Embed Size (px)
Citation preview

J Clin Pathol 1986;39:774-778
Cerebral and orbital Aspergillus infection due toinvasive aspergillosis of ethmoid sinus
J LOWE,* J BRADLEY,t
*Department ofNeuropathology, Queens Medical Centre, Nottingham, and the tDepartment ofRenal Medicine,Addenbrooks Hospital, Cambridge
SUMMARY Aspergillus fumigatus infection due to primary infection of the ethmoid sinus affectedthe brain and orbit of an otherwise healthy elderly woman. Primary nasal sinus infection may be a
chronic process analogous to aspergilloma of the lung: it may, however, assume a locally invasivecourse and spread to the orbit or brain, as in the case described. This form of Aspergillus infectionis rare in Europe but common in hot dry areas like the Sudan. The infection was probablycontracted by our patient while on holiday in South Africa.
Histological recognition of the condition is important in these unusual sites-many cases areclinically diagnosed as a tumour and undergo biopsy.
Case report
A 74 year old woman collapsed while out shopping.On recovery she gave a history of intermittent frontalheadaches, which she had had for one year sincereturning from a holiday to South Africa. Exam-ination showed a right ptosis and proptosis, but fullneurological examination was otherwise normal. Shewas admitted to hospital where she was noted to beintermittently confused and incontinent of urine.
Cranial radiographs and ultrasonographic exam-ination of her right orbit yielded normal results.Computed tomography showed a large multilobularmass affecting the frontal poles, with peripheralenhancement and severe surrounding oedema(Fig. 1). There was also a low density mass obscuringthe right ethmoid sinus, extending into the right orbit.This lesion was considered to be a primary cerebraltumour; surgery was not indicated. Her conditiondeteriorated, and she suffered increasing periods ofconfusion and drowsiness before her death.
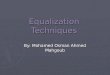
Post mortem examination showed that the tumourwas an abscess filled with cream coloured purulentmaterial. It occupied the right frontal pole mediallyand extended into the left frontal lobe. The abscesswas 4-5 cm in diameter and had irregular margins(Fig. 2). The inferior part of the cavity adhered to theorbital plate and surrounded the optic nerve close toits entry into the orbit. The bone was macroscopicallyintact. Examination of the right orbit showed the
Accepted for publication 11 February 1986
posterior structures to be obscured by firm whitetissue with no spread to the globe. Similar firm whitetissue without macroscopic necrosis obscured theethmoid sinus on the right. The other nasal sinuses
Fig. I Computed tomography scan ofbrain showingmultilobular mass infrontal pole.
774
on April 30, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.7.774 on 1 July 1986. Dow
nloaded from
Invasive aspergillosis of ethmoid sinus
w t ~~~~~~~~.0-- -I -
1 2 3(cm)
Fig. 2 Inferior aspect ofbrain showingfrontal abscess.
were normal macroscopically. The other organsshowed no macroscopic abnormalities.
Histology showed that the ethmoid sinus was oblit-erated by fibrous granulation tissue, with a heavychronic inflammatory cell infiltrate. There were alsodiscrete granulomata with histiocytic giant cells sur-rounding central zones of neutrophil leucocytes andfungal hyphae. Small granulomata were present inresidual ethmoid sinus mucosa and also containedfungal hyphae (Fig. 3). Examination of the orbitalcontents showed a large serpiginous abscess cavitywith surrounding dense fibrous tissue. This containedlarge numbers of partly degenerate fungal hyphaewith a granulomatous reaction. The abscess did notaffect the optic nerve (Fig. 4), or the globe. The cere-bral abscess was surrounded by reactive astrocyteswith a histiocytic and giant cell reaction. The cavitycontained necrotic material, degenerate fungal hyp-hae, and neutrophil leucocytes (Fig. 5). No vascularinvasion was seen in any of the tissues, but smallarteries in the orbit, however, were occluded byold organising thrombus in relation to the marginsof the abscess (Fig. 6). Histological examination ofother tissues at necropsy showed no evidence ofsystemic infection or of any condition that may have
775
predisposed the patient to an immune deficient state.Culture of material from the cerebral abscess wall
showed a pure growth of Aspergillusfumigatus.
Discussion
Spread to the nasal sinus by Aspergillus may takethree forms, which parallel those seen in the lowerrespiratory tract; saprophytic infection (mycetoma),allergic aspergillosis,' and invasive aspergillosis.
Saprophytic infection is a chronic indolent form ofthe disease localised to the nasal sinus. This is themost common form of sinus disease and is endemic inthe Sudan.2 3 There are thought to be three predis-posing factors to this high incidence in the Sudan: thedry climate, a high content of Aspergillus spores in thesoil, and a high atmospheric dust content. Clinically,symptoms include headache, rhinorrhoea, and post-nasal discharge.
Allergic Aspergillus sinusitis is a recently describedcondition in which the affected sinuses are filled withmucoid material containing numerous eosinophilleococytes, cellular debris, and Charcot-Leyden crys-tals. Scattered fungal hyphae are present.1
Invasive Aspergillus infection occurs when there isspread to the sinus wall and extension into the sur-rounding tissues. The reason for a saprophytic infec-tion becoming invasive is not known. Invasiveinfection stemming from a pulmonary primary site isoften seen in patients who are immunosuppressed.Notably, most of the published cases of primaryrhinocerebral Aspergillus infection are not recordedas having a condition liable to cause an immu-nosuppressed state. The most common pathogenicorganism in reported series of primary rhinocerebralaspergillosis has been Aspergillus flavus, but thesecases are mostly from the Sudan and may reflect alocal pattern of disease. Cases from outside the Sudanhave shown other species including Aspergillusfumigatus.247 8
Our patient probably developed a saprophyticsinus infection while she was on holiday in SouthAfrica, producing a localised disease which resulted inthe symptom of headache for one year. Invasive infec-tion then developed with local extension into the orbitand brain.
In a review of thirty cases of orbital aspergillosis(the bulk of published cases) 21 had proptosis, 24had nasal sinus disease, and six had cerebral disease.4Initial diagnosis was made mainly after histologicalexamination of biopsy material.The main histological diagnostic feature of rhino-
cerebral aspergillosis is the presence of a histiocytic orgiant cell reaction to fungal hyphae. The diagnosis ofa fungal infection in this site should be consideredwhenever a biopsy, usually performed to make a
on April 30, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.7.774 on 1 July 1986. Dow
nloaded from

776
Fig. 3 Mucosaftom ethmoid sinus showing Aspergillus granuloma (Periodic acid Schiff.) x 54.
1 ;
AY
(P
Fig. 4 Optic nerve (left) with margin ofAspergillus containing abscess. (Periodic acid Schiff.) x 13.
Fig. 5 Edge ofcerebral abscess containingfungal elements. (Periodic acid Schiff.) x 340.
Lowe, Bradley
on April 30, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.7.774 on 1 July 1986. Dow
nloaded from

Invasive aspergillosis ofethmoid sinus
-k2'Fig. 6 Blood vesselftom orbit at margin ofabscess. (Periodic acid Schif.) x 135.
diagnosis of a tumour, contains necrotic tissue withoccasional histiocytic giant cells. The identificationof fungal hyphae in this type of necrotic tissue may bedifficult due to degeneration and ballooning of thehyphae. The two main primary fungal infectionsaffecting the region of the nasal sinuses and brain areAspergillus and Zygomycosis (formerly phycomy-cosis). Histological sections show that the Aspergillushyphae are thin (3-6pm), have regular parallel wallswith easily seen septa, and show a regular dichoto-mous branching pattern at acute 450 angles. In con-trast, the hyphae in a zygomycotic infection are broad(6-25 pm), have irregular contours to the hyphalwalls, and have an irregular branching pattern withonly very occasional septa. It is usually impossible,however, to identify a fungus in a small biopsy with afew degenerate hyphae without resorting to culture.Degenerate Aspergillus hyphae will lose septa andbecome swollen so that they resemble a zygomycosis.Care should therefore be exercised in the inter-pretation of biopsy material.5 6A complication of cerebral invasion by asper-
gillosis is mycotic arteritis. This is due to directinvasion of small vessel walls by the fungal hyphae.In one reported case this led to fatal intracranialhaemorrhage.7
Treatment of invasive rhinocerebral aspergillosisby antifungal chemotherapy has been regarded asbeing generally ineffective. Surgical excision is recom-mended as the most effective means of controlling thedisease.4 8
In conclusion, we have described a case of Asper-gillus infection with a pattern, which, while well rec-ognised, is very unusual in Europe. With the increasein travel to climates in which this pattern of disease iscommon, awareness of this type of presentation andbiopsy diagnosis warrant wider consideration.
The culture of the Aspergillus was performed in thedepartment of microbiology, Queens Medical Centre,Nottingham, by Janet Crowley. We are grateful tothe Mycological Reference Laboratory, Colindale,for confirmation of the fungal type. We thank DrPJ Toghill for permission to report this case. Thephotomicrographs were produced by Mr BillBrackenbury of the department of histopathology.
References
Katzenstein AA, Sale SR, Greenberger PA. Pathologic findings inallergic Aspergillus sinusitis. Am J Surg Pathol 1983;7:439-43.
777
on April 30, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.7.774 on 1 July 1986. Dow
nloaded from

778
'Milosev B, Mahgoub S, Abdel Aal 0, El Hassan AM. Primaryaspergilloma of the paranasal sinuses in the Sudan. Br Surg1969;56:132-7.
3Veress B, Malik OA, El Tayeb AA, El Daoud S, Mahgoub ES,El Hassan AM. Further observations on primary paranasalAspergillus granuloma in the Sudan. Am J Trop Med Hyg1973;22:765.
'Green WK, Font RL, Zimmerman LE. Aspergillosis of the orbit.Arch Ophthalmol 1969;82:302-13.
5Binford CH, Connor DH, eds. Pathology of tropical and extra-ordinary diseases. Vol. 2. Washington, DC: Armed ForcesInstitute of Pathology, 1976:564-5.
'Chandler FW, Kaplan W, Ajello L. A colour atlas and textbook of
Lowe, Bradleythe histopathology of mycotic diseases. London: Wolfe MedicalPublications, 1980:34-8, 122-7.
'Fernando SSE, Lauer CS. Aspergillus fumigatus infection of theoptic nerve with mycotic arteritis of cerebral vessels. Histo-pathology 1982;6:227-34.
8Miglets AW, Saunders WH, Ayres L. Aspergillosis of the sphenoidsinuses. Arch Otolaryngol 1978;104:47-50.
Request for reprints to: Dr J Lowe, Department ofPathology, University Hospital, Queen's Medical Centre,Nottingham NG7 2UH, England.
on April 30, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.7.774 on 1 July 1986. Dow
nloaded from