Embed Size (px)
Citation preview

Sponsored by
Finding 1:Latin America has substantial room
to improve cancer care
Improving cancer outcomes:Key reforms
people will develop cancer in 2020 alone, leading to
Costs to publichealth systems
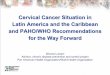
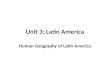
While global cancer deaths are rising, age-standardized cancer death rates are falling
The relative number of deaths is nearly double that of the US and other developed countries, due to insu�cient access to prevention, screening and key treatments like immunotherapy and precision radiotherapy.
Countries with strong decision-making systems, that leverage the best data, evidence and guidelines, will lower mortality
Health Technology Assessment agencies (HTAs) evaluate
cost-e�ectiveness. Argentina, Brazil and Mexico actively use HTAs for drug
approval and funding but regionally these are often absent or under-resourced.
Cancer care registries guide planning. Latin America has roughly 90, covering 20% of the population. Only 7% have
high quality information.
Mexico has the strongest vital registration data of the EIU’s study.
Cancer control plans provide strategic vision but only 11 out of out of
19 Latin American countries had cancer control plans
Peru’s Plan Esperanza integrates services and includes
marginalised groups.
Global death rates from cancer declined 17% between from 1990 to 2016. Cancer deaths, rate and age-standardized rate index, World Index of absolute number of
cancer deaths, the all ages death rate (measured as the number of deaths per 100,000) and age-standardized death rate (assuming a constant population age structure). Figures are indexed to the year 1990, where deaths and rates in 1990 are equal to 100.
1 milliondeaths.
regional increase in cancer incidence by 2030
Direct costs of lung cancer in the region
Annual cost of prostate cancer in Brazil by 2022, a 50% increase
ranges from 42% (Brazil) to 61% (Bolivia) among countries in this study
67%67%
$1.36bn$1.36bn $1.8bn$1.8bn
17%17%
1.7million
Health spending is low relative to GDP.
South America’s spending on cancer care is 0.125% of gross national income per capita (ranging from 0.06% in Venezuela to 0.29% in Uruguay) as compared with 0.51%, 0.6%, and 1.02% for the United Kingdom, Japan, and the US.
Ministries of Health
(& National Cancer Institutes)
RegulatoryBodies
HTA Bodies
Academic Partners
Payers and SocialSecurity
Legal Systems ( Judicialisation)
Regional & International
Bodies
Strengthen population-based cancer registries
Encourage data-sharing between government, pharmacies, hospitals and companies.
Support HTAs to accommodate emerging therapies
Develop evidence-based clinical guidelines
Twinning with global centres of excellence can improve sharing of best practices
Countries can lower costs by pool-purchasing drugs
NGOs can drive progress in fighting tobacco and supporting program monitoring
Greater academic participation can support policy; >80% of researchers in Argentina have
never contributed to decision-making but over 90% would like to.
0.125%South America1.02%
US
1990 1995 2000 2005 2010 20160
20
40
60
80
100
120
140
Total deaths
Death rate(all ages)
Death rate(age-standardized)
Source: OurWorldinData based on IHME, GBD CC BY
100
83
1990 2016
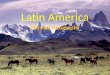
70%60%50%40%30%20%10%0%
All-Cancer Mortality-to-Incidence Ratios, 2018.
Argentina
Bolivia
Brazil
Chile
Colombia
Mexico
Panama
Peru
USA
Canada
Latin America (average)
Global(average)
The decision-makers
0.6%Japan
49%
Chile’s mortality- to-incidence ratio
compared to peer average of 23%.
Nodes ofdecision-making
Existingsources
Foundation
Informed decision-makers, institutions and processes
Robust Data
A model for understanding cancer care decision-making.
Population-based cancer
registries
Interoperableelectronic health
records
Real-world andclinical evidence
Balanceddecisioncriteria
Healthtechnologyassessment
Economicevaluation
Cancer controlplans
Care standardsand guidelines
Incentives
E�ective Assessment
Integrationinto care
Multi-stakeholder collaboration
Managing misperceptions, bias and influence
Cancer care in Latin America:Closing the gapLatin America's health systems are failing to support cancer patients, leading to high mortality rates. The Economist Intelligence Unit, sponsored by Varian, examines the key decisions that determine care quality and outcomes.
Latin America and the Caribbean is set for rising cancer incidence in the
coming decade
© The Economist Intelligence Unit, 2019
Cancer control:
Prudent investment
Greater collaboration
Invest in data and clinical protocols
In Argentina, fewer than half of patients withliver cancer received recommended treatment
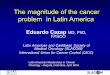
Country Decision-MakingEnvironment
Brazil Moderately Strong
Chile Moderate
Moderate
Moderate
Moderately Weak
Moderately Weak
Weak
Weak
IncomeGroup
Upper-Middle Income
High-Income
Upper-Middle Income
Upper-Middle Income
Upper-Middle Income
Upper-Middle Income
High-Income
Lower-Middle Income
Mexico
Colombia
Argentina
Peru
Panama
Bolivia
Summary ranking of enabling environments for cancer caredecision-making
Weak
Moderately weak
Moderately strong
Moderate
Not studied
Decision-making environments for optimisation of cancer care.
Overview of enablers and resisters to evidence-based decision-making for cancer care in Latin America.
Enablers Resistors
RobustData
Data Sources: Prioritisation of quality improvement and expansion of population-based cancer registries, electronic health records, and other sources of quality health data to inform more strategic decisions
Research: Strong health services research and public health workforce in the region to be better integrated into decision-making processes
Research: Research agenda often dictated by foreign donors which makes it di�cult to focus on regional priorities
Data Sources: Limited information in terms of real world evidence causes decisions to be made from “10,000 feet away”’ and make it challenging to hold decision-makers accountable
E�ectiveAssessment
Health technology assessment infrastructure: Growing regional collaboration for health technology assessments and other forms of assessment through RedETSA, ICES, ICES, LatAm HTAi Policy Forum, etc.
Workforce capacity: Emergence of educational programs and curriculum in medical training for health technology assessments, pharmacoeconomics, economic evaluations, etc.
Segmentation: Disparate agencies and bodies cause confusion and delay in health technology assessments and other assessments, with some agencies lacking independence
Judicialisation: In countries with rights to health, courts frequently do not consider cost-e�ectiveness analyses, health technology assessments, or resource allocation assessments already conducted in decisions
Integrationinto care
Planning: National cancer control plans largely in e�ect or being developed, with building recognition of their value
Localisation: Growing recognition of the value of localised cancer guidelines
Collaboration: Stronger inter-institutional and regional multi-stakeholder collaboration across the region to solve common challenges
Equity: Centralisation of cancer resources in large urban areas creating access issues for rural population
Fragmentation: Complex bureaucracy and regulation caused by fragmented health systems
Influences: Conflicting interests, misperceptions, and fragmentation influence decision processes, particularly in the absence of accessible, high-quality data
Immunotherapy and targeted agents are una�ordable to most patients in the region.
Six countries across the region of Latin America lack access to radiotherapy, a key treatment at curative and palliative stages. Across eight countries in the EIU study, coverage is only 50-75% of the need, with significant disparities between urban and rural.
0.51%United Kingdom
42%61% BrazilBolivia