Embed Size (px)
Citation preview
Cardiothoracic Surgery | Outcomes 2007
Outcomes 2007 Thoracic and Cardiovascular Surgery
The Department of Thoracic and Cardiovascular Surgery is pleased to present our annual edition of Outcomes. This is the second published version of cardiothoracic surgical results of The Chester County Hospital, relating our outcomes to national standards established by The Society of Thoracic Surgeons.
The outcomes reported here are the result of the collaborative efforts of cardiothoracic surgeons, cardiologists, cardiac anesthesiologists, vascular surgeons, and cardiovascular radiologists. In the future, treating patients with cardiovascular disease will become ever more complex and exciting as new surgical techniques and technologies emerge. Maintaining a high level of care for our patients will require maintaining a high level of collaboration between The Chester County Hospital, our Cleveland Clinic main campus, and our cardiothoracic colleagues nationally and internationally.
We hope that you will find this information helpful and thought provoking.
Bruce W. Lytle, M.D.Chairman,Department of Thoracic and Cardiovascular Surgery
Outcomes 2007 Thoracic and Cardiovascular Surgery3
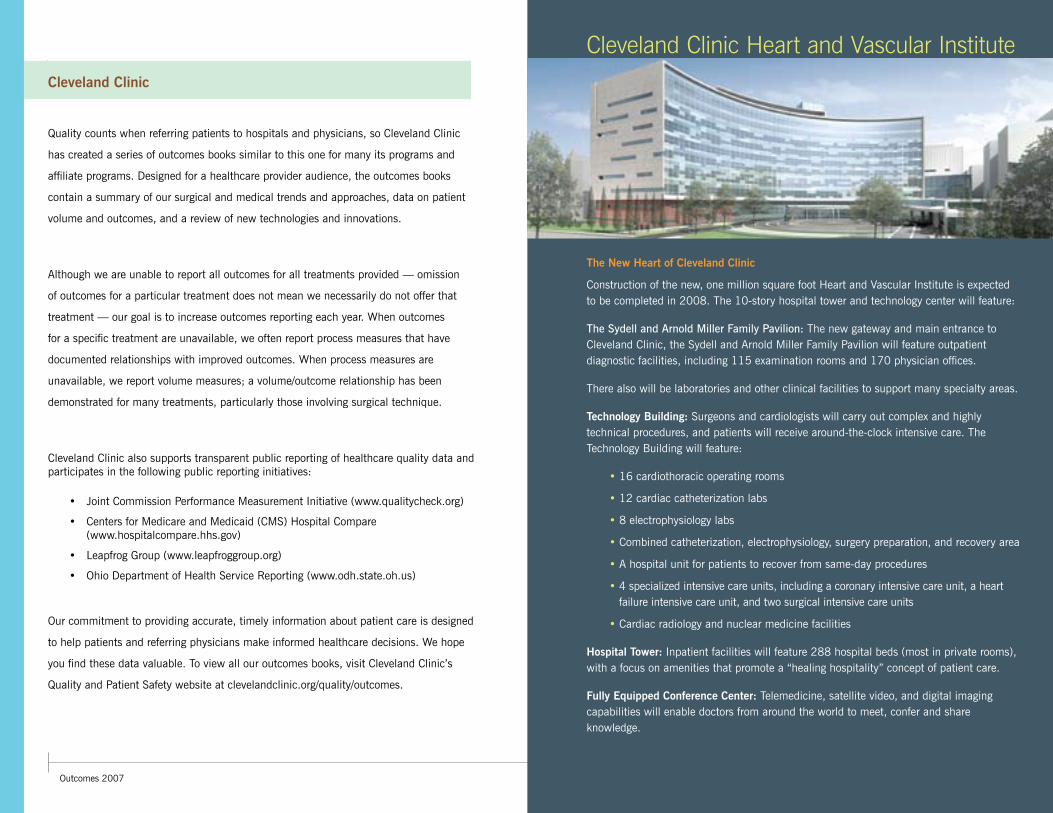
Cleveland Clinic Heart and Vascular Institute
The New Heart of Cleveland Clinic
Construction of the new, one million square foot Heart and Vascular Institute is expected to be completed in 2008. The 10-story hospital tower and technology center will feature:
The Sydell and Arnold Miller Family Pavilion: The new gateway and main entrance to Cleveland Clinic, the Sydell and Arnold Miller Family Pavilion will feature outpatient diagnostic facilities, including 115 examination rooms and 170 physician offices.
There also will be laboratories and other clinical facilities to support many specialty areas.
Technology Building: Surgeons and cardiologists will carry out complex and highly technical procedures, and patients will receive around-the-clock intensive care. The Technology Building will feature:
• 16 cardiothoracic operating rooms
• 12 cardiac catheterization labs
• 8 electrophysiology labs
• Combined catheterization, electrophysiology, surgery preparation, and recovery area
• A hospital unit for patients to recover from same-day procedures
• 4 specialized intensive care units, including a coronary intensive care unit, a heart failure intensive care unit, and two surgical intensive care units
• Cardiac radiology and nuclear medicine facilities
Hospital Tower: Inpatient facilities will feature 288 hospital beds (most in private rooms), with a focus on amenities that promote a “healing hospitality” concept of patient care.
Fully Equipped Conference Center: Telemedicine, satellite video, and digital imaging capabilities will enable doctors from around the world to meet, confer and share knowledge.
Quality counts when referring patients to hospitals and physicians, so Cleveland Clinic
has created a series of outcomes books similar to this one for many its programs and
affiliate programs. Designed for a healthcare provider audience, the outcomes books
contain a summary of our surgical and medical trends and approaches, data on patient
volume and outcomes, and a review of new technologies and innovations.
Although we are unable to report all outcomes for all treatments provided — omission
of outcomes for a particular treatment does not mean we necessarily do not offer that
treatment — our goal is to increase outcomes reporting each year. When outcomes
for a specific treatment are unavailable, we often report process measures that have
documented relationships with improved outcomes. When process measures are
unavailable, we report volume measures; a volume/outcome relationship has been
demonstrated for many treatments, particularly those involving surgical technique.
Cleveland Clinic also supports transparent public reporting of healthcare quality data and participates in the following public reporting initiatives:
• Joint Commission Performance Measurement Initiative (www.qualitycheck.org)
• Centers for Medicare and Medicaid (CMS) Hospital Compare (www.hospitalcompare.hhs.gov)
• Leapfrog Group (www.leapfroggroup.org)
• Ohio Department of Health Service Reporting (www.odh.state.oh.us)
Our commitment to providing accurate, timely information about patient care is designed
to help patients and referring physicians make informed healthcare decisions. We hope
you find these data valuable. To view all our outcomes books, visit Cleveland Clinic’s
Quality and Patient Safety website at clevelandclinic.org/quality/outcomes.
Cleveland Clinic
Thoracic and Cardiovascular SurgeryOutcomes 2007
what’s insideOverview 6
Coronary Disease 10
Valve Surgery 14
Thoracic Surgery 15
Innovation 16
Staff Biographies 20
Contact Information 21
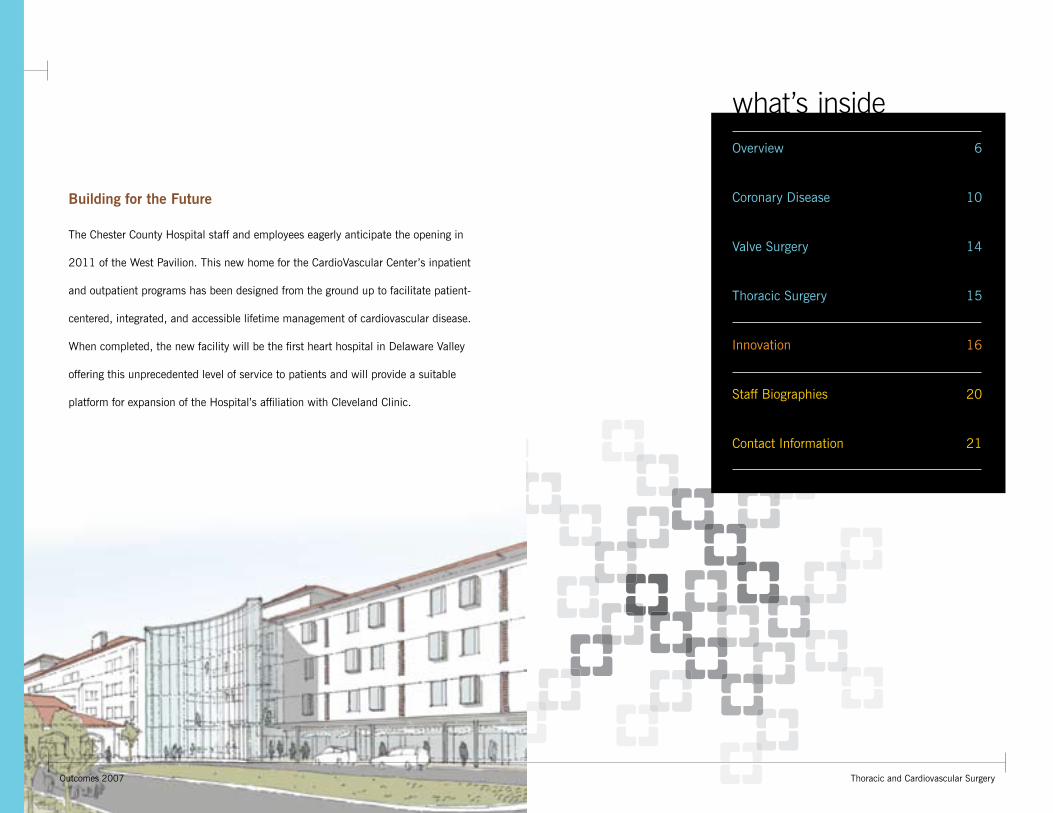
Building for the Future
The Chester County Hospital staff and employees eagerly anticipate the opening in
2011 of the West Pavilion. This new home for the CardioVascular Center’s inpatient
and outpatient programs has been designed from the ground up to facilitate patient-
centered, integrated, and accessible lifetime management of cardiovascular disease.
When completed, the new facility will be the first heart hospital in Delaware Valley
offering this unprecedented level of service to patients and will provide a suitable
platform for expansion of the Hospital’s affiliation with Cleveland Clinic.
6Outcomes 2007 Thoracic and Cardiovascular Surgery7
Overview
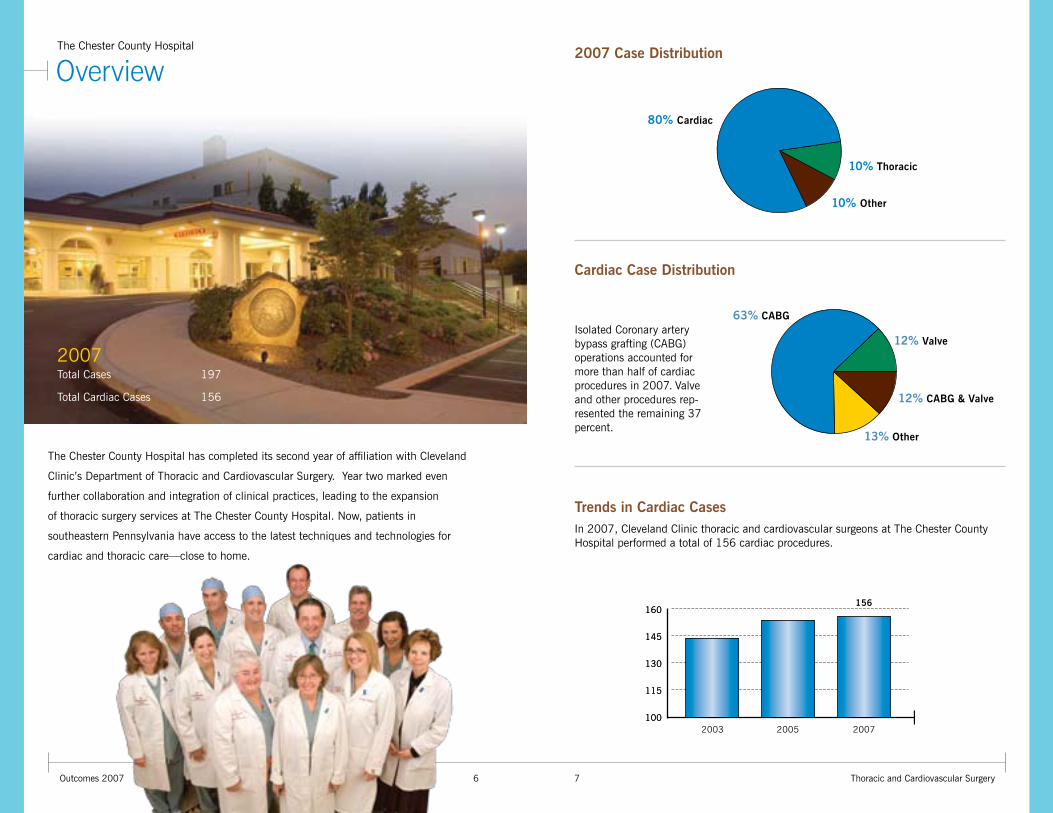
2007 Total Cases 197
Total Cardiac Cases 156
2003 2005 2007
156160160
145145
130130
115115
100100
2007 Case Distribution
Trends in Cardiac CasesIn 2007, Cleveland Clinic thoracic and cardiovascular surgeons at The Chester County Hospital performed a total of 156 cardiac procedures.
10% Thoracic
10% Other
Cardiac Case Distribution
63% CABG
12% Valve
12% CABG & Valve
13% Other
80% Cardiac
The Chester County Hospital has completed its second year of affiliation with Cleveland
Clinic’s Department of Thoracic and Cardiovascular Surgery. Year two marked even
further collaboration and integration of clinical practices, leading to the expansion
of thoracic surgery services at The Chester County Hospital. Now, patients in
southeastern Pennsylvania have access to the latest techniques and technologies for
cardiac and thoracic care—close to home.
The Chester County Hospital
Isolated Coronary artery bypass grafting (CABG) operations accounted for more than half of cardiac procedures in 2007. Valve and other procedures rep-resented the remaining 37 percent.
8Outcomes 2007 Thoracic and Cardiovascular Surgery9
Overview
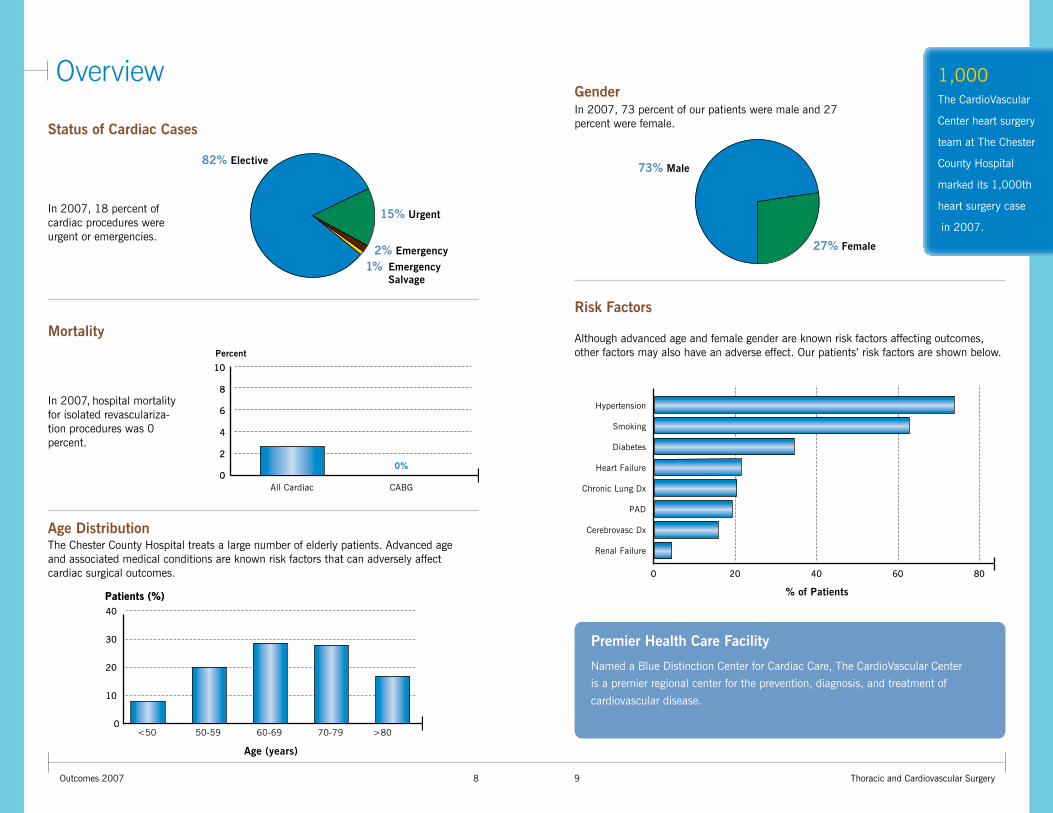
The Chester County Hospital treats a large number of elderly patients. Advanced age and associated medical conditions are known risk factors that can adversely affect cardiac surgical outcomes.
Age Distribution
00
4040
<50
2020
3030
1010
Patients (%)Patients (%)
60-6950-59
Age (years)
70-79 >80
Mortality
In 2007, hospital mortality for isolated revasculariza-tion procedures was 0 percent.
73% Male
27% Female
In 2007, 73 percent of our patients were male and 27 percent were female.
Gender
Although advanced age and female gender are known risk factors affecting outcomes, other factors may also have an adverse effect. Our patients’ risk factors are shown below.
Risk Factors
% of Patients
00 2020 4040 6060 8080
Hypertension
Smoking
Diabetes
Heart Failure
Chronic Lung Dx
PAD
Cerebrovasc Dx
Renal Failure
Premier Health Care Facility
Named a Blue Distinction Center for Cardiac Care, The CardioVascular Center
is a premier regional center for the prevention, diagnosis, and treatment of
cardiovascular disease.
In 2007, 18 percent of cardiac procedures were urgent or emergencies.
82% Elective
15% Urgent
2% Emergency
1% Emergency Salvage
1010
88
66
44
00
22
All Cardiac
Percent
CABG
0%
Status of Cardiac Cases
1,000The CardioVascular
Center heart surgery
team at The Chester
County Hospital
marked its 1,000th
heart surgery case
in 2007.
10Outcomes 2007 Thoracic and Cardiovascular Surgery11
Coronary Disease
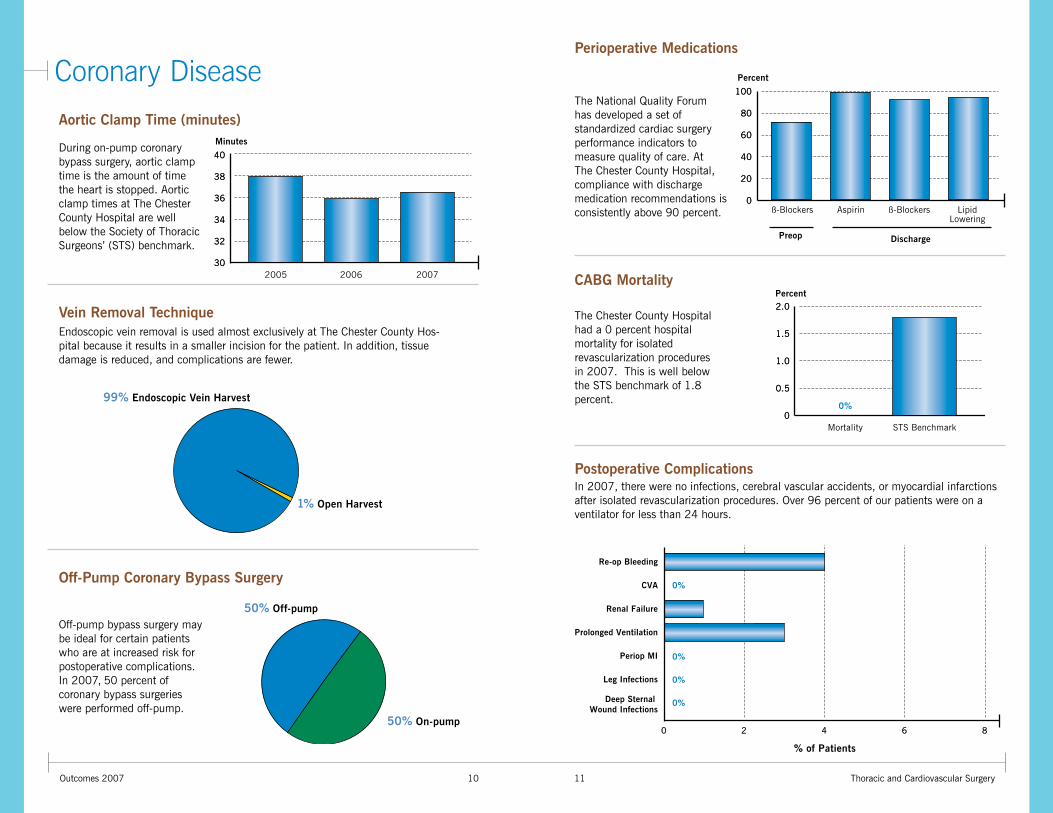
Postoperative ComplicationsIn 2007, there were no infections, cerebral vascular accidents, or myocardial infarctions after isolated revascularization procedures. Over 96 percent of our patients were on a ventilator for less than 24 hours.
Off-Pump Coronary Bypass Surgery
Off-pump bypass surgery may be ideal for certain patients who are at increased risk for postoperative complications. In 2007, 50 percent of coronary bypass surgeries were performed off-pump.
50% Off-pump
50% On-pump
Aortic Clamp Time (minutes)
Perioperative Medications
CABG Mortality
During on-pump coronary bypass surgery, aortic clamp time is the amount of time the heart is stopped. Aortic clamp times at The Chester County Hospital are well below the Society of Thoracic Surgeons’ (STS) benchmark.
Endoscopic vein removal is used almost exclusively at The Chester County Hos-pital because it results in a smaller incision for the patient. In addition, tissue damage is reduced, and complications are fewer.
Vein Removal Technique
99% Endoscopic Vein Harvest
1% Open Harvest
2005 2006 2007
Minutes
4040
3838
3636
3434
3232
3030
% of Patients
00 22 44 66 88
Prolonged Ventilation
Deep Sternal Wound Infections
0%
0%
0%
0%
Leg Infections
Re-op Bleeding
CVA
Periop MI
Renal Failure
ß-Blockers
Preop
Aspirin ß-Blockers
Discharge
LipidLowering
Percent
100100
8080
6060
4040
2020
00
2.02.0
1.51.5
1.01.0
0.50.5
00Mortality
Percent
STS Benchmark
0%
The National Quality Forum has developed a set of standardized cardiac surgery performance indicators to measure quality of care. At The Chester County Hospital, compliance with discharge medication recommendations is consistently above 90 percent.
The Chester County Hospital had a 0 percent hospital mortality for isolated revascularization procedures in 2007. This is well below the STS benchmark of 1.8 percent.
12Outcomes 2007 Thoracic and Cardiovascular Surgery13
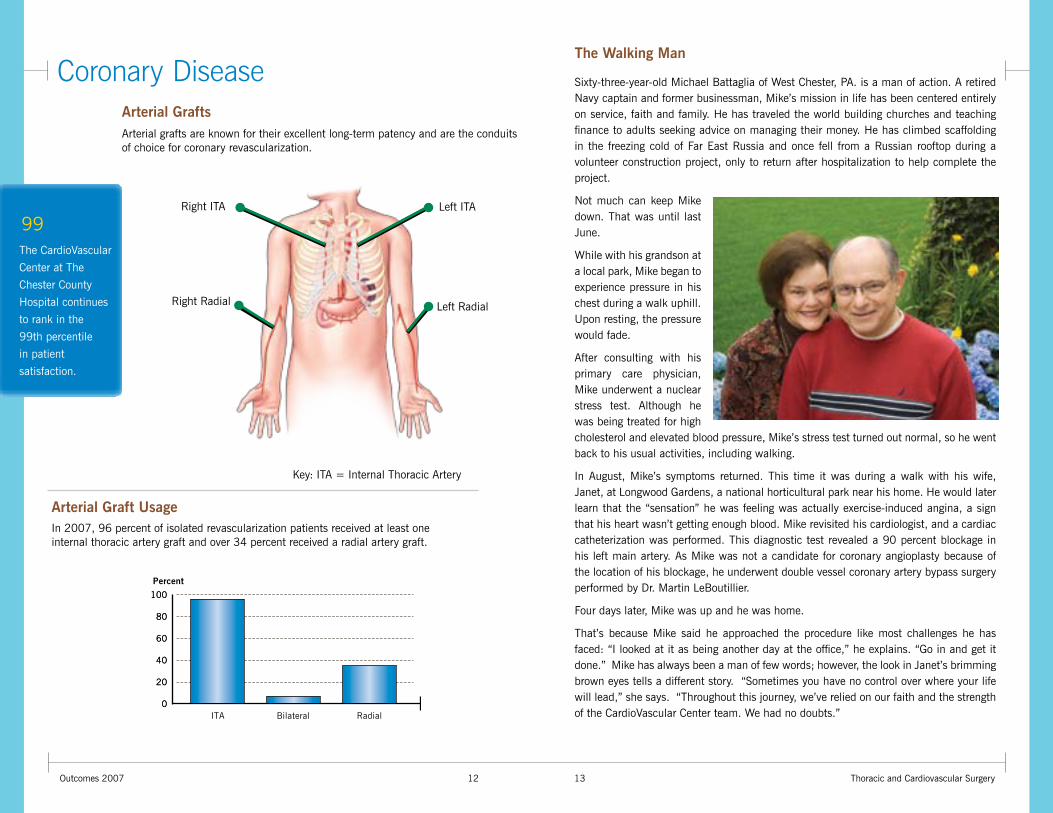
Coronary DiseaseArterial GraftsArterial grafts are known for their excellent long-term patency and are the conduits of choice for coronary revascularization.
Left ITA
Left RadialRight Radial
Right ITA
In 2007, 96 percent of isolated revascularization patients received at least one internal thoracic artery graft and over 34 percent received a radial artery graft.
Arterial Graft Usage
ITA Bilateral Radial
Percent
100100
8080
6060
4040
2020
00
Sixty-three-year-old Michael Battaglia of West Chester, PA. is a man of action. A retired Navy captain and former businessman, Mike’s mission in life has been centered entirely on service, faith and family. He has traveled the world building churches and teaching finance to adults seeking advice on managing their money. He has climbed scaffolding in the freezing cold of Far East Russia and once fell from a Russian rooftop during a volunteer construction project, only to return after hospitalization to help complete the project.
Not much can keep Mike down. That was until last June.
While with his grandson at a local park, Mike began to experience pressure in his chest during a walk uphill. Upon resting, the pressure would fade.
After consulting with his primary care physician, Mike underwent a nuclear stress test. Although he was being treated for high cholesterol and elevated blood pressure, Mike’s stress test turned out normal, so he went back to his usual activities, including walking.
In August, Mike’s symptoms returned. This time it was during a walk with his wife, Janet, at Longwood Gardens, a national horticultural park near his home. He would later learn that the “sensation” he was feeling was actually exercise-induced angina, a sign that his heart wasn’t getting enough blood. Mike revisited his cardiologist, and a cardiac catheterization was performed. This diagnostic test revealed a 90 percent blockage in his left main artery. As Mike was not a candidate for coronary angioplasty because of the location of his blockage, he underwent double vessel coronary artery bypass surgery performed by Dr. Martin LeBoutillier.
Four days later, Mike was up and he was home.
That’s because Mike said he approached the procedure like most challenges he has faced: “I looked at it as being another day at the office,” he explains. “Go in and get it done.” Mike has always been a man of few words; however, the look in Janet’s brimming brown eyes tells a different story. “Sometimes you have no control over where your life will lead,” she says. “Throughout this journey, we’ve relied on our faith and the strength of the CardioVascular Center team. We had no doubts.”
The Walking Man
Key: ITA = Internal Thoracic Artery
The CardioVascular
Center at The
Chester County
Hospital continues
to rank in the
99th percentile
in patient
satisfaction.
99
14Outcomes 2007 Thoracic and Cardiovascular Surgery15
Thoracic Surgery
2020
1515
1010
55
002006
Volume
2007
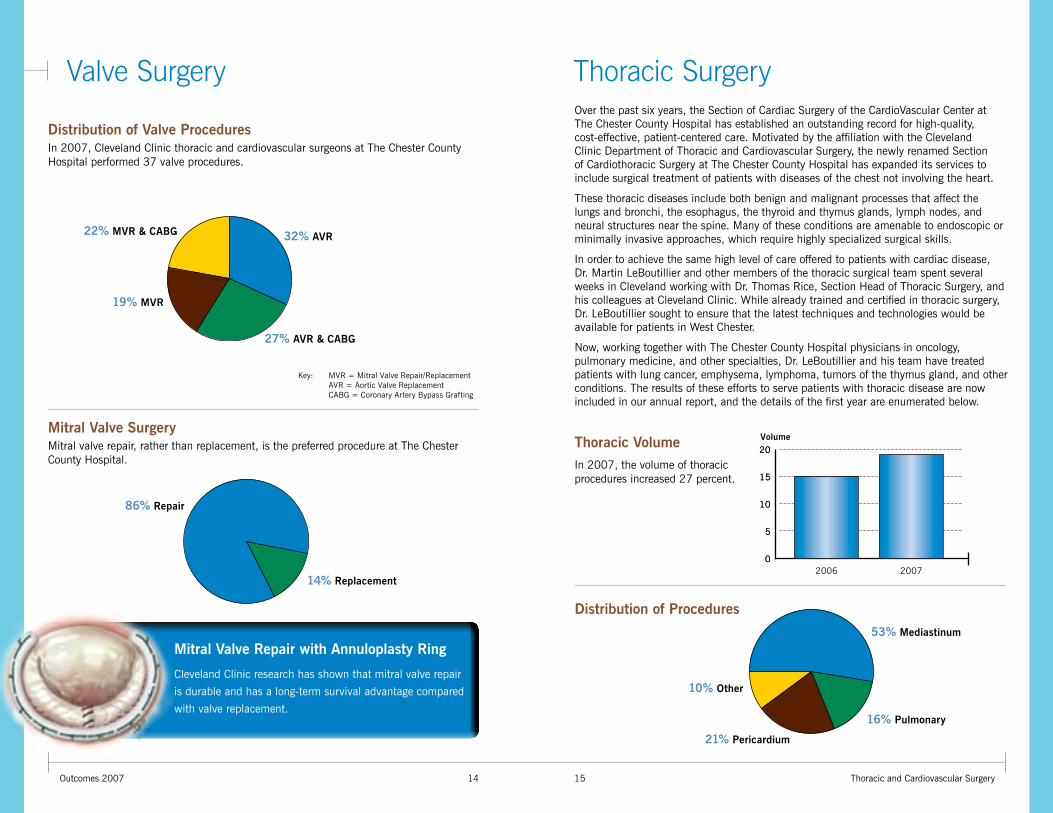
Thoracic Volume
Distribution of Procedures
16% Pulmonary
21% Pericardium
10% Other
53% Mediastinum
In 2007, the volume of thoracic procedures increased 27 percent.
Over the past six years, the Section of Cardiac Surgery of the CardioVascular Center at The Chester County Hospital has established an outstanding record for high-quality, cost-effective, patient-centered care. Motivated by the affiliation with the Cleveland Clinic Department of Thoracic and Cardiovascular Surgery, the newly renamed Section of Cardiothoracic Surgery at The Chester County Hospital has expanded its services to include surgical treatment of patients with diseases of the chest not involving the heart.
These thoracic diseases include both benign and malignant processes that affect the lungs and bronchi, the esophagus, the thyroid and thymus glands, lymph nodes, and neural structures near the spine. Many of these conditions are amenable to endoscopic or minimally invasive approaches, which require highly specialized surgical skills.
In order to achieve the same high level of care offered to patients with cardiac disease, Dr. Martin LeBoutillier and other members of the thoracic surgical team spent several weeks in Cleveland working with Dr. Thomas Rice, Section Head of Thoracic Surgery, and his colleagues at Cleveland Clinic. While already trained and certified in thoracic surgery, Dr. LeBoutillier sought to ensure that the latest techniques and technologies would be available for patients in West Chester.
Now, working together with The Chester County Hospital physicians in oncology, pulmonary medicine, and other specialties, Dr. LeBoutillier and his team have treated patients with lung cancer, emphysema, lymphoma, tumors of the thymus gland, and other conditions. The results of these efforts to serve patients with thoracic disease are now included in our annual report, and the details of the first year are enumerated below.
Valve Surgery
Mitral Valve Repair with Annuloplasty Ring
Cleveland Clinic research has shown that mitral valve repair
is durable and has a long-term survival advantage compared
with valve replacement.
In 2007, Cleveland Clinic thoracic and cardiovascular surgeons at The Chester County Hospital performed 37 valve procedures.
Distribution of Valve Procedures
32% AVR
27% AVR & CABG
19% MVR
22% MVR & CABG
Key: MVR = Mitral Valve Repair/Replacement AVR = Aortic Valve Replacement CABG = Coronary Artery Bypass Grafting
86% Repair
14% Replacement
Mitral valve repair, rather than replacement, is the preferred procedure at The Chester County Hospital.
Mitral Valve Surgery
16Outcomes 2007
Innovation
Thoracic and Cardiovascular Surgery17
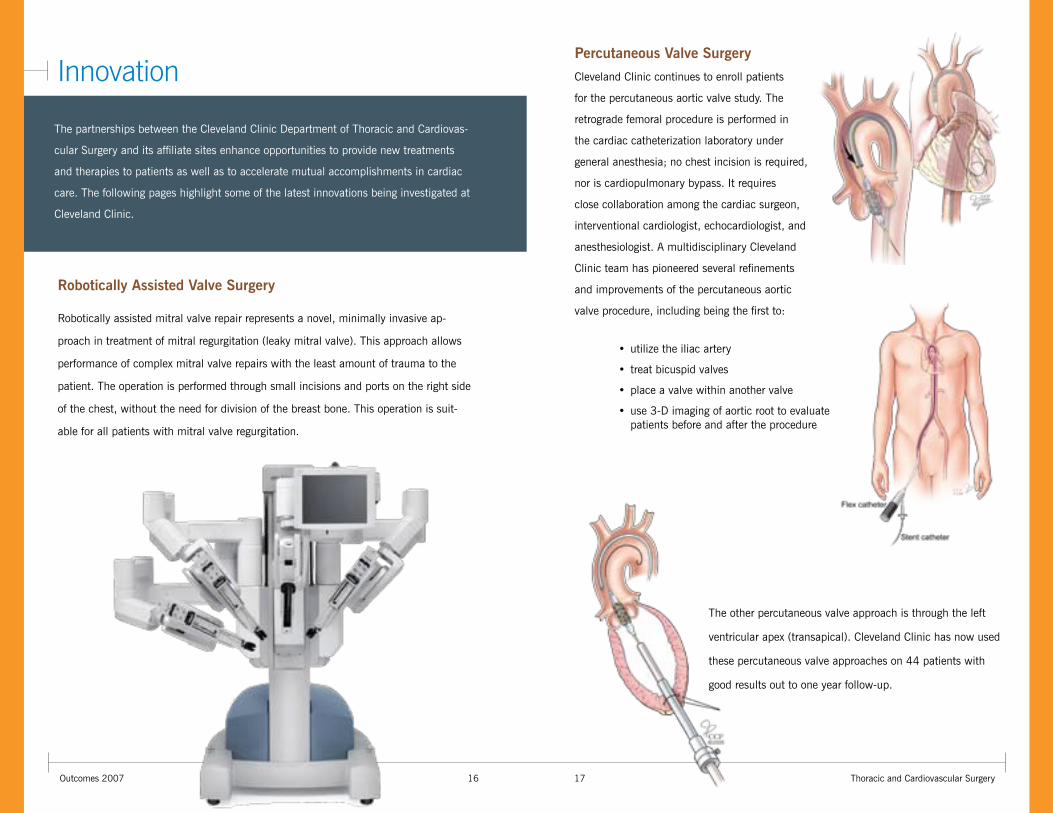
Robotically assisted mitral valve repair represents a novel, minimally invasive ap-
proach in treatment of mitral regurgitation (leaky mitral valve). This approach allows
performance of complex mitral valve repairs with the least amount of trauma to the
patient. The operation is performed through small incisions and ports on the right side
of the chest, without the need for division of the breast bone. This operation is suit-
able for all patients with mitral valve regurgitation.
The other percutaneous valve approach is through the left
ventricular apex (transapical). Cleveland Clinic has now used
these percutaneous valve approaches on 44 patients with
good results out to one year follow-up.
Robotically Assisted Valve Surgery
Cleveland Clinic continues to enroll patients
for the percutaneous aortic valve study. The
retrograde femoral procedure is performed in
the cardiac catheterization laboratory under
general anesthesia; no chest incision is required,
nor is cardiopulmonary bypass. It requires
close collaboration among the cardiac surgeon,
interventional cardiologist, echocardiologist, and
anesthesiologist. A multidisciplinary Cleveland
Clinic team has pioneered several refinements
and improvements of the percutaneous aortic
valve procedure, including being the first to:
Percutaneous Valve Surgery
• utilize the iliac artery
• treat bicuspid valves
• place a valve within another valve
• use 3-D imaging of aortic root to evaluate patients before and after the procedure
The partnerships between the Cleveland Clinic Department of Thoracic and Cardiovas-
cular Surgery and its affiliate sites enhance opportunities to provide new treatments
and therapies to patients as well as to accelerate mutual accomplishments in cardiac
care. The following pages highlight some of the latest innovations being investigated at
Cleveland Clinic.
18Outcomes 2007
Innovation
Thoracic and Cardiovascular Surgery19
E-Valve
Cleveland Clinic physicians are now in active trials
with E-Valve, a technology that treats patients expe-
riencing mitral regurgitation with a clip on the mitral
valve leaflets.
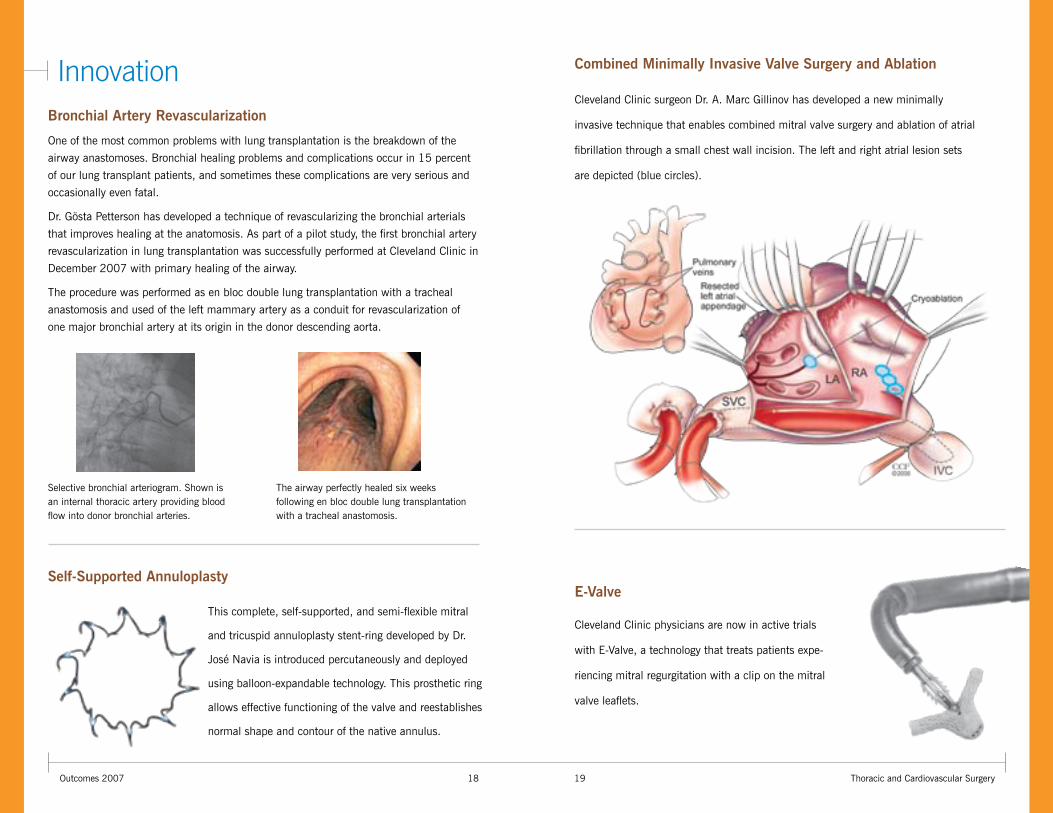
Combined Minimally Invasive Valve Surgery and Ablation
Cleveland Clinic surgeon Dr. A. Marc Gillinov has developed a new minimally
invasive technique that enables combined mitral valve surgery and ablation of atrial
fibrillation through a small chest wall incision. The left and right atrial lesion sets
are depicted (blue circles).
Self-Supported Annuloplasty
This complete, self-supported, and semi-flexible mitral
and tricuspid annuloplasty stent-ring developed by Dr.
José Navia is introduced percutaneously and deployed
using balloon-expandable technology. This prosthetic ring
allows effective functioning of the valve and reestablishes
normal shape and contour of the native annulus.
Bronchial Artery Revascularization
One of the most common problems with lung transplantation is the breakdown of the
airway anastomoses. Bronchial healing problems and complications occur in 15 percent
of our lung transplant patients, and sometimes these complications are very serious and
occasionally even fatal.
Dr. Gösta Petterson has developed a technique of revascularizing the bronchial arterials
that improves healing at the anatomosis. As part of a pilot study, the first bronchial artery
revascularization in lung transplantation was successfully performed at Cleveland Clinic in
December 2007 with primary healing of the airway.
The procedure was performed as en bloc double lung transplantation with a tracheal
anastomosis and used of the left mammary artery as a conduit for revascularization of
one major bronchial artery at its origin in the donor descending aorta.
The airway perfectly healed six weeks following en bloc double lung transplantation with a tracheal anastomosis.
Selective bronchial arteriogram. Shown is an internal thoracic artery providing blood flow into donor bronchial arteries.
20Outcomes 2007 Thoracic and Cardiovascular Surgery21
Staff Biographies Contact Informationwww.cchosp.comwww.866drheart.com
Bruce W. Lytle, M.D., Chairman
Eugene H. Blackstone, M.D.
A. Marc Gillinov, M.D.
Gonzalo Gonzalez-Stawinski, M.D.
David P. Mason, M.D.
Tomislav Mihaljevic, M.D.
Sudish C. Murthy, M.D., Ph.D.
José L. Navia, M.D.
Gösta B. Pettersson, M.D., Ph.D.
Thomas W. Rice, M.D.
Eric E. Roselli, M.D.
Joseph F. Sabik III, M.D.
Nicholas G. Smedira, M.D.
Lars G. Svensson, M.D., Ph.D.
Main Campus www.clevelandclinic.org/heartcenter
Call 610-738-2690, your one-stop cardiac surgery information source:
Evaluation for Cardiac Surgery Office support personnel expedite the request for consult, organize the patient’s schedule and address questions.
Hospital TransferThe cardiothoracic surgery office will facilitate the transfer of a patient from any hospital to The Chester County Hospital’s CardioVascular Center.
Direct to SurgeonThis is the cardiothoracic surgery office. Your call will be directed to one of our cardiac surgeons.
EmergenciesA cardiothoracic surgeon is available 24 hours every day. The on-call surgeon can be reached by calling this number any hour of the day.
Location The cardiothoracic surgery office is located at The Chester County Hospital, second floor, 701 E. Marshall Street, West Chester, PA., 19390. 610-738-2690
Martin LeBoutillier, III, M.D.Verdi J. DiSesa, M.D.
Staff Surgeon, Thoracic and Cardiovascular Surgery
The Chester County Hospital, a Cleve-land Clinic Thoracic and Cardiovascular Surgery Affiliate Program
Specialties: Aortic valve surgery, coronary artery bypass grafting, reoperations, left ventricle reconstruction surgery (Dor), surgical treatment of atrial fibrillation, minimally invasive heart surgery, mitral valve surgery, off-pump heart surgery, valvuloplasty, thoracic surgery
Medical Degree: Columbia University Col-lege of Physicians & Surgeons, New York
Special Training: New York University Medical Center, New York
Dr. LeBoutillier enjoys spending time with his family and motorcycling.
Chief, Cardiac Surgery
The Chester County Hospital, a Cleve-land Clinic Thoracic and Cardiovascular Surgery Affiliate Program
Specialties: Aortic valve surgery, coronary artery bypass grafting, reoperations, left ventricle reconstruc-tion surgery (Dor), surgical treatment of atrial fibrillation, minimally invasive heart surgery, mitral valve surgery, valvuloplasty
Medical Degree: University of Pennsylvania School of Medicine, Philadelphia
Special Training: Brigham & Women’s Hospital, Boston, Hospital of The Uni-versity of Pennsylvania, Philadelphia
Dr. DiSesa enjoys spending time with his family, sailing and traveling.

www.cchosp.comwww.clevelandclinic.org/heartcenter© Copyright 2008 The Cleveland Clinic Foundation. All rights reserved.