Embed Size (px)
Citation preview
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
Factors Impeding the Practical Implementationof Cardiovascular Prevention
An international market research project in 6 countries:Germany, France, Italy, Spain, the United Kingdom and Poland
This study was commissioned byEuropean Society of Cardiology (ESC)
Cardiovascular Round Table (CRT)Task Force 4
Sponsors: AVENTIS / BAYER / BOSTON SCIENTIFIC /GLAXOSMITHKLINE / NOVARTIS / MERCK-SCHERING PLOUGH / PFIZER
The study was carried out by Psyma International:
Alexander RummelMonica Bach
Dr. Britta Meyer-Lutz
Study No: 41057021December 2002
Psyma International MedicalMarketing Research GmbH
Gartenweg 290607 Rückersdorf/Nürnberg
Germanyphone: +49-911-95 785-0fax: +49-911-95 785-33
e-mail: [email protected]: www.psyma-international.com
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
Main Objectives
To understand the practical hurdles of CV risk prevention in daily practice.
Identify how physicians assess and manage risk
Obtain baseline data on guideline usage
Reveal barriers why guidelines are not applied
Determine what changes can be made to make them more readily adopted
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
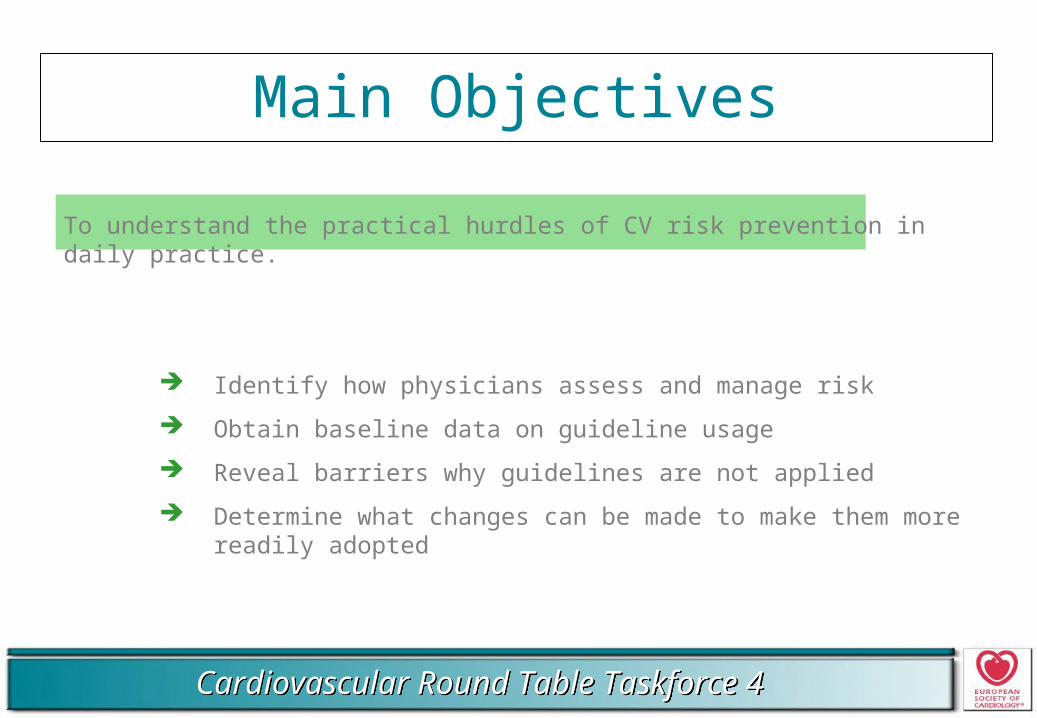
Methodology Sampling
D F I E UK PL
F2F in-depth interviews Total n = 30 50 50 30 30 30220
PCPs 21 35 35 21 21 21 154
Cards 9 15 15 9 9 9 66
Focus groups Total n = 2 2 1* 1* 6
PCPs 9 - - 7 9 10
Cards 7 - - 7
* PCPs only
ED F I
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
Screening Criteria
Work in outpatient care
< 60 years of age
Practicing as a PCP or cardiologist > 3 years
Must initiate drug treatments for patients presenting or at risk of CV disease
Work full-time (i.e. > 6 hrs per day)
Not participating in clinical trials on CV disease
Not working as a CV consultant for the pharmaceutical industry
GPs only
Must see and treat patients in at least 4 different indication areas
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
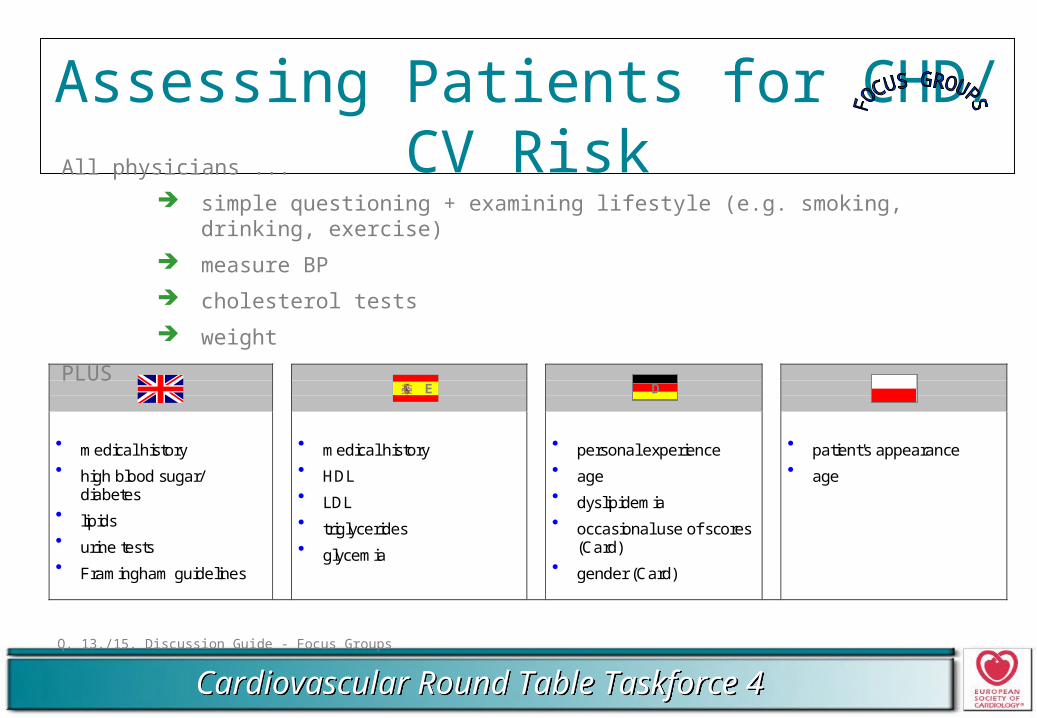
Assessing Patients for CHD/ CV Risk
Q. 13./15. Discussion Guide - Focus Groups
UK E D PL
medical history high blood sugar/
diabetes lipids urine tests Framingham guidelines
medical history HDL LDL triglycerides glycemia
personal experience age dyslipidemia occasional use of scores
(Card) gender (Card)
patient's appearance age
E D
All physicians ...
simple questioning + examining lifestyle (e.g. smoking, drinking, exercise)
measure BP
cholesterol tests
weight
PLUS
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
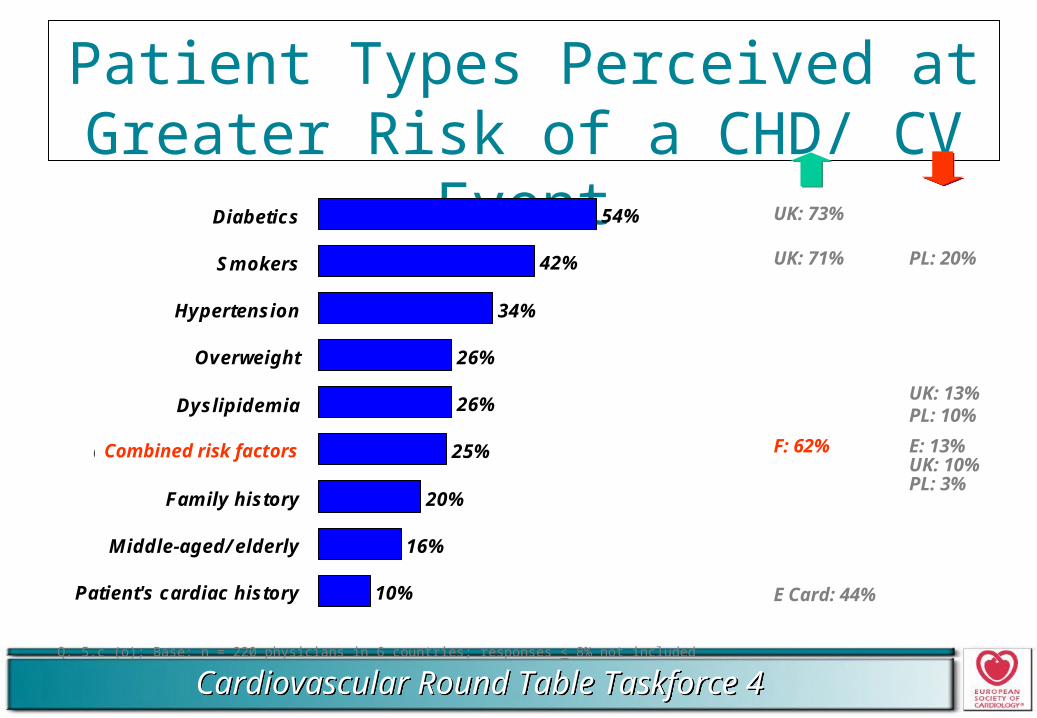
Patient Types Perceived at Greater Risk of a CHD/ CV Event
Q. 5.c (o); Base: n = 220 physicians in 6 countries; responses < 8% not included
54%
42%
34%
26%
26%
25%
20%
16%
10%
Diabetics
Smokers
Hypertension
Overweight
Dyslipidemia
Combined risk factors
Family history
Middle-aged/ elderly
Patient's cardiac history
UK: 73%
UK: 71% PL: 20%
UK: 13%PL: 10%
F: 62% E: 13%UK: 10%PL: 3%
E Card: 44%
Combined risk factors
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
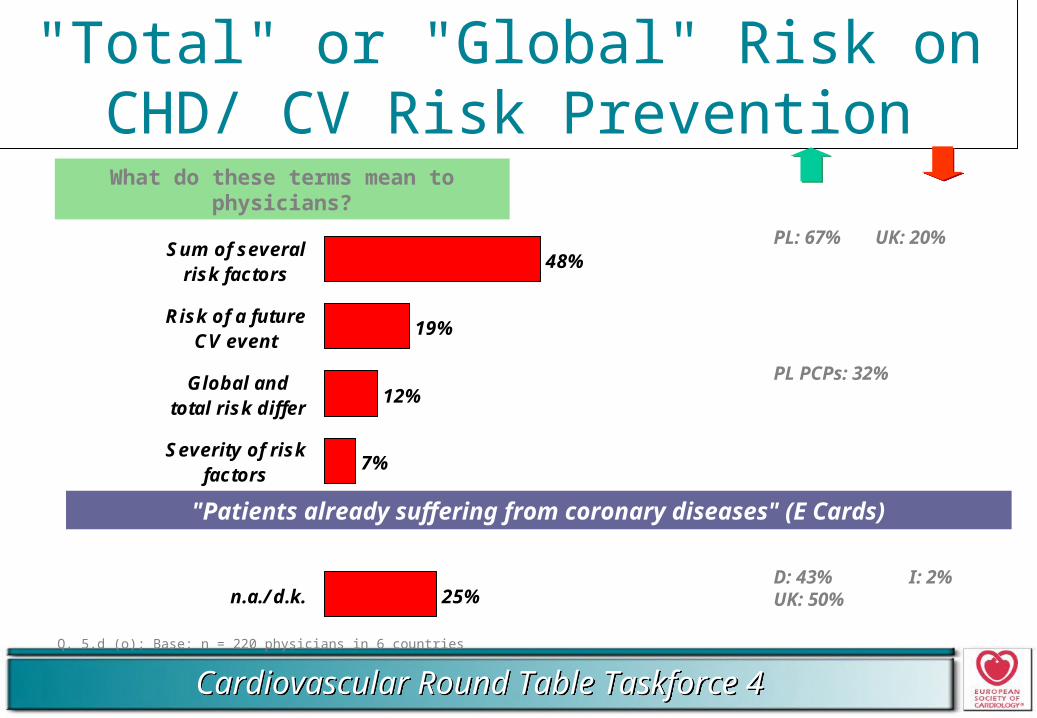
"Total" or "Global" Risk on CHD/ CV Risk Prevention
Q. 5.d (o); Base: n = 220 physicians in 6 countries
What do these terms mean to physicians?
PL: 67% UK: 20%
PL PCPs: 32%
D: 43% I: 2%UK: 50%
48%
19%
12%
7%
25%
Sum of severalrisk factors
Risk of a futureCV event
Global andtotal risk differ
Severity of riskfactors
n.a./ d.k.
"Patients already suffering from coronary diseases" (E Cards)
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
"Total" or "Global" Risk
25% of target sample don't know or can't explain terms
D 43%
UK 50%
EDUCATIONAL NEED
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
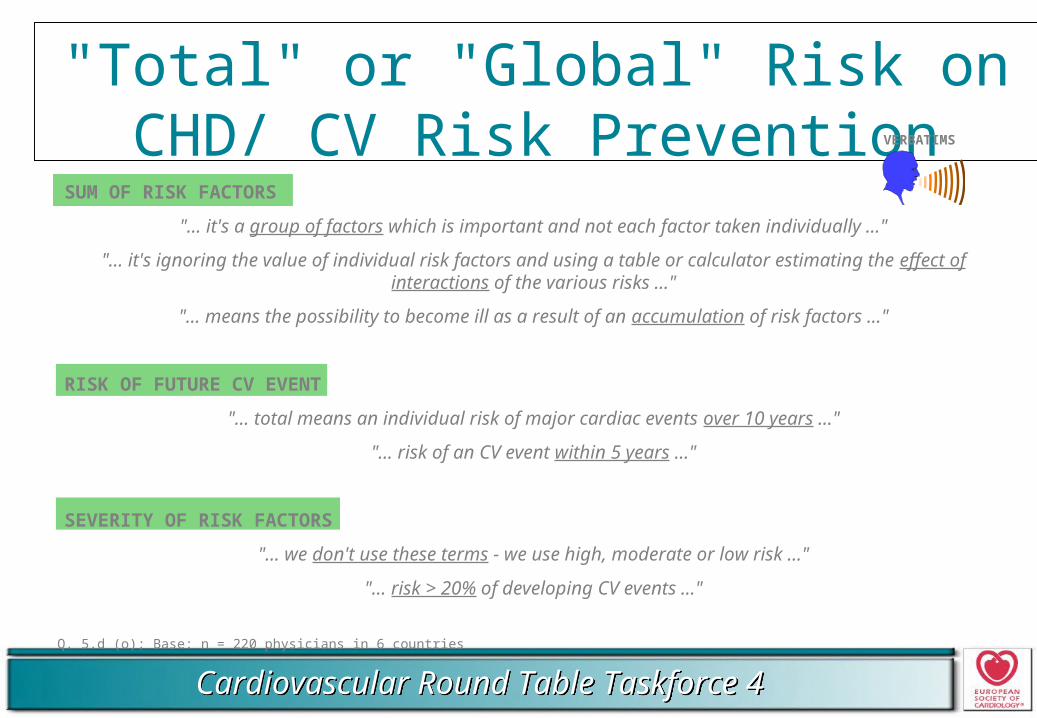
"Total" or "Global" Risk on CHD/ CV Risk Prevention
Q. 5.d (o); Base: n = 220 physicians in 6 countries
VERBATIMS
SUM OF RISK FACTORS
"... it's a group of factors which is important and not each factor taken individually ..."
"... it's ignoring the value of individual risk factors and using a table or calculator estimating the effect of interactions of the various risks ..."
"... means the possibility to become ill as a result of an accumulation of risk factors ..."
RISK OF FUTURE CV EVENT
"... total means an individual risk of major cardiac events over 10 years ..."
"... risk of an CV event within 5 years ..."
SEVERITY OF RISK FACTORS
"... we don't use these terms - we use high, moderate or low risk ..."
"... risk > 20% of developing CV events ..."
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
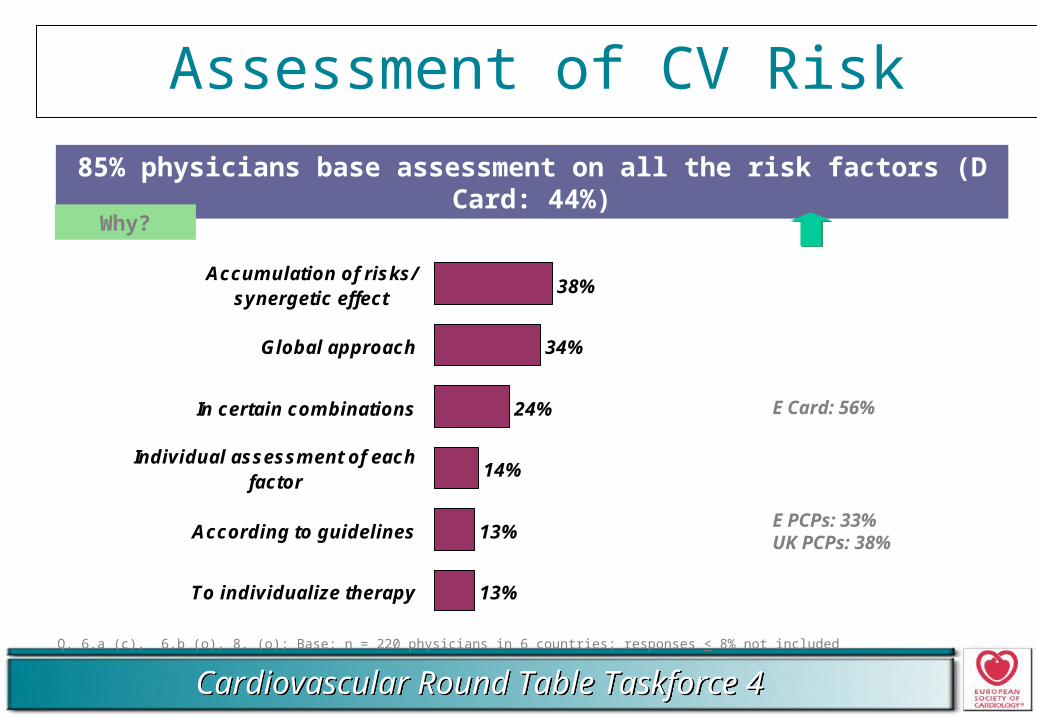
Assessment of CV Risk
85% physicians base assessment on all the risk factors (D Card: 44%)
E Card: 56%
E PCPs: 33%UK PCPs: 38%
Why?
38%
34%
24%
14%
13%
13%
Accumulation of risks/synergetic effect
Global approach
In certain combinations
Individual assessment of eachfactor
According to guidelines
To individualize therapy
Q. 6.a (c), 6.b (o), 8. (o); Base: n = 220 physicians in 6 countries; responses < 8% not included
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
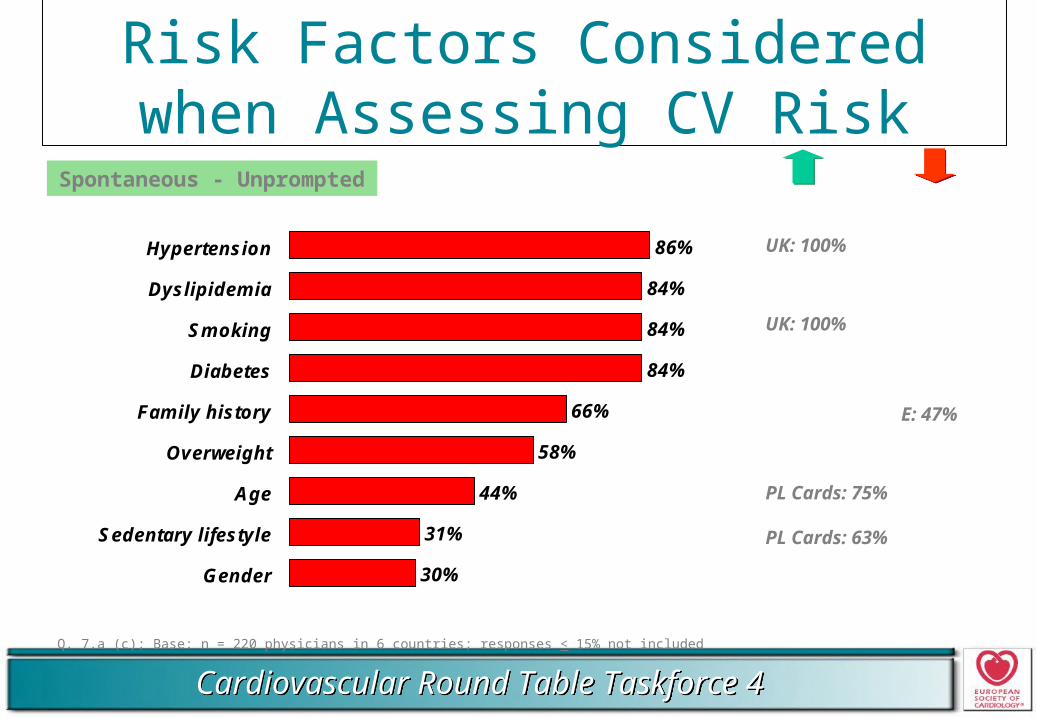
Risk Factors Considered when Assessing CV Risk
Q. 7.a (c); Base: n = 220 physicians in 6 countries; responses < 15% not included
Spontaneous - Unprompted
86%
84%
84%
84%
66%
58%
44%
31%
30%
Hypertension
Dyslipidemia
Smoking
Diabetes
Family history
Overweight
Age
Sedentary lifestyle
Gender
UK: 100%
UK: 100%
E: 47%
PL Cards: 75%
PL Cards: 63%
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
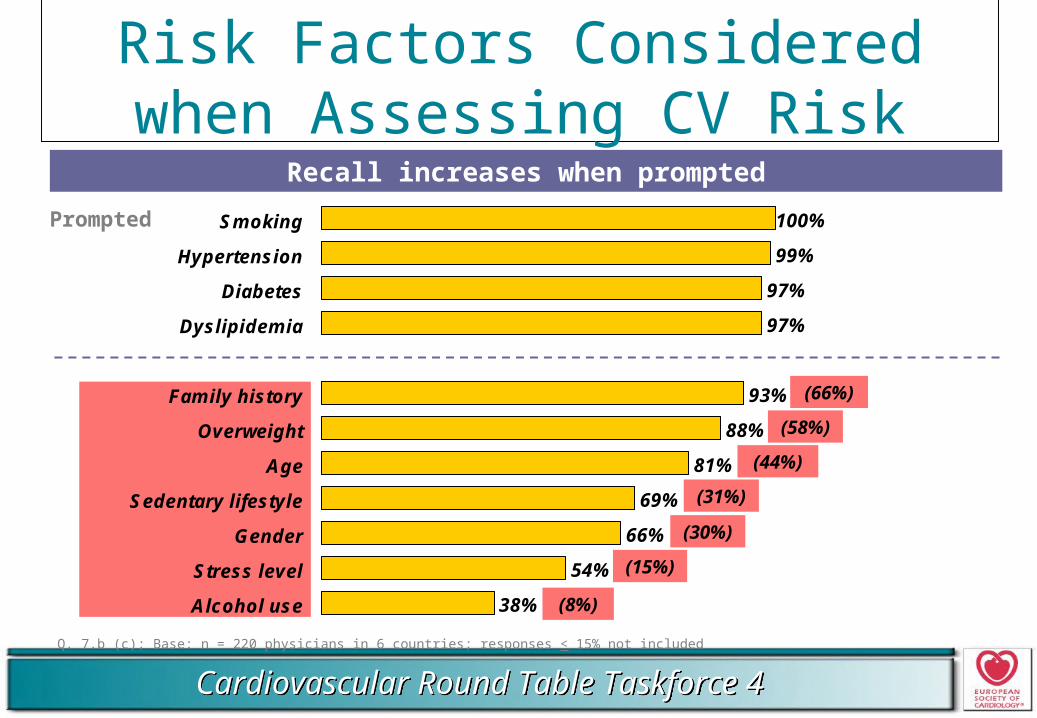
Recall increases when prompted
Risk Factors Considered when Assessing CV Risk
Q. 7.b (c); Base: n = 220 physicians in 6 countries; responses < 15% not included
Prompted 100%
99%
97%
97%
93%
88%
81%
69%
66%
54%
38%
Smoking
Hypertension
Diabetes
Dyslipidemia
Family history
Overweight
Age
Sedentary lifestyle
Gender
Stress level
Alcohol use
(66%)
(58%)
(44%)
(31%)
(30%)
(15%)
(8%)
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
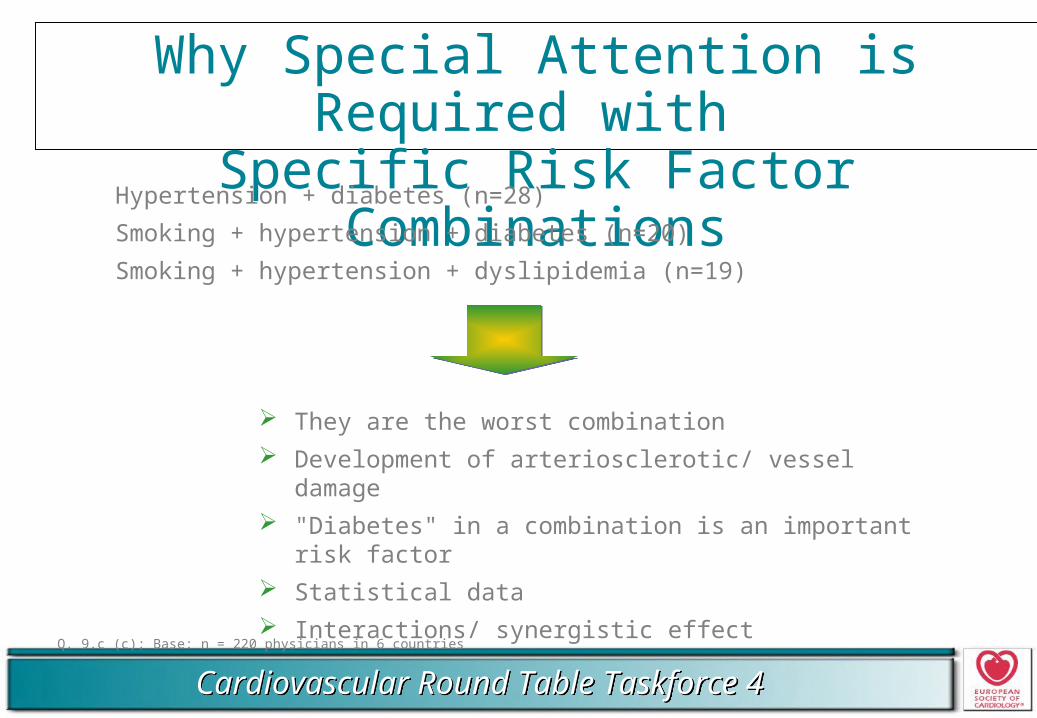
Why Special Attention is Required with Specific Risk Factor Combinations
Q. 9.c (c); Base: n = 220 physicians in 6 countries
Hypertension + diabetes (n=28)
Smoking + hypertension + diabetes (n=20)
Smoking + hypertension + dyslipidemia (n=19)
They are the worst combination
Development of arteriosclerotic/ vessel damage
"Diabetes" in a combination is an important risk factor
Statistical data
Interactions/ synergistic effect
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
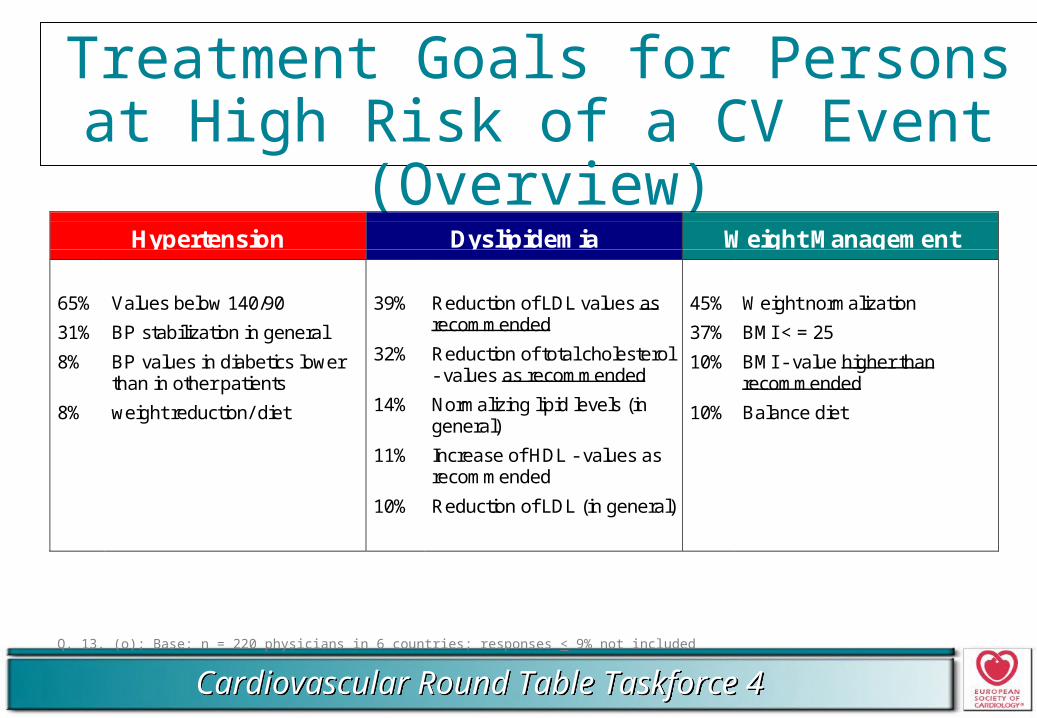
Treatment Goals for Persons at High Risk of a CV Event (Overview)
Q. 13. (o); Base: n = 220 physicians in 6 countries; responses < 9% not included
Hypertension Dyslipidemia Weight Management
65%
31%
8%
8%
Values below 140/90
BP stabilization in general
BP values in diabetics lowerthan in other patients
weight reduction/ diet
39%
32%
14%
11%
10%
Reduction of LDL values asrecommended
Reduction of total cholesterol- values as recommended
Normalizing lipid levels (ingeneral)
Increase of HDL - values asrecommended
Reduction of LDL (in general)
45%
37%
10%
10%
Weight normalization
BMI < = 25
BMI - value higher thanrecommended
Balance diet
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
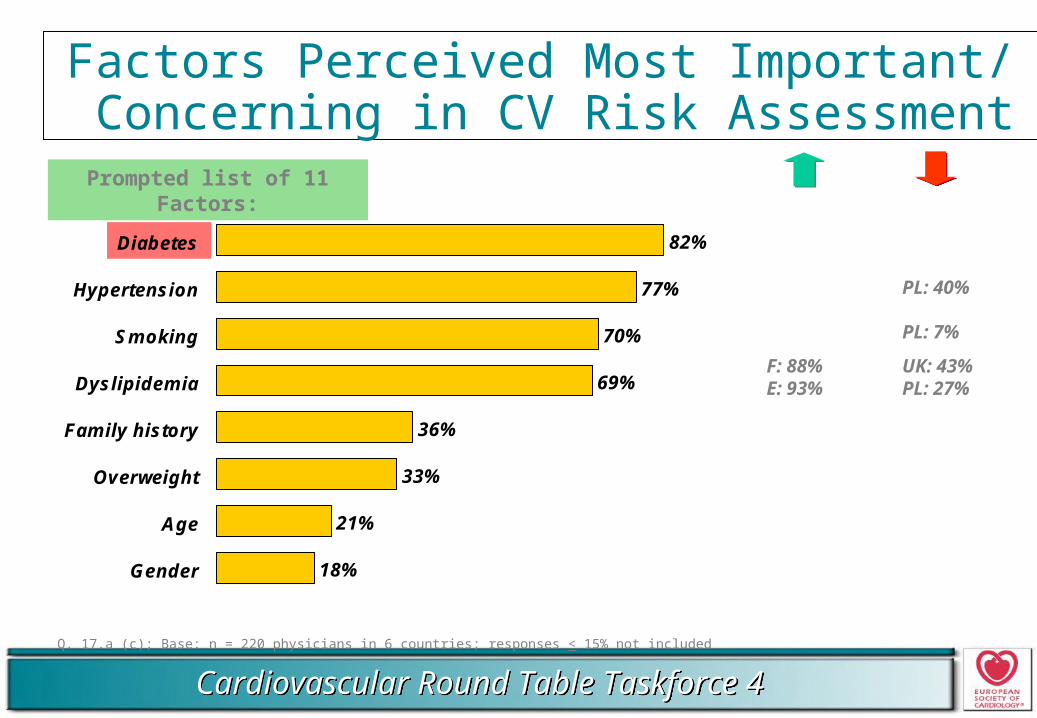
Factors Perceived Most Important/ Concerning in CV Risk Assessment
Q. 17.a (c); Base: n = 220 physicians in 6 countries; responses < 15% not included
Prompted list of 11 Factors:
82%
77%
70%
69%
36%
33%
21%
18%
Diabetes
Hypertension
Smoking
Dyslipidemia
Family history
Overweight
Age
Gender
PL: 40%
PL: 7%
F: 88% UK: 43%E: 93% PL: 27%
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
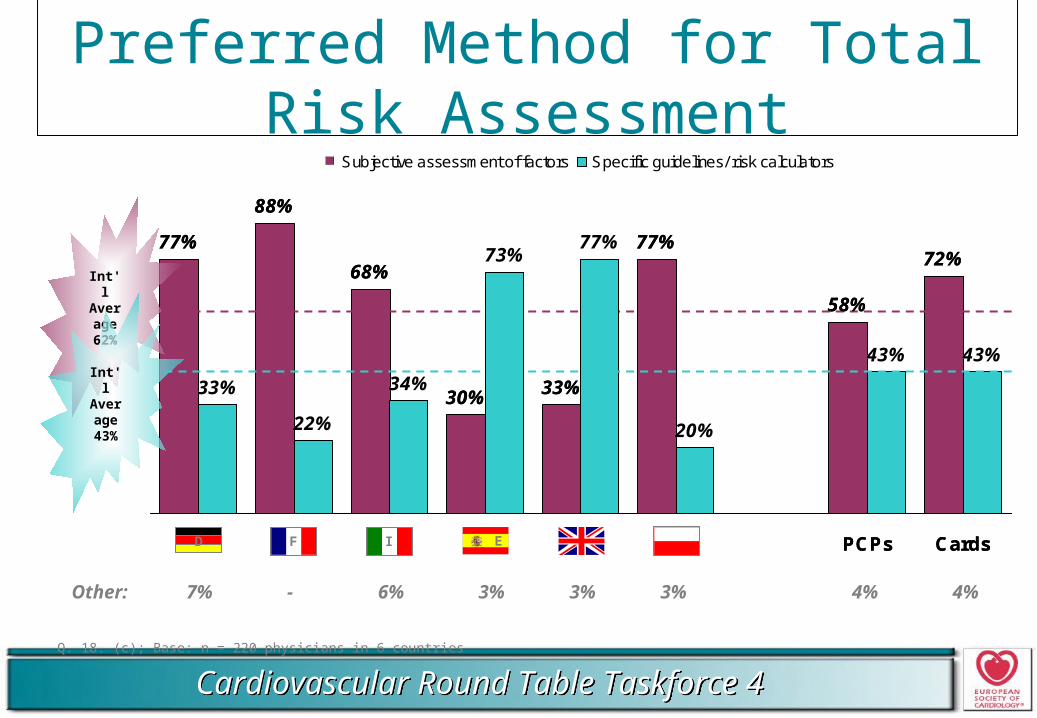
Preferred Method for Total Risk Assessment
Q. 18. (c); Base: n = 220 physicians in 6 countries
77%
88%
68%
30%
77%
58%
72%
33%
22%
34%
73%77%
20%
43% 43%
33%
D F I E UK PL PCPs Cards
Subjective assessment of factors Specific guidelines/ risk calculators
Int'lAvera
ge62%
ED F I
77%
88%
68%
30%
77%
58%
72%
33%
22%
34%
73%77%
20%
43% 43%
33%
D F I E UK PL PCPs Cards
Subjective assessment of factors Specific guidelines/ risk calculators
ED F I
Int'lAvera
ge43%
Other: 7% - 6% 3% 3% 3% 4% 4%
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
2.Awareness/ Usage of
Guidelines
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
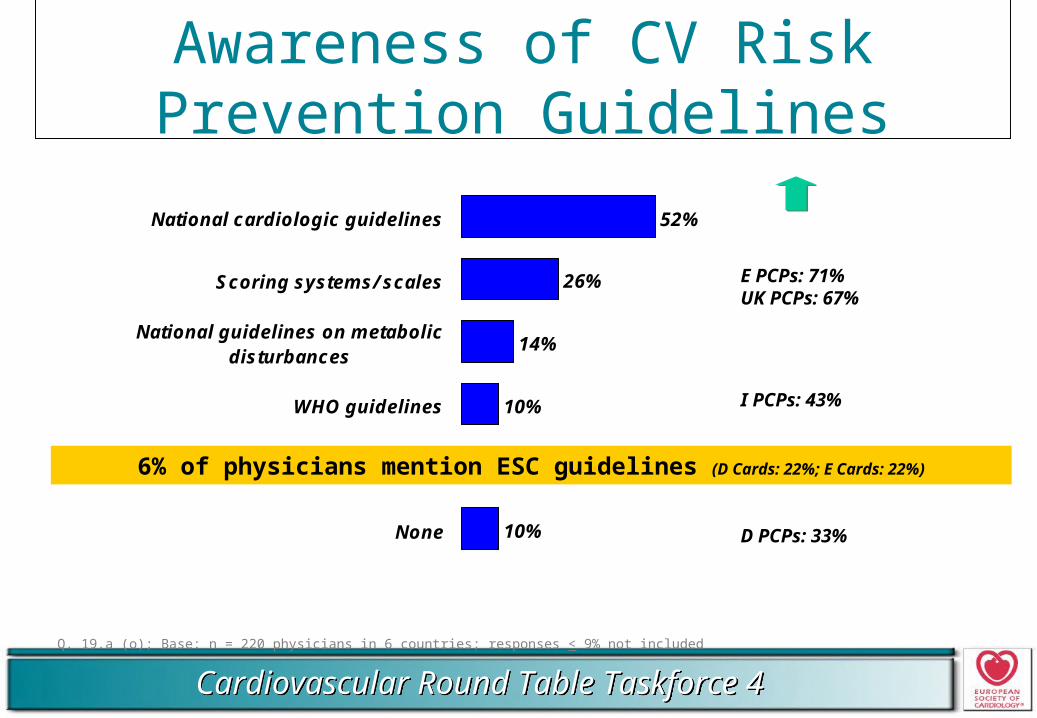
Awareness of CV Risk Prevention Guidelines
Q. 19.a (o); Base: n = 220 physicians in 6 countries; responses < 9% not included
52%
26%
14%
10%
10%
National cardiologic guidelines
Scoring systems/ scales
National guidelines on metabolicdisturbances
WHO guidelines
None
E PCPs: 71%UK PCPs: 67%
I PCPs: 43%
D PCPs: 33%
6% of physicians mention ESC guidelines (D Cards: 22%; E Cards: 22%)
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
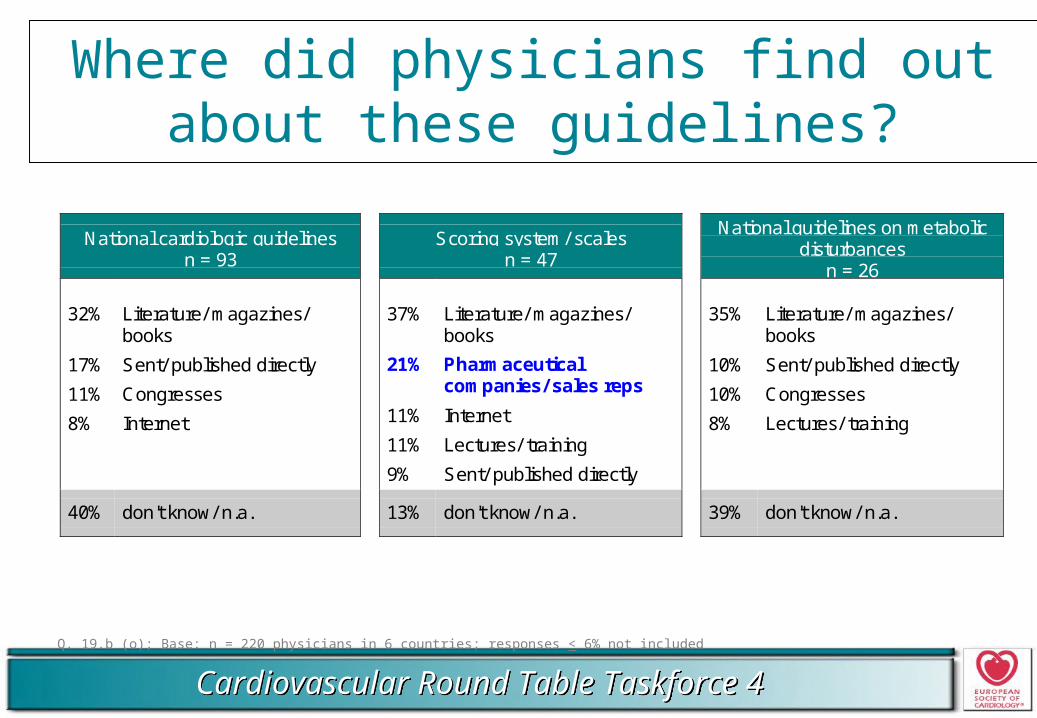
Where did physicians find out about these guidelines?
Q. 19.b (o); Base: n = 220 physicians in 6 countries; responses < 6% not included
National cardiologic guidelinesn = 93
Scoring system/ scalesn = 47
National guidelines on metabolicdisturbances
n = 26
32%
17%
11%
8%
Literature/ magazines/books
Sent/ published directly
Congresses
Internet
37%
21%
11%
11%
9%
Literature/ magazines/books
Pharmaceuticalcompanies/ sales reps
Internet
Lectures/ training
Sent/ published directly
35%
10%
10%
8%
Literature/ magazines/books
Sent/ published directly
Congresses
Lectures/ training
40% don't know/ n.a. 13% don't know/ n.a. 39% don't know/ n.a.
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
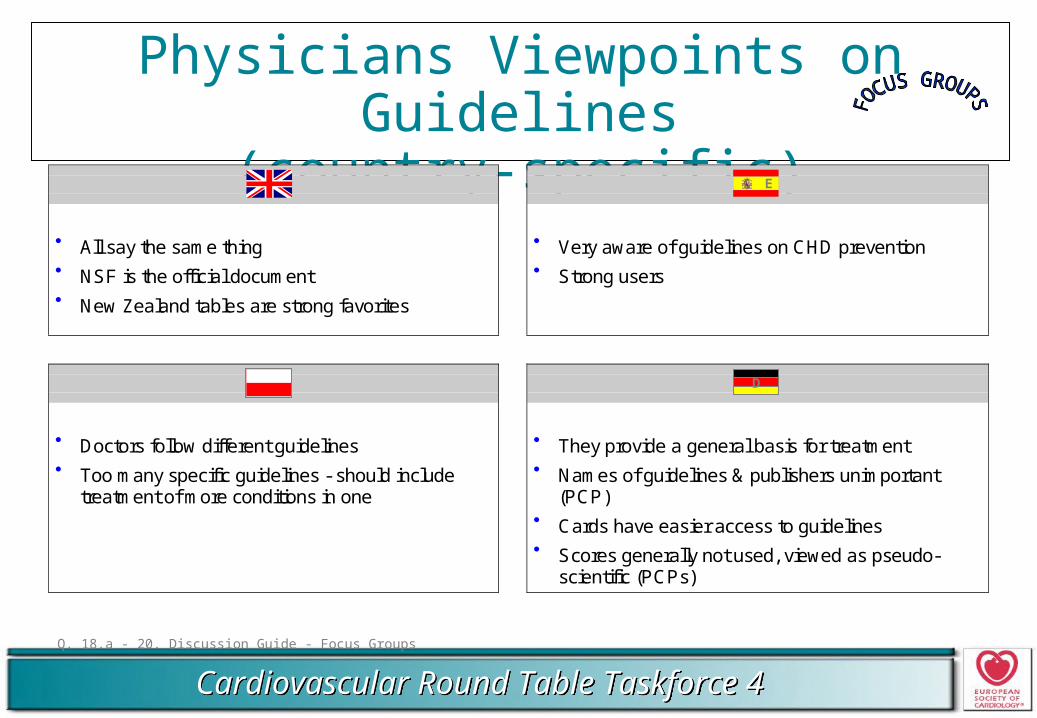
Physicians Viewpoints on Guidelines(country-specific)
Q. 18.a - 20. Discussion Guide - Focus Groups
UK E
All say the same thing NSF is the official document New Zealand tables are strong favorites
Very aware of guidelines on CHD prevention Strong users
PL D
Doctors follow different guidelines Too many specific guidelines - should include
treatment of more conditions in one
They provide a general basis for treatment Names of guidelines & publishers unimportant
(PCP) Cards have easier access to guidelines Scores generally not used, viewed as pseudo-
scientific (PCPs)
E
D
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
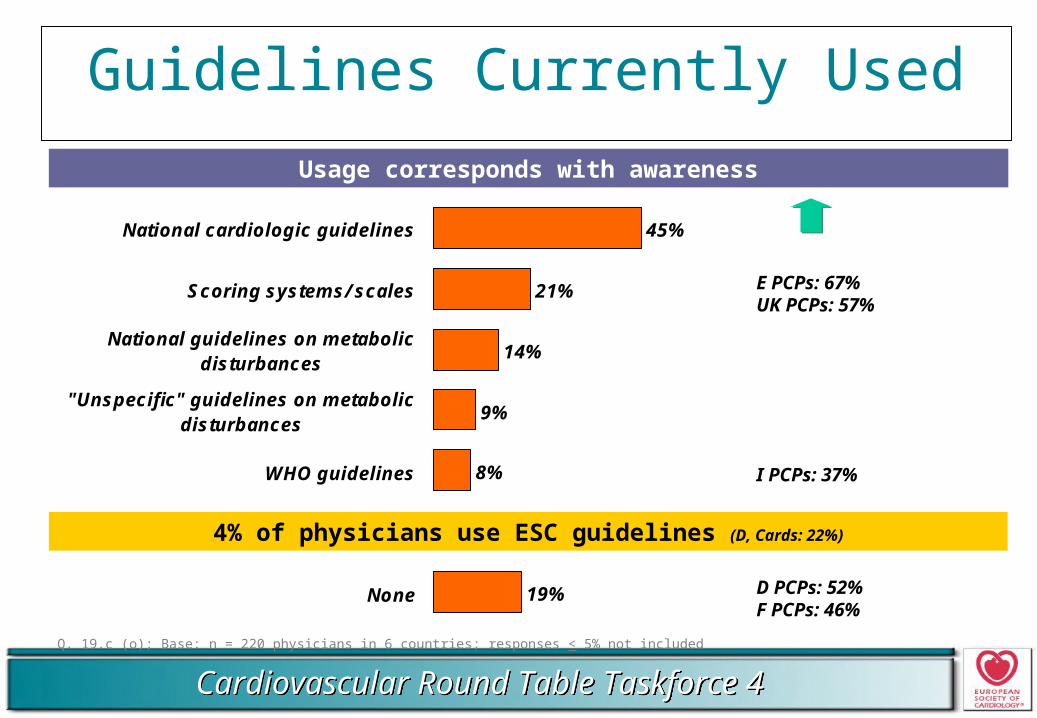
Guidelines Currently Used
Q. 19.c (o); Base: n = 220 physicians in 6 countries; responses < 5% not included
45%
21%
14%
9%
8%
19%
National cardiologic guidelines
Scoring systems/ scales
National guidelines on metabolicdisturbances
"Unspecific" guidelines on metabolicdisturbances
WHO guidelines
None
E PCPs: 67%UK PCPs: 57%
I PCPs: 37%
D PCPs: 52%F PCPs: 46%
4% of physicians use ESC guidelines (D, Cards: 22%)
Usage corresponds with awareness
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
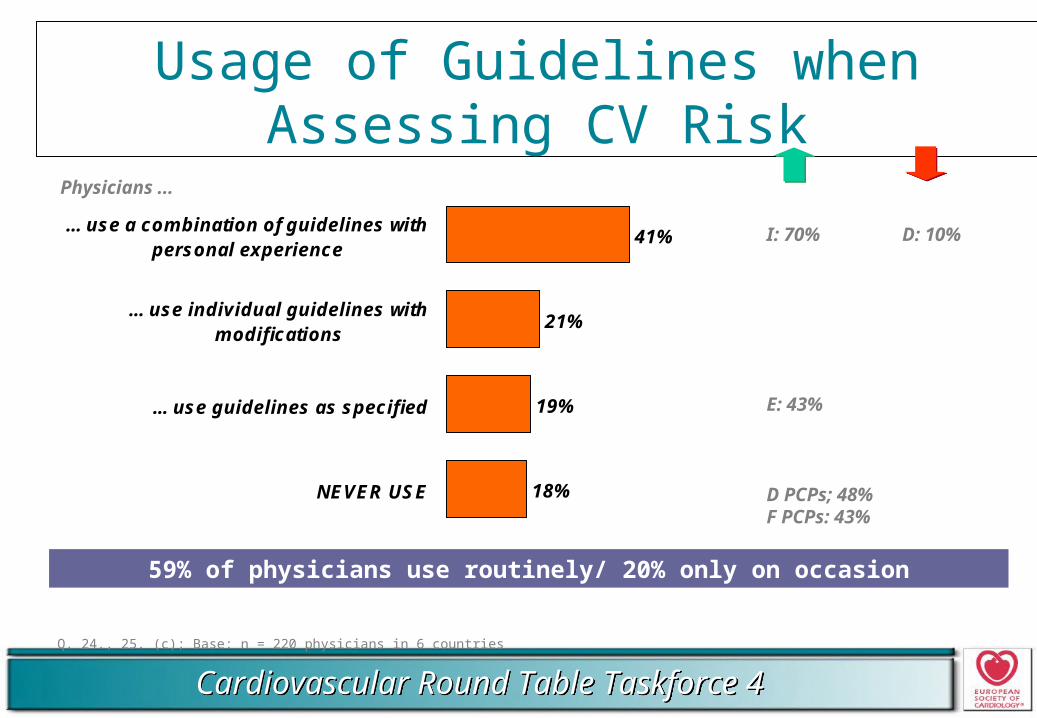
Usage of Guidelines when Assessing CV Risk
Q. 24., 25. (c); Base: n = 220 physicians in 6 countries
41%
21%
19%
18%
... use a combination of guidelines withpersonal experience
... use individual guidelines withmodifications
... use guidelines as specified
NEVER USE
Physicians ...
59% of physicians use routinely/ 20% only on occasion
I: 70% D: 10%
E: 43%
D PCPs; 48%F PCPs: 43%
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
Reasons for Not Using CV Risk Prevention Guidelines
Q. 19.c, 22. (o); Base: only physicians not using guidelines (n=34)
19% of physicians indicate not using CV risk prevention guidelines
Doesn't fit to my patients
Decide according to my own experience
Difficult to use/ values often change
Don't trust them
Not used by colleagues
Used guidelines in the past
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
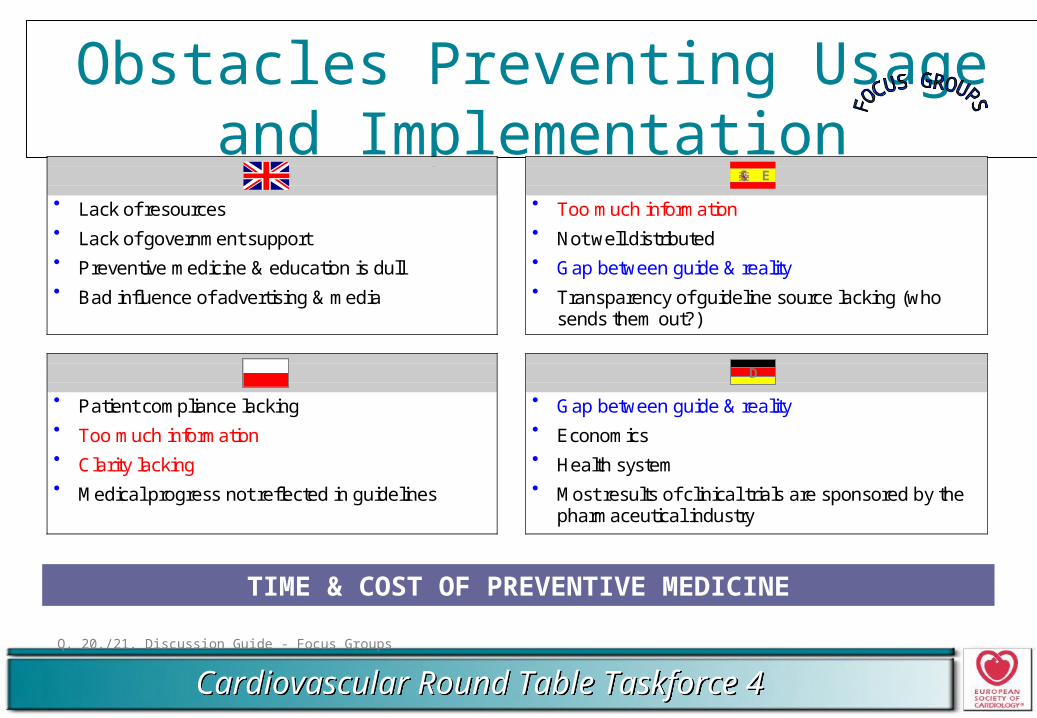
Obstacles Preventing Usage and Implementation
Q. 20./21. Discussion Guide - Focus Groups
UK E
Lack of resources Lack of government support Preventive medicine & education is dull Bad influence of advertising & media
Too much information Not well distributed Gap between guide & reality Transparency of guideline source lacking (who
sends them out?)
PL D
Patient compliance lacking Too much information Clarity lacking Medical progress not reflected in guidelines
Gap between guide & reality Economics Health system Most results of clinical trials are sponsored by the
pharmaceutical industry
E
D
TIME & COST OF PREVENTIVE MEDICINE
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
Improving Guidelines to Increase Future Use
Q. 25./26./27. Discussion Guide - Focus Groups
Easy to understand & easy to use
Include back-up data of latest scientific studies
Regular updates
Short
Realistic - possible to implement
Clear objectives - quick to implement
Solve gap between prevention (doctors) and lack of awareness (population)
Universal
Source must be credible & trustworthy
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
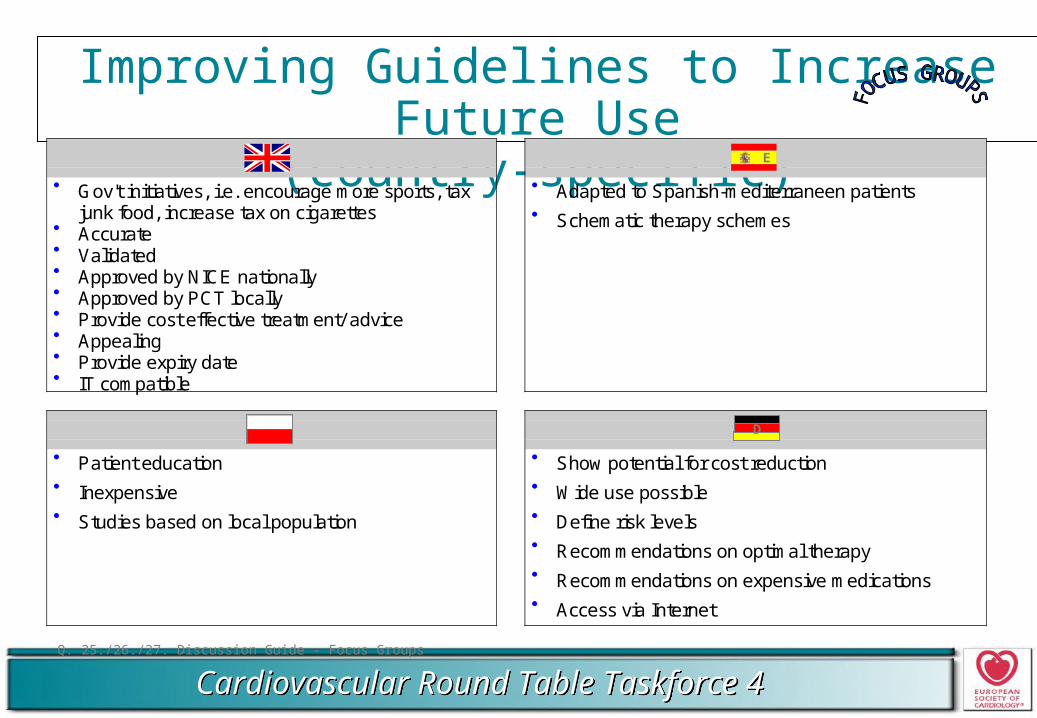
Improving Guidelines to Increase Future Use(country-specific)
Q. 25./26./27. Discussion Guide - Focus Groups
UK E
Gov't initiatives, i.e. encourage more sports, taxjunk food, increase tax on cigarettes
Accurate Validated Approved by NICE nationally Approved by PCT locally Provide cost effective treatment/ advice Appealing Provide expiry date IT compatible
Adapted to Spanish-mediterraneen patients Schematic therapy schemes
PL D
Patient education Inexpensive Studies based on local population
Show potential for cost reduction Wide use possible Define risk levels Recommendations on optimal therapy Recommendations on expensive medications Access via Internet
E
D
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
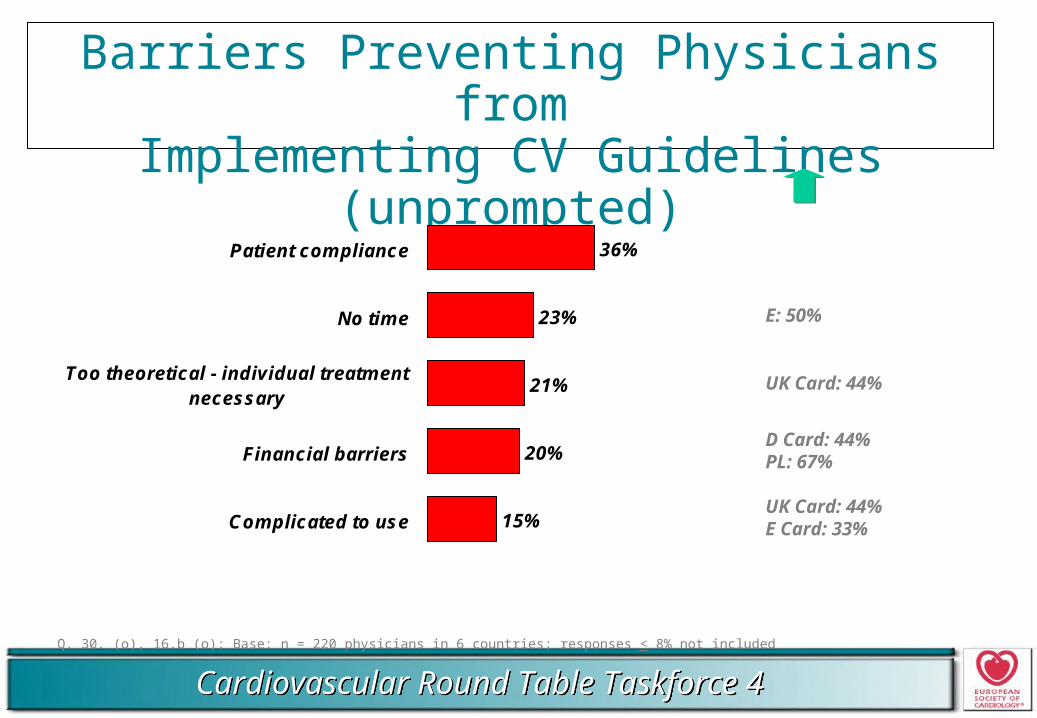
Barriers Preventing Physicians fromImplementing CV Guidelines (unprompted)
Q. 30. (o), 16.b (o); Base: n = 220 physicians in 6 countries; responses < 8% not included
36%
23%
21%
20%
15%
Patient compliance
No time
Too theoretical - individual treatmentnecessary
Financial barriers
Complicated to use
E: 50%
UK Card: 44%
D Card: 44%PL: 67%
UK Card: 44%E Card: 33%
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
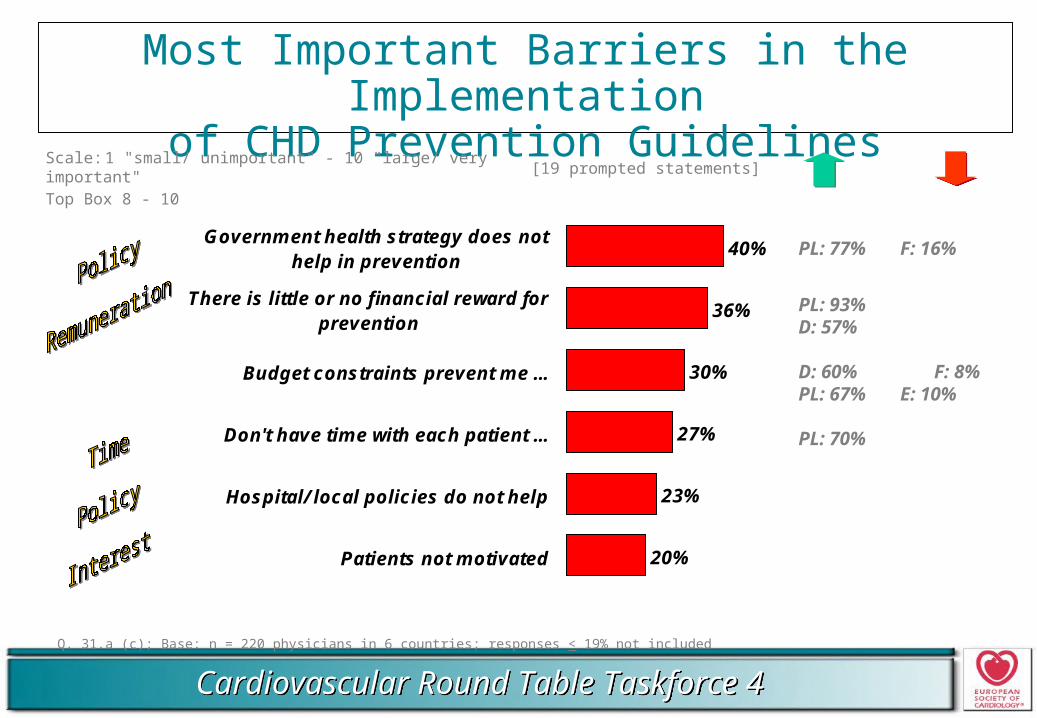
Most Important Barriers in the Implementationof CHD Prevention Guidelines
Q. 31.a (c); Base: n = 220 physicians in 6 countries; responses < 19% not included
Scale: 1 "small/ unimportant" - 10 "large/ very important"Top Box 8 - 10
[19 prompted statements]
40%
36%
30%
27%
23%
20%
Government health strategy does nothelp in prevention
There is little or no financial reward forprevention
Budget constraints prevent me ...
Don't have time with each patient ...
Hospital/ local policies do not help
Patients not motivated
PL: 77% F: 16%
PL: 93%D: 57%
D: 60% F: 8%PL: 67% E: 10%
PL: 70%
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
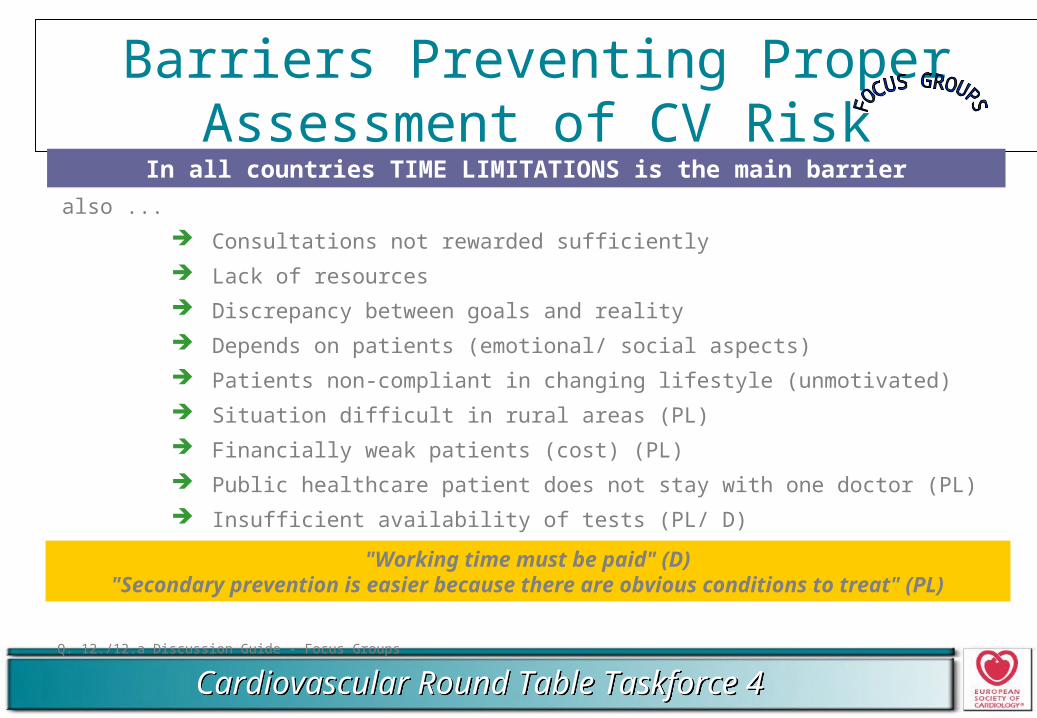
Barriers Preventing Proper Assessment of CV Risk
Q. 12./12.a Discussion Guide - Focus Groups
In all countries TIME LIMITATIONS is the main barrier
also ...
Consultations not rewarded sufficiently
Lack of resources
Discrepancy between goals and reality
Depends on patients (emotional/ social aspects)
Patients non-compliant in changing lifestyle (unmotivated)
Situation difficult in rural areas (PL)
Financially weak patients (cost) (PL)
Public healthcare patient does not stay with one doctor (PL)
Insufficient availability of tests (PL/ D)
"Working time must be paid" (D)"Secondary prevention is easier because there are obvious conditions to treat" (PL)
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
Barriers are Important because ....
Q. 31.b (c); Base: n = 220 physicians in 6 countries
There is little or no financial reward for prevention as opposed to treatment in my healthcare system
No extra payments for prevention Not enough money in the healthcare system Lack of incentives/ campaigns to support patients in prevention
Budget constraints prevent me from implementing guidelines for all patients
Budget problems with prescribing drug"... if one wanted to comply to the guidelines we would run into big problemsin regards to the budget ..."
Treatment only at high risk Impossible to implement prevention for all patients Lack of money for screening examinations
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
Barriers are Important because ....
Q. 31.b (c); Base: n = 220 physicians in 6 countries
I don't have time with each patient to undertake practical prevention Prevention is time intensive Too many patients Need time to motivate patients
"... it is difficult to find time for patients if there is a crowd of patients in thewaiting room ..."
"... I have too many patients, therefore I focus on the ones with the most important risk factors ..."
Hospital/ local policies do not help me to develop prevention No cooperation between docs & hospital No prevention in hospitals/ only treatment of urgent cases Rising costs are limiting
"... Patients always have to become really sick before anything happens andthen things become really expensive ..."
"... local policy means reduction of examination costs ...""... they are not interested because they are more involved in treating acute events ..."
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
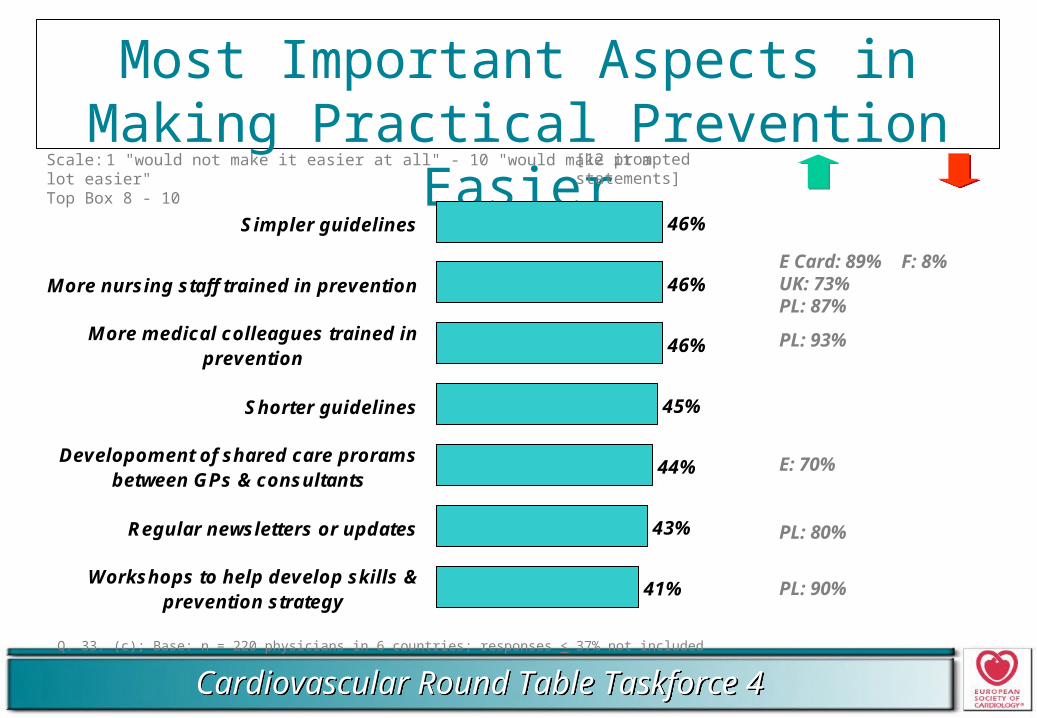
Most Important Aspects in Making Practical Prevention Easier
Q. 33. (c); Base: n = 220 physicians in 6 countries; responses < 37% not included
Scale: 1 "would not make it easier at all" - 10 "would make it a lot easier"Top Box 8 - 10
[12 prompted statements]
46%
46%
46%
45%
44%
43%
41%
Simpler guidelines
More nursing staff trained in prevention
More medical colleagues trained inprevention
Shorter guidelines
Developoment of shared care proramsbetween GPs & consultants
Regular newsletters or updates
Workshops to help develop skills &prevention strategy
E Card: 89% F: 8%UK: 73%PL: 87%
PL: 93%
E: 70%
PL: 80%
PL: 90%
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
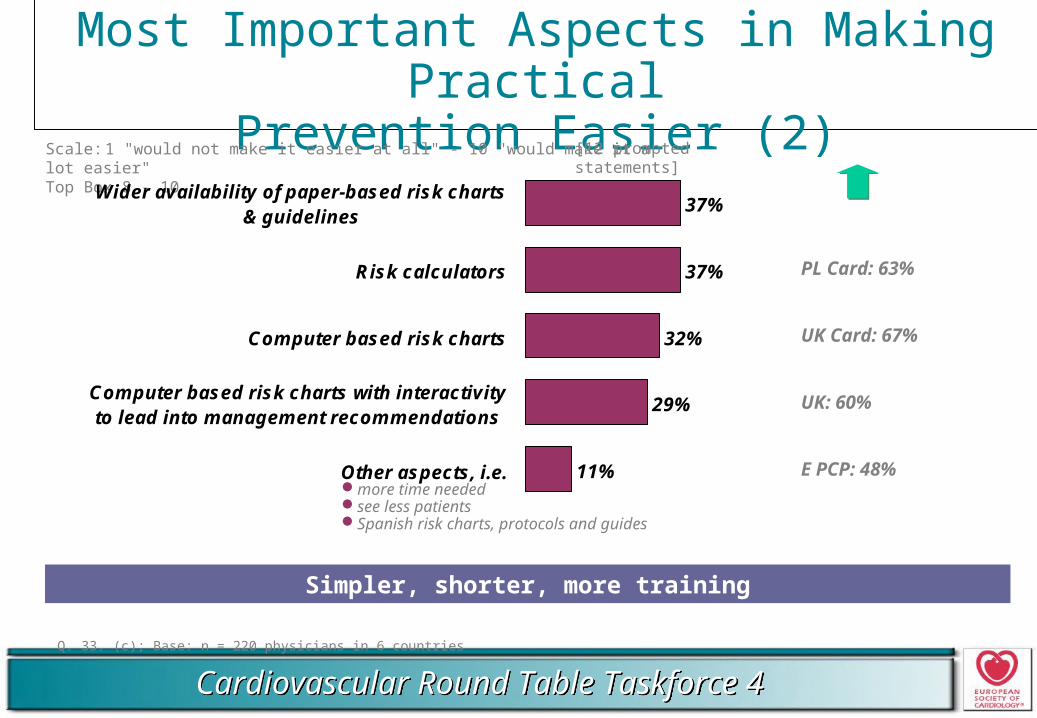
Most Important Aspects in Making PracticalPrevention Easier (2)
Q. 33. (c); Base: n = 220 physicians in 6 countries
Scale: 1 "would not make it easier at all" - 10 "would make it a lot easier"Top Box 8 - 10
[12 prompted statements]
37%
37%
32%
29%
11%
Wider availability of paper-based risk charts& guidelines
Risk calculators
Computer based risk charts
Computer based risk charts with interactivityto lead into management recommendations
Other aspects, i.e.
PL Card: 63%
UK Card: 67%
UK: 60%
E PCP: 48%
Simpler, shorter, more training
more time neededsee less patientsSpanish risk charts, protocols and guides
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
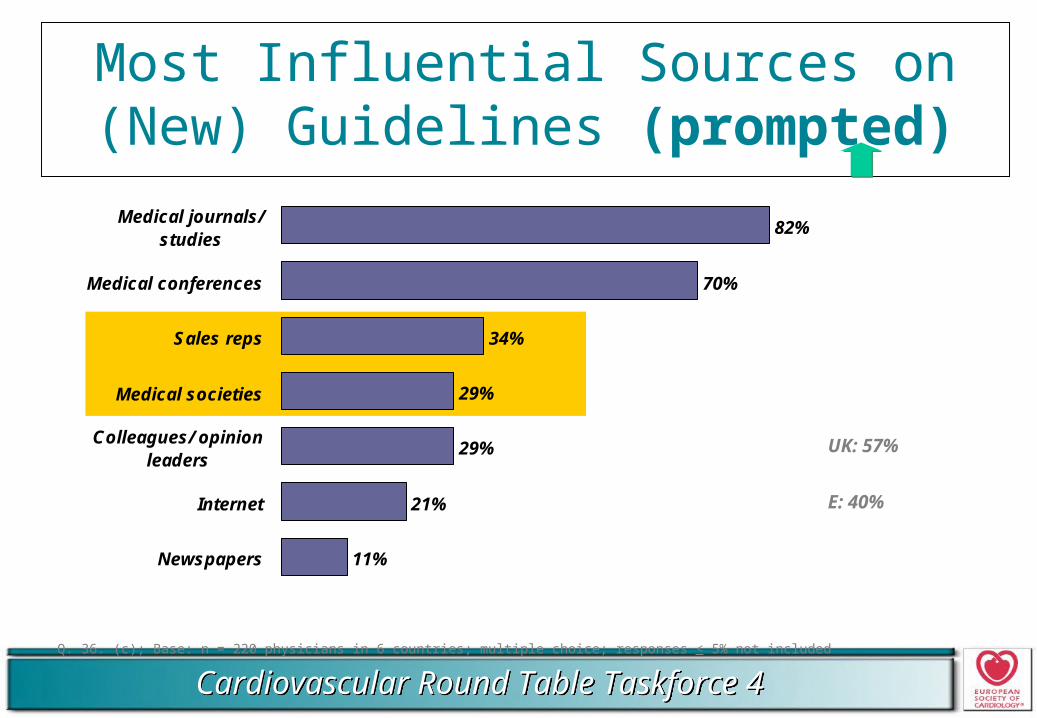
Most Influential Sources on (New) Guidelines (prompted)
Q. 36. (c); Base: n = 220 physicians in 6 countries; multiple choice; responses < 5% not included
82%
70%
34%
29%
29%
21%
11%
Medical journals/studies
Medical conferences
Sales reps
Medical societies
Colleagues/ opinionleaders
Internet
Newspapers
UK: 57%
E: 40%
Cardiovascular Round Table Taskforce 4Cardiovascular Round Table Taskforce 4
SUMMARY
CHD ASSESSMENT• Awareness that global risk approach is necessary to assess risk, yet physicians don’t fully understand the principle and they revert back to individual risk factor assessments
GUIDELINES• National guidelines are the predominant reference for recommendations• Uniform recognition of guidelines seem linked to a clearer source and consistency of guidance• Current use & understanding of guidelines does not necessarily translate into an understanding of the principles of global risk• Scoring systems seem to convey global risk more directly
Many BARRIERS TO IMPLEMENTATION
FUTURE AREAS OF FOCUS• Different countries may require focus on slightly different areas of implementation• Improving implementation goes beyond just developing a new set of guidelines