Embed Size (px)
Citation preview
+
Candida, when does it become a problemMoataz DaoudPharm D. student
+Outline
1. Definition of Candidemia Common pathogens Risk factors
2. Relevance to Critical Care Medicine
3. Prevention Strategies
4. Assessment of Risk Factors Colonization Index Candida Score
5. Drugs of Choice
+Mr. CC
Mr. CC is a 77 year old M admitted to the ICU with septic shock and respiratory failure secondary to cholangitis
PMH Cholecystectomy Hypothyroidism OA (R. HIP)
Blood, sputum, PTC, and urine cultures are sent
Patient is empirically started on piptazo, vancomycin X1, metronidazole X1 and received a single dose of gentamycin
+What is Candidemia
Invasive fungal infection in deep-seated tissue or other normally sterile sites (excluding the urine) documented by histopathology and/or microbiological
culture.
+Pathogenesis
Candida spp. May enter the bloodstream from colonization and growth on an intravascular catheter, or by translocation across gut mucosa Translocation is enhanced by fungal overgrowth commonly
associated with broad-spectrum antibiotic use Epithelial injury secondary to trauma or surgery in the GIT
also facilitates this
Annals of Intensive Care 2011, 1:37
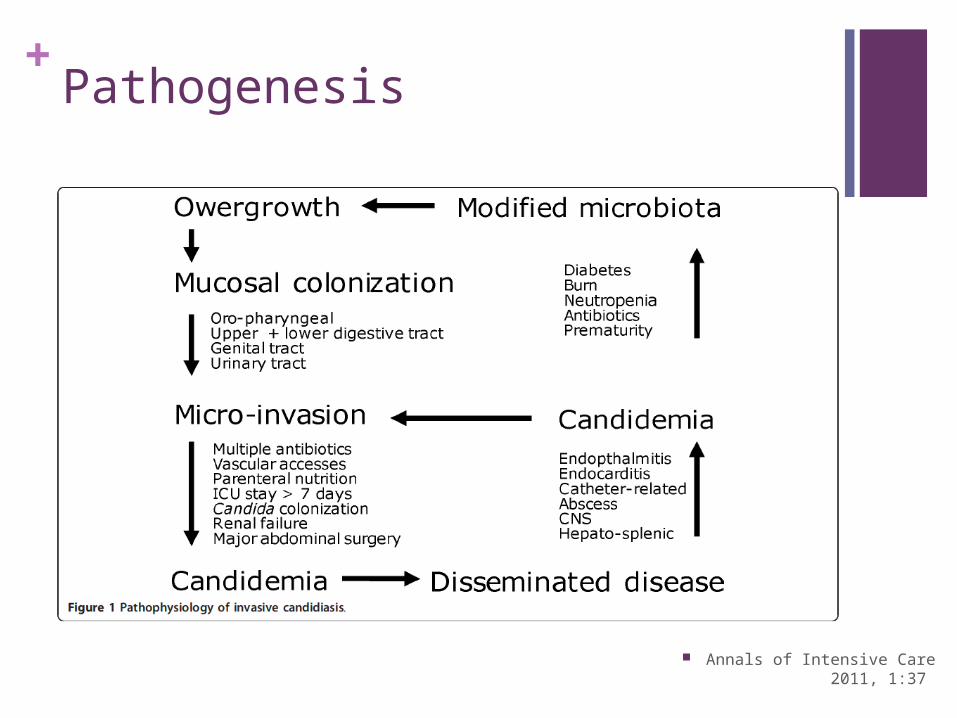
+Pathogenesis
Annals of Intensive Care 2011, 1:37
+Common Pathogens
The predominant organism across Canada remains C. albicans accounting for 62% of candida BSI’s
Other common candida spp. C. glabrata (15%) C. tropicalis (6%) C. parapsilosis (11%) C. krusei (3%)
AMMI Candidiasis Guidelines 2010
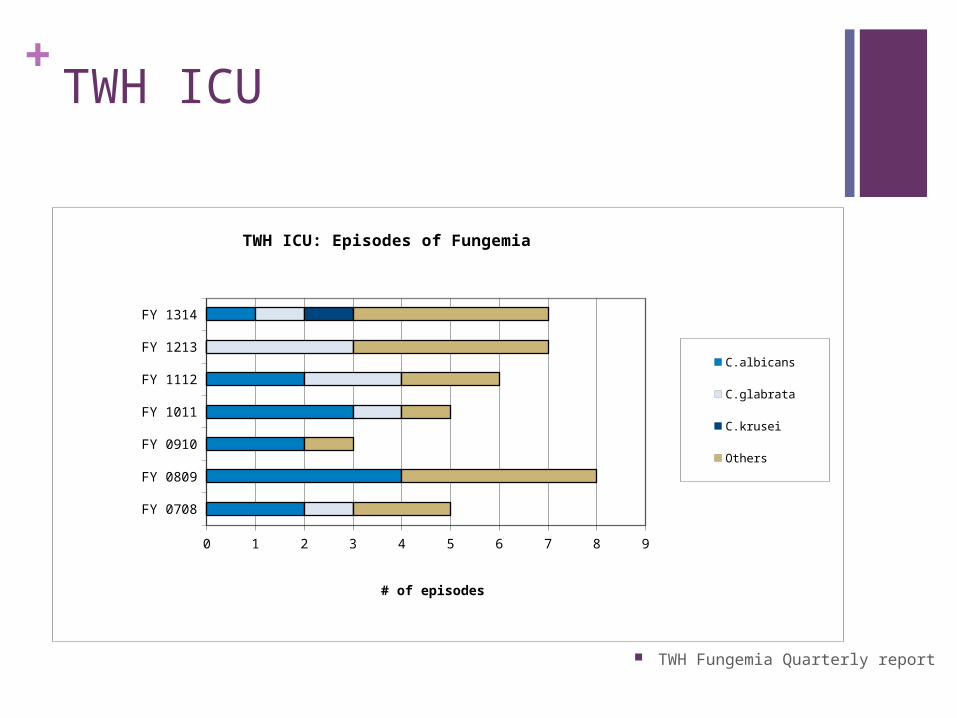
+TWH ICU
FY 0708
FY 0809
FY 0910
FY 1011
FY 1112
FY 1213
FY 1314
0 1 2 3 4 5 6 7 8 9
TWH ICU: Episodes of Fungemia
C.albicans C.glabrata
C.krusei Others
# of episodes
TWH Fungemia Quarterly report
+Risk Factors
Broad-spectrum antibacterial therapy
Central venous catheter use
Renal replacement therapy
Total parenteral nutrition
Corticosteroids (and other forms of cell-mediated immunosuppression)
Diabetes mellitus
Peritonitis without source control
Arch Intern Med 1989, 149:2349-2353.
+Why is it Important
Candidemia is still associated with high crude (35% to 61%) and attributable (24% to 49%) mortality rates
The economic impact of candidemia in Canada is profound A recent study found the cost of treating a case of
candidemia in Canada to be approximately $70,000
1/3 of all candidemia cases occur in the ICU 3rd most common nosocomial BSI in the US (5-10%)
Delay in therapy beyond 12 h after sampling of blood has been associated with an increase of in-hospital mortality from < 20% to 40%
Annals of Intensive Care 2011, 1:37 Crit Care Med. 2009;37:1612-8.
Epub 2009/03/28 Clin Infect Dis 2006, 43:25-31
+Prevention Strategies
Prophylaxis Treating patients with multiple risk factors for infection with
no documented micro or histological evidence
Pre-emptive Those with documented micro or histological evidence
(fungal colonization)
Annals of Intensive Care 2011, 1:37
+Colonization Index
The daily ratio between number of distinct body sites cultured with genotypically identical strains of Candida to total number of sites tested Independent predictor of IC/C
29 heavily colonized patients were assessed The average Candida colonization index was 0.47 for
colonized vs. 0.7 for infected patients, respectively (p < 0.01)
Threshold ≥0.5 identified all infected patients at an average of 6 days before diagnosis of IC
Ann Surg 1994, 220:751-758
Critical Care Med 2004, 32:2443-2449.
+Candida Score
Score ranging from 1-5
Severe sepsis (2 points)
Surgery (1 point)
TPN (1 point)
Multifocal Candida colonization (1 point)*
In a multicenter cohort of 1,007 patients staying for more than 7 days, only 13 of 565 (2.3%) patients with a score < 3 points developed a candidiasis: negative predictive value of 98%.
Crit Care Med 2006, 34:730-737.
+AMMI Guidelines (2010)
Prophylaxis Routine antifungal prophylaxis for all ICU patients is not
recommended but state the selected high risk patients may benefit High risk patients are defined as
Patients with recurrent GI perforations or anastomic leakage Patients admitted to a tertiary referral centre ICU (surgical or
medical) with a baseline risk for C/IC of 10% or greater if there is an anticipated stay of more than three days
Pre-emptive Pre-emptive antifungal therapy in non-neutropenic patients with
the presence of colonization is currently not recommended but empirical antifungal therapy may be beneficial in critically ill patients who meet specific criteria based on clinical prediction rules for C/IC
AMMI Candidiasis Guidelines
+Back to our Mr. CC (day 3)
Cultures come back Blood: enterobacter (ESBL), VRE PTC: GPC in chains, enterobacter Sputum: commensal flora, candida albicans (heavy growth)
Patient switched to meropenem
Is he a candidate for pre-emptive antifungal therapy? What’s his colonization index What’s his Candida score
+Which agents to use
Fluconazole Available as both PO and IV Excellent tolerability Inexpensive widely studied for prophylaxis in ICU patients Safe and effective in HD stable patients who are azole
naive
Echinocandins (Caspofungin, Micafungin) Only available as IV Expensive Broad spectrum but appropriate in HD unstable patients
due to
+
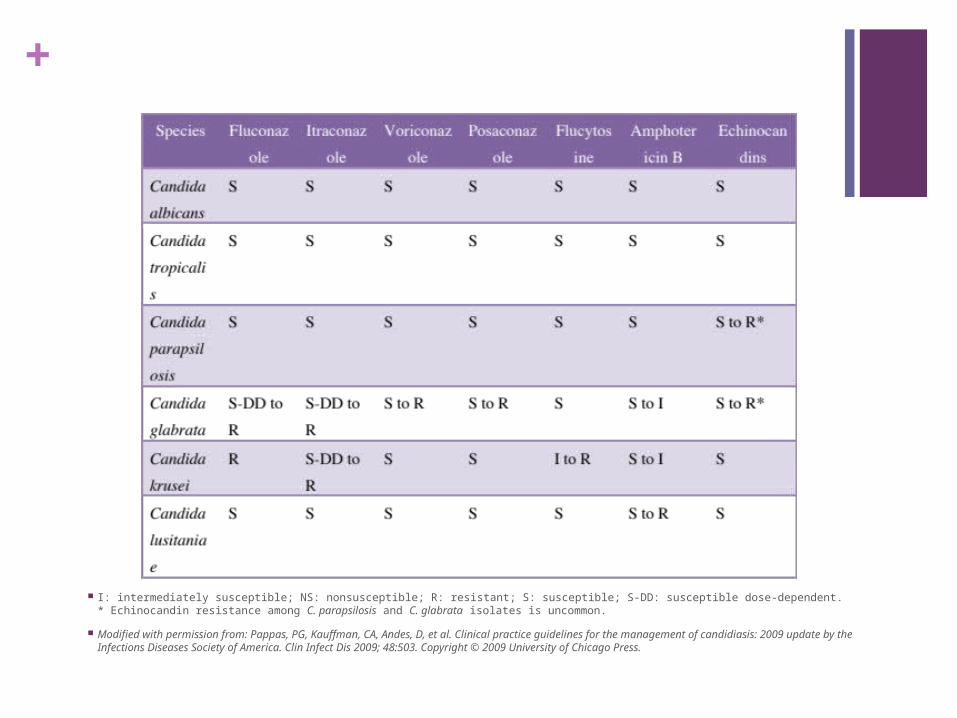
I: intermediately susceptible; NS: nonsusceptible; R: resistant; S: susceptible; S-DD: susceptible dose-dependent.* Echinocandin resistance among C. parapsilosis and C. glabrata isolates is uncommon.
Modified with permission from: Pappas, PG, Kauffman, CA, Andes, D, et al. Clinical practice guidelines for the management of candidiasis: 2009 update by the Infections Diseases Society of America. Clin Infect Dis 2009; 48:503. Copyright © 2009 University of Chicago Press.
+Azoles
Fluconazole remains efficacious in reducing C/IC and is cost effective at a loading dose of 800 mg followed by IV 400 mg daily for hemodynamically stable patients
+Echinocandins
caspofungin 70 mg IV as a loading dose followed by IV 50 mg daily
micafungin 100 mg IV daily
+References1. Philippe Eggimann, Jacques Bille and Oscar Marchetti: Diagnosis of invasive candidiasis in the ICU.
Annals of Intensive Care 2011, 1:37
2. Eric J Bow, et al.: Canadian clinical practice guidelines for invasive candidiasis in adults
3. ASP: Toronto Western ICU Fungemia Quarterly Report (unpublished)
4. Wey SB, Mori M, Pfaller MA, Woolson RF, Wenzel RP: Risk factors for hospital-acquired candidemia. A matched case-control study. Arch Intern Med 1989, 149:2349-2353.
5. Wey SB, Mori M, Pfaller MA, Woolson RF, Wenzel RP: Risk factors for hospital-acquired candidemia. A matched case-control study. Arch Intern Med 1989, 149:2349-2353.
6. Leroy O, Gangneux JP, Montravers P, Mira JP, Gouin F, Sollet JP, et al. Epidemiology, management, and risk factors for death of invasive Candida infections in critical care: a multicenter, prospective, observational study in France (2005-2006). Crit Care Med. 2009;37:1612-8. Epub 2009/03/28.
7. Garey KW, Rege M, Pai MP, Mingo DE, Suda KJ, Turpin RS, et al: Time to initiation of fluconazole therapy impacts mortality in patients with candidemia: a multi-institutional study. Clin Infect Dis 2006, 43:25-31.
8. Pittet D, Monod M, Suter PM, Frenk E, Auckenthaler R: Candida colonization and subsequent infections in critically ill surgical patients. Ann Surg 1994, 220:751-758.
9. Piarroux R, Grenouillet F, Balvay P, Tran V, Blasco V, Milloin M, et al: Assessment of preemptive treatment to prevent severe candidiasis in critically-ill surgical patients. Critical Care Med 2004, 32:2443-2449.
10. Leon C, Ruiz-Santana S, Saavedra P, Almirante B, Nolla-Salas J, varez- Lerma F, et al: A bedside scoring system ("Candida score”) for early antifungal treatment in nonneutropenic critically ill patients with Candida colonization. Crit Care Med 2006, 34:730-737.

![Prolonged Outbreak of Candida krusei Candidemia in ... · per 1000 admissions) [1]. Among Candida species causing candidemia, non-albicans Candida (NAC) species are the leading agents](https://img.pdfslide.net/doc/110x75/5ec53fd6a9dc5f3c0426d811/prolonged-outbreak-of-candida-krusei-candidemia-in-per-1000-admissions-1.jpg)





![Brych Technology LLC PRESENTATION [Recovered]](https://img.pdfslide.net/doc/110x75/5884b0291a28ab76798b6889/brych-technology-llc-presentation-recovered.jpg)
![Poster_IIC [Recovered] [Recovered]](https://img.pdfslide.net/doc/110x75/568bf4721a28ab89339e0ba6/posteriic-recovered-recovered.jpg)

![Presentation ABB Phasor [Recovered]](https://img.pdfslide.net/doc/110x75/55cf8527550346484b8b5387/presentation-abb-phasor-recovered.jpg)
![Volume.ppt [recovered]](https://img.pdfslide.net/doc/110x75/55631c69d8b42a81528b5342/volumeppt-recovered.jpg)
![Creative and media presentation [recovered]](https://img.pdfslide.net/doc/110x75/54462a9eafaf9f59178b457e/creative-and-media-presentation-recovered.jpg)





![Gap presentation (1) [recovered]](https://img.pdfslide.net/doc/110x75/55a83bd31a28abfa768b486e/gap-presentation-1-recovered.jpg)


![Govt Acctg Recovered] Recovered]](https://img.pdfslide.net/doc/110x75/577d26c61a28ab4e1ea2266a/govt-acctg-recovered-recovered.jpg)

![Evaluation media presentation1 [recovered] [recovered]](https://img.pdfslide.net/doc/110x75/5539c6115503464e418b4a65/evaluation-media-presentation1-recovered-recovered.jpg)
![Respimicro [recovered]](https://img.pdfslide.net/doc/110x75/554b0df7b4c90562098b478a/respimicro-recovered.jpg)
![Improve your presentation skills techniques a [recovered] lite](https://img.pdfslide.net/doc/110x75/55d054c5bb61ebb37b8b45c4/improve-your-presentation-skills-techniques-a-recovered-lite.jpg)
![Anglesinlife [Recovered]](https://img.pdfslide.net/doc/110x75/5592a5e61a28ab57798b46dd/anglesinlife-recovered.jpg)
