Embed Size (px)
Citation preview

CardiovascularCardiovascular A&P and Patho-physiology A&P and Patho-physiology
Irene Mueller, EdD, RHIA Irene Mueller, EdD, RHIA
Montana Hospital AssociationMontana Hospital AssociationMay 26, 2010May 26, 2010

Objectives – First HourObjectives – First Hour
• Functions of Circulatory System
• Heart & Vessels– Anatomy– Normal physiology
• Congenital – VSD– PDA– Coarctation of Aorta– ASD– Tetralogy of Fallot– Transposition of Great
Arteries Pathologies
– HTN

Objectives - 2Objectives - 2ndnd hour hour
Pathologies
– CAD– MIs– Anginas– Arrhythmias– CHF– Cor Pulmonale– Emboli
• Vessel Pathologies
– Congenital• AV Malformations
– Pathologies• Phlebitis• Thrombophlebitis• Emboli• Arteriosclerosis
• Resources
http://www.alleganynutrition.com/images/upload/blood-vessels-an.jpg

Functions of Circulatory SystemFunctions of Circulatory System
• 2 primary functions– Delivery of oxygen, nutrients, hormones, other
essential body substances to body cells– Removal of waste products from cells
• CO2 waste product of respiration
• Metabolism wastes carried to kidneys, skin, intestines– Nitrogenous
– RBCs carry O2 to cells; CO2 away from cells to lungs

3 sub-circulation systems3 sub-circulation systems
• Pulmonary– Exchange of O2 and CO2
– Carries blood to lungs • to receive O2 and remove CO2
• Coronary– Nutrition and health of heart muscle
• Systemic– Delivers blood and components to all tissues
• Except lungs and myocardium

A&PA&P
• Pericardium• Muscle (myocardium)• Chambers• Valves• Arteries• Veins• Flow of Blood• Systole• Diastole
• Coronary Arteries

EnclosureEnclosure• Pericardium
– 2 layers• Inner serous
– Visceral pericardium OR epicardium
• Outer fibrous– Parietal
– Between layers• Serous fluid• Reduces friction during heartbeat (function)

FactsFacts
• The heart is about the size of your fist
• Usu pumps about 50% of blood present in chamber at beginning of contraction (ejection fraction)
• Pumps about 5 quarts/minute
• Up to 5 gallons/min during exercise
• Pumps about 4,000 gallons/day

ChambersChambers
is 4-chambered hollow organ of strong muscle tissue
• Located in thorax between lungs
• 2 pumps side-by-side– R atrium and R ventricle
• Blood from body pumped to lungs (pulmonary circ)
– L atrium and L ventricle• Blood from lungs to body (systemic circulation)

ValvesValves
• 4 valves prevent backflow of blood in – AV Valve (Tricuspid)
• Between R atrium and R ventricle
– Pulmonic/Pulmonary valve• Between R ventricle and pulmonary arteries
– Bicuspid (Mitral)• Between L atrium and L ventricle
– Aortic Valve • Between L ventricle and Aorta

ChambersChambers
• Atria (upper chambers)– Thin-walled– Receive and hold blood before ventricles
• Ventricles– Thick-walled– Main pumps
• Septa – walls between chambers– Atrial septum– Ventricular septum
Where else do you have a septum?

Flow of Blood through Flow of Blood through (Cardiac cycle)(Cardiac cycle)
• http://kidshealth.org/misc/movie/parent/ASD_rev/ASD_rev.html

Cardiac CycleCardiac Cycle
• Cardiac muscle contraction cycle• One sequence of conduction pathway
– One heartbeat– PQRST segment on EKG
• Electrical stimulation triggers contractions– Sinoatrial (SA) node– Atrioventricular (AV) node– Bundle of His, R & L Bundle Branches– Purkinje fibers

PQRSTPQRST
• http://cygnus.et.put.poznan.pl/~piotrw/nauka/fibonacci/heartelec2.gif

A&PA&P
http://www.nhlbi.nih.gov/health/dci/Diseases/shock/shock_heartworks.html

Coronary ArteriesCoronary Arteries
• 1st vessels to branch from the aorta
• Right Coronary Artery supplies posterior • Left Main Coronary Artery divides into
– Left Anterior Descending• Supplies front of
– Left Circumflex• Wraps around the left and posterior
• http://myhealth.ucsd.edu/library/healthguide/en-us/images/media/medical/hw/h9991261_001.jpg

Great VesselsGreat Vessels
• “the large arteries and veins entering and leaving the heart. They include– the aorta, (3 cm diameter as leaves )– the pulmonary arteries and veins, and – the superior and inferior vena cava.”
• Superior drains upper body (about size of thumb)• Inferior drains lower body
http://medical-dictionary.thefreedictionary.com/great+vessel

Grey’s Anatomy.
Figure 489

Vessel A&PVessel A&P
• Arteries– Carry Oxygenated Blood
• Exception: • Pulmonary Arteries
– Very high pressure– Elastic, muscular– Thick Walls
• Tunica adventitia/externa• Tunica media (sm. muscle)• Tunica intima
http://www2.merriam-webster.com/mw/art/med/artery.htm

Vessel A & PVessel A & P
• Arterioles– Arteries branch into smaller and smaller sizes– Smallest arteries branch into arterioles
• Less smooth muscle in walls
– Arterioles branch into metarterioles• Loss of connective tissue/muscle layers• Give rise to Capillaries

Vessel A&PVessel A&P• Capillaries
– Smallest vessels– Microscopic– Connect metarterioles
• to venules
– Endothelial layer only– Very thin walls– Selective permeability
• O2/CO2
• Nutrition• WBCs/Plasma
http://www2.merriam-webster.com/mw/art/med/circulat.htm

Artery AnatomyArtery Anatomy
http://www.kidney-hypertension.com/arteries.gif

Vessel A & PVessel A & P
• Venules– Little larger than capillary, then larger, etc.– Have muscular layer also

Vessel A&PVessel A&P
• Veins– Carry de-oxygenated blood – 3 layers
• Tunica Externa, Media, Intima
– Much Less elastic/muscular– Thinner walls/less pressure– Valves
• One-way flow to heart• More in lower body
http://www2.merriam-webster.com/mw/art/med/vein.htm

Vessel A & PVessel A & P
• Venous Return– Contraction of skeletal muscles help– Breathing pressure changes help
– http://www.youtube.com/watch?v=HNuPWdfjDoc
• 62,000 miles of blood vessels in a human body

Vessel AnatomyVessel Anatomy
http://umanitoba.ca/faculties/medicine/units/anatomy/images/ArtVeincopy.JPG

Circulatory PhysiologyCirculatory Physiology
• Blood pressure
– Systolic (Top Number)• Moment of contraction in heart• Pressure against vessel walls/resistance
– Diastolic (Bottom Number)• Moment of relaxation of the heart• Less pressure against vessel walls
• Pulse pressure = systolic - diastolic

PulsePulse
• Pulse is usu. same as rate• Alternating, beating throbs at body
points– Brachial– Carotid (common)– Femoral– Dorsalis pedis– Popliteal– Radial– Temporal
Where is each of these points on your body?

Congenital Congenital Disease Disease

Congenital Congenital Disease Disease
• “Congenital Heart Defects (CHD) are the most common birth defect in the United States. About 35,000 children (1 of 120) are born with a CHD every year.” ACHA
• Can be diagnosed at any age– 10%+ of cases dx as adults
• 2008 - 1 million + people w/congenital heart disease have survived to adulthood

Etiologies of Congenital Etiologies of Congenital disease disease
• Genetic
• Other risk factors– Maternal rubella (German measles)– Poor maternal nutrition– Alcoholism/Drug abuse– Some medications during pregnancy

Congenital Congenital Conditions Conditions
• VSD (Ventricular Septal Defect)
• PDA (Patent Ductus Arteriosus)
• ASD (Atrial Septal Defect)
• Tetralogy of Fallot
• Coarctation of Aorta
• Transposition of Great Arteries

Fetal HeartFetal Heart
• Fetal lungs not used for breathing
• Blood enters R atrium, most of blood flows to L atrium through a special fetal opening - foramen ovale
• Fetal circulation shunts (bypasses lungs) from pulmonary artery to aorta through a connecting blood vessel - ductus arteriosus
• After Birth, normally both close

VSD (Ventricular Septal Defect)VSD (Ventricular Septal Defect)
• Opening in the ventricular septum remains
• Most common heart defect (25%)– "Hole in the heart“
• If small, often "heals" (closes) on its own• Blood flows from L ventricle to R ventricle at high
pressure, often a loud "murmur"
– Larger VSD requires surgery as baby– Smaller may be watched for years – http://www.med.ucla.edu/wilkes/Systolic.htm

PDAPDA
• Ductus Arteriosus– Connection between pulmonary artery and
aorta – Normal in fetal • Patent – does NOT close after birth
• Oxygenated blood goes back to lungs instead of to body – increases workload
• 2x more common in girls

ASDASD
• Opening between R and L atria
• Usu. Due to foramen ovale NOT closing
• Oxygenated blood goes from L to R atria– Never leaves lungs and heart
• More common in girls

Tetralogy of FallotTetralogy of Fallot
• Tetra = Four in Greek
• Very serious heart defect – Blue Baby
• Combination in varying degrees of– Pulmonary valve stenosis– R ventricle Hypertrophy– Ventricle Septal Defect– Abnormal placement of Aorta

S&S of Tetralogy of FallotS&S of Tetralogy of Fallot
• Cyanosis – increases with age
• Clubbing of fingers/toes
• Resting in squatting position– Breathe easier, improves venous return
• Growth retardation
• Severe dyspnea with exercise
• Frequent Respiratory infections

Coarctation of AortaCoarctation of Aorta
• Stricture (Varying degrees) of– Descending or thoracic aorta
• High blood pressure proximal to narrowing
• Lower blood pressure distal
• May cause bl press in arms, in legs
• Increases workload on heart
• May NOT be dx until adulthood

Transposition of Great ArteriesTransposition of Great Arteries• Aorta and Pulmonary artery are "transposed" from
normal position– Aorta arises from the R ventricle – Pulmonary artery arises from the L ventricle
• Oxygen-poor ("blue") blood from body is sent back to body
• Oxygen-rich ("red") blood from lungs is sent back to lungs
• Untreated, 50% + of infants die in 1st month , 90% percent in 1st year
• If no unusual risk factors, surgery successful for 95% + of NBs
• http://www.cincinnatichildrens.org/health/heart-encyclopedia/anomalies/graphicsummaries/transwf.htm

PathologiesPathologies
• HTN• CAD• MIs• Anginas• Arrhythmias• CHF• Cor Pulmonale• Emboli

Common S&S of Common S&S of Disease Disease
• Chest Pain• Dyspnea• Fatigue• Tachycardia
• Cardiac palpitations– Strong, rapid, irregular
heartbeats that pt feels
• Diaphoresis• Edema of extremities• N&V

HTNHTN
• Silent Killer – no symptoms– Leading cause of
stroke/heart failure– Reduced life
expectancy • When Diastolic is 90+
• Can be primary OR• 2nd (due to other disease)
– Cerebrovascular– Cardiovascular– Kidney
• 20% of Americans w/HTN• Higher % in
– Blacks– Postmenopausal women– South (Stroke Belt)
• Diet variation• More salt• More cholesterol• Less micronutrients

HTNHTN
• Normal = LESS than 120/80• Pre-HTN = 120-130/80-89• Stage 1 HTN = 140-159/90-99• Stage 2 HTN = 160+/100+
• Determined by action of heart and/or blood vessel resistance
• Kidney also has role

Primary/Essential HTNPrimary/Essential HTN
• 90% of cases• Idiopathic, but risk factors• Heredity (Black, Family Hx)• Diet – High salt and fat• Age• Obesity – increased heart workload• Smoking - vasoconstriction• Stress - vasoconstriction
– Type A personality

Salt and HTNSalt and HTN• Action of salt in body
– Kidneys excrete – if too much, stays in blood– Excess salt holds water, increases volume
• = high blood pressure
– Excess salt increases ouabain (hormone)• Keeps calcium in artery muscle cells• Triggers constriction and HTN
• Salt-sensitivity (50% of Americans)– African-Americans, elderly, diabetics

Salt in American Diet Salt in American Diet
• 3,436 mg sodium daily (Average)
• Many experts now (2010) • Lowering daily
consumption to 1,500 mg of sodium daily
• Prevent/lower high blood pressure
• Most dietary sodium in processed foods
• 1/4 teaspoon salt=
600 mg sodium• 1/2 teaspoon salt=
1,200 mg sodium• 3/4 teaspoon salt=
1,800 mg sodium• 1 teaspoon salt=
2,300 mg sodium• 1 teaspoon baking soda=
1,000 mg sodium

Complications of HTN Complications of HTN
• Arteriosclerosis and atherosclerosis
• Aneurysm • CAD/Angina/MIs• Enlarged L heart• Heart Failure• TIAs/Stroke/Dementia
• Kidney failure/scarring• Retinopathy• Optic neuropathy
• Sexual Dysfunction ♂• Osteoporosis• Sleep Apnea, but
– Sleep apnea increases blood pressure

Malignant HTNMalignant HTN
• S&S– Severe headache, blurred vision, dyspnea– Organ damage– Sudden onset
• Risk factor for CVA, renal damage, MI
• Etiology unknown, but stress may contribute
• 200+/120+

Break TimeBreak Time

Coronary Artery DiseaseCoronary Artery Disease(CAD)(CAD)
• Narrowing of arteries that supply muscle• #1cause of death in US (men and women)• Usu due to atherosclerosis
– Ischemia, necrosis of muscle tissue– Causes CHF
• Blocked artery (occlusion)– Slow – plaque (may have collateral arteries)– Fast – thrombus/embolus– Infarct (MI)
• AKA – CHD and arteriosclerotic disease

Risk Factors for CADRisk Factors for CAD
• Atherosclerotic risk factors– Heredity– Age– Sex (more in males
until menopause in women)
– Diabetes– Diet (more fat and
carbs = more athero)– Sedentary lifestyle– Smoking
• NOT smoking 10 X more effective than diet/exercise control
– Stress– HTN

AnginasAnginas
• Types of angina (an-JI-nuh or AN-juh-nuh) stable – unstable – variant (Prinzmetal)– microvascular
• Have different symptoms and require different treatments

Stable AnginaStable Angina
• AKA – Angina Pectoris, Cardiac Angina, Exertion Angina, Vasomotor Angina, Angina Syndrome, Angina Attack, Chest Pain
• Caused by lack of oxygen to muscle– Myocardial ischemia
• Symptom of impending MI• Triggered by exercise, stress, large meal
– Consistent pattern of events that trigger

Unstable AnginaUnstable Angina
• Doesn't follow a pattern
• Can occur w/wo physical exertion
• May not be relieved by rest or medicine
• Very dangerous
• Requires emergency treatment
• Sign that MI may happen soon

Variant (Prinzmetal) AnginaVariant (Prinzmetal) Angina
• Rare
• Usually occurs at rest, between midnight and early morning
• Pain can be severe
• Medicine can relieve this type of angina

Microvascular anginaMicrovascular angina
• Can be more severe and last longer than other types of angina
• Medicine may not relieve it
• May be a symptom of coronary MVD – Also called cardiac syndrome X and
nonobstructive CHD– More common in women

Myocardial Infarction (MI)Myocardial Infarction (MI)
• Infarct = necrosis• Decrease in blood
supply to muscle– CAD plaque– Thrombus, Embolus
• Mortality from MI– About 35%
• Anything that increases oxygen need may lead to MI– Physical exertion– Shock– Hemorrhage– Stress

Risk Factors for MIRisk Factors for MI
• HTN
• Smoking
• Sedentary lifestyle– Burn fewer calories watching TV than
sleeping
• Obesity
• High-cholesterol diet

S&S of MIS&S of MI
• Severe chest pain
• Diaphoresis
• Nausea
• Referred pain– L arm, neck, jaw
• Feeling of indigestion
• Cardiogenic shock

Areas of Referred PainAreas of Referred Pain
• Pain sites can be helpful, but require more evaluation to eliminate differential dx
• http://images.emedicinehealth.com/images/4453/4453-4478-10907-25156.jpg

S&S of MI in WomenS&S of MI in Women
• Frequently no chest pain – silent MI
• Can begin up to a month before MI occurs
• S&S BEFORE MI– Unusual fatigue - 70%– Sleep disturbance - 48%– Shortness of breath - 42%– Indigestion - 39%– Anxiety - 35%
• S&S DURING MI– Shortness of breath - 58%– Weakness - 55%– Unusual fatigue - 43%– Cold sweat - 39%– Dizziness - 39%

• http://www.womenshealth.gov/heart-stroke/heart-attack-signs/heart-attack-signs.gif

Arrhythmias (Irregular Heartbeats)Arrhythmias (Irregular Heartbeats)
• Any deviation from normal
• Abnormalities due to problem in conduction system
• Often idiopathic
http://www.spike.com/video/ekgecg-intrpretation/3182500?cmpnid=790&pt=sr&refsite=7118

S&S of ArrhythmiasS&S of Arrhythmias
• Palpitations
• Tachycardia
• Skipped beats
• Bradycardia
• Syncope
• Fatigue

Etiologies of ArrhythmiasEtiologies of Arrhythmias
• Disturbance of– SA node (slow impulse)– AV node– Bundle branches– Purkinje fibers– Block between SA and AV nodes (conduction)
• Ischemia
• Meds

Normal Normal Rhythm Rhythm
• Normal sinus rhythm =
• Between 60 and 100 beats/minute – Normally, women have slightly higher # in range
• Regular
• Normal conduction
• Originating in SA node

Fast ArrhythmiasFast Arrhythmias
• Flutter – Up to 350 beats/minute– Regular
• Fibrillation (Irregularly Irregular)– Uncoordinated, Irregular– Atrial – usually not serious– Ventricular (vfib) – life-threatening/emergency
http://filer.case.edu/~dck3/heart/sounds/af.wav

Fast ArrhythmiasFast Arrhythmias
• Atrial Tachycardia– 150-250 bpm– Normal rhythm– Sudden onset
• Irritable atrium• Normal conduction
• Atrial Fibrillation– >350 bpm– Ectopic discharging– AV node blocks some
impulses– Ventricle responds
irregularly
– No P waves

Fast ArrhythmiasFast Arrhythmias
• Ventricular Tachycardia– 150-250 bpm– Usu regular– 4+ PVCs at rapid rate– Advanced irritability of
myocardium– P wave buried in QRS
complex
• Often forerunner of vfib
• Ventricular Fibrillation– Lethal– Loss of consciousness
immediately– No peripheral pulses– No heart sounds– No blood pressure
• Fibers twitch

Slow ArrhythmiaSlow Arrhythmia
• Sinus Bradycardia– Less than 60 bpm– Regular– P wave unform
• Slow impulse in SA node
• Normal Conduction

Heart Block ArrhythmiasHeart Block Arrhythmias
• Interrupted conduction system– 1st Delay at AV node– 2nd AV node blocks impulse intermittantly– 3rd SA impluse is completely blocked
• Atria and ventricles beat independently• Requires pacemaker

Premature Premature Contractions Contractions
• Can affect atria or ventricles
• Ectopic beat starts in irritable ventricle
• Followed by compensatory pause
• AKA - "extrasystoles"

Multifocal ArrhythmiaMultifocal Arrhythmia• Regularly irregular PVCs• Ectopic beat(s) – no prior P wave
– Coupling – two beats in a row• regular occurrence of a premature beat
– Bigeminy – every other beat– Trigeminy – every third beat
• 2 normal QRS complexes are followed by a PVC – Quadrigeminy – every fourth beat
• heartbeats are grouped in fours• usually one sinus beat followed by three extrasystoles• a repetitive group of four of any composition is
quadrigeminal

CHFCHF
can’t pump enough blood for body• Failure of ventricles• Develops slowly• Usu. Follows cardiac condition increasing workload
– Acute CHF after MI– Chronic CHF after HTN, CAD, COPD, valve, arrhythmias,
cardiomyopathy– Other - thyroid disease, kidney disease, diabetes, or
congenital heart defects • R-sided =congestion of liver and spleen• L-sided = lung congestion
• http://www.health-res.com/EX/08-03-22/HeartFailureZones.gif

Progression of CHFProgression of CHF
• Decreased Cardiac Output (many etiologies)• Compensation mechanisms
– Vasoconstriction, increased resistance in L V– Increased rate and force, incr. work– Incr. sodium and water retentioin, incr volume, increased
work for heart
• L CHF - LV weakens – pulmonary congestion – Increased resistance for RV
• R CHF – increased blood in systemic circ– Edema in legs and Digestive system

S&S of CHFS&S of CHF• Depend on which ventricle fails• Dyspnea - L• Tachycardia• Tachypnea• Neck vein distention – R• Ascites - R• Pedal edema - R (CHF)
– Pitting edema (fluid is forced into interstitial spaces)– pitting is an assessment using grading scale of 1+ for
mild and up to 4+ for deep pitting.
• http://www.health-res.com/EX/07-28-04/55PJ35JA.jpg

Assessment of pitting edemaAssessment of pitting edema
• 1 + = 2mm or less – Slight pitting – Disappears rapidly – No visible distortion
• 2 + = 2-4mm– Somewhat deeper pit– Disappears in 10-15 secs– No easily detected distortion
• Assessment Chart for Pitting Edema adapted from the Guelph General Hospital Congestive Heart Failure Pathway
• 3 + = 4-6mm – Pit noticeably deep – May last more than 1 minute– Dependent extremity looks
fuller and swollen (4-6mm)
• 4 + Edema = 6-8mm– Pit is very deep – Lasts as long as 2-5 minutes– Dependent extremity is
grossly distorted (6-8mm)

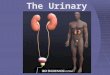
Cor PulmonaleCor Pulmonale
• Right-sided heart disease• R ventricle enlarges due to lung disease
– Acute – pulmonary emboli– Chronic - pulmonary HTN, emphysema,
lesions– Hypoxia = More RBCs = thicker blood
• S&S– Dyspnea, distended neck veins, edema of
extremities, enlarged/tender liver

Vessel PathologiesVessel Pathologies
• Congenital– Arteriovenous Malformations
• Pathologies– Phlebitis– Thrombophlebitis– Emboli– Arteriosclerosis
http://www2.merriam-webster.com/mw/art/med/vein.htm

Common S&S of Vessel DiseaseCommon S&S of Vessel Disease
• Pain
• Edema
• Cyanosis

Arteriovenous Malformations Arteriovenous Malformations
• Formed in fetus• Usu. NOT discovered before age 20• Usu. in brain, but can occur anywhere• Abnormal connection (no capillaries)• Fragile, tend to bleed/hemorrhage• When in brain, bleed can lead to S&S
similar to stroke• Cerebral AVMs have 10% mortality rate

PhlebitisPhlebitis
• Inflammation of vein
• Usu in lower legs, but can occur anywhere
• Superficial– Swelling, redness, warmth, cordlike mass
• Deep– Affects tunica intima, can cause clots
• Thrombophlebitis

ThrombophlebitisThrombophlebitis
• Formation of a thrombus on vein wall due to inflammation (phlebitis)
• Interferes with blood flow, causes edema• S&S - Pain, swelling, warmth, tender,
chills & fever• Causes
– Venous stasis (sitting in car/plane for long time, etc.), Hypercoagulability, blood disorders, injury to wall

EmbolusEmbolus
• Material transported by blood stream, sticks in small vessel, impedes circulation
• Thrombus - blood clot breaks loose and travels (DVTs, cardiac arrhythmias)
• Cholesterol -often from atherosclerotic plaque in vessel
• Fat – bone fracture or fat droplets
• Air (Gas) – air bubbles – surgery, injury, central cath, diving

EmbolusEmbolus
• Material transported by blood stream, sticks in small vessel, impedes circulation
• Septic – pus-containing bacteria, bacterial clumps
• Tissue – of small fragments of tissue (placenta, etc)
• FB – foreign materials such as talc and other small objects
• Amniotic fluid – amniotic fluid, fetal cells, hair, or other debris enters mother's bloodstream via placenta and triggers allergic reaction

S&S of EmboliS&S of Emboli
• Depend on Location and amount of tissue served by vessel
• Severe pain
• Pale, numb, cold extremities
• Arterial pulses absent beyond occlusion
• N&V, Fainting, Shock IF large artery

Causes of EmboliCauses of Emboli
• Bed rest
• Physical Inactivity
• Heart failure
• Arrhythmias
• Pressure on veins
• Decreased flow in veins

ArteriosclerosisArteriosclerosis
• Group of diseases - hardening of arteries
• 3 forms– Atherosclerosis
• Plaque w/in arterial tunica intima
– Moncheberg’s arteriosclerosis• Medial calcific sclerosis, tunica media• Destruction of muscle/fibers w/calcium deposits
– Arteriosclerosis• Arteriole walls thicken, lose elasticity/contractility

HomeworkHomework• Please access these two case studies and
identify ALL (not just Cardiovascular) narrative dx statements that you would code. (DO NOT code yet)– N.B.The second case covers several encounters
• Congestive Heart Failure Case Study. VHCT. School of Health Professions. University of Missouri – Columbia.– http://www.vhct.org/case1899/phys_exam.htm
• Lifestyle Issues in Cardiac Health. Robert L. Blake, Jr., MD. VHCT. School of Health Professions. University of Missouri – Columbia. – http://www.vhct.org/case2800/index.htm

15 leading causes of death 200615 leading causes of death 2006• Diseases of heart (heart disease) (CV, Lifestyle)• Malignant neoplasms (cancer) • Cerebrovascular diseases (stroke) (CV, Lifestyle)• Chronic lower respiratory diseases • Accidents (unintentional injuries) • Diabetes mellitus (diabetes) (CV, Lifestyle)• Alzheimer’s disease • Influenza and pneumonia • Nephritis, nephrotic syndrome and nephrosis (kidney disease) • Septicemia (CV)• Intentional self-harm (suicide) • Chronic liver disease and cirrhosis • Essential hypertension and hypertensive renal disease
(hypertension) – (CV, Lifestyle)
• Parkinson’s disease • Assault (homicide)

A&P/Pathophys ResourcesA&P/Pathophys Resources• American Heart Association/American Stroke Association. Cardiovascular media library.
http://www.medmovie.com/mmdatabase/mediaplayer.aspx?Message=VG9waWNpZD0wO0NsaWVudElEPTY1O1Zlcm5hY3VsYXJJRD0x%2DP83bCzVaVLA%3D
• American Heart Assoc. Adults With Congenital Heart Defects. 12/14/09. http://www.americanheart.org/presenter.jhtml?identifier=11062
• American Heart Assoc. Blood Pressure. (n.d.)http://www.americanheart.org/presenter.jhtml?identifier=4473.
• Cable, C. MD. Auscultation Assistant. 1997. – http://www.med.ucla.edu/wilkes/intro.html
• The Cardiac Exam: Auscultation – http://filer.case.edu/dck3/heart/listen.html
• Cincinnati Children's Hospital Medical Center. Cardiac Anomalies / Congenital Heart Defects – http://www.cincinnatichildrens.org/health/heart-encyclopedia/anomalies/default.htm
• EKG/ECG Interpretation (4+ minute video). – http://www.spike.com/video/ekgecg-intrpretation/3182500?cmpnid=790&pt=sr&refsite=7118

A&P/Patho ResourcesA&P/Patho Resources
• Frazier, M. S. and Drzymkowski, J. W. 2009. Essentials of Human Diseases and Conditions, 4th ed. Saunders.
• Fulcher, E.M., Soto, C.D., Fulcher, R.M. Pharmacology: Principles & Applications. A worktext for Allied Health Professionals, Saunders, 2003.
• Gray’s Anatomy. 1918. At Bartleby.com Great Books Online. – http://www.bartleby.com/cgi-bin/texis/webinator/sitesearch?
FILTER=col107&query=&x=12&y=10
• Health Resources. Heart Failure Zones.– http://www.health-res.com/EX/08-03-22/HeartFailureZones.gif
• Heartpoint Gallery. http://www.heartpoint.com/gallery.html

A&P/Patho ResourcesA&P/Patho Resources
• KidsHealth For Parents– http://kidshealth.org/misc/movie/parent/ASD_rev/ASD_rev.html
• Maryland Heart Center. About the Heart. University of Maryland Medical Center. – http://www.umm.edu/heart/anatomy.htm
• Mayo Clinic. High Blood Pressure (Hypertension). – http://www.mayoclinic.com/health/high-blood-pressure/HI00062
• Mayo Clinic. Coarctation of the Aorta.– http://www.mayoclinic.com/health/coarctation-of-the-aorta/DS00616/
DSECTION=symptoms
• MedlinePlus. U.S. National Library of Medicine and the National Institutes of Health.– http://medlineplus.gov/

A&P/Patho ResourcesA&P/Patho Resources
• Moisio M. A. & E. W. Moisio, Understanding Laboratory and Diagnostic Tests, Delmar, 1998 (2nd ed? later)
• National Heart Lung and Blood Institute. What Is Angina?– http://www.nhlbi.nih.gov/health/dci/Diseases/Angina/
Angina_WhatIs.html
• National Institute of Nursing Research. Women’s symptoms are new or different Prior to heart attack.– http://www.ninr.nih.gov/NR/rdonlyres/C76323E9-822F-47D9-853F-
61032685AC9E/4820/WomensSymptomsAreNeworDifferentPriortoHeartAttack.pdf
• Neighbors and Tannehill-Jones. Human Diseases. 2000. Delmar
• PQRST graphic– http://cygnus.et.put.poznan.pl/~piotrw/nauka/fibonacci/heartelec2.gif

A&P/Patho ResourcesA&P/Patho Resources
Robert Wood Johnson University Hospital. Heart Illustrations - Fetal Circulation http://www.rwjuh.edu/health_information/centers_heart_fetlcirc.html
•Scott, A. S. & Fong, E. Body Structures and Functions, 11th ed., Delmar, 2009
•St. Jude Medical. Heart Library. •http://www.heartlibrary.com/site-map.aspx (medical technology and services vendor)
•Tetralogy of Fallot. American Heart Assoc.•http://www.americanheart.org/presenter.jhtml?identifier=11071
•WebMD. Congenital Heart Disease. http://www.webmd.com/heart-disease/guide/congenital-heart-disease

VHCT CasesVHCT Cases
• Congestive Heart Failure Case Study. VHCT. School of Health Professions. University of Missouri – Columbia.– http://www.vhct.org/case1899/phys_exam.htm
• Lifestyle Issues in Cardiac Health. Robert L. Blake, Jr., MD. VHCT. School of Health Professions. University of Missouri – Columbia. – http://www.vhct.org/case2800/index.htm