-
CentralBringing Excellence in Open Access
JSM Ophthalmology
Cite this article: Morales-Fernandez L, Martinez-de-la-Casa JM,
Borrego L, Sanchez-Jean R, Arriola-Villalobos P, et al. (2015)
Glaucoma and Corneal De-compensation Following Cosmetic Iris
Prosthesis Implantation: A Case Report. JSM Ophthalmol 3(2):
1031.
*Corresponding authorLaura Morales-Fernandez, Department of
Ophthalmology, Hospital Clinico San Carlos, Health Research
Institute of the Hospital Clinico San Carlos (IdISSC), Profesor
Martin Lago SN, Madrid, Spain, Tele: 666-31-44-03; Email:
Submitted: 24 June 2015
Accepted: 13 July 2015
Published: 15 July 2015
ISSN: 2333-6447
Copyright© 2015 Morales-Fernandez et al.
OPEN ACCESS
Case Report
Glaucoma and Corneal Decompensation Following Cosmetic Iris
Prosthesis Implantation: A Case ReportLaura Morales-Fernandez1*,
Jose M. Martinez-de-la-Casa2-4, Lara Borrego1, Rubén Sanchez-Jean4,
Pedro Arriola-Villalobos1, Federico Saenz-Frances1, Enrique
Santos2, Sofía García-Saenz1 and Julian Garcia-Feijoo2-41Department
of Ophthalmology, Hospital Clinico San Carlos, Health Research
Institute of the Hospital Clinico San Carlos (IdISSC),
Spain2Department of Ophthalmology, Hospital Clinico San Carlos,
Health Research Institute of the Hospital Clinico San Carlos
(IdISSC), Spain3Department of Ophthalmology, Cooperative Research
Network on Age- Related Eye Pathology, Visual and Life Quality,
Health Institute Carlos III, Spain4Department of Optometry, Health
Research Institute Hospital Clinico San Carlos (IdISSC), Spain
INTRODUCTIONIris implants are intraocular prostheses that mimic
the
morphology and functions of the healthy iris [1,2]. Such
implants have been successfully used to resolve iris diseases and
with improving surgical techniques, their use for cosmetic purposes
has also started to gain popularity. The cosmetic implants
NewColorIris marketed by Kahn Medical Devices (Panama City, Panama)
were introduced as a safe alternative to colored contact
lenses for purely cosmetic use in healthy individuals (with no
history of eye disease). There are three color-options available
(hazel, green or blue).
These non–US Food and Drug Administration–approved cosmetic
implants have nevertheless been associated with several serious
complications: corneal edema, increased intraocular pressure (IOP),
pigment dispersion, uveitis, a reduced endothelial cell count,
uveitis–glaucoma–hyphema syndrome, glaucomatous
Keywords•Iris implant•NewColorIris•Glaucoma•Corneal
descompensation
Abstract
Purpose: This case report illustrates the difficult management
of complications produced following the bilateral iris implant of
the NewColorIris (NewColorIris, Kahn, and Medical Devices.
Methods: We report the case of a 36-year-old man who was
referred to our outpatient clinic because of bilateral glaucoma
showing a poor response to medical treatment and anti-glaucoma
surgery. The young man had received an iris implant (NewColorIris,
Kahn, Medical Devices) in both eyes for cosmetic purposes 5 years
earlier. Surprisingly, his clinical records revealed a strictly
normal ophthalmologic examination (visual acuity (VA) was 20/20 in
both eyes) following NewColorIris explantation. Subsequent to this
the patient required new artificial iris implantation, 2
anti-glaucoma surgeries (trabeculectomy+Ex-press®shunt placement)
and cataract surgery in both eyes, and DSAEK in the left eye. On
presentation, his VA was 20/200 in both eyes, endothelial cell
count was less than 1000 and he showed diffuse corneal edema, iris
retraction, anterior synechiae, iris implant in the sulcus,
multifocal IOL and an intraocular pressure of 40 mmHg in both
eyes.
Results: Poor pressure control was resolved through Ahmed valve
placement in both eyes though his vision remains poor.
Conclusions: This clinical case highlights the serious, poorly
manageable, irreversible complications produced by the NewColorIris
implant.
-
CentralBringing Excellence in Open Access
Morales-Fernandez et al. (2015)Email:
JSM Ophthalmol 3(2): 1031 (2015) 2/3
To control the severe IOP fluctuations refractory to
pharmacological treatment, an Ahmed valve was implanted in the
temporal zone behind the iris remnant, in front of the iris
prosthesis in both eyes (Figure 2).
Three months after presentation, the patient has an IOP of 10-12
mmHg in both eyes and BCVA is 20/400 in the RE and counting fingers
at 2 m in the LE. At the time of writing, corneal turbidity
detected in the LE suggests further surgery will be required to
improve visual acuity (Figure 3).
DISCUSSIONThe NewColorIris implant is a silicone, ring-shaped,
one-
piece diaphragm with 6 semicircular peripheral footplates, or
flaps. It is available in one size only, measuring 15.00 mm in
diameter, with a central pupil hole of diameter 3.50 mm and
thickness of 0.16 mm. However, despite the standard design,
individual variation seems common. According to Hoguet et al., [6],
“the implants were not identical and some, but not all, have
peripheral iridectomy cutouts of various sizes”. Also, Anderson
et
optic neuropathy, cystoid macular edema, trabecular meshwork
damage, and suprachoroidal hemorrhage. Since their initial use in
2004, these complications have been widely described in the
literature [2-6].
Many complications following NewColorIris implantation are
difficult to manage in the long term and may give rise to permanent
sequelae. Besides implant removal, the control of these
complications requires multiple surgical procedures and the visual
prognosis is uncertain.
We here report a clinical case that clearly shows the difficult
management of complications produced following the bilateral
implant of the NewColorIris. Besides explantation, the patient here
described required a series of complex surgical procedures to
stabilize clinical symptoms and avoid progressive vision loss.
CASE REPORTA 36-year-old man who had undergone NewColorIris
(Kahn,
Medical Devices) implantation in both eyes 5 years earlier (in
Panama) was referred to our outpatient clinic because of
progressive vision loss.
The patient had been treated one year after the iris
implantation surgery by a cornea and glaucoma specialist, who
removed the implants from both eyes without additional
complications. The reason for explantation was the observation of
anterior chamber inflammation, anterior synechiae, cataract and an
endothelial cell count under 1000 in both eyes. Following
explantation, intense iris retraction leaving scare remains of the
iris and 360 ºC of anterior synechiae were detected.
Subsequent to implant removal, the patient underwent cataract
extraction with multifocal intraocular lens (IOL) placement in both
eyes. Upon request of the patient and due to intense photophobia,
an artificial iris HMK ANI 2 (Ophtec/Polytech) was implanted in the
sulcus in both eyes. Due to poor IOP control using eye drops, the
patient underwent implantation of an Ex-press® shunt under a
scleral flap on two occasions per eye (first in the temporal
superior zone and then in the nasal superior zone). Finally, due to
corneal decompensation, the left eye was subjected to Descemet’s
stripping automated endothelial keratoplasty (DSAEK).
On examination at presentation, the patient was under treatment
with brimonidine and timolol eye drops twice a day in both eyes and
oral acetazolamide 250 mg three times per day. Best-corrected
visual acuity (BCVA) was 20/200 in both eyes. Slit lamp examination
revealed iris retraction and anterior synechiae along with an HMK
ANI 2 implant in both eyes. In each eye, the multifocal IOL could
be seen along with two Ex-press® filtration devices in the temporal
superior and nasal superior quadrants. The DSAEK endothelial graft
was observed in the left eye (LE) (Figure 1). A low endothelial
cell count was obtained in the RE (850 cells/mm2). Fundoscopy
examination revealed a cup-to-disc ratio of 0.4-0.5 in both eyes
and no macular or retinal abnormalities. In both eyes, IOP was 40
mmHg and the patient reported IOP fluctuations from 5 to 45 mmHg.
Visual field testing revealed a mildly reduced visual field and
retinal nerve fiber layer thinning in the superior and inferior
zones was detected in both eyes by optical coherence tomography
(OCT).
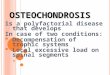
Figure 1 Anterior segment OCT image of the RE of the patient on
presentation. Note the closed angle, iris with synechiae occluding
the camerular angle, and a minimal remnant of iris remaining after
iris retraction.
Figure 2 Photograph of the RE taken 3 months after glaucoma
surgery. The photograph shows the well-positioned Ahmed valve tube
behind the remaining iris. The new iris implant and both Ex-press
shunts (nasal and temporal-superior) can also be seen.
Figure 3 Slit lamp photographs taken in the early postoperative
course of the LE following Ahmed valve implant. Note the
temporal-superior position of the device tube and the position of
the DSAEK lenticule with corneal transparency loss.
-
CentralBringing Excellence in Open Access
Morales-Fernandez et al. (2015)Email:
JSM Ophthalmol 3(2): 1031 (2015) 3/3
al., [3], reported irregular sharp edges observed by microscopy
and also stated that not all implants had 6 footplates.
The implant is designed for anterior chamber placement in phakic
eyes. Based on the long-standing use of phakic intraocular lenses,
it is well known that any anterior segment implant needs to be
suitably fitted to the size of the chamber to avoid the high
morbidity and vision loss produced by inadequate fitting [3-7].
There are numerous reasons for the serious complications arising
from NewColorIris implantation. Initial symptoms, most often
reddening and blurred vision, may appear within 6 months of surgery
though usually they appear within the first 2 years [3-6]. Once
initial signs arise, management usually involves implant removal.
Although explantation is not usually difficult, some complications
have been described such as crystalline lens opacification, cystic
macular edema and even suprachoroidal hemorrhage [6].
The use of cosmetic iris implants has also been linked to
significant endothelial cell loss [7]. Cell loss commences as soon
as the implant is inserted and unfolded in the anterior chamber
[3]. Some authors have described the instability and movement of
the prosthesis in the anterior chamber and decentration with
respect to the pupil can occur [3,6].
Although endothelial cell loss occurs in practically all cases,
only a few implants following their removal will give rise to
corneal decompensation resulting in a low visual acuity that may
require a corneal transplant, preferably DSAEK or a penetrating
keratoplasty [6].
The onset of ocular hypertension or glaucoma is also a frequent
complication. Among the many factors possibly leading to an
increase in IOP [1], instead of haptics, the NewColorIris has 6
footplates that rest on the corneal-scleral angle damaging the
trabecular meshwork, Schlemm canal and collector channels.
Several authors have described by means of anterior chamber OCT
and ultrasound biomicroscopy [3,7] the direct contact of the
implant with the iris which, added to its movement, promotes
pigment dispersion. In effect, this could be the initial IOP
elevation mechanism. Further, the irregular implant surface will
enhance pigment dispersion [3,7]. Inflammation, pigment
accumulation, hyphema and corticoid use are the main factors that
lead to this type of open-angle glaucoma [5]. However, although
less frequent, cases of angle closure have been related to anterior
synechiae sometimes affecting 360 degrees. This irreversible
situation even arising after explantation may rarely be accompanied
by iris retraction, as observed in our patient. A much more
frequent complication is cataract requiring surgery [3,6].
Our clinical case illustrates the series of complicated
surgeries needed because of the implant of this prosthesis in a
young, healthy, phakic individual. Despite explantation, surgical
treatment was needed for corneal decompensation, cataract,
complete iris retraction and glaucoma showing poor pressure
control.
In this clinical case, owing to the intense photophobia produced
by severe iris retraction and according to the patient’s wishes
after NewColorIris explantation, we decided to pursue the sulcus
implant of a HMK ANI 2 artificial iris. This is among the several
safe and efficient options currently available for iris
reconstruction. It is important to distinguish between the
NewColorIris implant and existing safe prosthetic iris models. In
general, these models are used in aphakic or pseudophakic patients
with congenital or posttraumatic iris abnormalities and have
received Conformity European (CE) marking [7].
In cases of difficult glaucoma control, a valve implant is the
surgical treatment of choice. Complete angular closure determines a
poor response to filtering surgery. In the present patient, several
operations to implant an Ex-press® shunt were unsuccessful and we
finally opted for an Ahmed valve. Posterior chamber implant of this
device is always preferable, especially in a case such as the
present involving prior DSAEK surgery. Given the intense retraction
of the iris shown by our patient, we positioned the Ahmed valve
tube behind the iris remnant, in front of the new prosthesis.
In summary, the NewColorIris implant gives rise to serious
irreversible complications that are poorly manageable. The final
outcome of such complications is usually severe morbidity
accompanied by poor vision. We recommend that the use of cosmetic
implants should be avoided at all costs.
REFERENCES 1. Pozdeyeva NA, Pashtayev NP, Lukin VP, Batkov YN.
Artificial iris-
lens diaphragm in reconstructive surgery for aniridia and
aphakia. J Cataract Refract Surg. 2005; 31: 1750-1759.
2. Burk SE, Osher RH. Surgical management of aniridia. In: Roy
FH, Arzabe CW, eds, Master Techniques in Cataract and Refractive
Surgery. Thorofare, NJ, Slack. 2004; 3–10.
3. Anderson JE, Grippo TM, Sbeity Z, Ritch R. Serious
complications of cosmetic NewColorIris implantation. Acta
Ophthalmol. 2010; 88: 700-704.
4. Thiagalingam S, Tarongoy P, Hamrah P, Lobo AM, Nagao K,
Barsam C, et al. Complications of cosmetic iris implants. J
Cataract Refract Surg. 2008; 34: 1222-1224.
5. Arthur SN, Wright MM, Kramarevsky N, Kaufman SC, Grajewski
AL. Uveitis-glaucoma-hyphema syndrome and corneal decompensation in
association with cosmetic iris implants. Am J Ophthalmol. 2009;
148: 790-793.
6. Hoguet A, Ritterband D, Koplin R, Wu E, Raviv T, Aljian J, et
al. Serious ocular complications of cosmetic iris implants in 14
eyes. J Cataract Refract Surg. 2012; 38: 387-393.
7. Price MO, Price FW Jr, Chang DF, Kelley K, Olson MD, Miller
KM. Ophtec iris reconstruction lens United States clinical trial
phase I. Ophthalmology. 2004; 111: 1847-1852.
Morales-Fernandez L, Martinez-de-la-Casa JM, Borrego L,
Sanchez-Jean R, Arriola-Villalobos P, et al. (2015) Glaucoma and
Corneal Decompensation Following Cosmetic Iris Prosthesis
Implantation: A Case Report. JSM Ophthalmol 3(2): 1031.
Cite this article
http://www.ncbi.nlm.nih.gov/pubmed/16246779http://www.ncbi.nlm.nih.gov/pubmed/16246779http://www.ncbi.nlm.nih.gov/pubmed/16246779http://www.ncbi.nlm.nih.gov/pubmed/19493251http://www.ncbi.nlm.nih.gov/pubmed/19493251http://www.ncbi.nlm.nih.gov/pubmed/19493251http://www.ncbi.nlm.nih.gov/pubmed/18571095http://www.ncbi.nlm.nih.gov/pubmed/18571095http://www.ncbi.nlm.nih.gov/pubmed/18571095http://www.ncbi.nlm.nih.gov/pubmed/19660735http://www.ncbi.nlm.nih.gov/pubmed/19660735http://www.ncbi.nlm.nih.gov/pubmed/19660735http://www.ncbi.nlm.nih.gov/pubmed/19660735http://www.ncbi.nlm.nih.gov/pubmed/22244609http://www.ncbi.nlm.nih.gov/pubmed/22244609http://www.ncbi.nlm.nih.gov/pubmed/22244609http://www.ncbi.nlm.nih.gov/pubmed/15465545http://www.ncbi.nlm.nih.gov/pubmed/15465545http://www.ncbi.nlm.nih.gov/pubmed/15465545
Glaucoma and Corneal Decompensation Following Cosmetic Iris
Prosthesis Implantation: A Case ReportAbstractIntroductionCase
ReportDiscussionReferences Figure 1Figure 2Figure 3