Embed Size (px)
Citation preview
DOCUMENT CONTROL:
Version: 10
Ratified by: Quality and Safety Sub Committee
Date ratified: 3 May 2017
Name of originator/author: Nurse Consultant, AMHS
Name of responsible committee/individual:
Clinical Quality Group
Date issued: 15 May 2017
Review date: May 2020
Target Audience Clinical Staff, Clinical Managers, Modern Matrons, Team Leaders.
Care Programme Approach (CPA)
Policy
Page 2 of 26
Section
CONTENTS
Page No
1 INTRODUCTION 4
2 POLICY CONTEXT 4
3 PURPOSE 5
4 SCOPE 5
5 RESPONSIBILITIES, ACCOUNTABILITIES AND DUTIES 5
5.1 Board of Directors 5
5.2 Chief Executive 5
5.3 Locality Managers, Service Managers, Modern Matrons and Team Managers
6
5.4 Care Coordinators 6
5.5 All Other Clinical Staff 6
6 PROCEDURE/IMPLEMENTATION 7
6.1 Assessment 7
6.1.1 Parenting responsibility 8
6.1.2 Physical health 8
6.1.3 Carers 9
6.1.4 Medication 9
6.1.5 Substance Misuse 9
6.2 CPA Eligibility 10
6.3 The Care Coordinator/Lead Professional 10
6.3.1 Allocating a Care Coordinator/Lead Professional 11
6.3.2 Change of Care Coordinator/Lead Professional 11
6.3.3 In-patient Admission 11
6.3.4 Role of the Care Coordinator 12
6.3.5 Role of the Lead Professional 13
6.4 Care planning 13
6.4.1 Inpatient Leave 15
6.4.2 Advance Statements and Advance Decisions 16
6.4.3 Self-directed care, Direct payments and Personal Budgets 16
6.5 CPA and None CPA Reviews 17
6.5.1 Planning a CPA/None CPA meeting 18
6.5.2 Who should be involved 18
6.5.3 Conducting CPA/None CPA Review Meeting 19
6.5.4 Discharge from CPA 20
6.5.5 Disengagement 20
6.6 Transfer 20
6.6.1 Internal Transfer 20
Page 3 of 26
Section
CONTENTS
Page No
6.6.2 Transfers Out of Area 21
6.6.3 Transfers into Area 21
6.6.4 Funding Responsibilities 21
6.7 Information Sharing 22
6.7.1 Patient information 22
6.7.2 Carer information 22
6.7.3 GP information 23
6.7.4 Other Agencies 23
7 TRAINING IMPLICATIONS 23
8 MONITORING ARRANGEMENTS 23
9 EQUALITY IMPACT ASSESSMENT SCREENING 24
9.1 Privacy. Dignity and Respect 24
9.2 Mental Capacity Act 24
10 LINKS TO ANY ASSOCIATED DOCUMENTS 25
11 REFERENCES 25
12. APPENDICES (none) 26

Page 4 of 26
1 INTRODUCTION
The Care Programme Approach (CPA) is an overarching system for co-ordinating the care of people with mental disorders. It requires close engagement with patients and their carers and includes arrangements for assessing, planning, delivering and reviewing care. Central to CPA is the CPA care plan which aims to ensure a transparent, accountable and coordinated approach to meeting wide ranging physical, psychological, emotional and social needs which are associated with a person’s mental disorder. The CPA also requires the clear identification of a named individual, the Care Co-ordinator, who has responsibility for co-ordinating the preparation, implementation and evaluation of the CPA care plan. The CPA should be used in secondary and tertiary mental healthcare to assess, plan, review and coordinate the range of treatment, care and support needs of those people in contact with secondary mental health services who have complex needs. CPA should include active involvement of and engagement with the patient at the heart of the process and focus on reducing distress and promoting social inclusion and recovery. The key principles of the CPA are applicable to all patients, even those who require only a uni-disciplinary intervention. All people receiving services have the right to a thorough assessment of their needs, the development of a care plan and a review of that care with the professionals involved in their care. This is good professional practice.
2 POLICY CONTEXT
CPA was introduced in 1991 to establish a multi-agency approach to health and social care, setting out arrangements for the care of people with mental health problems in the community. CPA aims to facilitate closer and integrated working, enabling a co-ordinated approach to care delivery and the recovery process. Additional care standards were also detailed in the 1999 Mental Health National Service Framework. The four main elements of the CPA process are: Systematic arrangements for assessing the health and social needs of
people accepted into specialist Mental Health Services The formulation of a care plan, which identifies the health and social
care needs, and support required from a variety of providers The appointment of a care co-ordinator to keep in close touch with the
patient and to monitor and co-ordinate care Regular review and, where necessary, agreed changes to the care plan. In October 1999 the Department of Health (DH) published ‘Effective Care Co-ordination in Mental Health Services – Modernising the Care Programme Approach’ and broadened the application of the CPA to all adults of working

Page 5 of 26
age who are under the care of the Secondary Mental Health Services (health and social care), regardless of setting. It stated that CPA is Care Management for those of working age in contact with specialist mental health and social care services. All agencies are expected to integrate their approach across health and social care for people with mental health problems. ‘Refocusing the Care Programme Approach: Policy and Positive Practice Guidance’ (DH, March 2008) was the outcome of a national review which had the intention of ensuring the national policy is more consistently and clearly applied and that unnecessary bureaucracy is removed. The revised (2008) national CPA policy stipulated that where it is ‘silent’ on a particular issue then the previous (1999) policy should be referred to. The essence of effective care co-ordination is sound professional judgement and practice. The implementation of any care co-ordination process can be no substitute for this but is intended to support good professional practice. This policy should be read in conjunction with other relevant national and local policies and guidance.
3 PURPOSE
This policy sets out how clinical assessment, care planning, review, transfer and discharge processes should be carried out according to best practice, within (but not limited to) the context of the CPA.
4 SCOPE
This policy is applicable to all Adult Mental Health (including older adults), Learning Disability and Forensic Services within The Trust, and to all staff working in those services.
5 RESPONSIBILITIES, ACCOUNTABILITIES AND DUTIES 5.1 Board of Directors
It is the duty of the Board of Directors to oversee that all individuals receiving treatment, care and support from Secondary Mental Health Services in the Trust receive high quality care based on an individual assessment of the range of their needs and choices. The Board of Directors delegates authority to the Chief Executive.
5.2 Chief Executive
The Chief Executive has overall responsibility for the implementation of this policy, and in turn this responsibility is delegated to the Directors and Senior Managers.
Page 6 of 26
5.3 Locality Managers, Service Managers, Modern Matrons and Team Managers
Managers and Modern Matrons are responsible for: Overseeing the implementation of this policy within their areas of
responsibility Raising awareness of this policy and its contents with any staff they
manage Bringing any issues which may affect the implementation of this policy to
the attention of the relevant assistant director Reporting any concerns that clinical staff may bring to their attention
which relate to operation of this policy Exploring unmet needs as brought to their attention by Care
Coordinators, assessing the case and specifying the action or process to be followed by the service in an attempt to meet the needs of the patient
Monitoring the implementation of this policy Making any necessary arrangements for their staff to attend any training
in relation to this policy Ensuring regular audit is undertaken and the results acted upon Providing regular supervision
5.4 Care Coordinators
Care Coordinators are responsible for: Implementing this policy and standards effectively Fulfilling the duties of the Care Coordinator role as outlined in this and
other related policies, to the required professional standards of their particular discipline
Bringing any issues which may affect implementation to the attention of their line manager
Identifying any unmet needs as part of the process of completing the assessment and accounting for this within the care plan
Informing the relevant manager when an identified action or intervention cannot be delivered, for example because of resource or availability problems
Identifying learning needs and attending relevant training Undertaking regular supervision
5.5 All Other Clinical Staff
All other clinical staff are responsible for: Implementing this policy effectively Bringing any issues which may affect implementation to the attention of
their line manager.
Page 7 of 26
6 PROCEDURE / IMPLEMENTATION
Assessment is used to identify and evaluate an individual’s presentation. It should also identifying needs for health and social care and should explore an individual’s goals, strengths and aspirations. The assessment processes, including safety and risk assessments, provide the basis for effective care planning and the evidence that supports all decision making.
6.1 Assessment
Everyone referred to Secondary Mental Health Services should have an assessment of their mental health needs. Patients and their carers (if appropriate) should be involved fully in the assessment. Patients with communication difficulties, including those whose first language is not English, should have communication support arranged in accordance with the Trust’s Interpreters Policy. Staff should also familiarise themselves with the NHS England Accessible Information Standard. Accessible Information aims to ensure that people with a disability, impairment or sensory loss get information about their health and care which they can read and understand (for example in easy read, braille or via email) and communication support if they need it (for example British Sign Language (BSL) interpretation). The assessment process should include full assessment of any risk to the patient or others, and this should be documented in the appropriate section of the electronic patient record (see the Trust’s Clinical Risk Assessment and Management Policy). The Mental Health National Service Framework sets out the range of issues and needs a multi-disciplinary health and social care assessment (and care plan) may cover depending on need. These include: Psychiatric, psychological and social functioning, including impact of
medication Risk to the individual and others, including contingency and crisis
planning Needs arising from co-morbidity (including substance misuse – see the
Trust’s Dual Diagnosis Policies) Personal circumstances including family and carers Housing needs Financial circumstances and capability Employment, education and training needs Physical health needs Equality and diversity issues Social inclusion, social contact and independence including a
comprehensive social care assessment Spiritual needs
Page 8 of 26
The assessment should also consider any safeguarding issues (see the Trust’s Safeguarding Adults Policy and Safeguarding Children Policy). The assessment and planning process should aim to meet the patient’s needs and choices and not just focus on what professionals and services can offer. It should address a person’s aspirations and strengths as well as their needs and difficulties. Any assessment should include consideration of social care needs and should be further assessed under the criteria set out in the care act 2014. All possible care and treatment options should be explained to the patient and their carer (where appropriate) enabling them to make informed decisions about their future care. Once the assessment is complete a decision should be made regarding the patients CPA eligibility. The outcome of the assessment must be communicated to the individual (in a way that they will understand) and the referrer promptly. This should include the patients CPA eligibility (see section 6.1 of this policy). Where a patient is to be offered on-going support from Secondary Mental Health Services a FACE risk assessment, care plan and mental health cluster tool should also be completed.
6.1.1 Parenting Responsibilities
For a family with children and young people under 18, an episode of mental ill-health can represent a significant crisis, not just in terms of a parent’s individual mental health but in family life overall. Assessment, including risk assessment, should assess the potential or actual impact of mental health on parenting, the parent and child relationship, the child and the impact of parenting on the adult’s mental health and what appropriate support might look like and how it can be accessed. Further guidance on this can be found in the Care Programme Approach Briefing: Parents with mental health problems and their children April 2008. Please consider the Trust’s Safeguarding Children Policy where appropriate.
6.1.2 Physical Health
The links between mental ill health and physical ill health are well documented. Research has shown that people with mental health problems have higher rates of physical illness, resulting in increased rates of morbidity and premature mortality. Certain medication, poor diet and a lack of exercise can cause or compound physical health risks. The patient’s physical health and well-being should be assessed using the electronic Physical Health Assessment (see the Trust’s Physical Health and
Page 9 of 26
Well-being Policy). 6.1.3 Carers
The assessment should take account of the needs of carers (including children who provide care) of patients, and must comply with The Carers and Disabled Children’s Act 2000, the National Service Framework for Mental Health, the National Service Framework for Older People, the NHS Plan and the standards in Caring about Carers. Carers should: Be identified on the patient record Be offered an assessment of their caring, physical and mental health
needs, repeated on at least annually Have their own written support plan developed in partnership with them Understand the patient’s care plan (subject to that person’s permission) Be offered information about or signposting to carer support services Know how to contact the Care Coordinator if they need to. Be offered separate carer support if appropriate Have their communication needs considered where appropriate in line
with the Trust Interpreters Policy and the NHS England Accessible Information Standard.
6.1.4 Medication
The assessment should include a thorough assessment of medication needs, which must be clearly documented in the patient record. It is essential that everyone involved in the care of the patient understands who prescribes the medication, where it is obtained from, the instructions for its administration, and what other medications are being prescribed for physical health problems. Specialist mental health pharmacists should, where possible, be involved in care planning for patients with complex medication needs. For guidance relating to medication reconciliation staff should refer to the Trust policy for Safe and Secure Handling of Medicines and NICE Guidance [NG5] Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes.
6.1.5 Substance Misuse
Any substance misuse past and present should be taken into account during the assessment. It should also be captured in patients risk assessment and care plan including where appropriate plans for education and harm reduction. Care Coordinators/lead professionals should routinely explore substance misuses with their patients, and should capture the type, method of administration/consumption, quantity and frequency of use.
Page 10 of 26
A patient’s current use of substances should be considered when deciding their CPA eligibility. For patients with complex, severe and enduring mental health illness and a co morbid substance misuse it would be appropriative for Mental Health Services to lead in their care, with supplementary specialist support offered by substance misuse services.
6.2 CPA Eligibility
CPA eligibility is not the same as eligibility for Secondary Mental Health Services or Social Care. The CPA should be used for individuals with a serious mental health problem including personality disorder, and are high risk of suffering deterioration in their mental condition which may include people with a learning disability and who need: Multi-agency support Active engagement Intense intervention Support with dual diagnoses
This will include (but is not limited to): Patients admitted to an inpatient unit Most people who are entitled to after-care under section 117 of the Act Patients subjected to guardianship orders Patients subject to Community Treatment Order (CTO) Some patients with parenting responsibilities Vulnerable adults (as defined in the Safeguarding Adults Policy) Patients with co-morbid substance misuse Patients with multi- agency involvement Patients with significant risk history including risk to self and/or others. Patients who have significant caring responsibilities Patients in unsettled accommodation Patients who have a learning disability who present with serious
irresponsible aggressive behaviour posing a risk to themselves of others
Decisions and reasons not to include individuals from the groups identified above should be clearly documented in care records. Once a decision as regards CPA eligibility has been made, the patient’s CPA status (that is, ‘CPA’ or ‘non CPA’) should be recorded in the appropriate place on the electronic patient record, and this should kept updated at all times.
6.3 The Care Coordinator/Lead Professional
The Care Coordinator role is one of the key elements of the CPA, and may be carried out by any registered health or social care professional. He or she must be able to support patients with multiple needs to access the services
Page 11 of 26
they require, and have the professional skills and authority to manage the coordination of the care package.
6.3.1 Allocating a Care Coordinator/Lead Professional
Once a patient is offered and accepts support from Secondary Mental Health Services they should be allocated a Care Coordinator/Lead professional.
The needs and wishes of the patient regarding who should be Care Co-ordinator and the skills needed for the role should be taken into account when allocating the Care Coordinator. Allocation should reflect any issues around gender, culture or religious needs. If there are any specific issues affecting the choice of Care Coordinator, these should be documented in the patient record. In community services the Care Coordinator should, wherever possible, be identified prior to the first CPA meeting. Where this hasn’t been done, allocation of a Care Coordinator should be an item on the meeting agenda. Ultimate responsibility for allocation rests with the team manager, and the team manager will be the Care Coordinator by default until another staff member is allocated this role.
Once agreed, the clinical record should identify the Care Coordinator.
6.3.2 Change of Care Coordinator/Lead professional
During periods of staff absences, there may be a need for other members of the care team to cover for the Care Coordinator/Lead professional, without requiring any formal transfer of Care Coordinator/Lead Professional responsibilities. Clear communication and healthcare records are therefore vital. However there may be a requirement for a change of Care Coordinator/Lead Professional during an episode of care, either due to patient choice or other circumstances. If this is a planned event, a formal handover of care will take place between the existing and new Care Coordinator/Lead Professional, with the involvement of the patient, and the carer where relevant. If this is unplanned, the role of Care Coordinator/Lead Professional will default to the team manager until a new Care Coordinator/Lead Professional can be allocated. The reasons for the change must be documented in the electronic patient record, and explained to the patient as far as possible.
In all circumstances, the team manager is responsible for ensuring that the patient’s needs are met at all times.
6.3.3 In-patient Admission
Most people being admitted to acute inpatient wards will meet the criteria for CPA, and the patient’s CPA status should be recorded to reflect this on
Page 12 of 26
admission. Where a patient is not put on CPA on admission, the reasons for this must be clearly documented in the electronic patient record.
Where an individual is admitted to hospital and a community based Care Coordinator is already allocated their worker will retain the role. It is the responsibility of the named nurse to initiate contact with the Care Coordinator, to jointly review the existing care plan. Good communication between Inpatient and Community Services should be maintained throughout the admission.
Where an individual not currently known to the Trust Mental Health Services (or known and not currently subject to CPA) is admitted to an inpatient unit and they meet the criteria (outlined in section 6.2 of this policy) for CPA, then the Named Nurse will assume Care Co-ordinator responsibilities. If the individual requires on-going care from a community team, then care co-ordination will transfer at the earliest opportunity, in order that the new Care Coordinator can facilitate engagement, involvement and discharge planning. If at the point of discharge no Care Coordinator has been identified, this role defaults to the manager of the receiving team. Under all circumstances, the receiving team should be involved in the discharge planning. Where the patient has a Lead Professional involved in their care the Lead Professional must maintain contact with the patient and the inpatient care team and should be involved in discussions relating to care treatment and discharge. The Lead Professional will retain and reprise their role on discharge unless alternative arrangements relating to a change of Lead Professional or transfer to a Care Coordinator have been made. Following admission to hospital a CPA review should be convened at the earliest opportunity.
6.3.4 Role of the Care Coordinator
The role of the Care Coordinator (as set out in the Rethink Care Programme Approach Factsheet) is to: Fully assess the patient’s needs Write a care plan in collaboration with the patient, which shows how the
NHS and other organisations will meet their needs Regularly review the plan with the patient to check the patient’s progress This will include: Actively engaging and building a therapeutic relationship with the patient,
and family or carers as appropriate Providing education and information, including information about
treatment options, to support patients to make informed choices Working with the patient to promote recovery and reduce crises and in-
patient admissions
Page 13 of 26
Liaising with other services involved in the patient’s care, including Primary Care Services; gathering all relevant patient information and sharing information as appropriate, in accordance with the Trust’s Information Governance Policy
Resolving and / or escalating disputes related to patient care Meeting all statutory responsibilities under the Mental Health Act
(including section 117 aftercare) Meeting all statutory responsibilities under the Mental Capacity Act Maintaining all clinical records to a high standard The Care Coordinator should also be aware of carer needs, and support the carer to continue providing care. Carers should be informed of their right to a carer’s assessment.
6.3.5 Role of the Lead Professional
Patients not subject to CPA should be allocated a Lead Professional. The Lead Professional has responsibility for:
Overseeing the package of care provided by Secondary Mental Health Services and ensuring that the on-going process of assessment, care planning and review is done in collaboration with the patient and carer (where appropriate).
Identifying carers involved and ensure they are aware of their own right to an assessment of need.
Liaising as necessary with others involved in the patients care.
Ensuring that all transfers of care, both internal and external are agreed and overseen, and that all relevant information is shared in an appropriate and timely manner.
6.4 Care Planning
The care plan aims to ensure a transparent, accountable and coordinated approach to meeting wide ranging physical, psychological, emotional and social needs which are associated with a person’s mental disorder. Any need identified in the assessment or risk assessment should be addressed in the care plan. Included with the care plan are:
A treatment plan which details medical, nursing, psychological and other
therapeutic support for the purpose of meeting individual needs promoting recovery and/or preventing deterioration.
Details regarding any prescribed medications Details of any actions to address physical health problems or reduce the
likelihood of health inequalities Details of how the person will be supported to achieve their personal goals Support provided in relation to social needs such as housing, occupation
and finances Support provided to carers
The patient’s own caring responsibilities Actions to be taken in the event of a deterioration of a person’s presentation

Page 14 of 26
Guidance on actions to be taken in the event of a crisis.
The Care Coordinator/Lead Professional (or named nurse on inpatients) is responsible for coordinating the care plan and recording it in the electronic patient record. Other members of the care team have a responsibility to communicate and liaise with the Care Coordinator/Lead Professional/Named Nurse regarding the delivery of the agreed care plan, including any difficulties with or changes to the agreed plan. An individual patient’s care plan will be based on the assessment of their health and social care needs, including risk factors identified through the risk assessment process, with the patient, and where appropriate the carer(s) being central to the process. Care plans should focus on patients' strengths and aspirations as well as their needs and choices and promote social inclusion and recovery. Care plans should recognise the diverse needs of patients, reflecting their cultural and ethnic background as well as their gender and sexuality. The care plan should be developed by the Care Coordinator/Lead Professional (or, in inpatient settings, by the Named Nurse in collaboration with the Care Coordinator/Lead Professional) with the patient, carers and other professionals where relevant. If the patient is too unwell to engage in the care planning process and does not have an advance directive in place, they should be involved at the earliest possible opportunity.
The care plan is likely to involve consideration of: Continuing mental healthcare The psychological needs of the patient and, where appropriate, of their
carers physical healthcare Daytime activities or employment Appropriate accommodation Identified risks and safety issues Any specific needs arising from, e.g. co-existing physical disability,
sensory impairment, learning disability or autistic spectrum disorder Any specific needs arising from drug, alcohol or substance misuse (if
relevant) Any parenting or caring needs Social, cultural or spiritual needs Counselling and personal support Assistance in welfare rights and managing finances Involvement of authorities and agencies in a different area, if the patient
is not going to live locally Involvement of other agencies, for example the probation service or
voluntary organisations (if relevant) For a restricted patient, the conditions which the Secretary of State for
Justice or the first-tier Tribunal has – or is likely to – impose on their conditional discharge, and
Contingency plans (should the patient’s mental health deteriorate) and crisis contact details

Page 15 of 26
It is important to acknowledge that on occasions there may be disagreements with the patient about the care planned. In these circumstances, it is important to record the reasons for disagreement. On-going discussion and negotiation should seek to resolve such disagreements.
Care plans completed on discharge from in-patient care must include specific plans for follow-up within seven days of discharge (measured as 7 x 24 hours from the time and date of discharge). Discharge care plans should be reviewed within one month of discharge. All care plans must include explicit crisis and contingency plans. A good crisis and contingency plan will include all necessary information to manage the situation, to prevent harm and distress caused by the escalation of problems. It will describe a staged approach to crisis and contingency management and include: Signs that things are going wrong (relapse indicators and triggers) Patients own resources for preventing any difficult situations or
distressing experiences from escalating (e.g. self-management skills and close support networks)
Where the situation worsens, details of other networks and resources including the person’s usual care team
If early de-escalation work is not successful, details of how to manage an emergency with the use of resources outside of the person’s usual care team, such as the Crisis Team, or possibly police, ambulance or hospital services
The crisis and contingency plan must include all relevant contact details. In the event of a crisis, if the patient contacts the care team it is their responsibility to assess the situation and respond appropriately. Care plans must include contact numbers for services both within and out of hours. Individual communication needs should be taken into consideration as regards how the care plan is presented. Once the care plan is completed, the patient should be offered a copy and this should be recorded in the patient record (including if the patient declines), ensuring that the patient fully understands the content of the plan.
6.4.1 Inpatient Leave
In circumstances when a patient goes on leave from in-patient care, whether that is short term or long-term extended leave, an appropriate care plan for the leave period must be in place, including a crisis and contingency plan. The responsible clinician or their deputy should be immediately informed of any significant deterioration or breakdown of the plan. Regular contact should be maintained with patients on leave. This responsibility rests with the Inpatient Team; however it may be delegated to the Community Team, in discussion and agreement with them. Consideration

Page 16 of 26
should be given to informing the GP of the leave, where this is for an extended period. Where it is not possible to contact patients on leave the Consultant Psychiatrist and Care Team must consider what action to take based on their knowledge of the patient and any risks. The Responsible Clinician should consider formally recalling the patient from leave. If appropriate the Trust Patients who are Absent or Missing without Leave (AWOL) Policy should be followed.
6.4.2 Advance Statements and Advance Decisions to Refuse Treatment
The Mental Capacity Act (MCA) 2005 came into force in October 2007 and provided a legal framework for acting and making decisions on behalf of vulnerable people who lack the mental capacity to make specific decisions for themselves. The MCA provides a statutory framework to empower and protect such individuals. It makes it clear who can take decisions, in which situations and how they should go about this. It also enables people to plan ahead for a time when they may lose capacity. An Advance Statement is an expression of wishes by a patient setting out how they would prefer to be cared for/treated if they lose the capacity to make decisions for themselves. Such expressions of wishes/preferences must be taken into account when considering an incapacitated patient's best interests, but are not legally binding. An Advance Decision is a refusal to accept certain treatments in the future if specified circumstances arise once the person has lost the capacity to make the specific decision. Advance Decisions are governed by the MCA 2005 and, if valid and applicable to the circumstances arising, are legally binding. Please see the Trust Policy for Advance Statements and Advance Decisions for further details and guidance.
6.4.3 Self-directed Care, Direct Payments and Personal Budgets
Requirements for the assessment for community care services under The Care Act 2014 does not sit separately from CPA. The Local Authority’s responsibilities under the requirements of this Act are met through the defined processes. CPA aims to promote effective liaison and communication between agencies, thereby managing assessed risk, and meeting the individual needs of people with mental health problems so that they are better able to function in society. The patient will have as much influence as possible in determining how they will be supported. Where they need help to manage this arrangement, this will be provided as an essential part of their support plan.
Page 17 of 26
6.5 CPA and None CPA Reviews
Reviews monitor and evaluate the effectiveness of the care plan and focus on how the needs of the patient can continue to be met. The CPA review also provides opportunity to deliver statutory responsibilities in relation to mental health legislation. Reviews should take place at least annually. Please note that the patient, carer or member of the care team can request a review of the care plan at any time. If the team decide that a review is not necessary the reasons for this must recorded and explained to the patient or carer. Circumstances where an urgent review should be considered: The patient wishes to withdraw from a significant component of their
care plan The patient discharges themselves from hospital against medical advice,
or threatens to do so There are specific circumstances where informal carers or relatives
should be told if they are likely to be exposed to violent behaviour or harm (with or without consent to protect an individual at risk of harm) this should be documented in the notes: the risk; the information; the assessment and the decision.
There is a major change in the patient’s mental health, personal or social circumstances include admission to hospital.
The Care Coordinator/Lead Professional and Care Team should tailor reviews to the circumstances of the individual patient. When deciding which review option is appropriate, staff should consider factors such as risk behaviour, the complexity of the care plan and the wishes of the patient. The following review options could be considered: A meeting between the Care Coordinator/Lead Professional and patient
to review the key elements of the care plan (within with a routine, planned contact);
A meeting between the Care Coordinator and patient, with others contributing by phone or in writing;
A full Multi-Disciplinary Team (MDT) review involving all appropriate professionals
MDT in which patient and carer(s) participate.
For patients with children or regular access to children where there is an allocated children’s worker, the worker should be routinely invited to attend review meetings. It is essential that CPA meetings are distinct and timetabled around the needs of the patients and their carers, with advocacy support if appropriate.
A review provides the opportunity to: Evaluate the care plan (progress, successes and setbacks)
Page 18 of 26
Explore alternative ways of supporting people to meet their goals Gather and share information Re-assess needs and risks Review patient consent to share information with carers Review the use or potential use of Direct Payments or Personal Budgets Review or explore the use of Advance Statements and Advance
Decisions Revise and agree the care plan Review CPA eligibility Review use of mental health legislation
It is good practice to hold a CPA meeting prior to a Managers’ Hearing or First Tier Tribunal or CTO hearing to inform and plan for any changes in circumstances. A CPA review should also be held prior to a patient being discharge from hospital. This provides the opportunity to review the CPA status and make appropriate plans for discharge.
6.5.1 Planning a CPA/None CPA review Meeting
There are many factors which need to be considered when deciding where and when to hold a CPA/None CPA review meeting, and it is important to adopt a flexible approach. The following should be considered in planning a review meeting: Where appropriate meetings should be planned and organised as far in
advance as possible The Care Coordinator should involve the patient and carer (where
appropriate) in any discussions and decisions about who will be invited to the meeting. The patient should know or be aware of who will be attending.
The patient should always be encouraged to attend and participate, with advocacy support where necessary, and the meeting arrangements should facilitate this
Arrangements should be made for interpretation services where needed 6.5.2 Who should be involved?
In order to ensure that the care plan reflects the needs of each patient, it is important to consider who needs to be involved, in addition to the patients themselves. Subject to the patient’s views, this may include:
The patient’s nearest relative (if there is one) or other carers Anyone with authority under the Mental Capacity Act 2005 (MCA) to act
on the patient’s behalf i.e. Lasting Power of Attorney or Deputy Appointed by the Court
An Independent Mental Capacity Advocate(IMCA), if the patient has one An Independent Mental Health Advocate (IMHA), if the patient has one Any other advocate who may be involved/supporting the person

Page 19 of 26
Any other representative nominated by the patient (partners, family members or friends where appropriate)
The patient’s Responsible Clinician Health and social care professionals involved in caring for the patient The patient’s GP and Primary Care Team (if there is one) A representative of any relevant voluntary organisations A representative of housing authorities, if accommodation is an issue An employment expert, if employment is an issue In the case of a restricted patient, multi-agency public protection
arrangements (MAPPA) co-ordinator In the case of a transferred prisoner, the probation service The Clinical Commissioning Group’s appointed clinical representative (if
appropriate) A person to whom the local authority is considering making direct
payments for the patient
People not directly involved in the patient’s care (for example students) should only be allowed to attend with the patient’s consent.
6.5.3 Conducting CPA/None CPA Review Meetings
The chairperson has a key role to play in supporting everyone’s views being heard, that decisions are reached, and that the meeting starts and finishes on time. Patients and carers should be encouraged to be first to express their opinions and views about the care they are receiving. The Care Coordinator should normally chair CPA meetings; however consideration may be given to the patient being supported to chair their own meeting. If the Care Coordinator is unable to chair, a chairperson should be identified at the beginning of the meeting
Patients should be aware that the multi-disciplinary team may discuss their care just prior to the meeting, and appropriate information from these discussions should be shared with them.
The following processes should be followed for all CPA/None CPA review meetings: All relevant documentation should be available Everyone present should introduce themselves in full and, if there might
be uncertainty, explain their reasons for involvement in the meeting; Issues for discussion should be identified at the start of the meeting Explanations should be offered to patients of any jargon or abbreviations
used in the meeting The Care Coordinator/Lead Professional should, if possible, spend time
with the patient both before and after the meeting to ensure maximum involvement in the process
The Care Coordinator/Lead Professional is responsible for records of the review, and for arranging for the distribution of the revised care plan to all relevant people
Page 20 of 26
A date for the next review should be agreed at the meeting and recorded in the review documentation
6.5.4 Discharge from CPA
At each review, it should be considered whether or not the patient needs to remain on the CPA. During the patient’s recovery the level or complexity of a patients needs may reduce and while the clinical process of care planning and review does not change, this may no longer need to be done within the CPA framework. However if a high level of input continues to be needed to maintain the patient, they will normally remain on CPA. Patients and carers should be reassured that discharge from the CPA will not affect their eligibility for health or social care services.
If the patient is discharged from the CPA there should be a handover of all relevant information to an identified lead professional within the team if the patient is remaining in Mental Health Services or to the patient’s GP if they are being discharged from the Trust. Patients appropriately subject to CPA on discharge from a secure hospital or prison should normally remain on CPA for a period of time in the community before being discharged.
6.5.5 Disengagement
In the event that a patient on CPA disengages from services it may be appropriate to discharge them from both CPA and Mental Health Services, however this should only be done after every effort has been made to re-engage them and in line with the Trust’s Disengagement Policy.
6.6 Transfers
Effective management of care transfers is a key part of the CPA process, however, it is not solely the responsibility of the Care Coordinator and is dependent on good communication between key individuals and agencies. Transfers may be between Trust services, with out of area services or with prisons. Short term input by another Trust team (for example Intensive Home Treatment) is not a care transfer, and responsibility for care coordination and CPA remain with the originating team. Discharges and transfers should be managed in accordance with the Trust’s Policy for the Planned Discharge/Transfer of Patients from In-Patient Services and Discharge/Transfer SOP’s appropriate to the service involved.
6.6.1 Internal Transfer
Where an existing patient needs to receive long-term interventions from another community-based service, discussion should take place to determine who would be the most appropriate person to take on the Care Coordinator role.
Page 21 of 26
Whenever a change of Care Coordinator takes place there must be a formal handover of care.
6.6.2 Transfer Out of Area
Some Trust patients are admitted to provider units out of area. As the responsible mental health service, the Trust must continue to provide a Care Coordinator, attend CPA reviews and be involved in discharge planning in line with this policy.
It should remain a priority where appropriate to bring such patients back into our services at the earliest opportunity. This should support effective discharge planning and after-care.
When a patient is to be transferred to another area it is important that their transfer is planned and organised to facilitate continuity of care with the receiving service. It is the duty of the Trust Care Coordinator to make a referral to the appropriate Mental Health Service, and provide a full suite of documentation. In complex cases a senior clinician should be involved. Where there is significant risk to the patient or others, this information should be shared directly in person or by telephone, and the discussion should be documented in the electronic patient record. The patient remains the responsibility of the original team until a handover of care has taken place. Agreements should be made about any period of joint working or follow-up by the referring team, where this is appropriate. If an out of area service refuses to accept a referral, this should be followed up by senior management as appropriate.
6.6.3 Transfer into Area
Referral from out of area services should be directed to the appropriate Trust team. The Team Manager and Consultant Psychiatrist from the receiving team should discuss the referral at the earliest opportunity and if the transfer is accepted, a Care Coordinator should be allocated. The new Care Coordinator should actively engage with the referring Mental Health Service to facilitate a smooth transition of care, and work with the referring team and the patient to develop a new care plan. The patient should be kept informed of the transfer arrangements and given contact details of their new care team. Any transfer of patients from secure services should be managed in line with the Trust Policy for the Acceptance of Patients on a Restriction Order or Restriction Direction into Trust Services.
6.6.4 Funding Responsibilities
Where patients transfer between areas, health and social care funding
Page 22 of 26
responsibilities are as set out in the Who Pays? Determining Responsibility for Payments to Providers August 2013 Guidance. Staff must record in the electronic patient record who the Responsible Commissioner is (as defined in the guidance), and should maintain contact with the responsible commissioner; in particular to inform them if one of their patients returns to hospital or if this is being planned. The following should be read in conjunction with the guidance document and should aid staff in identifying the responsible commissioner.
Patients discharged before 01 April 2013 come under the Who Pays?
Establishing the Responsible Commissioner 2007 guidance, where the legacy or originating CCG continues to be responsible for subsequent compulsory admissions under the MHA, and current and subsequent S117 services until such time as the patient is assessed as no longer needing these services.
Patients discharged between 01 April 2013 and 31 March 2016 fall
under the August 2013 Who Pays Guidance, where a patient originating in CCG A becomes the responsibility of CCG B if they are discharged into CCG B’s area and register with a GP in CCG B.
New revised guidance from 1 April 2016 will revert back to the pre 01
April 2013 position where the legacy or originating CCG continues to be responsible in most cases.
6.7 Information Sharing
Appropriate information sharing supports effective delivery of the CPA. Please note that where a range of agencies and people may be involved in care delivery it is vital to communicate clearly and avoid jargon wherever possible.
6.7.1 Patient Information
Patients should be offered a copy of their care plan as described above. Other information relevant to the CPA may be shared with the patient as appropriate.
Under the Freedom of Information Act 2000 and Access to Health Records, patients have a right to request access to all information held about them, and this should be taken into account when making records. Staff should be aware of their responsibilities outlined in the Trust’s Information Governance Policy.
6.7.2 Carer Information
If the patient consents, the carer should be offered a copy of the patient’s care plan (including the crisis and contingency plan). Other information may be shared with the carer as appropriate, subject to the patient’s consent.
Page 23 of 26
Where the patient does not consent to share information with the carer, this does not prevent the care team from gathering information from the carer about the patient and listening to their views. The care team may also appropriately share general information about mental health issues and Mental Health Services.
If a carer’s assessment has been done and / or a carer support plan agreed, a copy of this should be offered to the carer.
6.7.3 GP Information
A copy of the care plan and a summary of the review should be shared with the GP after every review meeting, including a summary of risks and the risk management plan.
6.7.4 Other Agencies
Information should always be sought from other involved agencies to inform the review process and the development of the care plan. All information received should be entered onto the electronic patient record.
Information should be shared with other agencies as appropriate and with the patient’s consent, unless safeguarding or risk issues override the need for consent, in line with the Safeguarding Adults Policy, Safeguarding Children Policy and Information Governance Policy.
7 TRAINING IMPLICATIONS
There are no specific training needs in relation to this policy, however the following staff will need to be familiar with its contents: All Service Managers, Modern Matrons and Team Leaders, clinical staff (qualified and unqualified) who have direct involvement with patient care, and any other individual or group with a responsibility for implementing the contents of this policy.
Staff will be made aware of this procedure and its contents in the following ways:
The review and re-issuing of the procedure is to be publicised in the Trust Daily News Bulletin
A copy of the procedure will be available on the Trust web
The procedure will be covered at local induction within their relevant areas
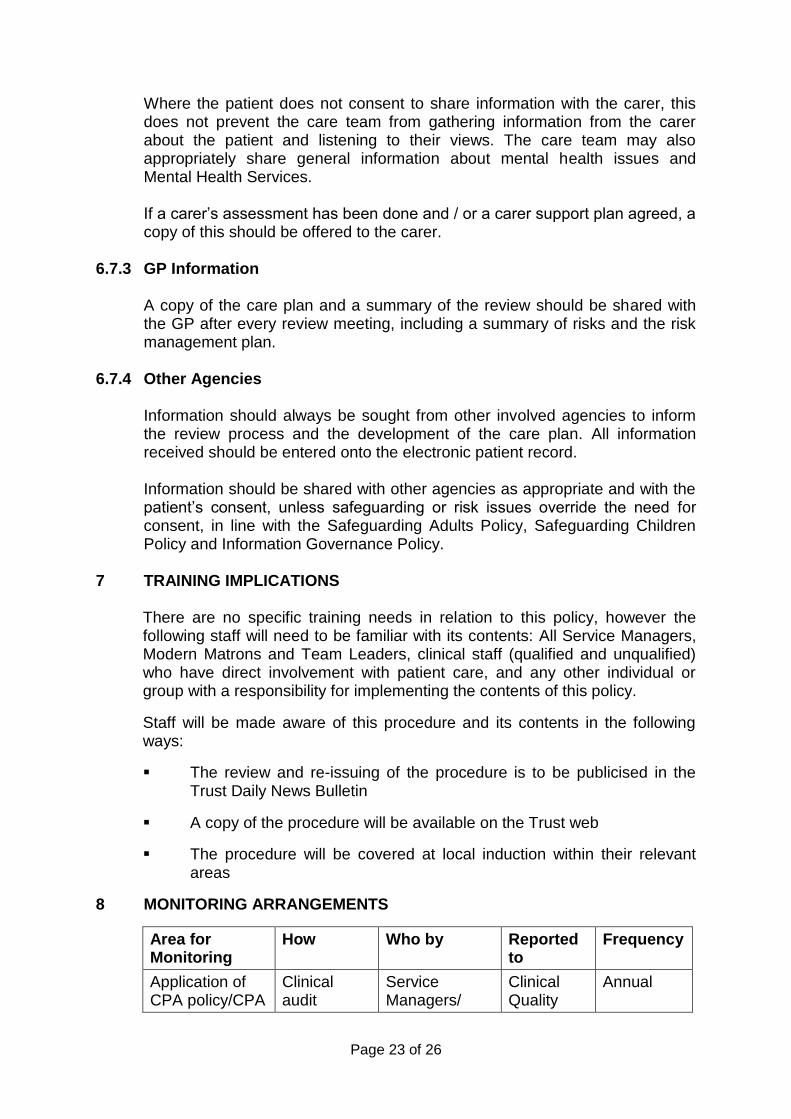
8 MONITORING ARRANGEMENTS
Area for Monitoring
How Who by Reported to
Frequency
Application of CPA policy/CPA
Clinical audit
Service Managers/
Clinical Quality
Annual
Page 24 of 26
Area for Monitoring
How Who by Reported to
Frequency
process Team Managers/ Team Leaders
Group?
7 Day Follow-up Patient Information System
Performance Team
Monitor Quarterly
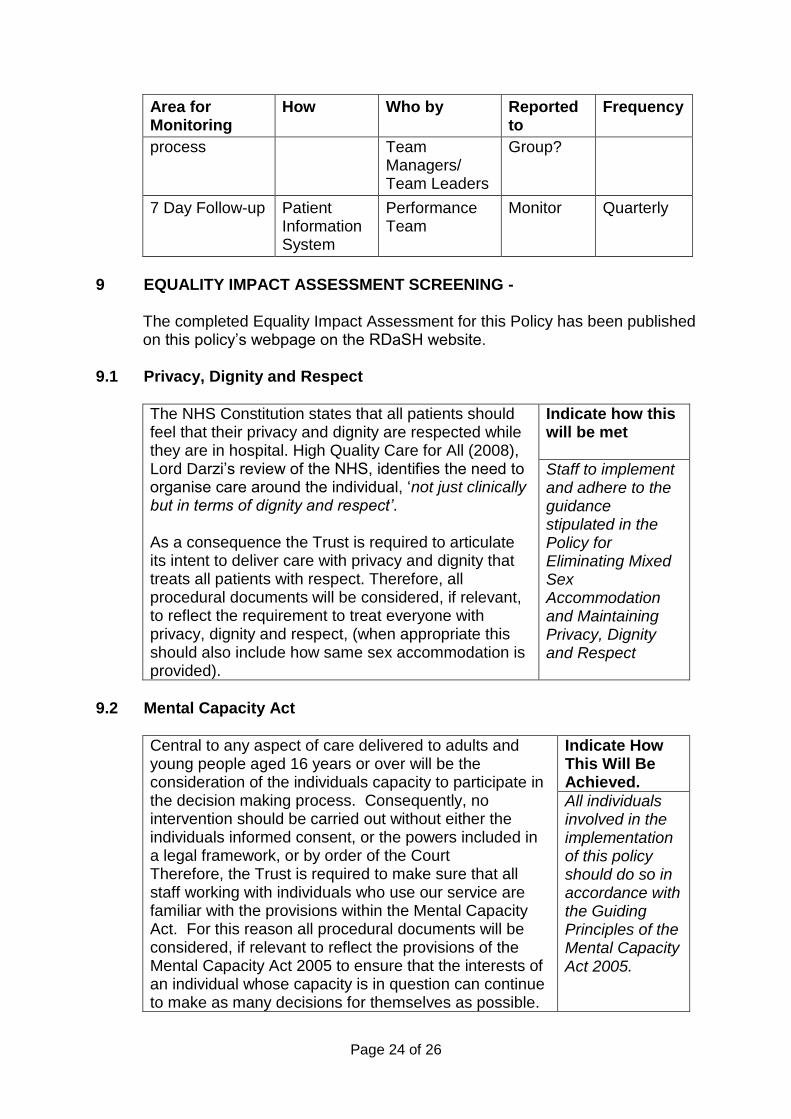
9 EQUALITY IMPACT ASSESSMENT SCREENING -
The completed Equality Impact Assessment for this Policy has been published on this policy’s webpage on the RDaSH website.
9.1 Privacy, Dignity and Respect
The NHS Constitution states that all patients should feel that their privacy and dignity are respected while they are in hospital. High Quality Care for All (2008), Lord Darzi’s review of the NHS, identifies the need to organise care around the individual, ‘not just clinically but in terms of dignity and respect’. As a consequence the Trust is required to articulate its intent to deliver care with privacy and dignity that treats all patients with respect. Therefore, all procedural documents will be considered, if relevant, to reflect the requirement to treat everyone with privacy, dignity and respect, (when appropriate this should also include how same sex accommodation is provided).
Indicate how this will be met
Staff to implement and adhere to the guidance stipulated in the Policy for Eliminating Mixed Sex Accommodation and Maintaining Privacy, Dignity and Respect
9.2 Mental Capacity Act
Central to any aspect of care delivered to adults and young people aged 16 years or over will be the consideration of the individuals capacity to participate in the decision making process. Consequently, no intervention should be carried out without either the individuals informed consent, or the powers included in a legal framework, or by order of the Court Therefore, the Trust is required to make sure that all staff working with individuals who use our service are familiar with the provisions within the Mental Capacity Act. For this reason all procedural documents will be considered, if relevant to reflect the provisions of the Mental Capacity Act 2005 to ensure that the interests of an individual whose capacity is in question can continue to make as many decisions for themselves as possible.
Indicate How This Will Be Achieved.
All individuals involved in the implementation of this policy should do so in accordance with the Guiding Principles of the Mental Capacity Act 2005.
Page 25 of 26
10 LINKS TO ANY ASSOCIATED DOCUMENTS
The CPA Policy should be read in conjunction with related policies which include:
Clinical Risk Assessment and Management Policy Discharge/Transfer of Patients from In-Patient Services Policy Records Management Policy – Lifecycle of Clinical and Corporate
Records Patient Advice and Liaison Service (PALS) Policy Advance Statements and Advance Decisions Policy Consent to Examination or Treatment Policy Policy and Procedure for the Handling of Formal Complaints Policy for the Development of Information for Patients Policy for Eliminating Mixed Sex Accommodation and Maintaining,
Privacy, Dignity and Respect Policy for Patients who are Absent Without Leave (AWOL) Safeguarding Adults Policy Safeguarding Children Policy Suicide Prevention Policy Patients with a Mental Health Problem and Learning Disability
Management Policy The Provision of Access to and Use of Interpreters Policy Transition Protocol: Child and Adolescent Mental Health Services to
Adult Mental Health Services Transition Protocol: Adult Mental Health Services to Older People’s
Mental Health Services Trust Policy for the Acceptance of Patients on a Restriction Order or
Restriction Direction into Trust Services Physical Health and Wellbeing Policy
11 REFERENCES
Department of Health (2012) The NHS Constitution. London: DH HM Government/Department of Health (2011) No Health Without Mental Health. London: DH H M Government (2010) Working Together to Safeguard Children. A guide to inter-agency working to safeguard and promote the welfare of children. Nottingham: DCSF Princes Royal Trust for Carers/National Mental Health Development Unit (2010) The Triangle of Care. Carers included: A guide to best practice in acute mental health care. National Patient Safety Agency (2009) Preventing Suicide – A Toolkit for MH Services. London: NPSA Department of Health (2008) Refocusing the Care Programme Approach – Policy and Positive Practice Guidance. London: DH
Page 26 of 26
Social Care Institute for Excellence/Department of Health (2008) Care Programme Approach (CPA) Briefing: Parents with mental health problems and their children. Care Services Improvement Partnership/NIMHE (2008) 3 Keys to A Shared Approach in Mental Health Assessment Department of Health (2007) Best Practice in Managing Risk. London: DH Department of Health (2001) An Audit Pack for Monitoring the Care Programme Approach. London: DH Department of Health (1999) Effective Care Coordination in Mental Health Services – Modernising the Care Programme Approach Department of Health (1999) National Service Framework for Mental Health
12. APPENDICES
None.














![Training Programme for Patient Care Counsellors · 29/9/2018 · September 28 &29, 2018 [Training Programme for Patient Care Counsellors] Page 4 Programme: Programme started with](https://img.pdfslide.net/doc/110x75/5f997b7534b7b43d63264c66/training-programme-for-patient-care-2992018-september-28-29-2018-training.jpg)














