Embed Size (px)
Citation preview

British Journal of Ophthalmology 1995; 79: 535-540
Longitudinal study of posterior subcapsularopacities using the National Eye Institutecomputer planimetry system
Maria Louella L Lopez, Valeria Freidlin, Manuel B Datiles III
AbstractBackground-The National Eye Institute(NEI) computer planimetry system hasproved to be helpful in cross sectionalstudies by providing clinically useful areameasurements of posterior subcapsularcataracts (PSC) and other opacities fromretroillumination photographs. In thisstudy, we evaluated the worth of thissystem in detecting PSC area changesover time.Methods-Using the Neitz-Kawaracamera, retroillumination photographs ofthe PSCs of 51 eyes were obtained every 6months for an average of 25 months. ThePSCs were outlined in a masked fashionon plastic overlays. Their tracings werethen digitised on to a computer using ascanner. PSC area was determined usinga special software program. For each eye,the rate ofPSC area change was estimatedby the slope of the regression line fitted tothe follow up measurements. Cataractprogression was classified as significant ifthe slope exceeded a critical value.Results-These showed that 14 of the 51eyes had PSC progression, while 37 didnot change.Conclusion-This study suggests thesystem is useful for longitudinally moni-toring PSC area changes from retro-illumination photographs. This systemwould serve in natural history studies ofPSCs and in clinical trials of anticataractdrugs. The slope based test can play a partin longitudinal studies with irregular timeintervals and variable number of visits.(Br_J Ophthalmol 1995; 79: 535-540)
National Eye Institute,National Institutes ofHealth, Bethesda,Maryland, USAOphthalmic Geneticsand Clinical ServicesBranchM L L LopezM B Datiles III
Division ofBiometryand EpidemiologyV Freidlin
Correspondence to:Manuel B Datiles III, MD,National Eye Institute,National Institutes of Health,Building 10, Room 1ON226,10 Center Drive MSC 1860,Bethesda, MD 20892-1860,USA.
Accepted for publication10 January 1995
Natural history and therapeutic studies ofcataracts require objective, standardisedmethods for in vivo quantification of posteriorsubcapsular cataracts (PSC) and other lensopacities. In the case of PSCs, much progresshas been made towards this goal. PSC charac-teristics have been reproducibly documentedwith retroillumination photography, a tech-nique optimised by Kawara and co-workers.'Computerised analysis systems for quantifica-tion of PSCs from retroillumination photo-graphs have subsequently been devised.2-8These systems quantify cataract severity withrespect to its extent or size. Most of these soft-ware systems employ an automated thresholdto distinguish cataractous areas from clearareas. This, however, makes it difficult to dif-ferentiate PSCs from cortical opacities or other
media opacities such as vitreous and comealopacities.Among the techniques that have been
developed is the National Eye Institute (NEI)computer planimetry method.8 This methoddiffers from the others in that it contains a stepfor the tracer (usually a trained clinician) todetermine what is the cataract of interest (forexample, PSC or cortical). This is done beforemeasurements are made by the computer.Datiles and co-workers,8 who described thismethod in 1987, found that the system canprovide clinically useful measurements of PSCarea from retroillumination photographs. Inaddition to the computer planimetry analysis,our work involved designing a statisticalmethod for determining cataract progressionbeyond system measurement error. Themethod uses the slopes of the regression linesfitted to follow up measurements. In thisstudy, we determined the usefulness of theNEI computer planimetry system in a longitu-dinal study - that is, in detecting PSC areachanges over time with this new method.
Materials and methodsThirty five subjects (age range 52-84 years;mean age 68-5 years), who had idiopathic age-related cataracts with posterior subcapsularopacities in at least one eye, were studied(Table 1). There were 18 males and 17females. They were part of an intramuralresearch board approved cataract protocol atthe National Eye Institute. The tenets of theDeclaration of Helsinki were followed andinformed consent was obtained.A total of 51 eyes from 35 subjects was
included in the study (both eyes from 16subjects, right eyes from six, and left eyes from
Table 1 Summary ofpatients' characteristics, by age, sex,and type ofposterior subcapsular cataracts (PSC)
Number (%o)Features ofpatients
Age (years):65 15 (43)
>65 20 (57)Sex:Males 18 (51)Females 17 (49)
Cataract type (idiopathic age-related):Pure PSC 0 (0)Mixed:CP 2 (6)NP 9 (26)NCP 24 (68)
Total 35 (100)
CP=cortical posterior subcapsular.NP=nuclear posterior subcapsular.NCP=nuclear cortical posterior subcapsular.
535
on 20 April 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.79.6.535 on 1 June 1995. D
ownloaded from

Lopez, Friedlin, Datiles
fiig
Initial visit 0.6 years 1.1 years
1-6years 2.1 years 2-6years
GSS3.1 years 3-7 years
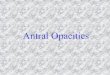
Fig lBFigure 1 (A) Serial retroillumination photographs of the posterior subcapsular cataracts(PSC) in the right eye ofsubject 16 over 3-7years. (B) Corresponding tracings of the PSCoutline (shaded area).
13). Subjects were followed up every 6 (SD 2)months for 8 to 68 (mean 25) months. Ninesubjects, however, were followed at irregularintervals because of illness, financial, or timeconstraints. Nevertheless, all subjects had abaseline and at least two follow up visits.During each visit, pupils were dilated maxi-mally with three doses each of 1% tropicamideand 255% phenylephrine hydrochloride oph-thalmic solution. While the pupils were stillmaximally dilated, retroillumination photo-graphs of the PSCs were taken using Polaroid667 film (Polaroid Corp, Cambridge, MA,USA) with a Neitz Kawara Retroilluminationcamera (Kowa Optimed Inc, Torrance, CA).The outline of the PSC was traced on a
plastic overlay (Fig 1B) by one of the authors(MBD) who was masked as to patient identityand visit date.8 For the sake of standardisation,outlining was confined to PSC found within acentral 7 mm diameter circular area of thepupil. Only the PSC that was in good focuswas outlined. Cortical opacities, dots, vac-uoles, and comeal artefacts were identified andexcluded by the outliner. The tracings werethen digitised on to a Macintosh Quadra 700using ScanMaker 600ZS (Microtek, Torrance,CA, USA). The area of the PSC outline (inmm2), was obtained using a software programdeveloped at NEI specifically for this purpose.Computer planimetry measurements werecalibrated using a retroillumination photo-graph of a millimetre scale (American OpticalMicrometer) positioned on the patient's head-rest.
In previous assessments ofPSC area,8 it wasfound that measurement error grew with thesize of the PSC. By calculating a square root ofthe PSC area, measurement error can be madeindependent of PSC size.8 We therefore usedsquare root of the PSC area for our analysis. Inthis paper, by measurement we mean thesquare root of the PSC area.There was another advantage in using the
square root of the PSC area. We were inter-ested in modelling rate of change in the followup measurements. It is natural to assume thatlinear elements of the cataract (for example,diameter) grow linearly with time (t) - thatis, proportionally to t. This implies that thearea of the cataract increases approximatelyquadratically - that is, like t2. If instead of areawe use a square root of the area, we will dealwith a linear growth which is easier to analyse.The scatter plots of follow up measurementsover time supported a linear trend of temporalchanges. This observation allowed us toreduce follow up data to least squares slopes byfitting individual regression lines to follow upmeasurements of study eyes.The following regression model was used.For eye j, j=1,. ..,5 1,Yk=Otj+Pjtjk+tjk (1)
Here Yjk is the follow up measurement for eyej at time tjk, k= 1,...,nj; aj is the intercept of thetrue regression line; and Ij is the slope of thetrue regression line. The error terms tjk areassumed independent and normally distrib-uted with mean 0 and variance independent of
536
on 20 April 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.79.6.535 on 1 June 1995. D
ownloaded from

Longitudinal study ofposterior subcapsular opacities using the National Eye Institute computer planimetry system
3.50 -
3.00-EEL-, 2-50
C.)X 2-00-,cooC.)
o 1.50-00Co1. 1.00
(7
0.50 -
0.00 -
X.Ijr
p measurementsn line (Y35=2.0+the angle formed.1 5t
3Time from first examination (years)
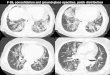
Figure 2 Plot of the follow up posterior subcapsular cataracts (PSC) area meast(expressed as area"12) in the left eye ofsubject 35 and its fitted regression line. Notb35 =0-3 greater than C35= 015 - that is, the regression line lies within the shadecorresponding to b>C35, thus indicating PSC area progression.
study eye. The intercept oj and slopeestimated by the usual leastestimators9 aj and bj, with bj giving an 4of the rate of change for eye j. The serror of bj, was calculated as9:
se(bi) t(nj 1) Var(tj)}
where &J2 is the variance of the measierror tjk; nj is the number of visits for eVar(tj) is the sample variance of timvisits for eye j. An estimate s2 of the varof measurement error was obtained ting'0 the residual mean squares s21 acrc
5'
Dni-2)sj22 =ls'
Y(nj- 2)
3.uu
Plot of follow up measurements-2.50
........ . Fitted regression line (Y16 = 0.94 + 0-02t)E250 rr Region outside the angle formed byE linesY=094+018tco
2.00g
C.500.-00
1.00 ---------.........
(1 0.50
0.00o 1 23
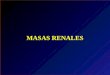
Time from first examination (years)Figure 3 Plot of the follow up posterior subcapsular cataracts (PSC) area measurements(expressed as areaI12) in the right eye of subject 16 and its fitted regression line. Note thatb16=0-02 is less than C16=0 18 - that is, the regression line lies outside the shaded regioncorresponding to b>C16, thus indicating no significant PSC area change.
Equation 2 for se(bj) shows how the standarderror of the slope decreases when the numberof visits or follow up time increases.For each eye j, PSC area change was
examined using the slope bj and its standarderror se(bj). We tested the null hypothesis thatthe slope bj was not different from zero at 5%level. If the absolute value of the slope bjexceeded the critical value Cj=1 96se(bj) thenull hypothesis of zero slope was rejected and achange (progression or regression) of the PSCarea beyond measurement error was said tohave occurred. If the absolute value of the
| slope bj was less than or equal to the critical0.3t) value Cj, then the rate of change in the PSCby area did not differ significantly from zero and
neither progression nor regression was said tohave occurred.
i' We compared the results of the slope basedtest with those of an earlier method described
4rements by Altman and Bland." This latter methodte that examines the difference between 1 year (or 2,d region year) measurement and the baseline. A visit
within plus or minus 2 months from 1 year (or2 years) was used for the 1 year (or 2 year)
l were measurement, respectively. To use thissquares method, the 95% error rangell 12 was esti-estimate mated for the difference between two repeat,tandard measurements - that is, the interval within
which 95% of the differences between repeatmeasurements are expected to lie. Assuming
(2) that the differences between repeat measure-ments follow a normal distribution, the 950/Oerror range is ±1 96 \2/o, where &2 is the
urement variance of the measurement error. If thebye j and difference between 1 year (or 2 year) measure-es tjk of ment and the baseline is within the 95%iance &2 error range, then no significant change hadby pool- occurred. Otherwise, a change beyond)ssj: measurement error is said to have occurred.
The list of the eyes found to have significantchange in cataract area by the slope based testwas compared with the list of the eyes with
(3) significant change by the Altman-Blandmethod.
ResultsA pooled estimate of the variance &2 ofmeasurement error was s2=009. Using thisestimate of the variance u2, we calculatedse(bj) using equation (2) for each eye j andthen compared each slope bj with its criticalvalue Cj= 1 96se(bj).To illustrate the above slope based test
graphically we also formulated it in terms ofregression lines. If l bjl>C, the regression linelies outside the angle formed by lines Yj=aj±Cit. For example, for the left eye of subject35, the slope b35=03, the standard error ofthe slope se (b35)=0078 and the critical valueC35=1*96XO-078=015. Figure 2 showsregression line Y35=20+0-3t fitted to thefollow up measurements on the left eye ofsubject 35. The shaded region is the area out-
4 side the angle formed by lines Y=2-0±015t.The slope b35=0-3 of regression line Y35exceeds the critical value C35=0-15 and theregression line Y35 lies within the shadedregion, indicating PSC area progression.
4
.:0. x
6Iz
.. Plot of follow upFitted regressiorRegion outside Ilines Y = 2.0 ± 0.
n\\.M,.`0 1 2
537
on 20 April 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.79.6.535 on 1 June 1995. D
ownloaded from

Lopez, Friedlin, Datiles
E 7-00 -
mx 6-00 -- /
4.0 000
v0-020
en o 1 2 3 5Time from first examination (years)
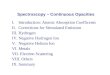
Figure 4 Temporal changes in posterior subcapsularcataracts (PSC) area (expressed as area"12) for 14 eyeswith significant PSC area progression.
Similarly, Figure 3 shows regression lineY16=094+002t fitted to the follow upmeasurements on the right eye of subject 16.The shaded region is the area outside theangle formed by lines Y16=094 ±018t. Theslope bl6=002 of regression line Y16 is lessthan the critical value C16= 0*18 and theregression line Yl6 lies outside the shadedregion, indicating a rate of progression notsignificantly different from zero.
For 14 (27%) of 51 eyes, the slope bj of theregression line exceeded the critical value,C7 -
that is, the regression line lay within the shadedregion and the null hypothesis of zero slopewas rejected. This was interpreted as a signifi-cant progression in the PSC area. Figure 4shows plots of follow up measurements forthese 14 eyes with a significant PSC area pro-gression.
For the other 37 eyes (73%), the absolutevalue of the slope did not exceed the criticalvalue C>- that is, the regression line lay outsidethe shaded region and the null hypothesis ofzero slope was not rejected. This was inter-preted as no significant change in PSC area
(Fig 5). No eye showed significant PSC area
regression.Among the 16 subjects who had both eyes
included in the study, two had progression ofthe PSC area in each eye, 11 had no area
changes, and three had progression in only oneeye. Among the 19 subjects with only one eyeincluded in the study, seven had progression oftheir PSC area and 12 had no area change(Table 2).For comparison, data were also evaluated
7.00E
m 6.00
5.00
4 004_
3.00-0
+ 2.00-0
1.00
~.o.oo
X 0 1 2 3 4 5 6Time from first examination (years)
Figure 5 Temporal changes in posterior subcapsularcataracts (PSC) area (expressed as area"12) for 37 eyeswith no significant PSC area change.
Table 2 Status ofpostenior subcapsular opacities in 51eyes during a mean follow up period of 2 1 years
Number (%)Cataract status of eyes
19 Subjects with one eye available for study 19 (100)Unchanged 12 (63)Progressed 7 (37)
16 Subjects with two eyes available for study 32 (100)Neither eye changed 25 (78)One eye progressed 3 (9)Both eyes progressed 4 (12)
using the Altman-Bland method at the 1 and 2year visits. Using this method, change beyondmeasurement error was defined as a differencebetween follow up measurement and the base-line greater than the 95°/O error range. The95% error range was calculated as ± 1 96\/_22= ±083 using the pooled estimatess2=0O09 of the variance U2 of measurementerror. Not all patients had a visit at 1 or 2 years(SD 2 months): seven eyes were excluded inthe 1 year analysis and 29 eyes were excludedin the 2 year analysis. In the 1 year analysis, sixeyes had PSC area progression and one eyehad area regression. In the 2 year analysis, sixeyes had PSC area progression and no eye hadarea regression. Only one eye showed PSCarea progression in both 1 and 2 year analyses.Of the 14 eyes with PSC area progression by
the slope based test (Table 3), 11 eyes demon-strated PSC area progression by the Altman-Bland method in either the 1 or 2 year analysis,two eyes were excluded because of lack offollow up visits at 1 and 2 years, and one eyedid not show a change in PSC area. The plot offollow up measurements for this eye (subject35, left eye) is shown in Figure 2. The differ-ence between 1 or 2 year measurement andbaseline was less than 0O83 (95% error range).Of the 37 eyes with no PSC area change by
the slope based test, one showed PSC arearegression at 1 year but no area change at 2years by the Altman-Bland method. No eyewith PSC area progression by the Altman-Bland method in either 1 or 2 year analysis wasmissed by the slope based test.
DiscussionThere has been very little information on the
Table 3 Cataract status by the Altman-Bland methodforthe 14 eyes with a significant progression by the slope basedtest
Eye Cataract status by the Altman-Bland method(left orright) 1 Year visit 2 Year visit Summary
R -* /t /R - / IR / Excludedt /R Excluded / /R / Excluded /R / Excluded /R _ Excluded /R Ecd EL Excluded Excluded ExcludedL Excluded Excluded ExcludedL J Excluded /L - / I
L - _ _
*-=No change by Altman-Bland method.t/ =Cataract progression by the Altman-Bland method.t=Excluded owing to lack of visit within 2 months from 2 years.
538
on 20 April 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.79.6.535 on 1 June 1995. D
ownloaded from

Longitudinal study ofposterior subcapsular opacities using the National Eye Institute computer planimetry system
natural history of cataracts, primarily becauseof the difficulty in standardising methods usedin documenting and quantifying them. Thisstudy serves to demonstrate a new system forlongitudinally followed PSCs using retro-illumination photographs analysed with com-puter planimetry and a slope based test. Anadvantage of using computer planimetry is theability to separate PSCs from cortical, as wellas separating out corneal or vitreous opacities.This allows completely regionally independentmonitoring of lens opacities. This is particu-larly important in PSCs of specific aetiologies(such as those associated with steroid intake,radiation exposure, retinitis pigmentosa, andgyrate atrophy) which may coexist with otherlens opacities not due to the same aetiology.Any specific therapy aimed at the aetiologicalmechanism will require monitoring only of thePSC involved.A statistical method was developed for
monitoring cataract progression in a longi-tudinal study with staggered entry andunequally timed visits. Unbalanced data ofthis kind is fairly common for studies ofelderly patients who may be prone to multiplesystemic illnesses during long term follow upand thus may have trouble in keeping theirclinic appointments. In this method, the slopeof the regression line was used as an estimateof rate of change ofPSC area. A hypothesis ofzero rate of change was tested individuallyfor each eye taking into account the numberof visits and time span of follow up for thiseye.
Since we were mainly interested in evaluat-ing the utility of the system, cataract progres-sion was evaluated per eye rather than perperson. Values obtained for PSC progressionin this study should therefore not be miscon-strued as representative of PSC progression ina population. They may, however, be usefulin estimating sample size requirements forclinical trials of anticataract drugs.
Comparison of the slope based test with theAltman-Bland method showed the formermethod to have a higher yield in detecting PSCarea changes. This is because the slope isobtained from all observations by smoothingfluctuations and it is less sensitive to measure-ment error. The Altman-Bland method, on theother hand, is more sensitive to fluctuations infollow up measurements because, in a sense, itestimates the slope from only two measure-ments. Only one eye demonstrated PSC areaprogression in both 1 and 2 year analyses. Forone eye a regression in PSC area was indicatedby the 1 year analysis because of a single lowmeasurement while the slope based test did notindicate a change.Some comments about the possible sources
of error are worthy of note. The quality ofretroillumination photographs may contributeto the irregular or jagged progression pattern(see Figs 4 and 5) in some eyes. Review of theretroillumination photographs of these eyesand their corresponding tracings showed thatsome photographs were slightly out of focus,overexposed, or underexposed (see Fig 1A).Some were taken with the eyes fixating
incorrectly. At times, these photographic diffi-culties were hard to avoid since the patients areelderly, and easily get tired or distracted. Thesevariations affected the visibility of the PSCedge, leading to differences in the outlinedareas. However, as pointed out by Shun-Shinet al,13 the irregular progression pattern canalso be due to the fact that the surface areas ofposterior subcapsular cataracts may decreasein time and may not necessarily be due tothe quality of retroillumination photograph.However, this variability was smoothed by theleast squares slope. In this study, we measuredthe PSC area from retroillumination photo-graphs of at least three clinic visits to obtain amore realistic trend of PSC growth. Anotherobservation was the usefulness of a 7 mmartificial pupil as a standard for pupil size.Despite using exactly the same regimen anddosage of mydriatic eye drops on all patients,the pupil size varied from visit to visit (pupil-lary diameter: mean 7-88 (067) mm; range6&25-1017 mm). This problem was overcomeby utilising the standard 7 mm diameterartificial pupil. We chose 7 mm as the standardpupillary diameter since 95% of the retro-illumination photographs (245 of 258photographs) had a pupil at least 7 mm indiameter. Thirteen pupils did not dilate to7 mm. The mean for these was 6-64 mm(range 6-25-6-92 mm).
Variables encountered in this study haveraised the need to streamline a system for longterm follow up of cataracts. Specifically, wehave demonstrated the value of a semi-automated system to replace most of themanual steps involved. This includes imageacquisition, image segmentation, and the useof software to analyse a region of interest fordensitometry.A subject not assessed in this paper is the
density ofPSC cataracts. Owing to the natureof the retroillumination technique, the densityof opacities in the photographs vary widelydep.ending on how much light is reflectedfrom the optic disc and/or retinal surface,making background illumination very variablefrom photograph to photograph. This isspecially true of retroillumination photo-graphs taken with the Kowa camera which weused in this study. Recent developments suchas the use of fixation targets and videoimaging as well as development of softwareto perform background subtraction andthreshold segmentation will help address thisproblem.14 15
Other areas which should be explored arethe need to develop ways to describe thecentrality of any opacity since more centrallylocated opacities may give rise to earlier distur-bances in visual function (versus peripherallylocated ones). Development of computerisedanalysis methods could help in the outlining ofaffected areas (in conjunction with the abovementioned background subtraction andthreshold segmentation) which can be thenrefined by a human tracer only when needed.The contribution of any nuclear opalescencemust also be studied to allow for changes in thenuclear area as they affect the retroillumination
539
on 20 April 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.79.6.535 on 1 June 1995. D
ownloaded from

Lopez, Friedlin, Datiles
image especially during longitudinal monitor-ing of PSC cataract.
ConclusionsThe NEI computer planimetry system is anobjective and relatively easy method ofestimating PSC area from retroilluminationphotographs. It is useful for cross sectionalstudies as shown previously8 and for monitor-ing progression or regression of PSCs as wasdemonstrated in this study. The system maythus be of value in natural history studies ofdifferent aetiological types ofPSCs, was well asin clinical trials of anticataract drugs. Theslope based test for monitoring PSC areachanges can serve in longitudinal studies withdata of varying frequency and time.
1 Kawara T, Obazawa H. A new method for retroilluminationphotography of cataractous lens opacities. Am JOphthalmol 1980; 90: 186-9.
2 Kawara T, Obazawa H, Nakano R, Sasaki M, Sakata T.Quantitative evaluation of cataractous lens opacities withretroillumination photography. Vpnm Clin Ophthalmol(Rinsho Ganka) 1979; 33: 21-6.
3 WolfeJK, ChylackLTJr. Objective measurement of corticaland subcapsular opacification in retroillumination photo-graphs. Ophthalmic Res 1990; 22 (suppl 1): 62-7.
4 Miyauchi A, Mukai S, Sakamoto Y. A new analysis methodfor cataractous images taken by retroillumination photo-graphy. Ophthalmic Res 1990; 22 (suppl 1): 74-7.
5 Khu PM, Kashiwagi T. Subjective (LOCS II) versusobjective (BGS) measures of cortical and subcapsularcataracts in retroillumination photographs. OphthalmicRes 1990; 22 (suppl 1); 68-70.
6 Sparrow JM, Brown NAP, Shun-Shin GA, Bron AJ. TheOxford modular cataract image analysis system. Eye 1990;4: 638-48.
7 Sasali K, Sakamoto Y, Shibata T, Emori Y. The multi-purpose camera: a new anterior eye segment analysissystem. Ophthalmic Res 1990; 22 (suppl 1): 3-8.
8 Datiles MB III, Podgor MJ, Sperduto RD, Kashima K,Edwards P, Hiller R. Measurement error in assessing thesize of posterior subcapsular cataracts from retroillumina-tion photographs. Invest Ophthalmol Vis Sci 1989; 30:1848-54.
9 Rosner B. Fundamentals of biostatistics. Boston: DuburyPress, 1986.
10 Palta M, Cook T. Some considerations in the analysis ofrates of changes in longitudinal studies. Stat Med 1987; 6:599-611.
11 Altman DG, Bland JM. Measurement in medicine: theanalysis of method comparison studies. Statistician 1983;32: 307-17.
12 Magno BV, Friedlin V, Datiles MB III. Reproducibility ofthe NEI scheimpflug cataract imaging system. InvestOphthalmol Vis SCi 1994; 35: 3078-84.
13 Shun-Shin GA, Brown NAP, Bron AJ, Sparrow JM. Thedynamic nature of posterior subcapsular cataract. Br JOphthalmol 1989; 73: 522-7.
14 Harris ML, Hanna KJ, Shun-Shin GA, Holden R, BrownNAP. Verification of a new method for the analysis ofretro-illumination photographs for use in longitudinalstudies of cataract. Eye 1993; 7: 572-7.
15 Harris ML, Brown NAP, Bron AJ. Application of chargecouple device Scheimpflug and retroillumination camerasto lens toxicity monitoring in man. Ophthalmic Res 1994;26 (suppl 1): 44-7.
540
on 20 April 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.79.6.535 on 1 June 1995. D
ownloaded from














![Subcapsular left hepatic lobe hematoma: A potentially life ......post-ERCP complication such as subcapsular hepatic hematoma was firstly described in 2000 [4]. Although it is rare](https://img.pdfslide.net/doc/110x75/5e62d63efcce8b4b4b73030e/subcapsular-left-hepatic-lobe-hematoma-a-potentially-life-post-ercp-complication.jpg)