Embed Size (px)
Citation preview

Case Based Teaching – Sepsis St. Joseph’s CTU Objectives: Medical Expert:
1. Review the different causes of sepsis in a newborn 2. Understand the indications and interpretation of investigations for sepsis 3. Review the initial investigations to come to a diagnosis 4. Understand the choice of antibiotics
Communicator:
1. Learn how to explain to parents why the team is concerned about infection 2. Learn the information needed to counsel around the impact of treatment for
sepsis in the case of culture negative and culture positive sepsis. Resources:
1. Polin RA, MD and the committee on Fetus and Newborn. Management of Neonates with suspected or Proven Early-Onset Bacterial Sepsis. American Academy of Pediatrics. Pediatrics Vol. 129 No. 5 May 1, 2012 pp. 1006 -1015
2. Committee on Infectious Diseases and Committee on Fetus and Newborn. Policy Statement-Recommendations for the Prevention of Perinatal Group B Streptococcal (GBS) Disease. American Academy of Pediatrics. Pediatrics; originally published online August 1, 2011
3. Baltimore R. Neonatal Sepsis: Epidemiology and Management. Paediatr Drugs. 2003;5(11):723-40.
4. Arnon S, Litmanovitz I. Diagnostic tests in neonatal sepsis. Current Opinion in Infectious Diseases 2008 Jun;21(3):223-7
5. Management of the infant at increased risk for sepsis. Position Statement (FN 2007-03). Paediatr Child Health. 2007 December; 12(10): 893–898.
Case Review:
• 39 5/7 week gestational infant • Born to 37 G3T1A1L1 mother • VDRL, Hep B, HIV GBS neg • O +ve Rubella immune • Normal antenatal US, No blood sugar or blood pressure issues • Induced for unstable lie • ROM for 13 hrs • SVD • APGARS 9, 9 • BW 3400 grams • Cord gas
- Art 7.16/66/19/24 - Ven 7.28/40/46/19
• 12 hrs later (midnight) call from NCR to peds. • Pt was born after they completed rounds and had not yet had newborn exam • Nurses called with tachypnea that developed at 10hrs of age • RR reported to be 80 • Infant feeding well
On exam:
- RR 84 no indrawing, HR 140 SpO2 99% - Occasional grunt - Infant responsive good tone - Good cap refill - No murmur normal femoral pulses - Good air entry no extra sounds
Discussion Is this a normal respiratory rate? What is your differential diagnosis at this time? What tests if any would you order?
Case CBC ordered at 0100, clotted times two
Now 3 a.m. infant still grunting HR 180’s BP 68/32 MAP 40 SPO2 95% caprefill 3-5 sec.
Discussion What would you do now? If you decided to start antibiotics which would you choose? What are the most common organisms that cause sepsis in neonates? Would your antibiotic choice be different if this infant was in the NICU for the past 7
days? How do you calculate the IT ratio? What is the significance of the IT ratio? Would you order a CRP?, How do you interpret the CRP? What is your interpretation of the blood gas? What intervention if any would you
consider with the physical exam findings? Results: CORRECTED LKCS | 3.7 | | X10 9/L | Corrected Leukocyte count appears when the Nucleated | Erythrocyte count is greater than 5.

> LKCS | 4.2 | L | 5.0-21.0 X10 9/L | 17/06/12 0633: | LKCS previously reported as: X10 9/L | TO FOLLOW > ERCS | 4.44 | | 4.0-6.6 x10 12/L > **HB** | 169 | | 145-225 g/L > **HCT** | 0.479 | | 0.450-0.670 > MCV | 107.9 | | 95-121 fL > MCH | 38.1 | | 28-40 pg > MCHC | 353 | | 290-360 g/L > RDW | 16.3 | H | 11.5-15.0 % > **PLT** | | 150-400 x10 9/L | Large platelet clumps present. Unable to estimate. | Few very large platelet clumps and fibrin strands present. | Query inadequate mixing of the sample at collection? | PLT CT previously reported as: 126 L x10 9/L | Preliminary count must be confirmed with morphology. > MPV | 8.4 | | 7.4-10.4 fL > SMEAR EXAMINE | Blood film made | | MANUAL DIFF. | | | > NERCS | 14 | | /100 LKC > ABSOLUTE BANDS | 0.8 | | x10 9/L > ABSOLUTE NEUTS | 0.9 | L | 1.5-10.0 x10 9/L > ABSOLUTE LYMPHS | 1.6 | L | 2.0-17.0 x10 9/L > ABSOLUTE MONOS | 0.1 | L | 0.5-1.9 x10 9/L > ABSOLUTE MYELOS | 0.1 | | x10 9/L > ABSOLUTE METAS | 0.2 | | x10 9/L CRP 40.8 Blood gas 7.18/46/47/17/-11
• Blood GBS positive after 7 hrs • CSF done June 18th
- BS 5.9 mmol/L - Protein 2.28 g/L - Leuks 3248 - RBC 4
• Gram Stain Pus cells Gram positive Cocci • CSF culture neg

Take Home Messages:
• No Risk factors does not mean no chance of infection • Don’t rely on labs to make clinical decisions • Be wary of respiratory rates that are normal at birth and increase subsequently • Review the importance of doing a full septic workup in the case of suspected
sepsis.

C
Diagnostic tests in neonatal sep
sisShmuel Arnona,b and Ita Litmanovitza,baNeonatal Department, Meir Medical Center, Kfar Sabaand bSackler Faculty of Medicine, Tel Aviv University,Tel Aviv, Israel
Correspondence to Dr Shmuel Arnon, Department ofNeonatology, Meir Medical Center Kfar Saba, 44281,IsraelTel: +972 9 747 2225; fax: +972 9 747 1189;e-mail: [email protected]
Current Opinion in Infectious Diseases 2008,21:223–227
Purpose of review
The present review examines the major developments in early detection of neonatal
sepsis, with an emphasis on the utility of diagnostic laboratory markers in clinical
practice.
Recent findings
Measures of acute phase proteins, cytokines, cell surface antigens, and bacterial
genomes have been used alone or in combination to improve diagnosis of neonatal
sepsis. Most studies evaluating laboratory diagnostic markers are retrospective cohorts
or single center experience with relatively small sample size. Interpretation of these
studies is confounded by inconsistent definitions of sepsis, heterogeneous sample
populations, and different thresholds for diagnostic markers. Furthermore, many
diagnostic markers are not available for routine care, they require specialized analytica
procedures, and are expensive to perform.
Summary
A better understanding of the neonatal inflammatory response to sepsis and
identification of sensitive and specific markers of inflammation or rapid microbe-specific
diagnostic tests would assist in the early detection of neonatal sepsis and in safely
withholding antibiotics for patients in whom sepsis is unlikely.
Keywords
acute phase reactant, cell surface antigens, cytokines, neonatal sepsis, polymerase
chain reaction
Curr Opin Infect Dis 21:223–227� 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins0951-7375
IntroductionThe diagnosis of sepsis in infants is difficult because
clinical signs, particularly early in the course of disease,
are subtle and nonspecific, and laboratory tests including
blood culture, the ‘gold standard’, are not always reliable
[1]. Clinicians have long sought reliable markers to detect
sepsis early in its course and to exclude diseases of
noninfectious origin [2–4]. Recent studies propose new
diagnostic laboratory markers used alone or in combi-
nation to improve sensitivity and specificity for early
detection of sepsis.
Clinical and laboratory scoresThe clinical signs of neonatal sepsis are nonspecific.
Fanaroff et al. [5] with the National Institute of Child
Health and Human Development (NICHD) Neonatal
Research Network found that increasing apnea, feeding
intolerance, abdominal distension or heme-positive
stools, increased respiratory support, lethargy, and hypo-
tonia were the most common presenting signs of late
onset sepsis (LOS). None was found to have high-
predictive accuracy [5]. However, many neonatologists,
particularly those practicing in clinical settings with lim-
ited resources, use clinical judgment or scores combined
opyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibite
0951-7375 � 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins
l
with complete blood count (CBC) and blood cultures for
the detection of neonatal sepsis [6,7]. Components of the
CBC that may become abnormal in sepsis have a positive
predictive value (PPV) as low as 11% [1]. This may be
explained by inter-observer variability in immature and
mature neutrophil identification [8], factors other than
sepsis that cause abnormalities of the CBC, and timing
of the CBC that is often normal at the time of initial
evaluation but abnormal a few hours later. Okascharoen
et al. [6] devised and tested a scoring system for the
diagnosis of LOS in preterm infants composed of the
following five clinical indicators: hypotension, hypother-
mia, hyperthermia, respiratory insufficiency, and umbilical
venous catheters between 1 and 7 days or more than 7 days;
and the two following hematological parameters: imma-
ture neutrophil count more than 1% and platelet count less
than 150 000/ml3. The clinical score had an acceptable
predictive performance [PPV 43%, negative predictive
value (NPV) 96%] but was no better than the clinicians’
estimate of LOS risk. The addition of C-reactive protein
(CRP) and micro erythrocyte sedimentation rate (mESR)
to a clinical score in detecting LOS had a high sensitivity
(95%) but a low specificity (18%). The positive likelihood
ratio (a measure of predictive value that is independent of
prevalence) was 1.61 (Table 1) [7,9–19].
d.

C
224 Paediatric and neonatal infections
Table 1 Accuracy of diagnostic tests at the time of sepsis evaluation
Diagnostic test [reference]No. of
patientsNo. of infected
patients EOS/LOS Cutoff valueSensitivity
(%)Positive
LRNPV(%)
ClinicalþCBCþCRPþ mESR [7] 220 60 LOS NA 95 1.61 91IL-6þCRP [9] 92 37 LOS 60 pg/ml, 1.4 mg/dl 92 1.56 80PCTþCRP [10] 85 28 LOS 0.5 mg/l, 1 mg/dl 93 1.18 80PCT [11] 100 61 LOS 0.59 mg/l 81 4.26 72SAA [12] 104 23 EOS 0.8 mg/dl 96 19 99CRP [13] 116 42 LOS 1 mg/dl 32 10.6 74SAA [13] 116 42 LOS 1 mg/dl 95 13.5 97CRP [14] 25 8 EOS 2.1 mg/dl 88 99.9 96LPB [14] 25 8 EOS 21.5 mg/l 100 16.6 100LPB [14] 22 8 LOS 17.1 mg/l 92 8.3 97CD64 [15] 338 115 EOS 6136 antibody PE molecules bound/cell 79 7.18 89CD64 [16] 110 32 LOS 4000 antibody PE molecules bound/cell 95 12 97IL-8 [17] 249 61 EOS 18.000 pg/ml 97 19.4 99IL-8þCRP [18] 1291 13 EOS 70 pg/ml, 1mg/dl 80 6.15 93PCR, 16S rRNA [19] 172 8 LOS NA 100 50 98
CBC, complete blood count; CRP, C-reactive protein; EOS, early onset sepsis; IL, interleukin; LPB, lipopolysaccharide-binding protein; LOS, lateonset sepsis; LR, likelihood ratio; mESR, micro erythrocyte sedimentation rate; NA, not available; NPV, negative predictive value; PCR, polymerasechain reaction; PCT, procalcitonin; PE, phycoerythrin; rRNA, ribosomal ribonucleic acid; SAA, serum amyloid A.
A recent advance in the diagnosis of neonatal sepsis is heart
rate characteristic (HRC) that monitors the presence of
reduced variability and transient decelerations, which
occur with increased frequency in the preclinical phases
of septicemia [20,21�,22,23]. The HRC index demon-
strated a significant association with both blood culture
proven sepsis and clinical LOS in neonates. The odds ratio
for the prediction of neonatal sepsis with high HRC index
was more than two. Both the clinical score and the HRC
index rose before the clinical diagnosis of illness, with
HRC being first [21�]. This noninvasive and inexpensive
index has the advantage of being available through con-
tinuous electrocardiogram monitoring and can add infor-
mation to conventional measures in the early diagnosis of
neonatal sepsis [23]. There is currently a large, multicenter
randomized controlled trial underway to evaluate the
impact of HRC monitoring on initiation of timing of
treatment for sepsis and infection-related morbidities
[impact of heart rate characteristics monitoring in neonates
(HeRO)3. ClinicalTrials.gov Identifier: NCT00307333].
Acute phase reactantsAcute phase reactants are endogenous peptides produced
by the liver as part of an immediate response to infection
or tissue injury. The most widely used in neonates is CRP
[24–27]. Given that there is a time lag of 12–24 h in the
response of CRP to infection, some clinicians use it in
combination with another serum marker such as inter-
leukins [26,27]. The specificity of CRP is low for early
onset sepsis (EOS), as a number of prenatal conditions
(maternal fever, fetal distress or stressful delivery, and
vacuum delivery) may lead to its elevation in the absence
of systemic infection. Recent studies, using CRP cutoff
values of 1.2–6 mg/dl to diagnose sepsis and guide
duration of therapy in EOS and LOS, showed specificity
between 84–96% and a NPV range of 93–99%. The
opyright © Lippincott Williams & Wilkins. Unautho
clinical practice of using higher CRP cutoff values led
to fewer days of antibiotics without an evidence of
infection relapse [24,25,27].
Procalcitonin (PCT) is an acute phase reactant produced
by monocytes and hepatocytes. PCT begins to rise 4 h
after exposure to bacterial endotoxin, peaks at six to
eight, and remains elevated for at least 24 h [28]. In
adults, it has been used for almost a decade to diagnose
the severity of systemic inflammatory response, to deter-
mine the progression of infection to sepsis and septic
shock, to assess responsiveness to treatment, and to
estimate prognosis [28]. A number of recent studies of
preterm infants confirmed that PCT compared with CRP
and proinflammatory cytokines had equivalent or better
sensitivity for diagnosis of LOS, but with lower values of
NPV and likelihood ratio [9–11,29] (Table 1). A recent
study showed that PCT had a lower diagnostic utility
(sensitivity 81.4%, specificity 80.6%) at the time of suspi-
cion of sepsis. Therefore, PCT is not sufficiently reliable
to be the sole marker of LOS, but may be useful as part of
an evaluation for sepsis in a neonate [11]. The diagnostic
utility of PCT in EOS is limited by its rapid physiological
postnatal endogenous increase [30,31]. For this reason,
age-related nomograms of PCT values were proposed
during the first days of life [30]. In summary, PCT level is
elevated during EOS and LOS and its overall diagnostic
utility is comparable with CRP.
Serum amyloid A (SAA) is an acute phase protein induced
by the inflammatory cytokines IL-1 and IL-6, and tumor
necrosis factor (TNF)-a in response to lipopolysacchar-
ide (LPS) gram-negative bacteria infection. There is a
robust increase in SAA levels from 8 to 24 h after the onset
of sepsis. Arnon et al. [12] showed that SAA had a better
diagnostic accuracy than CRP at septic evaluation in EOS
(�5 h after birth) (Table 1). However, vaginal delivery
rized reproduction of this article is prohibited.

C
Diagnostic tests in neonatal sepsis Arnon and Litmanovitz 225
that produces a transient elevation of SAA levels, even
higher than the cutoff point for the detection of sepsis
[32], might affect the diagnostic accuracy of SAA in EOS.
The same group of investigators showed that SAA levels
during LOS had a high sensitivity and NPV, suggesting it
may be a superior marker compared with CRP [13]
(Table 1). Recently, rapid SAA measurement has been
facilitated by the development of a fully automated kit
that required no specialized instrumentation and can be
done in any service laboratory [12].
Lipopolysaccharide-binding protein (LBP), a 50-kDa
acute-phase protein, is mainly synthesized in the liver.
It binds with high affinity to LPS in the plasma, transfers
LPS to membrane bound or soluble CD14, and modu-
lates the microbial-induced activation of the inflamma-
tory host response [33]. It was recently reported that LBP
has a better sensitivity and specificity for detecting sepsis
than LPS-soluble, CD14 complexes, and PCT in EOS,
but equally effective to CRP in detecting sepsis of infants
older than 48 h [14] (Table 1).
A number of acute phase proteins including a1-anti-
trypsin, fibronectin, haptoglobin, lactoferrin, neopterin,
inter-a inhibitor proteins (IaIp), granulocyte colony
stimulating factor (G-CSF), orosomucoid, and antithrom-
bin have been evaluated in relation to neonatal sepsis
[34]. Although these acute phase proteins may be candi-
date biomarkers for sepsis, none has been routinely used
clinically or studied on a large scale.
Cell surface antigensIn recent years, flow cytometric analysis of cell surface
antigens [CD11b, Fcg receptors I-III (CD64, CD32, and
CD16), CD69] has been performed to detect congenital
sepsis, EOS, and LOS [15,16,35]. For detection of EOS,
CD64 was shown to have a sensitivity of 81% and a NPV
of 89% [15] (Table 1). Twenty-four hours after onset of
sepsis, the sensitivity and NPV rose to 96 and 97%,
respectively. A large cohort study, assessing two neutro-
phil (CD11b and CD64) and two lymphocyte surface
markers (CD25 and CD45RO) for the diagnosis of LOS,
showed that CD64 had the highest sensitivity (95–97%)
and specificity (88–90%) for detecting sepsis at the onset
of infection and 24 h later [16] (Table 1). Combining
CD64 with IL-6 or CRP further enhanced the ability to
diagnose localized infections and improved the sensi-
tivity and NPV to 100% [31]. In response to infection,
preterm infants increase cell numbers of lymphocyte
populations (CD3, CD19, CD25, CD26, and CD71)
and human leukocyte antigen (HLA)-DR expression
on monocytes, and upregulate neutrophil surface anti-
gens (CD11b, CD11c, CD13, CD15, CD33, CD64, and
CD66b) [35,36�]. However, to date, no cell surface
markers alone or in combination have been tested and
opyright © Lippincott Williams & Wilkins. Unauth
shown to be sensitive and specific enough to allow
neonatologists to withhold antibiotic treatment in an
infant with clinical signs suggestive of infection. Further-
more, analysis of cell surface markers in the clinical
setting requires specialized equipment and qualified
personnel. Blood specimens, must be processed immedi-
ately to avoid neutrophil apoptosis and downregulation of
surface molecules [36�]. This limits the practical appli-
cation of this technology in the clinical setting.
Chemokines and cytokinesThe regulation and trafficking of leukocytes into specific
body tissues are principally controlled by chemokines or
cytokines, which are mainly divided into two subsets.
Proinflammatory cytokines [IL-2, IL-6, interferon
(IFN)g, TNFa] that are primarily responsible for initiat-
ing an effective defense against exogenous pathogens
and anti-inflammatory cytokines (IL-4 and IL-10) that
are crucial for downregulating the exacerbated inflam-
matory process and maintaining homoeostasis for proper
functioning of vital organs. A study analyzing 127 epi-
sodes of suspected LOS in very low birth weight (VLBW)
infants found both proinflammatory and anti-inflamma-
tory cytokines significantly increased in infected infants
compared with noninfected infants [37]. The very short
half-life of circulating cytokines increases the risk of false
negative results. For this reason, whole blood IL-8 (cell-
bound and extracellular IL-8) [17] (Table 1) or cytokines
combined with other more sustained markers of inflam-
mation [9,38] have been suggested as a better diagnostic
tool. A multicenter, randomized, controlled trial of 1291
infants suspected of EOS by at least one clinical sign
showed that the use of IL-8 more than 70 pg/ml and/or
CRP more than 10 mg/l to diagnose sepsis significantly
reduced antibiotic therapy from 49.6 to 36.1% (P< 0.05)
and increased the diagnostic utility of these markers [18]
(Table 1). No infection was missed and no significant
difference in the diagnostic accuracy was observed
between the untreated group and the control group [18].
In VLBW infants with suspected sepsis, plasma IL-10
(>208 ng/l), IL-6 (>168 ng/l), and regulated upon acti-
vation normal T-cell expressed and secreted (RANTES)
(<3110 ng/l) had sensitivity, specificity, PPV, and NPV of
100, 97, 85, and 100%, respectively, for identifying
infected patients who subsequently developed dissemi-
nated intravascular coagulation [39]. Another recent study
by the same group of researchers revealed that four mar-
kers of a panel of key chemokines and cytokines (IP-10,
MIG, IL-6, IL-10) achieved a sensitivity of more than 80%
and a specificity of more than 75%, for detecting sepsis for
each tested marker. Among them, the IP-10 with a cutoff
value of at least 1250 pg/ml exhibited the best sensitivity
(93%) and specificity (89%) [40��]. Owing to the rapid
decline of these inflammatory biomarkers after the onset of
sepsis, 24 h measurements had lower predictive values
orized reproduction of this article is prohibited.

C
226 Paediatric and neonatal infections
than those at 0 h. The use of multiple markers in combi-
nation only marginally improved the sensitivity of IP-10 by
0–7%, but adversely affected the specificity by 13–50%
[40��]. Owing to the processing costs, most chemokines
and cytokines are not routinely used for identifying neo-
natal sepsis or for predicting the severity and outcome of
infection. The measurement of IL-8 in the urine has
recently proven to be a reliable and an effective alternative
for detecting neonatal sepsis [41].
Molecular biomarkersNucleic acid amplification tests such as PCR have been
used successfully to diagnose a wide range of bacterial,
yeast, viral, and protozoal infectious diseases. In recent
years, PCR analysis has exploited the highly conserved
bacterial 16S ribosomal ribonucleic acid (rRNA) gene to
diagnose EOS and LOS. Shang et al. [19] used bacterial
16S rRNA gene PCR and DNA microarray analysis in 172
neonates with suspected sepsis and found a sensitivity of
100% and specificity of 97.8% (Table 1). Although the
16S rDNA PCR in near-term infants with EOS had high
specificity (97.5%) and NPV (99.2%) compared with
blood cultures, it failed to detect 59% of infants with
positive blood culture (sensitivity 41%, PPV 19%)
[42,43]. The use of staphylococcus-specific PCR to detect
bloodstream infection had comparable specificity (94.7–
100%) and NPV (95.4–98%) with inconsistent sensitivity
of 57.1–69.2% and PPV of 53.3–100% [44,45]. The main
advantage of PCR over blood cultures is that it is rapid
(4–6 h versus �18 h, respectively) and requires small
blood volume (0.2–0.3 ml versus 1 ml respectively).
PCR amplification does require specialized instrumenta-
tion and training perform and it is not routinely available
in many microbiology laboratories. A recent study [46]
showed that approximately eight antibiotic doses and 85
neonatal intensive care unit (NICU) hours per infant
could be saved using negative PCR results. Therefore,
due to the high NPV of PCR methods, it may influence
clinical practices and decision-making, leading to fewer
antibiotic doses per patient and shorter hospital stay.
Proteomic biomarker of intra-amnioticinflammationRecent advances in proteomics present a new opportu-
nity to search for biomarkers and generation of protein
profiles that can rapidly (1–3 h) aid in the prediction of
amniotic fluid inflammation and early neonatal sepsis.
The use of specific biomarkers to identify neonates with
increased risk for sepsis in utero would aid in the initiation
of appropriate therapy. Buhimschi et al. [47] showed that
proteomic mapping of amniotic fluid, a profile designed
as the mass restricted score, is highly characteristic of
intra-amniotic inflammation. The profile comprised four
protein biomarkers (neutrophil defensin-1 and neutrophil
opyright © Lippincott Williams & Wilkins. Unautho
defensin-2, calgranulin A and C) that provide qualitative
information (from a scale of 0–4 depending on the pre-
sence or absence of these 4 proteins) on the presence or
absence of intra-amniotic inflammation. Furthermore,
high mass restricted score (3–4) significantly correlated
with suspected or confirmed EOS. The strongest associ-
ation was for calgranulin A with a sensitivity, specificity,
PPV, and NPV of 55, 80, 44, and 86%, respectively
[48�,49]. Although intriguing, these findings need to be
validated in larger prospective studies of neonates sus-
pected of having sepsis.
ConclusionA better understanding of the neonatal inflammatory
response to infection has led to the identification of
multiple candidate biomarkers to improve diagnosis of
sepsis. At present, no single biomarker or panel of bio-
markers is sufficiently reliable for early detection of
neonatal sepsis. Complicated analytical measurement
further limits the utility of many biomarkers in clinical
practice. The use of biomarkers as a diagnostic tool for
the early discontinuation of empirical antibiotic treat-
ment for infants with suspected sepsis is promising, but
requires additional study.
AcknowledgementsThe authors thank Robert L. Schelonka, MD, Department of Pediatrics,University of Alabama, Birmingham, AL, for his critical review of themanuscript.
References and recommended readingPapers of particular interest, published within the annual period of review, havebeen highlighted as:� of special interest�� of outstanding interest
Additional references related to this topic can also be found in the CurrentWorld Literature section in this issue (p. 320).
1 Gerdes JS. Diagnosis and management of bacterial infections in the neonate.Pediatr Clin North Am 2004; 51:939–959.
2 Fischer JE, Bachmann LM, Jaeschke R. A readers’ guide to the interpretationof diagnostic test properties: clinical example of sepsis. Intensive Care Med2003; 29:1043–1051.
3 Ng PC, Lam HS. Diagnostic markers for neonatal sepsis. Curr Opin Pediatr2006; 18:125–131.
4 Mishra UK, Jacobs SE, Doyle LW, Garland SM. Newer approaches to thediagnosis of early onset neonatal sepsis. Arch Dis Child Fetal Neonatal Ed2006; 91:F208–F212.
5 Fanaroff AA, Korones SB, Wright LL, et al. Incidence, presenting features,risk factors and significance of late onset septicemia in very low birthweight infants. The National Institute of Child Health and Human Develop-ment Neonatal Research Network. Pediatr Infect Dis J 1998; 17:593–598.
6 Okascharoen C, Hui C, Cairnie J, et al. External validation of bedsideprediction score for diagnosis of late-onset neonatal sepsis. J Perinatol2007; 27:496–501.
7 Kudawla M, Dutta S, Narang A. Validation of a clinical score for the diagnosisof late onset neonatal septicemia in babies weighing 1000 2500 g. J TropPediatr 2008; 54:66–69.
8 Schelonka RL, Yoder BA, Hall RB, et al. Differentiation of segmented andband neutrophils during the early newborn period. J Pediatr 1995; 127:298–300.
rized reproduction of this article is prohibited.
C
Diagnostic tests in neonatal sepsis Arnon and Litmanovitz 227
9 Verboon-Maciolek MA, Thijsen SF, Hemels MA, et al. Inflammatory mediatorsfor the diagnosis and treatment of sepsis in early infancy. Pediatr Res 2006;59:457–461.
10 Turner D, Hammerman C, Rudensky B, et al. The role of procalcitonin as apredictor of nosocomial sepsis in preterm infants. Acta Paediatr 2006;95:1571–1576.
11 Lopez Sastre JB, Perez Solıs D, Roques Serradilla V, et al. Procalcitonin is notsufficiently reliable to be the sole marker of neonatal sepsis of nosocomialorigin. BMC Pediatrics 2006; 6:16.
12 Arnon S, Litmanovitz I, Regev RH, et al. Serum amyloid A: an early andaccurate marker of neonatal early-onset sepsis. J Perinatol 2007; 27:297–302.
13 Arnon S, Litmanovitz I, Regev R, et al. Serum amyloid A protein in the earlydetection of late-onset bacterial sepsis in preterm infants. J Perinat Med 2002;30:329–332.
14 Pavcnik-Arnol M, Hojker S, Derganc M. Lipopolysaccharide-binding protein,lipopolysaccharide, and soluble CD14 in sepsis of critically ill neonates andchildren. Intensive Care Med 2007; 33:1025–1032.
15 Ng PC, Li G, Chui KM, et al. Neutrophil CD64 is a sensitive diagnostic markerfor early-onset neonatal infection. Pediatr Res 2004; 56:796–803.
16 Ng PC, Li K, Wong RP, et al. Neutrophil CD64 expression: a sensitivediagnostic marker for late-onset nosocomial infection in very low birth weightinfants. Pediatr Res 2002; 51:296–303.
17 Orlikowsky TW, Neunhoeffer F, Goelz R, et al. Evaluation of IL-8-concentra-tions in plasma and lysed EDTA blood in healthy neonates and those withsuspected early onset bacterial infection. Pediatr Res 2004; 56:804–809.
18 Franz AR, Bauer K, Schalk A, et al. Measurement of interleukin 8 in combina-tion with C-reactive protein reduced unnecessary antibiotic therapy in new-born infants: a multicenter, randomized, controlled trial. Pediatrics 2004;114:1–8.
19 Shang S, Chen G, Wu Y, et al. Rapid diagnosis of bacterial sepsis with PCRamplification and microarray hybridization in 16S rRNA gene. Pediatr Res2005; 58:143–148.
20 Griffin MP, Lake DE, Moorman JR. Heart rate characteristics and laboratorytests in neonatal sepsis. Pediatrics 2005; 115:937–941.
21
�Griffin MP, Lake DE, O’Shea TM, Moorman JR. Heart rate characteristics andclinical signs in neonatal sepsis. Pediatr Res 2007; 61:222–227.
The study examines the relationship between HRC index and a clinical score inneonatal sepsis and points out that the former is adjunctive and not a substitute forclinical information.
22 Moorman JR, Lake DE, Griffin MP. Heart rate characteristics monitoring forneonatal sepsis. IEEE Trans Biomed Eng 2006; 53:126–132.
23 Goldstein B. Heart rate characteristics in neonatal sepsis: a promising testthat is still premature. Pediatrics 2005; 115:1070–1072; Comment onPediatrics. 2005; 115:937-941..
24 Bataineh HA, Alrashed KM. C-reactive protein in Neonates with suspectedsepticemia. Rawal Med J 2007; 32:25–27.
25 Couto RC, Barbosa JA, Pedrosa TM, Biscione FM. C-reactive protein-guidedapproach may shorten length of antimicrobial treatment of culture-provenlate-onset sepsis: an intervention study. Braz J Infect Dis 2007; 11:240–245.
26 Franz AR, Kron M, Pohlandt F, Steinbach G. Comparison of procalcitonin withinterleukin 8, C-reactive protein and differential white blood cell count for theearly diagnosis of bacterial infections in newborn infants. Pediatr Infect Dis J1999; 18:666–671.
27 Haque KN. Defining common infections in children and neonates. J HospInfect 2007; 65 (Suppl 2):110–114.
28 Tang BM, Eslick GD, Craig JC, McLean AS. Accuracy of procalcitonin forsepsis diagnosis in critically ill patients: systematic review and meta-analysis.Lancet Infect Dis 2007; 7:210–217.
29 Kocabas E, Sarkcoglu A, Aksaray N, et al. Role of procalcitonin, C-reactiveprotein, interleukin-6, interleukin-8 and tumor necrosis factor-a in the diag-nosis of neonatal sepsis. Turk J Pediatr 2007; 49:7–20.
30 Turner D, Hammerman C, Rudensky B, et al. Procalcitonin in preterm infantsduring the first few days of life: introducing an age related nomogram. Arch DisChild Fetal Neonatal Ed 2006; 91:F283–F286.
opyright © Lippincott Williams & Wilkins. Unauth
31 Llorente E, Prieto B, Cardo L, et al. Umbilical cord blood serum procalcitoninby time-resolved amplified cryptate emission (TRACE) technology: referencevalues of a potential marker of vertically transmitted neonatal sepsis. ClinChem Lab Med 2007; 45:1531–1535.
32 Golden SM, Hague I, Elwood R, et al. Serum amyloid A concentrations in full-term infant umbilical cord serum using a solid phase indirect ELISA. Lab Med2005; 36:357–360.
33 Zweigner J, Schumann RR, Weber JR. The role of lipopolysaccharide-bindingprotein in modulating the innate immune response. Microb Infect 2006;8:946–952.
34 Ersoy B, Nehir H, Altinoz S, et al. Prognostic value of initial antithrombin levelsin neonatal sepsis. Indian Pediatr 2007; 44:581–584.
35 Hodge G, Hodge S, Han P, Haslam R. Multiple leucocyte activation markersto detect neonatal infection. Clin Exp Immunol 2004; 135:125–129.
36
�Gille C, Orlikowsky TW. Flow cytometric methods in the detection of neonatalinfection. Transfus Med Hemother 2007; 34:157–163.
Summarizing the different flow cytometric markers to detect neonatal sepsis andtheir clinical and laboratory characteristics, the study stresses the role of cellsurface antigens to stop antibiotics when the child is healthy and the lack ofaccuracy of these markers to withhold antibiotics when the child is sick andsuspected of having sepsis.
37 Ng PC, Li K, Wong RP, et al. Proinflammatory and anti-inflammatory cytokineresponses in preterm infants with systemic infections. Arch Dis Child FetalNeonatal Ed 2003; 88:F209–F213.
38 Horisberger T, Harbarth S, Nadal D, et al. G-CSF and IL-8 for early diagnosisof sepsis in neonates and critically ill children – safety and cost effectivenessof a new laboratory prediction model: study protocol of a randomized con-trolled trial. Crit Care 2004; 8:R443–R450.
39 Ng PC, Li K, Leung TF, et al. Early prediction of sepsis-induced disseminatedintravascular coagulation with interleukin-10, interleukin-6, and RANTES inpreterm infants. Clin Chem 2006; 52:1181–1189.
40
��Ng PC, Li K, Chui KM, et al. IP-10 is an early diagnostic marker foridentification of late-onset bacterial infection in preterm infants. PediatrRes 2007; 61:93–98.
A well designed study showing that preterm infants have the ability to induce arobust chemokine and cytokine response during sepsis, with IP-10 being asensitive early marker of infection.
41 Bentlin MR, de Souza Rugolo LM, Junior AR, et al. Is urine interleukin-8 level areliable laboratory test for diagnosing late onset sepsis in premature infants?J Trop Pediatr 2007; 53:403–408.
42 Jordan JA, Durso MB, Butchko AR, et al. Evaluating the near-term infant forearly onset sepsis. Progress and challenges to consider with 16S rDNApolymerase chain reaction testing. J Mol Diagn 2006; 8:357–363.
43 Jordan JA, Durso MB. Real-time polymerase chain reaction for detectingbacterial DNA directly from blood of neonates being evaluated for sepsis.J Mol Diagn 2005; 7:575–581.
44 Makhoul IR, Yacoub A, Smolkin T, et al. Values of C-reactive protein,procalcitonin, and Staphylococcus-specific PCR in neonatal late-onset sep-sis. Acta Paediatr 2006; 95:1218–1223.
45 Makhoul IR, Smolkin T, Sujov P, et al. PCR-based detection of neonatalStaphylococca bacteremias. J Clin Microbiol 2005; 43:4823–4825.
46 Brozanski BS, Jones JG, Krohn MJ, Jordan JA. Use of polymerase chainreaction as a diagnostic tool for neonatal sepsis can result in a decrease in useof antibiotics and total neonatal intensive care unit length of stay. J Perinatol2006; 26:688–692.
47 Buhimschi CS, Bhandari V, Hamar BD, et al. Proteomic profiling of theamniotic fluid to detect inflammation, infection, and neonatal sepsis. PLoSMed 2007; 4:e18.
48
�Buhimschi CS, Buhimschi IA, Abdel-Razeq S, et al. Proteomic biomarkers ofintra-amniotic inflammation: relationship with funisitis and early-onset sepsis inthe premature neonate. Pediatr Res 2007; 61:318–324.
The study presents the emerging field of proteomics in the evaluation of thenewborn at risk for EOS. Amniotic fluid proteomic analysis showed that high massrestricted score was strongly associated with histological funisitis and with earlyneonatal sepsis.
49 Buhimschi IA, Christner R, Buhimschi CS. Proteomic biomarker analysis ofamniotic fluid for identification of intra-amniotic inflammation. BJOG 2005;112:173–181.
orized reproduction of this article is prohibited.

CLINICAL REPORT
Management of Neonates With Suspected or ProvenEarly-Onset Bacterial Sepsis
abstractWith improved obstetrical management and evidence-based use ofintrapartum antimicrobial therapy, early-onset neonatal sepsis is be-coming less frequent. However, early-onset sepsis remains one of themost common causes of neonatal morbidity and mortality in the pre-term population. The identification of neonates at risk for early-onsetsepsis is frequently based on a constellation of perinatal risk factorsthat are neither sensitive nor specific. Furthermore, diagnostic testsfor neonatal sepsis have a poor positive predictive accuracy. As a result,clinicians often treat well-appearing infants for extended periods of time,even when bacterial cultures are negative. The optimal treatment ofinfants with suspected early-onset sepsis is broad-spectrum antimicro-bial agents (ampicillin and an aminoglycoside). Once a pathogen is iden-tified, antimicrobial therapy should be narrowed (unless synergism isneeded). Recent data suggest an association between prolonged empir-ical treatment of preterm infants (≥5 days) with broad-spectrum anti-biotics and higher risks of late onset sepsis, necrotizing enterocolitis,and mortality. To reduce these risks, antimicrobial therapy should bediscontinued at 48 hours in clinical situations in which the probabilityof sepsis is low. The purpose of this clinical report is to provide apractical and, when possible, evidence-based approach to the manage-ment of infants with suspected or proven early-onset sepsis. Pediatrics2012;129:1006–1015
INTRODUCTION
“Suspected sepsis” is one of the most common diagnoses made in theNICU.1 However, the signs of sepsis are nonspecific, and inflammatorysyndromes of noninfectious origin mimic those of neonatal sepsis. Mostinfants with suspected sepsis recover with supportive care (with orwithout initiation of antimicrobial therapy). The challenges for cliniciansare threefold: (1) identifying neonates with a high likelihood of sepsispromptly and initiating antimicrobial therapy; (2) distinguishing “high-risk” healthy-appearing infants or infants with clinical signs who do notrequire treatment; and (3) discontinuing antimicrobial therapy oncesepsis is deemed unlikely. The purpose of this clinical report is toprovide a practical and, when possible, evidence-based approach to thediagnosis and management of early-onset sepsis, defined by the Na-tional Institute of Child Health and Human Development and VermontOxford Networks as sepsis with onset at ≤3 days of age.
Richard A. Polin, MD and the COMMITTEE ON FETUS ANDNEWBORN
KEY WORDSearly-onset sepsis, antimicrobial therapy, group B streptococcus,meningitis, gastric aspirate, tracheal aspirate, chorioamnionitis,sepsis screen, blood culture, lumbar puncture, urine culture,body surface cultures, white blood count, acute phase reactants,prevention strategies
ABBREVIATIONSCFU—colony-forming unitsCRP—C-reactive proteinCSF—cerebrospinal fluidGBS—group B streptococciI/T—immature to total neutrophil (ratio)PMN—polymorphonuclear leukocytePPROM—preterm premature rupture of membranes
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authorshave filed conflict of interest statements with the AmericanAcademy of Pediatrics. Any conflicts have been resolved througha process approved by the Board of Directors. The AmericanAcademy of Pediatrics has neither solicited nor accepted anycommercial involvement in the development of the content ofthis publication.
The guidance in this report does not indicate an exclusivecourse of treatment or serve as a standard of medical care.Variations, taking into account individual circumstances, may beappropriate.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-0541
doi:10.1542/peds.2012-0541
All clinical reports from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
1006 FROM THE AMERICAN ACADEMY OF PEDIATRICS
Guidance for the Clinician inRendering Pediatric Care

PATHOGENESIS ANDEPIDEMIOLOGY OF EARLY-ONSETSEPSIS
Before birth, the fetus optimally ismaintained in a sterile environment.Organisms causing early-onset sepsisascend from the birth canal eitherwhen the amniotic membranes ruptureor leak before or during the course oflabor, resulting in intra-amniotic infec-tion.2 Commonly referred to as “cho-rioamnionitis,” intra-amniotic infectionindicates infection of the amniotic fluid,membranes, placenta, and/or decidua.
Group B streptococci (GBS) can alsoenter the amniotic fluid through occulttears. Chorioamnionitis is a major riskfactor for neonatal sepsis. Sepsis canbegin in utero when the fetus inhalesor swallows infected amniotic fluid.The neonate can also develop sepsis inthe hours or days after birth whencolonized skin or mucosal surfaces arecompromised. The essential criterionfor the clinical diagnosis of chorio-amnionitis is maternal fever. Othercriteria are relatively insensitive. Whendefining intra-amniotic infection (cho-rioamnionitis) for clinical researchstudies, the diagnosis is typically basedon the presence of maternal fever ofgreater than 38°C (100.4°F) and at leasttwo of the following criteria: maternalleukocytosis (greater than 15 000 cells/mm3), maternal tachycardia (greaterthan 100 beats/minute), fetal tachycar-dia (greater than 160 beats/minute),uterine tenderness, and/or foul odor ofthe amniotic fluid. These thresholds areassociated with higher rates of neo-natal and maternal morbidity.
Nonetheless, the diagnosis of cho-rioamnionitis must be considered evenwhen maternal fever is the sole abnor-mal finding. Although fever is commonin women who receive epidural anes-thesia (15%–20%), histologic evidenceof acute chorioamnionitis is very com-mon in women who become febrileafter an epidural (70.6%).3 Furthermore,
most of these women with histologicchorioamnionitis do not have a positiveplacental culture.3 The incidence of clin-ical chorioamnionitis varies inverselywith gestational age. In the NationalInstitute of Child Health and HumanDevelopment Neonatal Research Net-work, 14% to 28% of women deliveringpreterm infants at 22 through 28 weeks’gestation exhibited signs compatiblewith chorioamnionitis.4 The major riskfactors for chorioamnionitis includelow parity, spontaneous labor, longerlength of labor and membrane rupture,multiple digital vaginal examinations(especially with ruptured membranes),meconium-stained amniotic fluid, internalfetal or uterine monitoring, and pres-ence of genital tract microorganisms(eg, Mycoplasma hominis).5
At term gestation, less than 1% ofwomen with intact membranes willhave organisms cultured from amni-otic fluid.6 The rate can be higher ifthe integrity of the amniotic cavity iscompromised by procedures beforebirth (eg, placement of a cerclage oramniocentesis).6 In women with pre-term labor and intact membranes, therate of microbial invasion of the amni-otic cavity is 32%, and if there is pre-term premature rupture of membranes(PPROM), the rate may be as high as75%.7 Many of the pathogens recoveredfrom amniotic fluid in women with pre-term labor or PPROM (eg, Ureaplasmaspecies or Mycoplasma species) donot cause early-onset sepsis.8–10 How-ever, both Ureaplasma and Myco-plasma organisms can be recoveredfrom the bloodstream of infants whosebirth weight is less than 1500 g.11 Whena pathogen (eg, GBS) is recovered fromamniotic fluid, the attack rate of neo-natal sepsis can be as high as 20%.12
Infants born to women with PPROMwho are colonized with GBS have anestimated attack rate of 33% to 50%when intrapartum prophylaxis is notgiven.13
The major risk factors for early-onsetneonatal sepsis are preterm birth,maternal colonization with GBS, ruptureof membranes >18 hours, and mater-nal signs or symptoms of intra-amnioticinfection.14–16 Other variables includeethnicity (ie, black women are at higherrisk of being colonized with GBS), lowsocioeconomic status, male sex, andlow Apgar scores. Preterm birth/lowbirth weight is the risk factor mostclosely associated with early-onset sep-sis.17 Infant birth weight is inverselyrelated to risk of early-onset sepsis.The increased risk of early-onset sep-sis in preterm infants is also related tocomplications of labor and deliveryand immaturity of innate and adaptiveimmunity.18
DIAGNOSTIC TESTING FOR SEPSIS
The clinical diagnosis of sepsis in theneonate is difficult, because many ofthe signs of sepsis are nonspecific andare observed with other noninfectiousconditions. Although a normal physicalexamination is evidence that sepsis isnot present,19,20 bacteremia can occurin the absence of clinical signs.21 Avail-able diagnostic testing is not helpful indeciding which neonate requires em-pirical antimicrobial therapy but canassist with the decision to discontinuetreatment.22
Blood Culture
A single blood culture in a sufficientvolume is required for all neonateswith suspected sepsis. Data suggestthat 1.0 mL of blood should be theminimum volume drawn for culturewhen a single pediatric blood culturebottle is used. Dividing the specimen inhalf and inoculating aerobic and an-aerobic bottles is likely to decrease thesensitivity. Although 0.5 mL of bloodhas previously been considered ac-ceptable, in vitro data from Schelonkaet al demonstrated that 0.5 mL wouldnot reliably detect low-level bacteremia
PEDIATRICS Volume 129, Number 5, May 2012 1007
FROM THE AMERICAN ACADEMY OF PEDIATRICS

(4 colony-forming units [CFU]/mL orless).23 Furthermore, up to 25% ofinfants with sepsis have low colonycount bacteremia (≤4 CFU/mL), andtwo-thirds of infants younger than 2months of age have colony counts <10CFU/mL.24,25 Neal et al demonstratedthat more than half of blood specimensinoculated into the aerobic bottle wereless than 0.5 mL.26 A study by Connellet al indicated that blood cultures withan adequate volume were twice aslikely to yield a positive result.27 A bloodculture obtained through an umbilicalartery catheter shortly after placementfor other clinical indications is an ac-ceptable alternative to a culture drawnfrom a peripheral vein.28 The risk ofrecovering a contaminant is greaterwith a blood culture drawn from anumbilical vein.29 There are, however,data to suggest that a blood culturedrawn from the umbilical vein at thetime of delivery using a doubly clam-ped and adequately prepared segmentof the cord is a reliable alternative toa culture obtained peripherally.30
Urine Culture
A urine culture should not be part of thesepsisworkup in an infant with suspectedearly-onset sepsis.31 Unlike urinary tractinfections in older infants (which areusually ascending infections), urinarytract infections in newborn infants areattributable to seeding of the kidneyduring an episode of bacteremia.
Gastric Aspirates
The fetus swallows 500 to 1000 mL ofamniotic fluid each day. Therefore, ifthere are white blood cells present inamniotic fluid, they will be present ingastric aspirate specimens at birth.However, these cells represent the ma-ternal response to inflammation andhave a poor correlation with neonatalsepsis.32 Gram stains of gastric aspiratesto identify bacteria are of limited valueand are not routinely recommended.33
Body Surface Cultures
Bacterial cultures of the axilla, groin,and the external ear canal have a poorpositive predictive accuracy. They areexpensive and add little to the evalu-ation of an infant with possible bac-terial sepsis.34,35
Tracheal Aspirates
Cultures and Gram stains of trachealaspirate specimens may be of value ifobtained immediately after endotra-cheal tube placement.36 Once an infanthas been intubated for several days,tracheal aspirates are of no value inthe evaluation of sepsis.37
Lumbar Puncture
The decision to perform a lumbar punc-ture in a neonate with suspected early-onset sepsis remains controversial. Inthe high-risk, healthy-appearing in-fant, data suggest that the likelihoodof meningitis is extremely low.38 In theinfant with clinical signs that are thoughtto be attributable to a noninfectiouscondition, such as respiratory distresssyndrome, the likelihood of meningitisis also low.39 However, in bacteremicinfants, the incidence of meningitis maybe as high as 23%.40,41 Blood culturealone cannot be used to decide whoneeds a lumbar puncture, becauseblood cultures can be negative in upto 38% of infants with meningitis.42,43
The lumbar puncture should be per-formed in any infant with a positiveblood culture, infants whose clinicalcourse or laboratory data stronglysuggest bacterial sepsis, and infantswho initially worsen with antimicro-bial therapy. For any infant who iscritically ill and likely to have cardio-vascular or respiratory compromisefrom the procedure, the lumbar punc-ture can be deferred until the infant ismore stable.
Cerebrospinal fluid (CSF) values indic-ative of neonatal meningitis are con-troversial. In studies that have excluded
infants with “traumatic taps” (ornonbacterial illnesses), the meannumber of white blood cells in un-infected preterm or term infants wasconsistently <10 cells/mm3.44–50 Cellcounts 2 standard deviations from themean were generally less than 20cells/mm3.46 In a study by Garges et al,the median number of white blood cellsin infants who were born at greaterthan 34 weeks’ gestation and hadbacterial meningitis was 477/mm3.43
In contrast, the median number of whiteblood cells in infants who were born atless than 34 weeks’ gestation and hadmeningitis was 110/mm3.51 Infants withmeningitis attributable to Gram-negativepathogens typically have higher CSFwhite blood cell counts than do infantswith meningitis attributable to Gram-positive pathogens.52 Adjusting theCSF white blood cell count for thenumber of red blood cells does notimprove the diagnostic utility (loss ofsensitivity with marginal gain in speci-ficity).53 In addition, the number of bandsin a CSF specimen does not predictmeningitis.54 With a delay in analysis(>2 hours), white blood cell countsand glucose concentrations decreasesignificantly.55
Protein concentrations in uninfected,term newborn infants are <100 mg/dL.44–50 Preterm infants have CSF pro-tein concentrations that vary inverselywith gestational age. In the normogly-cemic newborn infant, glucose con-centrations in CSF are similar to thosein older infants and children (70%–80%of a simultaneously obtained bloodspecimen). A low glucose concentrationis the CSF variable with the greatestspecificity for the diagnosis of menin-gitis.43,51 Protein concentrations arehigher and glucose concentrations arelower in term than in preterm infantswith meningitis. However, meningitisoccurs in infants with normal CSFvalues, and some of these infants havehigh bacterial inocula.43,51
1008 FROM THE AMERICAN ACADEMY OF PEDIATRICS

Peripheral White Blood Cell Countand Differential Count
Total white blood cell counts have littlevalue in the diagnosis of early-onsetsepsis and have a poor positive pre-dictive accuracy.56,57 Many investi-gators have analyzed subcomponentsof the white blood cell count (neutrophilindices)—absolute neutrophil count,absolute band count, and immature tototal neutrophil (I/T)ratio—to identifyinfected infants. Like most diagnostictests for neonatal sepsis, neutrophil in-dices have proven most useful for ex-cluding infants without infection ratherthan identifying infected neonates. Neu-tropenia may be a better marker forneonatal sepsis and has better speci-ficity than an elevated neutrophil count,because few conditions besides sepsis(maternal pregnancy-induced hyper-tension, asphyxia, and hemolytic dis-ease) depress the neutrophil count ofneonates.58 The definitions for neutro-penia vary with gestational age,58–61
type of delivery (infants born by cesar-ean delivery without labor have lowercounts than infants delivered vagi-nally),61 site of sampling (neutrophilcounts are lower in samples fromarterial blood),62 and altitude (infantsborn at elevated altitudes have highertotal neutrophil counts).63 In late pre-term and term infants, the definitionfor neutropenia most commonly usedis that suggested by Manroe et al(<1800/mm3 at birth and <7800/mm3
at 12–14 hours of age).58 Schmutz et alreinvestigated these reference rangesusing modern cell-counting instrumen-tation in 30 254 infants born at 23 to 42weeks’ gestation.61 Infants with diagnosesknown to affect neutrophil counts (eg,those born to women with pregnancy-induced hypertension or those withearly-onset sepsis) were excluded. Inthis study, the lower limits of normalfor neutrophil values at birth were3500/mm3 in infants born at >36 weeks’gestation, 1000/mm3 in infants born at
28 through 36 weeks’ gestation, and500/mm3 in infants born at <28 weeks’gestation. Peak values occurred at 6 to8 hours after birth; the lower limits ofnormal at that time were 7500/mm3,3500/mm3, and 1500/mm3 for infantsborn at >36 weeks’ gestation, 28 to36 weeks’ gestation, and <28 weeks’gestation, respectively.61 It is notewor-thy that the study by Schmutz et al wasperformed at 4800 feet above sea level,whereas that of Manroe et al was per-formed at 500 feet above sea level.
The absolute immature neutrophil countfollows a similar pattern to the absoluteneutrophil count and peaks at approx-imately 12 hours of life. The number ofimmature neutrophils increases from amaximal value of 1100 cells/mm3 atbirth to 1500 cells/mm3 at 12 hours ofage.58 Absolute immature counts havea poor sensitivity and positive predic-tive accuracy for early-onset sepsis.22
Furthermore, if exhaustion of bone mar-row reserves occurs, the number of im-mature forms will remain depressed.64
The I/T ratio has the best sensitivity ofany of the neutrophil indices. However,with manual counts, there are wideinterreader differences in band neu-trophil identification.65 The I/T ratio is<0.22 in 96% of healthy preterm infantsborn at <32 weeks’ gestational age.66
Unlike the absolute neutrophil countand the absolute band count, maximumnormal values for the I/T ratio occur atbirth (0.16) and decline with increasingpostnatal age to a minimum value of0.12.58 In healthy term infants, the 90thpercentile for the I/T ratio is 0.27.59
A single determination of the I/T ratiohas a poor positive predictive accuracy(approximately 25%) but a very highnegative predictive accuracy (99%).66
The I/T ratio may be elevated in 25% to50% of uninfected infants.67
Exhaustion of bone marrow reserveswill result in low band counts and leadto falsely low ratios. The timing of thewhite blood cell count is critical.68
Counts obtained 6 to 12 hours afterbirth are more likely to be abnormalthan are counts obtained at birth, be-cause alterations in the numbers (andratios) of mature and immature neutro-phils require an established inflammatoryresponse. Therefore, once the decision ismade to start antimicrobial therapysoon after birth, it is worth waiting 6 to12 hours before ordering a white bloodcell count and differential count.68,69
Platelet Counts
Despite the frequency of low plateletcounts in infected infants, they are anonspecific, insensitive, and late indica-tor of sepsis.70,71 Moreover, plateletcounts are not useful to follow clinicalresponse to antimicrobial agents, be-cause they often remain depressed fordays to weeks after a sepsis episode.
Acute-Phase Reactants
A wide variety of acute-phase reactantshave been evaluated in neonates withsuspected bacterial sepsis. However, onlyC-reactive protein (CRP) and procalcito-nin concentrations have been investiga-ted in sufficiently large studies.72,73 CRPconcentration increases within 6 to 8hours of an infectious episode in neo-nates and peaks at 24 hours.74,75 Thesensitivity of a CRP determination islow at birth, because it requires aninflammatory response (with releaseof interleukin-6) to increase CRP con-centrations.76 The sensitivity improvesdramatically if the first determinationis made 6 to 12 hours after birth. Benitzet al have demonstrated that excludinga value at birth, 2 normal CRP deter-minations (8–24 hours after birth and24 hours later) have a negative pre-dictive accuracy of 99.7% and a nega-tive likelihood ratio of 0.15 for provenneonatal sepsis.76 If CRP determina-tions remain persistently normal, it isstrong evidence that bacterial sepsis isunlikely, and antimicrobial agents can besafely discontinued. Data are insufficientto recommend following sequential CRP
PEDIATRICS Volume 129, Number 5, May 2012 1009
FROM THE AMERICAN ACADEMY OF PEDIATRICS

concentrations to determine the dura-tion of antimicrobial therapy in an infantwith an elevated value (≥1.0 mg/dL).Procalcitonin concentrations increasewithin 2 hours of an infectious episode,peak at 12 hours, and normalize within2 to 3 days in healthy adult volunteers.77
A physiologic increase in procalcitoninconcentration occurs within the first24 hours of birth, and an increase inserum concentrations can occur withnoninfectious conditions (eg, respira-tory distress syndrome).78 Procalcitoninconcentration has a modestly bettersensitivity than does CRP concentrationbut is less specific.73 Chiesa and col-leagues have published normal valuesfor procalcitonin concentrations in termand preterm infants.79 There is evidencefrom studies conducted in adult pop-ulations, the majority of which focusedon patients with sepsis in the ICU, thatsignificant reductions in use of anti-microbial agents can be achieved inpatients whose treatment is guided byprocalcitonin concentration.80
Sepsis Screening Panels
Hematologic scoring systems usingmultiple laboratory values (eg, whiteblood cell count, differential count, andplatelet count) have been recommen-ded as useful diagnostic aids. No matterwhat combination of tests is used, thepositive predictive accuracy of scoringsystems is poor unless the score isvery high. Rodwell et al described ascoring system in which a score of 1 wasassigned to 1 of 7 findings, includingabnormalities of leukocyte count, totalneutrophil count, increased immaturepolymorphonuclear leukocyte (PMN)count, increased I/T ratio, immature tomature PMN ratio >0.3, platelet count≤150 000/mm3, and pronounced degen-erative changes (ie, toxic granulations)in PMNs.81 In this study, two-thirdsof preterm infants and 90% of terminfants with a hematologic score≥3 did not have proven sepsis.81
Furthermore, scores obtained in thefirst several hours after birth have beenshown to have poorer sensitivity andnegative predictive value than scoresobtained at 24 hours of age.67 Sepsisscreening panels commonly includeneutrophil indices and acute-phase re-actants (usually CRP concentration). Thepositive predictive value of the sepsisscreen in neonates is poor (<30%);however, the negative predictive accuracyhas been high (>99%) in small clinicalstudies.22 Sepsis screening tests might beof value in deciding which “high-risk”healthy-appearing neonates do not needantimicrobial agents or whether therapycan be safely discontinued.
TREATMENT OF INFANTS WITHSUSPECTED EARLY-ONSET SEPSIS
In the United States, the most commonpathogens responsible for early-onsetneonatal sepsis are GBS and Escherichiacoli.17 A combination of ampicillin andan aminoglycoside (usually gentamicin)is generally used as initial therapy, andthis combination of antimicrobial agentsalso has synergistic activity againstGBS and Listeria monocytogenes.82,83
Third-generation cephalosporins (eg,cefotaxime) represent a reasonable al-ternative to an aminoglycoside. However,several studies have reported rapiddevelopment of resistance when cefo-taxime has been used routinely for thetreatment of early-onset neonatal sep-sis,84 and extensive/prolonged use ofthird-generation cephalosporins is a riskfactor for invasive candidiasis.85 Be-cause of its excellent CSF penetration,empirical or therapeutic use of cefo-taxime should be restricted for use ininfants with meningitis attributable toGram-negative organisms.86 Ceftriax-one is contraindicated in neonatesbecause it is highly protein boundand may displace bilirubin, leading to arisk of kernicterus. Bacteremia without anidentifiable focus of infection is generallytreated for 10 days.87 Uncomplicated
meningitis attributable to GBS is trea-ted for a minimum of 14 days.88 Otherfocal infections secondary to GBS (eg,cerebritis, osteomyelitis, endocarditis)are treated for longer durations.88 Gram-negative meningitis is treated forminimum of 21 days or 14 days afterobtaining a negative culture, whicheveris longer.88 Treatment of Gram-negativemeningitis should include cefotaximeand an aminoglycoside until the resultsof susceptibility testing are known.87,88
The duration of antimicrobial therapyin infants with negative blood culturesis controversial. Many women receiveantimicrobial agents during labor asprophylaxis to prevent early-onset GBSinfections or for management of sus-pected intra-amniontic infection orPPROM. In those instances, postnatalblood cultures may be sterile (falsenegative). When considering the dura-tion of therapy in infants with negativeblood cultures, the decision shouldinclude consideration of the clinicalcourse as well as the risks associatedwith longer courses of antimicrobialagents. In a retrospective study by Cor-dero and Ayers, the average duration oftreatment in 695 infants (<1000 g)with negative blood cultures was 5 ±3 days.89 Cotten et al have suggestedan association with prolonged adminis-tration of antimicrobial agents (>5 days)in infants with suspected early-onsetsepsis (and negative blood cultures)with death and necrotizing enterocoli-tis.90 Two recent papers also supportthis association.91,92
PREVENTION STRATEGIES FOREARLY-ONSET SEPSIS
The only intervention proven to decreasethe incidence of early-onset neonatalsepsis is maternal treatment withintrapartum intravenous antimicro-bial agents for the prevention of GBSinfections.93 Adequate prophylaxis isdefined as penicillin (the preferredagent), ampicillin, or cefazolin given for
1010 FROM THE AMERICAN ACADEMY OF PEDIATRICS

≥4 hours before delivery. Erythromycinis no longer recommended for prophy-laxis because of high resistance rates.In parturients who have a nonseriouspenicillin allergy, cefazolin is the drugof choice. For parturients with a historyof serious penicillin allergy (anaphy-laxis, angioedema, respiratory com-promise, or urticaria), clindamycin isan acceptable alternative agent, butonly if the woman’s rectovaginal GBSscreening isolate has been tested anddocumented to be susceptible. If theclindamycin susceptibility is unknownor the GBS isolate is resistant to clin-damycin, vancomycin is an alternativeagent for prophylaxis. However, nei-ther clindamycin nor vancomycin hasbeen evaluated for efficacy in pre-venting early-onset GBS sepsis inneonates. Intrapartum antimicrobialagents are indicated for the followingsituations93:
1. Positive antenatal cultures or molec-ular test at admission for GBS (ex-cept for women who have a cesareandelivery without labor or membranerupture)
2. Unknown maternal colonization sta-tus with gestation <37 weeks, rup-ture of membranes >18 hours, ortemperature >100.4°F (>38°C)
3. GBS bacteriuria during the currentpregnancy
4. Previous infant with invasive GBSdisease
Management guidelines for the new-born infant have been published93 andare available online (http://www.cdc.gov/groupbstrep/guidelines/index.html).
CLINICAL CHALLENGES
Challenge 1: Identifying NeonatesWith Clinical Signs of Sepsis Witha “High Likelihood” of Early-OnsetSepsis Who Require AntimicrobialAgents Soon After Birth
Most infants with early-onset sepsisexhibit abnormal signs in the first 24
hours of life. Approximately 1% of infantswill appear healthy at birth and thendevelop signs of infection after a vari-able time period.21 Every critically illinfant should be evaluated and receiveempirical broad-spectrum antimicrobialtherapy after cultures, even when thereare no obvious risk factors for sepsis.The greatest difficulty faced by clini-cians is distinguishing neonates withearly signs of sepsis from neonateswith noninfectious conditions with rel-atively mild findings (eg, tachypnea withor without an oxygen requirement). Inthis situation, data are insufficient toguide management. In more matureneonates without risk factors for in-fection who clinically improve over thefirst 6 hours of life (eg, need for oxygenis decreasing and respiratory distressis resolving), it is reasonable to with-hold antimicrobial therapy and monitorthe neonates closely. The 6-hour win-dow should not be considered absolute;however, most infants without infec-tion demonstrate some improvementover that time period. Any worsening ofthe infant’s condition should prompt
starting antimicrobial agents after cul-tures have been obtained.
Challenge 2: IdentifyingHealthy-Appearing Neonates Witha “High Likelihood” of Early-OnsetSepsis Who Require AntimicrobialAgents Soon After Birth
This category includes infants with 1 ofthe risk factors for sepsis noted pre-viously (colonization with GBS, prolongedrupture of membranes >18 hours, ormaternal chorioamnionitis). GBS is nota risk factor if the mother has receivedadequate intrapartum therapy (penicil-lin, ampicillin, or cefazolin for at least4 hours before delivery) or has a ce-sarean delivery with intact membranesin the absence of labor.93 The risk ofinfection in the newborn infant variesconsiderably with the risk factor pres-ent. The greatest risk of early-onsetsepsis occurs in infants born to womenwith chorioamnionitis who are alsocolonized with GBS and did not receiveintrapartum antimicrobial agents. Early-onset sepsis does occur in infants whoappear healthy at birth.21 Therefore,
FIGURE 1Evaluation of asymptomatic infants <37 weeks’ gestation with risk factors for sepsis. aThe diagnosisof chorioamnionitis is problematic and has important implications for the management of thenewborn infant. Therefore, pediatric providers are encouraged to speak with their obstetricalcolleagues whenever the diagnosis is made. bLumbar puncture is indicated in any infant witha positive blood culture or in whom sepsis is highly suspected on the basis of clinical signs, re-sponse to treatment, and laboratory results. IAP, intrapartum antimicrobial prophylaxis; WBC, whiteblood cell; Diff, differential white blood cell count.
PEDIATRICS Volume 129, Number 5, May 2012 1011
FROM THE AMERICAN ACADEMY OF PEDIATRICS

some clinicians use diagnostic testswith a high negative predictive accuracyas reassurance that infection is notpresent (allowing them to withholdantimicrobial agents). The decision ofwhether to treat a high-risk infantdepends on the risk factors present,the frequency of observations, andgestational age. The threshold for
initiating antimicrobial treatment gen-erally decreases with increasing num-bers of risk factors for infection andgreater degrees of prematurity. Sug-gested algorithms for management ofhealthy-appearing, high-risk infants areshown in Figs 1, 2, and 3. Screeningblood cultures have not been shown tobe of value.21
CONCLUSIONS
The diagnosis and management of neo-nates with suspected early-onset sepsisare based on scientific principles mod-ified by the “art and experience” of thepractitioner. The following are well-established concepts related to neo-natal sepsis:
1. Neonatal sepsis is a major cause ofmorbidity and mortality.
2. Diagnostic tests for early-onsetsepsis (other than blood or CSF cul-tures) are useful for identifying in-fants with a low probability of sepsisbut not at identifying infants likely tobe infected.
3. One milliliter of blood drawn beforeinitiating antimicrobial therapy isneeded to adequately detect bacter-emia if a pediatric blood culture bot-tle is used.
4. Cultures of superficial body sites,gastric aspirates, and urine are ofno value in the diagnosis of early-onset sepsis.
5. Lumbar puncture is not needed inall infants with suspected sepsis (es-pecially those who appear healthy)but should be performed for infantswith signs of sepsis who can safelyundergo the procedure, for infantswith a positive blood culture, for in-fants likely to be bacteremic (on thebasis of laboratory data), and infantswho do not respond to antimicrobialtherapy in the expected manner.
6. The optimal treatment of infants withsuspected early-onset sepsis isbroad-spectrum antimicrobial agents(ampicillin and an aminoglycoside).Once the pathogen is identified,antimicrobial therapy should benarrowed (unless synergism isneeded).
7. Antimicrobial therapy should bediscontinued at 48 hours in clinicalsituations in which the probabilityof sepsis is low.
FIGURE 2Evaluation of asymptomatic infants ≥37 weeks’ gestation with risk factors for sepsis. aThe diagnosisof chorioamnionitis is problematic and has important implications for the management of thenewborn infant. Therefore, pediatric providers are encouraged to speak with their obstetricalcolleagues whenever the diagnosis is made. bLumbar puncture is indicated in any infant witha positive blood culture or in whom sepsis is highly suspected on the basis of clinical signs, re-sponse to treatment, and laboratory results. WBC, white blood cell; Diff, differential white blood cellcount.
FIGURE 3Evaluation of asymptomatic infants ≥37 weeks’ gestation with risk factors for sepsis (nochorioamnionitis). aInadequate treatment: Defined as the use of an antibiotic other than penicillin,ampicillin, or cefazolin or if the duration of antibiotics before delivery was <4 h. bDischarge at 24 his acceptable if other discharge criteria have been met, access to medical care is readily accessible,and a person who is able to comply fully with instructions for home observation will be present. Ifany of these conditions is not met, the infant should be observed in the hospital for at least 48 h anduntil discharge criteria are achieved. IAP, intrapartum antimicrobial prophylaxis; WBC, white bloodcell; Diff, differential white blood cell count.
1012 FROM THE AMERICAN ACADEMY OF PEDIATRICS

LEAD AUTHORRichard A. Polin, MD
COMMITTEE ON FETUS ANDNEWBORN, 2011–2012Lu-Ann Papile, MD, ChairpersonJill E. Baley, MDWilliam Benitz, MDWaldemar A. Carlo, MDJames Cummings, MDPraveen Kumar, MDRichard A. Polin, MD
Rosemarie C. Tan, MD, PhDKasper S. Wang, MDKristi L. Watterberg, MD
FORMER COMMITTEE MEMBERVinod K. Bhutani, MD
LIAISONSCAPT Wanda Denise Barfield, MD, MPH – Centersfor Disease Control and PreventionGeorge Macones, MD – American College ofObstetricians and Gynecologists
Ann L. Jefferies, MD – Canadian Paediatric SocietyRosalie O. Mainous, PhD, RNC, NNP – NationalAssociation of Neonatal NursesTonse N. K. Raju, MD, DCH – National Institutesof Health
FORMER LIAISONWilliam Barth, Jr, MD – American College ofObstetricians and Gynecologists
STAFFJim Couto, MA
REFERENCES
1. Escobar GJ. The neonatal “sepsis work-up”:personal reflections on the development ofan evidence-based approach toward newborninfections in a managed care organization.Pediatrics. 1999;103(1, suppl E):360–373
2. Polin RA, St Geme JW III. Neonatal sepsis.Adv Pediatr Infect Dis. 1992;7:25–61
3. Riley LE, Celi AC, Onderdonk AB, et al. Asso-ciation of epidural-related fever and non-infectious inflammation in term labor. ObstetGynecol. 2011;117(3):588–595
4. Stoll BJ, Hansen NI, Bell EF, et al; EuniceKennedy Shriver National Institute of ChildHealth and Human Development NeonatalResearch Network. Neonatal outcomes ofextremely preterm infants from the NICHDNeonatal Research Network. Pediatrics.2010;126(3):443–456
5. Tita AT, Andrews WW. Diagnosis and man-agement of clinical chorioamnionitis. ClinPerinatol. 2010;37(2):339–354
6. Gibbs RS, Duff P. Progress in pathogenesisand management of clinical intraamnioticinfection. Am J Obstet Gynecol. 1991;164(5pt 1):1317–1326
7. Romero R, Quintero R, Oyarzun E, et al.Intraamniotic infection and the onset oflabor in preterm premature rupture of themembranes. Am J Obstet Gynecol. 1988;159(3):661–666
8. DiGiulio DB, Romero R, Kusanovic JP, et al.Prevalence and diversity of microbes in theamniotic fluid, the fetal inflammatory response,and pregnancy outcome in women with pre-term pre-labor rupture of membranes. Am JReprod Immunol. 2010;64(1):38–57
9. DiGiulio DB, Romero R, Amogan HP, et al.Microbial prevalence, diversity and abun-dance in amniotic fluid during pretermlabor: a molecular and culture-based in-vestigation. PLoS ONE. 2008;3(8):e3056
10. Viscardi RM. Ureaplasma species: role indiseases of prematurity. Clin Perinatol.2010;37(2):393–409
11. Goldenberg RL, Andrews WW, Goepfert AR,et al The Alabama Preterm Birth Study:umbilical cord blood Ureaplasma ure-alyticum and Mycoplasma hominis cul-tures in very preterm newborn infants.Am J Obstet Gynecol. 2008;198(1):43.e1–43.e5
12. Benitz WE, Gould JB, Druzin ML. Risk factorsfor early-onset group B streptococcal sep-sis: estimation of odds ratios by criticalliterature review. Pediatrics. 1999;103(6).Available at: www.pediatrics.org/cgi/content/full/103/6/e77
13. Newton ER, Clark M. Group B streptococcusand preterm rupture of membranes. ObstetGynecol. 1988;71(2):198–202
14. Schuchat A, Zywicki SS, Dinsmoor MJ, et al.Risk factors and opportunities for preven-tion of early-onset neonatal sepsis: a multi-center case-control study. Pediatrics. 2000;105(1 pt 1):21–26
15. Schrag SJ, Hadler JL, Arnold KE, Martell-Cleary P, Reingold A, Schuchat A. Risk fac-tors for invasive, early-onset Escherichiacoli infections in the era of widespreadintrapartum antibiotic use. Pediatrics. 2006;118(2):570–576
16. Martius JA, Roos T, Gora B, et al. Risk fac-tors associated with early-onset sepsis inpremature infants. Eur J Obstet GynecolReprod Biol. 1999;85(2):151–158
17. Stoll BJ, Hansen NI, Sánchez PJ, et al;Eunice Kennedy Shriver National Institute ofChild Health and Human Development Neo-natal Research Network. Early onset neonatalsepsis: the burden of group B Streptococcaland E. coli disease continues. Pediatrics.2011;127(5):817–826
18. Wynn JL, Levy O. Role of innate hostdefenses in susceptibility to early-onsetneonatal sepsis. Clin Perinatol. 2010;37(2):307–337
19. Escobar GJ, Li DK, Armstrong MA, et al.Neonatal sepsis workups in infants >/=2000
grams at birth: A population-based study.Pediatrics. 2000;106(2 pt 1):256–263
20. Buckler B, Bell J, Sams R, et al. Unnecessaryworkup of asymptomatic neonates in theera of group B streptococcus prophylaxis[published online ahead of print August 22,2010]. Infect Dis Obstet Gynecol. doi:
21. Ottolini MC, Lundgren K, Mirkinson LJ,Cason S, Ottolini MG. Utility of completeblood count and blood culture screening todiagnose neonatal sepsis in the asymp-tomatic at risk newborn. Pediatr Infect DisJ. 2003;22(5):430–434
22. Gerdes JS. Clinicopathologic approach tothe diagnosis of neonatal sepsis. Clin Per-inatol. 1991;18(2):361–381
23. Schelonka RL, Chai MK, Yoder BA, Hensley D,Brockett RM, Ascher DP. Volume of bloodrequired to detect common neonatal patho-gens. J Pediatr. 1996;129(2):275–278
24. Dietzman DE, Fischer GW, Schoenknecht FD.Neonatal Escherichia coli septicemia—bacterial counts in blood. J Pediatr. 1974;85(1):128–130
25. Kellogg JA, Ferrentino FL, Goodstein MH,Liss J, Shapiro SL, Bankert DA. Frequency oflow level bacteremia in infants from birthto two months of age. Pediatr Infect Dis J.1997;16(4):381–385
26. Neal PR, Kleiman MB, Reynolds JK, Allen SD,Lemons JA, Yu PL. Volume of blood sub-mitted for culture from neonates. J ClinMicrobiol. 1986;24(3):353–356
27. Connell TG, Rele M, Cowley D, Buttery JP,Curtis N. How reliable is a negative bloodculture result? Volume of blood submittedfor culture in routine practice in a children’shospital. Pediatrics. 2007;119(5):891–896
28. Pourcyrous M, Korones SB, Bada HS, Patter-son T, Baselski V. Indwelling umbilical arte-rial catheter: a preferred sampling site forblood culture. Pediatrics. 1988;81(6):821–825
29. Anagnostakis D, Kamba A, Petrochilou V,Arseni A, Matsaniotis N. Risk of infection
PEDIATRICS Volume 129, Number 5, May 2012 1013
FROM THE AMERICAN ACADEMY OF PEDIATRICS

associated with umbilical vein catheterization.A prospective study in 75 newborn infants.J Pediatr. 1975;86(5):759–765
30. Polin JI, Knox I, Baumgart S, Campman E,Mennuti MT, Polin RA. Use of umbilical cordblood culture for detection of neonatal bac-teremia. Obstet Gynecol. 1981;57(2):233–237
31. Visser VE, Hall RT. Urine culture in theevaluation of suspected neonatal sepsis.J Pediatr. 1979;94(4):635–638
32. Vasan U, Lim DM, Greenstein RM, Raye JR.Origin of gastric aspirate polymorphonuclearleukocytes in infants born after prolongedrupture of membranes. J Pediatr. 1977;91(1):69–72
33. Mims LC, Medawar MS, Perkins JR, GrubbWR. Predicting neonatal infections by evalu-ation of the gastric aspirate: a study in twohundred and seven patients. Am J ObstetGynecol. 1972;114(2):232–238
34. Choi Y, Saha SK, Ahmed AS, et al. Routineskin cultures in predicting sepsis pathogensamong hospitalized preterm neonates inBangladesh. Neonatology. 2008;94(2):123–131
35. Evans ME, Schaffner W, Federspiel CF, CottonRB, McKee KT, Jr, Stratton CW. Sensitivity,specificity, and predictive value of bodysurface cultures in a neonatal intensivecare unit. JAMA. 1988;259(2):248–252
36. Sherman MP, Goetzman BW, Ahlfors CE,Wennberg RP. Tracheal asiration and itsclinical correlates in the diagnosis ofcongenital pneumonia. Pediatrics. 1980;65(2):258–263
37. Srinivasan HB, Vidyasagar D. Endotrachealaspirate cultures in predicting sepsis inventilated neonates. Indian J Pediatr. 1998;65(1):79–84
38. Johnson CE, Whitwell JK, Pethe K, Saxena K,Super DM. Term newborns who are at riskfor sepsis: are lumbar punctures necessary?Pediatrics. 1997;99(4). Available at: www.pediatrics.org/cgi/content/full/99/4/e10
39. Eldadah M, Frenkel LD, Hiatt IM, Hegyi T.Evaluation of routine lumbar punctures innewborn infants with respiratory distresssyndrome. Pediatr Infect Dis J. 1987;6(3):243–246
40. Isaacs D, Barfield CP, Grimwood K, McPheeAJ, Minutillo C, Tudehope DI; Australian StudyGroup for Neonatal Infections. Systemicbacterial and fungal infections in infantsin Australian neonatal units. Med J Aust.1995;162(4):198–201
41. May M, Daley AJ, Donath S, Isaacs D; Aus-tralasian Study Group for Neonatal Infec-tions. Early onset neonatal meningitis inAustralia and New Zealand, 1992–2002. ArchDis Child Fetal Neonatal Ed. 2005;90(4):F324–F327
42. Stoll BJ, Hansen N, Fanaroff AA, et al. To tapor not to tap: high likelihood of meningitiswithout sepsis among very low birth weightinfants. Pediatrics. 2004;113(5):1181–1186
43. Garges HP, Moody MA, Cotten CM, et al.Neonatal meningitis: what is the correlationamong cerebrospinal fluid cultures, bloodcultures, and cerebrospinal fluid parame-ters? Pediatrics. 2006;117(4):1094–1100
44. Shah SS, Ebberson J, Kestenbaum LA, HodinkaRL, Zorc JJ. Age-specific reference values forcerebrospinal fluid protein concentration inneonates and young infants. J Hosp Med.2011;6(1):22–27
45. Byington CL, Kendrick J, Sheng X. Normativecerebrospinal fluid profiles in febrile in-fants. J Pediatr. 2011;158(1):130–134
46. Ahmed A, Hickey SM, Ehrett S, et al. Cere-brospinal fluid values in the term neonate.Pediatr Infect Dis J. 1996;15(4):298–303
47. Bonadio WA, Stanco L, Bruce R, Barry D, SmithD. Reference values of normal cerebrospinalfluid composition in infants ages 0 to 8 weeks.Pediatr Infect Dis J. 1992;11(7):589–591
48. Nascimento-Carvalho CM, Moreno-CarvalhoOA. Normal cerebrospinal fluid values infull-term gestation and premature neo-nates. Arq Neuropsiquiatr. 1998;56(3A):375–380
49. Martín-Ancel A, García-Alix A, Salas S, DelCastillo F, Cabañas F, Quero J. Cerebrospi-nal fluid leucocyte counts in healthy neo-nates. Arch Dis Child Fetal Neonatal Ed.2006;91(5):F357–F358
50. Kestenbaum LA, Ebberson J, Zorc JJ, HodinkaRL, Shah SS. Defining cerebrospinal fluidwhite blood cell count reference values inneonates and young infants. Pediatrics. 2010;125(2):257–264
51. Smith PB, Garges HP, Cotton CM, Walsh TJ,Clark RH, Benjamin DK Jr. Meningitis inpreterm neonates: importance of cerebro-spinal fluid parameters. Am J Perinatol.2008;25(7):421–426
52. Smith PB, Cotten CM, Garges HP, et al. Acomparison of neonatal Gram-negative rodand Gram-positive cocci meningitis. J Per-inatol. 2006;26(2):111–114
53. Greenberg RG, Smith PB, Cotten CM, MoodyMA, Clark RH, Benjamin DK Jr. Traumaticlumbar punctures in neonates: test per-formance of the cerebrospinal fluid whiteblood cell count. Pediatr Infect Dis J. 2008;27(12):1047–1051
54. Kanegaye JT, Nigrovic LE, Malley R, et al;American Academy of Pediatrics, PediatricEmergency Medicine Collaborative ResearchCommittee. Diagnostic value of immatureneutrophils (bands) in the cerebrospinalfluid of children with cerebrospinal fluidpleocytosis. Pediatrics. 2009;123(6). Available
at: www.pediatrics.org/cgi/content/full/123/6/e967
55. Rajesh NT, Dutta S, Prasad R, Narang A. Effectof delay in analysis on neonatal cerebrospinalfluid parameters. Arch Dis Child FetalNeonatal Ed. 2010;95(1):F25–F29
56. Christensen RD, Rothstein G, Hill HR, Hall RT.Fatal early onset group B streptococcalsepsis with normal leukocyte counts.Pediatr Infect Dis. 1985;4(3):242–245
57. Engle WD, Rosenfeld CR. Neutropenia inhigh-risk neonates. J Pediatr. 1984;105(6):982–986
58. Manroe BL, Weinberg AG, Rosenfeld CR,Browne R. The neonatal blood count inhealth and disease. I. Reference values forneutrophilic cells. J Pediatr. 1979;95(1):89–98
59. Schelonka RL, Yoder BA, desJardins SE, HallRB, Butler J. Peripheral leukocyte countand leukocyte indexes in healthy newbornterm infants. J Pediatr. 1994;125(4):603–606
60. Mouzinho A, Rosenfeld CR, Sánchez PJ, RisserR. Revised reference ranges for circulatingneutrophils in very-low-birth-weight neonates.Pediatrics. 1994;94(1):76–82
61. Schmutz N, Henry E, Jopling J, ChristensenRD. Expected ranges for blood neutrophilconcentrations of neonates: the Manroeand Mouzinho charts revisited. J Perinatol.2008;28(4):275–281
62. Christensen RD, Rothstein G. Pitfalls in theinterpretation of leukocyte counts of newborninfants. Am J Clin Pathol. 1979;72(4):608–611
63. Lambert RM, Baer VL, Wiedmeier SE, HenryE, Burnett J, Christensen RD. Isolated ele-vated blood neutrophil concentration ataltitude does not require NICU admission ifappropriate reference ranges are used.J Perinatol. 2009;29(12):822–825
64. Christensen RD, Rothstein G. Exhaustion ofmature marrow neutrophils in neonateswith sepsis. J Pediatr. 1980;96(2):316–318
65. Schelonka RL, Yoder BA, Hall RB, et al. Dif-ferentiation of segmented and band neu-trophils during the early newborn period.J Pediatr. 1995;127(2):298–300
66. Lloyd BW, Oto A. Normal values for matureand immature neutrophils in very pretermbabies. Arch Dis Child. 1982;57(3):233–235
67. Gerdes JS, Polin RA. Sepsis screen in neo-nates with evaluation of plasma fibronec-tin. Pediatr Infect Dis J. 1987;6(5):443–446
68. Newman TB, Puopolo KM, Wi S, Draper D,Escobar GJ. Interpreting complete bloodcounts soon after birth in newborns at riskfor sepsis. Pediatrics. 2010;126(5):903–909
69. Rozycki HJ, Stahl GE, Baumgart S. Impairedsensitivity of a single early leukocyte countin screening for neonatal sepsis. PediatrInfect Dis J. 1987;6(5):440–442
1014 FROM THE AMERICAN ACADEMY OF PEDIATRICS

70. Manzoni P, Mostert M, Galletto P, et al. Isthrombocytopenia suggestive of organism-specific response in neonatal sepsis?Pediatr Int. 2009;51(2):206–210
71. Guida JD, Kunig AM, Leef KH, McKenzie SE,Paul DA. Platelet count and sepsis in very lowbirth weight neonates: is there an organism-specific response? Pediatrics. 2003;111(6 pt1):1411–1415
72. Vouloumanou EK, Plessa E, KarageorgopoulosDE, Mantadakis E, Falagas ME. Serumprocalcitonin as a diagnostic marker forneonatal sepsis: a systematic review andmeta-analysis. Intensive Care Med. 2011;37(5):747–762
73. Benitz WE. Adjunct laboratory tests in thediagnosis of early-onset neonatal sepsis.Clin Perinatol. 2010;37(2):421–438
74. Gabay C, Kushner I. Acute-phase proteins andother systemic responses to inflammation.N Engl J Med. 1999;340(6):448–454
75. Philip AG. Response of C-reactive proteinin neonatal Group B streptococcal in-fection. Pediatr Infect Dis. 1985;4(2):145–148
76. Benitz WE, Han MY, Madan A, RamachandraP. Serial serum C-reactive protein levels inthe diagnosis of neonatal infection. Pedi-atrics. 1998;102(4). Available at: www.pedi-atrics.org/cgi/content/full/102/4/e41
77. Dandona P, Nix D, Wilson MF, et al. Procalci-tonin increase after endotoxin injection innormal subjects. J Clin Endocrinol Metab.1994;79(6):1605–1608
78. Lapillonne A, Basson E, Monneret G, BienvenuJ, Salle BL. Lack of specificity of procalcitoninfor sepsis diagnosis in premature infants.Lancet. 1998;351(9110):1211–1212
79. Chiesa C, Natale F, Pascone R, et al. C re-active protein and procalcitonin: referenceintervals for preterm and term newbornsduring the early neonatal period. Clin ChimActa. 2011;412(11-12):1053–1059
80. Hayashi Y, Paterson DL. Strategies for re-duction in duration of antibiotic use inhospitalized patients. Clin Infect Dis. 2011;52(10):1232–1240
81. Rodwell RL, Leslie AL, Tudehope DI. Earlydiagnosis of neonatal sepsis using a he-matologic scoring system. J Pediatr. 1988;112(5):761–767
82. Baker CN, Thornsberry C, Facklam RR. Syn-ergism, killing kinetics, and antimicrobialsusceptibility of group A and B streptococci.Antimicrob Agents Chemother. 1981;19(5):716–725
83. MacGowan A, Wootton M, Bowker K, HoltHA, Reeves D. Ampicillin-aminoglycoside in-teraction studies using Listeria monocy-togenes. J Antimicrob Chemother. 1998;41(3):417–418
84. Bryan CS, John JF, Jr, Pai MS, Austin TL.Gentamicin vs cefotaxime for therapy of neo-natal sepsis. Relationship to drug resistance.Am J Dis Child. 1985;139(11):1086–1089
85. Manzoni P, Farina D, Leonessa M, et al. Riskfactors for progression to invasive fungalinfection in preterm neonates with fungalcolonization. Pediatrics. 2006;118(6):2359–2364
86. Bégué P, Floret D, Mallet E, et al. Pharma-cokinetics and clinical evaluation of cefo-taxime in children suffering with purulentmeningitis. J Antimicrob Chemother. 1984;14(suppl B):161–165
87. Nizet V, Klein JO. Bacterial sepsis and men-ingitis. In: Remington JS, Klein JO, WilsonChristopher B, Nizet V, eds. Infectious Dis-eases of the Fetus and Newborn Infant. 7thed. Philadelphia, PA: Saunders; 2010:222–275
88. Pickering LK, Baker CJ, Kimberlin DW, LongSS, eds. Red Book: 2009 Report of theCommittee on Infectious Diseases. 28th ed.Elk Grove Village, IL: American Academy ofPediatrics; 2009
89. Cordero L, Ayers LW. Duration of empiricantibiotics for suspected early-onset sep-sis in extremely low birth weight infants.Infect Control Hosp Epidemiol. 2003;24(9):662–666
90. Cotten CM, Taylor S, Stoll B, et al; NICHDNeonatal Research Network. Prolonged du-ration of initial empirical antibiotic treat-ment is associated with increased rates ofnecrotizing enterocolitis and death forextremely low birth weight infants. Pedi-atrics. 2009;123(1):58–66
91. Kuppala VS, Meinzen-Derr J, Morrow AL,Schibler KR. Prolonged initial empiricalantibiotic treatment is associated with ad-verse outcomes in premature infants.J Pediatr. 2011;159(5):720–725
92. Alexander VN, Northrup V, Bizzarro MJ.Antibiotic exposure in the newborn in-tensive care unit and the risk of necrotiz-ing enterocolitis. J Pediatr. 2011;159(3):392–397
93. Centers for Disease Control and Prevention.Prevention of perinatal group B strepto-coccal disease—revised guidelines fromCDC, 2010. MMWR Recomm Rep. 2010;59(RR-10):1–36
PEDIATRICS Volume 129, Number 5, May 2012 1015
FROM THE AMERICAN ACADEMY OF PEDIATRICS

DOI: 10.1542/peds.2011-1466; originally published online August 1, 2011;Pediatrics
NEWBORNCOMMITTEE ON INFECTIOUS DISEASES AND COMMITTEE ON FETUS AND
DiseaseRecommendations for the Prevention of Perinatal Group B Streptococcal (GBS)
http://pediatrics.aappublications.org/content/early/2011/07/28/peds.2011-1466
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Mc Master University on November 26, 2012pediatrics.aappublications.orgDownloaded from

POLICY STATEMENT
Recommendations for the Prevention of Perinatal GroupB Streptococcal (GBS) Disease
abstractThe Centers for Disease Control and Prevention (CDC) guidelines forthe prevention of perinatal group B streptococcal (GBS) disease wereinitially published in 1996. The American Academy of Pediatrics (AAP)also published a policy statement on this topic in 1997. In 2002, the CDCpublished revised guidelines that recommended universal antenatalGBS screening; the AAP endorsed these guidelines and published rec-ommendations based on them in the 2003 Red Book. Since then, theincidence of early-onset GBS disease in neonates has decreased by anestimated 80%. However, in 2010, GBS disease remained the leadingcause of early-onset neonatal sepsis. The CDC issued revised guide-lines in 2010 based on evaluation of data generated after 2002. Theserevised and comprehensive guidelines, which have been endorsed bythe AAP, reaffirm the major prevention strategy—universal antenatalGBS screening and intrapartum antibiotic prophylaxis for culture-positive and high-risk women—and include new recommendations forlaboratory methods for identification of GBS colonization during preg-nancy, algorithms for screening and intrapartum prophylaxis forwomen with preterm labor and premature rupture of membranes,updated prophylaxis recommendations for women with a penicillinallergy, and a revised algorithm for the care of newborn infants. Thepurpose of this policy statement is to review and discuss the differ-ences between the 2002 and 2010 CDC guidelines that are most rele-vant for the practice of pediatrics. Pediatrics 2011;128:000
INTRODUCTIONGroup B streptococcal (GBS) disease has been a leading cause of neo-natal morbidity and mortality since the 1970s.1,2 Maternal colonizationwith GBS in the genitourinary or gastrointestinal tract and transmis-sion to the infant during the labor-and-delivery process is the principalrisk factor for early-onset invasive GBS disease.3 Women who are iden-tified as being GBS-colonized through culture-based screening aremore than 25 times more likely to deliver an infant with early-onsetinfection than are women with negative prenatal cultures.4 Identifica-tion of maternal colonization through universal, culture-based screen-ing with intrapartum antibiotic prophylaxis (IAP) for women with pos-itive screening results has been recommended since 2002.5 Thisstrategy, endorsed by the American Academy of Pediatrics, has beenwidely adopted in the United States and has resulted in an estimated80% decrease in early-onset GBS infection.6
COMMITTEE ON INFECTIOUS DISEASES AND COMMITTEE ONFETUS AND NEWBORN
KEY WORDSgroup B Streptococcus, early onset, diagnosis, prophylaxis,penicillin allergy, treatment
ABBREVIATIONSGBS—group B streptococcal/StreptococcusIAP—intrapartum antibiotic prophylaxisCDC—Centers for Disease Control and PreventionCBC—complete blood cell
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authorshave filed conflict of interest statements with the AmericanAcademy of Pediatrics. Any conflicts have been resolved througha process approved by the Board of Directors. The AmericanAcademy of Pediatrics has neither solicited nor accepted anycommercial involvement in the development of the content ofthis publication.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-1466
doi:10.1542/peds.2011-1466
All policy statements from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
FROM THE AMERICAN ACADEMY OF PEDIATRICS
Organizational Principles to Guide and Define the ChildHealth Care System and/or Improve the Health of all Children
PEDIATRICS Volume 128, Number 3, September 2011 1 at Mc Master University on November 26, 2012pediatrics.aappublications.orgDownloaded from

However, even in the era of universalscreening, cases of GBS disease con-tinue to occur.7–11 To evaluate datapublished after the Centers for Dis-ease Control and Prevention (CDC) is-sued guidelines for the prevention ofGBS perinatal disease in 2002, the CDCcalled a meeting of clinical and publichealth representatives in June 2009.The goal of the meeting was to identifypotentially modifiable reasons for con-tinued GBS disease and to addressthese issues. The American Academyof Pediatrics was represented bymembers of its Committee on Infec-tious Diseases and Committee on Fe-tus and Newborn. The purpose of thispolicy statement is to review and dis-cuss the differences between the 2002and 2010 CDC guidelines that are mostrelevant for the practice of pediatrics.Table 1 outlines the evidence-basedrating system that supports each rec-ommendation; strength (indicated bya letter) and quality (indicated by aroman numeral) of evidence areshown in parentheses. The 2010 CDCguidelines can be accessed online(www.cdc.gov/groupbstrep/guidelines/guidelines.html).
LABORATORY DIAGNOSIS OF GBSCOLONIZATION
The2002guidelines from theCDC recom-mended universal culture-based screen-ing forGBSat35 to37weeksofgestation.In the intervening years, new diagnostictechnologies have been developed, in-cluding pigmented enrichment broths,chromogenic agars, DNA probes, andnucleic acid amplification tests (NAATs).These methods have been validated forantenatal testing for GBS colonizationand are used in many clinical laborato-ries, which enables more rapid identifi-cation of GBS. A positive test result forGBS by culture, DNA probe, or NAAT per-formed during antenatal screening indi-cates colonization, and the womanshould receive IAP. However, infantswithearly-onset GBS can be born to womenwith negative antenatal screening re-sults, because all laboratory-screeningmethods are imperfect. Culture-basedscreening, especially if processing in thelaboratory does not always follow theCDC guidelines, may not identify all colo-nized women.7,11 Infants with signs andsymptoms of sepsis should be managedaccording to the neonatal algorithm (Fig1) and receive an initial antibiotic reg-
imen that includes ampicillin regard-less of maternal screening results.
Recommendations
● Options for GBS identification fromculture of maternal vaginal/rectalswabs have been expanded to in-clude a positive identification fromchromogenic agarmedia. Identifica-tion of GBS directly by nucleic acidamplification tests (NAATs), such ascommercially available polymerasechain reaction assays, can also beused after broth enrichment if labo-ratories have validated their NAATperformance and instituted appro-priate quality controls (CII).
INTRAPARTUM ANTIBIOTICPROPHYLAXIS
Penicillin and ampicillin have eachbeen demonstrated in controlled clini-cal trials to be effective in preventingearly-onset GBS disease when admin-istered during labor.12,13 Penicillin andampicillin at the recommended dos-ages for IAP rapidly achieve therapeu-tic concentrations in the fetal circula-tion and then amniotic fluid. Cefazolinhas similar pharmacokinetics whencompared with penicillin, and IAP dos-
TABLE 1 Evidence-Based Rating System Used to Determine Strength of Recommendations
Category Definition Recommendation
Strength of recommendationA Strong evidence for efficacy and substantial clinical benefit Strongly recommendedB Strong or moderate evidence for efficacy, but only limited clinical benefit Generally recommendedC Insufficient evidence for efficacy, or efficacy does not outweigh possible adverse consequences OptionalD Moderate evidence against efficacy or for adverse outcome Generally not recommendedE Strong evidence against efficacy or for adverse outcome Never recommendedQuality of evidence supportingrecommendationI Evidence from at least 1 well-executed randomized, controlled trial or 1 rigorously designed
laboratory-based experimental study that has been replicated by an independentinvestigator
II Evidence from at least 1 well-designed clinical trial without randomization; cohort or case-controlled analytic studies (preferably from more than 1 center); multiple time-seriesstudies; dramatic results from uncontrolled studies; or some evidence from laboratoryexperiments
III Evidence from opinions of respected authorities based on clinical or laboratory experience,descriptive studies, or reports of expert committees
Adapted with permission from Centers for Disease Control and Prevention. Guidelines for the prevention and treatment of opportunistic infections among HIV-exposed and HIV-infectedchildren: recommendations from CDC, the National Institutes of Health, the HIV Medicine Association of the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society,and the American Academy of Pediatrics. MMWR Recomm Rep. 2009;58(RR-11):1–166.
2 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Mc Master University on November 26, 2012pediatrics.aappublications.orgDownloaded from

ing achieves high intra-amniotic con-centrations.14–16 Cefazolin has been thepreferred alternative for IAP forpenicillin-allergic women at low risk ofanaphylaxis since 2002, although it hasbeen used uncommonly for this indica-tion. At least 4 hours of IAP with one ofthese �-lactam antibiotics is effectivein preventing early-onset GBS diseasein neonates. The definition of adequateIAP has been clarified to include peni-cillin, ampicillin, or cefazolin for atleast 4 hours before delivery. Duration
of IAP shorter than 4 hours and allother regimens, including clindamycinand vancomycin, are considered to beinadequate prophylaxis for infants be-cause of lack of data regarding effi-cacy and limited data regarding favor-able pharmacokinetics. No clinicaltrials have evaluated the efficacy ofnon–�-lactam regimens for IAP inwomen with serious penicillin allergy.Although clindamycin is the most com-monly chosen IAP regimen in theUnited States for penicillin-allergic
women at low risk of anaphylaxis, cur-rent data indicate that approximately20% of GBS isolates are resistantto clindamycin. Clindamycin shouldnever be used for IAP if susceptibilitytesting of the mother’s GBS isolate hasnot been performed. Several recentstudies have revealed that susceptibil-ity testing is rarely performed on GBSisolates,5,6,17 and early-onset GBS dis-ease has been reported in infants bornto mothers who have received clinda-mycin IAP.11,17
Recommendations
● Penicillin remains the agent ofchoice for IAP, and ampicillin is anacceptable alternative (AI).
● Penicillin-allergic women who donot have a history of anaphylaxis,angioedema, respiratory distress,or urticaria after administration ofpenicillin or a cephalosporin shouldreceive cefazolin (BII).
● Penicillin-allergic women at highrisk of anaphylaxis should receiveclindamycin if their GBS isolate issusceptible or vancomycin if theirGBS isolate is intrinsically resistantto clindamycin (CIII).
● The definition of adequate IAP hasbeen clarified to be at least 4 hoursof penicillin, ampicillin, or cefazolin.The initial intravenous dose of peni-cillin is 5 million units; for ampicillinand cefazolin, the initial dose is 2 g(AIII).
● All other antibiotics, doses, or dura-tions are considered inadequate forthe purposes of neonatal manage-ment (AIII).
PREVENTION OF EARLY-ONSET GBSDISEASE
The revised 2010 GBS American Acad-emy of Pediatrics guidelines for neona-tal management were designed tobroaden the scope to include all neo-nates, to increase the clarity of the rec-ommendations, and to decrease un-
No
No
No
No
Yes
No
Yes
Yes
Yes
Yes
YesSigns of neonatal sepsis? Full diagnostic evaluationa Antibiotic therapyb
Maternal chorioamnionitis?c Limited evaluationd
Antibiotic therapyb
GBS prophylaxis indicated for mother?e
Routine clinical caref
Mother received ≥4 h of penicillin, ampicillin, or cefazolin IV?
Observation for ≥48 hf,g
≥37 wk and duration of membrane rupture < 18 h?
Observation for ≥48 hf,h
Either <37 wk or duration of membrane rupture ≥ 18 h?
Limited evaluationd
Observation for ≥48 hf
FIGURE 1Algorithm for the prevention of early-onset GBS infection in the newborn. (Adapted with permissionfrom Centers for Disease Control and Prevention. Prevention of perinatal group B streptococcaldisease: prevention of perinatal group B streptococcal disease from CDC, 2010. MMWR Recomm Rep.2010;59[RR-10]:1–32.) a Full diagnostic evaluation includes a blood culture; CBC count, including whiteblood cell differential and platelet counts; chest radiograph (if respiratory abnormalities are pres-ent); and lumbar puncture (if the patient is stable enough to tolerate procedure and sepsis issuspected). b Antibiotic therapy should be directed toward the most common causes of neonatalsepsis, including intravenous ampicillin for GBS and coverage for other organisms (including Esche-richia coli and other Gram-negative pathogens) and should take into account local antibiotic-resistance patterns. c Consultation with obstetric providers is important in determining the level ofclinical suspicion for chorioamnionitis. Chorioamnionitis is diagnosed clinically, and some of thesigns are nonspecific. d Limited evaluation includes blood culture (at birth) and CBC count withdifferential and platelets (at birth and/or at 6–12 hours of life). e GBS prophylaxis is indicated if 1 ormore of the following is true: (1) mother is GBS-positive within the preceding 5 weeks; (2) GBS statusis unknown and there are 1 or more intrapartum risk factors, including �37 weeks’ gestation,rupture of membranes for �18 hours, or temperature of �100.4°F (38.0°C); (3) GBS bacteriuriaduring current pregnancy; or (4) history of a previous infant with GBS disease. f If signs of sepsisdevelop, a full diagnostic evaluation should be performed, and antibiotic therapy should be initiated.g If at�37 weeks’ gestation, observation may occur at home after 24 hours if other discharge criteriahave been met, there is ready access to medical care, and a person who is able to comply fully withinstructions for home observation will be present. If any of these conditions is not met, the infantshould be observed in the hospital for at least 48 hours and until discharge criteria have beenachieved. h Some experts recommend a CBC count with differential and platelets at 6 to 12 hours ofage.24 IV indicates intravenously.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 3, September 2011 3 at Mc Master University on November 26, 2012pediatrics.aappublications.orgDownloaded from

necessary laboratory evaluations andempirical antibiotics for infants at lowrisk. Although this strategy will neverprevent all infections, the revisedguidelines should result in a furtherdecrease in cases of perinatal GBS dis-ease. The management of neonatescontinues to be based on clinical signs,the presence of maternal risk factorsfor GBS neonatal disease, and thelikely efficacy of IAP (or maternal anti-microbial treatment in the case of clin-ical or occult chorioamnionitis) inpreventing early-onset disease. The re-vised infant management algorithm(Fig 1) is derived from recent datasummarized in the published CDC doc-ument regarding the epidemiology ofGBS disease and the usefulness of a“limited evaluation” of well-appearingneonates.
All newborn infants with signs sugges-tive of sepsis should have a full diag-nostic evaluation, including a lumbarpuncture if the infant is stable enoughto undergo the procedure; 15% to 38%of infants with early-onset meningitishave sterile blood cultures, so evaluat-ing the cerebrospinal fluid is requiredfor optimal diagnostic sensitivity.18–21 Ifthe care provider believes that a non-infectious condition is responsible forthe infant’s signs (eg, transient tachy-pnea of the newborn) and there are nomaternal risk factors for sepsis in anotherwise well-appearing infant, thelumbar puncture can be deferred oreliminated. Empirical antimicrobialtherapy, typically intravenous ampicil-lin and gentamicin (unless localantibiotic-resistance patterns suggestthe need for another combination),then should be initiated promptly. Cho-rioamnionitis continues to be a signif-icant risk factor for early-onset GBSsepsis in infants born to GBS-colonizedwomen. All well-appearing newborn in-fants born to women who have a clini-cal diagnosis of chorioamnionitis fromtheir obstetric provider should un-
dergo a “limited evaluation,” which in-cludes a complete blood cell (CBC)count and differential and a blood cul-ture before initiation of empirical anti-microbial therapy. The sensitivity ofthe CBC count is improved if delayedfor 6 to 12 hours after birth. Empiricaltherapy should be discontinued assoon as the clinical course and labora-tory evaluation exclude sepsis.
The indications for maternal IAPremain unchanged and include 1 ofmore of the following: (1) GBSculture–positive within preceding 5weeks; (2) GBS status unknown with1 or more intrapartum risk factors in-cluding less than 37 weeks’ gestation,prolonged rupture of membranesfor �18 hours, or temperature of�100.4°F (38.0°C); (3) GBS bacteriuriaduring current pregnancy; and (4) his-tory of a previous infant with GBS dis-ease. When a cesarean delivery isperformed before onset of labor withintact amniotic membranes, the risk ofearly-onset GBS disease among infantsis extremely low22,23; therefore, IAP isnot recommended as a routine prac-tice for cesarean deliveries performedunder these circumstances, regard-less of the GBS colonization status ofthe woman or the gestational age ofthe infant.
In well-appearing newborn infantsborn to women without an indicationfor IAP, routine clinical care is indi-cated unless signs of sepsis develop.For well-appearing term newborn in-fants born to mothers with an indica-tion for IAP to prevent GBS diseaseand receipt of 4 or more hours ofpenicillin, ampicillin or cefazolin atthe appropriate doses before deliv-ery, routine care, and 48 hours of ob-servation continue to be recom-mended. However, if these infantsmeet other discharge criteria, in-cluding term birth and ready accessto medical care, discharge can occuras early as 24 hours after birth. In
this latter circumstance, follow-upcare by a care provider within 48 to72 hours is recommended.
In well-appearing term newborn in-fants whosemothers had an indicationfor GBS prophylaxis and rupture ofmembranes for�18 hours but who re-ceived inadequate IAP—either by du-ration before delivery or by inappro-priate agent or dose—observation inthe hospital for at least 48 hours is rec-ommended. These infants would in-clude infants born to women with a se-rious penicillin allergy who receivedeither clindamycin or vancomycin. Thisrevised recommendation is based onthe poor sensitivity of the “limited-evaluation” assessments in this cir-cumstance and also data indicatingthat signs of early-onset GBS sepsis ap-pear in more than 98% of neonateswithin this interval of hospitalization.The authors of several studies have re-ported the sensitivity of an abnormalCBC count in predicting GBS sepsis torange from 41% to 68%, whereas thepresence of clinical signs has a sensi-tivity of 92%.24–27 The yield of bloodculture can be low among newborninfants exposed to intrapartum antibi-otics.28 Finally, for all preterm neo-nates (�37 weeks of gestation) or forterm newborn infants born in the set-ting of rupture ofmembranes 18 hoursor more before delivery without ade-quate maternal IAP, a limited evalua-tion and observation for at least 48hours is recommended.
Recommendations forManagement of Newborn Infants
● All newborn infants with signs ofsepsis should undergo a full diag-nostic evaluation (including a lum-bar puncture) and receive empiri-cal antimicrobial therapy (AII).
● All well-appearing newborn infantsborn to women given a diagnosisof chorioamnionitis by their obstet-rical provider should undergo a
4 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Mc Master University on November 26, 2012pediatrics.aappublications.orgDownloaded from

limited diagnostic evaluation (nolumbar puncture) and receive em-pirical antimicrobial therapy (AII).
● For all women who received ade-quate IAP defined as penicillin (pre-ferred), ampicillin, or cefazolin(penicillin-allergic women at lowrisk of anaphylaxis) for 4 or morehours before delivery, their new-born infants require only routinecare and observation in the hospitalfor 48 hours (BIII). If these infantsmeet other discharge criteria, in-cluding term birth and ready accessto medical care, discharge can oc-cur as early as 24 hours after birthwith follow-up care by a care pro-vider within 48 to 72 hours (CII).
● Well-appearing term newborn in-fants whose mothers received no orinadequate IAP (including clindamy-cin or vancomycin) and had ruptureof membranes for less than 18hours require only observation for48 hours (BIII).
● Well-appearing term infants born towomen with no or inadequate IAPand rupture ofmembranes for 18 ormore hours before delivery shouldundergo a “limited evaluation” (ie,blood culture and CBC count withdifferential and platelets at birth)and observation for at least 48hours (BIII).
● All preterm infants born to womenwith no or inadequate IAP should un-dergo a limited evaluation and ob-servation for at least 48 hours (BIII).
LEAD AUTHORSCarol J. Baker, MDCarrie L. Byington, MDRichard A. Polin, MD
COMMITTEE ON INFECTIOUS DISEASES,2010–2011Michael T. Brady, MD, ChairpersonHenry H. Bernstein, DOCarrie L. Byington, MDKathryn M. Edwards, MDMargaret C. Fisher, MDMary P. Glode, MDMary Anne Jackson, MDHarry L. Keyserling, MDDavid W. Kimberlin, MDYvonne A. Maldonado, MDWalter A. Orenstein, MDGordon E. Schutze, MDRodney E. Willoughby, MD
LIAISONSBeth Bell, MD, MPH – Centers for DiseaseControl and PreventionRobert Bortolussi, MD – Canadian PaediatricSocietyMarc A. Fischer, MD – Centers for DiseaseControl and PreventionBruce Gellin, MD – National Vaccine ProgramOfficeRichard L. Gorman, MD – National Institutes ofHealthLucia Lee, MD – Food and Drug AdministrationR. Douglas Pratt, MD – Food and DrugAdministrationJennifer S. Read, MD – National Institutes ofHealthJeffrey R. Starke, MD – American ThoracicSociety
Jack Swanson, MD – Committee on PracticeAmbulatory MedicineTina Q. Tan, MD – Pediatric Infectious DiseasesSociety
EX OFFICIOCarol J. Baker, MD – Red Book Associate EditorSarah S. Long, MD – Red Book Associate EditorH. Cody Meissner, MD – Red Book AssociateEditorLarry K. Pickering, MD – Red Book Editor
CONSULTANTLorry G. Rubin, MD
STAFFJennifer Frantz, MPH
COMMITTEE ON FETUS AND NEWBORN,2010–2011Lu-Ann Papile, MD, ChairpersonJames Cummings, MDJill E. Baley, MDVinod K. Bhutani, MDWaldemar A. Carlo, MDPraveen Kumar, MDRichard A. Polin, MDRosemarie C. Tan, MD, PhDKasper S. Wang, MDKristi L. Watterberg, MD
LIAISONSCapt Wanda D. Barfield, MD, MPH – Centers forDisease Control and PreventionWilliam H. Barth Jr, MD – American College ofObstetricians and GynecologistsAnn L. Jefferies, MD – Canadian PaediatricSocietyRosalie O. Mainous, PhD, RNC, NNP – NationalAssociation of Neonatal NursesTonse N. K. Raju, MD, DCH – National Institutesof Health
STAFFJim Couto, MA
REFERENCES
1. Baker CJ. Early onset group B streptococcaldisease. J Pediatr. 1978;93(1):124–125
2. Baker CJ, Barrett FF, Gordon RC, Yow MD.Suppurative meningitis due to streptococciof Lancefield group B: a study of 33 infants.J Pediatr. 1973;82(4):724–729
3. Baker CJ, Barrett FF. Transmission of groupB streptococci among parturient womenand their neonates. J Pediatr. 1973;83(6):919–925
4. Boyer KM, Gotoff SP. Strategies for chemo-prophylaxis of GBS early-onset infections.Antibiot Chemother. 1985;35:267–280
5. Schrag S, Gorwitz R, Fultz-Butts K, SchuchatA. Prevention of perinatal group B strepto-coccal disease. Revised guidelines from
CDC. MMWR Recomm Rep. 2002;51(RR-11):1–22
6. Van Dyke MK, Phares CR, Lynfield R, et al.Evaluation of universal antenatal screeningfor group B Streptococcus. N Engl J Med.2009;360(25):2626–2636
7. Pulver LS, Hopfenbeck MM, Young PC, et al.Continued early onset group B streptococ-cal infections in the era of intrapartum pro-phylaxis. J Perinatol. 2009;29(1):20–25
8. Phares CR, Lynfield R, Farley MM, et al. Epi-demiology of invasive group B streptococ-cal disease in the United States, 1999–2005.JAMA. 2008;299(17):2056–2065
9. Centers for Disease Control and Prevention.Perinatal group B streptococcal disease af-
ter universal screening recommendations:United States, 2003–2005. MMWR MorbMortal Wkly Rep. 2007;56(28):701–705
10. Pinto NM, Soskolne EI, Pearlman MD, FaixRG. Neonatal early-onset group B strepto-coccal disease in the era of intrapartumchemoprophylaxis: residual problems. JPerinatol. 2003;23(4):265–271
11. Puopolo KM, Madoff LC, Eichenwald EC.Early-onset group B streptococcal diseasein the era of maternal screening. Pediat-rics. 2005;115(5):1240–1246
12. Garland SM, Fliegner JR. Group B Strepto-coccus (GBS) and neonatal infections: thecase for intrapartum chemoprophylaxis.Aust N Z J Obstet Gynaecol. 1991;31(2):119–122
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 3, September 2011 5 at Mc Master University on November 26, 2012pediatrics.aappublications.orgDownloaded from

13. Boyer KM, Gotoff SP. Prevention of early-onset neonatal group B streptococcal dis-ease with selective intrapartum chemopro-phylaxis. N Engl J Med. 1986;314(26):1665–1669
14. Fiore Mitchell T, PearlmanMD, Chapman RL,Bhatt-Mehta V, Faix RG. Maternal and trans-placental pharmacokinetics of cefazolin.Obstet Gynecol. 2001;98(6):1075–1079
15. Allegaert K, van Mieghem T, Verbesselt R, etal. Cefazolin pharmacokinetics in maternalplasma and amniotic fluid during preg-nancy. Am J Obstet Gynecol. 2009;200(2):170.e1–170.e7
16. Popovic J, Grujic Z, Sabo A. Influence of preg-nancy on ceftriaxone, cefazolin and genta-micin pharmacokinetics in caesarean vs.non-pregnant sectioned women. J ClinPharm Ther. 2007;32(6):595–602
17. Blaschke AJ, Pulver LS, Korgenski EK, SavitzLA, Daly JA, Byington CL. Clindamycin-resistant group B Streptococcus and failureof intrapartum prophylaxis to preventearly-onset disease. J Pediatr. 2010;156(3):501–503
18. Ansong AK, Smith PB, Benjamin DK, et al.
Group B streptococcal meningitis: cerebro-spinal fluid parameters in the era of intra-partum antibiotic prophylaxis. Early HumDev. 2009;85(10 suppl):S5–S7
19. Garges HP, Moody MA, Cotten CM, et al. Neo-natal meningitis: what is the correlationamong cerebrospinal fluid cultures, bloodcultures, and cerebrospinal fluid parame-ters? Pediatrics. 2006;117(4):1094–1100
20. Stoll BJ, Hansen N, Fanaroff AA, et al. To tapor not to tap: high likelihood of meningitiswithout sepsis among very low birth weightinfants. Pediatrics. 2004;113(5):1181–1186
21. Wiswell TE, Baumgart S, Gannon CM, SpitzerAR. No lumbar puncture in the evaluationfor early neonatal sepsis: will meningitis bemissed? Pediatrics. 1995;95(6):803–806
22. Ramus R, McIntire D, Wendall G. Antibioticchemoprophylaxis for group B strep is notnecessary with elective cesarean section atterm [abstract]. Am J Obstet Gynecol. 1999;180(suppl):S85
23. Håkansson S, Axemo P, Bremme K, et al;Swedish Working Group for the Preventionof Perinatal Group B Streptococcal Infec-tions. Group B streptococcal carriage in
Sweden: a national study on risk factors formother and infant colonisation. Acta ObstetGynecol Scand. 2008;87(1):50–58
24. Greenberg DN, Yoder BA. Changes in the dif-ferential white blood cell count in screeningfor group B streptococcal sepsis. PediatrInfect Dis J. 1990;9(12):886–889
25. Hsu KK, Pelton SI, Shapiro DS. Detection ofgroup B streptococcal bacteremia in simu-lated intrapartum antimicrobial prophy-laxis. Diagn Microbiol Infect Dis. 2003;45(1):23–27
26. Gerdes JS, Polin RA. Sepsis screen in neo-nates with evaluation of plasma fibronectin.Pediatr Infect Dis J. 1987;6(5):443–446
27. Ottolini MC, Lundgren K, Mirkinson LJ, Ca-son S, Ottolini MG. Utility of complete bloodcount and blood culture screening to diag-nose neonatal sepsis in the asymptomaticat risk newborn. Pediatr Infect Dis J. 2003;22(5):430–434
28. Escobar GJ, Li DK, Armstrong MA, et al. Neo-natal sepsis workups in infants �2000grams at birth: a population-based study.Pediatrics. 2000;106(2 pt 1):256–263
6 FROM THE AMERICAN ACADEMY OF PEDIATRICS at Mc Master University on November 26, 2012pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2011-1466; originally published online August 1, 2011;Pediatrics
NEWBORNCOMMITTEE ON INFECTIOUS DISEASES AND COMMITTEE ON FETUS AND
DiseaseRecommendations for the Prevention of Perinatal Group B Streptococcal (GBS)
ServicesUpdated Information &
/peds.2011-1466http://pediatrics.aappublications.org/content/early/2011/07/28including high resolution figures, can be found at:
Citations
/peds.2011-1466#related-urlshttp://pediatrics.aappublications.org/content/early/2011/07/28This article has been cited by 1 HighWire-hosted articles:
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Mc Master University on November 26, 2012pediatrics.aappublications.orgDownloaded from

Paediatr Child Health Vol 12 No 10 December 2007 893
Neonatal sepsis continues to cause a significant propor-tion of perinatal mortality and long-term morbidity in
the term and preterm infant population. The most commonsingle organism that causes early-onset neonatal sepsis is thegroup B streptococcus (GBS or Streptococcus agalactiae) (1).Invasive early-onset GBS disease has an incidence ofapproximately two per 1000 live-born infants in theabsence of intrapartum antibiotic prophylaxis (IAP) (2,3),with a case-fatality rate of between 2% and 13% in recentstudies (4-6). Therefore, preventive strategies have beenpromoted and recently endorsed by the Society ofObstetricians and Gynaecologists of Canada (7). It hasbeen demonstrated that the administration of intravenouspenicillin at least 4 h before delivery to mothers colonizedwith GBS is highly effective in preventing perinatal trans-mission and early-onset invasive infection in the newborn(8). The recommendations are to screen all mothers withrectovaginal cultures at 35 to 37 weeks, and treat those withpositive cultures for GBS at the time they present in labour.This strategy leads to as many as 22% of all mothers inlabour at term being treated with IAP to prevent disease in0.2% of infants and prevent mortality in 0.01% of infants(9). In the United Kingdom, it was calculated that it wouldrequire 24,000 antepartum cultures and 7000 women inlabour treated with antibiotics to prevent one neonataldeath (10). As a consequence, other authorities have devel-oped different recommendations, questioning whetherroutine IAP is an appropriate use of resources (10,11), andwhether the pressure exerted for the development of bacte-rial resistance is justified. In Canada, the current incidenceof invasive neonatal GBS disease is uncertain because thereis no centralized or mandatory reporting system.
PURPOSE OF THE STATEMENTThe aim of the present statement is to develop evidence-based practice guidelines answering the following question:How should an infant be monitored, investigated andtreated given the presence of clinical signs of sepsis, theGBS culture status of the mother (positive, negative orunknown), the treatment status of the mother (completed,incomplete or no IAP), and the presence or absence ofmaternal risk factors for neonatal sepsis?
METHODS OF STATEMENT DEVELOPMENTA search was carried out in MEDLINE and the Cochranelibrary, and last updated in January 2006. The MEDLINEsearch terms were ‘Streptococcus agalactiae’ and ‘newborn’.The hierarchy of evidence from the Centre for Evidence-Based Medicine (United Kingdom) was applied and, for thisstatement, the levels of evidence for treatment, prognosisand diagnosis were used (www.cebm.net, click on the EBMTools tab or www.cebm.net/levels_of_evidence.asp#levels).
DEFINITIONSLimited diagnostic evaluationLimited diagnostic evaluation consists of a complete bloodcount (CBC), and observation of vital signs every 4 h for aperiod of 24 h. The newborn can be cared for and observedin the mother’s postpartum room. If the CBC shows a lowtotal white blood cell (WBC) count of less than 5.0×109/L,then the risk of sepsis is substantially increased and a fulldiagnostic evaluation and initiation of therapy wouldusually be indicated.
Full diagnostic evaluationFull diagnostic evaluation consists of a CBC, blood cultureand lumbar puncture (LP); a chest x-ray should be obtainedif respiratory difficulties are present. LP can be deferred inunstable infants, and performed later to ascertain thepresence of hypoglycorrhachia or pleocytosis. Infants whoseonly sign of sepsis is respiratory distress may also beconsidered for deferment of LP if close follow-up can beensured.
THE UNWELL INFANTThe initial signs of sepsis may be subtle, and may includetemperature instability, tachycardia, poor peripheralperfusion and respiratory distress. Because the progression ofinvasive disease is very rapid, any infant with clinical signssuggestive of infection should be treated immediatelyfollowing a prompt full diagnostic evaluation; delaybetween presentation and therapy increases the risk of apoor outcome (12) (evidence level 2b). There is no cleardistinction in the clinical signs present when the infant hasGBS sepsis compared with any other invasive organism.
Management of the infant at increased riskfor sepsis
POSITION STATEMENT (FN 2007-03)
Français en page 899
Correspondence: Canadian Paediatric Society, 2305 St Laurent Boulevard, Ottawa, Ontario K1G 4J8. Telephone 613-526-9397, fax 613-526-3332, Web sites www.cps.ca, www.caringforkids.cps.ca
©2007 Canadian Paediatric Society. All rights reserved

Although IAP with a penicillin dramatically reduces thefrequency of early-onset invasive GBS disease, it does notaffect the frequency of sepsis caused by other organisms(1,13) (evidence level 2b). Of note, invasive GBS can stilloccur in infants of mothers who have had a negativescreening culture at 35 to 37 weeks; now that IAP iswidespread and effective, the majority of the remaininginfants with invasive GBS are those whose maternalcultures were negative (14), but who became colonizedbetween screening and delivery (evidence level 2b). Also,invasive GBS disease is still possible, even if very rare, inmothers who received adequate IAP (15) (evidence level 4).Thus, neither the maternal screening history norintrapartum exposure to antibiotics should affect theapproach to the management of the infant with clinicalsigns of sepsis (recommendation category B). Therefore,prospective therapy, while awaiting culture results, shouldcover the most common bacteria: GBS, other streptococci,Escherichia coli, other Gram-negative organisms and Listeriamonocytogenes.
An infant with signs of sepsis does not require confirma-tory tests other than obtaining cultures before commencingtherapy, because no other tests have an adequately high neg-ative predictive value to avoid therapy (evidence level 2a).In particular, a normal WBC count or differential should notprevent treatment in such an infant because the negativelikelihood ratio of a normal CBC is approximately 0.7(recommendation grade B) (16).
Empirical therapyThere are no good prospective studies to indicate optimalchoice of therapy in the newborn infant with possible sepsis(17), but ampicillin and gentamicin are usually appropriatebased on the usual susceptibilities of the predominantorganisms causing early-onset sepsis (evidence level 4).Infants with a positive cerebrospinal fluid (CSF) evaluationor with clinical signs of meningitis if the LP has beendeferred, should be treated with antibiotics which bothpenetrate the CSF and are active against the likely organ-isms (Table 1). If there is information from the maternal
history suggesting an organism that is unlikely to respond tothese antibiotics, empirical therapy should be adjustedappropriately. Blood cultures using modern automated sys-tems are almost always positive by 48 h (18). Therefore, ifthe laboratory results and clinical course do not indicatebacterial infection, therapy may be discontinued after 48 h.The majority of antibiotic courses are given to infants whoeventually prove not to have had sepsis; strategies forfurther reduction of the duration of antibiotic therapy insuch infants should be considered. For example, becausegentamicin is usually now given once per day in the full-term infant, and ampicillin is given every 12 h, the initialantibiotic order could be to give ampicillin for four dosesevery 12 h and gentamicin for two doses every 24 h,followed by reassessment after verification of culture resultsat 48 h, and reordering the antibiotics in case of positivecultures (or ongoing signs of sepsis).
WELL-APPEARING INFANT OF A GBS-POSITIVEMOTHER, WHO RECEIVED IAP MORE THAN
4 H BEFORE DELIVERYIAP with a penicillin for least 4 h is highly effective ateradicating GBS transmission (19), and thus preventingthe majority of invasive neonatal GBS disease (evidencelevel 1b) (20). Therefore, if a GBS-positive woman receivesintrapartum antibiotics for at least 4 h before delivery and ifthe newborn appears healthy and is more than 35 weeksgestational age, the newborn requires no therapy forprevention of early-onset GBS (recommendation grade A).
If the baby remains well at 24 h of age and is otherwiseeligible for discharge at this time, early discharge can becontemplated provided the caregiver knows the appropriateresources in the community for accessing health care and isable to transport the baby immediately to a health carefacility if clinical signs of sepsis develop.
There is insufficient information regarding the efficacyof alternative antibiotics (used when the mother is at risk ofanaphylaxis from penicillin). Such infants should bemanaged as if the mother received incomplete IAP (nextheading) until further data are available.
Paediatr Child Health Vol 12 No 10 December 2007894
CPS Statement: FN 2007-03
Table 1Empirical therapy for infants with positive cerebrospinal fluid (CSF) evaluation
Suggested expectant antimicrobialsCSF findings Most common organisms for early-onset meningitis
Gram-positive cocci Group B streptococci, less commonly: Ampicillin or penicillin plus gentamicinStaphylococcus species or enterococci
Gram-positive rods Listeria monocytogenes Ampicillin plus gentamicin
Gram-negative rods Escherichia coli, less commonly: Klebsiella, Cefotaxime plus gentamicinPseudomonas and Citrobacter
Gram-negative cocci Uncommon Cefotaxime
Pleocytosis, or other findings strongly Any of the above are possible Ampicillin plus gentamicinsuggestive of meningitis, but Gram stain-negative, or too unstable to have an LP
LP Lumbar puncture. Source: Canadian Paediatric Society, 2007

WELL-APPEARING INFANT OF A GBS-POSITIVEMOTHER WHO RECEIVED IAP LESS THAN 4 H
BEFORE DELIVERY OR NOT AT ALL The risk of invasive early-onset GBS disease in an infantwhose mother is GBS-positive and does not receive IAP isapproximately 1% (21). Only one-quarter of these babiesare asymptomatic at birth. This risk of significant diseaseprobably does not justify routine empirical treatment inthese circumstances, and careful observation with treat-ment at the first clinical sign of infection appears to be rea-sonable. Ninety-five per cent of infants with early-onsetGBS infection present with clinical signs within 24 h (22)(either temperature instability, tachycardia, poor peripheralperfusion, respiratory distress or abnormal CBC). Four percent of infected infants present between 24 h and 48 h ofage, with only 1% developing signs after 48 h of age. Thus,prolonging hospitalization from 24 h to 48 h would requirethe observation of more than 2000 infants to detect eachcase of invasive infection. Therefore, if careful assessmentof the infant at 24 h confirms that they remain well, dis-charge at that time may well be appropriate as long as ade-quate patient education and follow-up are ensured.
The use of the CBC is sometimes promoted for determin-ing risk, both for GBS and for other organisms, amonginfants who are at elevated risk but appear well. However,the positive predictive value of an abnormal CBC is low inthe newborn and it is, therefore, uncertain how to proceedwhen an infant is clinically well but has an abnormal CBC;unfortunately, most studies investigating the usefulness of theCBC have not been confined to well-appearing infants and,therefore, their usefulness in this specific situation is some-what conjectural. One study (23) confined to well-appearingterm infants showed a positive predictive value of 1.5% of an‘abnormal’ CBC (total WBC of 5.0×109/L or lower, or30×109/L or greater, or an absolute polymorphonuclear cellcount of less than 1.5×109/L or an immature to mature poly-morphonuclear cell ratio greater than 0.2) in identifying thedevelopment of ‘clinical sepsis’ in 1665 healthy term infantswho were at risk; of note, none of these infants developed apositive blood culture (evidence level 2b).
Several scoring systems have been developed foranalyzing CBC results (24), and all involve analysis of thecount of immature neutrophils, but there is very wide inter-observer variability in the identification of immature or‘band’ neutrophils (25). Even the best scoring system onlyachieves a likelihood ratio of between four and eight (24)(evidence level 2a). Finding a ‘left-shift’ or an elevatedtotal WBC count is not sufficiently predictive to alter man-agement. The individual finding on a CBC with the highestpositive predictive value is a low total WBC count of lessthan 5.0×109/L; if this finding is present, the likelihoodratio is between 10 and 20 (16), leading to a post-test prob-ability of sepsis of approximately 10% to 20% (evidencelevel 2b) and, therefore, probably justifying treatment evenin a well-appearing infant after a full diagnostic workup.However, only between 22% and 44% of infants with sepsiswill have such a low total WBC count (16).
WELL-APPEARING INFANT OF A GBS-NEGATIVE MOTHER WHO HAD RISK
FACTORS AT DELIVERY Before the recommendation for universal culture-basedscreening, IAP was recommended for mothers with any oneof the following five risk factors: over 18 h rupture ofmembranes, pyrexia higher than 38°C, premature labour atless than 36 weeks, GBS bacteriuria at anytime duringpregnancy or previous child with invasive GBS disease.These risk factors were present in as many as 22% ofmothers, and only identified approximately 50% of infantswho eventually developed invasive GBS disease (26,27)(evidence level 2b).
Although invasive GBS disease does occur in infantswhose mothers have negative screening cultures at 35 to37 weeks, the risk is very low even in those with prolongedrupture of membranes or intrapartum pyrexia (28)(evidence level 2b). It is suggested that a limited diagnos-tic evaluation be performed in this newborn population(recommendation grade B).
WELL-APPEARING INFANT OF A MOTHER WITHUNKNOWN GBS STATUS AND NO RISK FACTORS A mother who has not had an antenatal GBS culture orwhose results are not readily available, and her newbornbaby, should be managed according to the risk factors listedin the previous section. In the absence of these risk factors,and if the baby remains well, no specific intervention isrequired (recommendation grade B).
WELL-APPEARING INFANT OF A MOTHERWITH UNKNOWN GBS STATUS
WITH RISK FACTORSThe five risk factors mentioned above occur in approxi-mately 20% of deliveries at term, and are present in approx-imately 50% of infants with invasive GBS disease (26,27).This fourfold increase in risk to the infant in a mother withunknown GBS status has led to the recommendation thatshe should receive IAP (7). In this circumstance, the infantshould be treated in the same way as he or she would betreated if the mother were GBS-positive (ie, IAP more than4 h before delivery and routine neonatal care; IAP less than4 h or no IAP, limited diagnostic evaluation and minimum24 h observation) (recommendation grade B).
THE LATE PRETERM INFANTThe mother who delivers at less than 37 weeks will oftennot have results of antenatal GBS screening available. Insuch a case, the infant has a ‘risk factor’ (prematurity) forinvasive GBS disease and, if he or she appear well, shouldhave a limited diagnostic evaluation. Infants of thisgestational age should not be discharged before 48 h at theearliest (Figure 1).
CHORIOAMNIONITIS Chorioamnionitis is a difficult condition to diagnosebecause the prevalence of pyrexia during labour is high
Paediatr Child Health Vol 12 No 10 December 2007 895
CPS Statement: FN 2007-03
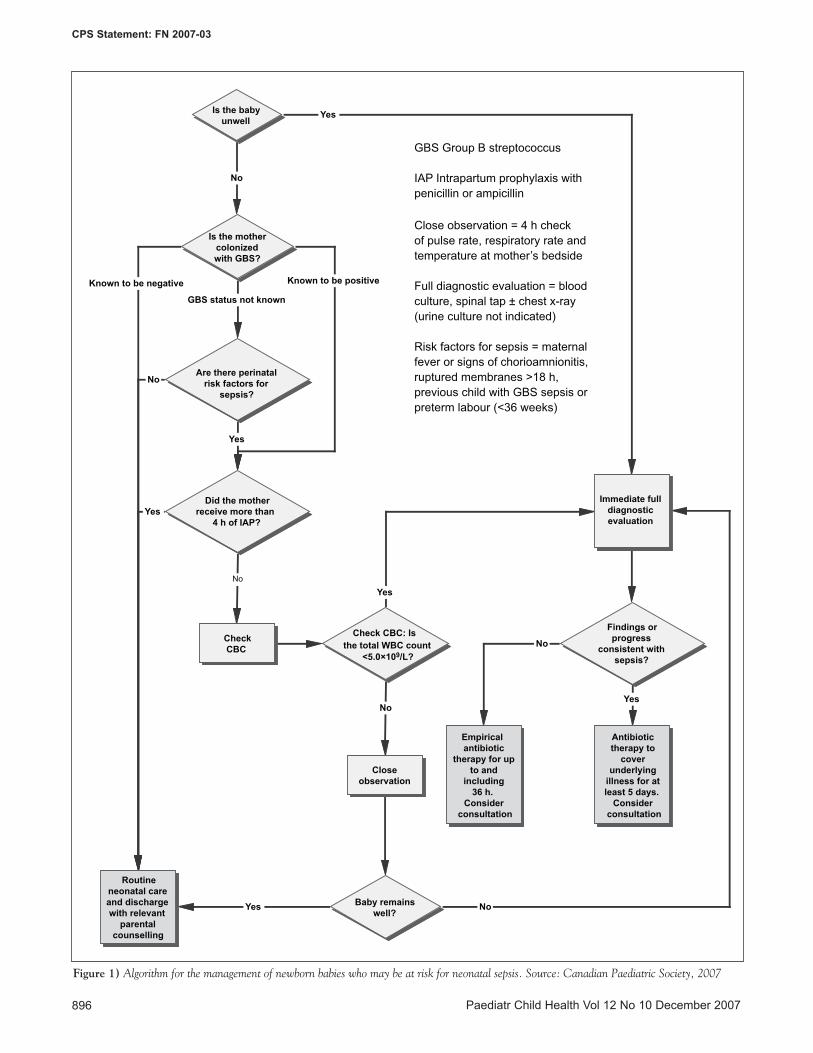
Paediatr Child Health Vol 12 No 10 December 2007896
CPS Statement: FN 2007-03
No
Yes
Yes
Yes
No
No
Yes
Known to be negative
Yes No
Known to be positive
GBS status not known
No
Yes
No
Routine neonatal care and discharge with relevant
parental counselling
Closeobservation
Empirical antibiotic
therapy for up to and
including 36 h.
Consider consultation
Antibiotic therapy to
cover underlying
illness for at least 5 days.
Consider consultation
Are there perinatal risk factors for
sepsis?
Is the mother colonized with GBS?
Is the baby unwell
Did the mother receive more than
4 h of IAP?
Check CBC: Is the total WBC count
<5.0×109/L?
Immediate full diagnostic evaluation
Findings or progress
consistent with sepsis?
Baby remains well?
GBS Group B streptococcus
IAP Intrapartum prophylaxis with penicillin or ampicillin
Close observation = 4 h check of pulse rate, respiratory rate and temperature at mother’s bedside
Full diagnostic evaluation = blood culture, spinal tap ± chest x-ray (urine culture not indicated)
Risk factors for sepsis = maternal fever or signs of chorioamnionitis, ruptured membranes >18 h, previous child with GBS sepsis or preterm labour (<36 weeks)
CheckCBC
Figure 1) Algorithm for the management of newborn babies who may be at risk for neonatal sepsis. Source: Canadian Paediatric Society, 2007

(29), especially if the mother has had epidural analgesia (30).Other signs of chorioamnionitis are less frequent; there ispoor correlation between clinical signs of chorioamnionitisand histology (29). Therefore, chorioamnionitis is frequentlyclassified as ‘possible’, when the main sign is fever, and‘definite’, when the classical triad of fever, left-shift in theWBC and lower uterine tenderness is present.
The risk of sepsis (which may be due to a variety ofdifferent organisms, including GBS, E coli and other Gram-negative organisms) in an infant whose mother had definitechorioamnionitis is approximately 8%, and is approximately3% to 4% if ‘possible’ and ‘definite’ chorioamnionitis areconsidered together (31,32) (evidence level 2b); among allmothers with fever, the incidence is 2% to 6% dependingon the height of the fever (31) (evidence level 2b). Infantswho do not have signs at birth are unlikely to developsepsis, the odds ratio for sepsis among infants who are wellat birth is 0.26 (95% CI 0.11 to 0.63) (31). The incidenceof invasive infection in the present study in an initiallywell-appearing infant with a maternal history of fever orchorioamnionitis was less than 2%, and this is confirmed byother data (33) (evidence level 2b). Therefore, it seemsreasonable to perform a CBC and closely observe such aninfant, and to only perform a full diagnostic evaluation andtreat with antibiotics if the CBC is strongly suggestive ofinfection (low total WBC count) or if clinical signsdevelop. A requirement for extensive resuscitation at birthshould be considered a sign of possible infection in suchinfants (32,33).
RECOMMENDATIONS• Any newborn infant with clinical signs suggestive of
sepsis should have an immediate full diagnosticevaluation followed by the institution of empiricalantibiotic therapy without delay (recommendationcategory B).
• If a mother who is GBS-positive receives IAP with apenicillin more than 4 h before delivery, no furtherevaluation or observation for invasive GBS disease in awell-appearing infant is required (recommendationcategory A).
• If a GBS-positive woman receives IAP less than 4 hbefore delivery (or receives no antibiotics or anonpenicillin regimen), then a limited diagnosticevaluation is required, and the infant should not bedischarged before 24 h of age. At the time of discharge,the infant should be evaluated and the parents shouldbe educated regarding signs of sepsis in the newborn.Discharge at 24 h to 48 h is conditional on theparents’ ability to immediately transport the baby to ahealth care facility if clinical signs of sepsis develop(recommendation grade B).
• If the CBC reveals a total WBC count less than5.0×109/L, full diagnostic evaluation and empiricalantibiotic therapy should be considered(recommendation grade B).
• If a GBS-negative woman with risk factors delivers ababy who remains well, the infant does not requireevaluation for GBS (recommendation grade B).
• If a woman with unknown GBS status and with riskfactors at the time of delivery receives IAP more than4 h before delivery, the infant requires no specificintervention (recommendation grade B).
• If a woman with unknown GBS status and with riskfactors at the time of delivery receives IAP less than4 h before delivery, limited diagnostic evaluation isrequired and the infant is not discharged before 24 h oflife (recommendation grade B).
• The well-appearing infant born at less than 36 weeksgestation with an unknown maternal GBS statusshould have a limited diagnostic evaluation and is nota candidate for early discharge.
• The well-appearing infant of a mother with possiblechorioamnionitis requires a limited diagnosticevaluation for sepsis (recommendation grade B).
ACKNOWLEDGEMENTS: The present position statement wasreviewed by the Canadian Paediatric Society CommunityPaediatrics Committee and the Infectious Diseases andImmunization Committee.
Paediatr Child Health Vol 12 No 10 December 2007 897
CPS Statement: FN 2007-03
REFERENCES1. Baltimore RS, Huie SM, Meek JI, Schuchat A, O’Brien KL.
Early-onset neonatal sepsis in the era of group B streptococcalprevention. Pediatrics 2001;108:1094-8.
2. Zangwill KM, Schuchat A, Wenger JD. Group B streptococcaldisease in the United States, 1990: Report from a multistate activesurveillance system. MMWR 1992;41:25-32.
3. Davies H, LeBlanc J, Bortolussi R, McGeer A; PICNIC. ThePediatric Investigators Collaborative Network on Infections inCanada (PICNIC) study of neonatal group B streptococcalinfections in Canada. Paediatr Child Health 1999;4:257-63.
4. Dahl MS, Tessin I, Trollfors B. Invasive group B streptococcalinfections in Sweden: Incidence, predisposing factors and prognosis.Int J Infect Dis 2003;7:113-9.
5. Kalliola S, Vuopio-Varkila J, Takala AK, Eskola J. Neonatal group B streptococcal disease in Finland: A ten-year nationwidestudy. Pediatr Infect Dis J 1999;18:806-10.
6. Grimwood K, Darlow BA, Gosling IA, et al. Early-onset neonatalgroup B streptococcal infections in New Zealand 1998-1999. J Paediatr Child Health 2002;38:272-7.
7. Money DM, Dobson S; Society of Obstetricians and Gynaecologistsof Canada. The prevention of early-onset neonatal group Bstreptococcal disease. J Obstet Gynaecol Can 2004;26:826-40.
8. Hafner E, Sterniste W, Rosen A, et al. Group B streptococci duringpregnancy: A comparison of two screening and treatment protocols.Am J Obstet Gynecol 1998;179:677-81.
9. Embleton N, Wariyar U, Hey E. Mortality from early onset group Bstreptococcal infection in the United Kingdom. Arch Dis ChildFetal Neonatal Ed 1999;80:F139-41.
10. Royal College of Obstetricians and Gynaecologists. Prevention ofearly onset neonatal group B streptococcal disease (36) – November2003. <http://www.rcog.org.uk/index.asp?PageID=520> (Version current at November 2, 2007).

Paediatr Child Health Vol 12 No 10 December 2007898
CPS Statement: FN 2007-03
11. Canadian Task Force on Preventive Health Care. Prevention ofgroup B streptococcal infection in newborns: Recommendationstatement from the Canadian Task Force on Preventive HealthCare. CMAJ 2002;166:928-30.
12. Lannering B, Larsson LE, Rojas J, Stahlman MT. Early onset group B streptococcal disease. Seven year experience and clinicalscoring system. Acta Paediatr Scand 1983;72:597-602.
13. Daley AJ, Isaacs D; Australasian Study Group for NeonatalInfections. Ten-year study on the effect of intrapartum antibioticprophylaxis on early onset group B streptococcal and Escherichia colineonatal sepsis in Australasia. Pediatr Infect Dis J 2004;23:630-4.
14. Puopolo KM, Madoff LC, Eichenwald EC. Early-onset group Bstreptococcal disease in the era of maternal screening. Pediatrics2005;115:1240-6.
15. Pinto NM, Soskolne EI, Pearlman MD, Faix RG. Neonatal early-onset group B streptococcal disease in the era of intrapartumchemoprophylaxis: Residual problems. J Perinatol 2003;23:265-71.
16. Fowlie PW, Schmidt B. Diagnostic tests for bacterial infection frombirth to 90 days: A systematic review. Arch Dis Child FetalNeonatal Ed 1998;78:F92-8.
17. Mtitimila EI, Cooke RW. Antibiotic regimens for suspected earlyneonatal sepsis. Cochrane Database Syst Rev 2004;(4)CD004495.
18. Kurlat I, Stoll BJ, McGowan JE Jr. Time to positivity for detectionof bacteremia in neonates. J Clin Microbiol 1989;27:1068-71.
19. Boyer KM, Gadzala CA, Kelly PD, Gotoff SP. Selectiveintrapartum chemoprophylaxis of neonatal group B streptococcalearly-onset disease. III. Interruption of mother-to-infanttransmission. J Infect Dis 1983;148:810-6.
20. Boyer KM, Gotoff SP. Prevention of early-onset neonatal group Bstreptococcal disease with selective intrapartum chemoprophylaxis.N Engl J Med 1986;314:1665-9.
21. Schrag S, Gorwitz R, Fultz-Butts K, Schuchat A. Prevention ofperinatal group B streptococcal disease. Revised guidelines fromCDC. MMWR Recomm Rep 2002;51(RR-11):1-22.
22. Bromberger P, Lawrence JM, Braun D, Saunders B, Contreras R,Petitti DB. The influence of intrapartum antibiotics on the clinical
spectrum of early-onset group B streptococcal infection in terminfants. Pediatrics 2000;106:244-50.
23. Ottolini MC, Lundgren K, Mirkinson LJ, Cason S, Ottolini MG.Utility of complete blood count and blood culture screening todiagnose neonatal sepsis in the asymptomatic at risk newborn.Pediatr Infect Dis J 2003;22:430-4.
24. Rodwell RL, Leslie AL, Tudehope DI. Early diagnosis of neonatalsepsis using a hematologic scoring system. J Pediatr 1988;112:761-7.
25. Schelonka RL, Yoder BA, Hall RB, et al. Differentiation ofsegmented and band neutrophils during the early newborn period. J Pediatr 1995;127:298-300.
26. Schrag SJ, Zell ER, Lynfield R, et al; Active Bacterial CoreSurveillance Team. A population-based comparison of strategies toprevent early-onset group B streptococcal disease in neonates. N Engl J Med 2002;347:233-9.
27. Towers CV, Suriano K, Asrat T. The capture rate of at-risk termnewborns for early-onset group B streptococcal sepsis determinedby a risk factor approach. Am J Obstet Gynecol 1999;181(5 Pt 1):1243-9.
28. Benitz WE, Gould JB, Druzin ML. Antimicrobial prevention ofearly-onset group B streptococcal sepsis: Estimates of risk reductionbased on a critical literature review. Pediatrics 1999;103:e78.
29. Smulian JC, Bhandari V, Vintzileos AM, et al. Intrapartum fever atterm: Serum and histologic markers of inflammation. Am J ObstetGynecol 2003;188:269-74.
30. Lieberman E, Lang JM, Frigoletto F Jr, Richardson DK, Ringer SA,Cohen A. Epidural analgesia, intrapartum fever, and neonatal sepsisevaluation. Pediatrics 1997;99:415-9.
31. Escobar GJ, Li DK, Armstrong MA, et al. Neonatal sepsis workupsin infants >/=2000 grams at birth: A population-based study.Pediatrics 2000;106:256-63.
32. Alexander JM, McIntire DM, Leveno KJ. Chorioamnionitis andthe prognosis for term infants. Obstet Gynecol 1999;94:274-8.
33. Jackson GL, Engle WD, Sendelbach DM, et al. Are complete bloodcell counts useful in the evaluation of asymptomatic neonatesexposed to suspected chorioamnionitis? Pediatrics 2004;113:1173-80.
FETUS AND NEWBORN COMMITTEEMembers: Drs Khalid Aziz, Royal Alexandra Hospital, Edmonton, Alberta (board representative 2000-2006); Keith James Barrington, Royal VictoriaHospital, Montreal, Quebec (chair); Joanne E Embree, University of Manitoba, Winnipeg, Manitoba (board representative); Haresh M Kirpalani,McMaster Children’s Hospital, Hamilton, Ontario; Shoo Lee, Capital Health, Edmonton, Alberta (2000-2006); Koravangattu Sankaran, RoyalUniversity Hospital, Saskatoon, Saskatchewan; Hilary EA Whyte, The Hospital for Sick Children, Toronto, Ontario; Robin K Whyte, IWK HealthCentre, Halifax, Nova ScotiaLiaisons: Drs Dan Farine, Mount Sinai Hospital, Toronto, Ontario (Society of Obstetricians and Gynaecologists of Canada); David Keegan, London,Ontario (College of Family Physicians of Canada); Catherine McCourt, Public Agency of Canada, Ottawa, Ontario (Health Canada); Alfonso JSolimano, BC’s Children’s Hospital, Vancouver, British Columbia (Canadian Paediatric Society, Neonatal-Perinatal Medicine Section); Ann Stark,Texas Children’s Hospital, Houston, Texas, USA (American Academy of Pediatrics, Committee on Fetus and Newborn); Ms Shahirose Premji,University of Calgary, Calgary, Alberta (Canadian Association of Neonatal Nurses); Ms Amanda Symington, McMaster Children’s Hospital,Hamilton, Ontario (Canadian Association of Neonatal Nurses, 1999-2006)Principal Author: Dr Keith James Barrington, Royal Victoria Hospital, Montreal, Quebec
The recommendations in this statement do not indicate an exclusive course of treatment or procedure to be followed. Variations, takinginto account individual circumstances, may be appropriate. Internet addresses are current at time of publication





























