Embed Size (px)
Citation preview

Original Article
Case Series of Anterior Intervertebral Graft Extrusions in Transforaminal Lumbar
Interbody Fusion Surgeries
Alan T. Villavicencio1,2, E. Lee Nelson1, Sharad Rajpal1,2, Federica Otalora2, Sigita Burneikiene1,2
-BACKGROUND: According to the published reports,revision surgery is sometimes recommended even in pa-tients with asymptomatic anterior lumbar intervertebralgraft migrations. The main purpose of this chart reviewstudy was to report on the clinical course and outcomes ofpatients who had anterior intervertebral graft extrusionsafter transforaminal lumbar interbody fusion (TLIF).
-METHODS: From July 2002 to July 2014, 1259 consecu-tive TLIF surgeries were performed. These were reviewed,and patients who had anterior intervertebral graft extru-sions were identified.
-RESULTS: The incidence of graft extrusion was 0.6% (7of 1259 patients). There were 6 female patients and 1 malepatient with an average age of 65.7 years (range, 44e80years). All patients underwent TLIF with bilateral pediclescrew fixation, and 6 received recombinant human bonemorphogenetic protein-2. Graft migrations were diagnosedbetween 5 days and 8 months postoperatively except for 2cases in which migration occurred intraoperatively. Thepatients were closely followed for an average of 27.4months (range, 12e43 months). All patients remainedasymptomatic during the follow-up period and had solidfusion despite extrusions with an average time to fusion of13 months (range, 10e18 months). No other adverse eventsoccurred during the follow-up period.
-CONCLUSIONS: The risks of additional and highlyinvasive revision surgery should be weighed against thepotential short-term and long-term complications associ-ated with graft extrusions or migrations. It was demon-strated that fusion may take longer but can be achieved,
Key words- Complications- Graft extrusions- Lumbar fusion
Abbreviations and AcronymsCT: Computed tomographyPEEK: PolyetheretherketonerhBMP-2: Recombinant human bone morphogenetic protein-2TLIF: Transforaminal lumbar interbody fusion
130 www.SCIENCEDIRECT.com WORLD NEU
and close observation may be adequate for asymptomaticpatients.
INTRODUCTION
umbar intervertebral graft extrusion is a complication thatcan occur during or after lumbar interbody fusion pro-
Lcedures. The clinical implications of graft extrusiondepend on the location. Posterior implant migrations into thespinal canal can cause nerve root compression symptoms andusually require revision surgery.1-6 Kuslich et al.7 reported 1.7% ofposterior implant migrations requiring reoperation and 1.4%without reoperation. The reported rate for posterior graftmigration is 0.8%e3.2%.1,4,6-9 Only 1 posterior lumbar implantmigration case out of 11,817 spinal operations accounted for majorneurologic deficit (paraparesis) that resulted in spinal canalcompromise.10
Anterior graft extrusions are less frequent but may occur moreeasily if the structural integrity of the anterior anulus fibrosus orthe anterior longitudinal ligaments is inadvertently compromised.A few published case reports described complications andmanagement strategies associated with retroperitoneal graftmigrations. Retroperitoneal migrations may lead to vascularcomplications,11-13 damage to the viscera,14 or radicularsymptoms.15 Revisions for asymptomatic cage migrations3,16 andpseudarthrosis17 were also described in the literature. Thereported rate for anterior graft migrations is 0.8% withreoperation and 1.5% without reoperation.7 According to thepublished reports, revision surgery is sometimes recommendedin cases of anterior lumbar intervertebral graft extrusions.3,16
The main purpose of this retrospective chart review study was toreport on the clinical course and outcomes of patients who had
From 1Boulder Neurosurgical Associates; and 2Justin Parker Neurological Institute, Boulder,Colorado, USA
To whom correspondence should be addressed: Sigita Burneikiene, M.D.[E-mail: [email protected]]
Citation: World Neurosurg. (2016) 85:130-135.http://dx.doi.org/10.1016/j.wneu.2015.08.047
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2016 Elsevier Inc. All rights reserved.
ROSURGERY, http://dx.doi.org/10.1016/j.wneu.2015.08.047
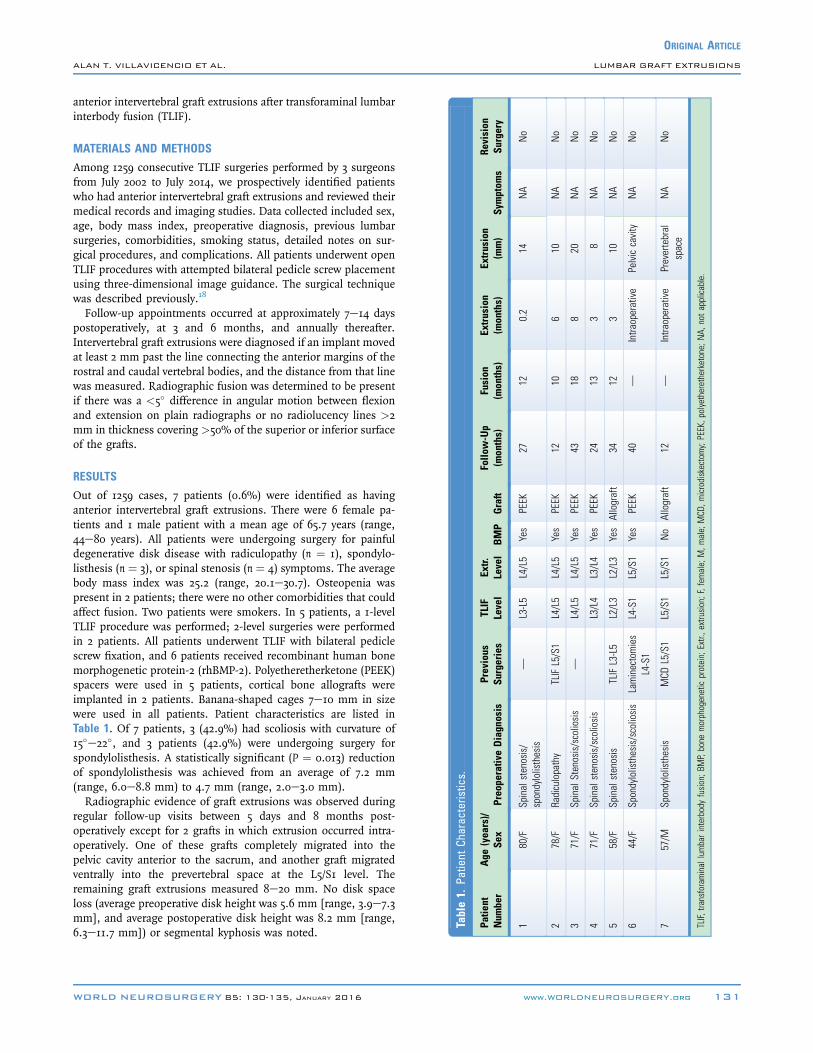
Table1.
Patient
Charac
teristics.
Patie
ntNum
ber
Age
(yea
rs)/
Sex
Preope
rativ
eDiagn
osis
Previous
Surgeries
TLIF
Level
Extr.
Level
BMP
Graft
Follo
w-Up
(months)
Fusion
(mon
ths)
Extrusion
(months)
Extrusion
(mm)
Symptom
sRe
vision
Surgery
180/F
Spinalstenosis/
spondylolisthesis
—L3-L5
L4/L5
Yes
PEEK
2712
0.2
14NA
No
278/F
Radiculopathy
TLIFL5/S1
L4/L5
L4/L5
Yes
PEEK
1210
610
NA
No
371/F
SpinalStenosis/scoliosis
—L4/L5
L4/L5
Yes
PEEK
4318
820
NA
No
471/F
Spinalstenosis/scoliosis
L3/L4
L3/L4
Yes
PEEK
2413
38
NA
No
558/F
Spinalstenosis
TLIFL3-L5
L2/L3
L2/L3
Yes
Allograft
3412
310
NA
No
644/F
Spondylolisthesis/scoliosis
Laminectomies
L4-S1
L4-S1
L5/S1
Yes
PEEK
40—
Intra
operative
Pelviccavity
NA
No
757/M
Spondylolisthesis
MCD
L5/S1
L5/S1
L5/S1
No
Allograft
12—
Intra
operative
Prevertebral
space
NA
No
TLIF,
transforaminal
lumbarinterbodyfusion;B
MP,bone
morphogeneticprotein;
Extr.,extrusion;F,fem
ale;
M,m
ale;
MCD
,microdiskectomy;PEEK,p
olyetheretherketone;
NA,
notapplicable.
ORIGINAL ARTICLE
ALAN T. VILLAVICENCIO ET AL. LUMBAR GRAFT EXTRUSIONS
anterior intervertebral graft extrusions after transforaminal lumbarinterbody fusion (TLIF).
MATERIALS AND METHODS
Among 1259 consecutive TLIF surgeries performed by 3 surgeonsfrom July 2002 to July 2014, we prospectively identified patientswho had anterior intervertebral graft extrusions and reviewed theirmedical records and imaging studies. Data collected included sex,age, body mass index, preoperative diagnosis, previous lumbarsurgeries, comorbidities, smoking status, detailed notes on sur-gical procedures, and complications. All patients underwent openTLIF procedures with attempted bilateral pedicle screw placementusing three-dimensional image guidance. The surgical techniquewas described previously.18
Follow-up appointments occurred at approximately 7e14 dayspostoperatively, at 3 and 6 months, and annually thereafter.Intervertebral graft extrusions were diagnosed if an implant movedat least 2 mm past the line connecting the anterior margins of therostral and caudal vertebral bodies, and the distance from that linewas measured. Radiographic fusion was determined to be presentif there was a <5� difference in angular motion between flexionand extension on plain radiographs or no radiolucency lines >2mm in thickness covering >50% of the superior or inferior surfaceof the grafts.
RESULTS
Out of 1259 cases, 7 patients (0.6%) were identified as havinganterior intervertebral graft extrusions. There were 6 female pa-tients and 1 male patient with a mean age of 65.7 years (range,44e80 years). All patients were undergoing surgery for painfuldegenerative disk disease with radiculopathy (n ¼ 1), spondylo-listhesis (n ¼ 3), or spinal stenosis (n ¼ 4) symptoms. The averagebody mass index was 25.2 (range, 20.1e30.7). Osteopenia waspresent in 2 patients; there were no other comorbidities that couldaffect fusion. Two patients were smokers. In 5 patients, a 1-levelTLIF procedure was performed; 2-level surgeries were performedin 2 patients. All patients underwent TLIF with bilateral pediclescrew fixation, and 6 patients received recombinant human bonemorphogenetic protein-2 (rhBMP-2). Polyetheretherketone (PEEK)spacers were used in 5 patients, cortical bone allografts wereimplanted in 2 patients. Banana-shaped cages 7e10 mm in sizewere used in all patients. Patient characteristics are listed inTable 1. Of 7 patients, 3 (42.9%) had scoliosis with curvature of15�e22�, and 3 patients (42.9%) were undergoing surgery forspondylolisthesis. A statistically significant (P ¼ 0.013) reductionof spondylolisthesis was achieved from an average of 7.2 mm(range, 6.0e8.8 mm) to 4.7 mm (range, 2.0e3.0 mm).Radiographic evidence of graft extrusions was observed during
regular follow-up visits between 5 days and 8 months post-operatively except for 2 grafts in which extrusion occurred intra-operatively. One of these grafts completely migrated into thepelvic cavity anterior to the sacrum, and another graft migratedventrally into the prevertebral space at the L5/S1 level. Theremaining graft extrusions measured 8e20 mm. No disk spaceloss (average preoperative disk height was 5.6 mm [range, 3.9e7.3mm], and average postoperative disk height was 8.2 mm [range,6.3e11.7 mm]) or segmental kyphosis was noted.
WORLD NEUROSURGERY 85: 130-135, JANUARY 2016 www.WORLDNEUROSURGERY.org 131

ORIGINAL ARTICLE
ALAN T. VILLAVICENCIO ET AL. LUMBAR GRAFT EXTRUSIONS
The average follow-up time was 27.4 months (range, 12e43months), and the patients’ clinical status was closely monitoredduring that time. All patients remained asymptomatic and allextrusions remained stable during the follow-up period. A softlumbar corset was prescribed for 6 weeks, but the patients wereencouraged to become active as soon as possible after surgery withlimited lifting and bending or twisting of the lumbar spine. Afterthis 6-week period, standard physical therapy was recommendedwith limited range of motion, flexion, extension, and lateralbending until fusion had been documented. All patients had solidfusion despite extrusions. For the patients who had intervertebralspace graft extrusions, the average time of fusion was 13 months(range, 10e18 months).
Case StudyA 44-year-old woman presented with axial low back pain andbilateral radiculopathy resulting from foraminal stenosis andspondylolisthesis at L4/L5 and L5/S1 levels with spinal instability.She previously underwent multiple laminectomies at L4/L5 and L5/S1 at an outside institution and developed a postlaminectomysyndrome, which was also complicated by postoperative pseudo-meningocele and required operative repair. Two-level posteriordecompressions and TLIFs with bilateral pedicle screw fixationwere performed. The pedicle screws were placed at L5 on the rightand bilaterally at S1 and L4. The left L5 pedicle was dysplastic andwould not accept the screw. The rods were inserted, and somereduction of spondylolisthesis was achieved. Diskectomies wereperformed at L4/L5 and L5/S1. After complete removal of diskmaterial and placement of a PEEK cage into the L5/S1 space, thecage felt slightly loose, and it subsequently slipped into the pelviccavity and anterior to the sacrum. The additional portions of the
Figure 1. Postoperative plain x-rays (lateral view) demonstrateposition of the graft 3 years later (B).
132 www.SCIENCEDIRECT.com WORLD NEU
ventral aspects of the disk were removed, but the implant couldnot be removed, and it was decided to leave it in place. Anotherintervertebral PEEK graft was selected and inserted into the L5/S1disk space. Postoperatively, there were no clinical signs of eitherarterial or venous vascular occlusion. A vascular surgeon wasconsulted, and it was decided that there was no need forcomputed tomography (CT) angiography or surgical interventionto retrieve this graft because it was highly unlikely that it wouldcause any vascular injury.The patient experienced significant improvement of her symp-
toms after surgery. She was closely followed for 40 months, andthe extruded implant remained proximal to the sacral prominencewith no signs of migration (Figure 1).
DISCUSSION
In addition to shortcomings in surgical technique that includeperforation of the anulus fibrosus and anterior longitudinal liga-ment, disk space violation, inadequate fixation, improper endplatepreparation or graft placement, and multiple other risk factorsresponsible for graft migration have been explored. Graft migra-tion can also occur in the settings of osteomyelitis, diskitis, orpseudarthrosis.4,19 Zhoa et al.6 retrospectively analyzed posteriorgraft migrations in 6 of 512 TLIF surgery cases and found thatthe size and shape of the graft, number of fused segments, andadjacent segment endplate shape may be contributing factors.McAfee et al.3 questioned the posterior approach per se as notbeing able to achieve sufficient distraction of the disk space andas a result placement of cages that are too small. Kimura et al.9
described “pear-shaped disks,” which are widely open anteriorlyas they have a concave surface in the anterior portion and aconvex surface in the posterior portion of the superior and
graft extrusion into the pelvic cavity (A) and stable
ROSURGERY, http://dx.doi.org/10.1016/j.wneu.2015.08.047

ORIGINAL ARTICLE
ALAN T. VILLAVICENCIO ET AL. LUMBAR GRAFT EXTRUSIONS
inferior endplates. Of 9 retropulsions after posterior lumbarinterbody fusion, 8 were reported in patients with pear-shapeddisks, especially if the L5/S1 level was involved. The authors alsosuggested that cages with 3�e5� lordosis do not fit the pear-shaped disks because they lack stability in the posterior aspectand sagittal plane of the disk space. Similar conclusions in regardto the shape and size of the implants were reached by Aoki et al.,8
but they also noted that higher posterior disk height and unilateralpedicle screw fixation, especially if scoliosis was present, couldfacilitate posterior graft migrations. Although we did notspecifically evaluate the risk factors in this study, 3 (42.9%) of 7patients in our study had spine scoliotic curvature of 15�e22�,and we believe this contributed to some degree to the spinalmisalignment and resulted in the reduced interface and stabilitybetween the implant and bone surface.Pedicle screw and rod fixation provides immediate stability
before the healing process occurs and an implant is secured in thedisk space. Although bilateral pedicle fixation was attempted in allpatients in our series, 1 patient had unilateral pedicle fixation atthe level of the extruded graft because the pedicle was not solidenough after repositioning, and an additional pedicle screw wasplaced at the adjacent level. During screw placement, 2 patientshad slight fractures in the pedicles, and fixation was reinforcedwith interspinous process fixation devices. Another patient had apoor bone-screw interface, which was reinforced with cement. Asa result, 4 of 5 patients with postoperatively extruded grafts hadsuboptimal pedicle screw placement and fixation in cases in whichgraft extrusions occurred postoperatively. There was an anteriorannular tear in both of the intraoperative graft extrusion cases. Webelieve that shortcomings in surgical technique were the leadingcause for all these anterior graft extrusions.The shape and type of the cage and positioning also could affect
cage migration.9,20-22 The titanium cages migrated ventrally withinthe disk space more easily than PEEK grafts: The change in po-sition of the interbody devices was 15.8% � 7.8% for titaniumcages versus 8.2% � 7.1% for PEEK grafts. The authors did notreport any graft extrusions, but they concluded that if migration istoo pronounced, it may lead to a loss of the restored disk height.21
Similar findings were reported by Smith et al.22 in a prospectivecohort study that compared carbon fiber implants withbiodegradable implants made from poly-L-lactide-co-D,L-lactidein patients undergoing instrumented TLIF procedures. Of 44patients, 8 (18.2%) had biodegradable cage posterior migrations,and 3 patients had pseudarthrosis as a result.Osteolysis caused by the use of rhBMP-2 was also identified in
several reports as a contributing factor responsible for graftmigration.23-25 Vaidya et al.25 thought that because of transientosteolysis and endplate resorption as a normal part of the boneremodeling process at the site of rhBMP-2 implantation, thepostoperative period from immediately postoperatively to 3months carries a higher risk for implant loosening, migration, andsubsidence. They did not observe any migrations beyond 6 monthsafter new bone formation occurred, but the reported 33% posteriorimplant migration rate as a result of significant osteolysis is quitehigh. In our series, rhBMP-2 was used in all but 1 patient, andmost of the patients had graft extrusion diagnosed by the 3-monthfollow-up. In 1 patient, graft extrusion was identified at 8 monthspostoperatively, and it took 18 months for the patient to achieve
WORLD NEUROSURGERY 85: 130-135, JANUARY 2016
fusion. Although there are contradicting previous reports onwhether osteolysis or graft subsidence affects fusion,26,27 weobserved that it took significantly longer (13 months on average) toachieve fusion in the patients who had a graft extruded in theintervertebral space compared with the results of our previouslypublished study, where an average time of 4.1 months (range,2e10 months) was reported, and all patients achieved radio-graphic fusion by 10 months.18
In the case of retroperitoneal graft migration, some authorssuggest that CT angiography and consultation with a vascularsurgeon should be considered to determine the relationship of themigrated implant and the major vascular structures. In the casesreported here, a vascular surgeon was consulted, but it wasdecided not to perform CT angiography. These migrationsoccurred at the L5/S1 level, which lies below the bifurcation of thevascular structures, and the grafts were thought not to be in thedirect proximity to major vessels. It can be justified that the de-cisions not to perform CT angiography are being made individu-ally on a case-by-case basis. However, after reviewing theliterature, we would recommend performing CT angiography todetermine the exact location of the extruded graft given the po-tential devastating consequence of such complications. Yoshimotoet al.13 reported a case of deep venous thrombosis after posteriorlumbar interbody fusion that was caused by a migrated bone graftfragment from the interbody site at L5/S1, which occluded the leftcommon iliac vein at the bifurcation. The patient becamesymptomatic on the second postoperative day and underwentrevision surgery and excision of the bone fragment. Anotherdevastating complication was reported by Cakmak et al.14 In thiscase, the patient had a history of multiple fusion proceduresfrom L3 through S1 complicated by surgical infection followedby a corpectomy at L5 and revisions of interbody fusion throughan anterior approach. A femur bone graft from the interbodyfusion site migrated to the colon perforating the medial aspectof the cecum. Pawar et al.12 suggested a “lasso technique”: ANo. 1 polyglactin 910 (Vicryl) suture is looped through the holesin the implant and removed when an optimal implantplacement is achieved. The authors reported an inadvertentlaceration of the inferior vena cava and migration of a titaniumcage into the pulmonary artery. An attempt to use an oversizedimplant in a patient with spondylodiskitis and severe stretch ofthe anterior vascular structures may have contributed to thiscomplication. Although a retroperitoneal approach was requiredto stop the bleeding, it was decided to leave the implant inplace and monitor the patient closely because of the highmorbidity of such a procedure.Several authors performed revision surgeries because of
asymptomatic anterior cage migrations. McAfee et al.3 reported apatient who underwent laparoscopic lumbar fusion using Bagbyand Kuslich cages. Although the patient was asymptomatic, aCT scan performed at the 6-week follow-up evaluation revealed adislodged cage anterior to the L5-S1 disk space. Revision surgerywas also performed laparoscopically, and fusion was achieved at24 months. Proubasta et al.16 reported intraoperativeretroperitoneal titanium-threaded cage migration during a poste-rior lumbar interbody fusion procedure at L5/S1. The posteriorapproach was abandoned at this stage, and the next day, after a CTscan confirmed the position of the cage near the great vessels, the
www.WORLDNEUROSURGERY.org 133
ORIGINAL ARTICLE
ALAN T. VILLAVICENCIO ET AL. LUMBAR GRAFT EXTRUSIONS
patient underwent laparotomy to extract the migrated implantfollowed by posterolateral fusion with instrumentation.Revision surgeries are more complex and associated with a
higher risk of complications. In a series of 14 patients, 8 of whomhad pseudarthrosis or infection with cage migration, 57% of pa-tients had vascular complications, and 1 patient died while un-dergoing revision surgeries using either transperitoneal orretroperitoneal approaches.17 The patients who initially underwentanterior lumbar interbody fusion had even higher rates of vascularcomplications. The average blood loss was 1400 mL (range,150e5700 mL), the average operative time was 270 minutes(range, 119e420 minutes), and the average hospital stay was 9days (range, 4e43 days). Fantini et al.11 retrospectively reviewedand reported on the incidence of major vascular injury during
134 www.SCIENCEDIRECT.com WORLD NEU
anterior lumbar spinal surgery. There was 1 case among 345operations in which anterior migration of a posteriorly placedinterbody implant was identified. The implant breached theanterior longitudinal ligament and adhered to the posterioraspect of the common iliac vein. Anterior revision surgery wasperformed with an estimated blood loss of 5000 mL.
CONCLUSIONS
The risks of additional and highly invasive revision surgery shouldbe weighed against the potential short-term and long-term com-plications associated with graft extrusions or migrations.Although fusion may take longer, this can be achieved, and closeobservation may be adequate for asymptomatic patients.
REFERENCES
1. Elias WJ, Simmons NE, Kaptain GJ, Chadduck JB,Whitehill R. Complications of posterior lumbarinterbody fusion when using a titanium threadedcage device. J Neurosurg. 2000;93:45-52.
2. Faundez AA, Schwender JD, Safriel Y, Gilbert TJ,Mehbod AA, Denis F, et al. Clinical and radio-logical outcome of anterior-posterior fusionversus transforaminal lumbar interbody fusion forsymptomatic disc degeneration: a retrospectivecomparative study of 133 patients. Eur Spine J.2009;18:203-211.
3. McAfee PC, Cunningham BW, Lee GA,Orbegoso CM, Haggerty CJ, Fedder IL, et al.Revision strategies for salvaging or improvingfailed cylindrical cages. Spine (Phila Pa 1976). 1999;24:2147-2153.
4. Tormenti MJ, Maserati MB, Bonfield CM,Gerszten PC, Moossy JJ, Kanter AS, et al. Peri-operative surgical complications of transforaminallumbar interbody fusion: a single-center experi-ence. J Neurosurg Spine. 2012;16:44-50.
5. Xu H, Tang H, Li Z. Surgical treatment of adultdegenerative spondylolisthesis by instrumentedtransforaminal lumbar interbody fusion in the Hannationality. J Neurosurg Spine. 2009;10:496-499.
6. Zhao FD, Yang W, Shan Z, Wang J, Chen HX,Hong ZH, et al. Cage migration after trans-foraminal lumbar interbody fusion and factorsrelated to it. Orthop Surg. 2012;4:227-232.
7. Kuslich SD, Ulstrom CL, Griffith SL, Ahern JW,Dowdle JD. The Bagby and Kuslich method oflumbar interbody fusion. History, techniques, and2-year follow-up results of a United States pro-spective, multicenter trial. Spine (Phila Pa 1976).1998;23:1267-1278; discussion 1279.
8. Aoki Y, Yamagata M, Nakajima F, Ikeda Y,Shimizu K, Yoshihara M, et al. Examining riskfactors for posterior migration of fusion cagesfollowing transforaminal lumbar interbody fusion:a possible limitation of unilateral pedicle screwfixation. J Neurosurg Spine. 2010;13:381-387.
9. Kimura H, Shikata J, Odate S, Soeda T,Yamamura S. Risk factors for cage retropulsionafter posterior lumbar interbody fusion: analysis of1070 cases. Spine (Phila Pa 1976). 2012;37:1164-1169.
10. Cramer DE, Maher PC, Pettigrew DB, Kuntz CT.Major neurologic deficit immediately after adultspinal surgery: incidence and etiology over 10years at a single training institution. J Spinal DisordTech. 2009;22:565-570.
11. Fantini GA, Pappou IP, Girardi FP, Sandhu HS,Cammisa Jr FP. Major vascular injury duringanterior lumbar spinal surgery: incidence, riskfactors, and management. Spine (Phila Pa 1976).2007;32:2751-2758.
12. Pawar UM, Kundnani V, Nene A. Major vesselinjury with cage migration: surgical complicationin a case of spondylodiscitis. Spine (Phila Pa 1976).2010;35:E663-E666.
13. Yoshimoto H, Sato S, Nakagawa I, Hyakumachi T,Yanagibashi Y, Nitta F, et al. Deep vein throm-bosis due to migrated graft bone after posteriorlumbosacral interbody fusion. Case report.J Neurosurg Spine. 2007;6:47-51.
14. Cakmak A, Gyedu A, Kepenekci I, Ozcan C,Unal AE. Colon perforation caused by migrationof a bone graft following a posterior lumbosacralinterbody fusion operation: case report. Spine(Phila Pa 1976). 2010;35:E84-85.
15. Oh HS, Lee SH, Hong SW. Anterior dislodgementof a fusion cage after transforaminal lumbarinterbody fusion for the treatment of isthmicspondylolisthesis. J Korean Neurosurg Soc. 2013;54:128-131.
16. Proubasta IR, Vallve EQ, Aguilar LF,Villanueva CL, Iglesias JJ. Intraoperative ante-pulsion of a fusion cage in posterior lumbarinterbody fusion: a case report and review of theliterature. Spine (Phila Pa 1976). 2002;27:E399-402.
17. Nguyen HV, Akbarnia BA, van Dam BE,Raiszadeh K, Bagheri R, Canale S, et al. Anteriorexposure of the spine for removal of lumbarinterbody devices and implants. Spine (Phila Pa1976). 2006;31:2449-2453.
ROSURGERY, http://
18. Villavicencio AT, Burneikiene S, Nelson EL,Bulsara KR, Favors M, Thramann J. Safety oftransforaminal lumbar interbody fusion and inter-vertebral recombinant human bonemorphogeneticprotein-2. J Neurosurg Spine. 2005;3:436-443.
19. Ormond DR, Albert Jr L, Das K. Poly-etheretherketone (PEEK) rods in lumbar spinedegenerative disease: a case series [e-pub ahead ofprint]. J Spinal Disord Tech. 2012; http://dx.doi.org/10.1097/BSD.0b013e318277cb9b.
20. Abbushi A, Cabraja M, Thomale UW,Woiciechowsky C, Kroppenstedt SN. The influ-ence of cage positioning and cage type on cagemigration and fusion rates in patients withmonosegmental posterior lumbar interbodyfusion and posterior fixation. Eur Spine J. 2009;18:1621-1628.
21. Recnik G, Kosak R, Vengust R. Influencingsegmental balance in isthmic spondylolisthesisusing transforaminal lumbar interbody fusion.J Spinal Disord Tech. 2013;26:246-251.
22. Smith AJ, Arginteanu M, Moore F, Steinberger A,Camins M. Increased incidence of cage migrationand nonunion in instrumented transforaminallumbar interbody fusion with bioabsorbablecages. J Neurosurg Spine. 2010;13:388-393.
23. Knox JB, Dai 3rd JM, Orchowski J. Osteolysis intransforaminal lumbar interbody fusion with bonemorphogenetic protein-2. Spine (Phila Pa 1976).2011;36:672-676.
24. Mroz TE, Wang JC, Hashimoto R, Norvell DC.Complications related to osteobiologics use inspine surgery: a systematic review. Spine (Phila Pa1976). 2010;35:S86-104.
25. Vaidya R, Sethi A, Bartol S, Jacobson M, Coe C,Craig JG. Complications in the use of rhBMP-2 inPEEK cages for interbody spinal fusions. J SpinalDisord Tech. 2008;21:557-562.
26. Behrbalk E, Uri O, Parks RM, Musson R, Soh RC,Boszczyk BM. Fusion and subsidence rate of standalone anterior lumbar interbody fusion using PEEKcage with recombinant human bone morphoge-netic protein-2. Eur Spine J. 2013;22:2869-2875.
dx.doi.org/10.1016/j.wneu.2015.08.047
ORIGINAL ARTICLE
ALAN T. VILLAVICENCIO ET AL. LUMBAR GRAFT EXTRUSIONS
27. Vaidya R, Weir R, Sethi A, Meisterling S,Hakeos W, Wybo CD. Interbody fusion withallograft and rhBMP-2 leads to consistent fusionbut early subsidence. J Bone Joint Surg Br. 2007;89:342-345.
Conflict of interest statement: A.T.V. has received industrygrant/research support from Orthofix, Zimmer Spine,Alphatec Spine, Grifols, Covidien, ProFibrix, Globus Medical,and Medtronic; has physician-owned distributorship forLeading Edge Spinal Implants; and holds membership in the
WORLD NEUROSURGERY 85: 130-135, J
American Association of Neurological Surgeons/JointSponsorship Council and North American Spine SocietyEducational Council Committee. E.L.N. has received industrygrant/research support from Medtronic Navigation, and hasspeaking/teaching arrangements with Medtronic Navigation.S.R. has received consultant fees from Medtronic, ZimmerBiomet, and K2M and has received an honorarium from theCleveland Clinic Foundation. F.O. and S.B. have no conflictsto report.
Received 30 June 2015; accepted 8 August 2015
ANUARY 2016 ww
Citation: World Neurosurg. (2016) 85:130-135.http://dx.doi.org/10.1016/j.wneu.2015.08.047
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
1878-8750/$ - see front matter ª 2016 Elsevier Inc.All rights reserved.
w.WORLDNEUROSURGERY.org 135





























