Embed Size (px)
Citation preview
Case ReportRare Case of Rapidly Worsening REM SleepInduced Bradycardia
Ayyappa S. Duba, Suneetha Jasty, Ankit Mahajan, Vijay Kodadhala,Raza Khan, Prithviraj Rai, and Mohammad Ghazvini
Howard University Hospital, Washington, DC, USA
Correspondence should be addressed to Ankit Mahajan; [email protected]
Received 31 May 2015; Revised 26 July 2015; Accepted 30 July 2015
Academic Editor: Tayfun Sahin
Copyright © 2015 Ayyappa S. Duba et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Sinoatrial arrest also known as sinus pause occurs when sinoatrial node of the heart transiently ceases to generate the electricalimpulse necessary for the myocardium to contract. It may last from 2.0 seconds to several minutes. Etiologies of sinoatrial arrestcan be complex and heterogeneous. During rapid eyemovement (REM) sleep, sinus arrests unrelated to apnea or hypopnea are veryrare and only a few cases have been reported. Here we report a case of 36-year-oldmale with no significant past medical history whopresented to our hospital after a syncopal episode at night. Physical examination showed no cardiac or neurological abnormalitiesand initial EKG and neuroimaging were normal. Overnight telemonitor recorded several episodes of bradyarrhythmia with sinusarrest that progressively lengthened over time. Sleep study was done which confirmed that sinus arrests occurredmore during REMsleep and are unrelated to apnea or hypopnea. Electrophysiology studies showed sinus nodal dysfunction with no junctional escape,subsequently a dual chamber pacemaker placed for rapidly worsening case of REM sleep induced bradycardia.
1. Introduction
Rapid eye movement (REM) related bradyarrhythmia syn-drome and sinus arrest in the absence of an underlying car-diac or physiologic sleep disorder were first described in theearly 1980s [1]. Very few cases have been reported suggestingthat the prevalence of this nighttime rhythm abnormality isvery rare. According to a literature review published in 2011,only 8 cases (mean age 34 11 years; 88% male) of REM sleeprelated cardiac arrest have been identified [2]. Interestingly,most of them had vague “daytime” chest pain, dizziness, andsyncope as part of their symptom complex. Our patient hadno daytime symptoms and could easily have been missed, ifnot for the only episode of syncope he had at night after hewoke up from sleep.
2. Case Report
A 36-year-old Caucasian male with no significant past medi-cal history presented after an episode of loss of consciousnessand fall. Patient reported waking up from sleep and feeling
dizzy while walking to the restroom. When he was aboutto urinate he passed out, fell, and hit his head. He regainedconsciousness as soon as he hit the floor. He denied pal-pitations, chest pain, or diaphoresis before or after loss ofconsciousness. He is a social drinker and nonsmoker anddenied using any recreational drugs.
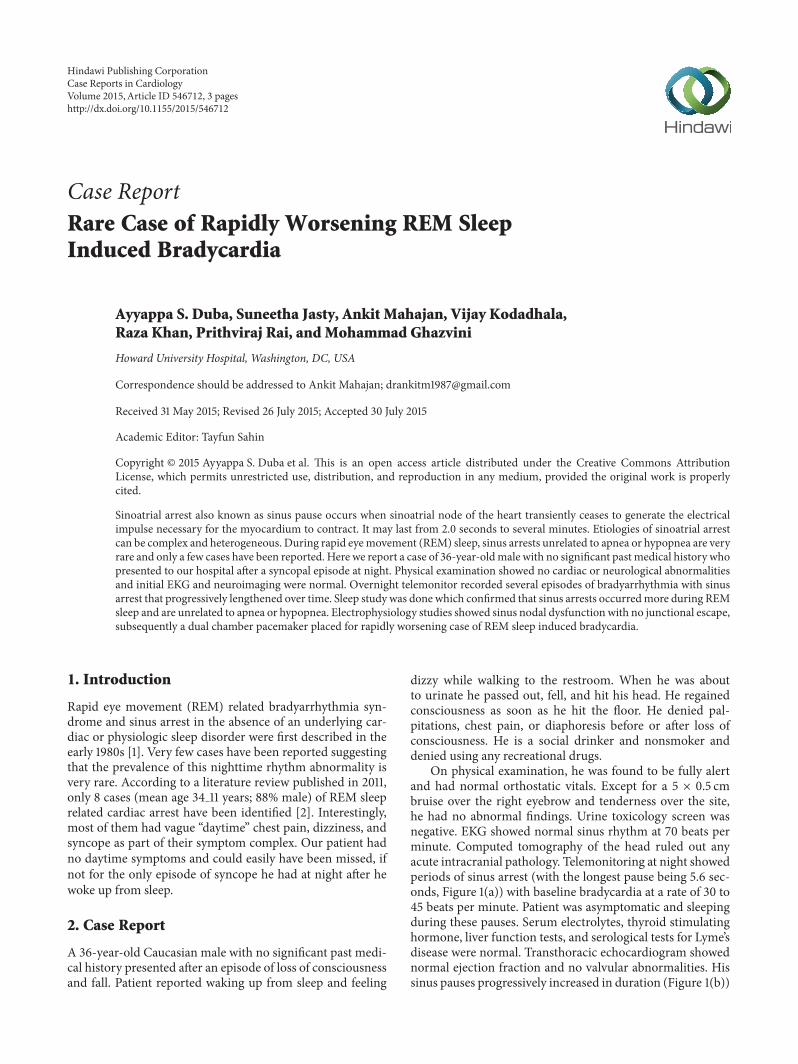
On physical examination, he was found to be fully alertand had normal orthostatic vitals. Except for a 5 × 0.5 cmbruise over the right eyebrow and tenderness over the site,he had no abnormal findings. Urine toxicology screen wasnegative. EKG showed normal sinus rhythm at 70 beats perminute. Computed tomography of the head ruled out anyacute intracranial pathology. Telemonitoring at night showedperiods of sinus arrest (with the longest pause being 5.6 sec-onds, Figure 1(a)) with baseline bradycardia at a rate of 30 to45 beats per minute. Patient was asymptomatic and sleepingduring these pauses. Serum electrolytes, thyroid stimulatinghormone, liver function tests, and serological tests for Lyme’sdisease were normal. Transthoracic echocardiogram showednormal ejection fraction and no valvular abnormalities. Hissinus pauses progressively increased in duration (Figure 1(b))
Hindawi Publishing CorporationCase Reports in CardiologyVolume 2015, Article ID 546712, 3 pageshttp://dx.doi.org/10.1155/2015/546712
2 Case Reports in Cardiology
5.6 s
(a)
7.4 s
(b)
8.6 s
(c)
Figure 1: Telemetry strips during sleep showed progressively prolonging periods of sinus arrest.
Table 1: Basic results of polysomnographic recordings.
BMI (kg/m2) 23.4Total sleep time (TST) 405 minutesREM 19.3%Central apnea/hypopnea events 2/4Obstructive apnea/hypopnea events 0/0Apnea/hypopnea index 1.1Number of AV blocks (>2.4 seconds) 0Number of sinus arrests (>2.4 seconds) 16Duration of cardiac pauses 2.5–7.8 secsSleep stage during cardiac pause REMMean oxygen saturation in REM 97.9%Minimal oxygen saturation in REM 94.5%Minimal oxygen saturation 91.4%% TST oxygen saturation <90% 0%
every successive night and the longest pause lasted for 8.6 sec(Figure 1(c)). During the day, his telemetry was normal ata rate ranging between 65 and 75 beats per minute withoutany episodes of sinus pause. On exercise, patient showedan appropriate increase in heart rate. After a thoroughliterature review, a very rare diagnosis of REM sleep relatedbradyarrhythmia syndrome with malignant vagotonia wasconsidered.
Polysomnographic study (Table 1) was done to evaluatesleep apnea and time sinus pauses with sleep cycle. Studydid not involve video monitoring but snoring was generallyabsent. A few mild central respiratory events were noted.However, these did not reach frequency threshold for diag-nosing sleep apnea. Cardiac telemetry showed normal sinusrhythm. During REM sleep, he demonstrated prolongedsinus pauses. Five sinus pauses of at least 3.5 seconds werenoted during REM sleep. The longest one lasted for 7.8seconds. Minimum pulse rate in wake and NREM cycle was
48.0 and 46.0, respectively. The patient appeared clinicallyasymptomatic all through the study and denied any symp-toms compatible with REM sleep behavior disorder.
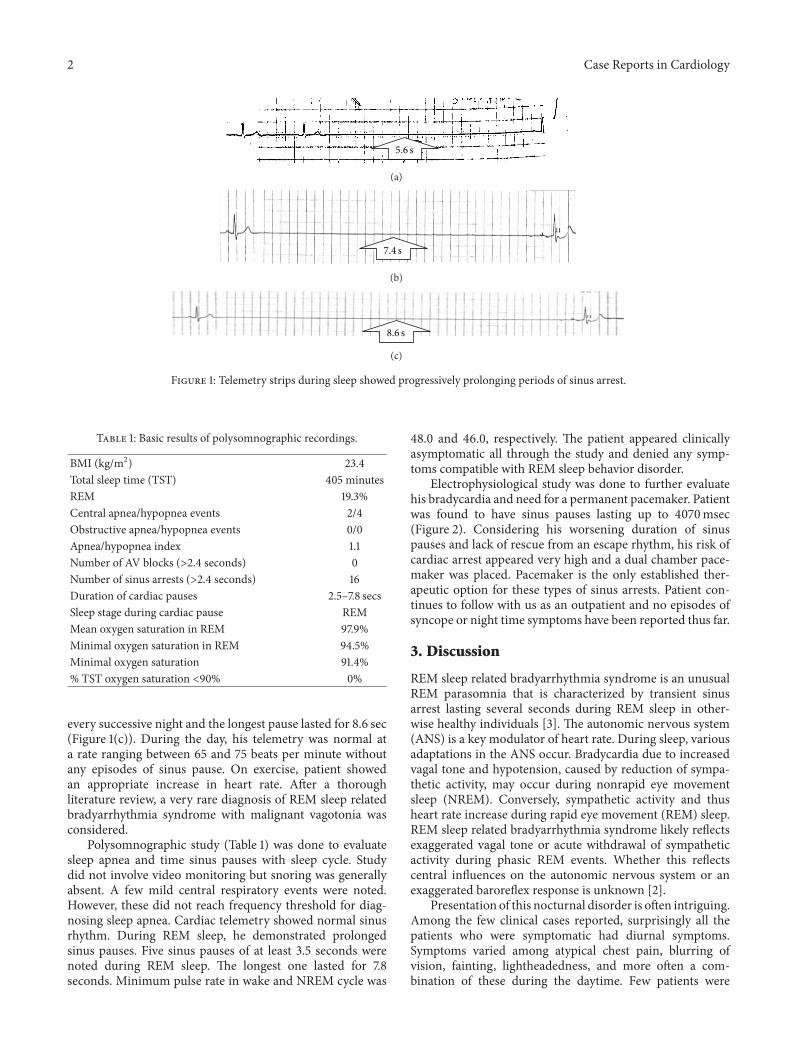
Electrophysiological study was done to further evaluatehis bradycardia and need for a permanent pacemaker. Patientwas found to have sinus pauses lasting up to 4070msec(Figure 2). Considering his worsening duration of sinuspauses and lack of rescue from an escape rhythm, his risk ofcardiac arrest appeared very high and a dual chamber pace-maker was placed. Pacemaker is the only established ther-apeutic option for these types of sinus arrests. Patient con-tinues to follow with us as an outpatient and no episodes ofsyncope or night time symptoms have been reported thus far.
3. Discussion
REM sleep related bradyarrhythmia syndrome is an unusualREM parasomnia that is characterized by transient sinusarrest lasting several seconds during REM sleep in other-wise healthy individuals [3]. The autonomic nervous system(ANS) is a key modulator of heart rate. During sleep, variousadaptations in the ANS occur. Bradycardia due to increasedvagal tone and hypotension, caused by reduction of sympa-thetic activity, may occur during nonrapid eye movementsleep (NREM). Conversely, sympathetic activity and thusheart rate increase during rapid eye movement (REM) sleep.REM sleep related bradyarrhythmia syndrome likely reflectsexaggerated vagal tone or acute withdrawal of sympatheticactivity during phasic REM events. Whether this reflectscentral influences on the autonomic nervous system or anexaggerated baroreflex response is unknown [2].
Presentation of this nocturnal disorder is often intriguing.Among the few clinical cases reported, surprisingly all thepatients who were symptomatic had diurnal symptoms.Symptoms varied among atypical chest pain, blurring ofvision, fainting, lightheadedness, and more often a com-bination of these during the daytime. Few patients were
Case Reports in Cardiology 3
II
III
aVL
aVR
aVF
V1
I
4070ms
Figure 2: Electrophysiology study showed sinus of 4070 milliseconds (4.07 secs).
accidentally detected while undergoing a polysomnographicstudy for other reasons. In REM related bradyarrhythmiawith sinus arrests, since episodes occur during REM sleep,patients might remain asymptomatic. Some cases of suddenunexpected death during sleep in apparently healthy individ-uals can be explained by these prolonged REM sleep relatedsinus arrests.Unlike the previously reported cases, our patienthad progressive worsening of maximal sinus pauses everysuccessive night, which posed an imminent threat of suddencardiac death. Only one case was previously reported inliterature, where patient had a similar worsening of maximalsinus pauses [4]. However, unlike our patient, his worseningof pauses occurred at a far slower pace (over a year).
Management of these cases is often very challenging.Pacemaker implantation is the only successful therapeu-tic approach described in the literature for patients withsymptomatic REM sleep related bradyarrhythmias and sinusarrests. In a literature review, eight patients with REM relatedsinus arrest were collectively analyzed [2]. Among them,7 patients were symptomatic (diurnal symptoms) and onepatient was asymptomatic. Six of the 7 symptomatic patientswere eventually treatedwith implantable cardiac pacemakers.Of these, five patients were followed on the long-term.Interestingly, all stayed asymptomatic for a mean follow-upduration of 3.7 ± 2.9 years. Although symptomatic benefits ofcardiac pacing are quite evident from this review, systematicverification of this assumption and postulating a mortalitybenefit is difficult due to paucity of this condition. In theabsence of diurnal symptoms, we do not know whethercertain cases of sudden cardiac death might have been thefirst presentation of this nocturnal arrhythmia [1]. WhetherREM related sinus arrest predisposes to sudden nocturnalcardiac death is unknown, but implanting a pacemaker mayalleviate this potential risk [2].
4. Conclusion
This is a unique presentation of REM sleep related brad-yarrhythmia with rapidly worsening maximal sinus arrestduration. All the patients previously reported with this disor-der presented with vague diurnal symptoms or were asymp-tomatic. Our patient presented with exclusive nocturnalsymptoms (dizziness during sleep interruptions even whilelying and an episode of syncope), which are more congruentwith the timing of this rhythm disturbance. This will be thefirst reported case of REM sleep related bradyarrhythmiawith exclusive nocturnal symptoms and rapidly worseningmaximal sinus arrest duration.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
References
[1] C. Guilleminault, P. Pool, J.Motta, andA.M.Gillis, “Sinus arrestduring REM sleep in young adults,”TheNew England Journal ofMedicine, vol. 311, no. 16, pp. 1006–1010, 1984.
[2] J.-E. C. Holty and C. Guilleminault, “REM-related brad-yarrhythmia syndrome,” Sleep Medicine Reviews, vol. 15, no. 3,pp. 143–151, 2011.
[3] W. Janssens, R. Willems, D. Pevernagie, and B. Buyse, “REMsleep-related brady-arrhythmia syndrome,” Sleep and Breathing,vol. 11, no. 3, pp. 195–199, 2007.
[4] N. Sanna, C. Della Marca, M. Bianco et al., “Prolonged asystoliain a young athlete: a case of sinus arrest during REM sleep,”International Journal of Sports Medicine, vol. 25, no. 6, pp. 457–460, 2004.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com













![ProvRem_Reyes v. Lim [Judicial Deposit as a Prov Rem in Case of EQUITY]](https://img.pdfslide.net/doc/110x75/5695d41d1a28ab9b02a05973/provremreyes-v-lim-judicial-deposit-as-a-prov-rem-in-case-of-equity.jpg)