Embed Size (px)
Citation preview

Septic arthritis of the hip is associ-ated with devastating complica-tions if not treated promptly.1,2
These complications include os-teomyelitis of the proximal femur,growth arrest of the proximal femurwith resulting limb-length discrepancy,coxa magna, coxa vara, pathologic dis-location, avascular necrosis of thefemoral head and arthrosis.2–5 Epiphysi-olysis or epiphyseal separation after sep-tic arthritis has been reported in infants.Most of these reports were publishedin the preantibiotic era,6,7 or in the early1960s8–10 before urgent arthrotomy be-
came the standard treatment for acuteseptic arthritis. We describe a case ofslipped capital femoral epiphysis, previ-ously unreported, complicating delayedtreatment of septic arthritis of the hipin an adolescent boy.
CASE REPORT
A 13-year-old boy, who was previ-ously in good health, sustained apainful blow to his right hip whileplaying hockey. He was able to con-tinue playing but had continued hippain causing him to limp. Three days
after the injury a fever developed(body temperature, 38.3 °C). Thenext day he sought medical help. Hisfamily physician diagnosed a musclestrain and prescribed acetaminophenand codeine for the pain.The boy’s fever persisted over the
next 10 days and his pain increased.Consultations with an orthopedic sur-geon and another family physiciansupported the diagnosis of a musclestrain of the hip. Fourteen days afterthe injury, the boy presented to theemergency department of his localhospital. He was referred to The Hos-
Case ReportÉtude de cas
SLIPPED CAPITAL FEMORAL EPIPHYSIS AFTER SEPTICARTHRITIS OF THE HIP IN AN ADOLESCENT: REPORT OF A CASE
Robert G. Marx, MD, MSc; James G. Wright, MD, MPH
From the Division of Orthopedic Surgery, The Hospital for Sick Children, Toronto, Ont.
Accepted for publication Nov. 11, 1997.
Correspondence to: Dr. James G. Wright, S 107, Division of Orthopedic Surgery, The Hospital for Sick Children, 555 University Ave., Toronto ON M5G 1X8
© 1999 Canadian Medical Association (text and abstract/résumé)
Septic arthritis of the hip must be managed promptly to avoid the serious complications associated with thecondition. In the case reported here, the diagnosis was delayed and was complicated by a slipped capitalfemoral epiphysis. The patient, an adolescent boy previously in good health, presented with a 2-week his-tory of hip pain and systemic illness. Septic arthritis was diagnosed and was managed by incision anddrainage and antibiotic therapy. Two weeks later he presented with a subcutaneous abscess and a slippedcapital femoral epiphysis, which was pinned in situ. There was a 2.5-cm leg-length discrepancy. Avascularnecrosis of the femoral head subsequently developed leaving the boy with a permanentdisability.
Il faut traiter rapidement l’arthrite aiguë suppurée de la hanche afin d’éviter les complications sérieuses as-sociées à cet état. Dans le cas décrit ici, le diagnostic a été posé en retard et a été compliqué par une luxa-tion de l’épiphyse de la tête du fémur. Le patient, un adolescent auparavant en bonne santé, se plaignaitd’avoir une douleur à la hanche et des malaises depuis deux semaines. On a diagnostiqué une arthrite aiguësuppurée qui a été traitée par incision et drainage, et administration d’antibiotiques. Deux semaines plustard, il s’est présenté avec un abcès sous-cutané et une luxation de l’épiphyse de la tête du fémur, qui a étéfixée in situ. Le patient avait une jambe plus longue que l’autre de 2,5 cm. Une nécrose vasculaire de latête du fémur a fait son apparition par la suite et causé à l’adolescent une incapacité permanente.
CJS, Vol. 42, No. 2, April 1999 145

pital for Sick Children in Toronto.On examination, the boy was
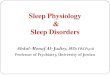
lethargic and had a temperature of39.1 °C. His hip, held in slight flexionand external rotation, was extremelypainful with any motion. Radiographsof the hip and pelvis revealed a small lytic area, possibly due to os-teomyelitis, adjacent to the epiphysealplate (Fig. 1). There was no evidenceof a slipped epiphysis. His leukocytecount was 8.6 × 109/L and the ery-throcyte sedimentation rate was 123mm/h. Ultrasonography of the hipshowed an effusion with debris pre-sent in the joint. The presumptive di-agnosis of septic arthritis of the hipwas made.Emergency incision and drainage
of the right hip through an anteriorapproach revealed a large amount ofpus. The articular cartilage of thefemoral head and acetabulum wasdarkened in 50% of the surface area. Aclosed suction drain was placed in thehip, and the subcutaneous tissue andskin were closed. Within 24 hours, theboy’s temperature returned to nor-mal, his pain lessened and he was able
to bear weight on the affected leg.Staphylococcus aureus sensitive tocloxacillin was grown from a cultureof hip tissue. The drain was removedon postoperative day 2. Cloxacillinwas given intravenously for 6 days. Hewas then discharged home, bearingpartial weight on the affected leg andwas prescribed cloxacillin orally 1 gevery 6 hours.Two weeks later he returned to the
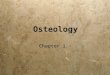
outpatient clinic, complaining of in-creasing pain and inability to bearweight. There was a small amount ofpurulent drainage from the drain site.Radiographs of the hip revealed aslipped capital femoral epiphysis of theright hip with a slight relative increasein the density of the epiphysis (Fig. 2).A subcutaneous abscess was drainedand he was given cloxacillin intra-venously 1 g every 6 hours. Postoper-atively, he was placed in skin traction.Six days later, he underwent percuta-neous pinning of the slipped epiphysisin situ.One week later (1 month after the
initial operation) he was readmittedbecause of severe right hip pain. Radi-
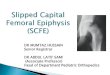
ographs revealed obvious relative ra-diodensity of the capital epiphysis, in-dicating avascular necrosis of thefemoral head (Fig. 3). He was givenphysical therapy, and when he was inbed the leg was placed in slings and al-lowed to swing free. The pain gradu-ally diminished and he was discharged10 days after admission.Eleven months after the initial op-
eration, the boy underwent removalof the pin because the tip of the screwwas approaching the hip joint. Be-cause of the avascular necrosis and as-sociated growth arrest of the proximalfemur, the patient had a length dis-crepancy of 2.5 cm. Two monthslater, he underwent a left distalfemoral epiphysiodesis (performedunder fluoroscopic guidance using a4-mm Association for Osteosynthesisdrill and a curette by way of medialand lateral incisions).At follow-up, 2 years postopera-
tively, the boy was free of pain. He hada Trendelenberg lurch and a leg-length discrepancy of 2 cm. The rangeof motion of the right hip was 15° ofadduction, no abduction, 35° of exter-
MARX AND WRIGHT
146 JCC, Vol. 42, No 2, avril 1999
FIG. 1. Two weeks after the onset of pain, the radiograph shows no evidenceof a slipped capital femoral epiphysis. There is an area of possible os-teomyelitis adjacent to the epiphyseal plate (arrow).
FIG. 2. Two weeks after incision and drainage of the hip, the radiographshows a slipped capital femoral epiphysis of the right hip with a slight rela-tive increase in the density of the epiphysis. There is also a slight decreasein the joint space compared with the contralateral side.

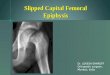
nal rotation, 5° of internal rotation andflexion from 20° to 90°. Radiographsshowed avascular necrosis and collapseof the femoral head (Fig. 4).
DISCUSSION
Complications secondary to septicarthritis of the hip have become rela-tively less frequent since the advent ofantibiotics and recognition of the im-portance of prompt surgical drainage.Although the potential complicationsof the delayed treatment are multi-ple,4,9,11 the 2 commonest complica-tions are chondrolysis12,13 and avascu-lar necrosis.14
In our case, in which an adolescentboy received delayed treatment forseptic arthritis of the hip and later pre-sented with a slipped capital femoralepiphysis, the coexistence of a slip anda septic arthritis may have been due tothe delay in treating the infection andsecondary damage to the growth platewith subsequent slip. Alternatively,the boy may have had an undisplacedslip at the time of the initial presenta-
tion, complicated by septic arthritisand subsequent worsening of the slip.The former cause is more likely forseveral reasons. First, slipped epiphysisis a known complication of septicarthritis and has been documented inyounger children in the preantibioticera6,7 and before urgent arthrotomybecame the standard of care for septichips.8–10 Second, a traumtic undis-placed slip of the femoral capital epi-physis in an otherwise healthy boy ofnormal weight is quite unusual. Asnoted in Fig. 1, there was no radi-ographic evidence of displacement ofthe capital femoral epiphysis when wefirst examined the hip. Third, the boywas able to continue playing hockeyafter the injury, which would be un-likely in the event of a traumatic slip.Slipped capital femoral epiphysis
secondary to delayed treatment of sep-tic arthritis of the hip in an adolescentis previously unreported. The patient’sheight and weight were in the 70thpercentile for his age so obesity wasnot a contributing factor in the slip.The infectious agent in this case was
S. aureus, the commonest infectingorganism in septic arthritis2 and a par-ticularly virulent pathogen.4 It is pos-sible that the prolonged delay beforeinitiating therapy led to the destruc-tion of the cartilage of the growthplate, resulting in the slip.Chronic osteomyelitis and avascu-
lar necrosis of the femoral head hasbeen treated by excision of the head,6
subtrochanteric osteotomy4 or simpledrainage with spontaneous absorptionof the head.6,9 When the boy in ourcase presented with a subcutaneousabscess and the slipped epiphysis, thepreferred treatment was uncertain forseveral reasons. First, the femoral headmay have been a sequestrum, whichcould have led to implant infection orfailure of fixation had the fixationbeen undertaken at the time of thedrainage procedure. Second, the opti-mal timing and indications for pin fix-ation of an infected slipped capital epi-physis are unknown.Our management protocol for this
condition was irrigation and débride-ment of the subcutaneous abscess, fol-
SLIPPED CAPITAL FEMORAL EPIPHYSIS
CJS, Vol. 42, No. 2, April 1999 147
FIG. 3. One month after incision and drainage of the hip, and after pin fixa-tion of the slipped capital femoral epiphysis, there is a relative increase inthe radiodensity of the femoral head, indicating avascular necrosis. Thejoint space is significantly narrowed compared with the contralateral side.
FIG. 4. Two years after the initial presentation, the radiograph shows avas-cular necrosis and collapse of the femoral head.

lowed by traction and delayed in-situhip pinning. The rationale of the cho-sen treatment was to keep the hipanatomy as normal as possible. In ourcase, the boy did not suffer any of thepotential infectious complications ofthis treatment and regained somepain-free motion of his hip joint at the2-year follow-up. However, there re-mained a leg-length discrepancy andrestricted motion at the hip, and hewas left with a permanent disability.
Dr. Robert G. Marx is supported by theArthritis Society, the Insitute for Work andHealth and the Surgical Scientist Program atthe University of Toronto. Dr. James G.Wright is an MRC Scientist.
References
1. Daniel D, Akeson W, Amiel D, RyderM, Boyer J. Lavage of septic joints inrabbits: effects of chondrolysis. J Bone
Joint Surg [Am] 1976;58(3):393-5.
2. Gillespie R. Septic arthritis Clin Orthop1973;96:152-9.
3. Fabry G, Meire E. Septic arthritis ofthe hip in children: poor results afterlate and inadequate treatment. J Pedi-atr Orthop 1983;3:461-6.
4. Morrey BF, Bianco AJ, Rhodes KH.Suppurative arthritis of the hip in chil-dren. J Bone Joint Surg [Am] 1976;58 :388-92.
5. Paterson DC. Acute suppurative arthri-tis in infancy and childhood. J BoneJoint Surg [Br] 1970;52(3):474-82.
6. Badgley CE, Yglesias L, Perham WS,et al. Study of the end results in 113cases of septic hips. J Bone Joint Surg1936;18(4):1047-61.
7. Green WT. Osteomyelitis in infancy.JAMA 1935;105(23):1835-9.
8. Blanche DW. Osteomyelitis in infants.J Bone Joint Surg [Am] 1952;34(1) :71-85.
9. Eyre-Brook AL. Septic arthritis of thehip and osteomyelitis of the upper endof the femur in infants. J Bone JointSurg [Br] 1960;42(1):11-20.
10 Lloyd-Roberts GC. Suppurative arthri-tis of infancy. J Bone Joint Surg [Br]1960;42(4):706-20.
11. Stetson JW, DePonte RJ, SouthwickWO. Acute septic arthritis of the hip inchildren. Clin Orthop 1968;56:105-16.
12. Curtiss PH, Klein L. Destruction of ar-ticular cartilage in septic arthritis; I. Invitro studies. J Bone Joint Surg [Am]1963;45(4):797-806.
13. Curtiss PH, Klein L. Destruction of ar-ticular cartilage in septic arthritis; II. Invivo studies. J Bone Joint Surg [Am]1965;47(8):1595-604.
14. Kemp HBS, Lloyd-Roberts GC. Avas-cular necrosis of the capital epiphysisfollowing osteomyelitis of the proximalfemoral metaphysis. J Bone Joint Surg[Br] 1974;56(4):688-97.
MARX AND WRIGHT
148 JCC, Vol. 42, No 2, avril 1999
SESAP Critique / Critique SESAP
ITEMS 615–616
Chest pain is often the initial symptom of patients with bronchogenic carcinoma invading the chest wall. Resectionfor cure with an absolute five-year survival of 30% to 50% is possible when patients have no positive nodes. Patientswith positive mediastinal nodes or distant metastases are essentially incurable. Prethoracotomy evaluation should in-clude complete staging and assessment of pulmonary reserve. Cardiac stress testing should be reserved for patientswith clinical evidence of coronary artery disease. Cell type, tumor size, depth of chest wall invasion, and extent ofchest wall or lung resection have no significant influence on survival. The efficacy of adjuvant postoperative radio-therapy is unproven except for control of local recurrence in the event of poor chest wall surgical margins.
615 B 616 C
References615–616/1. Allen MS, Mathisen DJ, Grillo HC, Wain JC, et al: Bronchogenic carcinoma with chest wall invasion.Ann Thorac Surg 51:948-951, 1991615–616/2. Patterson GA, Ilves R, Ginsberg RJ, Cooper JD, et al: The values of adjuvant radiotherapy in pul-monary and chest wall resection for bronchogenic carcinoma. Ann Thorac Surg 34:692-697, 1982615–616/3. Piehler JM, Pairolero PC, Weiland LH, Offord KP, et al: Bronchogenic carcinoma with chest wall in-vasion: Factors affecting survival following en bloc resection. Ann Thorac Surg 34:684-692, 1982