-
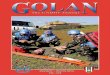
Zonaglomerulosa
Angiotensin IIK+
ACTH
Aldosterone
Cortisol,androgens
11-hydroxylase17-hydroxylase
Aldosteronesynthase
Zonafasciculata/reticularis
-
CHAPTER 28 / Pharmacology of the Adrenal Cortex 491
protects the mineralocorticoid receptor from activation by
cortisol in a variety of cell types, including endothelial cells
and vascular smooth muscle cells. In contrast, cortisone can be
converted back to cortisol (also referred to as hydrocorti-sone )
in the liver by 11 -hydroxysteroid dehydrogenase type 1 (11 -HSD 1,
Fig. 28-3A). The interplay between these op-posing reactions
determines overall glucocorticoid activity. In addition, as
discussed below, the activity of these enzymes is important in
glucocorticoid pharmacology.
Physiologic Actions Like other steroid hormones, unbound
cortisol diffuses through the plasma membrane into the cytosol of
target cells, where the hormone binds to a cytosolic receptor.
There are two types of glucocorticoid receptors: the Type I
(mineralo-corticoid) and Type II glucocorticoid receptors . The
Type I receptor is expressed in the organs of excretion (kidney,
colon, salivary glands, sweat glands) and other tissues in-cluding
the hippocampus, vasculature, heart, adipose tissue, and peripheral
blood cells. The Type II receptor has a broader
overall capacity, whereas albumin has low cortisol affi nity but
high overall capacity. Only molecules of cortisol that are unbound
to protein (the so-called free fraction ) are bioavail-able, that
is, available to diffuse through plasma membranes into cells. Thus,
the affi nity and capacity of plasma bind-ing proteins regulate the
availability of active hormone and, consequently, hormone
activity.
The liver and kidneys are the primary sites of peripheral
cortisol metabolism. Through reduction and subsequent con-jugation
to glucuronic acid, the liver is responsible for inacti-vating
cortisol in the plasma. The conjugation reaction makes cortisol
more water soluble, thus enabling renal excretion. Importantly, the
liver and kidneys express different isoforms of the enzyme 11
-hydroxysteroid dehydrogenase , a regu-lator of cortisol activity.
The two isoforms catalyze opposing reactions. In distal collecting
duct cells of the kidney, 11 -hydroxysteroid dehydrogenase type 2
(11 -HSD 2) converts cortisol to the biologically inactive compound
cortisone , which (unlike cortisol) does not bind to the
mineralocorticoid receptor (see below, Fig. 28-3B). Expression of
11 -HSD 2
ACTH
CholesterolAminoglutethimideKetoconazole (high)
Feedback inhibition
Trilostane
Metyrapone
Ketoconazole
Trilostane
Metyrapone
Pregnenolone
17-hydroxypregnenolone
17-hydroxyprogesterone
11-deoxycortisol
Cortisol
GlucocorticoidsMineralocorticoids Sex steroids
Progesterone
11-deoxycorticosterone
Corticosterone
Aldosterone
Dehydroepiandrosterone
Androstenedione
Testosterone
Anterior pituitary gland
Adrenal gland
Trilostane
17
21
11
1721
11
FIGURE 28-2. Hormone synthesis in the adrenal cortex. The
hormones of the adrenal cortex are steroids derived from
cholesterol. The rate-limiting step in adrenal hormone biosynthesis
is the modifi cation of cholesterol to pregnenolone by side-chain
cleavage enzyme. From this step, pregnenolone metabolism can be
directed toward the formation of aldosterone, cortisol, or
androstenedione. The fl ux of metabolites through each of these
pathways depends on the tissue-specifi c expression of enzymes in
the different cell types of the cortex and on the relative activity
of the different synthetic enzymes. Note that several enzymes are
involved in more than one pathway and that defects in these enzymes
can affect the synthesis of more than one hormone. For example, a
defect in steroid 21-hydroxylase prevents the synthesis of both
aldoster-one and cortisol. This overlap of synthetic activities
also contributes to the nonselective action of glucocorticoid
synthesis inhibitors such as trilostane. Enzymes are shown as
numbers: 17, steroid 17 -hydroxylase; 21, steroid 21-hydroxylase;
11, steroid 11 -hydroxylase. Aminoglutethimide and high levels of
ketoconazole inhibit side-chain cleavage enzyme. Ketoconazole also
inhibits 17, 20-lyase. Trilostane inhibits 3 -hydroxysteroid
dehydrogenase. Metyrapone inhibits steroid 11 -hydroxylase.
-
O
O
H
H
H
O
OHOH
O
HO
H
H
H
O
OHOH
O
O
H
H
H
O
OHOH
O
HO
H
H
H
O
OHOH
CortisoneCortisol(agonist at mineralocorticoid
receptor)(inactive at mineralocorticoid
receptor)
CortisolCortisone
11-HSD 1
A
B
(liver)
11-HSD 2
(kidney)
-
CHAPTER 28 / Pharmacology of the Adrenal Cortex 493
stores little cortisol, ACTH regulates cortisol production by
promoting synthesis of the hormone. ACTH also has a trophic effect
on the zona fasciculata and zona reticularis of the adrenal cortex,
and hypertrophy of the cortex can occur in response to chronically
elevated levels of ACTH.
As in other endocrine axes, the hormone (cortisol) pro-duced by
the target organ (adrenal cortex) exerts negative feedback
regulation at the level of both the hypothalamus and the anterior
pituitary gland. High cortisol levels de-crease both synthesis and
release of CRH and ACTH. Be-cause ACTH has important trophic
effects on the adrenal cortex, the absence of ACTH leads to atrophy
of the cortisol-producing zona fasciculata and the
androgen-producing zona reticularis. However, the
aldosterone-producing zona glom-erulosa cells continue to function
in the absence of ACTH, because angiotensin II and blood potassium
continue to stimulate the production of aldosterone.
Pathophysiology Diseases affecting glucocorticoid physiology can
be divided into disorders of hormone defi ciency and disorders of
hor-mone excess. Addisons disease is the classic example of
adrenocortical insuffi ciency, while Cushings syndrome ex-emplifi
es cortisol excess.
Adrenal Insuffi ciency Addisons disease is an example of a
primary adrenal insuf-fi ciency in which the adrenal cortex is
selectively destroyed, most commonly due to a T cell-mediated
autoimmune reac-tion but alternatively due to infection, infi
ltration, cancer, or hemorrhage. Destruction of the cortex results
in decreased synthesis of all classes of adrenocortical hormones.
By comparison, secondary adrenal insuffi ciency is caused by
hypothalamic or pituitary disorders or by prolonged admin-istration
of exogenous glucocorticoids. In secondary adrenal insuffi ciency,
the decrease in ACTH levels causes decreased
CRH then travels through the hypothalamicpituitary por-tal
system and binds to G protein-coupled receptors on the surface of
corticotroph cells in the anterior pituitary gland. CRH binding
stimulates the corticotrophs to synthesize proo-piomelanocortin
(POMC) , a precursor polypeptide that is cleaved into multiple
peptide hormones including ACTH. The neurons in the paraventricular
nucleus that respond to stress by synthesizing and secreting CRH
can also respond to stress by synthesizing and secreting
vasopressin. This vasopressin is released into the
hypothalamicpituitary portal system to-gether with CRH, and it
synergizes with CRH to increase the release of ACTH by the anterior
pituitary gland. Interestingly, the stress-responsive parvocellular
neurons that secrete CRH and vasopressin into the
hypothalamicpituitary portal system are different from the
osmolality-responsive magnocellular neurons that synthesize
vasopressin and transport this hor-mone to the posterior pituitary
gland (see Chapter 26), even though both types of neurons are
located in the paraventricu-lar nucleus of the hypothalamus.
Potential crosstalk between the parvocellular and magnocellular
systems in the paraven-tricular nucleus is an area of active
investigation.
Proteolytic cleavage of POMC yields not only ACTH but also
-melanocytestimulating hormone (MSH), lipotropin, and -endorphin.
MSH binds to receptors on skin melano-cytes, promoting
melanogenesis and thereby increasing skin pigmentation. Because of
the similarities between the ACTH and MSH peptide sequences, high
concentrations of ACTH can also bind to and activate MSH receptors.
This action becomes apparent in primary hypoadrenalism (see below),
in which increased ACTH levels result in increased skin
pigmentation. The role of lipotropin in human physiology is
uncertain but is thought to involve control of lipolysis.
-Endorphin is an endogenous opioid that is important for pain
modulation and for regulation of reproductive physiology.
Because steroid hormones are able to diffuse freely through cell
membranes and because the adrenal gland
FIGURE 28-4. The immuneadrenal axis. Cortisol has profound
immunosuppressive effects. Cortisol inhibits the action of several
mediators of infl ammation (eicosanoids, serotonin, platelet
activating factor [PAF], bradykinin). Cortisol also inhibits the
release of a number of cytokines from macrophages, including IL-1 ,
IL-1 , IL-6, and TNF- . Because these cytokines in turn promote the
hypothalamic release of CRH and thereby increase serum cortisol
levels, it is hypothesized that the stress-induced increase in
cortisol limits the extent of the infl ammatory response.
Pituitarygland
Adrenalgland
HypothalamusCRH
ACTH
Cortisol
Mediators of inflammation(eicosanoids, serotonin,
PAF, bradykinin)
Thermoregulatorycenters
Fever
Immunestimulus
Macrophages
Inflammatorycytokines
(IL-1, IL-1, IL-6, TNF-)