Embed Size (px)
Citation preview

British3rournal ofOphthalmology 1994; 78: 441-445
Increased prevalence of disciform maculardegeneration after cataract extraction withimplantation of an intraocular lens
Theo L van der Schaft, CorneliaM Mooy, Wim C de Bruijn, Paul GH Mulder, JanH Pameyer,Paulus T VM de Jong
Erasmus University,Rotterdam, TheNetherlandsInstitute ofOphthalmologyT L van der SchaftCM MooyJ H PameyerPT V M de Jong
Institute of PathologyCM MooyW C de Brui;n
Institute of BiostatisticsP G H MulderCorrespondence to:P T V M de Jong, Institute ofOphthalmology, ErasmusUniversity Rotterdam,PO Box 1738, 3000 DRRotterdam, The Netherlands.Accepted for publication1 February 1994
Figure I Light microscopicimage ofa human maculawith geographic atrophy(GA, between blackarrows). On the right theretinal pigment epithelium(RPE) and thephotoreceptors (PR) areatrophic. Basal laminardeposit (BLD), grade 3, ispresent under the atrophicRPE. A soft druse (D) canbe seen between the RPEand Bruch's membrane(white arrows). Thechoriocapillaris(arrowheads) is locatedunder Bruch's membrane.(Mallory stain,magnification xl05.)
AbstractAfter cataract extraction with implantation ofan intraocular lens the increased transmissionof ultraviolet and blue light may accelerate thedevelopment of age-related macular degenera-tion by producing free radicals in the retina.The maculae of 82 randomly selected post-mortem human pseudophakic eyes and 16fellow phakic eyes were examined by lightmicroscopy. The presence of a basal laminardeposit, hard and soft drusen, thickening andcalcification ofBruch's membrane, geographicatrophy, subretinal neovascularisation, anddisciform scars was assessed in a standardisedway. An age-matched series of 126 post-mortem phakic eyes was used as control group.There was no difference between the twogroups, except for a higher prevalence of harddrusen (exact trend test, p=0038) and disci-form scars for the pseudophakic eyes (Fisher'sexact test, p=0007). There was no significantcorrelation between either age-related changesin the macula or disciform degeneration andthe length of time between cataract surgeryand death. No significant difference was foundbetween pseudophakic eyes with or withoutultraviolet filter. These findings do not confirmthat disciform scar formation is caused by anincrease in ultraviolet or blue light.(Br3r Ophthalmol 1994; 78: 441-445)
The most common cause of poor vision in theelderly is caractact.' 2 In the United States morethan one million cataract operations are per-
-~~~~~~~~~~~~~~4
formed each year, accounting for 12% of allMedicare payments.34 After cataract extractionand implantation of an intraocular lens (IOL),visual acuity is regained in a high percentage ofcases. Thus the second most common reason forvisual loss in the Western world has becomemore important: age-related macular degenera-tion (ARMD), which is now the leading causeof irreversible blindness in the elderly in theWestern world.' 2 Development of ARMD aftercataract extraction and IOL implantation hasbeen described previously.S6
After the first two decades of life the naturallens becomes yellower and partly filters out theharmful blue light and ultraviolet radiation ofthesun.78 With the development of cataract thisfiltering capacity of the lens increases, protectingthe posterior pole of the eye against possible freeradicals formed under the influence of the blueand ultraviolet light.7-" At cataract extractionthis biological filter is removed. During theoperation, the retina is exposed to the lightsource of the operating microscope, which hasbeen shown to induce phototoxic damage to themacula."I The cataractous lens is replaced by acrystal clear IOL with or without an ultravioletfilter. It has been postulated that increasedultraviolet and blue light radiation affects normalmacular functioning and thus that cataractextraction might stimulate ARMD.""I1-"Advanced ARMD will become manifest as
either geographic atrophy of the retinal pigmentepithelium (RPE) and the photoreceptors (Fig 1)or a disciform reaction, which consists of theingrowth of new blood vessels from the chorio-capillaris through Bruch's membrane under theRPE. A subsequent haemorrhage from thesevulnerable vessels often results in disciform scarformation (Fig 2).16
Neovascularisation can reach the subretinalspace through gaps in Bruch's membrane.'7"8These gaps can be caused mechanically in thepresence of extensive calcification of Bruch'smembrane,'9 by macrophagal enzymatic diges-tion'18 20 or other factors. Pronounced calcificationor thickening of Bruch's membrane probablyincreases the rigidity of this membrane and thusmakes it more fragile.'8One of us (P de J) had the impression from
clinical practice that extracapsular cataractextraction with implantation of an IOL in theaged was sometimes followed, within 1 month,by the development of a subretinal haemorrhageand subsequent disciform reaction. The hypo-thesis was formulated that ruptures in Bruch'smembrane might be induced by sudden changesin intraocular pressure and in the volume of the
441
on 4 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.6.441 on 1 June 1994. D
ownloaded from
van derSchaft, Mooy, Bruijn, Mulder, Pameyer, dej7ong
eye during surgery, which would cause deforma-tipn of the eye.The aim of this histological investigation was
to study this hypothesis and to determine thepossible role of the increased transmission ofblue and ultraviolet light in the development ofARMD and macular aging in pseudophakic eyes
without an ultraviolet filter compared withpseudophakic eyes with an ultraviolet filter. Theprevalence ofARMD in pseudophakic eyes withbrown or blue irises was also compared. Litera-ture on the histology of macular aging is exten-sive," 17 IO-- but to the best of our knowledge thisis the first report on the histopathology ofa seriesof human maculae after cataract extraction andimplantation ofan IOL.
Materials and methods
MATERIALSWe obtained 89 postmortem pseudophakic eyesof white humans from a corneal transplantationbank and autopsies. At a later stage seven
pseudophakic eyes were excluded from thisstudy because information on age and date ofcataract extraction was not available. Otherwiseno selection was made. The remaining 82 eyes
included 21 pairs of pseudophakic eyes, 16pseudophakic eyes of which the phakic felloweye was also available for this study, and 24 singlepseudophakic eyes without the fellow eye. Anage-matched series of 126 unpaired phakic eye
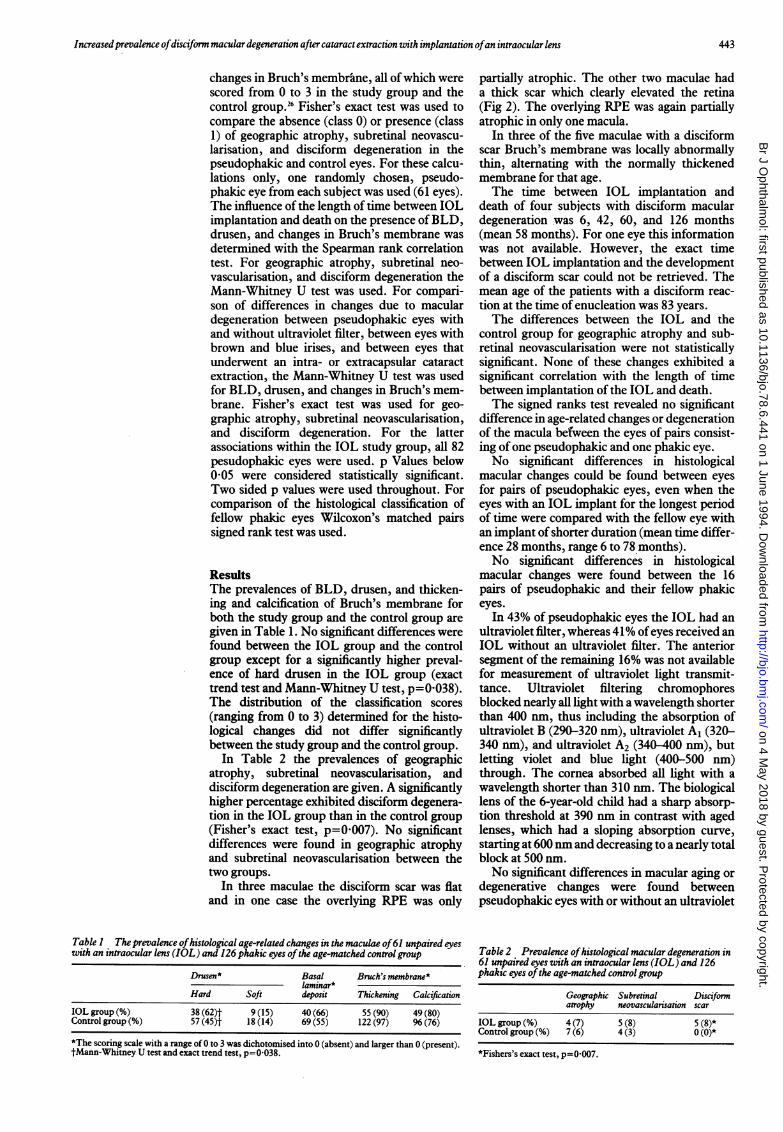
bank or autopsy eyes was used as control group.The age distributions for the study group and thecontrol group were similar (Fig 3). The controlgroup taken was larger than the group of eyes
with an IOL in order to increase power. Forstatistical reasons, the subject (and not the eye)was considered to be the experimental unit.Age at the time of death ranged from 62 to 100
years for both the pseudophakic group (mean81-3 (SD 7-6) years) and the control group (mean78 5 (8 9) years). The difference in mean agebetween these two groups is not statisticallysignificant. The time between IOL implantationand death ranged from 3 to 168 months (mean 52(40) months, median=48).
The maculae were prepared for light micro-scopy as described in a previous study.26 Thepresence of a basal laminar deposit (BLD), hardand soft drusen, thickening and calcification ofBruch's membrane, geographic atrophy, sub-retinal neovascularisation, and a disciform reac-tion in the macula was assessed blind in astandardised way, using the classification systemdescribed earlier.26
MICROSCOPIC EXAMINATIONBLD was defined by light microscopic examina-tion as amorphous, granular material locatedbetween the RPE and the inner layer of Bruch'smembrane (Fig 1).23126 It stained pale blue withthe Mallory stain.26 Thickening of Bruch'smembrane was assessed with the periodic acidSchiff(PAS) stain. Calcification ofBruch's mem-brane was studied with the von Kossa stain,which stains calcium phosphates brownish-black.26Drusen are deposits of material between the
basement membrane of the RPE and the innercollagenous zone of Bruch's membrane. Thedrusen were divided into hard drusen, whichwere usually dome-shaped with a hyalinisedappearance and stained brownish-blue with theMallory stain, and soft drusen, which wereusually larger, had sloping edges, containedgranular material which stained pale blue withthe Mallory stain or appeared to be opticallyalmost empty (Fig 1).The absence or presence of ultraviolet absorb-
ing chromophores in the IOLs was measuredwith a spectrophotometer through the intactanterior segment of the eyes. As a control theanterior segments of five phakic aged eyes, onephakic eye of a 6-year-old child, two aphakiceyes, and a single IOL with and without ultra-violet filter were measured.
STATISTICAL ANALYSISFor statistical analysis the Mann-Whitney U testand the exact trend test were used to compare thepresence of BLD, hard and soft drusen, and
60-69 70-79 80-89 90-100Years
* IOL eyes E3 Control eyes
Figure 3 Age distribution ofthe 61 subjects with anintraocular lens and the 126 phakic control eyes. Notice thesimilarity in distribution. For statistical reasons only one eyefrom each patient is included here. The control group waslarger to increase the statistical power.
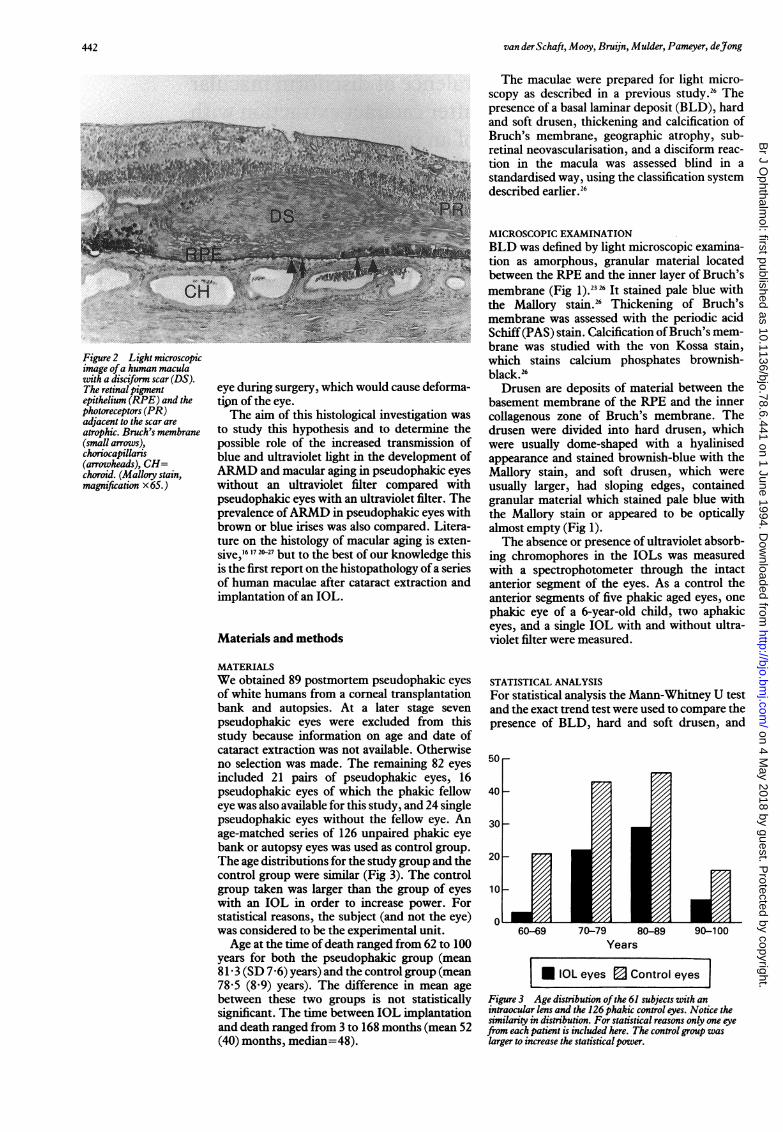
Figure 2 Light microscopicimage ofa human maculawith a disciform scar (DS).The retinalpigmentepithelium (RPE) and thephotoreceptors (PR)adjacent to the scar areatrophic. Bruch's membrane(small arrows),choriocapillaris(arrowheads), CH=choroid. (Mallory stain,magnification x65.)
442
on 4 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.6.441 on 1 June 1994. D
ownloaded from
Increased prevalence ofdisciform macular degeneration after cataract extraction with implantation ofan intraocular lens
changes in Bruch's membrane, all of which werescored from 0 to 3 in the study group and thecontrol group.26 Fisher's exact test was used tocompare the absence (class 0) or presence (class1) of geographic atrophy, subretinal neovascu-larisation, and disciform degeneration in thepseudophakic and control eyes. For these calcu-lations only, one randomly chosen, pseudo-phakic eye from each subject was used (61 eyes).The influence of the length of time between IOLimplantation and death on the presence ofBLD,drusen, and changes in Bruch's membrane wasdetermined with the Spearman rank correlationtest. For geographic atrophy, subretinal neo-vascularisation, and disciform degeneration theMann-Whitney U test was used. For compari-son of differences in changes due to maculardegeneration between pseudophakic eyes withand without ultraviolet filter, between eyes withbrown and blue irises, and between eyes thatunderwent an intra- or extracapsular cataractextraction, the Mann-Whitney U test was usedfor BLD, drusen, and changes in Bruch's mem-brane. Fisher's exact test was used for geo-graphic atrophy, subretinal neovascularisation,and disciform degeneration. For the latterassociations within the IOL study group, all 82pesudophakic eyes were used. p Values below0-05 were considered statistically significant.Two sided p values were used throughout. Forcomparison of the histological classification offellow phakic eyes Wilcoxon's matched pairssigned rank test was used.
ResultsThe prevalences of BLD, drusen, and thicken-ing and calcification of Bruch's membrane forboth the study group and the control group aregiven in Table 1. No significant differences werefound between the IOL group and the controlgroup except for a significantly higher preval-ence of hard drusen in the IOL group (exacttrend test and Mann-Whitney U test, p=0 038).The distribution of the classification scores(ranging from 0 to 3) determined for the histo-logical changes did not differ significantlybetween the study group and the control group.
In Table 2 the prevalences of geographicatrophy, subretinal neovascularisation, anddisciform degeneration are given. A significantlyhigher percentage exhibited disciform degenera-tion in the IOL group than in the control group(Fisher's exact test, p=0 007). No significantdifferences were found in geographic atrophyand subretinal neovascularisation between thetwo groups.
In three maculae the disciform scar was flatand in one case the overlying RPE was only
Table I The prevalence ofhistological age-related changes in the maculae of61 unpaired eyeswith an intraocular lens (IOL) and 126 phakic eyes ofthe age-matched control group
Drusen* Basal Bruch's membrane*laminar*
Hard Soft deposit Thickening Calcification
IOL group (%) 38 (62)t 9 (15) 40 (66) 55 (90) 49 (80)Control group (%) 57 (45)t 18 (14) 69 (55) 122 (97) 96(76)
*The scoring scale with a range of 0 to 3 was dichotomised into 0 (absent) and larger than 0 (present).tMann-Whitney U test and exact trend test, p=0-038.
partially atrophic. The other two maculae hada thick scar which clearly elevated the retina(Fig 2). The overlying RPE was again partiallyatrophic in only one macula.
In three of the five maculae with a disciformscar Bruch's membrane was locally abnormallythin, alternating with the normally thickenedmembrane for that age.The time between IOL implantation and
death of four subjects with disciform maculardegeneration was 6, 42, 60, and 126 months(mean 58 months). For one eye this informationwas not available. However, the exact timebetween IOL implantation and the developmentof a disciform scar could not be retrieved. Themean age of the patients with a disciform reac-tion at the time of enucleation was 83 years.The differences between the IOL and the
control group for geographic atrophy and sub-retinal neovascularisation were not statisticallysignificant. None of these changes exhibited asignificant correlation with the length of timebetween implantation of the IOL and death.The signed ranks test revealed no significant
difference in age-related changes or degenerationof the macula befween the eyes of pairs consist-ing of one pseudophakic and one phakic eye.No significant differences in histological
macular changes could be found between eyesfor pairs of pseudophakic eyes, even when theeyes with an IOL implant for the longest periodof time were compared with the fellow eye withan implant ofshorter duration (mean time differ-ence 28 months, range 6 to 78 months).No significant differences in histological
macular changes were found between the 16pairs of pseudophakic and their fellow phakiceyes.
In 43% of pseudophakic eyes the IOL had anultraviolet filter, whereas 41% ofeyes received anIOL without an ultraviolet filter. The anteriorsegment of the remaining 16% was not availablefor measurement of ultraviolet light transmit-tance. Ultraviolet filtering chromophoresblocked nearly all light with a wavelength shorterthan 400 nm, thus including the absorption ofultraviolet B (290-320 nm), ultraviolet Al (320-340 nm), and ultraviolet A2 (340-400 nm), butletting violet and blue light (400-500 nm)through. The cornea absorbed all light with awavelength shorter than 310 un. The biologicallens of the 6-year-old child had a sharp absorp-tion threshold at 390 nm in contrast with agedlenses, which had a sloping absorption curve,starting at 600 un and decreasing to a nearly totalblock at 500 nm.No significant differences in macular aging or
degenerative changes were found betweenpseudophakic eyes with or without an ultraviolet
Table 2 Prevalence ofhistological macular degeneration in61 unpaired eyes with an intraocular lens (IOL) and 126phakic eyes ofthe age-matched control group
Geographic Subretinal Disciformantophy neovascularisation scar
IOL group (%) 4(7) 5 (8) 5 (8)*Control group (%) 7 (6) 4 (3) 0 (0)*
*Fishers's exact test, p=0 007.
443
on 4 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.6.441 on 1 June 1994. D
ownloaded from

van derSchaft, Mooy, Bruijn, Mulder, Pameyer, dejong
filter., nor between pseudophakic eyes after intra-or extracapsular cataract extraction. Of the fiveeyes with a disciform scar, three IOLs had anultraviolet filter. In four of the five pseudophakiceyes with a disciform scar the IOLs wereimplanted after extracapsular cataract extrac-tion. No statistically significant differences werefound between pseudophakic eyes with brown orblue irises.
DiscussionIn this study we found a significantly higherprevalence of histological disciform maculardegeneration after cataract extraction and subse-quent implantation of an IOL than for an age-matched control group of phakic eyes. This isfurther reinforced by the observation of subse-quent disciform macular degeneration in one ofthe seven pseudophakic eyes that were excludedfrom the series because of a lack of informationabout age. It is assumed that the longer a lens isin situ, the longer free radicals can be formed inthe eye by photic energy, a process which candamage the retina.'3 However, there was nosignificant correlation between the period oftimebetween IOL implantation and death and thehistological degree of aging or degeneration ofthe macula. The absence of ultraviolet blockingchromophores in the IOLs was not associatedwith an increase in macular aging or degenera-tion. There was no significant correlationbetween iris colour and macular aging. There-fore our findings do not support the assumedincrease in both the formation of free radicalsand macular aging or degeneration.The results of several studies on the preval-
ence of cataract andARMD are rather contradic-tory. Some authors think that the developmentof a cataract protects the eye from harmfulultraviolet light which might stimulate thedevelopment ofARMD.1 " Others conclude thatcataract and ARMD are age-related changeswhich develop simultaneously in the sameperson. 16 The results of another study indicate adirect correlation between ARMD and corticalcataract and an inverse correlation betweenARMD and nuclear cataract.7 Aphakic eyesexhibited a twofold increase in the prevalence ofARMD with respect to phakic eyes without lensopacities.'Our own results suggest that the incidence of
disciform macular degeneration is higher aftercataract extraction with an IOL implant thanwould be expected for a normal population.However, we must keep in mind that a few celllayers of fibrocytes, considered to be the begin-ning of a disciform scar, can only be seen by thepathologist and not by the ophthalmologist withbiomicroscopy. Clinically a disciform scar is firstvisible when it comprises five or six cell layers.'7Therefore clinical data on disciform maculardegeneration might represent an underestima-tion compared with our histological data. In theFood and Drug Administration (FDA) report onintraocular lenses, postoperative maculardegeneration was not considered as an adversereaction but as a confounder and these eyes(number not mentioned) were excluded from theresults.28
For the development of disciform maculardegeneration there must be an ingrowth of newvessels, originating from the choriocapillaris,into the sub-RPE space. Normally Bruch'smembrane forms a firm continuous mechanicalbarrier between the- choriocapillaris and theRPE. Thus a pathway through Bruch's mem-brane must be created.One possibility is that the surgical trauma
causes ruptures in Bruch's membrane, which isknown to be more fragile when thickened andcalcified. 16 The subsequent passage of newvessels from the choroid into the sub-RPE spaceis followed by exudation of serous fluid orhaemorrhage and the formation of a disciformscar. In the four eyes with a disciform scar,Bruch's membrane was not more calcified thanin either the other pseudophakic or the controleyes. In the fifth eye Bruch's membrane wasmarkedly calcified, like an eggshell, andexhibited many breaks. If we assume thatcalcification is the main indicator for fragility ofBruch's membrane, our findings do not confirmthe hypothesis that breaks in a calcified Bruch'smembrane are the main cause of postoperativesubretinal neovascularisation, but it can be oneof the causes.A second explanation might be that macro-
phages, coming from the choroid, create a path-way for neovascularisation by breaking down thelayers of Bruch's membrane. Usually the thick-ness of Bruch's membrane increases with age,26but in our study Bruch's membrane in threemaculae with a disciform scar was abnormallythin and sometimes even showed breaks, whichwere covered by the scar tissue. Adjacent to thesebreaks, at the side of the choriocapillaris,histiocytic cells were seen in two of these eyes.Others reported that after experimental lasercoagulation of the retina, Bruch's membranefirst remained intact.29 However, macrophageswere attracted, probably by released chemotacticfactors, and created gaps in Bruch's membraneafter several days or weeks.29 Macrophages canalso induce angiogenesis.3" This laser inducedchemoattraction of macrophages might besimilar to the mechanism in eyes with an IOL, inwhich cataract extraction or more generally thesurgical trauma acted as the initiating factor forrelease of chemotactic factors that attract macro-phages.A third explanation is based on the differ-
ences, seen in Table 2, in subretinal neovascu-larisation between the control group of normalphakic eyes (3%) and the IOL group (8%). It iswell known that these new vessels easily leak orbleed, even under physiological conditions.'7During surgery several non-physiological condi-tions occur, such as the rise in orbital pressureduring peribulbar anaesthesia, the drop in intra-ocular pressure after incision, and mechanicalforces arising from manipulation of the eye,irrigation, and aspiration of lens material, andnowadays the highly energetic ultrasound wavesused for phacoemulsification. All of thesenon-physiological conditions might weaken pre-existing new vessels or provoke further out-growth or haemorrhage and thus subsequentdisciform reaction.
Other possibilities are the infiltration of
444
on 4 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.6.441 on 1 June 1994. D
ownloaded from

Increased prevalence ofdisciform macular degeneration after cataract extraction with implantation ofan intraocular lens
Bruch's membrane by endothelial cells and peri-cytes of the choriocapillaris without pre-existingbreaks.20 Even the infiltration of Bruch's mem-brane by single RPE cells has been reported.3'The importance of the latter two possibilities isunknown.The prevalence of large confluent soft drusen,
clinically often associated with neovascularisa-tion, in the IOL group was similar to that in thecontrol group so it is unlikely that soft drusen areresponsible for the difference in the prevalenceof disciform reactions.22 24The higher prevalence of hard drusen in
pseudophakic eyes compared with phakic eyescould not be explained. However, the presenceof hard drusen is not correlated with serious lossof vision' or with the development of a disciformreaction,2' 22 and a causal relation is thusunlikely.
There was no significant relation between thepresence of cataract and the development of age-related changes in the macula. Thus there was noindication that protection of the retina againstultraviolet light by the cataractous lens in theyears before cataract extraction had preventedaging or other degenerative changes in themacula.The best reference for assessment of the
changes in a pseudophakic eye after age-relatedcataract surgery is the non-operated phakicfellow eye, because the only difference betweenthe fellow eye and the pseudophakic eye is thecataract extraction with implantation of an IOLand the resulting change in conditions. Nodifferences were found between these twogroups of eyes. However, the number of pairswas relatively small so that no valid conclusionscan be drawn from this finding.We can conclude that in this study increased
prevalences of histological disciform maculardegeneration and hard drusen were found aftercataract extraction with implantation of an IOL.The exact cause remains unclear, but a directrelation between either an increase in ultravioletlight on the retina caused by IOLs withoutultraviolet filter or the duration of the increasedamount of ultraviolet light could not be demon-strated. As far as the disciform scars are con-cerned it seems more likely that either theharmful effects of surgical trauma on Bruch'smembrane or pre-existing sub-RPE vessels orthe attraction of macrophages, which breakdown Bruch's membrane and stimulate neo-vascular membrane formation, plays animportant role. Further research is necessary todiscover any predictable risk factors or causesthat can be avoided.Presented in part at the annual meeting of the Association forResearch in Vision and Ophthalmology (ARVO), Sarasota,Florida, USA, 7 May 1992 and at the 18th meeting of the ClubJules Gonin, Vienna, Austria, 8 September 1992.The authors certify that they have no affiliation with or financial
involvement in any organisation or entity with a direct financialinterest in the subject matter or materials discussed in themanuscript.
We thank Eurotransplant Foundation, Leiden, the cornea bankof the Netherlands Ophthalmic Research Institute, Amsterdam,and the Eye Hospital Rotterdam for providing most of the eyes.
1 Leibowitz HM, Krueger DE, Maunder LR, Milton RC, KiniMM, Kahn HA, et al. Framingham eye study monograph.Surv Ophthalmol 1980; 24 (suppl): 335-610.
2 Klein BE, Klein R. Cataracts and macular degeneration inolder Americans. Arch Ophthalmol 1982; 100: 571-3.
3 Jensen AD. Cataract PPOs. Arch Ophthalmol 1990; 108:501-2.
4 Foreman J. Federal agency to develop cataract managementguidelines by January 1991. Arch Ophthalmol 1990; 108:1391.
5 Van de Hoeve J. Senile Makuladegeneration und senileLinsentrubung. Graefes Arch Ophthalmol 1918; 98: 1-6.
6 Gjessing HGA. Gibt es einen Antagonismus zwischenCataracta senilis und Haabscher seniler MakulaVeranderungen? Acta Ophthalmol 1953; 31: 401-21.
7 Liu IY, White L, La Croix AZ. The association of age-relatedmacular degeneration and lens opacities in the aged.AmJ7 Public Health 1989; 79: 765-9.
8 Lermnan S. Ocular photoxicity. N Engl J Med 1988; 319:1475-7.
9 Rao NA, Thaete LG, Delmage JM, Sevanian A. Superoxidedismutase in ocular structures. Invest Ophthalmol Vis Sci1985; 26: 1778-81.
10 Mainster MA, Han WT, Delori FC. Potential retinal hazards.Ophthalmology 1983; 90: 927-32.
11 Young RW. Solar radiation and age-related macular degenera-tion. Surv Ophthalmol 1988; 32: 252-69.
12 Michels M, Sternberg P. Operating microscope-inducedretinal phototoxicity: pathophysiology, clinical manifesta-tions and prevention. Surv Ophthalmol 1990; 34: 237-52.
13 Taylor HR, Munoz B, West S, Bressler NM, Bressler SB,Rosenthal FS. Visible light and risk of age-related maculardegeneration. Trans Ajn Ophthalmol Soc 1990; 88: 163-73.
14 Zrenner E. Lichtindiiierte Schade am Augen. FortschrOphthalmol 1990; 87: 941-5 1.
15 Werner JS, Steele VG, PfoffDS. Loss ofhuman photoreceptorsensitivity associated with chronic exposure to ultravioletradiation. Ophthalmology 1989; %: 1552-8.
16 Green WR. Pathology of the macula. In: Spencer WH, ed.Ophthalmic pathology. 3rd ed. Philadelphia: Saunders,1985; 2: 924-89, 1023.
17 Sarks SH. New vessel formation beneath the retinal pigmentepithelium in senile eyes. BrJ7 Ophthalmol 1973; 57: 951.
18 Penfold PL, Killingsworth MC, Sarks SH. An ultrastructuralstudy of the role of leucocytes and fibroblasts in thebreakdown of Bruch's membrane. AustJI Ophthalmol 1984;12:23-31.
19 Garner A. Pathology of macular degeneration in the elderly.Trans Ophthalmol Soc UK 1975; 95: 54-61.
20 Killingsworth MC, Sarks JP, Sarks SH. Macrophages relatedto Bruch's membrane in age-related macular degeneration.Eye 1990; 4: 613-21.
21 Sarks SH. Ageing and degeneration in the macular region: aclinico-pathological study. BrJr Ophthalmol 1976; 60: 324-41.
22 Green RW, McDonnel PJ, Yeo JH. Pathologic features ofsenile macular degeneration. Ophthalmology 1985; 92: 615-27.
23 SchaftTL van der, de Bruijn WC, Mooy CM, Ketelaars GAM,De Jong PTVM. Is basal laminar deposit unique for age-related macular degeneration? Arch Ophthalmol 1991; 109:420-5.
24 Sarks JP, Sarks SH, Killingsworth MC. Evolution of geo-graphic atrophy ofthe retinal pigment epithelium. Eye 1988;2: 552-77.
25 Young RW. Pathophysiology ofage-related macular degenera-tion. Surv Ophthalmol 1987; 31: 291-305.
26 Schaft TL van der, Mooy CM, de Bruiin WC, Oron FG,Mulder PGH, de Jong PTVM. Histologic features of theearly stages of age-related macular degeneration: a statisticalanalysis. Ophthalmology 1992; 99: 278-86.
27 Schaft TL van der, de Bruijn WC, Mooy CM, Ketelaars GAM,de Jong PTVM. Element analysis of the early stages of age-related macular degeneration. Arch Ophthalmol 1992; 110:389-94.
28 Stark WJ, Worthen DM, Holladay JT, Bath PE, Jacobs ME,Murray GC, et al. The FDA report on intraocular lenses.Ophthalmology 1983; 90: 311-7.
29 Pollack A, Korte GE, Weitzner AL, Henkind P. Ultra-structure of Bruch's membrane after krypton laser photo-coagulation. I Breakdown of Bruch's membrane. ArchOphthalmol 1986; 104: 1372-6.
30 Penfold PL, Provis JM, Billson FA. Age-related maculardegeneration: ultrastructural studies of the relationships ofleucocytes to angiogenesis. Graefes Arch Clin ExpOphthalmol 1987; 225: 70-6.
31 Grindle CFJ, Marshall J. Ageing changes in Bruch's mem-brane and their functional implications. Trans OphthalmolSoc UK 1978; 98: 172-5.
445
on 4 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.78.6.441 on 1 June 1994. D
ownloaded from





![Overview of Congenital, Senile and Metabolic Cataractrelated cataract [7] and metabolic cataract [8]. Congenital & Senile Cataract Cataract is a clouding of the eye’s natural lens](https://img.pdfslide.net/doc/110x75/5f361b7a353bcc123d74d127/overview-of-congenital-senile-and-metabolic-cataract-related-cataract-7-and-metabolic.jpg)






















