Embed Size (px)
Citation preview
Centre for Research in Geriatric Medicine
Centre for Research in Geriatric Medicine
FRAILTY IN OLDER INPATIENTS
Associate Professor Ruth E. HubbardBSc, MBBS, MRCP, MSc, MD, FRACP
21st October, 2016

Centre for Research in Geriatric Medicine
Objectives
1. Describe and compare frailty measures
2. Consider frailty in relation to failure of a complex
system
3. Review importance of frailty in older surgical patients

Centre for Research in Geriatric Medicine
Tomorrow’s Objectives
1. Review a new instrument to measure frailty in routine
practice
2. Discuss limitations and potential pitfalls of frailty
Centre for Research in Geriatric Medicine
Centre for Research in Geriatric Medicine
BACKGROUND
Centre for Research in Geriatric Medicine
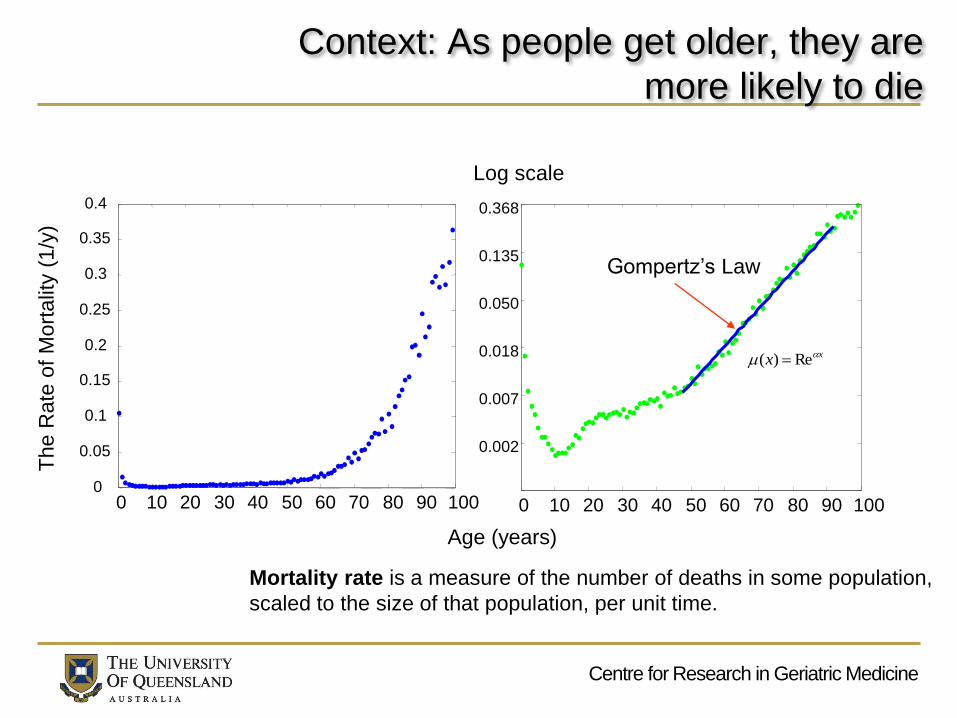
Context: As people get older, they are
more likely to die
0 10 20 30 40 50 60 70 80 90 1000
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0 10 20 30 40 50 60 70 80 90 100
0.002
0.007
0.018
0.050
0.135
0.368
Age (years)
The R
ate
of
Mort
alit
y (
1/y
)
Log scale
Gompertz’s Law
Mortality rate is a measure of the number of deaths in some population,
scaled to the size of that population, per unit time.
xx Re)(

Centre for Research in Geriatric Medicine
How a system’s components are
arranged may affect the rate of failure
A string of Christmas tree lights
Electricity supplied to many rooms in
a house simultaneously
Organs
Tissues

Centre for Research in Geriatric Medicine
How do systems prevent failure?
Living systems: redundancy
– The great merit of this is that we can quantify it with deficit
accumulation
Machines: QC of individual parts
Centre for Research in Geriatric Medicine
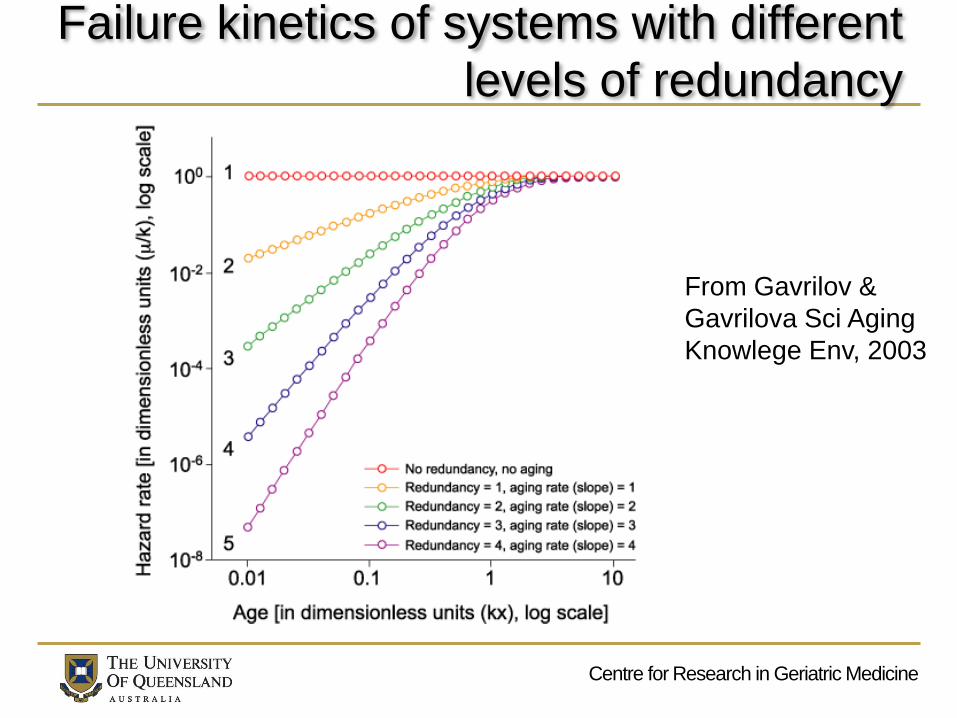
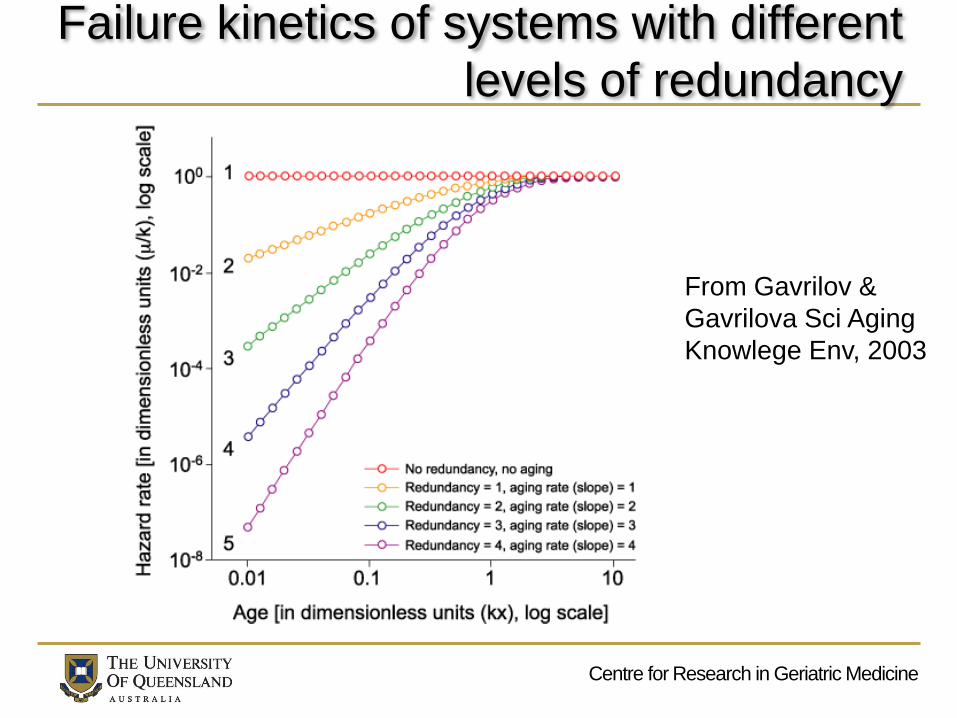
Failure kinetics of systems with different
levels of redundancy
From Gavrilov &
Gavrilova Sci Aging
Knowlege Env, 2003

Centre for Research in Geriatric Medicine
Centre for Research in Geriatric Medicine
HOW DOES THIS RELATE TO
FRAILTY?
Centre for Research in Geriatric Medicine
What is frailty?
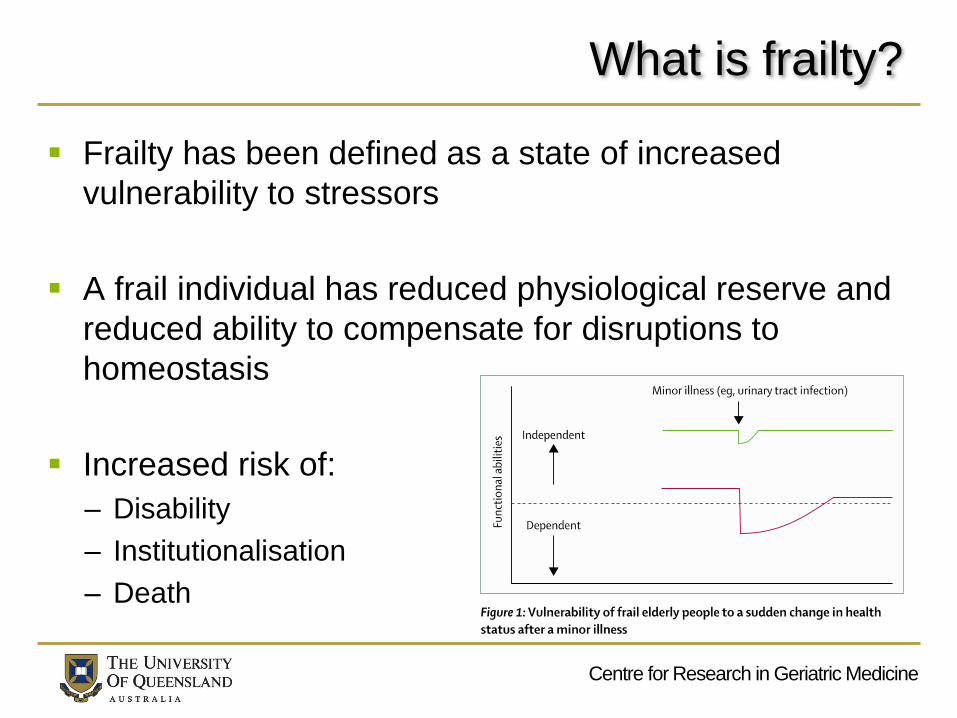
Frailty has been defined as a state of increased
vulnerability to stressors
A frail individual has reduced physiological reserve and
reduced ability to compensate for disruptions to
homeostasis
Increased risk of:
– Disability
– Institutionalisation
– Death
Centre for Research in Geriatric Medicine
How can frailty be measured?
Understanding frailty has become the focus of extensive
research
The associations of frailty are now well described
However, little is known about how frailty can be
assessed in hospital inpatients
3 main approaches
– Clinical syndrome or phenotype
– Subjective opinion
– Multidimensional risk state
Centre for Research in Geriatric Medicine
Definitions
Clinical syndrome: a set of signs and symptoms
Lists and algorithms derived from clinical judgment
Combinations:– Physical inactivity and weight loss (Chin a Paw, 1999)
– Gait speed, peak expiration, hand grip, sitting position, visual impairment (Klein, 2005)
– Fatigue, resistance, ambulation, illness, loss of weight (Abellanvan Kahn, 2008)
– Age, sex, daily drugs use, sensory deficits, physical inactivity, calf circumference, independent activities of daily living, gait and balance, pessimism about one’s health (Ravaglia, 2008)
Centre for Research in Geriatric Medicine
Fried phenotype
The most well known and widely used phenotype
Criteria
– unintentional weight loss of 10 lbs or more in past year
– self reported exhaustion
– weak grip strength
– slow walking speed
– low physical activity
Centre for Research in Geriatric Medicine
Question 1
In older people, which is the strongest predictor of future disability?
Weight loss
Muscle weakness
Slow walking speed
Cognitive impairment
Results
Centre for Research in Geriatric Medicine
Fried phenotype
Strengths
– Clinical coherency
– Reproducibility
– Wasting disorder with sarcopenia as pathophysiological feature
Weaknesses
– Omission of mood and cognition
– Selection of initial cohort
– Dichotomous/ trichotomous outcome
– Reliance on performance based tests
Centre for Research in Geriatric Medicine
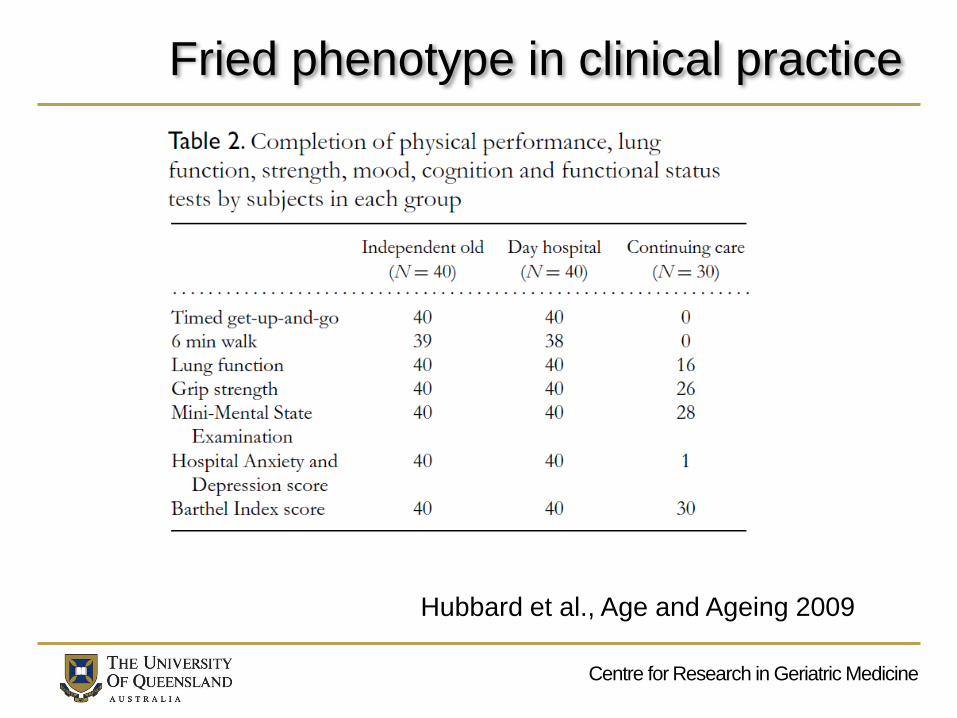
Fried phenotype in clinical practice
Hubbard et al., Age and Ageing 2009

Centre for Research in Geriatric Medicine
Subjective opinion
“We know it when we see it”
Visual estimation of biological age
– a checklist of age-associated changes in appearance,
communication and mobility.
– Good inter-rater agreement
Global measures
– Studenski et al, JAGS 2004
– Rockwood et al, CMAJ 2005
Centre for Research in Geriatric Medicine
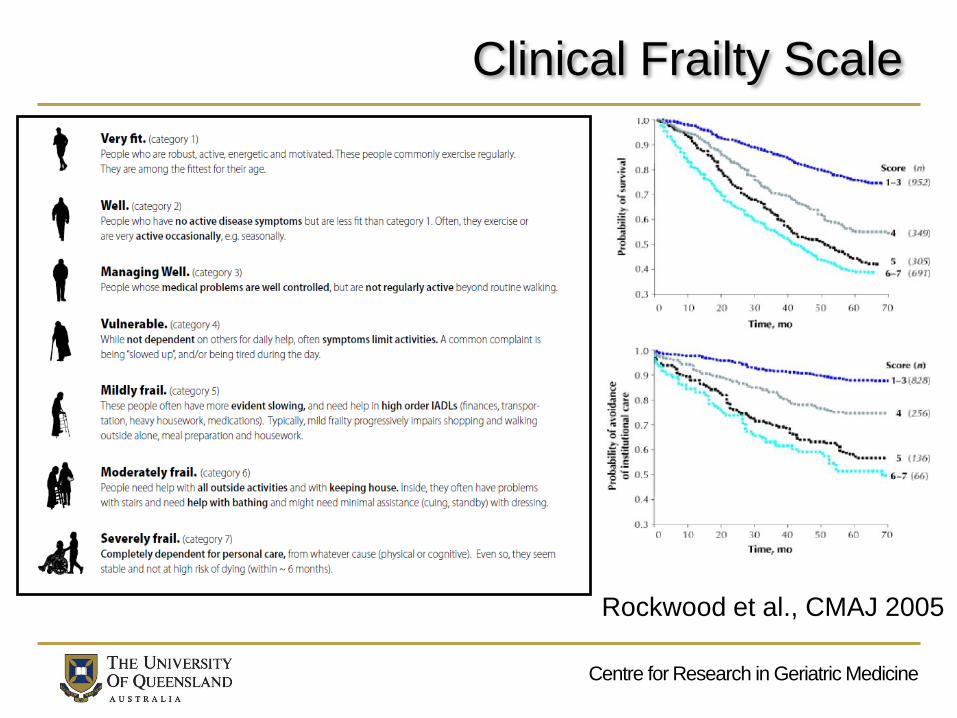
Clinical Frailty Scale
Rockwood et al., CMAJ 2005

Centre for Research in Geriatric Medicine
CFS in clinical practice
5764 admissions
through ED
>75 years
CFS an independent
predictor of in-patient
mortality, transfer to
Geriatric Ward and
long LOS.

Centre for Research in Geriatric Medicine
Subjective opinion in clinical practice
Such measures have strong
face validity
But limited generalisability
They rely on judgement
– which varies between
clinicians and between health
systems
and depend on geriatric
expertise
– e.g. accurate assessment of
functional status
Centre for Research in Geriatric Medicine
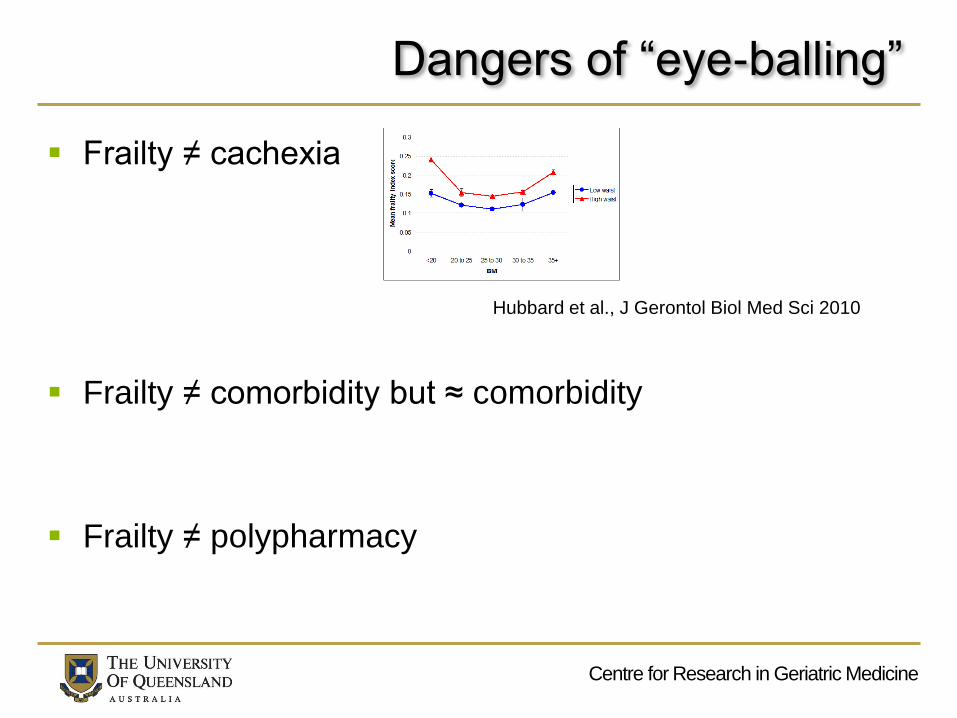
Dangers of “eye-balling”
Frailty ≠ cachexia
Frailty ≠ comorbidity but ≈ comorbidity
Frailty ≠ polypharmacy
Hubbard et al., J Gerontol Biol Med Sci 2010
Centre for Research in Geriatric Medicine
Deficit accumulation
Frailty = multidimensional risk state
Can be measured by quantity rather than by the nature
of health problems
Various disorders are accumulated by individuals during
their lives
The more deficits that are accumulated, the more likely
that person is to be frail
Rockwood and Mitnitski, 2001

Centre for Research in Geriatric Medicine
Deficit accumulation
Deficits can be symptoms, signs, diseases, disabilities, abnormal laboratory measurements
– Accumulate with age
– Associated with adverse outcome
– Do not saturate
– Cross different domains
– Use same items longitudinal data
FRAILTY INDEX
Minitski et al., 2001; Searle et al., 2008

Centre for Research in Geriatric Medicine
Frailty Index
Frailty indices can be constructed from different numbers and types of variables
36,424 older people– FI values closely comparable across countries
– increasing with age at approximately 3% per year in community-dwellers
– correlating highly with mortality (Mitnitski et al., 2005)
Risk of adverse outcomes defined more precisely by deficit indices than by chronological age (Romero-Ortuno and Kenny, 2012)
Centre for Research in Geriatric Medicine
Failure kinetics of systems with different
levels of redundancy
From Gavrilov &
Gavrilova Sci Aging
Knowlege Env, 2003
Centre for Research in Geriatric Medicine
Mean a
ccum
ula
tion o
f deficits
65 70 75 80 85 90 95
ALSA
CSHA-screen
CSHA-exam
NHANES
NPHS
SOPS
Breast cancer
CSHA-inst
Myoc Infarct
US-LTHS
H70-75
0.1
0.2
0.3
0.5
1.0
0.05
Age (years)
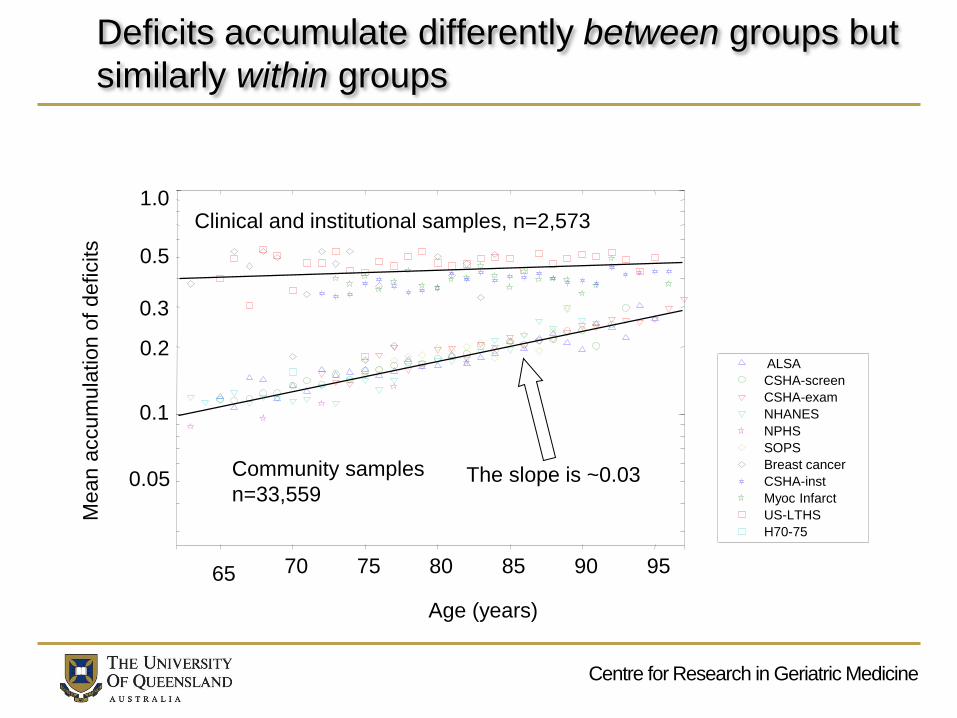
Clinical and institutional samples, n=2,573
The slope is ~0.03Community samples
n=33,559
Deficits accumulate differently between groups but
similarly within groups
Centre for Research in Geriatric Medicine
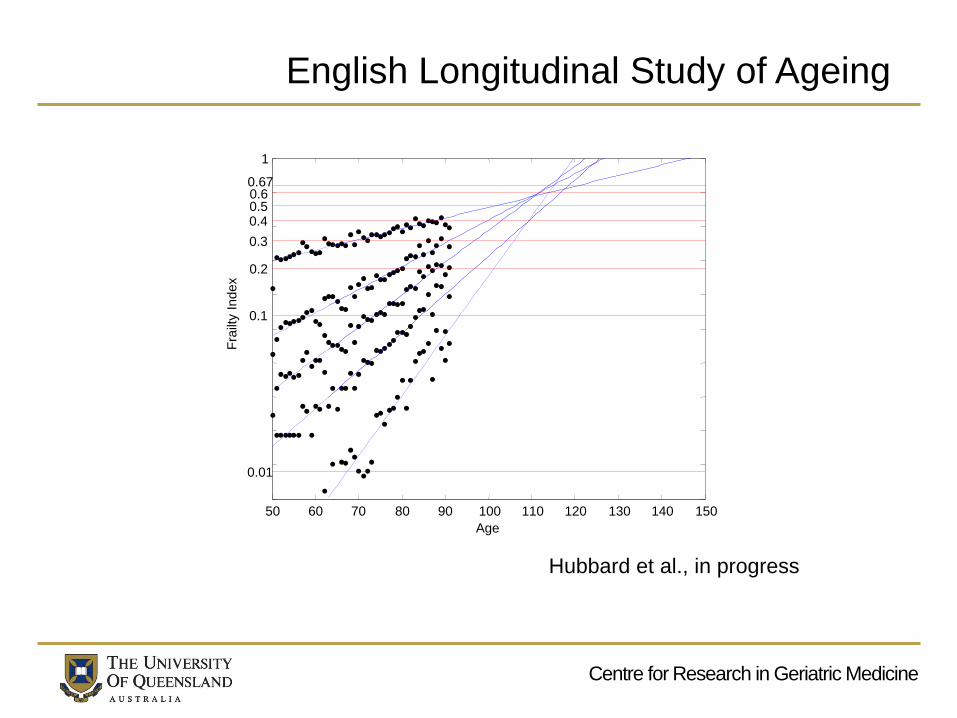
50 60 70 80 90 100 110 120 130 140 150
1
Age
0.670.60.50.4
0.3
0.2
0.1
0.01
Fra
ilty I
ndex
English Longitudinal Study of Ageing
Hubbard et al., in progress
Centre for Research in Geriatric Medicine
Jeanne Calment 1875 - 1997
Centre for Research in Geriatric Medicine
Question 2
Of the top ten verified oldest living people in the world, how many are men?
0
1
3
6
Results

Centre for Research in Geriatric Medicine
Ageing and the Sex-Frailty Paradox
0 0.1 0.2 0.3 0.4 0.50
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.50
0.2
0.4
0.6
0.8
1
B
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
Age (years)
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
A
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
Age (years)
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
A
Death
rate
0 0.1 0.2 0.3 0.4 0.50
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.50
0.2
0.4
0.6
0.8
1
Frailty index
B
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
Age (years)
Fra
ilty
index
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
A
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
Age (years)
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
A
Death
rate
0 0.1 0.2 0.3 0.4 0.50
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.50
0.2
0.4
0.6
0.8
1
B
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
Age (years)
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
A
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
Age (years)
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
A
Death
rate
0 0.1 0.2 0.3 0.4 0.50
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.50
0.2
0.4
0.6
0.8
1
Frailty index
B
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
Age (years)
Fra
ilty
index
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
A
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
Age (years)
65 70 75 80 85 90 95
0.1
0.2
0.4
0.05
A
Death
rate
Centre for Research in Geriatric MedicineCentre for Research in Geriatric Medicine
FRAILTY & COMPLEX
SYSTEM FAILURE
Centre for Research in Geriatric Medicine
Geriatric giants and loss of redundancy
A frail older person is analagous to a complex system
on the threshold of failure, redundancy has been lost.
When a complex system fails, it fails with higher order
functions first.
Higher order functions
– Upright bipedal ambulation
– Divided thinking

Centre for Research in Geriatric Medicine
The Geriatric Giants
Falls
Immobility
Incontinence
Delirium
Geriatric syndromes need multifaceted assessment and
holistic management

Centre for Research in Geriatric Medicine
Centre for Research in Geriatric Medicine
FRAILTY IN OLDER SURGICAL
PATIENTS

Centre for Research in Geriatric Medicine
Frailty in the Old Old and Oldest Old
Systematic review
Patients’ mean age ≥ 75 years
23 studies
Surgery
– Cardiac, oncological, vascular, general, vascular, orthopaedic
Frailty
– Measured in 21 different ways
Centre for Research in Geriatric Medicine
Results
Strong evidence (N, quality, consistency)
– Increased mortality
– Post operative complications
– LOS
Weak evidence
– Discharge to higher level of care
– Functional decline
– Low quality of life
Centre for Research in Geriatric Medicine
Summary
1. Describe and compare frailty measures
phenotypes, subjective opinion, deficit accumulation
2. Consider frailty in relation to failure of a complex
system
minor insults can be devastating for a frailer person
3. Review importance of frailty in older surgical patients
associated with relevant adverse outcomes
Centre for Research in Geriatric Medicine
Global Forum on Acute Care Excellence
38
Ensuring safe passage for frail and vulnerable adults across the hospital continuum
February 20-21, 2017





























