment of patients with high Loa loa microfilaraemia. Ophthalmic Epidemiol 7: 27‐39.
Fokom Domgue J. (2006). Effets secondaires graves survenant après le traitement de massede l'onchocercose par
l'ivermectine: profil cytokinique et influence de l'infection à Plasmodium. Medical Thesis, University of
Yaounde I.
Gallin M.Y., Jacobi A.B., Büttner D.W., Schonberger O., Marti T. and Erttmann K.D. (1995). Human autoantibody to
defensin: disease association with hyperreactive onchocerciasis (sowda). J. Exp. Med. 182: 41–47.
Gardon J., Boussinesq M., Kamgno J., Gardon‐Wendel N., Demanga N. and Duke B.O. (2002). Effects ofstandard
and high doses of ivermectin on adult worms of Onchocerca volvulus: a randomised controlled trial.
Lancet 360(9328): 203‐210.
Gardon J., Gardon‐Wendel N., Demanga N., Kamgno J., Chippaux J. P. and Boussinesq M. (1997). Serious reactions
after mass treatment of onchocerciasis with ivermectin in an area endemic for Loa loa infection. Lancet
350(9070): 18‐22.
57
Recent advances in onchocerciasis research and implications for control
Garms R., Lakwo T.L., Ndyomugyenyi R., Kipp W., Rubaale T., Tukesiga E., Katamanywa J., Post R.J. and Amazigo
U.V. (2009). The elimination of the vector Simulium neavei from the Itwara onchocerciasis focus in
Uganda by ground larviciding. Acta Tropica 111: 203‐210.
Garnham P.C.C. and McMahon J.P. (1954). The Eradication of Simulium neavei Roubaud from an onchocerciasis
area in Kenya colony. Bull. Entom. Res., 37: 619‐628.
Garnham P.C.C. and McMahon J.P. (1981). Eradication of black fly Simulium neavei Roubaud from an
Onchocerciasis from Kenya. Mosq. News. 41. 619‐628.
Gilbert J., Nfon C.K., Makepeace B.L., Njongmeta L.M., Hastings I.M., Pfarr K.M., Renz A., Tanya V.N. and Alexander
J. Trees (2005). Antibiotic chemotherapy of onchocerciasis: in a bovine model, killing of adult parasites
requires a sustained depletion of endosymbiotic bacteria (Wolbachia). Journal of Infectious Diseases 192:
1483‐1493.
Graham S.P., Wu Y., Henkle‐Duehrsen K., Lustigman S., Unnasch T.R., Braun G., Williams S.A., McCarthy J., Trees
A.J. and Bianco A.E. (1999). Patterns of Onchocerca volvulus recombinant antigen recognition in a bovine
model of onchocerciasis. Parasitology 119: 603–612.
Greene B.M., Gbakima A.A., Albiez E.J. and Taylor H.R. (1985a). Humoral and cellular Immune responses to
Onchocerca volvulus infection in humans. Rev Infect Dis.7: 789‐795.
Greene B.M., Taylor H.R., Cupp E.W., Murphy R.P., White A.T., Aziz M.A., Schulz‐Key H., D'AnnaS.A., Newland H. S.,
Goldschmidt L.P. et al. (1985b). Comparison of ivermectin and diethylcarbamazine in the treatment of
onchocerciasis. N. Engl. J. Med.313: 133‐138.
Gustavsen K., Hopkins A. and Sauerbrey M. (2011). Onchocerciasis in the Americas: from arrival to (near)
elimination. Parasites and Vectors 4:205 doi: 10.1186/1756‐3305‐4‐205
Guzzo C.A., Furtek C.I., Porras A.G., Chen C., Tipping R., Clineschmidt C.M., SciberrasD.G., HsiehJ.Y. and Lasseter
K.C. (2002). Safety, tolerability, and pharmacokinetics of escalating high doses of ivermectin in healthy
adult subjects. J. Clin. Pharmacol.42: 1122‐1133.
Gyapong M., Gyapong J.O. and Owusu‐Banahene G. (2000). Community‐directed treatment: the way forward to
eliminating lymphatic filariasis as a public‐health problem in Ghana. Anna.Trop. Med. Parasitol.95: 77‐ 86.
Hagan M. (1998). Onchocercal dermatitis: clinical impact. Ann. Trop. Med. Parasitol.92 (Suppl 1): S85 ‐ S96.
Hansen R. D. E., Trees A.J., Bah G.S., Hetzell U., Martin C., Bain O., Tanya V. N. and Makepeace1 B.L. (2010). A
worm’s best friend: recruitment of neutrophils by Wolbachia confounds eosinophil degranulation against
the filarial nematode Onchocerca ochengi. Proc. R. Soc. Bdoi: 10.1098/rspb.2010.2367.
Henkle‐Dührsen K., Eckelt V.H.O., Wildenburg G., Blaxter M. and Walter R.D. (1998). Gene structure, activity, and
localisation of catalase from intracellular bacteria in Onchocerca volvulus. Mol. Biochem. Parasitol. 96: 69‐
81.
Henry M.C. and Meredith S.E.O. (1990). The Onchocerciasis focus at Kinsuka/Kinshasa (Republic of Zaire) in 1985. I.
Entomological aspect. Ann. Trop. Med. Parasitol. 84. (4) 369‐379.
58
Recent advances in onchocerciasis research and implications for control
Hervouet J.P. and Prost A. (1979). Organisation de l’espace et epidemiologie de l’onchocercose. In: Maitrise de
l’espace agraire et developpement en Afrique tropicale. Memoires ORSTOM, number 89. Paris: ORSTOM.
pp. 179–190.
Hise A.G., Gillette‐Ferguson I. and Pearlman E. (2004).The role of endosymbiotic Wolbachia bacteria in filarial
disease.Cellular Microbiology 6: 97–104.
Hitchen C.S. and Going H.H. (1966). Note on the control of Simulium damnosum in the region of the Kainji Dam
Project, Northern Nigeria. World Health Org. mimeographed document AFR/Oncho/8 Rev. 1
WHO/ONCHO/66.43 5 pp.
Hodgkin C., Molyneux D.H., Abiose A., Philippon B., Reich M.R., Remmes J.H., Thylefors B., Traore M. and Grepin K.
(2007). The future of onchocerciasis control in Africa. PLoS Negl Trop Dis 1(1): e74.
doi:10.1371/journal.pntd.0000074
Hoerauf A., Mand S., Adjei O., Fleischer B.and Buttner D.W. (2001). Depletion of Wolbachia endobacteria in
Onchocerca volvulus by doxycycline and microfilaridermia after ivermectin treatment. Lancet 357: 1415‐
1416.
Hoerauf A., Mand S., Fischer K., Kruppa T., Marfo‐Debrekyei Y., Debrah A.Y., Pfarr K.M., Adjei O. and Buttner D.W.
(2003a). Doxycycline as a novel strategy against bancroftian filariasis‐depletion of Wolbachia
endosymbionts from Wuchereria bancrofti and stop of microfilaria production. Med. Microbiol. Immunol.
192: 211‐216.
Hoerauf A., Mand S., Volkmann L., Buttner M., Marfo‐Debrekyei Y., Taylor M., Adjei O. and Buttner D.W. (2003b).
Doxycycline in the treatment of human onchocerciasis: Kinetics of Wolbachia endobacteria reduction and
of inhibition of embryogenesis in female Onchocerca worms. Microbes Infect5: 261‐273.
Hoerauf A., Nissen‐Pahle K., Schmetz C., Henkle‐Duhrsen K., Blaxter M.L., Buttner D.W., Gallin M.Y., Al‐Qaoud K.M.,
Lucius R. and Fleischer B. (1999). Tetracycline therapy targets intracellular bacteria in the filarial
nematode Litomosoides sigmodontis and results in filarial infertility. J. Clin. Invest. 103:11–18.
Hoerauf A., Specht S., Marfo‐Debrekyei Y., Büttner M., Debrah A.Y., Mand S., Batsa L., Brattig N., Konadu P., Bandi
C., Fimmers R., Adjei O. and Büttner D.W. (2009). Efficacy of 5‐week doxycycline treatment on adult
Onchocerca volvulus. Parasitol. Res. 104: 437 – 447.
Hoerauf A., Volkmann L., Hamelmann C., Adjei O., Autenrieth I.B., Fleischer B. and Buttner D.W. (2000a).
Endosymbiotic bacteria in worms as targets for a novel chemotherapy in filariasis. Lancet 355: 1242‐1243.
Hoerauf A., Volkmann L., Nissen‐Pàehle K., Schmetz C., Autenrieth I., Büttner D.W. and Fleischer B. (2000b).
Targetting of Wolbachia endobacteria in Litomosoides sigmodontis: comparison of tetracyclines with
chloramphenicol, macrolides and ciprofloxin. Trop. Med. Int. Health 5: 275‐279.
Homeida M., Braide E., Elhassan E., Amazigo U.V., Liese B., Benton B., Noma M., Etya'ale D., Dadzie K.Y., Kale
O.O.and Seketeli A. (2002). APOC's strategy of community‐directed treatment with ivermectin (CDTI) and
its potential for providing additional health services to the poorest populations. African Programme for
Onchocerciasis Control. Ann. Trop. Med. Parasitol. 96 Suppl 1: S93‐104.
Hotez P.J. and Kamath A. (2009). Neglected tropical diseases in Sub‐saharan Africa: Review of their prevalence,
distribution and disease burden. PLoS Neglected Trop. Dis. 3(8), e412.doi:101371/journal.pntd.0000412.
59
Recent advances in onchocerciasis research and implications for control
Hougard J.M., Escaffre H., Darnet F., Lochouarn L., Riviere F. et al. (1992). An episode of resistance to permethrin in
larvae of Simulium squamosum (Diptera: Simuliidae) from Cameroon, after 3.5 years of control. J. Am.
Mosq. Control Assoc. 8 (2): 184‐186.
Hussein S., Bird A. and Jones B. (1987). Ocular lesion seen in phase III trial of ivermectin therapy of onchocerciasis
in Togo. Trop. Med. Parasitol. 38: 67.
Kamgno J. (2005). Etude sur l'impact de l'onchocercose, l'effet macrifilaricide de l'ivermectine et les difficultés liées
à la co‐endémie avec la loase. Thèse PhD Université Pierre et Marie Curie, France.
Kamgno J., Bouchite B., Baldet T., Folefack G., Godin C. and Boussinesq M. (1997). Study of the distribution of
human filariasis in West Province of Cameroon. Bull. Soc. Pathol. Exot. 90: 327‐330.
Kamgno J.and Boussinesq M. (2001). Hyperendemic loaiasis in the Tikar plain, shrub savanna region of Cameroon.
Bull. Soc. Pathol. Exot. 94: 342‐346.
Kamgno J., Boussinesq M., Labrousse F., Nkegoum B., Thylefors B. I. and Mackenzie C. D. (2008). Encephalopathy
after ivermectin treatment in a patient infected with Loa loa and Plasmodium spp. Am. J. Trop. Med.
Hyg.78: 546‐551.
Kamgno J., Gardon J., Enyong P. and Bouchite B. (1998). L'onchocercose dans la région de Mamfé‐Kumba, Province
du Sud‐Ouest Cameroun. Bull. Liais Doc. OCEAC 31: 33‐38.
Kamgno J., Pion S.D. and Boussinesq M. (2003). Demographic impact of epilepsy in Africa: results of a 10‐year
cohort study in a rural area of Cameroon. Epilepsia 44: 956‐963.
Kamgno J., Pion S.D., Mackenzie C.D., Thylefors B. and Boussinesq M. (2009). Loa loa microfilarial periodicity in
ivermectin‐treated patients: comparison between those developing and those free of serious adverse
events. Am. J. Trop. Med. Hyg.81: 1056‐1061.
Kamgno J., Sodahlon Y.K., Ogoussan K., Nyuyfomo Tukov D., Ntep M., Klion A., Boussinesq M., Mackenzie C.D. and
Hopkins A. (2011). Incidence and geographical distribution of serious adverse events following mass
administration of ivermectin in Cameroon from 1999 to 2009. Am. J. Trop. Med. Hyg.85: 150.
Kamgno J., Tenaguem J., Kamtchuen J., Wawo Y., Kagmeni G., Fotsing R., Nana Djeunga H., Boussinesq M., Klion A.
and Hopkins A. (2010). Evaluation of loiasis impact on the eye and the heart in Akonolinga Health Distric
in Cameroon. Mectizan Experts Commitee Meeting.
Katabarwa M.N., Eyamba A., Nwane P., Enyong P., Yaya S., Baldiagaï J., Madi T.K. , Yougouda A., Andze G.O. and
Richards F.O. (2011). Seventeen years of annual distribution of Ivermectin has not interrupted
Onchocerciasis transmission in North Region, Cameroon. Am. J. Trop. Med. Hyg., 85: 1041–1049.
Kläger S., Whitworth J.A.G., Post R.J., Chavasse D.C. and Downham M.D. (1993). How long do the effects of
ivermectine on adult Onchocerca volvulus persist? Tropical Medicine and Parasitology44: 305 – 310.
Keisler D.H., Bettencourt C.M. and Moffatt R.J. (1993).Effects of ivermectin on reproductive functions in ewes. J.
Anim. Sci.71: 2293‐2296.
Keiser P.B., Reynolds S.M., Awadzi K., Ottesen E.A., Taylor M.J. and Nutman T.B. (2002). Bacterial endosymbionts of
Onchocerca volvulus in the pathogenesis of post treatment reactions. J. Infect. Dis.185: 805‐811.
60
Recent advances in onchocerciasis research and implications for control
Khalid A.E., Elfatih M.M., Tarig A., Salah H.A., Abdalla H.E., Mahmoud A.M., Asma H.E and Ishag A. (2009).
Feasibility and acceptability of home‐based management of malaria strategy adapted to Sudan’s condition
using artemisin‐based combination therapy and rapid diagnostic test. Malaria Journal. Available from:
URL.http://www.malariajournal.com/cntent/8/1/39.
Kipp W., Bamhuhiiga J., Rubaale T. and Buttner D.W. (2003). Adverse reactions to ivermectin treatment in
Simulium neavei‐transmitted onchocerciasis. Am. J. Trop. Med. Hyg.69: 621‐623.
Knab J., Darge K. and Buttner D.W. (1997). Immunohistological studies on macrophages in lymph nodes of
onchocerciasis patients after treatment with ivermectin. Trop. Med. Int. Health 2: 1156‐1169.
Kozek W.J. and Marroquin H.F. (1977). Intracytoplasmic bacteria in Onchocerca volvulus. Am. J. Trop. Med. Hyg. 26:
663 – 678.
Kramer L.H., Passeri B., Corona S., Simoncini L. and Casiraghi M. (2003). Immunohistochemical/immunogold
detection and distribution of the endosymbiont Wolbachia of Dirofilaria immitis and Brugia pahangi using
a polyclonal antiserum raised against WSP (Wolbachia surface protein). Parasitol. Res. 89: 381‐386.
Lagraulet J. (1971). Epidemiology of ocular onchocerciasis in French‐speaking countries of West Africa. Israel J.
Med. Sci. 8: 1153–1155.
Langworthy N.G., Renz A., Meckenstedt U., Henkle‐Duhrsen K., Bronsvoort M., Tanya V.N., Donnelly M.J. and Trees
A.J. (2000). Macrofilaricidal activity of tetracycline against the filarial nematode, Ochocerca ochengi:
elimination of Wolbachia precedes worm death and suggests a dependent relationship. Proc. R. Soc.
London B 267: 1063‐1069.
Lariviere M., Beauvais B., Aziz M., Garin J.F., Abeloos J., Derouin F., Bamba M., Bossebceuf C., Ferly‐Therizol M.,
Sarfati C. et al. (1989a). A study in the Ivory Coast (1985‐1987) of the efficacy and tolerance of ivermectin
(Mectizan) in human onchocerciasis. I. A comparative double‐blind study of 220 patients with 19
onchocerciasis treated with a single oral dose of 100, 150 or 200 mcg/kg]. Bull. Soc. Pathol. Exot. Filiales
82: 35‐47.
Lariviere M., Beauvais B., Aziz M., Garin J.F., Abeloos J., Derouin F., Bamba M., Ferly‐Therizol M., Sarfati C., Basset
D. et al. (1989b). A study in the Ivory Coast (1985‐1987) of the efficacy and tolerance of ivermectin
(Mectizan) in human onchocerciasis. II. Evaluation in the light of mass campaigns on the effect of yearly or
half‐yearly administration of single oral doses of 100, 150 or 200 mcg/kg. Bull. Soc. Pathol. Exot. Filiales
82: 48‐57.
Lariviere M., Beauvais B., Aziz M., Garin J.F., Peignot C., Abeloos J., Kouakou P., Ferly‐Therizol M., Derouin F.,
Sarfati C. et al. (1989c). A study in the Ivory Coast (1985‐1987) of the efficacy and tolerance of ivermectin
(Mectizan) in human onchocerciasis. III. The tolerance and efficacy of a single oral dose of 150 mcg/kg in
children. Bull. Soc. Pathol. Exot. Filiales 82: 58‐64.
Lariviere M., Vingtain P., Aziz M., Beauvais B., Weimann D., Derouin F., Ginoux J., Schulz‐Key H., Gaxotte P., Basset
D. and Sarfati C. (1985). Double‐blind study of ivermectin and diethylcarbamazine in African
onchocerciasis patients with ocular involvement. Lancet 2(8448): 174‐177.
Le Goff L., Martin C., Oswald I.P., Vuong P.N., Petit G., Ungeheuer M.N. and Bain O. (2000). Parasitology and
immunology of mice vaccinated with irradiated Litomosoides sigmodontis larvae. Parasitology 120: 271‐
280.
61
Recent advances in onchocerciasis research and implications for control
Leveque C. (1989). The use of insecticides in the Onchocerciasis Control Programme and aquatic monitoring in
West Africa. In: Bourdeau P., Haines J.A., Klein W. and Krishna Murti C.R. (eds). Ecotoxicology and Climate.
Published by John Wiley & Sons Ltd. London, Pp317‐335.
Little M.P., Basanez M.G., Breitling L.P., Boatin B.A. and Alley E.S. (2004). Incidence of blindness during the
Onchocerciasis Control Programme in West Africa, 1971‐2002. J. Infect. Dis.189: 1932‐1941.
Lucius R., Büttner D.W., Kirsten C. and Diesfeld H.J. (1986). A study on antigen recognition by onchocerciasis
patients with different clinical forms of disease. Parasitology 92: 569–580.
Lucius R., Textor G., Kern A. and Kirsten C. (1991). Acanthocheilonema viteae: vaccination of jirds with irradiation‐
attenuated stage‐3 larvae and with exported larval antigen. Exp. Parasitol.73: 184–196.
Lustigman S. and McCarter J.P. (2007). Ivermectin Resistance in Onchocerca volvulus: toward a genetic basis. PLoS
Negl. Trop. Dis. 1(1): e76. doi:10.1371/journal. pntd.0076.
Macé J.M., Boussinesq M., Ngoumou P., Enyegue Oye J., Koéranga A. and Godin C. (1997). Country‐wide rapid
epidemiological mapping of onchocerciasis (REMO) in Cameroon Annals of Tropical Medicine and
Parasitology 91: 379‐391.
Mackenzie C.D., Williams J.F., Sisley B.M., Steward M.W. and O’Day J. (1985). Variations in host responses and the
pathogenesis of human onchocerciasis. Rev. Infect. Dis. 7: 802–808.
Maizels R.M. and Yazdanbakhsh M. (2003). Regulation of the immune response by helminth parasites: cellular and
molecular mechanisms. Nat Rev Immunol 3:733–743.
Maizels R.M.,BundyD.A.P., Selkirk M.E., Smith D.F. and Anderson R.M. (1993). Immunological modulation and
evasion by helminth parasites in human populations. Nature 365: 797‐804.
Makepeace B.L., Siv Aina Jensen S.A., Sandra J. Laney S.J., Nfon C.K., Njongmeta L.M., Tanya V.N., Williams S.A.,
Bianco A.E., Alexander J. Trees A.J. (2009). Immunisation with a multivalent, subunit vaccine reduces
patent infection in a natural bovine model of onchocerciasis during intense field exposure. PLoS Neglected
Tropical Diseases 3(11): e544 doi:10.1371/journal.pntd.0000544.t001.
Mas J., Ascaso C., Escaramis G., Abellana R., Duran E., Sima A., Sanchez M.J., Nkogo P.R., Nguema R., Untoria M.D.,
Echeverria M.A., Ardevol M.M. and de Jimenez Anta M.T. (2006). Reduction in the prevalence and
intensity of infection in Onchocerca volvulus microfilariae according to ethnicity and community after 8
years of ivermectin treatment on the island of Bioko, Equatorial Guinea. Trop. Med. Int. Health 11: 1082‐
1091.
McCall J.W., Jun J.J. and Bandi C. (1999). Wolbachia and the antifilarial properties of tetracycline. An untold story.
Ital. J. Zool. 66: 7–10.
McGarry H.F., Pfarr K., Egerton G., Hoerauf A., Akue J.P., Enyong P., Wanji S., Kläger S.L., Bianco A.E., Beeching N.J.
and Taylor M.J. (2003). Evidence against Wolbachia symbiosis in Loa loa. Filaria J. 2: 9. doi:10.1186/1475‐
2883‐2‐9
McMahonJ.P. (1967). A review of the control of Simulium vectors of onchocerciasis. Bull. Wld Hlth Org. 37: 415‐
430.
62
Recent advances in onchocerciasis research and implications for control
McMahon J.P., Highton R.B. and Goiny H. (1958). The eradication of Simulium neavei from Kenya. Bull.Wld Hlth
Org. 19:75‐107.
MEC/TCC (2004). Guidelines: Recommendations for the treatment of Onchocerciasis with Mectizan® in areas co‐
endemic for Onchocerciasis and Loiasis. http://www.mectizan.org/ loarecs.asp.
Miller T.W., Chaiet L., Cole D.J., Flor J.E., Goegelman R.T., Joshua H., Kempf A.J., Krellwitz W.R., Monaghan R.L.,
Ormond R.E., Wilson K.E., Albert‐Schonberg G. and Putter I. (1979). Avermectin, a new family of potent
anthelminthic agents: isolation and chromatographic properties. Antimicrob. Agents Chemother. 15: 368‐
371.
Molyneux D.H. (2005). Onchocerciasis control and elimination: coming of age in resource‐constrained health
systems. Trends in Parasitol. 21: 525–529.
Molyneux D.H. and Davies J.B. (1997). Onchocerciasis control: moving towards the millennium. Parasitol. Today 13:
418‐425.
Murdoch M.E., Hay R.J., Mackenzie C.D., Williams J.F., Ghalib H.W., Cousens S., Abiose A. and Jones B.R. (1993). A
clinical classification and grading system of the cutaneous changes in onchocerciasis. Br. J. Dermatol. 129:
260‐269.
Murdoch M.E., Payton A., Abiose A., Thomson W., Panicker V.K., Dyer P.A., Jones B.R, Maizels R.M. and Ollier W.E.
(1997). HLA‐DQ alleles associate with cutaneous features of onchocerciasis. The Kaduna‐London‐
Manchester Collaboration for Research on Onchocerciasis. Hum. Immunol. 55: 46–52.
Mustafa K.Y., Turunen U. andGumaa K.A. (1979). Serum vitamin A levels of patients with onchocerciasis from two
areas of the Sudan. J. Trop. Med. Hyg. 82: 122–127.
Newland H.S. White A.T., Greene B.M., Murphy R.P. and Taylor H.R. (1991). Ocular manifestations of
onchocerciasis in a rain forest area of West Africa. Br. J. Ophthalmol. 75:163 ‐ 169.
Newland H.S., White A.T., Greene B.M., D'Anna S.A., Keyvan‐Larijani E., Aziz M.A., Williams P.N. and Taylor H.R.
(1988). Effect of single‐dose ivermectin therapy on human Onchocerca volvulus infection with onchocercal
ocular involvement. Br. J. Ophthalmol.72: 561‐569.
Nfon C. K., Makepeace B., Njongmeta L., Tanya V. N., Bain O. and Trees A. (2006). Eosinophils contribute to killing
of adult Onchocerca ochengi within onchocercomata following elimination of Wolbachia. Microbes and
Infection 8: 2698‐2705.
Ngoumou P., Walsh J.F.and Mace J.M. (1994). A rapid mapping technique for the prevalence and distribution of
onchocerciasis: a Cameroon case study. Ann Trop Med Parasitol. 88: 463‐474.
Njoo F.L., Belling G.A., Oosting J., Vetter J.C., Stilma J.S. and Kijlstra A. (1993). Concurrent parasitic infections in
onchocerciasis and the occurrence of adverse reactions after ivermectin treatment. Am. J. Trop. Med.
Hyg.48: 652‐657.
Noma M., Nwoke B.E.B., Nutall I., Tambala P.A., Enyong P., Namsenmo A., Remme J., Amazigo U.V., Kale O.O. and
Seketeli A. (2002). Rapid epidemiological mapping of onchocerciasis (REMO): its application by the African
Programme for Onchocerciasis Control (APOC). Annals of Tropical Medicine and Parasitology 96 (S1): S29‐
S39.
63
Recent advances in onchocerciasis research and implications for control
Norgbey S.W. (1997). Control of onchocerciasis (river blindness) in West Africa: ecology, risk and resettlement.
Journal of Environment and Development. www.accessmylibrary.com/article‐1G1‐20629607.
Oladepo O., Brieger W.R., Otusanya S., Kale O.O., Offiong S. and Titiloye M. (1997). Farm land size and
onchocerciasis status of peasant farmers in south‐western Nigeria. Trop. Med. Int. Health 2: 334–340.
Omura S. and Crump A. (2004). The life and times of ivermectin ‐ a success story. Nat. Rev. Microbiol. 2: 984‐989.
Osei‐Atweneboana M.Y., Awadzi K., Attah S.K., Boakye D.A., Gyapong J.O. and Prichard R.K. (2011). Phenotypic
evidence of emerging ivermectin resistance in Onchocerca volvulus. PLoS Negl. Trop. Dis.5(3): e998.
Osei‐Atweneboana M.Y., Eng J.K., Boakye, D.A., Gyapong J.O. and Prichard R.K. (2007). Prevalence and intensity of
Onchocerca volvulus infection and efficacy of ivermectin in endemic communities in Ghana: a two‐phase
epidemiological study. Lancet 369: 2021‐2029.
Ottesen E.A. (1984). Immunological aspects of lymphatic filariasis and onchocerciasis in man. Trans R. Soc. Trop.
Med. Hyg.78: 9 ‐18.
Ottesen E.A. (1995). Immune responsiveness and the pathogenesis of human onchocerciasis. J. Infect. Dis. 171:
659–671.
Pacque M., Munoz B., Poetschke G., Foose J., Greene B.M. and Taylor H.R. (1990). Pregnancy outcome after
inadvertent ivermectin treatment during community‐based distribution. Lancet 336 (8729): 1486‐1489.
Philippon B. (1977). Etude de la transmission d'Onchocerca volvulus (Leuckart, 1983) Nematoda, Onchocercidae)
par Simulium damnosum (Theobald, 1903) (Diptera, Simuliidae) en Afrique tropicale. Travaux et
Documents ORSTOM, No. 63.
Pion S.D., Grout L., Kamgno J., Nana‐Djeunga H. and Boussinesq M. (2011). Individual host factors associated with
Onchocerca volvulus microfilarial densities 15, 80 and 180 days after a first dose of ivermectin. Acta Trop.
120 Suppl 1: S91‐99.
Pion S.D., Kamgno J., Demanga N. and Boussinesq M. (2002). Excess mortality associated with blindness in the
onchocerciasis focus of the Mbam Valley, Cameroon. Ann. Trop. Med. Parasitol. 96: 181–189.
Plaisier A. P., van Oortmarssen G.J., Remme J. and Habbema J.D. (1991). The reproductive life span of Onchocerca
volvulus in West African savanna. Acta Trop 48: 271‐284.
Plaisier A.P., Van Oortmarssen G.J., Habbena J.D.P., Remme J. and Alley E.S. (1990). ONCHOSIM: a model and
computer simulation program for the transmission and control of onchocerciasis. Comp. meth. Programs
in Biomed. 31: 43 ‐56.
Poul J.M. (1988). Effects of perinatal ivermectin exposure on behavioral development of rats. Neurotoxicol.
Teratol.10: 267‐272.
Prost A. (1986). The burden of blindness in adult male in the savanna villages of West Africa exposed to
onchocerciasis. Trans R. Soc. Trop. Med. Hyg. 80: 525–527.
Rao R., Moussa H. and Weil G.J. (2002). Brugia malayi: Effects of antibacterial agents on larval viability and
development invitro. Exp. Parasitol. 101: 77‐81.
Remme J.H. (2004). Research for control: the onchocerciasis experience. Trop. Med. Int. Health 9: 243–254.
64
Recent advances in onchocerciasis research and implications for control
Remme J., Baker R.H., De Sole G., Dadzie K.Y., Walsh J.F., Adams M.A., Alley E.S. and Avissey H.S.(1989). A
community trial of ivermectin in the onchocerciasis focus of Asubende, Ghana. I. Effect on the microfilarial
reservoir and the transmission of Onchocerca volvulus. Trop. Med. Parasitol. 40: 367‐374.
Renz A., Trees A.J., Achukwi D., Edwards G. and Wahl G. (1995). Evaluation of suramin, ivermectin and CGP20376
in a new macrofilaricidal drug screen, Onchocerca ochengi in African cattle. Tropical Medicine and
Parasitology 46: 31‐37.
Robles R. (1919). Onchocercose humaine au Guatemala produisant la cécité et "l'érysipèle du littoral " (erisipela de
la costa). Bull. Soc. Pathol. Exot. 12: 442‐463.
Seketeli A., Adeoye G., Eyamba A., Nnoruka E., Drameh P., Amazigo U.V., Noma M., Agboton F., Aholou Y., Kale
O.O. and Dadzie K.Y. (2002). The achievements and challenges of the African Programme for
Onchocerciasis Control (APOC). Ann. Trop. Med. Parasitol. 96 (Suppl 1): S15–S28.
Smith H.L. and Rajan T.V. (2000). Tetracycline inhibits development of the infective‐stage larvae of filarial
nematodes in vitro. Exp. Parasitol. 95: 265–270.
Somo R.M., Enyong P.A., Fobi G., Dinga J.S., Lafleur C., Agnamey P., Ngosso A. and Ngolle E.M. (1993a). A study of
onchocerciasis with severe skin and eye lesions in a hyperendemic zone in the forest of southwestern
Cameroon: clinical, parasitologic, and entomologic findings. Am. J. Trop. Med. Hyg. 48: 14‐19.
Somo R.M., Ngosso A., Dinga J.S., Enyong P.A.and Fobi G. (1993b). A community‐based trial of ivermectin for
onchocerciasis control in the forest of southwestern Cameroon: clinical and parasitologic findings after
three treatments. Am. J. Trop. Med. Hyg. 48: 9‐13.
Specht S., Mand S., Marfo‐Debrekyei Y., Debrah A.Y., Konadu P., Adjei O., Büttner D.W. and Hoerauf A. (2008).
Efficacy of 2‐ and 4‐week rifampicin treatment on the Wolbachia of Onchocerca volvulus. Parasitol Res.
103: 1303‐1309.
Stouthamer R., Breeuwer J.A. and Hurst, G.D. (1999). Wolbachia pipientis: microbial manipulator of arthropod
reproduction. Annu. Rev. Microbiol.53:71–102.
Stürchler D., Tanner M., Hanck A., Betschart B., Gautschi K., Weiss N., Burnier E., Del Giudice G. and Degrémont A.
(1987). A longitudinal study on relations of retinol and parasitic infections and the immune response of
children in Kikwawila village, Tanzania. Acta Trop. 44, 213–217.
Tamarozzi F., Halliday A., Gentil K., Hoerauf A., Pearlman E., Taylor M.J. (2011). Onchocerciasis: the role of
Wolbachia bacterial endosymbionts in parasite biology, disease pathogenesis, and treatment. Clin.
Microbiol. Rev. 24: 459‐468.
Takougang I., Meremikwu M., Wandji S., Yenshu E.V., Aripko B., Lamlenn S.B., Eka B.L., Enyong P., Meli J., Kale O.
and Remme J.H. (2002). Rapid assessment method for prevalence and intensity of Loa loa infection. Bull.
World Health Organ. 80: 852‐858.
Taylor M.J., Bandi C. and Hoerauf A. (2005). Wolbachia bacterial endosymbionts of filarial nematodes. Adv.
Parasitol. 60: 245–284.
Taylor M. J., Bilo K., Cross H.F., Archer J.P. and A. P. Underwood A.P. (1999). 16S rDNA phylogeny and
ultrastructural characterization of Wolbachia intracellular bacteria of the filarial nematodes Brugia malayi,
B. pahangi and Wuchereria bancrofti. Exp. Parasitol. 91: 356–361.
65
Recent advances in onchocerciasis research and implications for control
Taylor H.R. and Greene B.M. (1989). The status of ivermectin in the treatment of human onchocerciasis. Am. J.
Trop. Med. Hyg. 41: 460‐466.
Taylor M. J. and Hoerauf A. (1999). Wolbachia bacteria of filarial nematodes. Parasitology Today 15: 437‐442.
Taylor M.J., Hoerauf A. and Bockarie M. (2010). Lymphatic filariasis and onchocerciasis. Lancet 376: 1175–1185.
Taylor H.R., Murphy R.P., Newland H.S., White A.T., D'Anna S.A., Keyvan‐Larijani E., Aziz M.A.,Cupp E.W. and
Greene B.M. (1986). Treatment of onchocerciasis: the ocular effects of ivermectin and
diethylcarbamazine. Arch. Ophthalmol. 104: 863‐870.
Tchakouté V.L., Bronsvoort M., Tanya V., Renz A and Trees A.J. (1999). Chemoprophylaxis of Onchocerca
infections: in a controlled, prospective study ivermectin prevents calves becoming infected with O.
ochengi. Parasitology 118: 195‐199.
Tchakouté V.L., Graham S.P., Jensen S.A., Makepeace B.L., Nfon C.K., Njongmeta L.M., Lustigman S., Enyong P.A.,
Tanya V.N., Bianco A.E. and Trees A.J. (2006). In a bovine model of Onchocerciasis, protective immunity
exists naturally, is absent in drug‐cured hosts and is induced by vaccination. PNAS 103: 5971‐5976.
Townson S., Siemienska J., Hollick L. and Hutton D. (1999). The activity of rifampicin, oxytetracycline and
chloramphenicol against Onchocerca lienalis and O. gutturosa. Trans. R. Soc. Trop. Med. Hyg. 93: 123–124.
Townson S., Hutton D., Siemienska J., Hollick L., Scanlon T., Tagboto S.K. and Taylor M.J. (2000). Antibiotics and
Wolbachia in filarial nematodes: antifilarial activity of rifampicin, oxytetracycline and chloramphenicol
against Onchocerca gutturosa, Onchocerca lienalis and Brugia pahangi. Ann. Trop. Med. Parasitol. 94:
801–816.
Townson S., Tagboto S., McGarry H.F., Egerton G.L. and Taylor M.J. (2006). Onchocerca parasites and Wolbachia
endosymbionts: evaluation of a spectrum of antibiotics types for activity gainst Onchocerca gutturosa in
vitro. Filaria J. 5:4.
Traore M.O., Sarr M.D., Badji A., Bissan Y., Diawara L., Doumbia K., Goita S.F., Konate L., Mounkoro K., Seck A.F,
Toe L., Toure S., Remme J.H.F. (2012). Proof‐of‐principle of onchocerciasis elimination with ivermectin
treatment in endemic foci in Africa: final results of a study in Mali and Senegal. PLoS Negl Trop Dis 6(9):
e1825. doi:10.1371/journal.pntd.0001825.
Traore S., Wilson M.D., Sima A., Barro T., Ake A., Coulibaly S., Cheke R.A., Meyer R.R.F., Mas J., McCall P.J., Post
R.J., Zoure H., Noma M., Yameogo L., Seketeki A.V., and Amazigo U.V. (2009). The elimination of the
Onchocerciasis vector from the island of Bioko as a result of larviciding by the WHO African Programme
for Onchocerciasis Control. Acta Tropica 111: 211‐218.
Trees A.J., Graham S.P., Renz A., Bianco A.E. and Tanya V. (2000). Onchocerca ochengi infections in cattle as a
model for human onchocerciasis: recent developments. Parasitology. 120: S133‐S142.
Trees A.J., Wood V.L., Bronsvoort M., Renz A. and Tanya V.N. (1998). Animal models‐Onchocerca ochengi and the
development of chemotherapeutic and chemoprophylactic agents for onchocerciasis. Annals of Tropical
Medicine and Parasitology 92 (1): s175‐s179.
Turner J.D., Langley R.S., Johnston K.L., Gentil K., Ford L., Wu B., Graham M., Sharpley F., Slatko B., Pearlman E. and
Taylor M.J. (2009). Wolbachia lipoprotein stimulates innate and adaptive immunity through toll‐like
receptors 2 and 6 to induce disease manifestations of filariasis. J. Biol. Chem. 284: 22364–22378.
66
Recent advances in onchocerciasis research and implications for control
Turner M.J. and Schaeffer J. M. (1989). Mode of action of ivermectin. In: Campbell W.C. (ed). Ivermectin and
Abermectin,pp73‐88, Springer‐Verlag, New York.
Twum‐Danso N.A. (2003a). Loa loa encephalopathy temporally related to ivermectin administration reported from
onchocerciasis mass treatment programs from 1989 to 2001: implications for the future. Filaria J.2 Suppl.
1: S7.
Twum‐Danso N.A. (2003b). Serious adverse events following treatment with ivermectin for onchocerciasis control:
a review of reported cases. Filaria J 2 Suppl 1: S3.
Vingtain P., Pichard E., Ginoux J., Coulibaly S.M., Bissan Y., Ranque P. and Thillaye B. (1988). Ivermectin and human
onchocerciasis: a study of 234 onchocerciasis patients in the Republic of Mali. Bull. Soc. Pathol. Exot.
Filiales 81: 260‐270.
Vlassoff C., Weiss M., Ovuga E.B., Eneanya C., Newel P.T., Babalola S.S., Awedoba A.K., Theophilus B., Cofie P. and
Shetabi P. (2000). Gender and the stigma of onchocercal skin disease in Africa. Soc. Sci. Med. 50: 1353–
1368.
Volkmann L., Fischer K., Taylor M. and Hoerauf A. (2003). Antibiotic therapy in murine filariasis (Litomosoides
carinii) : Comparative effects of doxycycline and rifampicin on Wolbachia and filarial viability. Trop. Med.
Int. Health 8: 392‐401.
Vuong P.N., Traore S., Wanji S., Diarrassouba S., Balaton A. and Bain O. (1992). Ivermectin in human
onchocerciasis: a clinical‐pathological study of skin lesions before and three days after treatment. Ann.
Parasitol. Hum. Comp. 67: 194‐196.
Wahl G., Ekale D. and Schmitz A. (1998a). Onchocerca ochengi: assessment of the Simulium vector in North
Cameroon. Parasitology 116: 327‐336.
Wahl G., Enyong P., Ngosso A., Schibel J.M., Moyou R., Tubbesing H., Ekale D. and Renz A. (1998b). Onchocerca
ochengi: epidemiological evidence of cross‐protection against Onchocerca volvulus in man. Parasitology
116: 349–362.
Walsh J.F. (1990). Review of vector control prior to the OCP. Acta Leiden 59: 61‐78
Walsh J.F., Davies J.B. and Le Berre R. (1979). Entomological aspects of the first five years of the Onchocerciasis
Control Programme in the Volta River Basin. Tropenmed Parasitol. 30: 328‐344.
Wanji S., Takougang I., Yenshu E.V., Meremikwu M., Enyong P., Braide E. et al. (2001). Rapid assessment
procedures for loiasis. Report of a Multi‐centre study, UNDP/World Bank/ WHO Special Programme for
Research and Training in Tropical Diseases TDR/IDE/RP/RAPL/01.1. 2001doi:
10.1179/000349804225003253.
Wanji S., Akotshi D.O., Mutro M.N., Tepage F., Ukety T.O., Diggle P.J., Remme J.H. (2012). Validation of the rapid
assessment procedure for loiasis (RAPLOA) in the Democratic Republic of Congo. Parasit and Vectors 5: 25
doi: 10.1186/1756‐3305‐5‐25.
Wanji S., Tendongfor N., Esum M., Yundze S.S., Taylor M.J.and Enyong P. (2005). Combined utilisation of Rapid
Assessment Procedures for Loiasis (RAPLOA) and Onchocerciasis (REA) in Rain forest Villages of
Cameroon. Filaria J.4: 2.
67
Recent advances in onchocerciasis research and implications for control
Wanji S., Tendongfor N., Nji T., Esum M., Che J. N., Nkwescheu A., Alassa F., Kamnang G.,
Enyong P.A., Taylor M.J., Hoerauf A. and Taylor D.W. (2009). Community‐directed delivery of doxycycline for the
treatment of onchocerciasis in areas of co‐endemicity with loiasis in Cameroon. Parasit and Vectors 2:
39doi:10.1186/1756‐3305‐2‐39.
Waters H.R., Rehwinkel J.A. and Burnham G. (2004). Economic evaluation of Mectizan distribution. Trop. Med. Int.
Health 9 (Suppl): A16–A25.
Winnen M., Plaisier A.P., Alley E.S., Nagelkerke N.J.D., Van Oortmarssen G., Boatin B.A. and Habbena J.D.F. (2000).
Can ivermectin mass treatments eliminate onchocerciasis in Africa? Bull. World Health Org. 80: 384 ‐390.
Werren J.H., Zhang W. and Guo L.R. (1995). Evolution and phylogeny of Wolbachia: reproductive parasites of
arthropods. Proc R Soc London B Biol Sci 261:55–63.
White A.T., Newland H.S., Taylor H.R., Erttmann K.D., Keyvan‐Larijani E., Nara A., Aziz M.A., D'Anna S.A., Williams
P.N. and Greene B.M. (1987). Controlled trial and dose‐finding study of ivermectin for treatment of
onchocerciasis. J. Infect. Dis.156: 463‐470.
Whitworth J.A., Morgan D., Maude G.H., Downham M.D. and Taylor D.W. (1991). A community trial of ivermectin
for onchocerciasis in Sierra Leone: clinical and parasitological responses to the initial dose. Trans. R. Soc.
Trop. Med. Hyg. 85: 92‐96.
WHO (1987). Expert committee on Onchocerciasis, third report. World Health Org. Tech. Rep. Ser. 752: 1‐162.
WHO (1989). 25 Years of OCP 1974 – 1999.
WHO (1995a). Onchocerciasis and its control. WHO Tech. Rep. Ser. 852:1 ‐103.
WHO (1995b). Onchocerciasis and its control. Reportof a WHO expert committee on onchocerciasis control. WHO
Technical Report Series, number 852. Geneva: World Health Organization. 110p.
WHO (1996). Community‐directed treatment with ivermectin: report of a multi‐country study. Special Programme
for Research andTraining in Tropical Diseases. WHO Geneva.
WHO (2005). Onchocerciasis (river blindness). Weekly epidemiological record 80: 257–260. Available:
http:⁄⁄www.who. int/wer/2005/wer8030.pdf.
WHO, (2011). Onchocerciasis Control Programme in West Africa (OCP).
http://www.who.int/apoc/onchocerciasis/ocp/en/index.html
Wildenburg G., Darge K., Knab J., Tischendorf F.W., Bonow I. and Buttner D.W. (1994). Lymph nodes of
onchocerciasis patients after treatment with ivermectin: reaction of eosinophil granulocytes and their
cationic granule proteins. Trop. Med. Parasitol. 45: 87‐96.
Wildenburg G., Korten S., Mainuka P. and Buttner D. W. (1998). Ivermectin influence on the mast cell activity in
nodules of onchocerciasis patients. Trop. Med. Int. Health 3: 918‐925.
Williams J.F., Abu Yousif A.H., Ballard M., Awad R., El Tayeb M. and Rasheed M. (1985). Onchocerciasis in Sudan:
the Abu Hamed focus. Trans. R. Soc.Trop. Med. Hyg. 79: 464–468.
Winnen M., Plaisier A.P., Alley E.S., Nagelkerke N.J., van Oortmarssen G., Boatin B.A. and Habbema J.D. (2002). Can
ivermectin mass treatments eliminate onchocerciasis in Africa? Bull. World Health Organ. 80: 384‐391.

68
Recent advances in onchocerciasis research and implications for control
Xie H., Bain O. and Williams S.A. (1994). Molecular phylogenetic studies on filarial parasites based on 5s ribosomal
spacer sequences. Parasite 1: 141‐151.
Yameogo L. (2003). Thirty Years of Onchocerciasis Control in West Africa: Black fly larviciding and environmental
protection. IRD Edition, Paris 2003.
Zambou N.F., Mbiapo T.F., Lando G., Tchana K.A. and Gouado I. (1999). Effect of Onchocerca volvulus infestation
on plasma vitamin A concentration in school children in a rural region of Cameroon. Cahiers Santé 9:151‐
155.
69
Recent advances in onchocerciasis research and implications for control
Appendices

70
Recent advances in onchocerciasis research and implications for control
Appendix A
Statement of task
Research in Onchocerciasis particularly that concerned with chemotherapy and immunity has been limited by the
lack of an appropriate animal model for Onchocerca volvulus. Of all animal models used, only O. volvulus in
chimpanzees closely resembles O. volvulus in man. This is, however, impractical for use on a large scale for
research. Rodents are non‐permissive to O. volvulus. In recent years, work carried out by a team of Cameroonian,
British and German scientists in natural cattle infections at the Veterinary Research Laboratory of IRAD Wakwa,
Ngaoundere, Cameroon and in experimental infections in the University of Liverpool, United Kingdom, identified
the bovine species, O. ochengi as an analogue of O. volvulus for chemotherapeutic and immunological research.
Published results of the studies have direct relevance to the development of improved means of controlling river
blindness. In fact, another team of Cameroonian researchers working in collaboration with Ghanaian, British and
German scientists have applied these results in human trials using mass community‐directed approach. Another
leading Cameroonian scientist has studied extensively the occurrence of adverse reactions to Mectizan treatment
especially in areas of O. volvolus co‐infection with Loa loa in Cameroon, the Democratic Republic of Congo, Angola
and Sudan.
All of the above shows that Cameroonian scientists and their partners have generated a large amount of crucial
scientific data that can be useful in the control of human Onchocerciasis. A lot of the data is really groundbreaking
scientific development. Unfortunately, it is buried in different scientific journals and is not available to
stakeholders (donors, policy makers, disease control officials and nongovernmental organisations) involved in
treatment and control efforts.
In recognition of its advocacy role, the Cameroon Academy of Sciences (CAS) through its National Forum for Public
Health decided to convene an expert panel to bring together the data, analyse it and offer conclusions and
recommendations pertinent for research and policy reorientations for human Onchocerciasis. The panel
synthesized and discussed relevant evidence and knowledge based on findings from research and recommended
actions targeted at policy and decision makers, funding agencies, nongovernmental organisations, researchers and
disease control officials.
The specific aims of the study were to:
Describe the global magnitude of human Onchocerciasis and the situation in Cameroon.
Describe the pathological and socio‐economic effects of Onchocerciasis (River blindness) in humans.
Examine current treatment and control strategies and the gaps therein.
Carry out an analytical synthesis of onchocerciasis research carried out by Cameroonian scientists and
their foreign partners with particular reference to:
o Chemotherapy and immunology – using insights from the O. ochengi/cattle model.
71
Recent advances in onchocerciasis research and implications for control
o Key experimental findings of the O. ochengi/cattle model that have direct relevance to the
development of improved means of controlling river blindness.
o Use of doxycycline against onchocerciasis in clinical settings and mass community‐directed
approach in West and Central Africa.
o Observations on the current use of Mectizan in the control of Onchocerca volvolus in West and
Central Africa.
Examine the effectiveness of alternative treatment and control strategies resulting from the above
studies.
Recommend strategies to improve the control and possible elimination of onchocerciasis.
It was hoped that the report of this study would present, subject to available published evidence, sound
advice and reasoning for reorientation of the current Onchocerciasis control strategies and funding for more
research and also provoke dialogue among stakeholders and draw public attention.

72
Recent advances in onchocerciasis research and implications for control
Appendix B
Biographical sketch of committee members
Vincent N. TANYA, DVM, M.Sc., PhD, is Chief Research Officer with the Institute of Agricultural Research for
Development (IRAD), Cameroon and Technical Adviser No 1 in Cameroon’s Ministry of Scientific Research and
Innovation. He is also the Programme Officer for the Cameroon Academy of Sciences. He is a Fellow of the
Cameroon Academy of Sciences. In recognition of his leadership role in the O. ochengi/cattle model system for
immunological and chemotherapeutic studies on onchocerciasis and the groundbreaking results on the antibiotic
therapy of onchocerciasis, he was elected into the Third World Academy of the Sciences in 2004. He attended the
University of Ibadan, Nigeria, the University of Edinburgh, UK and the University of Florida, Gainesville, USA, and
obtained the degrees of DVM, M.Sc. and PhD respectively. As an arbovirologist/epidemiologist, he has studied and
supervised students on foot and mouth disease, bluetongue virus, rinderpest virus, avian influenza and
onchocerciasis. He has been either principal investigator or co‐investigator on research grants financed by the FAO,
DFID (formerly ODA/NRI), MACROFIL (WHO), AUF (formerly AUPELF‐UREF), Wellcome Trust and the European Union.
He has been Head of the Veterinary Research Laboratory at the IRAD Regional Research Centre of Wakwa,
Ngaoundere, the Chief of the IRAD Regional Centres at Wakwa, Ngaoundere and Bambui and the Scientific
Coordinator for Animal and Fisheries Production at IRAD Headquarters. He has 75 articles in peer‐reviewed
journals. He is Chair of the CAS Panel for this study.
Samuel Wanji, B.Sc., M.Sc., Doc. Uni., HDR, is Associate Professor of Molecular Parasitology and Entomology at the
University of Buea, Cameroon. He has degrees of B.Sc. from the University of Orleans, France, M.Sc. and Doctorate
from the University of Montpellier II, France, and HDR from the University of Nantes, France. He is Executive
Director of the Research Foundation in Tropical diseases and Environment, Buea, Cameroon. He is Member of the
American society of Tropical Medicine and Hygiene (ASTMH), the French Society of Parasitology and the
Cameroonian Society of Parasitology. He is a Consultant for the Special Programme for Research and Training in
Tropical Diseases for the World Health Organisation, in which he is involved with the development and validation
of the Rapid Assessment Procedures for Loiasis (RAPLOA) and community‐directed interventions for major health
problems in Africa. He has been involved in the mapping of Loiasis using RAPLOA in different African countries like
the Democratic Republic of Congo, Republic of Congo, Sudan, Angola, Equatorial Guinea and Cameroon for the
African Programme for Onchocerciasis Control (APOC). He has had several research grants as either principal
investigator or co‐investigator from the European Union, l’AUPELF‐UREF, UNDP/World Bank/WHO Special
Programme for Research and training in Tropical diseases, FICU, the African Programme for Onchocerciasis control
(APOC), the Volkswagen Foundation, the Wellcome Trust, Medical Research Council,UK, and DFG Germany. He has
52 articles.
Joseph KAMGNO, MD, MPH, PhD, is Senior Lecturer in the Department of Public Health, Faculty of Medicine and
Biomedical Sciences of the University of Yaoundé I, Cameroon. After graduating as a medical doctor from the same
University, he later on obtained the Diploma in epidemiology of transmissible diseases in Pasteur Institute in Paris,
the degree of Masters and PhD in Public Health and epidemiology from the University of Paris 6. He has been a
general practitioner (1994 – 1999) at the Pasteur Centre of Cameroon, Research Assistant (2000 ‐2002) at the
same Centre and Technical Adviser (2003 – present) for the National Programme for Onchocerciasis Control. He is

73
Recent advances in onchocerciasis research and implications for control
the Director of Filariasis and other Tropical Diseases Research Center. He is also Adviser for the
Mectizan/Albendazole Experts Committee and member of the Committee of Expert Evaluators of the Development
of Moxidectin. He is a member of the American Society of Tropical Medicine and Hygiene. He has worked on the
effects of ivermectin on O. volvulus and problems related to co‐endemicity with loaisis, the cartography of
parasites in Cameroon and the diagnosis and handling of post ivermectin adverse events in Cameroon, Democratic
Republic of Congo, Angola and Sudan. He has many research grants from Mectizan Donation Program,
UNDP/World Bank/WHO Special Programme for Research and training in tropical diseases, Bertrand Buisson
Institute, US Lymphatic Filaria Support Center, Helen Keller International/RTI and WHO/APOC. He has 57 papers in
peer‐reviewed journals.
Daniel M. ACHUKWI, DVM, PhD, is Chief Research Officer and Director of Scientific Research with IRAD in Yaounde,
Cameroon. He obtained the degree of DVM from the University of Ibadan, Nigeria and later on the PhD from
Strathclyde University in Glasgow, UK. He is also Head of IRADs Animal Health Programme. He was IRAD’s Regional
Scientific Coordinator for the High Guinea Savanna Agro‐ecological Zone from 2006 to May 2011. He has wide
experience in local/rural agricultural production systems and tropical livestock diseases. He has attended several short
courses including specialization in research‐extension linkages, systems‐oriented management and planning basis for
the improvement of animal health in the tropics and immunology/molecular biology of vector transmitted parasitic
diseases of livestock. He teaches immunology at postgraduate level to students of the Department of Biological
Sciences, University of Ngaoundere, molecular parasitology at postgraduate level in the Faculty of Science,
University of Buea and immunology at undergraduate level in the School of Veterinary Sciences and Medicine of
the University of Ngaoundere, Cameroon. He is currently supervising 4 doctoral students. He has been either
principal investigator (PI) or co‐PI on competitive grants financed by IFS, FAO, MACROFIL (WHO), DFG, European
Union, Leverhulme Trust, and AUSAid (CORAF/WECARD) for research on protozoan diseases of economic
importance in livestock and onchocerciasis. He has 35 publications in peer‐reviewed journals.
Peter Ayuk ENYONG, Lic. es Sc., Maitrise es Sc., DEA, Doct. es Sc., was a Senior Researcher of the Institute for
Medical Research and Study of Medicinal Plants. For years, he was the Chief of the Tropical Medicine Research
Station in Kumba. He is presently Senior Research Fellow at the Research Foundation in Tropical Diseases and
Environment, Buea, Cameroon. He is holder of the degrees of Licence es Sciences (chemistry/biology), Maitrise es
Sciences (chemistry/biology), DEA (animal biology), Maitrise es Sciences (entomology) and Doct. Es Sc. from the
University of Paris‐Sud Orsay, France. In collaboration with several colleagues, he has had several grants from the
European Union, WHO/TDR, Edna McConnell Clark Foundation, AUPELF‐UREF, NIH, The Wellcome Trust, Medical
Research Council, UK, and DFG Germany. He continues to act as a consultant for the WHO and APOC and
supervises graduate students. Throughout his long career, he studied the entomology of Simulium damnosum, the
vector of O. volvolus, the biology and ecology of Anopheles gambiae, the control of nuisance of Aedes caspius in
the Langueduc canals in Southern France, the control of Culex quinquefaciatus in Kumba, Cameroon and the
malaccology of Schistosomiasis and Paragonimiasis. He is presently working on a European Union funded research
project on novel release system and bio‐based utilities for mosquito repellent textiles and garments. The project
entails the field testing of various repellent garments and bed net materials against mosquitoes (especially
Anopheles). He has 45 articles in peer‐reviewed journals.