Embed Size (px)
Citation preview

Cardiology Rx for ChangeClinician-Assisted Tobacco Cessation
Funded by the Flight Attendant Medical Research Institute (FAMRI)

TRAINING OVERVIEW
Epidemiology of Tobacco Use Tobacco & Second-hand Smoke: CVD Risk Nicotine Addiction and Withdrawal Medications for Quitting Smoking Changing Behavior: How You Can Help

Ad campaigns from the 1950s featured physicians and assured the public that
cigarettes were safe.

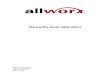
STATE-SPECIFIC PREVALENCE of SMOKING among ADULTS, 2007
Centers for Disease Control and Prevention. (2008). MMWR 58:221–226.
< 18.0%18.0 – 19.9%20.0 – 21.9%22.0 – 23.9%≥ 24.0%
Prevalence of current smoking (2007)

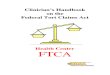
TRENDS in ADULT SMOKING, by SEX—U.S., 1955–2009
Trends in cigarette current smoking among persons aged 18 years or older
Graph provided by the Centers for Disease Control and Prevention. 1955 Current Population Survey; 1965–2009 NHIS. Estimates since 1992 include some-day smoking.
Per
cen
t
Male
Female 23.51%
17.9%
20.6% of adults are current smokers.
Year
70% want to quit

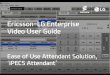
PREVALENCE of SMOKING by INSURANCE STATUSU.S. ADULTS AGED 18-64, 2007
17% Privately insured
33% Medicaid
26% Other
32% Uninsured
Centers for Disease Control and Prevention. (2007). MMWR 56:1157–1161.

FORMS of TOBACCO
Cigarettes are, by far, the most common form of tobacco used in the U.S.
Other forms of tobacco exist, and some are increasing in popularity.
All forms of tobacco are harmful.
Attention to all forms of tobacco is needed.

CIGARS: 1950–2007U.S. CONSUMPTION
Data from U.S.D.A. (2004 & 2007)
One cigar can deliver enough nicotine to establish and maintain dependence

TOBACCO and SECOND-HAND SMOKE: CARDIOVASCULAR DISEASE RISK

HEALTH CONSEQUENCES of SMOKING
Cancers Acute myeloid leukemia Bladder and kidney Cervical Esophageal Gastric Laryngeal Lung Oral cavity and pharyngeal Pancreatic
Pulmonary diseases Acute (e.g., pneumonia) Chronic (e.g., COPD) Tuberculosis
Cardiovascular diseases Abdominal aortic aneurysm Coronary heart disease Cerebrovascular disease Peripheral arterial disease Sudden death Heart failure
Reproductive effects Reduced fertility in women Poor pregnancy outcomes Infant mortality
Other effects: type 2 diabetes, peptic ulcer, cataract, osteoporosis, periodontitis, poor surgical outcomes (occlusion of bypass grafts & stents)
USDHHS. (2004). The Health Consequences of Smoking: A Report of the Surgeon General.

USDHHS. (2006). The Health Consequences of Involuntary Exposure to Tobacco Smoke: Report of the Surgeon General.
There is no safe level of second-hand
smoke.
Second-hand smoke (SHS) causes premature death and disease in nonsmokers: Immediate adverse effects on the
cardiovascular system Increased risk for coronary heart disease
and lung cancer
2006 REPORT of the SURGEON GENERAL: INVOLUNTARY EXPOSURE to TOBACCO SMOKE

ANNUAL U.S. DEATHS ATTRIBUTABLE to TOBACCO USE & SHS, 2000-2004
Centers for Disease Control and Prevention. (2008). MMWR 57:1226–1228.
32%
29%
21%
8%
10%
Cardiovascular diseases are the #1 cause of death among smokers.
Cardiovascular diseases
141,900
Lung cancer 128,900
Respiratory diseases 92,900
Cancers other than lung
35,300
Other 44,000
Total deaths annually: 443,000
Percentage of all smoking-attributable deaths*
* In 2005, it was estimated that nearly 50,000 persons died due to SHS exposure.

BRITISH MALE DOCTORS’
STUDY
On average, cigarette smokers die about 10 years younger than do
nonsmokers.
At least half of chronic smokers will die due to a tobacco-related disease.
Doll et al. (2004). BMJ 328(7455):1519–1527.
Prospective study of 34,439 male doctors studied from 1951 to
2001

EFFECTS of SMOKING & SHS on the CARDIOVASCULAR SYSTEM
Platelet activation Endothelial
dysfunction Inflammation &
infection Atherosclerosis
Low HDL levels Platelet instability Increased oxidized
LDL Increased oxidation
stress Decreased energy
metabolism
Increased insulin resistance
Outcome measures Increased infarct
size Decreased heart
rate variability Increased arterial
stiffness Increased risk of
coronary disease events
Barnoya & Glantz. (2005). Circulation111:2684-2698

META-ANALYSIS of CHD RISK DUE to CHRONIC SHS among NEVER-SMOKERS
Overall RR = 1.78 for active smokers
Overall RR = 1.31 for passive nonsmokers 1
1.2
1.4
1.6
1.8
2
NeverSmoker
SHSNever
Smoker
ActiveSmoker
Barnoya & Glantz. (2005). Circulation111:2684–2698.
Long-term SHS exposure in the work or home is associated with a 30% increased risk for CHD in adult nonsmokers.
Rel
ativ
e ri
sk
N = 29 studies

Copyright ©2004 BMJ Publishing Group Ltd.
Whincup et al. (2004). BMJ 329:200-205.
"Light passive" refers to the lowest quarter of cotinine concentration among nonsmokers(0-0.7 ng/ml), "heavy passive" to the upper three-quarters of cotinine concentration combined
(0.8-14.0 ng/ml), "light active" to men smoking 1-9 cigarettes a day.
PROPORTION of MEN with MAJOR CHD by YEARS of FOLLOW-UP: LIGHT ACTIVE, HEAVY PASSIVE, LIGHT PASSIVE

After the last cigarette…< 30 min
8 hr
24 hr
48 hr
72 hr
2-12 weeks
1 year
3 years
5-15 years
Blood pressure and pulse return to normal
O2 and CO levels in blood return to normal
Chance of heart attack decreases
Nerve endings begin regrowth
Breathing becomes easier; lung capacity increases
Lung function increases 30%; circulation improves
Risk of CHD is half that of a smoker
MI risk is similar to that of never-smokers
Stroke risk reduced to that of never-smokers

Standard treatments reduce the risk of death in patients with CVD by 15–35% Aspirin = 15% Beta blockers = 23% ACE inhibitors = 23% Statins = 29–35%
Smoking cessation reduces the risk of death by 36% and reduces the risk of future cardiac events by 50%
TOBACCO CESSATION as TREATMENT for CVD

SUMMARY: REASONS to ADDRESS TOBACCO in CARDIOLOGY
Smoking and SHS act synergistically with other CVD risk factors
Smoking increases risk for surgical complications
Quitting smoking improves survival Quitting smoking improves quality of life Quitting reduces risk of future CVD events
TOBACCO CESSATION is an essential component of prevention and treatment for CVD.

NICOTINE ADDICTION and WITHDRAWAL

NICOTINE DISTRIBUTION
Henningfield et al. (1993). Drug Alcohol Depend 33:23–29.
0
10
20
30
40
50
60
70
80
0 1 2 3 4 5 6 7 8 9 10
Minutes after light-up of cigarette
Pla
sma n
icoti
ne (
ng/m
l) Arterial
Venous
Nicotine reaches the brain within 11 seconds.

Nicotine enters brain
Stimulation of nicotine receptors
Dopamine release
DOPAMINE REWARD PATHWAYPrefrontal
cortex
Nucleus accumbens
Ventral tegmental
area

NEUROCHEMICAL and RELATED EFFECTS of NICOTINE
Dopamine
Norepinephrine
Acetylcholine
Glutamate
Serotonin
-Endorphin
GABA
N
I
C
O
T
I
N
E
Pleasure, appetite suppression
Arousal, appetite suppression
Arousal, cognitive enhancement
Learning, memory enhancement
Mood modulation, appetite suppression
Reduction of anxiety and tension
Reduction of anxiety and tension
Benowitz. (2008). Clin Pharmacol Ther 83:531–541.

Irritability/frustration/anger Anxiety Difficulty concentrating Restlessness/impatience Depressed mood/depression Insomnia Impaired performance Increased appetite/weight gain Cravings
NICOTINE PHARMACODYNAMICS: WITHDRAWAL EFFECTS
Hughes. (2007). Nicotine Tob Res 9:315–327.
Most symptoms manifest within the first 1–2 days, peak
within the first week, and subside within 2–
4 weeks.
HANDOUT

NICOTINE ADDICTION CYCLE
Reprinted with permission. Benowitz. (1992). Med Clin N Am 2:415–437.

TOBACCO DEPENDENCE:A 2-PART PROBLEM
Tobacco Dependence
Treatment should address the physiologic and the behavioral
aspects of dependence.
Physiologic Behavioral
Treatment Treatment
The addiction to nicotine
Medications for cessation
The habit of using tobacco
Behavior change program

MEDICATIONS for QUITTING SMOKING

PHARMACOLOGIC METHODS
First-line (FDA approved) Nicotine replacement therapy (NRT) Bupropion SR (Zyban) Varenicline (Chantix)
Second-line (evidence based but not FDA approved) Nortriptyline Clonidine

PLASMA NICOTINE CONCENTRATIONS for NICOTINE-CONTAINING PRODUCTS
0
5
10
15
20
25
1/0/1900 1/10/1900 1/20/1900 1/30/1900 2/9/1900 2/19/1900 2/29/1900
Pla
sma
nic
oti
ne
(mcg
/l)
Cigarette
Moist snuff
Nasal spray
Inhaler
Lozenge (2mg)
Gum (2mg)
Patch
0 10 20 30 40 50 60
Time (minutes)
Cigarette
Moist snuff

NRT: PRECAUTIONS
Patients with underlying CVD: Recent MI (within past 2 weeks) Serious arrhythmias Serious or worsening angina
NRT may be appropriate for these patients if they are under medical supervision
Experts believe the risks of NRT in heart patients are small in relation to the risks of continued tobacco use.

TRANSDERMAL NICOTINE PATCH
DISADVANTAGES Patients cannot titrate
the dose Allergic reactions to
adhesive may occur Vivid/disturbing dreams
may occur with nocturnal patch use (can remove before sleep)
ADVANTAGES The patch
provides consistent nicotine levels
The patch is easy to use and conceal
Fewer compliance issues are associated with the patch

PATIENT EDUCATION :Nicotine Patch
Apply patch to hairless area—new location daily
Water will not harm the nicotine patch if it is applied correctly; patients may bathe, swim, shower, or exercise while wearing the patch
Do not cut patches to adjust dose Nicotine may evaporate from cut edges Patch may be less effective
Keep new and used patches out of the reach of children and pets

NICOTINE GUM & LOZENGE
DISADVANTAGES Gastrointestinal side
effects may be bothersome
Gum may be socially unacceptable and difficult to use with dentures
Patients must use proper chewing technique to minimize adverse effects
ADVANTAGES Patients can titrate
therapy to manage withdrawal symptoms
May satisfy oral cravings
May delay weight gain

NICOTINE GUM:
CHEWING TECHNIQUE SUMMARY
Park between cheek & gum
Stop chewing at first sign of peppery taste or tingling sensation
Chew slowly
Chew again when peppery taste or tingle fades
Do not eat or drink 15 min before or
after use.

NICOTINE INHALERDISADVANTAGES
Initial throat or mouth irritation can be bothersome
Cartridges should not be stored in very warm conditions or used in very cold conditions
Patients with underlying bronchospastic disease must use the inhaler with caution
ADVANTAGES Patients can easily
titrate therapy to manage withdrawal symptoms
The inhaler mimics hand-to-mouth ritual of smoking

NICOTINE NASAL SPRAY
DISADVANTAGES Nasal/throat
irritation may be bothersome
Dependence can result*
Patients must wait 5 min before driving or operating heavy machinery
* The data on higher dependence are not definitive and are based on small trials.
ADVANTAGES Most rapidly
absorbed form of nicotine replacement
Patients can easily titrate therapy to rapidly manage withdrawal symptoms

BUPROPION SRDISADVANTAGES Should be avoided in
patients with an increased risk for seizures
Side effects:Common: dry mouth, anxiety, insomnia (avoid bedtime dosing)
Less common: tremor, skin rash
ADVANTAGES Easy to use Can be used with
NRT or varenicline May delay cessation-
related weight gain May be beneficial in
patients with coexisting depression

BUPROPION: CONTRAINDICATIONS and PRECAUTIONS
History of seizure Current or prior eating disorder History of cranial trauma, stroke, or neurosurgical
intervention Treatment with medications that lower the seizure
threshold (e.g., antipsychotics, antidepressants, theophylline)
Treatment with MAOIs in the past 2 weeks Abrupt discontinuation of alcohol or sedatives
(including benzodiazepines) Severe hepatic cirrhosis

BUPROPION:MECHANISM OF ACTION
Atypical antidepressant thought to affect levels of various brain neurotransmitters Dopamine
Norepinephrine
Clinical effects craving for cigarettes
symptoms of nicotine withdrawal

BUPROPION SR: DOSING for SMOKING CESSATION
Initial treatment 150 mg po q AM x 3 days
Then, if tolerated… 150 mg po bid x 7–12 weeks
If 300 mg is not well tolerated… Reduce dose to 150 mg and reassure that
150 mg dose is still efficacious (Swan et al., 2003)
Patients should begin therapy one week PRIOR to quitting to assure therapeutic plasma levels
of drug are achieved when patient is no longer
smoking.

BUPROPION: ADDITIONAL PATIENT EDUCATION
Can be safely used with NRT or varenicline Dose tapering is not necessary when
discontinuing treatment If no significant progress toward abstinence
by 7th week, therapy is unlikely to be effective Discontinue treatment Reevaluate and restart at later date
FDA boxed warning added in July 2009

VARENICLINE
DISADVANTAGES Common side effects:
Nausea (in up to 33% of patients)
Sleep disturbances (insomnia, abnormal dreams)
Constipation Flatulence Vomiting
ADVANTAGES Oral formulation with
twice-a-day dosing Offers a new
mechanism of action for persons who previously failed using other medications
Early industry-sponsored trials suggest this agent is superior to bupropion SR

VARENICLINE:MECHANISM of ACTION
Binds with high affinity and selectivity at 42 neuronal nicotinic acetylcholine receptors Stimulates low-level agonist activity
Competitively inhibits binding of nicotine
Clinical effects symptoms of nicotine withdrawal
Blocks dopaminergic stimulation responsible for reinforcement & reward associated with smoking

VARENICLINE: DOSINGPatients should begin therapy 1 week PRIOR to
theirquit date. The dose is increased gradually to
minimize treatment-related nausea and insomnia.Treatment Day Dose
Days 1–3 0.5 mg qd
Days 4–7 0.5 mg bid
Day 8 – week 12 1 mg bid
Initial dose titration

VARENICLINE: ADDITIONAL PATIENT EDUCATION
Do not combine with NRT—increase in side effects, including nausea, headache, vomiting, fatigue
Doses should be taken after eating, with a full glass of water
Nausea and insomnia are side effects that are usually temporary
Dose tapering is not necessary when discontinuing treatment

FDA BOXED WARNINGS
On July 1, 2009, varenicline and bupropion received Boxed Warnings concerning the risk of serious neuropsychiatric symptoms:
Patients should be advised to stop taking varenicline or bupropion and to contact a health-care provider immediately if they experience agitation, depressed mood, and any changes in behavior that are not typical of nicotine withdrawal, or if they experience suicidal thoughts or behavior.

VARENICLINE USE in PATIENTS with CVD: EFFICACY & SAFETY
Study of 714 patients with stable, documented CVD (other than hypertension alone) diagnosed for > 2 months 51% angina, 49% MI, 49% coronary
revascularization Randomized to 12 weeks varenicline or
placebo Monitored over 52 weeks Multisite trial funded by Pfizer, Inc.
Rigotti et al. (2010). Circulation; 121:221-9.

CONTINUOUS ABSTINENCE RATES: VARENICLINE vs. PLACEBO
Rigotti et al. (2010). Circulation; 121:221-9.

VARENICLINE: ADVERSE EVENTS
Most frequent events in the varenicline group: Nausea (30%), headache (13%), insomnia (12%),
vomiting (8%), and abnormal dreams (8%) 9.6% stopped the drug because of an adverse
event; compared to 4.3% receiving placebo
Serious adverse events occurred in 6.5% of participants in the varenicline group and 6.0% in the placebo group
No reported depression, suicidality, or abnormal behavior

LONG-TERM (6 month) QUIT RATES for AVAILABLE CESSATION MEDICATIONS
0
5
10
15
20
25
30
Nicotine gum Nicotinepatch
Nicotinelozenge
Nicotinenasal spray
Nicotineinhaler
Bupropion Varenicline
Active drugPlacebo
Data adapted from Cahill et al. (2008). Cochrane Database Syst Rev; Stead et al. (2008). Cochrane Database Syst Rev; Hughes et al. (2007). Cochrane Database Syst Rev.
Per
cen
t q
uit 18.0
15.8
11.3
9.9
16.1
8.1
23.9
11.8
17.1
9.1
19.0
10.3 11.2
20.2

Varenicline vs. NRT
Aubin et al. (2008). Thorax 63:717-724.
OR = 1.40 (95% CI = 0.99–1.99)
Pe
rce
nt q
uit
smok
ing

COMBINATION PHARMACOTHERAPY
Combination NRT
Long-acting formulation (patch)
Produces relatively constant levels of nicotine
PLUS
Short-acting formulation (gum, inhaler, nasal spray)
Allows for acute dose titration as needed for nicotine withdrawal symptoms
Bupropion SR + Nicotine Patch
Regimens with enough evidence to be “recommended” first-line

EXTENDED TREATMENTS
STANDARD TREATMENT (ST)12 weeks: group counseling, NRT, and bupropion
EXTENDED CBT (E-CBT)ST + 11 individual CBT sessions over 40 weeks
EXTENDED NRT (E-NRT)ST + 40 weeks of nicotine gum availability
EXTENDED CBT+ NRTE-CBT + 40 weeks NRT
N = 402 older adult smokers (50+ yrs old), motivated to quit, 10+ cpd at baseline
Hall et al. (2009). Addiction 104:1043-1052.

TREATMENT TIMELINES
Bupropion
NRT
NRT + BUPR
Varenicline
Clinical contacts
QUIT DATE
1 WEEK PRIOR 12 WEEKS POST 150 mg 300 mg
Patch and consider prn gum/lozenge
0.5 mg qd 0.5 mg bid 1 mg bid
150 mg 300 mg Patch and consider prn gum/lozenge

$0
$1
$2
$3
$4
$5
$6
$7
$8
Trade $6.58 $5.26 $3.89 $5.29 $3.72 $7.40 $4.75
Generic $3.28 $3.66 $1.90 - - $3.62 -
Gum Lozenge Patch Inhaler Nasal sprayBupropion
SRVarenicline
COMPARATIVE DAILY COSTS of PHARMACOTHERAPY
$/d
ay
Average cost/pack of cigarettes, $4.32

MEDICARE COVERAGE
Medicare Part D covers cessation medications prescribed by a physician; OTC products not covered
Affordable Care Act: any Medicare beneficiary who smokes will be able to receive counseling from a "qualified physician or other Medicare-recognized practitioner" who can help them quit smoking 4 sessions per quit attempt Up to 2 covered quit attempts per year

TOBACCO DEPENDENCE:A 2-PART PROBLEM
Tobacco Dependence
Treatment should address the physiologic and the behavioral
aspects of dependence.
Physiological Behavioral
Treatment Treatment
The addiction to nicotine
Medications for cessation
The habit of using tobacco
Behavior change program

Changing Behavior:How You Can Help
HANDOUT

TOBACCO CESSATION REQUIRES BEHAVIOR CHANGE
Fewer than 5% of people who quit without assistance are successful in quitting for more than a year
Many patients underestimate the impact that counseling can have on their ability to quit
Few patients adequately PREPARE and PLAN for their quit attempt
Many patients assume they can just “make themselves quit” when they are ready to do soBehavioral counseling is a key component of treatment
for tobacco use and dependence.

0
10
20
30
No clinician Self-helpmaterial
Nonphysicianclinician
Physicianclinician
Type of Clinician
Est
imate
d a
bst
inence
at
5+
month
s
1.0 1.11.7
2.2
N = 29 studies
Fiore et al. (2008). Treating Tobacco Use and Dependence: 2008 Update.
With help from a clinician, the odds of quitting approximately double.
Compared to patients who receive no assistance from a clinician, patients who receive assistance are 1.7–2.2 times as likely to quit successfully for 5 or more months.
CLINICIAN ADVICE MAKES a DIFFERENCE

Esti
mate
d a
bsti
nen
ce
rate
at
5+
mon
ths
0
10
20
30
None One Two Three or more
Number of Clinician Types
1.0
1.8(1.5-2.2)
2.5(1.9-3.4)
2.4(2.1-3.4)
N = 37 studies
The NUMBER of CLINICIANS CAN MAKE a DIFFERENCE, TOO
Compared to smokers who receive assistance from no clinicians, smokers who receive assistance from two or more clinicians are 2.4–2.5 times as likely to quit successfully for 5 or more months.
Fiore et al. (2008). Treating Tobacco Use and Dependence: 2008 Update.

The 5 A’s
ASK about tobacco USE
ADVISE tobacco users to QUIT
ASSESS READINESS to make a quit attempt
ASSIST with the QUIT ATTEMPT
ARRANGE FOLLOW-UP care
HANDOUT

Ask about tobacco use “Do you, or does anyone in your household, ever
smoke or use any type of tobacco?”
“We ask all of our patients about tobacco use and secondhand smoke exposure, because it is so important for good cardiovascular health.”
ASK
STEP 1: ASK

tobacco users to quit “Quitting tobacco is a critical component of your
care.”
“Quitting smoking is the best thing you can for your heart.”
“Patients who continue to smoke after a heart attack have lower survival than patients who quit smoking.”
“It will be important for your family and close friends to either quit with you or be supportive of your quitting.”
“Creating a smoke-free environment at home is critical to your heart health and success with quitting smoking.”
ADVISE
STEP 2: ADVISE

STEP 3: ASSESS
readiness to quit Ask every tobacco user if s/he is willing to quit at this
time.
If willing to quit, provide resources and assistance See STEP 4, ASSIST
If NOT willing to quit at this time, provide resources and enhance motivation. Ask three questions:
“Do you ever plan to quit?” [If yes, continue with…] “How will it benefit you to quit later, as opposed to
now?” “What is the worst thing that could happen if you were
to quit tomorrow?”
ASSESS

STEP 4: ASSIST
tobacco users with a quit plan Discuss reasons for quitting and benefits of quitting
Review past quit attempts—what helped, what led to relapse
Discuss support from family, friends, and coworkers
Set a quit date—within 2 weeks
Encourage use of pharmacotherapy when not contraindicated
Anticipate challenges, particularly during the first few weeks Nicotine withdrawal, stress-related smoking, etc.
ASSIST

STEP 5: ARRANGE
follow-up care Status of attempt
Ask about support from friends, family, coworkers Identify ongoing temptations and triggers for relapse
(stress, negative affect, smokers, eating, alcohol, cravings)
Slips and relapse Has the patient used tobacco at all—even a puff?
Cessation medication compliance, plans for termination
Is the regimen being followed? Are withdrawal symptoms being alleviated?
ARRANGE
PROVIDE ASSISTANCE THROUGHOUT THE QUIT ATTEMPT.

RELAPSE in PATIENTS with CARDIOVASCULAR DISEASE
Less than half of patients will be tobacco free 6 months following an MI hospitalization
Predictors of relapse: Not receiving a discharge recommendation
for cardiac rehabilitation (OR = 1.80) Depressive symptoms during hospitalization
(OR = 1.75) Treating hospital does not have a smoking
cessation program (OR = 1.71)Dawood et al. (2008). Arch Intern Med 168:1961-1967.

patients to other resources: A doctor, nurse, pharmacist, or other clinician, for
additional counseling Local program: [insert your med center’s
program] The support program provided free with each smoking
cessation medication Web sites like smokefree.gov or quitnet.org The toll-free national quit line: 1-800-QUIT-NOW
REFER
IN the ABSENCE of TIME or EXPERTISE: REFER

REFERRAL to a TOLL-FREE TELEPHONE QUIT LINE
Referring patients to a toll-free quit line is simple and easily integrated into routine patient care
Quit line callers receive one-on-one coaching from trained counselors
Follow-up counseling is provided Quit lines are effective and are provided at no cost to
the caller
1-800-QUIT-NOW

TREATING TOBACCO DEPENDENCE in HOSPITALIZED CVD PATIENTS
• Meta-analysis: 11 RCTs (N = 2,751), 1990–2007
• Quit rates: intervention (42%) vs. usual care (34%)
• Greater quit rates: • > 6 interactions: OR = 1.67• Greater duration & intensity: OR = 3.17• Concurrent use of NRT or bupropion: OR =
2.13Behavioral smoking cessation interventions initiated during hospitalization result in a significantly higher
quit rate compared to usual smoking cessation advice. Aziz et al. (2009). Int J Cardiology.

TOBACCO CESSATION TREATMENT in PATIENTS with CHD
• Meta-analysis: 16 RCTs (N = 2,677), 1974–2003
• Positive treatment effect at 6–12 mos: OR = 1.66• Brief interventions: OR = 0.92 (not significant)• Telephone support: OR = 1.58• Self-help: OR = 1.48• Behavioral therapies: OR = 1.69• Intense interventions (follow-up after 1 month): OR = 1.98
Behavioral smoking cessation interventions in patients with CHD are effective in promoting abstinence at
1 year, provided they are of sufficient duration.Barth et al. (2008). Cochrane Reviews.

Mills et al. (2009). Nicotine Tob Res.
SMOKE-FREE HOMES SUPPORT TOBACCO CESSATION
Prevalence of smoke-free homes has been increasing over time
Review of 16 longitudinal and 7 cross-sectional studies: Smokers with smoke-free home were
significantly more likely to make a quit attempt and be abstinent

THE CARDIOLOGY TEAM’s RESPONSIBILITY
The cardiology team has a professional obligation
to address tobacco use and can have an important role in helping patients with
CVD, and their family members,plan for their quit attempts.
TOBACCO CESSATION is an essential component of CVD TREATMENT
for ALL PATIENTS who use tobacco.

TOBACCO TREATMENTS with DEMONSTRATED EFFICACY
Physician advice Formal smoking cessation programs
Individual counseling Web and telephone counseling:
www.smokefree.gov 1-800-QUIT-NOW (national toll-free quit line)
Group programs Aversion therapy NRT, bupropion, varenicline, Nortriptyline, clonidine

TOBACCO TREATMENTS LACKING EVIDENCE of EFFICACY
SSRIs and SNRI
Anxiolytics: Sedative, hypnotics,
buspirone
Homeopathic treatments
Hypnotherapy
Herbal supplements
Lobeline
Massage therapy
Acupuncture
Laser therapy
Nicotine Anonymous

SET REALISTIC EXPECTATIONS
It’s a learning process. Reframe success! Most people make
multiple quit attempts before they are successful.
Longer prior quit attempts predict future success.Hall et al. (2009). Addiction, 104:1043-1052.

Address tobacco use with all patients.
At a minimum, commit to incorporating brief tobacco interventions as part of routine patient care:
Ask, Advise, and Refer.
Become an advocate for smoke-free hospitals and clinics, workplaces, and public places.
MAKE a COMMITMENT…