Embed Size (px)
Citation preview

CD34 Selection as a Stem Cell Purging Strategy for Neuroblastoma:Preclinical and Clinical Studies
John Donovan,1 Jennifer Temel,1 Amy Zuckerman,1 John Gribben,1
Junjie Fang,2 Giuliana Pierson,2 Amy Ross,4 Lisa Diller,3 andStephan A. Grupp2*
Background. The suitability of CD34 selec-tion for purging peripheral blood progenitorcells (PBPC) collected from patients with neu-roblastoma (NB) has been called into question,largely because of reports of detection of lowlevels of CD34 on the surface of some NB celllines and tumors. Procedure. We used threeapproaches to address the issue of purging ofNB from stem cell specimens and possible la-beling of NB: 1) Flow cytometric detection ofCD34 on NB cell lines. We assessed CD34 ex-pression using a panel of anti-CD34 monoclo-nal antibodies (MoAbs) including 9C5, 12.8,and QBend10 and showed no increase in la-beling over secondary-only control. 2) Spikingexperiments with the Isolex 50 system. NB celllines were used to contaminate aliquots ofPBPC collections, after which the productswere purified using the Isolex 50. Purging of NBwas assessed by quantitative multiplex RT-PCR(TaqMan system) using a tumor-specific tran-script, GAGE. We demonstrated >2 logs of tu-
mor cell depletion from these specimens. 3)Analysis of clinical specimens. PBPC pre- andpost-CD34 selection were analyzed from pa-tients treated on the CHP-594 transplant trial.Results. In nine specimens selected using theCeprate LC CD34 selection system where tu-mor was detectable by immunocytochemistrypreselection, we observed >2.4 to >4.6 logs ofNB purging after selection. We then analyzed23 aliquots of PBPC infused into patients post-CD34 selection and compared them to theproduct preselection; 20/23 specimens showeddepletion of NB, although some level of GAGEmessage was observed in most post-CD34 se-lection specimens. Conclusion. These datashow that purging of NB from PBPC specimensusing CD34 selection is feasible, yielding in-fused products that are negative at the level ofICC but often positive at the level of RT-PCR.Med. Pediatr. Oncol. 35:677–682, 2000.© 2000 Wiley-Liss, Inc.
Key words: pediatric; CD34 selection; stem cell transplant; neuroblastoma
INTRODUCTION
High-dose chemotherapy with stem cell rescue hasbeen shown to improve outcome in patients with high-risk neuroblastoma (NB) [1]. One of the potential limi-tations of this approach is the possibility that tumor cellsmay contaminate the stem cell product. Although noclinical trial in autologous transplantation has shown asurvival advantage for patients who received stem cellproducts purged of tumor cells, there is indirect evidencethat tumor purging of stem cell products may improveoutcome in NB. Gene-marked tumor cells infused withautologous marrow have been found at sites of relapse,suggesting that NB inadvertently collected with autolo-gous marrow can be clonogenic [2]. In other diseases,such as lymphoma, patients who receive stem cells inwhich tumor cannot be detected have a better outcome[3], but whether this phenomenon is due to fewer tumorcells in the stem cell product used to support the therapyor more successful treatment of the disease in the patientis unclear.
A variety of disease or even patient-specific tech-niques to purge stem cell products of tumor have beendeveloped, depending on recognition of tumor cells to
remove them from the product (called negative selec-tion). Another, more general approach has been termedpositive selection, in which stem and progenitor cellsrequired for both rapid and durable engraftment are pu-
Abbreviations: FITC, fluorescein isothiocyanate; HDT, high-dosetherapy; ICC, immunocytochemistry; MoAbs, monoclonal antibodies;PBPC, peripheral blood progenitor cell; PE, phycoerythrin; RT-PCR,reverse transcriptase-polymerase chain reaction.1Department of Adult Oncology, Dana-Farber Cancer Institute, Bos-ton, Massachusetts2Department of Pediatrics, Division of Oncology, Children’s Hospitalof Philadelphia, University of Pennsylvania, School of Medicine,Philadelphia, Pennsylvania3Department of Pediatric Oncology, Dana-Farber Cancer Institute andDepartment of Medicine, Children’s Hospital, Boston, Massachusetts4Diagnostics Division, Nexell Therapeutics, Inc. Irvine, California
Grant sponsors: the University of Pennsylvania Cancer Center, theBenacerraf/Frei Clinical Investigator Award, Dana-Farber Cancer In-stitute, the Fiftieth Anniversary Program for Scholars in Medicine,Harvard Medical School.
*Correspondence to: Stephan Grupp, M.D. Ph.D., Children’s Hospitalof Philadelphia, 3516 Civic Center Blvd., Abramson 902, Philadel-phia, PA 19104. E-mail: [email protected].
Medical and Pediatric Oncology 35:677–682 (2000)
© 2000 Wiley-Liss, Inc.

rified from the stem cell product. The principal methodused for positive selection is selection for the antigenCD34, which is expressed on hematopoietic stem andprogenitor cells. CD34 selection devices select for andpurify CD34+ cells [4], yielding 2–3 log depletion ofCD34-cells, including possible contaminating tumorcells [5]. This method is appropriate for purging of tumortypes which do not express CD34 (including most solidtumors), but not for malignancies which may expressCD34 (such as leukemias). CD34 selection has been usedto purge stem cell products in patients with neuroblas-toma, but concerns have been raised that some NB cellsor cell lines may express CD34 or cross-react withMoAbs that recognize CD34 [6,7]. In order to furthercharacterize the potential utility of CD34 selection inNB, in these studies we examine the issue of CD34 ex-pression on NB and demonstrate tumor cell depletion ofboth NB cell lines and NB contaminating patient periph-eral blood progenitor cell (PBPC) specimens.
MATERIALS AND METHODSPBPC Sources
PBPC used in these studies were obtained from one ofthree sources. Clinical specimens were obtained after in-formed consent from patients enrolled on the Children’sHospital of Philadelphia / Dana Farber Cancer Institutestudy of tandem PBPC transplant for high risk NB (en-titled CHP-594 or 94-131 at the respective institutions).Patients were eligible for this study if they were over 1year of age with INSS Stage 48 disease or INSS Stage 3with MYCNamplification. PBPC specimens from normalvolunteer donors were provided by Nexell (Irvine, CA).For some of the preclinical studies, we utilized PBPCsamples collected from patients who did not subse-quently undergo transplantation, again after informedconsent. Protocols and consent forms were approved byeach participating hospital’s institutional review boardand informed consent was obtained from the parents ofeach child after the diagnosis was confirmed.
PBPC Collections
Patients typically underwent their PBPC collection af-ter the third cycle of induction chemotherapy [9]. Prod-ucts intended for use were collected with a goal of 4 ×106/kg CD34+ cells (minimum of 1 × 106/kg) availablefor each cycle of HDT/SCR. After cryopreservation of analiquot of unselected PBPC as a backup, the first day’scollection was held overnight and pooled with the secondday’s collection. Then, both pheresis products underwentCD34+ selection using the Ceprate SC device (CellPro,Bothell, WA) or the Isolex 300i device (Nexell). Samplesto assess for neuroblastoma contamination were cryopre-served from both the input and the selected populations.
Immunocytochemical Detection of NB
Clinical samples of blood and bone marrow were ana-lyzed by standard ICC at BIS Laboratories (Reseda, CA)using a cocktail of three antibodies specific for neuro-blastoma as previously described [10]. Aliquots fromdaily PBPC collections also underwent high-sensitivityICC analysis in studies to quantify tumor depletion andhas been described elsewhere [9]. Briefly, an aliquot ofpheresate was CD34 selected using the Ceprate LC labo-ratory CD34 selection column (CellPro). Both pre- andpostselection fractions were analyzed for NB by ICC ina slide-based assay using a cocktail of four antibodieswhich recognize NB cells (181.4, ERIC-1, UJ13A, and5.1H1111). Cell seeding experiments with the NB cellline CCL-127 have shown that this investigational ICCassay has a sensitivity of 10−5 to 10−6 (data not shown).The positive control CCL-127 line, negative control, pre-and postselection specimens were independently inter-preted by two investigators.
RT-PCR Detection of NB
RNA was isolated using RNA-STAT-60 (Tel-Test,Friendswood, TX) according to manufacturer’s recom-mendations. 2mg total RNA was reversed transcribedwith Superscript II reverse transcriptase (Gibco-BRL,Gaithersburg, MD) and oligo dT primers (PE Biosys-tems, Foster City, CA). TaqMan PCR using GAGE andtyrosine hydroxylase specific primers and probes wasperformed in multiplex with primers and probes forGAPDH on an ABI PRISM 7700 sequence detector. The50 ml quantification reactions contained 2ml cDNA(10% of RT reaction), 5ml 10X TaqMan Buffer A (500mM KCl, 100 mM Tris-HCl, pH 8.3; PE Biosystems), 5ml 25 mM MgCl2, 200 mM of each of dATP, dCTP,dTTP, dGTP, 1.25 U Platinum Taq DNA polymerase(Gibco BRL), and 100 nM TaqMan probe (PE Biosys-tems). Primer concentrations were optimized for multi-plex PCR. Standard curves for quantification were pro-duced by 10-fold serial dilution of plasmids containingGAGE, tyrosine hydroxylase, and GAPDH cDNAs.
Flow Cytometry
A panel of NB cell lines was used for these studies,including CHLA-90 and SK-N-RA (kind gift of Dr. P.Reynolds), IMR-5, SY5Y, CHP134, and NLF (kind giftof Dr. A. Evans). The CD34+ cell KG-1a was used as aCD34+ control. Anti-CD34 monoclonal antibodies(MoAbs) included biotin-12.8 (CellPro), 9C5 (Nexell),QBend10 (Miltenyi, Auburn, CA), HPCA-1 andHPCA-2 (Becton-Dickinson, San Diego, CA). A positivecontrol for NB staining was provided by MoAb UJ13A(kind gift of Dr. J. Kemshead). These antibodies weredetected with phycoerythrin (PE)-streptavidin (in thecase of biotin-12.8) or PE- or fluorescein isothiocyanate
678 Donovan et al.
(FITC)-labeled affinity purified goat antimouse IgG(Jackson Immunoresearch, Grove, PA). For staining,0.3mg (UJ13A), 1 mg (CD34 MoAbs), or 20mL(HPCA-1 and HPCA-2) of the primary antibody wasadded to 2 × 106 cells for 20 min at 4°C, followed bywashing and a further incubation with 4mg of secondarylabel. Flow cytometry was performed on the FACS Cali-bur or the FACS Scan (Becton-Dickinson). Secondary-only control was performed for each cell line and fluo-rochrome.
RESULTSDetection of CD34 on NB Cell Lines
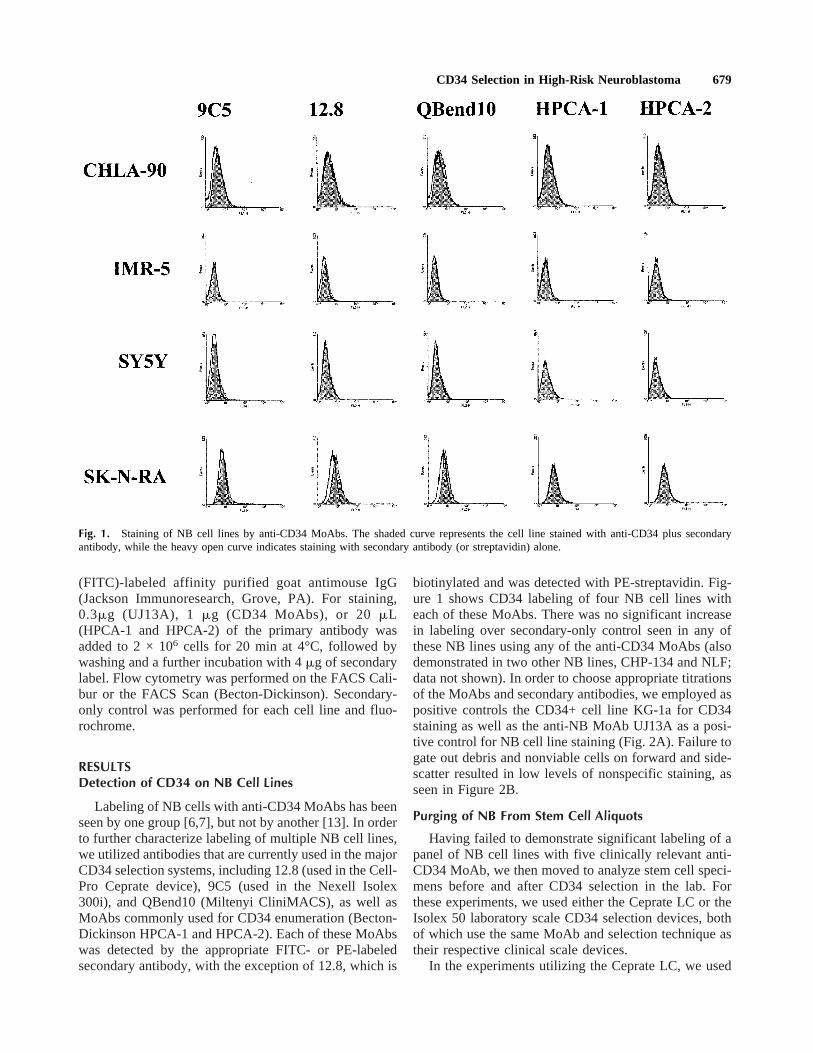
Labeling of NB cells with anti-CD34 MoAbs has beenseen by one group [6,7], but not by another [13]. In orderto further characterize labeling of multiple NB cell lines,we utilized antibodies that are currently used in the majorCD34 selection systems, including 12.8 (used in the Cell-Pro Ceprate device), 9C5 (used in the Nexell Isolex300i), and QBend10 (Miltenyi CliniMACS), as well asMoAbs commonly used for CD34 enumeration (Becton-Dickinson HPCA-1 and HPCA-2). Each of these MoAbswas detected by the appropriate FITC- or PE-labeledsecondary antibody, with the exception of 12.8, which is
biotinylated and was detected with PE-streptavidin. Fig-ure 1 shows CD34 labeling of four NB cell lines witheach of these MoAbs. There was no significant increasein labeling over secondary-only control seen in any ofthese NB lines using any of the anti-CD34 MoAbs (alsodemonstrated in two other NB lines, CHP-134 and NLF;data not shown). In order to choose appropriate titrationsof the MoAbs and secondary antibodies, we employed aspositive controls the CD34+ cell line KG-1a for CD34staining as well as the anti-NB MoAb UJ13A as a posi-tive control for NB cell line staining (Fig. 2A). Failure togate out debris and nonviable cells on forward and side-scatter resulted in low levels of nonspecific staining, asseen in Figure 2B.
Purging of NB From Stem Cell Aliquots
Having failed to demonstrate significant labeling of apanel of NB cell lines with five clinically relevant anti-CD34 MoAb, we then moved to analyze stem cell speci-mens before and after CD34 selection in the lab. Forthese experiments, we used either the Ceprate LC or theIsolex 50 laboratory scale CD34 selection devices, bothof which use the same MoAb and selection technique astheir respective clinical scale devices.
In the experiments utilizing the Ceprate LC, we used
Fig. 1. Staining of NB cell lines by anti-CD34 MoAbs. The shaded curve represents the cell line stained with anti-CD34 plus secondaryantibody, while the heavy open curve indicates staining with secondary antibody (or streptavidin) alone.
CD34 Selection in High-Risk Neuroblastoma 679

aliquots of clinical PBPC specimens collected from pa-tients with NB on the tandem transplant trial (see Mate-rials and Methods). These data have been published else-where [9] and are summarized here. A minimum of 2.25× 106 cells from each of 30 PBPC aliquots were assessedby high-sensitivity immunocytochemistry (ICC). Thistechnique has previously been shown to have a sensitiv-ity of NB detection in PBPC between 10−5 and 10−6 (datanot shown). These aliquots, containing a minimum of 108
cells, were then CD34 selected on the Ceprate LC andagain analyzed by ICC. 1–2 × 106 CD34 selected cellswere analyzed for each aliquot. Nine of 30 PBPC speci-mens had detectable NB prior to CD34 selection, rangingfrom 2.7 to 367 NB cells/106 PBPC, while no tumor wasdetected in the remaining 21 aliquots. After CD34 selec-tion, all of the 21 NB-negative aliquots were still nega-tive. Of the nine specimens with detectable tumor, sixwere negative by ICC after CD34 selection. The remain-ing three had 0.8–4 NB cells/106 PBPC detected. Assum-ing 1% of total input cells were recovered after CD34selection (typical for these specimens and the CeprateLC), tumor cell depletion in the specimens where tumorwas detectable was between >2.5 to >4 logs.
In further experiments examining the Isolex technol-ogy, we used PBPC aliquots from both patients and nor-mal donors. 2–5 × 108 PBPC were contaminated with0.5–2% NB cells from either the IMR-5, CHLA-90, orSK-N-RA cell lines. The PBPC were then CD34 selectedon the Isolex 50. For tumor detection in these experi-ments, we used quantitative RT-PCR utilizing probe-primers recognizing GAGE family members [12] in theTaqMan system (PE Biosystems). GAGE detection dem-onstrated a sensitivity of approximately 10−5, while de-tection of tyrosine hydroxylase message was consider-ably less sensitive in this quantitative system (data notshown). In a total of 12 purifications performed on theIsolex 50, depletion of tumor was seen in each case; 8/12postselection samples were negative by RT-PCR forGAGE message. Mean tumor cell depletion (again, ad-justed for cell number) was >4.6 logs (Fig. 3).
NB Purging From Infused Products
The majority of the patients treated on the tandemtransplant protocol received CD34-selected PBPC insupport of tandem courses of high-dose chemotherapy[9].
Fig. 2. Cytometric controls.The leftmost profile inA showsthe NB cell line IMR-5 unstained.Positive staining of NB cells isdemonstrated with the anti-NBMoAb UJ13A as well as positivelabeling of the CD34+ cell lineKG-1a with 9C5. Both stains uti-lize the same antibody titrationand goat antimouse secondary an-tibody as in Figure 1.B: The ef-fect of gating on labeling, show-ing the gating strategy (leftdotplot), staining of the wholecell population (right histogram)vs. gating eliminating debris andnonviable cells (middle histo-gram).
680 Donovan et al.

Prior to CD34 selection, specimens were analyzed forNB contamination using standard ICC (BIS Laborato-ries), which has been reported to have a sensitivity of10−5. Of 29 pooled PBPC collections analyzed by stan-dard ICC, tumor was detected in only one PBPC product,revealing 1 NB cell/105 PBPC. Because 107 cells arerequested for this analysis, representing a large fractionof a CD34 selected graft in a smaller patient, only fivesamples obtained after CD34 selection were assayed byICC for tumor cell contamination, and none of these werepositive.
Specimens were also cryopreserved from both thepooled PBPC product and the post-CD34 selection prod-uct. These specimens were analyzed for NB contamina-tion using the same TaqMan RT-PCR quantitation ofGAGE message described above. Twenty-seven speci-mens were analyzed in triplicate. Of these, two werepaired (pre and post) specimens from normal donors pro-cessed using the Isolex 300i device as negative controlsfor GAGE expression, 19 were patient specimens pro-cessed using the Ceprate SC device (one specimen wasrun twice; see below), and five were patient specimensselected on the Isolex 300i. The two normal donor speci-mens were negative for GAGE pre- and post-CD34 se-lection. Of the patient specimens, 6/25 were RT-PCRnegative pre- and 11/25 negative postselection. Onespecimen was negative prior to selection but then becameRT-PCR positive after Ceprate SC selection. Enoughtemplate existed in the postselection specimen to repeatthis triplicate analysis one further time, and the repeatRT-PCR was negative both pre and post (specimens 6and 7 in Fig. 4). In the 20 specimens in which tumordepletion could be estimated, the mean depletion was>2.9 logs (Fig. 4), and all but specimen 6 showed tumordepletion.
DISCUSSION
High-dose chemotherapy with stem cell rescue hascontributed to increased event-free survival in severalhigh-risk solid tumors including NB. The toxicity of thisintensive treatment modality has been decreased with thenear-universal move from bone marrow as a stem cellsource in autologous transplant to PBPC. In tumorswhich have a high likelihood of bone marrow metastasis,there is the possibility that tumor cells may be inadver-tently collected with the stem cell product. Again, thereis data to suggest that fewer tumor cells may be collectedwith PBPC than autologous marrow. The extent to whichreinfused tumor plays a clinically significant role in therisk of relapse is unknown, and no clinical study hasshown an advantage for purging tumor cells from stemcell products in patient outcome.
Negative purging strategies used to remove tumorcells from marrow may significantly delay engraftment,although much of this experience has come in collectionof compromised marrow from heavily pretreated pa-tients. In addition, negative purging strategies are depen-dent on development and, eventually, FDA approval oftumor-specific antibody “cocktails” which may be cum-bersome from a scientific and drug/device developmentstandpoint. The alternative, examined in the studies pre-sented here, is positive selection of CD34+ cells, an ap-proach which has been approved for PBPC purging bythe FDA. CD34 selection of PBPC as a purging strategyfor patients with NB has three potential advantages. Thefirst is that PBPC may have less tumor cell contamina-tion than marrow. The patients on the tandem transplantstudy had minimal contamination of the PBPC producteven prior to CD34 selection. The second advantage ofCD34+ selection is that it causes no delay in engraftment,despite a decrease in the number of stem cells infused(see Grupp et al. in this issue [19] and [5,9]).
Fig. 3. Depletion of NB cell lines from PBPC specimens using theIsolex 50 system. Minimum log depletion of tumor cells is shown asassessed by quantitative RT-PCR. Specimen numbers are listed alongthe X axis. The starred (*) bars indicate specimens that were RT-PCR-negative after purging. Log purging is estimated based on lower limitsof detection in the RT-PCR negative specimens.
Fig. 4. Tumor cell depletion by CD34 selection from infused PBPCspecimens; 21 of 27 specimens with tumor detectable by RT-PCRprior to CD34 selection are included. The remaining specimens werenegative both pre- and post-CD34 selection and cannot be assessed fordepletion. Specimen numbers are listed along the X axis. Specimens 6and 7 are repeat determinations from the same sample, with[6 nega-tive pre and positive post and[7 negative both pre and post (indicatedby **).
CD34 Selection in High-Risk Neuroblastoma 681

The third advantage of CD34+ selection of PBPC isthat positive selection of stem cells is not dependent ontumor type for depletion, as long as the tumor cells do notexpress CD34 or an epitope recognized by the anti-CD34monoclonal antibody used for selection. The extent towhich this may be observed is uncertain [6,7,13], and wedid not observe any labeling of six NB cell lines with anyof five anti-CD34 MoAb. Further, we examined thedepletion of NB from stem cell products using two majorCD34 selection technologies in an attempt to determinewhether any such labeling is clinically relevant. We findthat CD34+ selection depletes neuroblastoma cells fromPBPC, as has been shown by others [14–18].
However, although we demonstrate depletion of NBfrom clinical specimens by CD34 selection, we also findthat the majority of stem cell products infused into thesepatients in support of high-dose chemotherapy still havedetectable tumor cells by RT-PCR. The clinical rel-evance of that finding, however, is unknown. To furtherimprove on the purging results obtained by CD34 selec-tion, there is the potential to add negative selection withanti-NB MoAb to the automated CD34 selection processusing the Isolex device. Determination of the role ofCD34 selection and the impact of purging on EFS willrequire a larger clinical trial. In regard to purging, aPhase III randomized groupwide trial to be performed bythe Children’s Oncology Group has been designed tocompare outcome in patients who receive immunomag-netically purged PBPC to patients who receive unse-lected PBPC.
REFERENCES
1. Matthay KK, Villablanca JG, Seeger RC, et al. Treatment of high-risk neuroblastoma with intensive chemotherapy, radiotherapy,autologous bone marrow transplantation, and 13-cis-retinoic acid.N Engl J Med 1999;341:1165–1173.
2. Brenner M, Rill D, Moen R, et al. Gene-marking to trace origin ofrelapse after autologous bone-marrow transplantation. Lancet1993;341:85–86.
3. Freedman AS, Neuberg D, Mauch P, et al. Long-term follow-up ofautologous bone marrow transplantation in patients with relapsedfollicular lymphoma. Blood 1999;94:3325–33.
4. Civin CI, Trischmann T, Kadan NS, et al. Highly purified CD34-positive cells reconstitute hematopoiesis. J Clin Oncol 1996;14:2224–2233.
5. Shpall EJ, Jones RB, Bearman SI, et al. Transplantation of en-riched CD34-positive autologous marrow into breast cancer pa-tients following high-dose chemotherapy: influence of CD34-positive peripheral-blood progenitors and growth factors onengraftment. J Clin Oncol 1994;12:28–36.
6. Hafer R, Voigt A, Gruhn B, et al. Neuroblastoma cells can expressthe hematopoietic progenitor cell antigen CD34 as detected atsurface protein and mRNA level. J Neuroimmunol 1999;96:201–206.
7. Voigt A, Hafer R, Gruhn B, et al. Expression of CD34 and otherhaematopoietic antigens on neuroblastoma cells: consequences forautologous bone marrow and peripheral blood stem cell transplan-tation. J Neuroimmunol 1997;78:117–126.
8. Brodeur GM, Pritchard J, Berthold F, et al. Revisions of the in-ternational criteria for neuroblastoma diagnosis, staging, and re-sponse to treatment. J Clin Oncol 1993;11:1466–1477.
9. Grupp SA, Stern JW, Bunin N, et al. Tandem high dose therapy inrapid sequence for children with high-risk neuroblastoma. J ClinOncol 2000;18:2567–2575.
10. Moss TJ, Reynolds CP, Sather HN, et al. Prognostic value ofimmunocytologic detection of bone marrow metastases in neuro-blastoma. N Engl J Med 1991;324:219–226.
11. Rogers DW, Treleaven JG, Kemshead JT, et al. Monoclonal an-tibodies for detecting bone marrow invasion by neuroblastoma.J Clin Pathol 1989;42:422–426.
12. Cheung IY, Cheung N-KV. Molecular detection of GAGE expres-sion in peripheral blood and bone marrow: utility as a tumormarker for neuroblastoma. Clin Cancer Res 1997;3:821–826.
13. Greenfield D, Franklin WA, Tyson RW, et al. CD34 expression onpediatric solid tumors. Proc ASPHO, 1996.
14. Lode HN, Handgretinger R, Schuermann U, et al. Detection ofneuroblastoma cells in CD34+ selected peripheral stem cells usinga combination of tyrosine hydroxylase nested RT-PCR and anti-ganglioside GD2 immunocytochemistry. Eur J Cancer 1997;33:2024–2030.
15. Tchirkov A, Kanold J, Giollant M, et al. Molecular monitoring oftumor cell contamination in leukapheresis products from stage IVneuroblastoma patients before and after positive CD34 selection.Med Pediatr Oncol 1998;30:228–232.
16. Handgretinger R, Greil J, Schurmann U, et al. Positive selectionand transplantation of peripheral CD34+ progenitor cells: feasi-bility and purging efficacy in pediatric patients with neuroblas-toma. J Hematother 1997;6:235–242.
17. Kanold J, Yakouben K, Tchirkov A, et al. Long-term follow-upafter CD34+ cell transplantation in children with neuroblastoma.Blood 1998;92:445a (Abstr. 1842).
18. Kanold J, Yakouben K, Tchirkov A, et al. Long-term results ofCD34+ cell transplantation in children with neuroblastoma. MedPediatr Oncol 2000;35:1–7.
19. Grupp SA, Stern JW, Bunin NJ, et al. Rapid sequence tandemtransplant for children with high-risk neuroblastoma. Med PedOncol 2000;35:696–700.
682 Donovan et al.