Embed Size (px)
Citation preview

http://nro.sagepub.com/The Neuroscientist
http://nro.sagepub.com/content/19/4/409The online version of this article can be found at:
DOI: 10.1177/1073858412467377
2013 19: 409 originally published online 30 November 2012NeuroscientistSukhvinder Kalsi-Ryan, Spyridon K. Karadimas and Michael G. Fehlings
Increasingly Prevalent and Devastating DisorderCervical Spondylotic Myelopathy: The Clinical Phenomenon and the Current Pathobiology of an
Published by:
http://www.sagepublications.com
can be found at:The NeuroscientistAdditional services and information for
http://nro.sagepub.com/cgi/alertsEmail Alerts:
http://nro.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Nov 30, 2012OnlineFirst Version of Record
- Jul 1, 2013Version of Record >>
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

The Neuroscientist19(4) 409 –421© The Author(s) 2012Reprints and permissions: sagepub.com/journalsPermissions.navDOI: 10.1177/1073858412467377nro.sagepub.com
Progress in Clinical Neuroscience
IntroductionCervical spondylotic myelopathy (CSM) is a degenerative condition that results in neurological impairment second-ary to degeneration of structures in the spinal column in the cervical region, which causes narrowing of the spinal canal. The narrowing causes cord compression over time that is non-traumatic in nature and essentially causes tet-rapariesis. Severity of the compression and deficits varies across individuals. Since the narrowing or compression is degenerative in nature, progression is slow and generates adaptive deficits in both the cord and periphery.
The purpose of this review is to introduce CSM and to summarize its clinical presentation in addition to the cur-rent knowledge of the pathobiology of this unique disease. CSM represents the most common cause of spinal cord dysfunction globally yet remains one of the most unex-plored neurological diseases. As soon as CSM captures
the interest of the neuroscience community, the molecu-lar mechanisms of this intractable disease will begin to be elucidated, which, in turn, could lead to development of
467377 NROXXX10.1177/1073858412467377The NeuroscientistKalsi-Ryan et al.
1Department of Physical Therapy, University of Toronto, Toronto, Ontario, Canada2Krembil Neuroscience Centre, Toronto Western Hospital, Toronto, Ontario, Canada3Toronto Rehabilitation Institute, Toronto, Ontario, Canada4Institute of Medical Science, University of Toronto, Toronto, Ontario, Canada5Department of Surgery, and Neuroscience Program, University of Toronto, Toronto, Ontario, Canada
Corresponding Author:Michael G. Fehlings, Division of Neurosurgery, Toronto Western Hospital, 399 Bathurst Street, Suite 4WW-449, Toronto, ON M5T2S8, Canada. Email: [email protected]
Cervical Spondylotic Myelopathy: The Clinical Phenomenon and the Current Pathobiology of an Increasingly Prevalent and Devastating Disorder
Sukhvinder Kalsi-Ryan1,2,3, Spyridon K. Karadimas2,4, and Michael G. Fehlings5
Abstract
Cervical spondylotic myelopathy (CSM) is a common disorder involving chronic progressive compression of the cervical spinal cord due to degenerative disc disease, spondylosis, or other degenerative pathology. CSM is the most common form of spinal cord impairment and causes functional decline leading to reduced independence and quality of life. Despite a sound understanding of the disease process, clinical presentation and management, a universal definition of CSM and a standardized index of severity are not currently used universally. Work is required to develop a definition and establish clinical predictors of progression to improve management of CSM. Despite advances in decompressive and reconstructive surgery, patients are often left with residual disability. Gaps in knowledge of the pathobiology of CSM have limited therapeutic advances to complement surgery. Although the histopathologic and pathophysiologic similarities between CSM and traumatic spinal cord injury have long been acknowledged, the unique pathomechanisms of CSM remain unexplored. Increased efforts to elucidate CSM pathobiology could lead to the discovery of novel therapeutic targets for human CSM and other spinal cord diseases. Here, the natural history of CSM, epidemiology, clinical presentation, and current methods of clinical management are reported, along with the current state of basic scientific research in the field.
Keywords
cervical spondylotic myelopathy, spinal cord injury, cervical spine, epidemiology, pathobiology
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

410 The Neuroscientist 19(4)
reparative and regenerative treatments for human CSM and other spinal cord diseases, including acute spinal cord injury (SCI).
EpidemiologyIncidence and Prevalence
The exact incidence and prevalence of CSM remains unknown. However, since CSM is a disease that is caused by degeneration of the spinal structures, the larg-est group affected by this disease is the elderly. Recent studies suggest that CSM is one of the most common spinal cord disorders in the older population. It was the most the most common diagnosis (23.6% of all cases), in 2104 patients with nontraumatic spastic parapareisis or tetraparesis (Moore and Blumhardt 1997). CSM more commonly affects men than women, at a ratio of 2.7:1. The average age of diagnosis is approximately 64 years. Despite the presence of multilevel disease in most cases, C5 and C6 are the most common levels at which com-pression of the cord occurs (Northover and others 2012).
Cervical spondylosis is the main cause of CSM. However, age-related cervical spondylosis does not always result in CSM. The radiographic incidence in an asymptomatic population in their 70s, was reported as 95% in men and 70% in women (Gore and others 1986) and in patients older than 40 years, nearly 60% had disc degeneration and 20% had foraminal stenosis (Boden and others 1990). CSM is the sequelae of a narrow spinal canal (secondary to spondylosis) that results in spinal cord com-pression causing neurological deficits. Ossification of the posterior longitudinal ligament (OPLL) is a condition more commonly seen in the Asian population. OPLL essentially causes compression on the cord, and, although there is controversy as to whether this truly constitutes CSM, we consider the posterior longitudinal ligament part of the spinal column, and thus consider OPLL as one cause of CSM. It occurs in 1.5% to 2.4% of the Caucasian population and 1.9% to 4.3% of the Asian population who present with adult cervical disorders over the age of 50 years (Matsunaga and Sakou, 2006)
A narrow spinal canal can occur secondary to two fac-tors: 1) age-related cervical spondylosis and 2) a devel-opmentally narrow canal. Individuals who have a developmentally narrow canal will develop symptoms of CSM with milder spondylosis than those with a normal canal. Furthermore, CSM secondary to a narrow canal typi-cally presents at a younger age (Epstein and others 1979). It is known from cadaver studies that females have narrower canals than men and that individuals 60 years and older have significantly narrower canals than younger individu-als. It is estimated that cervical stenosis is present in 4.9% of the adult population, in 6.8% of the population 50 years
and older, and in 9% of the population 70 years and older (Lee and others 2007). Furthermore, CSM is the key underlying risk factor predisposing patients to traumatic central cord syndrome, the most common cervical SCI (van Middendorp and others 2010). Recent evidence also suggests a genetic predisposition to CSM with first- and third-degree relatives implicated (Patel and others 2012).
In summary, CSM is a common disorder, especially in the elderly, that causes neurological impairment and functional decline, leading to reduced independence and quality of life. Thus, there has been a recent motivation by the neuroscience community to elucidate the pathobi-ology of the disease and further investigate the discovery of novel clinically relevant therapeutic targets for transla-tion in human patients.
Disability Related to Cervical Spondylotic MyelopathyThe disability caused by CSM varies greatly from indi-vidual to individual. Presentation can be as minimal as some numbness of the hands or be as significant as full tetraplegia. Deficits include the following: neuropathic pain, weakness and numbness of the upper extremities, loss of manual dexterity, gait deficits, and spasticity of the lower extremities. In addition, bowel and bladder symptoms may appear. Any one, or a combination of these deficits, will ultimately cause decline in function and independence, which leads to a reduced quality of life (King and others 2003). Although the disability asso-ciated with this degenerative condition is progressive and has a profound effect on people’s lives, it may remain undiagnosed for a long time. Thus, early identification and management of this disease is desirable.
Clinical Presentation of Cervical Spondylotic MyelopathyNatural History of the Disease
It is necessary to describe the natural history of the dis-ease in order to optimize treatment. Symptoms usually deteriorate without surgery, sometimes stabilize, and rarely improve. A 2009 systematic review reported expert consensus that progression can either be slow with step-wise decline (class III evidence) or a long period of qui-escence (Matz and others 2009). Though older literature reports improvement without intervention, these studies are considered flawed because of their heterogeneous patient population and inconsistent end-point measures (Lees and Turner 1963). Some studies have consistently shown progressive deterioration without surgery (Sadasivan and others 1993; Symon and Lavender 1967), particularly in patients with moderate to severe CSM.
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

Kalsi-Ryan et al. 411
A subject of controversy has been the natural history of patients who present with mild myelopathy. It was found that in 56 patients with mild CSM (Japanese Orthopaedic Association [JOA] score ≥13) managed con-servatively, 11/56 deteriorated to moderate and severe symptoms. However, the results were not statistically sig-nificant (Shimomura and others 2007). In patients with mild CSM (mJOA score >16) and aged younger than 75 years, symptoms rarely progress measurably. In a case series of patients with mild CSM (JOA score >13) and increased signal intensity on T2-weighted MRI, who were managed conservatively, 16/45 patients progressed to requiring surgery, and 2/45 subsequently needed surgery after acute SCI following minor trauma. At 5 and 10 years after diagnosis, 82% and 56% of patients, respectively, did not require surgery respectively (Oshima and others 2012). Some identified risk factors for deterioration from mild CSM include female gender, increased cervical mobility (Barnes and Saunders 1984), focal disc hernia-tion, segmental kyphosis in the area of maximum cord compression, total cervical range of motion (Oshima and others 2012), and circumferential spinal cord compression at the maximum compression segment (Shimomura and others 2007). Asymptomatic patients with evidence of cervical stenosis, abnormal electromyography, or radicu-lar signs, are likely to become myelopathic in the future. Although some work has been done to understand the natural history of the disease, larger multicenter studies are required to further this understanding with consis-tent use of outcomes across centers to allow for cross-comparison and analysis.
Symptoms and Signs of Cervical Spondylotic MyelopathyThe initial identification of CSM is based heavily on the presence of symptoms. A patient with CSM may seek medical attention when they experience any number of the following symptoms: neck pain or stiffness, numb and/or clumsy hands, weakness, bilateral arm parasthesia, gait impairment, and/or L’Hermitte’s phenomenon (Gemici 2010; Ono and others 1987; Tracy and Bartleson 2010). Autonomic symptoms include increased urinary urgency and frequency and urinary incontinence, which are typically not the first symptoms noted by the individual, but present in conjunction with other symptoms (Hattori and others 1990).
Some studies have concluded that a subtle gait distur-bance is the most common presentation of CSM (Gorter 1976; Lunsford and others 1980) and that spastic gait occurs first, followed temporally by upper extremity numbness and loss of fine motor control of the hands. However, gait impairment in CSM can have a broad range of clinical presentation. Florid spastic parapareisis is the most severe clinical presentation with individuals
able to walk at a normal speed with a relatively mild gait deficit (a slight limp) describing only some tightness in the legs. Similarly, the hands can also present with mild sensory deficit that does not affect function or be so severe that dysfunction in the hands does not allow an individual to perform simple tasks such as eating inde-pendently (Epstein and others 1987). Because there is such disparity in patients with CSM, the characterization of gait and hand impairment/function requires further refinement. Assessment tools to better define and docu-ment impairment and function quantitatively will be use-ful in identifying the actual clinical presentation and the impact on independence for these individuals.
A neurological exam is used to confirm the presence of spinal cord dysfunction. Manifestation of clinical signs is used to determine the extent of spinal cord dysfunction and include: corticospinal tract signs, hyperreflexia, posi-tive plantar response, ataxia of gait, spasticity/clonus, and the Hoffmann’s reflex (Lunsford and others 1980). The presence of any of these signs signifies disruption of the descending motor pathway. Essentially, these tests verify the presence or absence of upper motor neuron lesions for many neurological disorders. Table 1 summarizes the diagnostic value of the common signs and symptoms of CSM. Thus, the presence of signs alone is not sufficient for a diagnosis of CSM. Signs must be accompanied by symptoms and a positive MRI for cord compression.
Once CSM is diagnosed, duration of symptoms is used to define how long the individual has had cord compres-sion. However, there are two unanswered questions. The first of these relates to how long the cord has been com-pressed prior to presentation of symptoms; the second per-tains to what extent neural plasticity has occurred to compensate for the compression of neural tissue, since the compression on the cord is a slow process. Based on stud-ies of cortical plasticity specific to CSM, it is known that the cortical map adapts before and after surgery (Holly and others 2007; Tam and others 2010). Based on this plasticity and the findings in acute SCI studies of spinal cord func-tion post-injury (Cadotte and others 2012), it is reasonable to speculate that the spinal cord has the time and the space to adapt under chronic progressive compression.
Magnetic Resonance ImagingThe role of imaging is to identify the structural causes of myelopathy, and to determine the extent of compression on the neural tissues. Although plain films and CT scans are inexpensive and can show changes in the disc space, verte-bral body sclerosis, osteophytes, cervical lordosis, estimate sagittal diameter (Gore and others 1986), and identify insta-bility (Tracy and Bartleson 2010), the diagnostic imaging of choice is MRI because it yields the most information in relation to the neural tissue (Tracy and Bartleson 2010).
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

412 The Neuroscientist 19(4)
Table 1. Diagnostic Indicators of Cervical Spondylotic Myelopathy.
MRI indicators Clinical symptoms Neurological signs
Full effacement of CSF and deformation of cord Numb hands Corticospinal tract signsT1 signal change Bilateral arm parasthesia HyperreflexiaT2 signal change Spastic Ataxic gait Positive Hoffman signSegmentation of T2 signal change L’Hermitte’s phenomenon Positive plantar responseReduction in transverse area of cord Weakness Ataxia Atrophy of hand muscles Spasticity/clonus
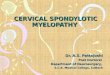
Figure 1. T2-weighted signal change on MRI. The white arrows point out the signal change on T2-weighted imaging. The signal change is present in more than one slice of the MRI. This individual is a 59-year-old male who presents with clumsy hands, impaired upper extremity function, profound spastic gait; essentially marked tetrapariesis. This patient presented with a Nurick grade of 5 and mJOA (modified Japanese Orthopaedic Association) score of 8. Although ambulatory at baseline, he was very disabled with all aspects of functioning and independence.
MRI defines the etiology of canal stenosis and identifies the degree of cord deformation and signal intensity (SI) changes caused by the anatomical spinal structures. Currently, MRI is a tool that contributes to the clinical decision-making process, influences the type of surgery and, more recently, is becoming useful in the prediction of post-operative outcomes (Arvin and others 2011).
MRI Measures of Spinal Cord CompressionThe majority of MRI parameters used are quantitative. These include anteroposterior diameter, compression ratio, and transverse area of the spinal cord (Ahn and oth-ers 2010; Chen and others 2001; Chung and others 2002; Shin and others 2010; Uchida and others 2005; Yamazaki and others 2003). It has been established that the progno-sis for decompressive surgery is unfavorable if the com-pression ratio is less than 0.4 (Fujiwara and others 1989) and the transverse area is less than 45 mm2 (Fukushima and others 1991).
Signal Intensity Change within the Spinal CordCSM often appears as increased intramedullary SI in the cord on T2-weighted images (T2-WI) and as decreased SI on T1-weighted images (T1-WI; Green and others 2012). Both are related to poorer surgical outcomes (Fernandez de Rota and others 2007). Some experts argue that changes on both T2 and T1 indicate irreversibility, chronicity of the disease, and severity of compression (Matsuda and others 1999; Papadopoulos and others 2004; Yagi and others 2010; Yukawa and others 2007). Studies show that intense and well-defined borders of SI changes on T2-WI are associated with more severe histological changes whereas diffuse borders indicate milder changes (Avadhani and others 2010; Chen and others 2001; Uchida and others 2005; Yukawa and others 2007). In addition, the position of SI changes on axial sections has been shown to predict
functional recovery after surgery (Mizuno and others 2003; Shen and others 2009). The specific appearance of irreversible necrosis of gray matter on T2-WI has been named “snake-eye appearance,” which was found to be associated with poor surgical outcomes (Mizuno and oth-ers 2003). Some studies have classified SI changes on T2-WI into focal (when increased SI was confined to one disc level) and multisegmental involvement (more than one disc level; Papadopoulos and others 2004; Wada and others 1995; Wada and others 1999). However, it is reported that MRI is not sufficiently sensitive to detect edema seen as focal T2-WI, whereas the occurrence at multiple levels represents more severe damage, such as a cavitation or necrosis, and is more easily detected. Figure 1 illustrates the presence of
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

Kalsi-Ryan et al. 413
focal T2-weighted signal change, on an MRI of an indi-vidual with profound CSM. In summary, the majority of studies agree that SI changes on T1- and T2-weighted sequences plus the occurrence of SI changes at multi-ple levels are suggestive of a cavity (necrosis) in the spinal cord and poor surgical outcome (Fernandez de Rota and others 2007; Mastronardi and others, 2007; Papadopoulos and others 2004; Park and others 2006; Wada and others 1999).
Although there is no confirmed consensus in the use of MRI parameters and the relationship to clinical pre-sentation, clinicians and scientists agree that MRI is invaluable to the diagnosis of CSM. Ultimately it is the superior method for noninvasive visualization of neural compression. However, MRI findings are only one part of the investigation and should always be considered alongside a thorough neurological examination. Basic studies in animal models of CSM will allow precise correlation between MRI signal changes and the corre-sponding histopathology during progressive compres-sion, which will further progress the field. Furthermore, quantitative neuroimaging methods such as diffusion tensor imaging, fMRI, and MR spectroscopy are cur-rently being developed in traumatic SCI and multiple sclerosis. These techniques show promise for use in defining the cord morphology in CSM noninvasively (Bosma and Stroman 2012; Cadotte and others 2012; Nagashima and others 2010; Rajasekaran and others 2012).
Defining Cervical Spondylotic MyelopathyHistorically, CSM has been defined by the clinical presen-tation of neurological signs and symptoms but, more recently, MRI has also been used to confirm the diagnosis and provide assistance in clinical decision making. However, an internationally accepted definition of CSM does not exist and is desirable to allow for consistency in the international diagnosis, management, and investiga-tion of CSM.
Recent and current studies have defined CSM by the presence of at least one neurological sign and at least one neurological symptom in addition to a positive MRI for compression of the cord. Ultimately, unless all three of these elements are present one cannot be diagnosed with CSM. The signs and symptoms may be present without a positive MRI, which would lead a clinician to look elsewhere for the cause of the deficits. Table 1 provides all possible signs, symptoms, and MRI indicators that would be considered positive indi-cators for CSM. We concur that this current system is useful for the diagnosis of CSM and should continue to be used.
Outcome Measurement
The two most commonly used measures to quantify CSM are the Japanese Orthopedic Association or JOA scale (Hirabayashi and others 1981) and the Nurick grade (Nurick 1972). Both are measures of neurological signs and symptoms that evaluate gait, lower extremity func-tion, hand function, and bladder control. Despite the widespread use of both these outcomes, they lack the sensitivity needed to assess the full range of CSM sever-ity, especially mild cases of CSM. Commonly used self-perceived measures of improvement are the Neck Disability Index and the SF-36 (Short Form Health Survey). These measures have both been validated for use with cervical spine groups and provide adequate information regarding self-perceived functioning. These four outcomes do not, however, assess gait, balance, or hand function in a quantitative or sensitive manner as it may relate to a patient’s ability to function on a daily basis. Thus, a method using surrogate measures to define severity is required in the field to define clinical presenta-tion in a standardized manner.
Currently in our clinical research program, we are studying the use of surrogate functional outcome mea-sures that quantify gait, balance and hand strength, hand function, and self-perceived function. The use of more sensitive measures is necessary to define the milder sub-population within CSM and to define the predictors of progression in the milder population; particularly for those individuals who are not offered surgery at the first diagno-sis of CSM. Use of these surrogate measures will also pro-vide the pertinent information required to establish predictors of recovery and outcome after intervention.
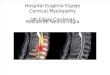
Clinical ManagementTo date, the most common method of treating CSM is by conservative management or performing decompressive surgery. Decompressive surgery is done either from the anterior or posterior approach. Surgery is more com-monly offered to those with moderate to severe presenta-tion of CSM. However, there is an increase in the number of individuals with mild CSM having surgery. Surgical techniques and approaches have evolved over the past 2 decades and, as a result, outcomes are much improved (Mummaneni and others 2009). The choice of surgical technique remains a clinical decision, which varies based on individual patients and clinicians. However, studies have shown close consensus among clinicians in how they select the most beneficial proce-dure for the patient (Anderson and others 2009; Matz and others 2009; Ryken and others 2009). Figure 2 sum-marizes the preoperative and postoperative presentation of an individual with severe CSM. This example outlines
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

414 The Neuroscientist 19(4)
Figure 2. Case vignette, clinical example. This figure presents a 77-year-old male who presented with a 2-year history of arm pain and weakness, numbness, and clumsiness of the hands, and florid spastic gait. Clinical signs were positive for corticospinal distribution motor deficits, atrophy of hand muscles, hyperreflexia, Hoffman’s reflex, plantar response, and spastic gait. The preoperative MRI (left) shows the cause of spinal cord dysfunction; spondylosis at C1 and C2, causing progressive myelopathy. A posterior cervical decompression and instrumented fusion at the levels C1 to C3 was performed. The postoperative MRI (right) defines a posterior and complete decompression. All clinical tests performed show marked improvement. Preoperatively, this individual presented with: Nurick grade of 5, mJOA (modified Japanese Orthopaedic Association) score of 10, Berg Balance Scale of 26/56, 30-m walk test, cadence of 78, time of 52 seconds, and grip strength of 10 kgf. Postoperatively, this individual presented with: Nurick grade of 4, mJOA score of 13, Berg Balance Scale of 41/56, 30-m walk test, cadence of 52, time of 32 seconds, and grip strength of 22 kgf. Ultimately, this individual presented with significant deficits preoperatively and did show marked improvements clinically.
patient presentation and outcome based on the currently available methods of management.
Ultimately, it will be useful to identify predictors of disease progression, as these will allow clinicians to pro-vide intervention before the irreversible sequelae of CSM are manifested. Understanding the natural history of the disease is also valuable in establishing the best course of treatment for each individual patient whether that is a sur-gical approach, medication or a combination of the two.
The benefits of riluzole are currently being studied in the CSM population receiving surgery in a randomized control trial (http://clinicaltrials.gov/ct2/show/NCT01257828). For progress in the clinical field to occur, much work remains in the basic and preclinical fields of CSM
research. This work should be done in parallel with the clinical research to enhance translation as rapidly as pos-sible. The basic and preclinical research for CSM has lagged, secondary to the lack of an adequate animal model of progressive compression, which would allow for surgical decompression.
Pathophysiology and Pathology of Cervical Spondylotic MyelopathyStructural Pathophysiology
A causative relationship between anatomic compression of the neurological structures and the clinical develop-ment of neurological symptoms was recognized in the 19th century (Garrett and others 2011). Cervical spondy-losis results from progressive biomechanical stress and strain on the spinal joints and can be compounded by repetitive trauma. The process that contributes to spondy-losis is noninflammatory disc degeneration that is accom-panied by facet joint osteoarthritis, as well as pathologic changes of the posterior longitudinal ligament (PLL) and ligamentum flavum (hypertrophy, laxity, ossification; Winn 2004).
As part of normal aging, degenerative biochemical changes occur in the disc, which cause biomechanical changes in bone growth. Hypermobility and increase in structure cause infolding and peeling of the PLL leading to hypertrophy and ossification. Loss of disc height causes straightening of the cervical lordosis, eventually leading to kyphosis of the cervical spine. This leads to abnormal cervical spine biomechanics and hypertrophy of the liga-mentum flavum and laxity of the facet joint. Any one, or all, of the following structures can show degeneration: disc, vertebral body, ligamentum flavum, PLL, and facet joint, ultimately leading to narrowing of the spinal canal and subsequent cord compression in a portion of those who have degenerative changes in the spine.
Pathogenesis of neural structures can be subdivided into three main components that are responsible for the final cord changes. The first component is the static fac-tors: structural changes that cause canal stenosis and cord compression. The second is dynamic factors character-ized by repetitive movement of the compressed cord; the third factor is the histopathological and vascular changes causing ischemia and rearrangement of blood supply, infarction, oligodendrocyte apoptosis, and other cyto-toxic cell changes (Winn 2011).
PathologyThe mechanical compression and hypothesized restriction placed on the spinal cord microvasculature likely results in cystic cavitation, gliosis, central gray and medial white
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

Kalsi-Ryan et al. 415
matter degeneration, Wallerian degeneration of posterior columns and posterolateral tracts and anterior horn cell loss (Table 2; Bohlman and Emery 1988; Fehlings and Skaf 1998; Swagerty 1994). Although these neuropathological features have been well characterized in human CSM, little is known regarding how chronic compression can account for the intriguing neurological deficits of both upper and lower extremities in CSM. Furthermore, it is unclear to what extent plasticity may be induced with chronic pro-gressive compression in the cervical enlargement.
Current Knowledge in Cervical Spondylotic Myelopathy Pathobiology
Based on work done in acute SCI models, it has been postulated that a similar series of cellular and molecular secondary injury events, including glutamatergic excito-toxicity, free radical generation, lipid peroxidation, inflammation, and ischemia play a key role in the patho-biology of CSM. Although acute SCI models may pro-vide some insight into the mechanisms of CSM, this slow progressive condition is unique from previously studied acute CNS injuries. Although it has been thought that histopathologic and pathophysiologic similarities between CSM and traumatic SCI are sufficient to extrap-olate from the latter to the former, CSM is unique and its pathomechanisms remain unexplored. A clear limitation to advancing the field had been the lack of a reliable animal model of progressive compression of the cervical spinal cord. We believe that the recently developed rat CSM model, which duplicates the neuropathological features and deficits of the human disease as well as being MRI compatible and allowing for surgical decom-pression, will facilitate the elucidation of the molecular mechanisms of CSM and will be the platform for many translationally oriented studies (Karadimas and others 2012c). A summary of the current knowledge related to the pathomechanisms of the disease is presented in Figure 3.
Compromise of Spinal Cord Microvasculature
There is considerable evidence to indicate that the chronic interruption of the vascular supply to the spinal cord may be a significant component in the origin and pathophysiology of CSM and the potential determinant of its natural course. Postmortem studies (Baron and Young 2007) in CSM patients demonstrating abnormal histologi-cal findings, such as spinal cord necrosis and gray matter cavitations, have indicated spinal cord ischemia as a potential mechanism in CSM. This is further supported by the fact that the region of the spinal cord most affected by CSM (levels C5 to C7) is also the area with the most vulnerable vascular supply (Baron and Young, 2007;
Table 2. Main Histopathological Characteristics of Cervical Spondylotic Myelopathy.
Central gray matter degenerationMedial white matter degenerationWallerian degeneration of the posterior columns and posterolateral tracts
Cystic cavitationGliosisAtrophy of the anterior hornsAnterior horn cell loss
Figure 3. Current knowledge about cervical spondylotic myelopathy (CSM). Progressive compression of the cervical spinal cord causes a chronic hypoxic/ischemic insult that damages oligodendrocytes (oligo) and neurons, eliciting an inflammatory response. Furthermore, the compression-induced ischemic state leads to endothelial cell loss—disrupting the neurovascular unit (NVU) and leading to compromise of the blood–spinal cord barrier (BSCB). BSCB permeability and inflammation have been demonstrated in the chronic stages of CSM. Inflammation can potentiate the initial cellular loss and BSCB permeability. It is thought that the enhanced cross talk between the peripheral immune system and the spinal cord microenvironment, which occurs in CSM through the impaired BSCB, potentiates inflammation. Moreover, it has been suggested that inflammatory Fas ligand (FasL) signaling can lead to apoptosis of neurons and oligodendrocytes. Neuronal loss and axonal damage are responsible for the upper limb dysfunction, spasticity, and gait disturbances seen in humans with CSM.
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

416 The Neuroscientist 19(4)
Firooznia and others 1985; Yue and others 2001). Several studies have reported evidence of ischemia in animal models of CSM based on microangiography, autoradio-graphy, and hydrogen clearance (Fehlings and Skaf 1998). It has also been shown that spinal cord hypoperfu-sion in combination with chronic compression could induce myelopathy in dogs. Although these experimental observations support the vascular hypothesis in CSM, they are not representative of human spondylotic myelop-athy. Recently, Kurokawa and others (2010) showed that the ratio between the blood flow of the C5-C6 segment to that of the C3-C4 segment was significantly lower in a group that underwent 12 weeks of compression at the C5-C6 level compared with the sham group. Unfortunately, the authors did not correlate the decrease in blood flow with histopathological findings and did not compare the absolute numbers of the blood flow in the rostral and caudal segments adjacent to the compression epicenter between the compression and control groups.
A key consequence of CSM is the progressive com-pression that causes flattening and widening of the spinal cord. This mechanical distortion may stretch the intrinsic transverse vessels or terminal branches of the anterior spinal artery resulting in endothelial cell loss and dys-function (Bohlman and Emery 1988). Although endothe-lial cells are more resistant than neurons or glia to injury (Kinouchi and others 1993), hypoxia-ischemia–induced endothelial cell death or injury may exacerbate primary tissue damage and contribute to breakdown of the blood–spinal cord barrier (BSCB), leading to increased vascular permeability and vasogenic spinal cord edema. The BSCB includes endothelial cells joined with tight junction pro-teins, basal lamina, pericytes, and astrocytic end feet—forming what is called a neurovascular unit. BSCB permeability in CNS injuries is typically seen as a detri-mental event that damages the CNS through increased edema and entry of blood-borne toxic/inflammatory sub-stances. Following acute neurotrauma, the BSCB remains compromised long after the initial damage because of the effects of inflammatory mediators on endothelial cells and loss of endothelial cells. However, this barrier is eventu-ally reformed (Loy and others 2002; Noble and Wrathall 1989). Karadimas and others (2012c) in a recent study using a novel rat model of CSM showed that the progres-sive chronic cervical spinal cord compression causes sig-nificant endothelial cell loss. Of note, additional results from the same study demonstrate BSCB permeability at chronic stages following the onset of compression in this model suggesting that the dynamics of BSCB permeabil-ity in CSM—and the underlying mechanisms—could be unique to this chronic condition. However, the mecha-nisms of microvascular dysfunction, chronic BSCB dis-ruption, and the associated neuroinflammatory changes have yet to be fully elucidated in animal models of CSM.
Glutamate Excitotoxicity
Glutamate is the major excitatory neurotransmitter in the mammalian CNS. To date, research suggests that gluta-mate excitotoxicity caused by an increase in the extracel-lular level of glutamate is involved in neuronal and oligodendrocytic death in acute and chronic neurologic diseases including stroke, traumatic SCI, and prolonged seizure activity (Fehlings and Skaf 1998). This mechanism of slow glutamate excitotoxicity may be involved in neu-ronal death in chronic neurodegenerative diseases such as mitochondrial encephalomyelopathies, Huntington’s dis-ease, spinocerebellar degeneration syndromes, and motor neuron diseases such as amyotrophic lateral sclerosis (Fehlings and Skaf 1998). It has also been hypothesized that the slow glutamate excitotoxicity plays an important role in initiating neuronal degeneration and promoting the development of neurological deficits under the chronic progressive compression of the cervical spinal cord (Fehlings and Skaf 1998).
Riluzole, the only Food and Drug Administration–approved pharmacotherapy for amyotrophic lateral scle-rosis, is thought to decrease glutamate excitotoxicity by blocking glutamate receptors and by increasing glutamate transporter activity. Recently, riluzole was administered daily for 5 weeks after the onset of symptoms in a preclini-cal experimental animal model of CSM (Karadimas and others 2012b). The results of this study showed that admin-istration of Riluzole led to significant functional improve-ment, axonal preservation, attenuation of astrogliosis, and decreased levels of neuronal apoptosis after chronic pro-gressive compression. Furthermore, the authors demon-strated that administration of riluzole, combined with surgical decompression, resulted in restoration of a normal, smooth, and rhythmic gait pattern in the animals, robust preservation of the main corticospinal tracts, and signifi-cantly decreased astrogliosis and neuronal apoptosis compared with the decompressive surgery-only group. These results provide evidence that, in the chronic hypoxic/ischemic state of CSM, a slow glutamate excito-toxicity process is activated which is involved in neuro-nal degeneration. Finally, this study demonstrated, for the first time, the potential use of a neuroprotective agent in CSM as an adjuvant to surgical decompression. This informs and supports the CSM Protect clinical trial, which will examine the synergistic effects of decompres-sive surgery and riluzole in CSM in humans.
ApoptosisApoptosis is programmed cell death, which begins with signal cascades and ends in patterned DNA fragmenta-tion. The technique known as terminal deoxynucleotidyl transferase–mediated deoxyuridine triphosphate nick-end
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

Kalsi-Ryan et al. 417
labeling (TUNEL) can be used to find evidence of apop-totic DNA fragmentation. The induction of apoptosis in the chronically compressed cervical spinal cord has been well characterized. TUNEL-positive neurons and oligo-dendrocytes and caspase-3 positive neurons and oligo-dendrocytes were detected in chronically compressed cervical spinal cords of an autopsied patient with CSM and mice exhibiting chronic spinal cord compression (Yu and others 2009). These findings add to the evidence that apoptosis in neurons and oligodendrocytes contributes to the pathobiology of CSM. However, the signal pathway of apoptosis in the chronically compressed cervical spi-nal cord remains unclear. Yu and others (2011) found evidence in human tissue and twy/twy mice of increased Fas ligand–mediated apoptosis of neurons and oligoden-drocytes; these experiments showed that neutralizing the Fas-ligand with an antibody improves functional neuro-logical recovery. Recent work also implicates tumor necrosis factor–α as an external signal in initiating apoptosis (Inukai and others 2009). Moreover, Takenouchi and others (2008) demonstrated that the mitogen-activated protein kinase pathways, including ASK-1, p-38, and JNK, which are intracellular signaling systems inducing optimal stress responses, are activated in neurons and oligodendrocytes during chronic cervical spinal cord compression. Thus, further work is required to identify the signal pathway of spinal cord cell apopto-sis to establish methods to intervene.
NeuroinflammationAlthough the inflammatory response to a CNS injury is integral to wound healing (Bomstein and others 2003; Popovich and others 2002; Shaked and others 2004), there is compelling evidence that neuroinflammation is a critical player in the pathomechanisms of cell death fol-lowing neurotrauma. One might assume that CSM and acute SCI share the same inflammatory profiles; however, it is now becoming apparent that there are many differ-ences in the innate and adaptive immune responses to acute SCI versus CSM. Beattie and Manley (2011) reported that the inflammatory process is unique in CSM in that it is slow and driven by chronic progressive com-pression. However, little is known regarding the temporal profile of cellular inflammation, the temporal profile of key inflammatory mediators and what aspects of inflam-mation are beneficial or detrimental in this unique chronic condition. Insight into the nature of inflammatory responses to chronic spinal cord compression will pro-vide the basis for development of therapeutics that alter elements of inflammation accordingly.
Recently, Yu and others (2011) showed that the chronic spinal cord compression seen in patients with CSM causes cellular inflammation and that neutrophils, activated
monocytes/macrophages, and lymphocytes are recruited to the lesion in human CSM. Furthermore, the results from Yu and others suggest that, even in slow progressive injuries of the cervical spinal cord, a reduction of inflam-mation leads to less apoptosis and possibly less demyelin-ation and consequent axonal damage. However, there is much left to learn about this progressive disorder and the role of the innate and adaptive immune response in the development of myelopathy.
Matrix metaloproteinases (MMPs) are important for extracellular matrix remodeling and are integral to mor-phogenesis, inflammation, and wound healing. It has been observed that there are reduced numbers of neutrophils in the acute injured spinal cord in MMP-9-depleted mice, a finding consistent with the role of MMP-9 in the transmi-gration of neurotrophils from the vascular component (Noble and others 2002). Moreover, administration of an MMP-9 inhibitor was highly effective in blocking neutro-phil administration and tissue damage when administered hours after injury (Noble and others 2002). This suggests that MMP-9 plays a significant role in the sustained phases of inflammatory cell recruitment. Moreover, MMP-9 has been implicated in promoting blood-brain barrier disrup-tion and subsequent exaggeration of the inflammatory process in different CNS diseases. Interestingly, a recent study on a new rabbit model of CSM (Klironomos and others 2011) revealed that the MMP-9 immunoreactivity was significantly higher in spinal cord tissue from rabbits that underwent chronic compression of the cervical spinal cord for 20 weeks (Karadimas and others 2012a). Unfortunately, these authors did not evaluate the role of MMP-9 under the chronic progressive compression of the cervical spinal cord by blocking or deleting MMP-9.
Compensatory Changes in the Chronically Compressed Spinal CordNeurotrophic factors are proteins that regulate neuronal survival, axonal growth, and synaptic plasticity. Neurotrophic factors have been widely used to promote axonal regeneration in the injured CNS. Several studies report structural regeneration associated with partial func-tional recovery after the administration of the neuro-trophic factors brain-derived neurotrophic factor (BDNF) or neurotrophin-3 (NT-3; Jones and others 2001). A recent study on the twy/twy mouse model of CSM revealed that the expression levels of BDNF, NT-3, and their receptors were significantly higher at the rostral and caudal sites immediately adjacent to the maximal compression site in comparison with their expression at normal and less or noncompressed sites (Uchida and others 2003). These findings are consistent with the increased number of neu-rons and oligodendrocytes rostral and caudal to the injury epicenter (Yu and others 2009) and together suggest that
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

418 The Neuroscientist 19(4)
BDNF and NT-3 may contribute to neuronal and oligo-dendrocyte survival in CSM. Moreover, it has been indi-cated that targeted retrograde adenovirus (AdV)-NT-3 gene and AdV-BDNF-gene transfections are feasible in twy/twy mouse and that NT-3 and BDNF enhance sur-vival and regeneration of anterior horn cells and provoke elongation of neurites even under chronic mechanical compression of the spinal cord (Uchida and others 2008; Xu and others 2006).
Growth-associated protein 43 (GAP-43) is a protein synthesized in the nerve cell bodies and quickly trans-ported in axons. It is located at the cytoplasmic side of the plasma membrane of axons and growth cones and is a component of the membrane skeleton of such cones. GAP-43 is usually expressed in neurons during develop-ment and in some regenerating axons. Therefore, it is considered to be implicated in axonal growth and regen-eration (Li and others 1996). Using a rat model of acute compressive injury, Li and others (1996) reported that the mode and the extent of GAP-43 expression var-ied with the degree of injury. In line with this report, Uchida and others (2002) demonstrated increased GAP-43 immunoreactivity in spinal cord tissue coming from twy/twy mice, which was well correlated with the mag-nitude and the period of the chronic compression. These results suggest that regeneration of axons and the mecha-nisms involved in axonal repair may occur in the white matter during the chronic compression. This evidence collectively reveals that the cervical spinal cord tries to adapt and compensate against the chronic, slow and pro-gressive compression. However, further research is required to reveal any potential endogenous compensa-tory mechanisms in the cervical spinal cord during the compression phase.
ConclusionCSM is the most common cause of spinal cord dysfunc-tion among adults older than 55 years (Young 2000) and is the key underlying risk factor predisposing patients to traumatic central cord syndrome. Clearly, as the popula-tion ages, the frequency of CSM will continue to increase; however, the unique features of CSM versus other causes of spinal cord dysfunction are understud-ied. The development of animal models of slow com-pressive injury to the cervical spinal cord, such as that currently being characterized in Fehlings’s lab, is imperative to provide a means for discovering the molecular mechanisms of CSM and for evaluating therapeutic strategies that will complement surgical decompression for this increasingly important clinical entity. In our opinion, the study of pathomechanisms and plasticity in the cervical enlargement under the slow progressive compression could pave the way for new cellular treatments in CSM and other diseases of
the spinal cord. Communication between clinician-sci-entists and translationally oriented basic scientists is a key element that will move the field forward in estab-lishing more appropriate and sensitive methods to quan-tify CSM in humans, establish a more formal understanding of disease progression and determine new methods of detection and intervention.
Acknowledgments
We acknowledge the assistance of J. Mary Yang and Alina Karpova in writing this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Ahn JS, Lee JK, Kim BK. 2010. Prognostic factors that affect the surgical outcome of the laminoplasty in cervical spon-dylotic myelopathy. Clin Orthop Surg 2:98–104.
Anderson PA, Matz PG, Groff MW, Heary RF, Holly LT, Kaiser MG, and others. 2009. Joint section on disorders of the spine and peripheral nerves of the American Association of Neurological Surgeons and Congress of Neurological Surgeons. J Neurosurg Spine 11(2):150-6.
Arvin B, Kalsi-Ryan S, Karpova A, Mercier D, Furlan JC, Massicotte EM, and others. 2011. Postoperative magnetic resonance imaging can predict neurological recovery after surgery for cervical spondylotic myelopathy: a prospective study with blinded assessments. Neurosurgery 69:362–8.
Avadhani A, Rajasekaran S, Shetty AP. 2010. Comparison of prognostic value of different MRI classifications of signal intensity change in cervical spondylotic myelopathy. Spine J 10:475–85.
Barnes MP, Saunders M. 1984. The effect of cervical mobility on the natural history of cervical spondylotic myelopathy. J Neurol Neurosurg Psychiatry 47:17–20.
Baron EM, Young WF. 2007. Cervical spondylotic myelopathy: a brief review of its pathophysiology, clinical course, and diagnosis. Neurosurgery 60(1 suppl 1):S35–41.
Beattie MS, Manley GT. 2011. Tight squeeze, slow burn: inflam-mation and the aetiology of cervical myelopathy. Brain 134:1259–61.
Boden SD, McCowin PR, Davis DO, Dina TS, Mark AS, Wiesel S. 1990. Abnormal magnetic-resonance scans of the cervical spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am 72:1178–84.
Bohlman HH, Emery SE. 1988. The pathophysiology of cer-vical spondylosis and myelopathy. Spine (Phila Pa 1976) 13:843–6.
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

Kalsi-Ryan et al. 419
Bomstein Y, Marder J, Vitner K, Smirnov I, Lisaey G, Butovsky O, and others. 2003. Features of skin-coincubated macro-phages that promote recovery from spinal cord injury. J Neuroimmunol 142:10–6.
Bosma R, Stroman PW. 2012. Diffusion tensor imaging in the human spinal cord: development, limitations, and clinical applications. Crit Rev Biomed Eng 40:1–20.
Cadotte DW, Stroman PW, Mikulis D, Fehlings MG. 2012. A systematic review of spinal fMRI research: outlining the elements of experimental design. J Neurosurg Spine 17:102–18.
Chen CJ, Lyu RK, Lee ST, Wong YC, Wang LJ. 2001. Intra-medullary high signal intensity on T2-weighted MR images in cervical spondylotic myelopathy: prediction of prognosis with type of intensity. Radiology 221:789–94.
Chung SS, Lee SS, Chung KH. 2002. Factors affecting the sur-gical results of expansive laminoplasty for cervical spondy-lotic myelopathy. Int Orthop 26:334–8.
Epstein JA, Carras R, Hyman RA, Costa S. 1979. Cervical myelopathy caused by developmental stenosis of the spinal canal. J Neurosurg 51:362–7.
Epstein N, Epstein J, Carras R. 1987. Cervical spondyloste-nosis and related disorders in patients over 65: current management and diagnostic techniques. Orthotransactions 11:15.
Fehlings MG, Skaf G. 1998. A review of the pathophysiology of cervical spondylotic myelopathy with insights for potential novel mechanisms drawn from traumatic spinal cord injury. Spine (Phila Pa 1976) 23:2730–7.
Fernandez de Rota JJ, Meschian S, Fernandez de Rota A, Urbano V, Baron M. 2007. Cervical spondylotic myelopa-thy due to chronic compression: the role of signal intensity changes in magnetic resonance images. J Neurosurg Spine 6:17–22.
Firooznia H, Ahn JH, Rafii M, Ragnarsson KT. 1985. Sudden quadriplegia after a minor trauma. The role of preexisting spinal stenosis. Surg Neurol 23:165–8.
Fujiwara K, Yonenobu K, Ebara S, Yamashita K, Ono K. 1989. The prognosis of surgery for cervical compression myelop-athy. An analysis of the factors involved. J Bone Joint Surg Br 71:393–8.
Fukushima T, Ikata T, Taoka Y, Takata S. 1991. Magnetic reso-nance imaging study on spinal cord plasticity in patients with cervical compression myelopathy. Spine (Phila Pa 1976) 16(10 suppl):S534–8.
Garrett M, Bartolomei J, Sonntag VKH. 2011. Anterior approach for cervical spondylotic myelopathy. In: Winn HR, editor. Youmans neurological surgery, vol. 3. Philadel-phia: Elsevier. p 2876–87.
Gemici C. 2010. Lhermitte’s sign: review with special emphasis in oncology practice. Crit Rev Oncol Hematol 74:79–86.
Gore DR, Sepic SB, Gardner GM. 1986. Roentgenographic findings of the cervical spine in asymptomatic people. Spine (Phila Pa 1976) 11:521–4.
Gorter K. 1976. Influence of laminectomy on the course of cer-vical myelopathy. Acta Neurochir (Wien) 33:265–81.
Green C, Butler J, Eustace S, Poynton A, O’Byrne JM. 2012. Imaging modalities for cervical spondylotic stenosis and myelopathy. Adv Orthop 2012:908324.
Hattori T, Sakakibara R, Yasuda K, Murayama N, Hirayama K. 1990. Micturitional disturbance in cervical spondylotic myelopathy. J Spinal Disord 3:16–8.
Hirabayashi K, Miyakawa J, Satomi K, Maruyama T, Wakano K. 1981. Operative results and postoperative progression of ossification among patients with ossification of cervical pos-terior longitudinal ligament. Spine (Phila Pa 1976) 6:354–64.
Holly LT, Dong Y, Albistegui-DuBois R, Marehbian J, Dobkin B. 2007. Cortical reorganization in patients with cervical spon-dylotic myelopathy. J Neurosurg Spine 6:544–51.
Inukai T, Uchida K, Nakajima H, Yayama T, Kobayashi S, Mwaka ES, and others. 2009. Tumor necrosis factor-alpha and its receptors contribute to apoptosis of oligodendro-cytes in the spinal cord of spinal hyperostotic mouse (twy/twy) sustaining chronic mechanical compression. Spine (Phila Pa 1976) 34:2848–57.
Jones LL, Oudega M, Bunge MB, Tuszynski MH. 2001. Neuro-trophic factors, cellular bridges and gene therapy for spinal cord injury. J Physiol 533:83–9.
Karadimas SK, Klironomos G, Papachristou DJ, Papanikolaou S, Papadaki E, Gatzounis G. 2012a. Immunohistochemical profile of NF-κB/p50, NF-κB/p65, MMP-9, MMP-2 and u-PA in experimental cervical spondylotic myelopathy. Spine (Phila Pa 1976) Jun 5 [Epub ahead of print]
Karadimas SK, Moon ES, Fehlings MG. 2012b. The sodium channel/gluatamate blocker riluzole is complementary to decompression in a preclinical experimental model of cervi-cal spondylotic myelopathy (CSM): implications for trans-lational clinical application. Neurosurgery 71:E543.
Karadimas SK, Moon ES, Satkunendrarajah K, Fehlings MG. 2012c. Novel animal model of cervical spondylotic myelop-athy: an opportunity to identify new therapeutic targets. 28th Annual Meeting of the AANS/CNS Section on the Dis-orders of the Spine and Peripheral Nerves, Orlando, Florida.
King JT Jr, McGinnis KA, Roberts MS. 2003. Quality of life assessment with the medical outcomes study short form-36 among patients with cervical spondylotic myelopathy. Neu-rosurgery 52:113–20.
Kinouchi H, Sharp FR, Hill MP, Koistinaho J, Sagar SM, Chan PH. 1993. Induction of 70-kDa heat shock protein and hsp70 mRNA following transient focal cerebral ischemia in the rat. J Cereb Blood Flow Metab 13:105–15.
Klironomos G, Karadimas S, Mavrakis A, Mirilas P, Savvas I, Papadaki E, and others. 2011. New experimental rabbit animal model for cervical spondylotic myelopathy. Spinal Cord 49:1097–102.
Kurokawa R, Murata H, Ogino M, Ueki K, Kim P. 2010. Altered blood flow distribution in the rat spinal cord under chronic compression. Spine (Phila Pa 1976) 36:1006–9.
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

420 The Neuroscientist 19(4)
Lee MJ, Cassinelli EH, Riew KD. 2007. Prevalence of cervi-cal spine stenosis. Anatomic study in cadavers. J Bone Joint Surg Am 89:376–80.
Lees F, Turner JW. 1963. Natural history and prognosis of cervi-cal spondylosis. BMJ 2:1607–10.
Li GL, Farooque M, Holtz A, Olsson Y. 1996. Increased expres-sion of growth-associated protein 43 immunoreactivity in axons following compression trauma to rat spinal cord. Acta Neuropathol 92:19–26.
Loy DN, Crawford CH, Darnall JB, Burke DA, Onifer SM, Whittemore SR. 2002. Temporal progression of angiogen-esis and basal lamina deposition after contusive spinal cord injury in the adult rat. J Comp Neurol 445:308–24.
Lunsford LD, Bissonette DJ, Zorub DS. 1980. Anterior surgery for cervical disc disease. Part 2: treatment of cervical spon-dylotic myelopathy in 32 cases. J Neurosurg 53:12–9.
Mastronardi L, Elsawaf A, Roperto R, Bozzao A, Caroli M, Ferrante M, and others. 2007. Prognostic relevance of the postoperative evolution of intramedullary spinal cord changes in signal intensity on magnetic resonance imag-ing after anterior decompression for cervical spondylotic myelopathy. J Neurosurg Spine 7:615–22.
Matsuda Y, Shibata T, Oki S, Kawatani Y, Mashima N, Oishi H. 1999. Outcomes of surgical treatment for cervical myelopa-thy in patients more than 75 years of age. Spine (Phila, Pa 1976) 24:529–34.
Matsunaga S, Sakou T. 2006. OPLL: disease entity, incidence, lit-erature search and prognosis. In: Yonenobu K, Nakamura K, Toyama Y, editors. OPLL: ossification of the posterior longi-tudinal ligament. 2nd edition. New York: Springer. p 11–7.
Matz PG, Anderson PA, Holly LT, Groff MW, Heary RF, Kaiser MG, and others. 2009. The natural history of cervi-cal spondylotic myelopathy. J Neurosurg Spine 11:104–11.
Mizuno J, Nakagawa H, Inoue T, Hashizume Y. 2003. Clinico-pathological study of “snake-eye appearance” in compres-sive myelopathy of the cervical spinal cord. J Neurosurg Spine 2:162–8.
Moore AP, Blumhardt LD. 1997. A prospective survey of the causes of non-traumatic spastic paraparesis and tetraparesis in 585 patients. Spinal Cord 35:361–7.
Mummaneni PV, Kaiser MG, Matz PG, Anderson PA, Groff MW, Heary RF, and others. 2009. Cervical surgi-cal techniques for the treatment of cervical spondylotic myelopathy. J Neurosurg Spine 11:130–41.
Nagashima H, Morio Y, Meshitsuka S, Yamane K, Nanjo Y, Teshima R. 2010. High-resolution nuclear magnetic reso-nance spectroscopic study of metabolites in the cerebrospi-nal fluid of patients with cervical myelopathy and lumbar radiculopathy. Eur Spine J 19:1363–8.
Noble LJ, Donovan F, Igarashi T, Goussev S, Werb Z. 2002. Matrix metalloproteinases limit functional recovery after spinal cord injury by modulation of early vascular events. J Neurosci 22:7526–35.
Noble LJ, Wrathall JR. 1989. Distribution and time course of protein extravasation in the rat spinal cord after contusive injury. Brain Res 482:57–66.
Northover JR, Wild JB, Braybrooke J, Blanco J. 2012. The epidemiology of cervical spondylotic myelopathy. Skeletal Radiol 41:1543–6.
Nurick S. 1972. The pathogenesis of the spinal cord disorder associated with cervical spondylosis. Brain 95:87–100.
Ono K, Ebara S, Fuji T, Yonenobu K, Fujiwara K, Yamashita K. 1987. Myelopathy hand. New clinical signs of cervical cord damage. J Bone Joint Surg Br 69:215–9.
Oshima Y, Seichi A, Takeshita K, Chikuda H, Ono T, Baba S, and others. 2012. Natural course and prognostic factors in patients with mild cervical spondylotic myelopathy with increased signal intensity on T2-weighted magnetic reso-nance imaging. Spine (Phila Pa 1976) 37:1909–13.
Papadopoulos CA, Katonis P, Papagelopoulos PJ, Karampekios S, Hadjipavlou AG. 2004. Surgical decompression for cer-vical spondylotic myelopathy: correlation between opera-tive outcomes and MRI of the spinal cord. Orthopedics 27:1087–91.
Park YS, Nakase H, Kawaguchi S, Sakaki T, Nikaido Y, Morim-oto T. 2006. Predictors of outcome of surgery for cervical compressive myelopathy: retrospective analysis and pro-spective study. Neurol Med Chir (Tokyo) 46(5):231–8.
Patel AA, Spiker WR, Daubs M, Brodke DS, Cannon-Albright LA. 2012. Evidence of an inherited predisposition for cervi-cal spondylotic myelopathy. Spine (Phila Pa 1976) 37:26–9.
Popovich PG, Guan Z, McGaughy V, Fisher L, Hickey WF, Basso DM. 2002. The neuropathological and behavioral consequences of intraspinal microglial/macrophage activa-tion. J Neuropathol Exp Neurol 61:623–33.
Rajasekaran S, Kanna RM, Shetty AP. 2012. Diffusion tensor imaging of the spinal cord and its clinical applications. J Bone Joint Surg Br 94:1024–31.
Ryken TC, Heary RF, Matz PG, Anderson PA, Groff MW, Holly LT, and others. 2009. Joint section on disorders of the spine and peripheral nerves of the American Association of Neurological Surgeons and Congress of Neurological Sur-geons. J Neurosurg Spine 11(2):142-9.
Sadasivan KK, Reddy RP, Albright JA. 1993. The natural his-tory of cervical spondylotic myelopathy. Yale J Biol Med 66:235–42.
Shaked I, Porat Z, Gersner R, Kipnis J, Schwarz M. 2004. Early activation of microglia as antigen presenting cells correlates with T cell-mediated protection and repair of the injured central nervous system. J Neuroimmunol 146:84–93.
Shen HX, Li L, Yang ZG, Hou TS. 2009. Position of increased signal intensity in the spinal cord on MR images: does it predict the outcome of cervical spondylotic myelopathy? Chin Med J (Engl) 122:1418–22.
Shimomura T, Sumi M, Nishida K, Maeno K, Tadokoro K, Miyamoto H, and others. 2007. Prognostic factors for
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

Kalsi-Ryan et al. 421
deterioration of patients with cervical spondylotic myelop-athy after nonsurgical treatment. Spine (Phila Pa 1976) 32:2474–9.
Shin JJ, Jin BH, Kim KS, Cho YE, Cho WH. 2010. Intramedul-lary high signal intensity and neurological status as prog-nostic factors in cervical spondylotic myelopathy. Acta Neurochir (Wien) 10:1687–94.
Swagerty DL Jr. 1994. Cervical spondylotic myelopathy: a cause of gait disturbance and falls in the elderly. Kans Med 95:226–7.
Symon L, Lavender P. 1967. The surgical treatment of cervical spondylotic myelopathy. Neurology 17:117–27.
Takenouchi T, Setoguchi T, Yone K, Komiya S. 2008. Expres-sion of apoptosis signal-regulating kinase 1 in mouse spi-nal cord under chronic mechanical compression: possible involvement of the stress-activated mitogen-activated pro-tein kinase pathways in spinal cord cell apoptosis. Spine (Phila Pa 1976) 33:1943–50.
Tam S, Barry RL, Bartha R, Duggal N. 2010. Changes in func-tional magnetic resonance imaging cortical activation after decompression of cervical spondylosis: case report. Neuro-surgery 67:E863–4.
Tracy JA, Bartleson JD. 2010. Cervical spondylotic myelopa-thy. Neurologist 16:176–87.
Uchida K, Baba H, Maezawa Y, Furukawa S, Omiya M, Kokubo Y, and others. 2003. Increased expression of neuro-trophins and their receptors in the mechanically compressed spinal cord of the spinal hyperostotic mouse (twy/twy). Acta Neuropathol 106:29–36.
Uchida K, Baba H, Maezawa Y, Kubota C. 2002. Progressive changes in neurofilament proteins and growth-associated protein-43 immunoreactivities at the site of cervical spinal cord compression in spinal hyperostotic mice. Spine (Phila Pa 1976) 27:480–6.
Uchida K, Nakajima H, Inukai T, Takamura T, Kobayashi S, Furukawa S, and others. 2008. Adenovirus-mediated ret-rograde transfer of neurotrophin-3 gene enhances survival of anterior horn neurons of twy/twy mice with chronic mechanical compression of the spinal cord. J Neurosci Res 86:1789–800.
Uchida K, Nakajima H, Sato R, Kokubo Y, Yayama T, Kobayashi S, and others. 2005. Multivariate analysis of the neurological outcome of surgery for cervical compressive myelopathy. J Orthop Sci 10:564–73.
van Middendorp JJ, Pouw MH, Hayes KC, Williams R, Chhabra HS, Putz C, and others. 2010. Diagnostic criteria of
traumatic central cord syndrome. Part 2: a questionnaire sur-vey among spine specialists. Spinal Cord 48:657–63.
Wada E, Ohmura M, Yonenobu K. 1995. Intramedullary changes of the spinal cord in cervical spondylotic myelopa-thy. Spine 20:2226–32.
Wada E, Yonenobu K, Suzuki S, Kanazawa A, Ochi T. 1999. Can intramedullary signal change on magnetic resonance imaging predict surgical outcome in cervical spondylotic myelopathy? Spine 24:455–61.
Winn HR. 2004. Youmans Neurological Surgery, 5th ed. Phila-delphia (PA): Saunders.
Xu K, Uchida K, Nakajima H, Kobayashi S, Baba H. 2006. Targeted retrograde transfection of adenovirus vector car-rying brain-derived neurotrophic factor gene prevents loss of mouse (twy/twy) anterior horn neurons in vivo sustain-ing mechanical compression. Spine (Phila Pa 1976) 31: 1867–74.
Yagi M, Ninomiya K, Kihara M, Horiuchi Y. 2010. Long-term surgical outcome and risk factors in patients with cervical myelopathy and a change in signal intensity of intramedul-lary spinal cord on magnetic resonance imaging. J Neuro-surg Spine 12:59–65.
Yamazaki T, Yanaka K, Sato H, Uemura K, Tsukada A, Nose T. 2003. Cervical spondylotic myelopathy: surgical results and factors affecting outcome with special reference to age dif-ferences. Neurosurgery 52:122–6.
Young WF. 2000. Cervical spondylotic myelopathy: a common cause of spinal cord dysfunction in older persons. Am Fam Physician 62:1064–70.
Yu WR, Baptiste DC, Liu T, Odrobina E, Stanisz GJ, Fehlings MG. 2009. Molecular mechanisms of spinal cord dys-function and cell death in the spinal hyperostotic mouse: implications for the pathophysiology of human cervical spondylotic myelopathy. Neurobiol Dis 33:149–63.
Yu WR, Liu T, Kiehl TR, Fehlings MG. 2011. Human neuro-pathological and animal model evidence supporting a role for Fas-mediated apoptosis and inflammation in cervical spondylotic myelopathy. Brain 134:1277–92.
Yue WM, Tan SB, Tan MH, Koh DC, Tan CT. 2001. The Torg–Pavlov ratio in cervical spondylotic myelopathy: a com-parative study between patients with cervical spondylotic myelopathy and a nonspondylotic, nonmyelopathic popula-tion. Spine (Phila Pa 1976) 26:1760–4.
Yukawa Y, Kato F, Yoshihara H, Yanase M, Ito K. 2007. MR T2 image classification in cervical compression myelopathy. Spine (Phila Pa 1976) 32:1675–8.
at St Petersburg State University on January 8, 2014nro.sagepub.comDownloaded from

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具