Embed Size (px)
Citation preview

120 Vol.20,No.1,2006
CARVEDILOL AGGRAVATES ORTHOSTATIC HYPOTENSION IN A DIABETIC PATIENT WITH CHRONIC RENAL FAILURE
Tsuan-ShihYu,Chin-FengTseng,Lai-KingYeung,Kuo-ChengLu,Chuan-ChiehLiu
A 64-year-old male was admitted because of progressive dyspnea, bipedal edema and reduced urine output. His medical history included coronary artery disease with coronary artery bypass graft, hypertension and type 2 diabetes mellitus with chronic renal failure and retinopathy. During admission, he developed severe postural dizziness. Positional blood pressure and heart rate measurements revealed fluctuations in systolic blood pressure greater than 20 mmHg but no significant heart rate change. Two days after stopping carvedilol, systolic blood pressure declined by only 10 mmHg and heart rate increased significantly with positional changes. Orthostatic hypotension due to autonomic neuropathy was suspected. Nerve conduction velocity study showed severe sensorimotor polyneuropathy. Sympathetic skin response and RR interval variability tests indicated autonomic dysfunction.
Combinations of alpha- and beta-blockers should always be administered with caution in diabetics, who are likely to have autonomic nervous system dysfunction and in whom the use of such medications may increase the risk of orthostatic hypotension. (Acta Nephrologica 2006; 20: 120-125)
Key words: orthostatic hypotension, carvedilol, diabetes, renal failure, autonomic neuropathy
DepartmentofMedicine,CardinalTienHospital,SchoolofMedicine,Fu-JenCatholicUniversity,Taipei,TaiwanReceived:May,2005 Revised:July,2005 Accepted:January,2006Addressforreprintsandcorrespondence:Dr.Chuan-ChiehLiu,DepartmentofMedicineCardinalTienHospital,SchoolofMedicine,Fu-JenCatholicUniversity,Taipei,Taiwan,No362,Chung-ChengRd,HsinTienCity,TaipeiCounty,TaiwanTel:886-2-22193391Fax:886-2-29451602E-mail:[email protected]
INTRODUCTION
TheAmericanAutonomicSocietyandtheAmericanAcademy of Neurology defines orthostatic hypotension (OH)asadeclineinsystolicbloodpressureofat least20mmHgbeyond3minutesof standingorpassivehead-uptiltpositionat60degrees.1,2ManyfactorshavebeenlinkedtoOH,includingage,prolongedbedrest,lowbodymassindex,systemicdiseases(e.g.,diabeticautonomic neuropathy, stroke, multiple sclerosis,amyloidosis, adrenal insufficiency)andmedications(e.g., antipsychotic agents, peripheral vasodilators,specificallyalpha-blockersandnon-dihydropyridinecalciumchannelantagonists).3
IfapatientsuspectedofhavingOHishypertensiveand requires antihypertensive medications, pre-treatmentmeasurementsarenecessary to identify thepresenceofbaselineOH.IfnobaselineOHisdetected,antihypertensivemedicationsmaybeprescribedwhileregularlymonitoring forOH. Ifpre-treatmentOH isfound,clinicians shouldbalance thepossible riskof
worseningposturalhypotensionduetoantihypertensivetherapy against the hemodynamic benefits of improved bloodpressurecontrol.
Wereportapatientwithdiabeticnephropathyandneuropathy,whopresentedcarvedilolaggravatedOH.
CASE REPORT
A 64-year-old male was admitted because ofprogressivedyspnea,bipedaledemaandreducedurineoutputof threeweeksduration.Hehasahistoryofcoronaryarterydiseasewith3-vesseldiseaseforwhichhehad receivedcoronaryarterybypassgraft surgeryoneyearprior to thisadmission.Healsohashadtype2 diabetes mellitus for the past 16 years; diabeticretinopathy,chronicrenalfailureandhypertensionhadbeennotedsince2yearsbeforethisadmission.At thetimeofadmission,hismedicalprescription includedcombined regular and intermediate acting insulinpreparations,digoxin0.125mg/day,irbesartan150mg/day,pravastatin20mg/day,clopidogrel75mg/day,and
120-591-尤鑽石.indd 120 2006/6/30 10:57:12 AM

ActaNephrologica CarvedilolandOrthostaticHypotension 121
furosemide80mg/day.Hehadsmokedaboutonepackofcigarettesdailyforthepast40yearsbuthadstoppedtakingalcoholicdrinksforthepast10years.
Uponpresentation,BPwas90/50mmHg,HRwas89beats/min,andrespiratoryratewas18/min.Physicalexamination revealed a jugular venous pressure ofabout6cmabovethesternalborder,anoldmid-sternallongitudinal surgical scarandpittingedemaofbothlowerextremities.Hemoglobin levelwas lowat4.9g/dlandhematocritwasonly15%.Bloodbiochemistryrevealedelevated levelsofbloodureanitrogen level(150mg/dl)andserumcreatinine(4.4mg/dl)butnormallevelsofserumsodium(140mmol/L)andpotassium(4.3mmol/L).Serumdigoxin levelwasslightly lowat0.4ng/ml.Twenty-fourhoururinecreatinineclearance(CCr)was22.65ml/min.
Electrocardiogram revealed sinus rhythm withaheart rateof90/min,QT intervalof320msec,andaQTcof393msec.Echocardiogramrevealeda leftventricularejectionfractionof62%andregionalwallmotion abnormality. On the third hospital day, thepatientdevelopedtarrystoolsbutuppergastrointestinalpanendoscopy revealed only duodenitis and superficial gastritis.He receiveda transfusionofeightunitsofpackedRBCforsevereanemia.Hemoglobinlevelontheseventhhospitaldaywas10.2g/dl.Allantihypertensivemedicationswerediscontinueduponadmissionduetohypotensionbutwereresumedon thesecondhospitaldayduetorecurrenceofhighbloodpressure.Carvedilol(25mg/day)wasgivenstartingonthethirdhospitaldayduetopersistentlyhighbloodpressure.Increasedurineoutputandgradual resolutionofbipedaledemawerenotedfollowingintravenousfurosemideadministrationalthoughmildperipheraledemapersisted.Thejugularvenouspressure level remainedapproximately5cmabovethesternalborderandtherewasnoevidenceofvolumedepletion.
After one week of carvedilol administration,he developed progressively severe dizziness withvertigo,particularlywithchanges inposition.On the9thdayofcarvedilol treatment,hewasnoted tohavesensoryataxiawithinvoluntaryfallingepisodes.Uponneurological consultation, polyneuropathy due tounderlyingdiabeteswithchronic renal failureand/orvertebrobasilar insufficiencywere suspected.Nerveconductionvelocitystudyshowedseveresensorimotorpolyneuropathy.Carotiddopplerscanningrevealed50%stenosisoftheleftcommoncarotidarteryandmoderatetosevereatherosclerosisofbothcommoncarotidandinternalcarotidarteriesalthoughtotalvertebralarteryblood flow was adequate. Positional blood pressure and heartratechangesweremeasuredinthesupine,sittingandstandingpositionsfor2consecutivedays.Systolic
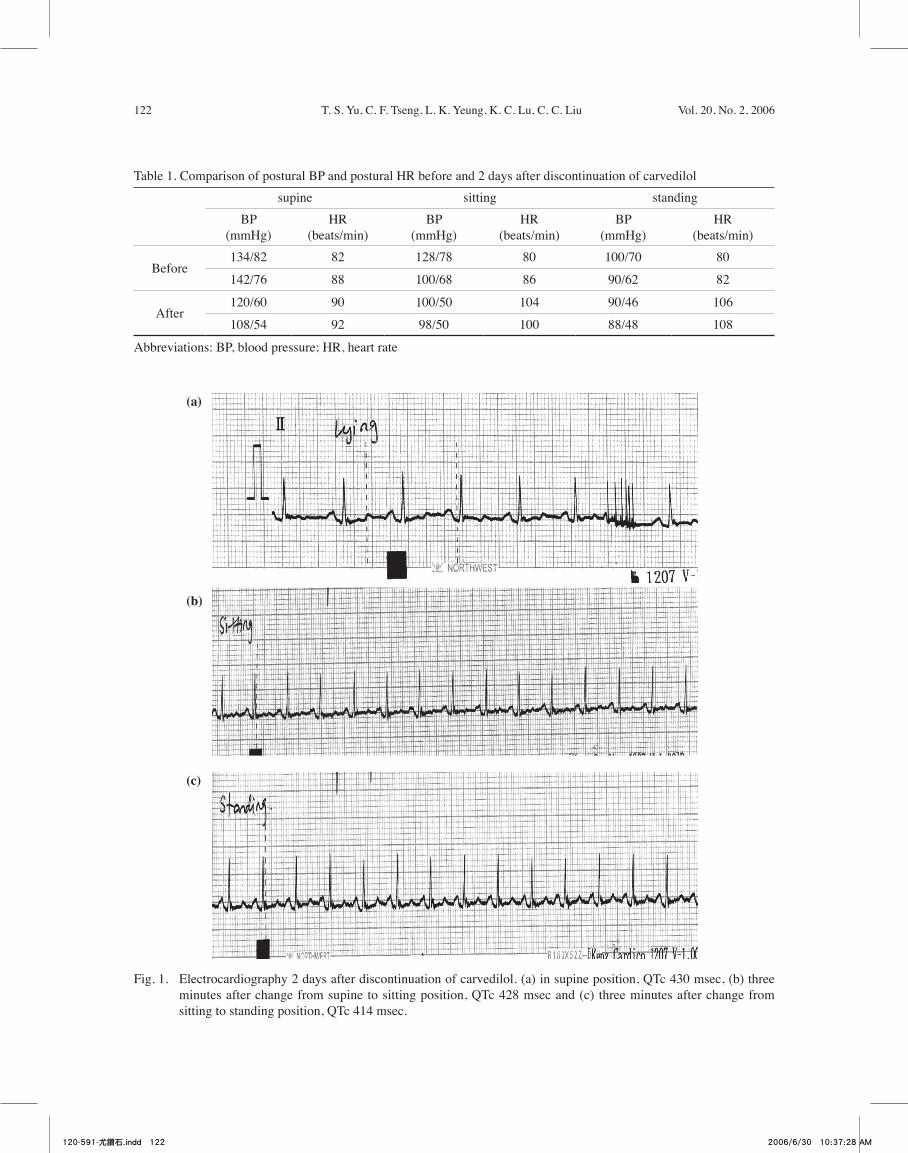
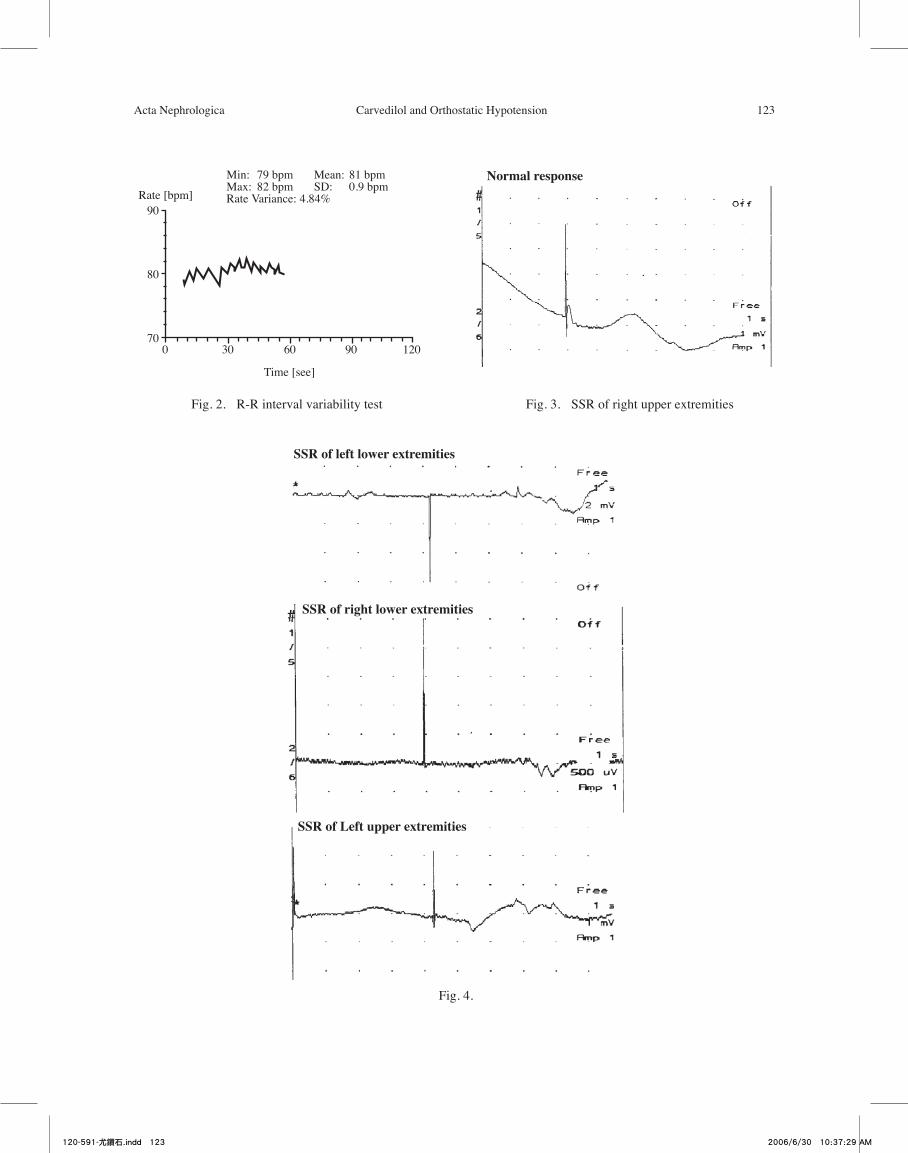
bloodpressuredeclinedbymore than20mmHgwithchanges in position but heart rate did not changesignificantly (Table 1). Upon review of his medications, carvedilolwassuspectedas themostprobablecauseofOHandwas therebydiscontinued.Twodaysafterstoppingcarvedilol, thepatient claimed thathe feltmuchbetter.Electrocardiographywasdone to recordR-Rintervalinthesupine,sitting,andstandingpositionsforatleast3minutes(Fig.1).SupineQTwas356msecandQTcwas430msec.SittingQTwas326msecandQTcwas428msec.StandingQTwas312msecandQTcwas414msec.Simultaneousbloodpressure readingsshoweda10mmHgdeclineinsystolicbloodpressure;tachycardiawasalsonotedwithchanges inposition(Table1).Nofurtherepisodesofposturaldizzinessorsensoryataxiawerenotedonfollow-up.Wesuspectedthat the10mmHgfall insystolicbloodpressureafterstoppingcarvedilolmightbeduetounderlyingdiabeticautonomicneuropathy.Thus,sympatheticskinresponse(SSR)andRRintervalvariability(RRIV)studieswereperformed.Results revealedRRIV4.84%against anormalvalue>10%(Fig.2).NormalSSRwasseenon rightupperextremities. (Fig.3) andabsentSSRon the leftupperandboth lowerextremities. (Fig.4)These twostudies indicate thepresenceofautonomicdysfunction in thisdiabeticpatientwithchronicrenalfailure.
DISCUSSION
Diabetes is the leadingcauseofneuropathyin theWesternworld,andneuropathy is themostcommoncomplication and the greatest source of morbidityandmortality indiabetics.2Diabeticneuropathymaymanifestassensorimotorneuropathy,distalsymmetricalpolyneuropathyor autonomicneuropathy involvingthecardiovascular,gastrointestinalandgenitourinarysystems.Autonomicneuropathymayinvolveboth thesympatheticandparasympathetic innervationsof theheartandcoronaryvessels,4withhallmarksymptomsoforthostatichypotensionanddecreasedheart ratevariability.Theincidenceofcardiovascularautonomicneuropathyappears tobearound15% in type1and20% in type 2 diabetes patients.5 Cardiovascularautonomicneuropathymaycontributetoleftventriculardysfunction, silent or asymptomatic myocardialinfarction,andexerciseintolence.4,6
Autonomicnervoussystemdysfunctionmayalsodevelop inpatientswithuremia.7 Impotence,posturaldizziness, feeling of gastric fullness or delayedemptying,boweldysfunction, and reducedsweatingare themostcommonsymptoms.7Hemodialysismayimproveautonomic function inuremicpatients.8The
120-591-尤鑽石.indd 121 2006/6/30 10:37:27 AM
122 T.S.Yu,C.F.Tseng,L.K.Yeung,K.C.Lu,C.C.Liu Vol.20,No.2,2006
Table1.ComparisonofposturalBPandposturalHRbeforeand2daysafterdiscontinuationofcarvedilolsupine sitting standing
BP(mmHg)
HR(beats/min)
BP(mmHg)
HR(beats/min)
BP(mmHg)
HR(beats/min)
Before134/82 82 128/78 80 100/70 80
142/76 88 100/68 86 90/62 82
After120/60 90 100/50 104 90/46 106
108/54 92 98/50 100 88/48 108
Abbreviations:BP,bloodpressure;HR,heartrate
Fig.1. Electrocardiography2daysafterdiscontinuationofcarvedilol.(a)insupineposition,QTc430msec,(b)threeminutesafterchangefromsupinetosittingposition,QTc428msecand(c)threeminutesafterchangefromsittingtostandingposition,QTc414msec.
(a)
(b)
(c)
120-591-尤鑽石.indd 122 2006/6/30 10:37:28 AM
ActaNephrologica CarvedilolandOrthostaticHypotension 123
Fig.2. R-Rintervalvariabilitytest Fig.3. SSRofrightupperextremities
Normal responseMin: 79 bpm Mean: 81 bpmMax: 82 bpm SD: 0.9 bpmRate Variance: 4.84%Rate [bpm]
90
80
70
Time [see]
0 30 60 90 120
Fig.4.
SSR of left lower extremities
SSR of right lower extremities
SSR of Left upper extremities
120-591-尤鑽石.indd 123 2006/6/30 10:37:29 AM

124 T.S.Yu,C.F.Tseng,L.K.Yeung,K.C.Lu,C.C.Liu Vol.20,No.2,2006
incidenceofOHindiabeticswithchronicrenalfailureis37.5%.9Ourpatienthadchronic renal failureduetodiabeticnephropathyandpresentedwithazotemiawhichmayhaveaggravatedhisunderlyingautonomicneuropathy.
The regulationofbloodpressure andheart ratewithchanges inposition involves thecardiovascular,musculoskeletal,renal,endocrinologicalandautonomicnervous systems. Conditions that predispose anindividual to OH include advanced age, decreasedbaroreflex sensitivity, impaired β-adrenoceptor-mediated response,10 increasedvascularstiffness11anddecreasednumberofpacemaker cells in the sinoatrial node.12
DrugswhichmaycauseOHorworsenpositionalbloodpressurechangesincludepsychoactivemedicationssuchas tricyclicantidepressants,13antiparkinsonismagentsandcardiovascularmedications,suchasvasodilators.14,15Someantihypertensivemedicationsmayinterferewithposturalhaemodynamicstability , therebyaggravatingpositionalbloodpressureandpredisposingtoOH.3Ontheotherhand,certainantihypertensivemedicationsmay improve baroreflex sensitivity16 and decreasevascular stiffness,17whichmayamelioratepositionalbloodpressurechangesandlessentheriskofOH.
It iswellknown thatnon-selectivebeta-blockersreducebloodpressure,heartrateandmyocardialoxygendemand.However,animalstudieshaveshownthat thealpha-1blockersmay inducevasodilatation, increaseperipheralvascularbloodflowanddecreasedthelimbvascularresistance.18,19Sinceperipheralvasoconstrictionis an important counter-mechanismduringposturalchanges,patients receivingalpha-blockersmaybeatincreasedriskofdevelopingOH.
Carvedilolmaypreserve renal functionwithouteliciting reflex stimulationof the renin-angiotensin-aldosteronesystemor fluidretention.Carvedilolalsodoes not affect glucose tolerance or carbohydratemetabolismandisthereforesuitableforthetreatmentofhypertensivepatientswith type2diabetesmellitus. Invitroandanimalstudieshavealsoshownthatcarvedilolhas cardioprotective andneuroprotectivepropertiesthatmaybebeneficial inpatientswithanginapectorisorcongestiveheart failure.18Ourpatienthascoronaryarterydisease, type2diabetesmellituswithchronicrenalfailureandhypertensionandweusedcarvedilolfortheabovereasons.However,carvedilolisanonselectivebeta-adrenoreceptorwithalpha-blockingactivityandmaybeassociatedwitha40%increasedriskofOHinelderlypatients.20
In one study, patients on 25 mg of carvediloldailydevelopedadose-dependentfall insupinebloodpressure and standing blood pressure. In contrast,beta-blockerswith intrinsicsympathomimeticactivity
producedsimilarreductionsinsupinebloodpressurebutless significant reductions in standing blood pressure.20
Ourpatienthad systolicbloodpressure fluctuationsgreater than20mmHgwithchanges inpositionbutno significant change in the heart rate.After oraladministration,thehalf-lifeofcarvedilolis2to8hoursalthoughitmayonlybe2to5hoursintheelderly(age>65years).18Twodaysafterstoppingcarvedilol,ourpatient feltmuchbetterclinically.Followupsystolicbloodpressuredeclinedbyonly10mmHgandheartrate increased significantlywithpositionalchanges.The 10 mmHg fall in systolic blood pressure afterstoppingcarvedilolismostprobablyduetounderlyingautonomicneuropathy.Ourpatienthasa longhistoryofdiabetesandnerveconductionvelocityexaminationshowedseveresensorimotorpolyneuropathy.TheSSRtestprovidesuseful informationregardingsympatheticpostganglionic functionandanabsentSSRsupportsadiagnosisofdiabetic autonomicneuropathy.21,22AlowerRRIVmayalsobeseenindiabeticswithcardiacautonomic neuropathy and absent SSR.23,24 In ourpatient,absentSSRand lowRRIVboth indicate thepresenceofautonomicdysfunctionclinicallypresentingasOH.
Inconclusion,physiciansmustkeep inmind thatcarvedilolmayaggravateorthostatichypotensioninthediabeticpatientwithchronicrenalfailure,particularlythosewithunderlyingautonomicneuropathy.IfOHisaproblem, theuseofangiotensinconvertingenzymeinhibitors,angiotensinreceptorblockers,25beta-blockerswithintrinsicsympatomimeticactivity(e.g.,pindolol)26and calcium blockers such as verapamil27 may beconsidered.
REFERENCES
1.Consensus statements on the definition of orthostatichypotension,pureautonomic failure,andmultiplesystematrophy: the Consensus Committee of theAmericanAutonomicSocietyandtheAmericanAcademyofNeurology.Neurology1996;46(5):1470.
2.Consensus statements on the definition of orthostatichypotension,pureautonomic failure,andmultiplesystematrophy.JNeurolSci1996;144(1-2):218-9.
3.Hajjar I:Posturalbloodpressurechangesandorthostatichypotensionintheelderlypatient.Drugsaging2005;22(1):55-68.
4.VinikAI,MaserRE,MitchellBD,etal:Diabeticautonomicneuropathy.DiabetesCare2003;26:1553-79.
5.ZieglerD.Cardiovasculrautonomicneuropathy: clinicalmanifestationandmeasurement.DiabetesRev1999;7:342-57.
6.Vin ik AI , Park TS, Stansberry KB, et a l : Diabet icneuropathies.Diabetologia2000;43:957-73.
7.SavicaV,MusolinaR,RitaDL,etal:Autonomicdysfunctioninuremia.AmJkidneyDis2001;38Suppl1:S118-21.
8.HeidrederE,SchafferhansK,HeidlandA:Disturbancesof
120-591-尤鑽石.indd 124 2006/6/30 10:37:29 AM

ActaNephrologica CarvedilolandOrthostaticHypotension 125
peripheralandautonomicnervoussysteminchronicrenalfailure:Effectsofhemodialysisand transplantation.ClinNephrol1985;23:222-8.
9.OsamuS,HajimeN,SatokoN,etal:Orthostatichypotensionattheintroductoryphaseofhaemodialysispredictsall-causemortality.NephrolDialTransplant2005,20:377-81.
10.Hogikyan RV, Supiano MA:Arterial alpha-adrenergicresponsivenessisdecreasedandSNSactivity is increasedinolderhumans.AmJPhysiol1994;266(5Pt1):E717-24.
11.LakattaEG,MitchellJH,PomeranceA,etal:Humanaging:changes instructureandfunction.JAmCollCardiol1987;10(2Suppl.A):42A-7A.
12.BenarrochEE:Thecentralautonomicnetwork: functionalorganization,dysfunction,andperspective.MayoClinProc1993;68(10):988-1001.
13.Cyndya S,Alfredo G,Andre D, et al: Managementof Hypertension in the setting of autonomic failure.Hypertension2005;45:469-76.
14.Verhaverbeke I , Mets T: Drug- induced orthostat ichypotension in theelderly:avoiding itsonset.DrugSaf1997;17(2):105-18.
15.SchoenbergerJA.Drug inducedorthostatichypotension.DrugSaf1991;6(6):402-7.
16.FlorasJS,HassanMO,JonesJV,etal:Factorsinfluencingbloodpressureandheart ratevariability inhypertensivehumans.Hypertension1988;11(3):273-81.
17.MahmudA, Feely J: Effect of angiotensin II receptorblockade on arterial stiffness: beyond blood pressurereduction.AmJHypertens2002;15(12):1092-5.
18.McTavishD,Campoli-RichardsD,SorkinEM.Carvedilol:A reviewof itspharmacodynamicandpharmacokineticproperties,andtherapeuticefficacy.Drugs1993;45:232-58.
19.GelmanS,BredleDL,BradleyWE,etal:Angiotensinand
alpha-adrenoceptoractivationplayarole inhemodynamicresponsetoaorticcross-clamping.AmJPhysiol1990;259(1Pt2):H68-73.
20.Krum H, Conway EL, Broadbear JH, et al: Posturalhypotension inelderlypatientsgivencarvedilol.BMJ1994;309(6957):775-6.
21.NazhelB,Vetkin I, IrkecC,KocerB:Sympathetic skinresponse in diabetic neuropathy. Electromyogr ClinNeurophysiol2002;Apr-May;42(3):181-5.
22.TakebayashiK,AsoY,SugitaR,TakemuraY, InukaiT:Relationshipbetweensympatheticskinresponseandpowerspectralanalysisofheartratevariationinpatientswithtype2diabetes.JDiabetesComplications2004Jul-Aug;18(4):224-8.
23.WhangW,BiggerJTJr:ComparisonoftheprognosticvalueofRR-intervalvariabilityafteracutemyocardial infarction inpatientswithversus thosewithoutdiabetesmellitus.AmJCardiol2003Aug1;92(3):247-51.
24.OkaH,MochioS,YoshiokaM,MoritaM,InoueK:EvaluationofbaroreflexsensitivitybythesequencemethodusingbloodpressureoscillationsandR-Rintervalchangesduringdeeprespiration.EurNeurol2003;50(4):230-43.
25.RomeroR,CastelloteE,OconJ,etal:Controlledmulticentrestudywithquinapril,hydrochlorothiazideandcombinationinpatientswithmoderatetoseverehypertension.JCardiovascPharmacol1995;26(1):114-8.
26.DejgardA, Hilsted J: No effect of pindolol on posturalhypotension in type1(insulin-dependent)diabeticpatientswithautonomicneuropathy:a randomizeddouble-blindcontrolledstudy.Diabetologia1988;31(5):281-4.
27.ChamontinBF,MonstastrucJL,SalvadorMJ:Hypertensionwith orthostatic hypotension: interst of verapamil. JCardiovascPharmacol1987;10(Suppl.10):S114-6.
120-591-尤鑽石.indd 125 2006/6/30 10:37:30 AM





























