Embed Size (px)
Citation preview
Cardiac TestingPete Bell, MD
in collaboration with Julia Smith, FLMI

Cardiac Testing

Heart Anatomy

Who needs cardiac testing?
Clinically:
New onset of chest pain, dyspnea
Pre-operative evaluation
Elderly
Special occupation (pilot, police officer, bus driver)
In presence of known risk factors for heart disease
Known heart disease.

Who needs cardiac testing?
Underwriting--Applicants
Age and amount (ECG/ Treadmill for older ages/ higher face
amounts)
Abnormal resting ECG
History of heart disease

Cardiac Testing: pros and cons
Cardiac Test Pros ConsResting ECG Non-invasive/Easy/Portable
5-10 minLow sensitivity/Low specificity
Holter Monitor Evaluates arrhythmiaPainless/Non-invasive
Wear for a few daysCan’t take off/bathe
Exercise ECG aka Stress Test akaTreadmill test
Easy/AvailableDuration of exerciseInducible Changes
False positives
Nuclear Stress Testaka Perfusion
study aka SPECT akaThallium/Cardio
lite/Myoview
Often follows an abnormal resting ECG;
Good sensitivity/specificityEvaluates blood flow at
rest and at exercise
False Positives – chest wall attenuation
Invasive/radiationCostly
Stress Echo Often follows an abnormal stress test;
Anatomy/function before and after stress
Technical difficultiesIntra and Inter Observer Variation

Cardiac Testing: pros and consCardiac Test Pros Cons
M-mode Echo Non invasive/PortableAnatomy/Structure/
Function
More expensiveTechnical difficulties
2D/3D Echo Non invasive, Anatomy/Structure/Functi
on in fuller view, safe
Technical difficulties
Transesophageal Echo aka TEE
Clear, high quality, precise image, visualize LAE, clot,
mitral value and LV
More invasive/mild anesthesia
CT Angiography or heart scan
Detailed view of arteriesQuick (pictures in 5-10 sec)Non invasiveSubstitute for catheterization unless surgery contemplated
High dose radiation (equivalent to 600 CXRs)Expensive ($1000)Poor images when increased Ca deposit, obese patients or CKD
EBCTElectron beam computer
tomography, calcium scan
Non Invasive/painless/quickEarly atherosclerosis
Radiation, over sensitive$200-500 out of pocket
Catheterization The “gold standard”, CABG/Stent
Invasive, complications: bleeding, arterial damage
Labs (Troponin, cardiac enzymes, pro-BNP, C-
reactive protein)
Troponin very sensitive indicator of myocardial
damage, pro-BNP indicative of myocardial
disease
Pro-BNP has poor sensitivity and specificity, CRP non-
specific marker,

Does chest pain mean heart disease?
Common causes of chest pain: Angina due to coronary artery
disease, spasm, syndrome X Heart Attack Mitral Valve Prolapse Pericarditis Recent chest trauma Peptic Ulcer Aortic dissection Atypical chest wall pain Anxiety or panic disorder Asthma, bronchitis, pneumonia,
pleuritis Gastrointestinal
If chest pain is new onset, worsening, accompanied with chest tightness, dyspnea or risk factors associated with heart disease, then getting an ECG is the first step to evaluate.
If chest pain is chronic or recurrent, angina due to coronary artery disease is a possibility and treadmill testing is the first step
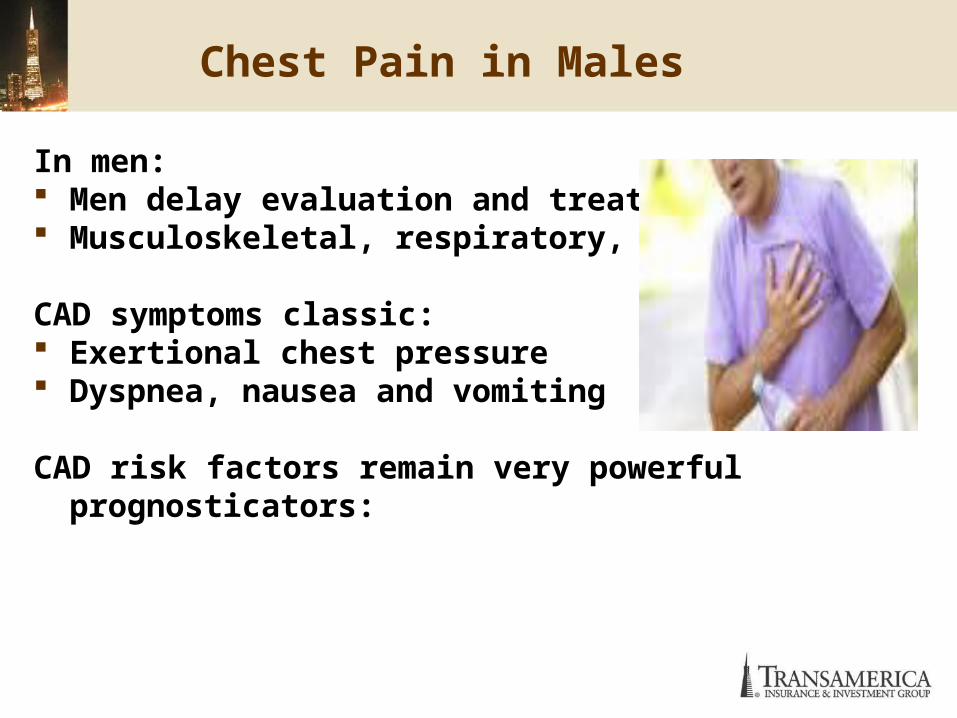
Chest Pain in Males
In men: Men delay evaluation and treatment. Musculoskeletal, respiratory, GI
CAD symptoms classic: Exertional chest pressure Dyspnea, nausea and vomiting
CAD risk factors remain very powerful prognosticators:

Chest Pain in Females
In women: Coronary artery disease onset is typically ten
years later than men Chest pain often due to other causes
– Mitral Valve Prolapse– Musculoskeletal, respiratory, gastro-
intestinal Symptoms of coronary artery disease may not
be classic:– Mid back pain– Nausea and vomiting
Risk factors for coronary artery disease remain very powerful prognosticators:

Risk Factors for Coronary Artery Disease
Tobacco exposure-includes cigarette/cigar smoking/chewing tobacco/secondhand cigarette smoke
Dyslipidemia Hypertension Diabetes Obesity Physical inactivity and low fitness Family history of cardiovascular disease in 1-st
degree relative < 55 years old in men < 65 years old in women

Medical Case #1
55 year old female, applying for 2.5 million of life insurance
Exam :BP 135/85, 5.5/145, no pertinent physical findings, family history negative for CAD
Labs: total cholesterol 217, HDL = 58, Ratio = 4.2 glucose 109, HOS WNL
Minor ST-T changes on ECGPresent History:– Sharp, fleeting (less than a minute) chest pain, onset 2
months ago– No shortness of breath, no palpitations.– Non-positional, stops spontaneouslyPast Medical History:– Mild osteoarthritis– Hypertension, treated x five years– Meds: Dyazide, Lisinopril and Aspirin as needed– Non-smoker

Probability of Disease

Medical case #1
Offer, postpone for additional testing?

ECG abnormalities
Major ST-T changes may give the appearance of ischemia
even if NO real ischemia is present.
Juvenile T Waves can be a normal variant-mostly seen in
young healthy females, persistently negative T wave
leads V1-V3, usually not deeply inverted.
Major T wave inversions – ischemia or LVH
Minor T wave changes potential causes: CAD * Obesity *
Electrolyte Imbalance-Hypokalemia * Hyperventilation *
Hypothyroid * Medication
Non specific ST changes are not diagnostic
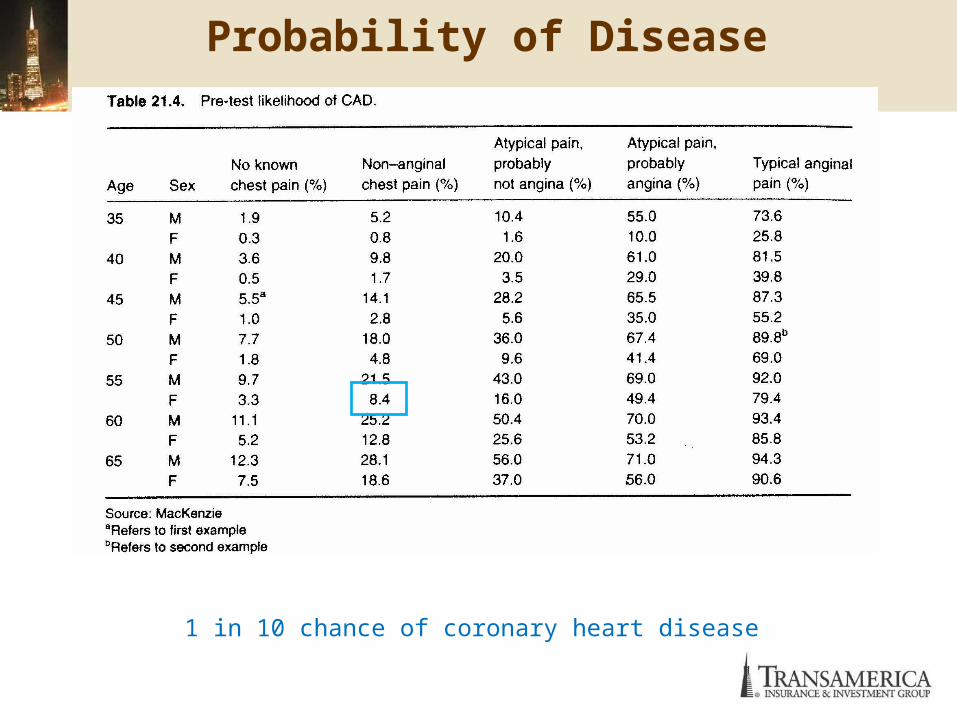
Probability of Disease
1 in 10 chance of coronary heart disease

Risk Assessment
Low risk for CAD

Medical case #2
Same applicant, 55 year old female, applying for 2.5 million of life
insurance
Same Minor T changes on insurance resting ECG.
Producer is concerned.
Medical Case #2
How to improve the offer?
Stress test?

Bruce Protocol
Stage Minutes % grade km/h MPH METS
1 3 10 2.7 1.7 4.7
2 6 12 4.0 2.5 7.0
3 9 14 5.4 3.4 10.1
4 12 16 6.7 4.2 12.9
5 15 18 8.0 5.0 15.0
6 18 20 8.8 5.5 16.9
7 21 22 9.6 6.0 19.1

METS and activity level
2-3 Walking at a slow pace ,Playing musical instrument, Dancing (slow), Golf using power cart, Bowling, Fishing4-5 Walking at a very brisk pace , Climbing stairs, Dancing (moderately fast), Bicycling <10 mph, leisurely, Slow swimming, Golf, carrying clubs6 Slow jogging (one mi/ 13 to 14 min) , Ice or roller skating, Doubles tennis (if you run a lot)6-8 Rowing, canoeing, kayaking vigorously, Dancing (vigorous), Some exercise apparatuses7-12 Singles tennis, squash, racquetball8 Jogging (1 mile every 12 min), Skiing downhill or cross country10 Running 6 mph (10-minute mile)13.5 Running 8 mph (7.5-minute mile)16 Running 10 mph (6-minute mile)

Poor prognostic findings on Stress Test
Low workload Mets <6.5 Time: < 5-6 minutes on Bruce protocol
Low peak Heart Rate Pulse < 120 without Beta-Blocker therapy
Systolic Blood Pressure decreased or flat response Remains under 130 mmHg
ST segment depression >2mm ST segment depression in multiple leads Prolonged ST depression after Exercise (>6 min) ST Elevation without abnormal Q wave Increase in complex ventricular ectopy Exercise induced typical Angina Frequent ventricular ectopy

Medical case #2
Same applicant, 65 year old female, applying for 2.5 million of life insurance Same Minor T changes on insurance resting ECG. How to reconsider the offer?
Minor ST changes on ECG=> Negative stress ECG Producer no longer concerned

Medical case #3
Same applicant, 55 year old female, applying for 2.5 million of life insurance Sharp, fleeting (less than a minute) chest
pain, onset 2 months ago no dyspnea or palpitations ECG with minor ST-T changes Standard treadmill test performed to
consider for improved offer, but it comes back with 1- 2 mm ST depression at 7 METS exercise.

Stress Test Tracing
Medical case #3
Minor ST changes on ECG=> Positive stress ECG
Now what?

Probability of Disease

Post-Test Probability
Post Test probability of disease is now 47%

Post-Test Decision
Flip a coin

Medical Case #2
Oh boy, what now?
Stress Echo?Perfusion Stress Test?

Stress test, Stress Echo, Nuclear stress
If the treadmill is equivocal or positive -- a stress perfusion treadmill or stress echocardiogram can be performed to investigate further.
If the workload on the follow up stress perfusion/echo is equal to or higher than that achieved on the original treadmill, then follow up stress perfusion/ echo results are considered valid.

Stress Echo
The echocardiogram is a cardiac ultrasound performed at rest
and after exercise.
It shows the structure of the heart valves chambers size and wall motion function wall thickness wall motion during exercise - abnormal may be indicative of ischemia.
Stress Echo

Nuclear stress
AKA - Perfusion study, Cardiolite study, Nuclear Test, Thallium
Study, Myocardial Perfusion Imaging (MPI), Stress SPECT. involves injecting a radioactive tracer into the bloodstream obtains images of the heart using a gamma camera. pictures are taken shortly after exercise and then after
resting for 2/3 hours
If the perfusion is normal during rest, but diminished following exercise, the results are consistent with a obstruction in one or more coronary arteries.
If the test shows reduced perfusion during both rest and exercise, then the blood flow is limited at all times and is consistent with a prior myocardial infarction
Stress Echo
6.0 minutes – stage II of Bruce protocol BP 173/98 Max HR = 159 7 METS Stopped because target heart rate achieved No chest pain or palpitations Echo showed no wall motion abnormalities, normal wall thickness,
chamber size and valves

Post-Test Probability
Post Test probability of disease is 10%

Risk Assessment
Low risk for CADHappy Producer
70 year old male, non smoker applying for $500,000, Term 5.6, 180 lbs 130/86, 140/80, 130/70 Ins labs 4/12 - Chol 171, ratio 3.4, HDL =
48. LDL 104 Meds – Vytorin, Lisinopril History of hypertension, hyperlipidemia,
OSA treated with CPAP Family history – non contributory
Medical case - #4

Medical case - #4
APS: 1/11/11 – Asymptomatic, resting ekg read as
previous inferior myocardial infarction 1/17/11 – treadmill to 10 METS, stopped due to
MPHR, no symptoms, normal BP response. NSSTW changes on tracings, SPECT scan => normal wall motion and thickness, mild inferior defect, can not exclude attenuation.
1/18/11 - Cath => 20 – 30% LM lesion, can not exclude catheter induced spasm, 30 – 40% mid – LAD lesion, 90% distal LAD lesion with collateral flow. MD notes “no significant CAD, continue with clinical treatment”

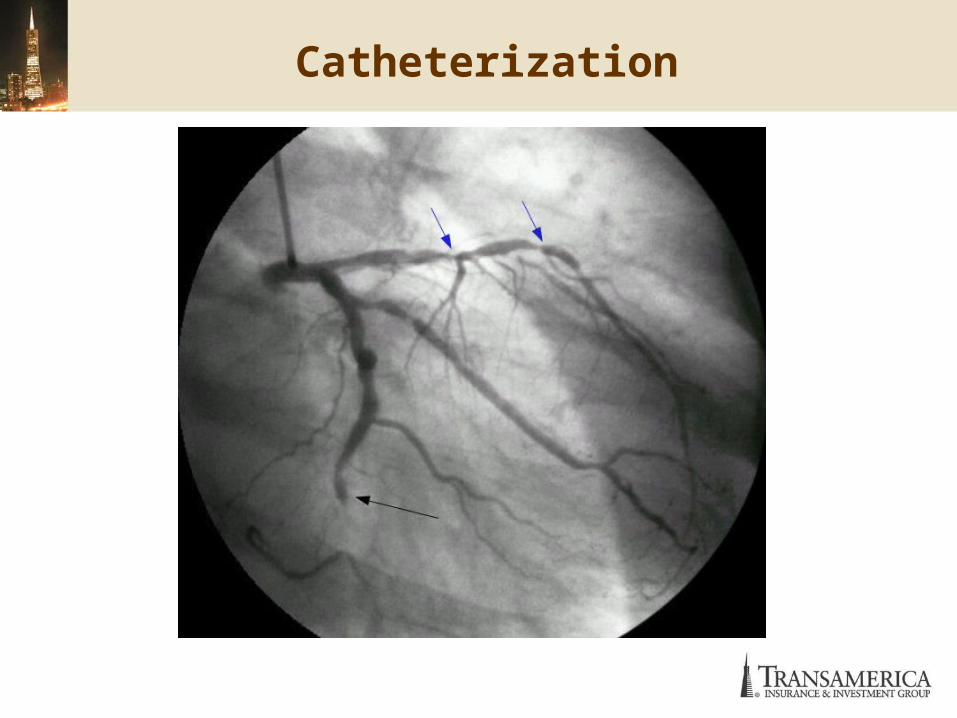
Cardiac Catheterization

Coronary Artery Catherization
Diagnostic gold standard. Invasive
Bleeding Arterial damage Infection
Also, can be therapeutic Stent Percutaneous Transluminal Coronary Angiography
Rate of progression Hard to predict Evidence of regression
Satins ACE inhibitor Exercise Favorable Factors

Coronary Artery Stenosis

CAD Significance
over 50% plaque obstruction coupled with typical angina symptoms at the bifurcation of 2 major (e.g.,LAD and Circumflex) or a
major and second-level (LAD and obtuse marginal ) vessel. 20 mm or greater in length in that it usually impedes flow
reserve regardless caliber. the report of “no flow-limiting lesions” has to be taken into
context with risk factors and symptoms. lesions < 50%, more significance for women than men, as
women are more prone to coronary artery spasm diffuse small lesions are fairly innocuous only in the elderly
or at any age if risk factors are meticulously controlled. lesions as they appear on cath are smaller when actually
seen, so the presence of symptoms are important to assess the significance.

Medical case - #4 - Solution
70 male with stable CAD per MD notes, good control of blood pressure and lipids.
The cath is equivocal for LM disease. Definite mid-LAD obstruction and a significant distal lesion. Assuming the reason there is no obstruction to blood flow is due to collateralization, as otherwise a lesion that size would obstruct proximal flow.
MD is continuing with clinical treatment only and doesn’t note CAD as significant.
Moderate risk of disease
Summary
Look at the likelihood of disease being present: Consider the history, symptoms and risk factors to develop a sense
of whether or not disease is present. And if so, what disease it is it?
Look at the studies: Does one appear better quality? Full versus sparse descriptions,
etc. A better quality testing labs? Referral center versus private office? What about the tests? One is very positive while the other may be
more ambiguous.
Draw a conclusion: No risk factors and the negative tests are more accurate, while the
positive tests are more likely false positive Many risk factors and the positive tests are more accurate, while
the negative tests are more likely to be false negative Consider the probability of disease being present. It may not be
what you think!

Questions