Embed Size (px)
Citation preview

7/31/14
1
David Glendenning Education Coordinator
New Hanover Regional Medical Center EMS
1
Objectives
• Review CPR technique and sequence • Review recent evidence & current studies in the use of
ACLS medications • Review metabolic chain of events during cardiac arrest
and how it relates to oxygenation • Review new research and methods of pre-hospital
Therapeutic Hypothermia
2
Where would you want to collapse in V-FIB?
� Dedicated training of responders
� A confined environment.
� Numerous security cameras.
� Collapse to shock time average is 4.4 minutes.
74% discharge if shock in 3 minutes!
Cardiac Arrest by the Numbers 2012 Cardiac Arrests Survival Rate Mortality Rate Deaths
Out-‐of-‐Hospital 359,400 9.5% 90.5% 325,257
In-‐Hospital 209,000 24.2% 75.8% 158,422
Total 568,400 483,679
For perspective:
Equivalent loss of life to 4 fully loaded Boeing
747s crashing everyday!
4

7/31/14
2
Back to Basics: Effective CPR is the key to successful resuscitation
5
THE BEGINNINGS…….
Almost 60 years later……
Dr. Kouwenhoven and Dr. Knickerbocker invent the defibrillator in 1957, discover the benefit of closed chest compression with Dr. James Jude in 1958, and adding Dr. Peter Safars' work with rescue breathing , create CardioPulmonary Resuscitation in 1960
CPR Technique We need proper: • Rate • Depth • Chest recoil • Minimal pauses • Proper ventilation
To achieve and maintain adequate coronary and cerebral blood flow and increase the likelihood of defibrillation success
8

7/31/14
3
Importance of Effective Compressions Depth Rate
Ventilation CPP 9
Coronary Perfusion Pressure
Current study being conducted out of Univ. of Washington comparing current AHA guidelines of 30:2 with Continuous Chest Compressions with ventilation every 6-8 seconds 10
REAL TIME CPR FEEDBACK
5m 10m 15m 20m 25m 30m 35m
Other Conditions Needed for Successful Defibrillation
• A heart that is not “overfilled” • Following the onset of V-fib the right
ventricle continues to be filled by residual venous return but with no forward flow the chambers expand
• Adequate level of myocardial cell ATP
Up to 2 minutes of high quality chest compressions before defibrillation has been shown to eject stored blood from ventricles and increase myocardial ATP levels by up to 30-40%
12

7/31/14
4
Note that as ATP decreases the V-fib amplitude decrease. Algorithms exist that predict likelihood of defibrillation success and ROSC based off the Amplitude Spectral Area (AMSA) and slope of V-fib waveform.
Myocardial Cell ATP levels and correlating waveform
13
Note RV expansion and decrease in strength of fibrillation with time
Right Ventricular filling in V-fib
14 YouTube
Defibrillation without compressions
Atria still contracting normally but no ventricular response before or after shock
15 YouTube
Defibrillation after Compressions
Only atria contracting prior to shock Atrial and ventricular contraction post shock
16 YouTube

7/31/14
5
Peri-shock Pause Independent Predictor of Survival
Resuscitation Science
Perishock PauseAn Independent Predictor of Survival From Out-of-Hospital Shockable
Cardiac Arrest
Sheldon Cheskes, MD; Robert H. Schmicker, MS; Jim Christenson, MD; David D. Salcido, MPH;Tom Rea, MD; Judy Powell, RN; Dana P. Edelson, MD; Rebecca Sell, MD; Susanne May, PhD;
James J. Menegazzi, PhD; Lois Van Ottingham, RN, BSN; Michele Olsufka, BSN;Sarah Pennington, RN; Jacob Simonini, ACP; Robert A. Berg, MD; Ian Stiell, MD, MSc;
Ahamed Idris, MD; Blair Bigham, MSc; Laurie Morrison, MD, MSc;on behalf of the Resuscitation Outcomes Consortium (ROC) Investigators
Background—Perishock pauses are pauses in chest compressions before and after defibrillatory shock. We examined therelationship between perishock pauses and survival to hospital discharge.
Methods and Results—We included out-of-hospital cardiac arrest patients in the Resuscitation Outcomes ConsortiumEpistry–Cardiac Arrest who suffered arrest between December 2005 and June 2007, presented with a shockable rhythm(ventricular fibrillation or pulseless ventricular tachycardia), and had cardiopulmonary resuscitation process data for atleast 1 shock (n!815). We used multivariable logistic regression to determine the association between survival andperishock pauses. In an analysis adjusted for Utstein predictors of survival, the odds of survival were significantly lowerfor patients with preshock pause !20 seconds (odds ratio, 0.47; 95% confidence interval, 0.27 to 0.82) and perishockpause !40 seconds (odds ratio, 0.54; 95% confidence interval, 0.31 to 0.97) compared with patients with preshock pause"10 seconds and perishock pause "20 seconds. Postshock pause was not independently associated with a significantchange in the odds of survival. Log-linear modeling depicted a decrease in survival to hospital discharge of 18% and14% for every 5-second increase in both preshock and perishock pause interval (up to 40 and 50 seconds, respectively),with no significant association noted with changes in the postshock pause interval.
Conclusions—In patients with cardiac arrest presenting in a shockable rhythm, longer perishock and preshock pauses wereindependently associated with a decrease in survival to hospital discharge. The impact of preshock pause on survivalsuggests that refinement of automatic defibrillator software and paramedic education to minimize preshock pause delaysmay have a significant impact on survival. (Circulation. 2011;124:58-66.)
Key Words: cardiopulmonary resuscitation ! heart arrest ! resuscitation ! survival
Resuscitation from out-of-hospital cardiac arrest (OHCA)continues to challenge emergency medical services
(EMS) systems.1,2 One key to improving survival may de-pend on the characteristic components of cardiopulmonaryresuscitation (CPR). Cardiopulmonary resuscitation metricssuch as chest compression fraction (proportion of timeperforming chest compressions during CPR), chest compres-sion depth, compression rate, and chest recoil can potentiallyaffect survival.3,4 Interruptions in chest compressions havealso been associated with adverse outcomes.5–10 Therefore,the recently published 2010 American Heart Associationguidelines stress the need to minimize interruptions in chest
compressions.11 One important determinant of chest com-pression interruption is compulsory rhythm analysis anddefibrillatory shock for shockable cardiac arrest. Defibrillatorcharacteristics and rescuer actions can contribute to thisinterruption. This specific interruption in chest compressionsbefore and after defibrillatory shock, called the perishockpause (Figure 1), may relate to outcome in a distinctivemanner because of the critical transition between the electricand mechanical characteristics of the heart. As opposed toother interruptions in which the rhythm and mechanical statusof the heart may not be expected to change, the goal ofminimizing perishock pause is successful defibrillation, re-
Received December 8, 2010; accepted April 18, 2011.From the University of Toronto, Toronto, ON, Canada (S.C., B.B., L.M.); University of Washington, Seattle (R.H.S., T.R., J.P., S.M., L.V.O., M.O.);
University of British Columbia, Vancouver, BC, Canada (J.C.); University of Pittsburgh, Pittsburgh, Pennsylvania (J.J.M., D.D.S.); St. Paul’s Hospital,Vancouver, BC, Canada (S.P.); Region of Peel, Emergency Medical Services, Brampton, ON, Canada (J.S.); University of Chicago Medical Center,Chicago, IL (D.E.); University of Ottawa, Ottawa, ON, Canada (I.S.); Children’s Hospital of Philadelphia and University of Pennsylvania, Philadelphia(R.A.B.); University of Texas Southwestern Medical Center, Dallas (A.I.); and University of California/San Diego, San Diego (R.S.).
Correspondence to Sheldon Cheskes, MD, Sunnybrook-Osler Centre for Pre-Hospital Care, Brown’s Line, Ste 100, Toronto, ON, Canada M8W 3S2.E-mail [email protected]
© 2011 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.110.010736
58 by guest on February 21, 2012http://circ.ahajournals.org/Downloaded from
17
turn of organized rhythm, and ultimately resumption ofspontaneous circulation. Although animal studies indicate astrong relationship between shorter perishock interruptions inchest compression and better outcomes,12,13 only a fewclinical studies have evaluated the role of perishock pausewith inconsistent results.14–16
Clinical Perspective on p 66The relationship between perishock pause and outcome has
important implications for care. If shorter perishock interrup-tions improve resuscitation outcome, then additional effortsshould focus on minimizing these interruptions. These effortsmay require improvements in defibrillator technology, bettersafety equipment for rescuers, or additional training toachieve improved rescuer performance. Thus, we undertookan investigation to determine the relationship between per-ishock pauses and survival to discharge in a large OHCAregistry.
MethodsSetting and DesignThe Resuscitation Outcomes Consortium (ROC) consists of 11regional clinical centers across North America. The goal of thesecenters is to promote prehospital research in the areas of cardiacresuscitation and life-threatening trauma.17 Beginning in December2005, the ROC prospectively collected cardiac arrest epidemiologi-cal data (ROC Epistry–Cardiac Arrest) on OHCA evaluated byparticipating agencies.18 Agencies participating in ROC capturedelectronic defibrillator CPR process data, including real-time mea-sures of chest compression fraction, compression depth, and com-pression rate during cardiac arrest resuscitation. Five EMS agencies(Toronto, ON, Canada; Ottawa ON, Canada; Vancouver, BC, Can-
ada; Pittsburgh, PA; Seattle/King County, Washington) participatedin this study.
Study SampleBetween December 1, 2005, and June 30, 2007, patients eligible forthis study included those who sustained OHCA with a first EMSshockable rhythm of ventricular fibrillation or pulseless ventriculartachycardia (VF/VT) for which CPR process data for at least 1 shockwere obtained. The initial rhythm was determined to be VF/VT if theinitial automatic external defibrillator analysis advised a shock or therhythm was interpreted as VF/VT by the initial EMS provider and ashock was provided. We excluded patients who received public-access defibrillation (n!16) before EMS arrival or were missinginformation on survival to hospital discharge (n!8).
MeasurementWe reviewed CPR process recordings from 815 resuscitationsavailable from PhysioControl (n!637), Phillips (n!99), Zoll(n!62), and other (n!17) defibrillators. Real-time data were rec-orded after electrodes were applied to the patients’ chests. Weassessed chest compression fraction, duration of preshock andpostshock pauses, compression depth (Zoll and Philips, n!77), andcompression rate. Following the principles of uniform reporting ofmeasured quality of CPR described by Kramer-Johansen et al,19
preshock pause was defined as the time interval between chestcompression cessation (as detected in the impedance channel wave-form) and shock delivery. Postshock pause was defined as the timebetween shock delivery and chest compression resumption (asdetected in the impedance channel waveform). Perishock pause wasdefined as the total preshock and postshock pause time. Trained dataabstractors used the above specific definitions and manually ab-stracted preshock and postshock intervals from all available CPRprocess files up to 11 shocks. The study principal investigator (S.C.)reviewed a random sample of 20% of cases from each site to ensurethe validity of the abstracted preshock and postshock pause intervals.
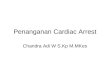
Figure 1. Diagram of preshock, postshock, and perishock pause. Preshock pause of 10 seconds, postshock pause of 2.3 seconds,and perishock pause of 12.3 seconds depicted in the impedance channel of the cardiopulmonary resuscitation process file.
Cheskes et al Perishock Pause Predicts Survival From VF/VT 59
by guest on February 21, 2012http://circ.ahajournals.org/Downloaded from
Study showed that odds of survival were significantly lower for patients with: 1. Pre-shock pause > 20 seconds 2. Peri-shock pause > 40 seconds
Perishock Pause = interruption in chest compressions before and after defibrillatory shock
Optimal Pre-Shock Pause: < 5 seconds, max of 10 seconds
Peri-shock Pause Independent Predictor of Survival
� Resuscitation Outcomes Consortium (ROC) � PRIMED trial 2013 � odds of survival with good CPC:
� pre-shock: highest in shocks < 10 seconds � peri-shock: highest in shocks < 20 seconds
� OR for survival: � decreases 6% for every 5 sec. delay Cheskes S et al. The impact of peri-shock pause on survival from out-of-hospital shockable cardiac arrest during
the Resuscitation Outcomes Consortium PRIMED trial. Resuscitation 2013 Oct 28; [e-pub ahead of print]. (http://dx.doi.org/10.1016/j.resuscitation.2013.10.014)
Do ACLS drugs improve outcomes?
19
Are we really helping our patients?
• AHA 2010 ACLS guidelines: • Epinephrine, Amiodarone, and Lidocaine are
all Class IIb weak “may be considered” recommendations
• Unproven therapies may be: • Beneficial • Inconsequential • Harmful
20

7/31/14
6
Benefit of Each Link in the Chain of Survival Stiell I et al. N Engl J Med 2004;351:647-56
• Ontario Prehospital Advanced Life Support (OPALS) study
• 5,638 Out-of-Hospital Cardiac Arrest patients • Assessed the benefit of each additional link in the
chain of survival to hospital discharge 21
IV Drug Administration in Cardiac Arrest Olasveengen TM et al. JAMA 2009; 301:2222-9
• Oslo, Norway • Randomized trial of resuscitation with and without the
use of ACLS IV medications • 851 Out-of-hospital cardiac arrest cases • Trial considered underpowered to address survival to
discharge
0%
10%
20%
30%
40%
50%
ROSC Admitted to Hospital Admitted to ICU Discharged Alive at 1 Year
Surv
ival
Rat
e
IV Meds
No Meds
22
Epinephrine: The Mainstay of Cardiac Arrest
Care since 1974 ACLS Guidelines
23
Prehospital Epinephrine Use & Survival in Japan Hagihara A et al. JAMA 2012; 307:1161-8
Retrospective study on data of 417,188 out-of- hospital cardiac arrests from 2005-2008
• Limitations to note • Not a randomized, placebo-controlled trial where all
variables are known and controlled • EMS personnel in Japan didn’t carry Epinephrine until 2006
and dosage was not standardized across agencies • Hospital care was variable and missing data in many cases • Less than 4% of cases administered Epinephrine
24

7/31/14
7
Outcome
Despite the known limitations of the study; due to trial size, the outcome of this study has opened the door for future trials
25
Effect of Epinephrine in Cardiac Arrest Jacobs I et al. Resuscitation 2011;82(9):1138-43
• Perth, Australia • Double blind, randomized, placebo controlled
trial of Epinephrine vs placebo • 4,103 Out-of-hospital cardiac arrests
• 534 cases randomized and included in study
0%
5%
10%
15%
20%
25%
30%
ROSC Discharged
Epinephrine
No Epinephrine
26
Antiarrhythmic Yes…No? We Don’t Know.
27
AMIODARONE FOR RESUSCITATION AFTER OOH-CA ARREST DUE TO VF N Engl J Med 1999; 341:871-878
• Seattle & King County ARREST study • Double blind, randomized trial of Amiodarone vs
placebo • 504 Out-of-hospital cardiac arrest cases • No statistical difference in survival to discharge
28

7/31/14
8
Amiodarone vs Lidocaine In PreHospital Refractory VF N Engl J Med 2002;346:884-90
• Toronto ALIVE study • Double-blind, randomized trial of Amiodarone
vs Lidocaine • 347 Out-of-hospital cardiac arrest cases • No statistical difference in survival to discharge
29
The Answer May Lie in the ALPS Trial
• ALPS: Amiodarone, Lidocaine, or Placebo Study
• Led by University of Washington • 10 locations across U.S. and Canada • 70 EMS agencies participating
• 3,000 patients over approximately 3 year period • First patient enrolled in June, 2012 • As of February, 2014 approximately 1,200 patients
enrolled
30
ALPS design
31
ALPS drug kits
32

7/31/14
9
Oxygenation: More is Not Always Better
33
Metabolic Chain of Events
Cell Death & Cerebral Injury
34
Oxygen Free Radicals Increased Blood Flow
& O2 Reperfusion
ROSC CPR, Defibrillation,
& ACLS Cell Damage
Widespread Ischemia (Ischemic Cascade)
Decrease of Blood Flow
Cardiac Arrest
Hyperoxia Post-Resuscitation Survival from Cardiac Arrest Kilgannon et al. JAMA 2010; 03(21):2165-2171
• 6,326 ICU patients from 120 hospitals • 18% patients hyperoxic (PaO2 > 300) • 63% patients normoxic (60 > PaO2 < 300) • 19% patients hypoxic (PaO2 < 60)
• Mortality higher with hyperoxia than hypoxia
0%
10%
20%
30%
40%
50%
60%
70%
Hyperoxia Normoxia Hypoxia
Mortality
35
Therapeutic Hypothermia
36

7/31/14
10
Early Trials Showed Great Promise
37
Induced Hypothermia (32-34º C) N Engl J Med 2002; 346 : 549-556
• Europe • 275 VF/VT ROSC patients • Cooled to 32-34ºC for 24 hours
0%
10%
20%
30%
40%
50%
60%
70%
Survival Good Neuro Outcome
Hypothermia Control
38
Induced Hypothermia (33º C) Bernard SA et al. N Engl J Med 2002; 346:557-63
• Australia • 73 Out-of-hospital ROSC patients • Cooled to 33ºC for 12 hours
0%
10%
20%
30%
40%
50%
60%
Survival
Hypothermia Control
39
Improved out-of-hospital cardiac arrest survival: the Wake County experience Ann Emerg Med. 2010 Oct;56(4):348-57
40

7/31/14
11
Current Research Has Painted a Different Picture
41
Prehospital Induction of Hypothermia in OOH-CA due to VF with 4ºC Ringers Lactate Bernard et. al. Circ 2010;122:737-42
• 234 Out-of-hospital ROSC patients • Cooling initiated immediately post-ROSC
• 2L of 4ºC Lactated Ringers • Cooled in ED to 33ºC for 24 hours • Study terminated early due to futility
0%
10%
20%
30%
40%
50%
60%
Survival
Cooled Not Cooled
42
The “Trials of Two Cities”
ROSC Cooling Temperature
Randomized Trial of Prehospital Induction of Hypothermia in OOH-CA with 4ºC Saline Kim et. al. JAMA. Epub 2013 Nov 17
• 1,359 Out-of-hospital ROSC patients • Grouped patients by presenting rhythm (VF or not)
• Cooling Initiated immediately post-ROSC • Cooled in ED to 32-34ºC for 24 hours
0%
10%
20%
30%
40%
50%
60%
70%
VF Not VF
Survival to Discharge
Cooled Not Cooled
44

7/31/14
12
Selective Brain Cooling: ‘RhinoChill’
• Non-invasive “preferential” brain cooling • Aerosolized coolant spray delivered through NC
• Very rapid cooling • Reaches target temperature of 34ºC two hours faster than
systemic cooling methods • Can be initiated early during arrest
45
PRINCE : Pre-ROSC IntraNasal Cooling Effectiveness Castren et al. Circulation 2010;122(7):729-36
• 194 Out-of-hospital cardiac arrest patients • 15 sites, 5 European countries
• RhinoChill Intranasal cooling initiated during arrest • Standard therapeutic hypothermia methods used
after hospital arrival 46
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
All CPR < 10 mins VF
Survival to Discharge
Control Rhinochill
This IS Working
47
Pit Crew Model:
� Same name…many versions � CPR
� Maximize compression fraction � Effective compression(rate/depth) � Provider fatigue
� Controlled ventilations � Defib
� Pre-charge @1:45 � Emphasis on Shock/Don’t’ shock

7/31/14
13
BLS &
ALS
Location
It’s a JUDGEMENT call
Termination of Efforts
30 minutes consider termination
You are a different kind of HERO

7/31/14
14
53
Effects of Permitting Family Members to Observe CPR Kristi L. Koenig, MD, FACEP, FIFEM reviewing Jabre P et al. Intensive Care Med 2014 May 23.
Despite data that suggest benefit to family members from allowing them to observe resuscitations (NEJM JW Emerg Med Mar 15 2013), emergency physicians may be reluctant to do so. In a prospective, cluster-randomized, controlled study involving 15 emergency medical services units in France, researchers compared psychological symptoms at 1 year between family members who were offered the chance to witness an adult resuscitation and those who were not offered the option. Of 570 family members, 72% were evaluated at 1 year by telephone. Family members in the control group were more likely to experience major depression (31% vs. 23%), complicated grief (36% vs. 21%), and post-traumatic stress disorder-related symptoms (adjusted odds ratio, 1.8). Grief, post-traumatic stress, and depression at 1 year were reduced when family members were permitted to witness resuscitation of loved ones.
Summary • Quality CPR is going to continue to be the foundation to
successful resuscitations • ACLS medications may not be as beneficial as
previously thought, and may even be detrimental to long term outcomes
• We must take a new focus on post resuscitation oxygenation and keep SaO2 between 94-99%
• The jury is still out on the utilization of pre-hospital Therapeutic Hypothermia
• Organized cardiac arrest care DOES lead to more survivors with a good CPC score
• Remember to keep an open mind to future changes!
54
Questions?
55