Embed Size (px)
Citation preview
Challenging bureaucracy

The NHS ConfederationThe NHS Confederation represents all organisationsthat commission and provide NHS services. It is theonly membership body to bring together and speak onbehalf of the whole of the NHS.
We help the NHS to guarantee high standards ofcare for patients and best value for taxpayers byrepresenting our members and working together withour health and social care partners.
We make sense of the whole health system, influencehealth policy, support our members to share andimplement best practice, and deliver industry-widesupport functions for the NHS.
www.nhsconfed.org
The voice of NHS leadership
For more information on our work,please contact:
The NHS Confederation50 Broadway London SW1H 0DBTel 020 7799 6666Email [email protected]
Published by the NHS Confederation © The NHS Confederation 2013You may copy or distribute this work, but you must give the author credit, you maynot use it for commercial purposes, and you may not alter, transform or build uponthis work.Registered Charity no: 1090329
BOK60069
Cover image taken from the NHS Confederation’s animation‘Reducing bureaucracy in the NHS’.

Letter to the Secretary of State 2
Key findings and recommendations 4
Introduction 6
What is bureaucracy? When is it a burden? 8
Managing the size of the burden 10
The cost of reporting 10
The impact of data requests 12
The trend 14
Clarifying responsibilities and definitions 15
Managing the volume better 18
Reducing the effort needed to manage information requests 23
Variation between providers 23
Increasing the value of information 27
Using data to improve care 27
Recommendations for further work 32
Conclusion: a three-part task 33
Acknowledgements 34
Further reading 35
Annex 1 – Table of recommendations 36
Contents

Dear Secretary of State for Health,
Earlier this year you requested I lead a review of bureaucracy in the NHS, with a focus on theburden coming from national bodies. Thisrequest came in the wake of Robert Francis QC’sreport into the tragic events at Mid Staffordshire.One of the important lessons borne of thatharrowing episode was the need to ensureinformation helps rather than hinders goodquality patient care. By making data in the NHSwork harder to improve patient outcomes, staffare enabled to get on with caring for patients.
You asked the NHS Confederation to carry outthis work because we are uniquely placed tospeak on behalf of the whole healthcare system. Our membership includes NHS acute,community, mental health and ambulancetrusts, as well as commissioners andindependent sector providers of NHS services.The Confederation’s independence andstanding among those responsible for deliveringcare also makes us well-placed to work withorganisations such as the Health & Social CareInformation Centre (HSCIC).
We have worked with the HSCIC and othernational bodies throughout this review toinvestigate how to reduce the burden ofinformation collection and reporting on a range of providers. We have also been mindfulof the other reviews you commissioned intocomplaints, patient safety and care quality. This review acknowledges the work of ProfessorDon Berwick, Ann Clwyd MP, Professor TriciaHart, Professor Sir Bruce Keogh and others, andcomplements their conclusions by advocating
Challenging bureaucracy02
Letter to the Secretary of State
an approach to reducing bureaucracy thatplaces patients front and centre of everyimprovement.
It is clear that providers, national bodies,commissioners, patients and staff are stilladjusting to a reformed healthcare system.There have been a number of system changessince April this year, and some confusion over areas of responsibility and accountability.It is now more crucial than ever before toprovide clarity on how we can reducebureaucracy that is unnecessary, who isresponsible for making that happen and how we can squeeze the most value out of the data already in use.
I want the NHS to be in line with the bestperforming industries across the world when it comes to using data effectively, and I believethe recommendations in this report provide ablueprint to do just that. If we want a 21stcentury NHS, we need to make sure the way weuse data and information is brought into the21st century. To do this, we must be ambitiousabout how information is used. The way data is collected and reported should not be punitiveor burdensome, but contribute to improvingcare and increasing transparency about the care people receive.
This review has discovered that the nationalburden of bureaucracy is much bigger thanoriginally thought – it’s now crystal clear thatwe need to manage the burden better. Whilevast amounts of NHS data and information arerelevant to patient care, the processes used tocollect and record them are often outdated and
concludes that those requesting data in theNHS must always be able to prove how that data will be used to support improvements inquality, safety and outcomes. It is only bysticking to these principles that we can truly liftthe ‘burden’ of bureaucracy in the NHS.
Yours sincerely,
Challenging bureaucracy 03
time-consuming for staff. That is why thisreview has not only looked at tackling thevolume of data, but reducing the effort it takesto gather it, and increasing the value that can be extracted from every bit.
We can address this volume, effort and valuechallenge by supporting trusts to use databetter so that staff can get on with their jobsand deliver better patient care. And we need toincentivise the use of smarter technology tostreamline data collection.
Data is precious. It can be incredibly valuablewhen it’s used to help deliver better, saferpatient care, and to understand what’s reallyhappening in the health service. This review
Mike FarrarFormer Chief Executive of the NHS Confederation

Challenging bureaucracy04
What we found
• Bureaucracy, including the recording,collection and reporting of information, is an essential part of any effective healthcaresystem. Much of the data the NHS collectsand reports on is of value and essential toassuring and improving patient care. Itenables clinicians to better understand thecare they provide. Where bureaucracybecomes burdensome is when it becomesexcessive or undue.
• We estimate that national bodies1 account for a quarter of the total reporting burden on NHS providers. The cost of nationallyrequired data collection and processing isapproximately £300–£500 million a year. This is a significantly higher cost thanpreviously estimated.
• National bodies and providers differ in theirunderstanding of the impact and cost of data requests. Trusts told us that the cost of configuring systems to collect new datarequests, or make small changes to existingones, could be significant.
• Clinicians, managers and national bodiesagreed that reporting requirements areincreasing. While some of this can beminimised through more efficient working,this increase is not necessarily a bad thing initself. An increasing focus on understandingthe quality of care, and how we measure it, isa positive development. We potentially needmore and better data to improve care forpatients, not less.
Key findings and recommendations
• National bodies overlap in holdingresponsibility for providers’ performance,resulting in duplication. This is furthercomplicated by the lack of a clear definition of ‘quality’ and core dataset to measure it.
• NHS providers vary in how they respond toreporting requirements. Supporting providersto adopt new information technology andimprove business processes could reduce theeffort involved in responding to requests.
• It is important that the right datasets arecollected, and that the information isprocessed and made available in a timely way to enable improvements in clinical care.Clinical staff largely understand the value ofthe data they collect and its relevance topatient care, but feel more could be done toincrease its value.
• There has been progress to reduce the volume and increase the efficiency of requestsfrom national bodies, but more still needs tobe done.
What we recommend
• The Health & Social Care Information Centreshould direct all bodies, including ministerialunits, to disclose the full cost of data collected(using an updated Review of Central Returnsmethodology) and provide a clear businessjustification for each request.
• The Health & Social Care Information Centreshould work with the Academy of MedicalRoyal Colleges, professional bodies, clinical
1. As we have not looked at the burden from commissioners during this review, this excludes NHS England.
Challenging bureaucracy 05
specialist societies, the Care QualityCommission’s chief inspector of hospitals andpatient representatives to ensure clinical andpatient engagement in agreeing the definitionof ‘quality’ and a core dataset.
• The Department of Health should introduce a tight governing concordat for nationalbodies, based on an agreed set of datacollections.
• It is important the Secretary of State forHealth is able to hold the national bodies toaccount in terms of reducing the overallburden. We therefore believe that requiringeach of the national bodies to reduce theirburden by 10 per cent over each of the nexttwo years would be a reasonable mechanismby which the Secretary of State could do this.
• The Health & Social Care Information Centreshould consider the options for piloting a trustrecharge scheme for national bodies for datarequests that fall outside a core dataset. If a
national body requests data outside of thecore dataset they would incur a charge for the cost incurred by the trust to collect, validateand report the data.
• To enable a better understanding of thevariation of effort across providers, NHS Englandshould lead the development of an index thatenables providers to self-assess and benchmarktheir information capabilities and businessprocesses to manage information requests. Theindex should be used to identify and facilitatethe sharing of best practice.
• Providers and the national bodies need towork together to build capabilities and skillsthroughout healthcare staff, to support themto better understand the information alreadyavailable and how they can use it.
• The Health & Social Care Information Centreshould commit to making submitted dataavailable to trusts within 30 days of submission(with fully validated data to follow).

Introduction
Challenging bureaucracy06
In February 2013, the Secretary of State forHealth commissioned the NHS Confederation tocomplete a review of the bureaucratic burdenson providers of NHS care from national bodies.The request followed the publication of RobertFrancis QC’s report into failings in care at Mid Staffordshire NHS Foundation Trust.
This report sets out what we found and whatactions should be taken to free the NHS fromunnecessary bureaucracy. We believe ourrecommendations will help ensure thathealthcare staff spend as much time as possibledelivering patient care.
Our review has focused on the effects and impact of unnecessary bureaucracy fromnational bodies. It is vital that further work isdone – as a matter of priority – to understand the burden from local bodies, includingcommissioners, local authorities and localHealthwatch. This should address instances of unnecessary bureaucracy throughout thecommissioning system, including the burdenexperienced by local commissioners themselves.
The problem we want to solve
We want to ensure data in the NHS worksharder to improve patient outcomes and enablestaff to focus on delivering high-quality patientcare, without being distracted by unnecessarybureaucracy.
Bureaucracy: help or hindrance?
Within public services, the term ‘bureaucracy’has become synonymous with processes andsystems that are unnecessarily burdensome. We challenge this assumption; regulation andoversight are essential to good governance and accountability, and the availability ofinformation about service quality and outcomes
is vital to enabling choice and engaging andempowering service users. It is also essential foreffective planning, research and scientificdevelopment. A 21st century healthcare systemrequires sophisticated information derived from robust data. A degree of ‘bureaucracy’, if taken to include the recording, collation,verification and reporting of information, isfundamental to understanding and improvingboth patient care and population outcomes.
But the NHS should neither generate nortolerate ‘burdensome’ – that is, excessive orundue – bureaucracy. In a new system withcompeting demands from several neworganisations, it is more important than ever for the health service to make the most ofavailable information, and achieve the rightbalance of regulation and oversight so thatproviders are not overwhelmed or distractedfrom patient care by requests for informationand inspection.
While we understand the need for bureaucracyin the NHS, we believe it can be done in a moreefficient way, and national bodies have animportant part to play in ensuring theirdemands do not become unnecessarilyburdensome. We view bureaucracy as a key part of ensuring and improving patient care;unnecessary bureaucracy, however, can detractfrom these goals.
Reducing volume, minimising effort,increasing value
This report examines how national bodies canwork together to reduce and better control thevolume of information requests and reports;how providers can be supported to reduce theeffort needed to respond to them; and how toensure clinical staff get the most value fromexisting data.

Challenging bureaucracy 07
We have identified three main ways to reduceunnecessary bureaucracy:
• understanding and actively policing thevolume of requests from national bodies
• minimising the amount of effort involved inresponding to information requests withaccurate data
• increasing the value from collectedinformation, for staff, the wider system and the public.
What we did, and how
We wanted our recommendations to be led and informed by real experiences and evidence,and so worked with seven providers of NHS care from across England to develop a bottom-up perspective of the burden associatedwith data requests from national bodies. Theproviders (see page 34) included a combinationof acute and mental health services, of whichfour were integrated with community services.
Each trust conducted a review of thebureaucratic burdens they experience fromnational bodies, using a standardisedmethodology that detailed which questions to cover and the approach to take.
We completed fieldwork with these trusts over a three-week period in the summer of 2013. We recognise that this is a limited sample oftrusts over a snapshot of time, and haveexercised caution when drawing generalisationsfrom our findings. However, we believe thetrusts we worked with represent a fairly typical spread of NHS organisations, and provided us with sufficient information on which to base our generalisations.
To oversee and guide the review, we weresupported by a Programme Advisory Group(PAG). The PAG included representation from alarge number of national bodies, as well asproviders and commissioners of NHS care (seepage 34). The group was invaluable in advisingand informing this review, and we recommendthat it continues in its advisory capacity tosupport the implementation of ourrecommendations, if accepted by the Secretaryof State, and any future associated work.
We also conducted a small number of interviewswith patient representatives, to understand theirperspective and experiences of bureaucracy inthe NHS. Their guidance and insight wereextremely useful.
Previous work
This report follows our interim report,Bureaucracy and regulatory review: a report ofearly findings and recommendations, publishedin March 2013, and builds on previous work bya range of organisations:
• NHS Confederation and IndependentHealthcare Advisory Services, What’s it all for?Removing unnecessary bureaucracy inregulation (2009)
• The Royal College of Physicians’ response tothe Equity & Excellence white paper (2011)
• The Royal College of Nursing’s Paperwork andadministration (2012)
• The Department of Health, Fundamentalreview of data returns (2009)
• The NHS Confederation, Information overload (2013)
• nhsManagers.net survey of NHS staff.
Challenging bureaucracy08
In undertaking this review, we have beenconscious that the term ‘bureaucracy’ is notneutral, and is often used to imply a set ofactivities that are obligatory and unnecessarilyburdensome.
In the NHS, it is usually associated with form-filling and box-ticking, and is viewed asburdensome because of the effort required torespond to numerous national, regional andlocal requirements.
But the NHS lacks a commonly agreed definition of ‘bureaucracy’. In this report, wedefine it as the combination of requests madeby national bodies to NHS providers as part ofnational reporting and assurance. It comes in a number of different forms, including routineand ad hoc reports, inspections andassessments (see Figure 1). We see bureaucracy as both what is done (whether it is valuable or not) and how it is done (whether it is efficient or not).
Inherently burdensome?
We challenge the assumption that bureaucracyis inherently burdensome. While we believethere is unnecessary bureaucracy in the system,a degree of oversight and regulation is essentialto any effective healthcare system, and much ofthe information the NHS collects and reports onis of value and crucial to assuring and improvingpatient care.
In fact, doctors and nurses told us thatevidence-based practice requires collecting and processing significant amounts of data. And the patient representatives we interviewedunderstood why the NHS needs bureaucracy, so long as it does not distract from delivering
high-quality patient care. But unnecessarybureaucracy is distracting staff from patient care.
Bureaucracy can be perceived as burdensomebased on the volume of requests and the effortrequired to respond to them. However, thevolume and effort involved might beproportionate to the value of the informationcollected, to both patients and professionals. It is also possible that the excessive time andeffort expended in some organisations is due toinefficient systems and technology, rather thanthe nature of the data request.
As such a bureaucratic burden is not just anassessment of the volume of data collected and the time and cost to do so, but whether thedata is valuable or not – whether that value isproportionate to the cost – and if it is beingprocessed efficiently, or not.
Our review has centred on finding the answersto three main questions: When is bureaucracyunnecessarily burdensome? What are thecauses? What can we do about it?
When is bureaucracy unnecessarilyburdensome?
Bureaucracy is unnecessarily burdensome, forexample, when:
• national bodies request that providers collect and record information that does notadd value
• there is excessive validation and follow up on data requests, either within trusts, bycommissioners or regulators
• information is requested by multiple bodiesand in different formats
• information requirements change regularly.
What is bureaucracy? When is it a burden?

Challenging bureaucracy 09
What causes unnecessarybureaucracy?
Unnecessary bureaucracy can occur, forexample, when:
• local or national processes are inefficient anddo not make the most of informationtechnology
• there is a lack of clarity of roles andresponsibilities across different organisations
• there is a lack of consistent definitions used,especially in relation to quality.
What can we do about it?
Our review has uncovered a number of ways toreduce unnecessary bureaucracy from nationalbodies on NHS providers. We believe ourrecommendations will help manage the volume of requests, reduce the effort involved in responding and, crucially, maximise the value of information for staff, patients and the public.
Figure 1. Where does bureaucracycome from?
Clinical, managerial andadministrative staff atproviders of NHS care
Requests from national bodies come in arange of forms:
Recurring or routine reports: data requeststhat are made on a regular basis
Ad hoc reports: data requests made on anirregular or one-off basis
Inspections: Preparation and support forperformance reviews such as the CareQuality Commission’s quality and safetyinspections
Assessments: preparation and support forevaluations and assessments, such asMonitor’s process for granting foundationtrust status
Planning: preparation for future plansrequested by national bodies.
The process for responding to a reporting request caninclude the following steps:
1. Preparation, data collection and entry
2. Internal validation
3. Report generation
4. Report submission
5. External validation
6. Report re-submission
7. Follow up action.
Requirementsfrom trusts
themselves tomanage theirorganisations
Requirementsfrom local bodies,
to secure andmanage care inthe local health
economy
Requirementsfrom national
bodies tomanage the
national healthcare system
Challenging bureaucracy10
The cost of reporting
We estimate that national bodies account for aquarter of the total reporting burden on NHSproviders. The cost of nationally required datacollection and processing is approximately£300–£500 million a year.
What we found
A significant amount of the informationrequested by national bodies is entirelyappropriate and reflects the need for scrutinyand assurance in a public health system – thisis recognised by many working in the NHS. Butthe cost of nationally required data collectionand processing is significantly higher thanpreviously estimated.
Reporting costs more than previously estimatedOur interviews suggested that national bodiesaccount for approximately 25 per cent of trusts’ costs associated with data collection,processing and reporting; the rest comes from the commissioning system and trusts’internal processes2 (see Figure 2). We recognise
Managing the size of the burden
that more work is needed to confirm thisbreakdown, but our research suggests this is a good indication.
National requests can, on average, cost a trustapproximately £1.4 million a year.3 This is madeup of:
1. the cost of routine reports, which can rangefrom £700,000 to £1.3 million, with anaverage of approximately £1 million
2. the cost of ad hoc reports, assessments,inspections, planning and fees, which addbetween £200,000 and £600,000, with anaverage of approximately £400,000.4
Multiplying £1.4 million across the(approximately) 220 acute and mental health trusts in England, the total cost to this type of provider could be in the region of £300 million. This excludes other types of NHS providers not included in this review.
We also used a second method to calculate the cost of national reporting. The Review of Central Returns (RoCR) methodology,operated by the Health & Social CareInformation Centre (HSCIC), estimated that its 154 centrally mandated reports costapproximately £50 million in total acrossEngland. But the trusts we worked withrecorded a per-report cost ten times greaterthan that listed in RoCR.5 The reason for this ispartly because not all of the reporting steps areincluded, including the validation andsubmission steps. Applying this multiple to the£50 million total burden of the RoCR list implies
• According to those we interviewed, nationalbodies account for approximately 25 per centof the bureaucratic burden
• Nationally required data collection andreporting costs approximately £1.4 million ayear per trust
Key statistics
2. Interviews were conducted with 79 clinical members of staff and 89 managerial and administrative staff.
3. This is based on feedback from the seven trusts and includes a combination of RoCR reports and others. It does not reflectall RoCR reports.
4. This is likely to be conservative as there appeared to be additional costs that trusts were unable to quantify.

Challenging bureaucracy 11
Recommendation Who By when
1 Revise the RoCR burden calculation methodology HSCIC Late 2013to include trust costs for all steps in the data return process.
a total national cost of £500 million. As such,the estimated cost of national reporting couldbe between £300–£500 million – this is asignificantly higher cost than previouslyestimated.
If the cost of nationally required data collectionand processing is between approximately£300–£500 million – which represents a quarterof the reporting cost on providers – the impliedtotal could be between £1–2 billion a year.However, much more work is needed to providean accurate figure.
What should be done
Develop a consistent approach to calculatingbureaucracyThe NHS is facing unprecedented financialchallenges. It is now more important than everto understand the true cost of bureaucracy tothe NHS, based on a consistent and agreedmethodology for calculating the burden. Anagreed methodology should be developed inconsultation with different parts of the systemand applied in a consistent way.
5. Reasons for this discrepancy include: partial coverage of burden type-burdens of assessments, inspections and planning arenot currently included; partial coverage of cost chain, the validation and submission (and, frequently, re-validation and re-submission) steps are not included; conservative assumption of clinical staff burden, does not reflect the steps needed for trusts to collect the required data and put it into the report format; conservative estimation of staff costs – analysis of theNHS staff survey indicates that RoCR may underestimate staff per diem rates by approximately 20-30 per cent.
Figure 2. Breakdown of where data collection, processing and reportingrequests come from
Source: NHS Confederation interviews with managerial and administrative staff
National/regulatory body (e.g. CQC, Monitor, NHS England)
Commissioning/local body (e.g. clinical commissioning group)
Internal (e.g. trust own performance management)
Other (e.g. research requests, local authorities)
25% 25%
45%
5%

Challenging bureaucracy12
The impact of data requests
National bodies and providers differ in theirunderstanding of the impact and cost of datarequests. NHS providers told us that the cost of configuring systems to collect new datarequests, or make small changes to existingones, could be significant.
What we found
National bodies told us they want to minimisethe amount of time providers spend oncollecting data, and the associated costs.However, many believed the resourcesnecessary to compile their reports wasreasonable. They told us:
• reports are generated or aggregated fromeveryday operational data that trusts shouldbe collecting
• as data is already collected, extracting it fromIT systems should be straightforward, withlittle effort required by trusts.
The trusts we spoke to told us a different story.They reported that the cost of configuring their systems to collect new data requests, or make small changes to existing ones, could be significant. National bodiesunderestimated these costs by around a factorof 10. While this may be one extreme, we heard that a new report can cost as much as£300,000 for a trust.
Front-line staff perceived that national bodies impose a small burden on them6
directly. However, the burden on managerialand administrative staff appeared to besubstantial; on average they reported that theyspend between five and 20 hours a week onnationally required data collection, reportingand validation.7
Managerial and administrative staff told us that duplication, ad hoc requests, changes and updates to routine reports and multiplereporting timelines were the main sources ofunnecessary burden.
• New reports can cost a trust as much as£300,000 to set up
• The majority of managerial and administrativestaff we interviewed reported that they spendbetween five and 20 hours a week onnationally required data collection, reportingand validation
Key statistics
6. Most of the data they collected was not specifically required by national bodies and would have been collected anyway, as part of delivering high-quality patient care.
7. Our evidence suggests that internal and external validation accounts for 41 per cent of total burden from national bodies,although this was proportionally less in the mental health trusts we worked with.
“Demands for reports changefrequently in terms of what they holdand how they are to be presented.Changing analysis tools and reporttemplates also take large amounts of time.”Service manager

Challenging bureaucracy 13
What should be done
Understand the impact of data requestsIt is important that there is an open andtransparent understanding of the cost andresource impact on providers from nationalbodies’ information requests. More clarity onthe rationale for requests would also bebeneficial.
Recommendation Who By when
2 Direct all bodies, including ministerial units, to HSCIC Immediatelydisclose the full cost of data collected (using the updated RoCR methodology when it is available) and provide a rationale for the request; a similar process should be used for changes to clinical data collections.

Challenging bureaucracy14
The trend
Clinicians and managers told us that datacollection and reporting have increased over thelast five years. National bodies reported thatchanges to the health system – especially theincreased focus on assuring the quality of care –were highly likely to further increase the volumeand type of data collected in future. While someof this can be minimised through more efficientworking, the health service will potentially needmore and better data to improve care, not less.
What we found
Clinicians, managers and national bodiesagreed that reporting requirements are set toincrease. This increase could be due to:• the health service operating in a new system
with several new organisations and a lack ofclarity of roles and responsibilities, resultingin duplicated requests
• an increased focus on quality and safety, but it is not always clear how they should be measured
• external pressures on the NHS driving thevolume of requests – just as trusts are under pressure from national bodies, thelatter are under pressure from Parliament and the public
• a lack of incentive or requirement for nationalbodies to check existing national datasetsbefore making new requests
• little incentive to cut back on requests, as the benefit of terminating a reportingrequirement is minimal
• many of the institutional barriers tounreasonable or duplicative data requestshave been removed in recent years, such asMonitor’s gateway evaluation of new reports.
What should be done
Collect, manage and coordinate the right dataPractical steps can be taken to better managethe increase in demand for information(addressed in later chapters of this report).
The increased focus on understanding the qualityand safety of care, and how it is measured, is apositive development. To transform patient careand improve quality for patients, the healthservice potentially needs more and better data,not less. For example, reorganising datacollections to maximise clinical outcomes maymean collecting more data to fill gaps in thelandscape. NHS England's consultation onhospital data is likely to expand the datacollected from hospitals.
Collecting and using data are essential to patient care. The health service will need tofocus on collecting the right data and ensuringit is managed in the most coordinated andefficient way.
• 70 per cent of clinical staff felt the increase indata collection and reporting over the last fiveyears has been significant
Key statistics
“We are seeing a growing appetite for data which is generating muchenthusiasm and exciting opportunitiesfor new ideas, new products and newanalyses. While this is of course anentirely positive development, it cannothappen at the expense of the time thatcare professionals spend at the front linewith people who need their services.”Kingsley Manning, Chair,Health & Social Care Information Centre
Challenging bureaucracy 15
Clarifying responsibilities and definitions
National bodies overlap in holding responsibilityfor providers’ performance, resulting induplication. This is further complicated by thelack of a clear definition of ‘quality’ and coredataset to measure it.
What we found
Overlapping jurisdictionsCentral oversight, scrutiny and control are anecessary and appropriate part of the NHS, but with more clarity on accountabilities andboundaries in the system, the cost of oversightcould be reduced. A degree of overlap betweenorganisations is inevitable and may even behealthy, as not every eventuality can bepredicted. But all seven trusts in our reviewconsidered overlapping jurisdictions between national bodies a major cause ofbureaucratic burden.
This is particularly problematic in the approachto quality of care. While ‘access’ and ‘finance’are relatively clear, both in definition andresponsible national organisations, intervieweesconsistently stated there was no clear definitionof ‘quality’, and warned of the significant risk ofoverlap between bodies claiming responsibilityfor quality assurance.
Individual quality measures reflect thisvagueness; terms are not always standardisednationally, and the results of these measuresnot readily comparable. Separate, overlappingoutcomes frameworks with slightly differentmeasures can also add to the data collectionburden.8
Many national bodies view quality as part oftheir oversight responsibilities, leading them todemand different information and reports onquality. Organisations such as the NHS TrustDevelopment Authority (TDA) and the CareQuality Commission (CQC) can claim a mandateto investigate and evaluate, with professionalbodies such as the General Medical Council(GMC) becoming involved if medical practice is implicated.
The issue is substantially exacerbated whenorganisations seek to understand and correctdeviations in provider performance. In such instances, the reporting burden ismultiplied as providers try to work with andrespond to sometimes contradictory requests. Trusts face the challenge of assuringexternal bodies that a situation is under control, while ever-growing demands from these organisations take time away fromestablishing control.
8. NHS Confederation (2013) Information overload.
“The current NHS regulatory system is bewildering in its complexity andprone to both overlaps of remit andgaps between different agencies. Itshould be simplified.”Berwick Review
Regulatory creepThere can be a tendency for regulators toexpand the boundaries of their responsibilities.With some regulators now having expandedroles and responsibilities, it is important there isongoing clarity for providers around who isresponsible for what.
Challenging bureaucracy16
Ministerial units are also taking a growinginterest in quality; the Department of Healthmakes a number of requests, and the CabinetOffice’s Implementation Unit has requesteddata on referral to treatment times.
What should be done
Establish a coordinated approach on key topicsMore needs to be done to ensure a coordinatedapproach from national bodies on key areas –operations, access, finance and quality – andthe process for collecting core data. This wouldencourage and facilitate the sharing of existingdata as the first response to data needs, withdemands to trusts as the last resort.
Set consistent definitions The trusts we interviewed were concernedabout inconsistent definitions. Establishing astandard, core set of definitions – including, forexample, what good quality care is – and what
metrics are used to measure it, is crucial. Thedefinitions must have clinical credibility,developed in consultation with clinicians andpatients. It is important that consistentdefinitions and templates for reports aredeveloped and aligned to clinical audits.
Establish a core datasetDeveloping a core dataset agreed by all national bodies will provide clarity on whatneeds to be collected to deliver and improvepatient care. This is an important first step toenable the Health & Social Care InformationCentre (HSCIC) to coordinate and manageduplicative requests for information fromdifferent national bodies. We recognise theremay be exceptional circumstances where itmight be necessary to request additionalinformation, and further consideration wouldbe required to understand how this would work in practice.
We are supportive of HSCIC’s and NHSEngland’s review of what data hospitals should be collecting; the development of a core dataset would need to align with this. In addition, it is important that a core dataset complements the Royal College ofPhysicians’ work to standardise the clinicalstructure and content of electronic patientrecords.9 If these record standards areimplemented in electronic patient records, they will enable datasets to be automaticallyextracted for secondary purposes, which willavoid separate, duplicate data collections.
9. The Royal College of Physicians (RCP) has led development of standards for the clinical structure and content of patientrecords in conjunction with healthcare professionals from multi-disciplinary backgrounds, patients, carers and healthinformation technology specialists.
“Action plans are required foreverything, often the same actions are in numerous plans, thereforeduplicating work. So much time isspent writing the action plans,detracting from time to actuallycomplete the actions.”Team manager
Challenging bureaucracy 17
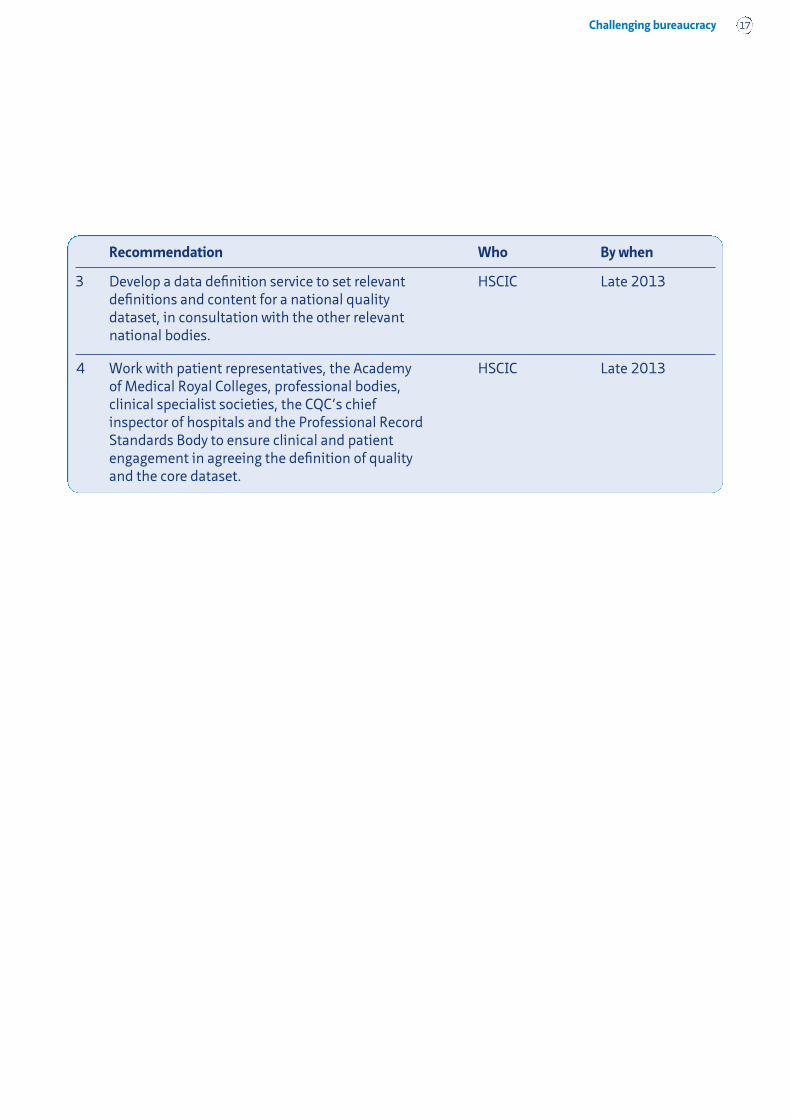
Recommendation Who By when
3 Develop a data definition service to set relevant HSCIC Late 2013definitions and content for a national quality dataset, in consultation with the other relevant national bodies.
4 Work with patient representatives, the Academy HSCIC Late 2013of Medical Royal Colleges, professional bodies, clinical specialist societies, the CQC’s chief inspector of hospitals and the Professional Record Standards Body to ensure clinical and patient engagement in agreeing the definition of quality and the core dataset.
Challenging bureaucracy18
Managing the volume better
There has been progress to reduce the volumeand increase the efficiency of requests fromnational bodies, but more still needs to be done.
What we found
Incentives needed to discourage proliferation of reportsNational bodies have all contributed to reducingthe volume of reports requested from providersand to improving the way remaining reports areprocessed. Since 2011, the number of reportslisted in the Fundamental Review of DataReturns has dropped by nearly half.
The Care Quality Commission (CQC) has alsorecently dramatically cut its collection requestsby 90 per cent without compromising its corepurpose. Following a recent consultation on its regulatory framework, the regulator reducedthe number of indicators from more than 1,000to fewer than 200.
There is a lack of incentives in the health servicefor streamlining data requests and reports.Every national body we interviewed expects thevolume of data requested from providers toincrease in the near future. It is thereforeimportant the existing principles of Betterregulation are adhered to.
Information sharing and coordination of data requestsThere is still a need for better informationsharing and coordination of data requests toreduce duplication; this confirms what we heardearlier this year through the nhsManagers.netsurvey. As national bodies demand data,particularly in response to concerns aboutperformance, trusts feel unable to challenge oreven streamline the process for supplyinginformation. In one example we heard, a trustheld 11 different meetings in a month withnational and local bodies to discuss A&Ewaiting time breaches. While recognising thiswas an inefficient use of their senior managers'time, the pressure to respond to each separatebody kept the trust’s leadership from having thebreathing space to better coordinate the various meetings.
Use of the Review of Central Returns (RoCR)process for ad hoc requests Although the Health & Social Care InformationCentre (HSCIC) has its RoCR process for reports,it is not consistently used for ad hoc requests.This is important as ad hoc requests can have asignificant impact on providers.
Reviewing new data requests and rejectingduplicative or excessively burdensome requestsNational bodies highlighted their concern aboutthe lack of a process for reviewing new data
• eliminate duplication and report only what is necessary
• standardise data report structures
• make requests clear and minimise changes
• streamline reporting timelines
• create a centralised system where nationalbodies can share the information they receive.
Top five suggestions from non-clinicalstaff to reduce unnecessary burden
Challenging bureaucracy 19
requests and dealing with duplicative orexcessively burdensome requests. Several alsoraised the need for a more aggressive review ofexisting data requests to ensure obsoletereports are quickly cancelled. Many intervieweesrecalled the processes in place a decade ago,including the 2004 Inspection Concordat10 andMonitor’s power to review all RoCR requestsmade of foundation trusts.
Changes and updates to routine reportsContinued changes and updates to routinereport formats are time-consuming, as trustsneed to reset systems and procedures to accountfor changes to data gathering.
Data collection processes and reporting timesNational bodies have different data collectionprocesses and reporting times. Thesedifferences undermine attempts to aggregatenational data, make inter-body datacomparisons extremely difficult, and feedconfusion at trust level that can result inmultiple trips around the ‘submission-externalvalidation’ cycle.
HSCIC processesWhile there was support for HSCIC’s central role,some interviewees felt the centre could improveseveral of its processes. For example, some toldus HSCIC’s website interface is not user-friendly; substantial amounts of non-sensitiveinformation are restricted (such ascommissioning codes) and users complained ofsevere delays when attempting to connect toHSCIC systems and services.
What should be done
Introduce a concordat for national bodiesThe Secretary of State should introduce andtake responsibility for a tight governingconcordat to govern the collection of data fromnational bodies and hold them to account, withthe HSCIC as the coordinator of all collected orextracted data. The concordat should aim toensure that:
• requests for information are coordinated – toimprove coordination and reduce duplication,an integrated system under HSCIC oversightshould be introduced to control andcoordinate demands from various nationalbodies (in a similar way to previous systems,such as the Review of Central Returns,Inspection Concordat, and gateway systemssuch as those formerly run by Monitor forfoundation trusts). Providers would benefit ifthey had more confidence that each requestfor information is handled and processed in aconsistent way.
• requests for information are clear and changesminimised – national bodies should be clearabout why a request is being made and what is to be included, ensuring any changes to requests are kept to an absoluteminimum, recognising the effort needed torespond to any essential changes.
• there is regular governance and review – asystem of governance and regular reviewwould ensure each report’s continued valueand remove those failing to justify theirburden, a requirement set out in the Healthand Social Care Act. This could include using
10. At the time of What’s it all for? in 2009, the Healthcare Commission had established the Concordat to improvecoordination and collaboration among regulators and inspection bodies. Responsibility for the Concordat passed to theCare Quality Commission when the Healthcare Commission’s functions became part of the regulator.

Challenging bureaucracy20
Streamline collection processes and reporting timesStandardising collection processes andreporting times would considerably reduce theburden across the system. A business supportofficer that we interviewed explained that:“Timeliness of reporting cycles are a bigproblem. The trust reporting cycle is clear andconcise. Locally there are several reportsrequired at different times of the month. Reportrequests only at the beginning/month endwould reduce the burden.”
Progress toward automatic data extractionMoving to automatic data extraction fromelectronic patient records, rather than separatedata collections, would have a large impact onreducing the burden.
the equivalent of ‘sunset’ clauses so thatwhen a requirement is no longer needed itcan be removed or updated, to help prevent acontinued rise in requests.
• information shared and available – thesharing of existing national body data shouldbe the first response to data needs, withdemands to trusts seen as the last resort. A list of all national collections andextractions should be published, detailing why the requests are of value.
Implement system-wide incentivesIt is vital that a balanced set of incentives and controls are set in place across the system.A provider recharge scheme for data requeststhat fall outside a core dataset should bepiloted.
Continue to remove unnecessary reportsWhere possible the recommendations of theDepartment of Health’s Fundamental Review of Data Returns, managed by the HSCIC, shouldbe implemented.
A small number of additional reports were identified as worth considering fordiscontinuation:
• reference cost reporting: trusts cited manyproblems with reference costs. Monitor isplanning to replace them with patient-levelinformation costs (PLICS) by 2016/17.
• estates information: reports such as theEstates Return Information Collection (ERIC)were cited as examples of reporting without aclear objective; it did not facilitate usefulbenchmarking or performance improvement,or give assurance to regulators about wise useof resources.
“The responsibility that the newreforms have placed on the Health & Social Care Information Centreregarding oversight of the system-wideburden and bureaucracy is clear. I expect that the HSCIC will act as the‘conscience’ for the front line on this.We will of course work collaborativelywith all of our partners. But there willbe occasions where we need to speakout and act in the interests of theservice – and therefore the public – at large.”Kingsley Manning, Chair, Health & Social Care Information Centre
Challenging bureaucracy 21
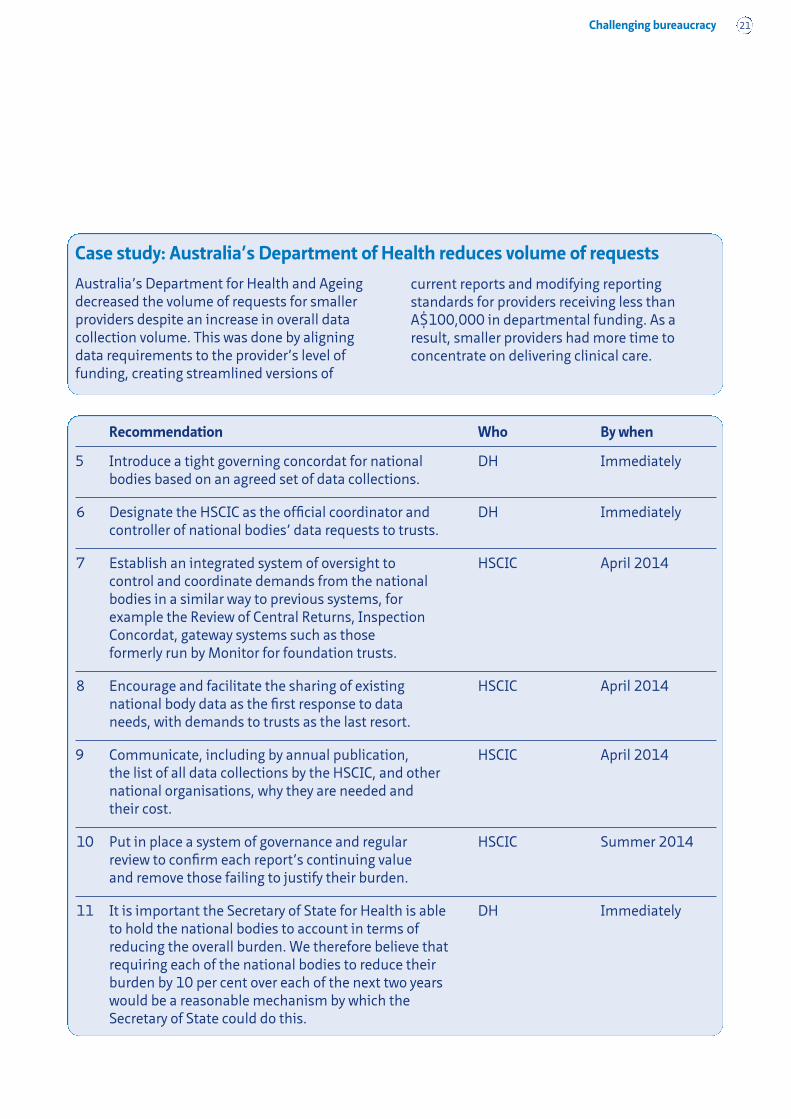
Australia’s Department for Health and Ageingdecreased the volume of requests for smallerproviders despite an increase in overall datacollection volume. This was done by aligningdata requirements to the provider’s level offunding, creating streamlined versions of
current reports and modifying reportingstandards for providers receiving less thanA$100,000 in departmental funding. As aresult, smaller providers had more time toconcentrate on delivering clinical care.
Case study: Australia’s Department of Health reduces volume of requests
Recommendation Who By when
5 Introduce a tight governing concordat for national DH Immediatelybodies based on an agreed set of data collections.
6 Designate the HSCIC as the official coordinator and DH Immediatelycontroller of national bodies’ data requests to trusts.
7 Establish an integrated system of oversight to HSCIC April 2014control and coordinate demands from the national bodies in a similar way to previous systems, for example the Review of Central Returns, Inspection Concordat, gateway systems such as those formerly run by Monitor for foundation trusts.
8 Encourage and facilitate the sharing of existing HSCIC April 2014national body data as the first response to data needs, with demands to trusts as the last resort.
9 Communicate, including by annual publication, HSCIC April 2014the list of all data collections by the HSCIC, and other national organisations, why they are needed and their cost.
10 Put in place a system of governance and regular HSCIC Summer 2014review to confirm each report’s continuing value and remove those failing to justify their burden.
11 It is important the Secretary of State for Health is able DH Immediatelyto hold the national bodies to account in terms of reducing the overall burden. We therefore believe thatrequiring each of the national bodies to reduce their burden by 10 per cent over each of the next two yearswould be a reasonable mechanism by which the Secretary of State could do this.
Challenging bureaucracy22
Recommendation Who By when
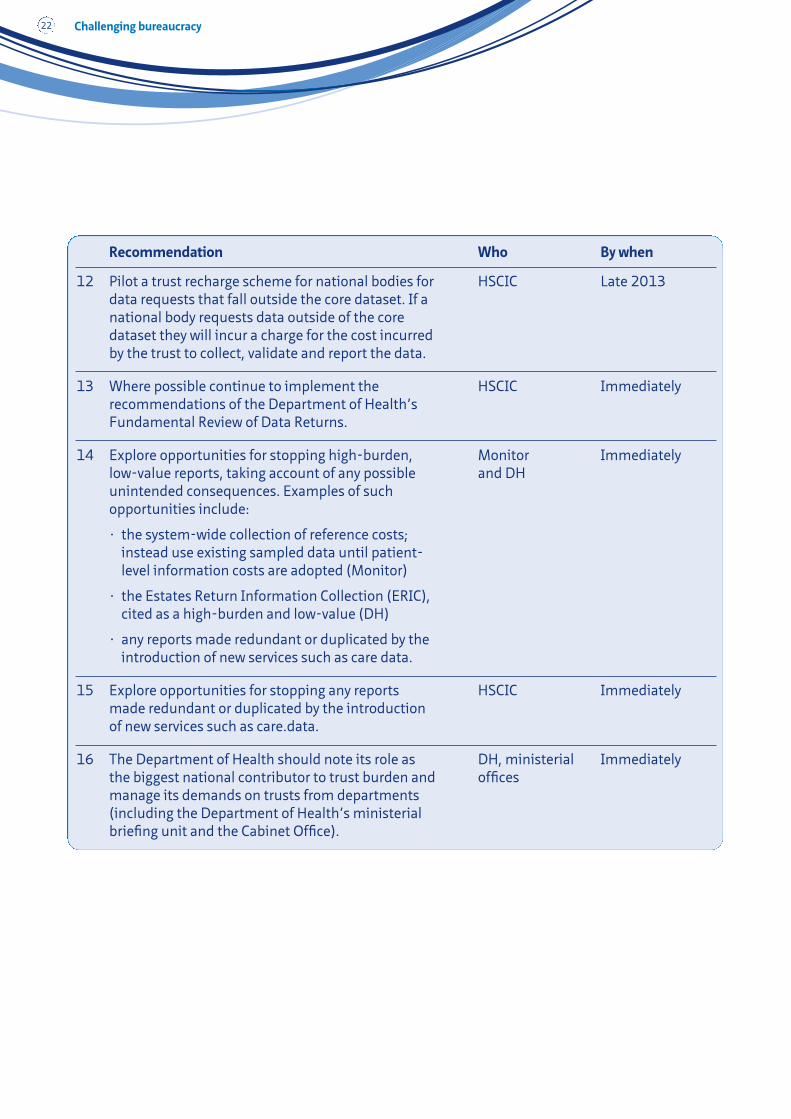
12 Pilot a trust recharge scheme for national bodies for HSCIC Late 2013data requests that fall outside the core dataset. If a national body requests data outside of the core dataset they will incur a charge for the cost incurred by the trust to collect, validate and report the data.
13 Where possible continue to implement the HSCIC Immediatelyrecommendations of the Department of Health’s Fundamental Review of Data Returns.
14 Explore opportunities for stopping high-burden, Monitor Immediatelylow-value reports, taking account of any possible and DHunintended consequences. Examples of such opportunities include:
• the system-wide collection of reference costs; instead use existing sampled data until patient-level information costs are adopted (Monitor)
• the Estates Return Information Collection (ERIC),cited as a high-burden and low-value (DH)
• any reports made redundant or duplicated by the introduction of new services such as care data.
15 Explore opportunities for stopping any reports HSCIC Immediatelymade redundant or duplicated by the introduction of new services such as care.data.
16 The Department of Health should note its role as DH, ministerial Immediatelythe biggest national contributor to trust burden and officesmanage its demands on trusts from departments (including the Department of Health’s ministerial briefing unit and the Cabinet Office).
Challenging bureaucracy 23
Variation between providers
NHS providers vary in how they respond toreporting requirements. This is why supportingproviders to adopt new information technologyand improve business processes could reduce theeffort involved in responding to requests.
What we found
Providers vary significantly in how they respondto requests for information, and have differentprocesses and digital capabilities for doing so.This was seen in the mix of reports cited as themost burdensome, whereby six trusts compileda list of the top ten most burdensome nationallymandated reports. The lists covered a total of 40 reports, of which only 11 appeared onmore than one trust’s list. The reporting burdenalso varied significantly by trust type, withmental health trusts identifying differentreports from acute trusts. Only the NHS SafetyThermometer and reference costs collectionspanned both types.
Reducing the effort needed tomanage information requests
Information technology can have a big impactWe support the drive for electronic capturing ofdata and the digitalisation of processes. Trustsin our sample without sophisticated informationtechnology systems, and in particular electronicpatient records (EPRs), reported more stepsinvolved to collect and submit data (andtherefore more time and cost).
One of the providers had an established EPRand found that the burden of data collectionand internal validation was lower than their lessautomated counterparts. This makes intuitivesense as the process of gathering andconfirming data would be significantlyshortened if supported by a good informationtechnology system. It would also enable greaterextraction of data from systems, rather thanfocussing on data collection.
For example, Salford Royal NHS FoundationTrust was the most technically advancedprovider in our sample. With one exception, itsself-assessed top ten burdens were significantlylower than those of the other acute trusts. Forexample, the trusts estimated the costassociated with the NHS Safety Thermometer;Salford's indicative cost was significantly lowerat £26,000, compared to other trusts that cited£95,000 and £70,000.
Information technology can also play animportant role in improving patient safety.Moving from paper-based records to an EPR, forexample, would allow important information tobe shared more quickly and reduce the risk ofpaper records being lost or misplaced.
11. Clinicians we interviewed expressed a strong view that many of the data entry and administrative tasks could andshould be performed by non-clinically trained staff, a position echoed by professional bodies such as the Royal Collegeof Nursing. This would, clinicians argue, free up more time for front-line staff to deliver direct care.
1. Better communication between departmentsand clinical divisions
2. Better IT interoperability
3. More administrative support for clinicians11
4. Greater automation of data collection andpresentation, potentially through anelectronic patient record
Clinical staff suggested the followingwould reduce the burden on staff

Challenging bureaucracy24
While we recognise the importance ofmaximising the use of technology to improvesafety and reduce the effort involved within thesystem, it is vital to develop a culture in whichstaff are supported, through clinical businesschanges. Systems must be designed to meet theneeds of patients and those who care for them.After all, information technology and tools areonly as good as the way they are used. Weshould also acknowledge that this is notnecessarily always concerned with investing innew technology, but also how providers canmaximise the value of the technology theyalready have.
Support for providers to improve is limitedProviders told us they can and want to improvetheir information management processes, make better use of information technology and maximise the information available to them. But there is limited support in the system to build their capability and skills to achieve this. For example, it can bedifficult for providers to know what ‘good’ looks like, how to achieve it and how otherproviders have succeeded in developing their capabilities.
Other factors have an impactTime and motion studies previously undertakenat trusts broadly confirm wide variations inbusiness processes and the amount of clinicaltime spent on administration, paperwork,writing notes, data entry or data collection. In addition to administrative duties, asignificant amount of time is spent away frompatients as a result of ward layout, handoverprotocols, and other issues that could be dealtwith by trusts’ management teams.
What should be done
Improving information management at trust levelProviders of NHS care should take a leading rolein improving how they manage information intheir own organisations. They should ensure asystematic approach to using data to betterunderstand the business, and set a culture inwhich this approach is the norm. They shouldalso avoid assurance procedures that dominatethe delivery of care in practice, focusing on datathat stems from clinical practice, not what sitson top of it. This will require a largecommunication and engagement exercise withNHS staff, and ideally their trade unions.
Sharing what ‘good’ looks likeMore work needs to be done to understand andshare good practice across the system, as part of a sustainable and sector-led approach toimproving how providers manage informationand adopt information technology. For example,the Health & Social Care Information Centre(HSCIC) has recently conducted fieldwork withseveral trusts and could play a valuable role insharing good practice.
Supporting providers to improve theircapabilitiesThere are a number of ways providers canimprove how they manage information and howthey use information technology. It can, however,be unclear how to achieve improvements andwhat the different options are as there isn’t a‘blueprint to success’. A number of differentsolutions and experiences exist. This intelligence,experience and learning should be shared andmade accessible across providers.
NHS England has created an index to benchmarkthe digital capabilities of providers to help driveimprovement, called the Clinical Digital MaturityIndex (CDMI). This will help providers understand

Challenging bureaucracy 25
their digital capabilities in relation to their peers,and how others have approached the challenge.We support the approach of using an index tosupport providers, and think this should beapplied to how providers manage informationmore broadly. We believe the use of an indexshould have four core aims:
• Enabling comparative assessment, baseliningand benchmarking the capabilities ofproviders to help them better understand thevariation of effort in the system and make thisinformation transparent.
• Documenting and sharing best practice, bymaking different approaches, insights andexpertise easy to identify.
• Becoming a rolling self and peer-assessmenttool that providers can choose to use as partof driving their own improvement.
• Facilitating discussions between providers,and engagement between providers andsuppliers, to create a more sustainable andsupportive approach to improvement ininformation technology.
As part of this focus on building support within the system to improve capabilities, it is
imperative that when NHS England developshospital data, it ensures that providers of NHScare are able to absorb it.12 We support thismove and recognise it as a first step in anambitious strategy to move the NHS onto adigitally enabled path.
Developing skills among NHS staffMore needs to be done to increase the skills and capabilities of staff within the system toempower them to understand the informationalready available and how they can use it toimprove care. This should include staff acrossthe NHS, not just those at board level. Raisingawareness of the range of information alreadyavailable to the system will form an importantpart of this.
12. NHS England’s development of hospital data will expand the data collected from hospitals as part of the transformationof hospital episode statistics (HES) into care episode statistics (CES), starting in early 2014.
13. SingHealth, Commonwealth Health Ministers’ Book 2008.
Case study: Information sharing in Singapore
Singapore’s health system encouraged information sharing and reduced duplication in electronicmedical records (EMRs). The Ministry of Health created and provided start up funds for an ElectronicMedical Record Exchange (EMRX) for clinicians in public hospitals and polyclinics to share patientrecords online. They adopted a pull-on-demand policy with appropriate safeguards rather than a pre-delivery model. The system prevents duplication and, due to its success, has been extended toinclude operating theatre reports, discharge summaries, immunisation reports, school medicalreports and key safety alerts.13
“Most healthcare organisations atpresent have very little capacity toanalyse, monitor, or learn from safetyand quality information. This gap iscostly, and should be closed.”Berwick Review

Challenging bureaucracy26
Recommendation Who By when
17 Improve the processes for trusts supplying HSCIC Process to begin information to the HSCIC, for example by creating in 2014a single upload platform for all its data requests.
18 Rationalise collection tools and ensure details about HSCIC Summer 2014each are widely available so national bodies can consider the practicalities when scoping new collections.
19 In implementing care.data it will be important for NHS England NHS England and HSCIC to work with clinicians and the provider sector to understand the barriers to implementation and what the cost of overcoming those barriers will be. We would counsel the HSCIC and NHS England to work closely with trusts to understand the implications of the changes proposed.
20 Develop an index for providers to enable them to NHS England April 2014self-assess and benchmark their information technology capabilities and their business processes in place to manage information requests. We anticipatethis could become part of the overall approach to governance.
21 Use the index to identify and incentivise provider- NHS England April 2014level best practice by sharing lessons learnt and facilitating sharing of experiences, including how to improve technology capability, business processes and how to use information.
22 Work together to build capabilities and skills National bodies April 2014throughout healthcare staff, to support them to and providersunderstand the information already available to them and how they can use it. We recommend this is an areathat the ongoing Programme Advisory Group (PAG)should look at in more detail.
Challenging bureaucracy 27
Using data to improve care
It is important that the right datasets arecollected, and for information to be processedand made available in a timely way to enableimprovements in clinical care. The clinical staffwe interviewed largely understood the value ofthe data they collect and its relevance to patient care, but felt more could be done toincrease its value.
What we found
It is important that the right datasets arecollected, and that clinicians have access to anybenchmarked, comparative or outcomes dataresulting from that collection. The clinical staffwe interviewed largely understood the value ofthe data they collect and its relevance to patientcare, but many still felt the clinical relevance ofreports was often weak. One sector manager toldus that smaller but more meaningful amounts ofdata/reports, with clear links to patients’outcomes, would reduce cost and increase value.
Increasing the value of information
Developing a shared understanding of qualityand a core dataset to measure it – agreed byproviders, healthcare professionals, nationalbodies and patients – will help ensure the rightdata is collected.
More can be done to increase the value of existing informationWhile the burden on clinicians from nationalbodies appears to be small, clinicians collect asignificant amount of data and more could bedone to increase its value. The Health & SocialCare Information Centre (HSCIC) needs to domore to improve the value of national dataalready collected and extracted. We alsorecognise that the care professions, patients,carers and providers will need to co-own thisagenda and help design the way information ismade available to them.
There is great value in data; correctly collected,validated and shared, it has enormous power to improve the quality of clinical care in theNHS. Those we interviewed identified a number of programmes where collecting data and comparing performance had enabled trusts to improve clinical performance.This extended to inspections. A number ofclinicians expressed enthusiasm for CareQuality Commission (CQC) visits, which enabled them to show the quality of care theydelivered and learn how their practice could be improved.
However, there was a clear message that morecould be done to increase the value of what isalready collected. For example, there wasfrustration at the lack of a national dataset toenable performance to be compared at trust,specialty and clinician level. There was a strong sense that increasing the comparabilityof data would bring substantial benefits to thesystem.
• Clinical staff spend between two and tenhours a week collecting, recording orvalidating data (from all sources)
• The clinical staff we interviewed reported, onaverage, that 65 per cent of the data they collectis useful and relevant to patient care; this breaksdown to 69 per cent for acute providers and 59per cent for mental health providers
Key statistics
“Ensure the data is clinically relevant – not just counting activity.”Consultant psychiatrist
Challenging bureaucracy28
Time lag between data submission and returnThe time lag between submissions and returncan be long enough to reduce the usefulness ofthe information received. One trust explainedthat hospital episode statistics (HES) data wasnot useful for planning purposes by the time itwas returned.
Even once reports were returned, they wereoften not made available to staff, or weredifficult to understand and relate to patientcare. This supports what we heard through thenhsManagers.net survey, where 41 per cent said they did not receive any feedback. Whilemany interviewees felt that the HSCIC was thenatural repository for data, they said it needs to make substantial improvements to itsinformation technology and customer service.
Clinicians were keen for more transparency inthe rationale for requests and the way theinformation is used to make decisions. A clinicaldirector told us: “We want to understand therationale for the request and what is done withit – many clinicians believe there is a black holefilled with the stuff.”
Valued reportsReports that enabled real improvements inclinical care were consistently cited as the mostvalued reports by clinical front-line staff, such asthe Systemic Anti-Cancer Therapy dataset. This
dataset is overseen by cancer specialists and hasa deliberately small number of data fields (42) asunsubstantiated additions were aggressivelychallenged and a premium placed on rapidturnaround (three months, despite limitedresources and a complex subject area coveringmultiple organs and treatment schedules).Users felt that the dataset’s objective –demonstrating effectiveness and value formoney for an expensive and opaque treatment –is supported by the insights it provides.
What should be done
“The communication between whowants the data and who produces it isoften unclear and therefore takes a lotmore effort.”Clinical nurse specialist manager
“As a clinician trying to deliver stuffbased on data, it is really hard when allmy spare time goes into generatingdata. Less experienced clinicians, suchas junior doctors and nurses, never getpast data collection.”Acute medicine consultant
1. Clear link to patient outcomes
2. Communicate its role in decision making
3. Improve feedback mechanisms
4. Increase accessibility
Clinical staff told us the followingwould increase the value of existinginformation
Reduce turnaround time for submitted data The providers we interviewed cited thetimeliness of information as a significant issue,and therefore a shorter turnaround time forsubmitted data is essential. Making submitteddata available to trusts in a significantly shortertimeframe, with fully validated data to follow,would greatly improve how data can be used toimprove care for patients.

Challenging bureaucracy 29
Enable meaningful comparisonsIncreasing the comparability of data wouldbring substantial benefits. Using datasets tobenchmark financial, operational and clinicalperformance would enable trusts to understand how they are performing againsttheir peers. To ensure effective benchmarking,methods for calculating indicators will need tobe robust and transparent.
Improve feedback mechanisms and access Clinical staff requested improved feedbackmechanisms and accessibility to data andreports. Enabling easier user access to HSCIC’s online resources would make access to information considerably more
straightforward. We have previouslyrecommended a web portal.14
Increase the transparency of informationWhile this report has focused on improving the use of information for healthcare staff,making information and data more transparent and accessible to patients and the public should be a priority. The patientrepresentatives we interviewed expressed how difficult it can be for patients to navigatetheir way through data in a timely and accurate manner. It is essential that patientsand the public are able to get the most valueout of the information available about theirhealth service.
Clinical Audit
Figure 3. Reports most valued by clinical staff
“Show levels of service quality against standards”
Pressure ulcer Audit “Provides quality and safety assurance”
Falls Audit “Provides quality and safety assurance”
DocumentationAudit
“Gives opportunity to reviewrecords and improve practice”
National heartfailure Audit
“Highlights specific areas to focus on”
DepartmentalAudits
“Looks at specific clinicalactivities and outcomes”
TARN/MajorTrauma
“Helps to understand how to plan/improve care”
Risk assessment “Clients’ needs and risk can be monitored”
Nursing andMidwifery Dashboard
“Gives assurance that goodquality care is delivered”
NHS SafetyThermometer
“For improving high priorityinterventions”
Patient SafetyIndicators
“Overview of what is happening toidentify areas of good practice andfor improvement
Patient surveys andfeedback
“Highlights what we are doing welland shows us what we need toimpove on”
Outcome measures“PROM/PREM measurement asthey are the closest we have to truemeasures of quality”
Serious incidentreporting
“Helps us to learn lessons andimprove clinical care”
Mortality &Morbidity
“Identify and minimise risk”
Peer review “Identifies areas for action”
14. NHS Confederation (2013), Information overload.

Challenging bureaucracy30
Improve communication about why requestsare made and how data is usedImproving communication with healthcare staff so that they understand how data is usedand the full value of information when it is made available is a necessary task. This should be done in a way that ensures the value isunderstood across healthcare staff, and not justat board level. The HSCIC should publish a list ofthe data it collects, who requested it and why it is valuable.
Build on the strengths of the Keogh ReviewsThe CQC should build on the strengths of theprocess used for the Keogh Reviews whendesigning its new inspection regime. One of thestrongest innovations in the process was thedata packs containing the key statistics and
background information for each trust in onedocument. These packs allowed everyoneinvolved to have a shared understanding ofperformance, and swift comparisons betweendepartments could be made. The scope andthoroughness of the site visits were one of thestrongest aspects of the reviews.
Enable effective use of aggregate dataTo ensure the health service derives the mostvalue from the data healthcare staff collect,there is a real opportunity to use aggregate dataat a national level to better understand serviceuse. Analysis of provider data alongside otherdata, for example on nutritional and physicalactivity, would help increase the impact ofstrategies and policies for broader health andwellbeing promotion.
The London office of the National CancerRegistration Service has focused on improvingthe availability, timeliness and quality of cancerclinical information collected, as reported byNHS trusts in London, to the National CancerRegistry Service (NCRS).
Approach: their approach focused on improving local processes, practices andsystems so that cancer staging data could becollected as part of routine clinical workflow. Clinical teams were directly involved in the datacollection and took ownership and responsibilityfor the data quality. The Cancer Registry Teamand Data Improvement Team provided supportand guidance.
Timely, regular feedback to multi-disciplinaryteams (MDT) was given on the data theyprovided, specifically highlighting:
• successful achievements
• areas for improvement
• comparative performance across London.
In most cases, organisations did not need to buynew systems to collect this data, needing only torelease the data from their current systems.
Outcome: There were significant improvementsin the MDT’s staging data returns, from initiallows of 10–20 per cent up to the 70 per centtarget or above.
Case study: Improving cancer data

Challenging bureaucracy 31
Recommendation Who By when
23 Build on the strengths of the Keogh process in CQC Immediatelydesigning its new inspection regime. By working with the trusts involved, it should also identify where there are opportunities to create more value for the NHS from process.
24 Ensure a shorter turnaround time for submitted HSCIC Early 2014data and commit to making it available to trusts within 30 days of submission (with fully validated data to follow).
25 Explore ways of supporting trusts to benchmark HSCIC Early 2014financial, operational and clinical performance based on submitted datasets, within 60 days of submission.
26 Explore ways of supporting specialist services to HSCIC Early 2014benchmark financial, operational and clinical performance based on submitted datasets, within 60 days of submission.
27 Explore how to make information and data more All national Immediatelytransparent and accessible to patients and the public bodiesso they too get the most value from the information available about their health service.
28 Improve communication with providers so they HSCIC Late 2013understand how data is used and the value of information when it is made available. This should include extensive engagement with NHS staff to ensure value is not just understood at board level.
29 Ensure healthcare staff have easy access to online HSCIC Late 2013resources.
30 Establish a piece of work to develop the opportunity NHS England, to use aggregate data at national level alongside HSCIC, Public other datasets, to help understand resource use, Health Englandlifestyles and consumer habits and subsequently develop health promotion strategies.
Challenging bureaucracy32
We hope the findings of this report havecontributed to a better understanding of thebureaucratic burden placed on NHS providers bynational bodies, and that implementation of itsrecommendations will go some way to reducebureaucracy in the NHS. However, we haveidentified a number of other areas we thinkrequire more work if we are to fully succeed inour ambition to reduce the burden ofbureaucracy. We recommend that:
1. Further work is done to understand nationalreporting in other types of providers,including community providers, ambulanceproviders and independent sector providersof NHS care. Although our sample included anumber of integrated providers, we think itwould be beneficial to look at the experienceof community providers in more detail. Thisis especially important as care increasinglymoves into community settings.
Recommendations for further work
2. More work is completed to understand theimpact of the commissioning system andlocally driven bureaucracy, including overlapsand duplications across local and nationalbodies. This should not be limited to theimpact on providers, but include thebureaucratic burden experienced bycommissioners. This should also look atintegration and information sharing acrossdifferent organisations, including acrosshealth and social care.
3. The Programme Advisory Group for thisreview continues to meet and act in anadvisory capacity for future pieces of work, and oversees progress againstrecommendations made. We alsorecommend it publishes a statement ofprogress against the recommendations in six months’ time.

Challenging bureaucracy 33
Bureaucracy is an essential part of an effectivehealthcare system, enabling it to understand,assure and improve patient care and outcomesfor local populations. The effectiveness of anysystem rests on its ability to identify, challengeand address practices and processes thatcompromise the quality of care it delivers.
After the publication of the Francis report, wewere commissioned to investigate the burden ofbureaucracy on providers of NHS care. Ourreview has identified several instances ofunnecessary bureaucracy arising from nationalbodies, and uncovered their potential impactand costs. We have sought to challenge themechanisms, drivers and incentives causingunnecessary bureaucracy, and made tangiblerecommendations to address the issues to helpensure NHS staff are free to focus on deliveringhigh-quality care.
Conclusion: a three-part task
We found that reducing unnecessarybureaucracy will require a three-part task totackle the volume of requests, reduce the effortinvolved in responding and maximise the valueof collected information.
This sets a challenge not only to nationalbodies, but NHS providers themselves to takethe lead, where they can, to make sure thatinformation works harder for patients.
We will work with our provider members, theHealth & Social Care Information Centre,Department of Health and all of the nationalbodies to review the extent to which therecommendations in this report have beentaken up and implemented.

Challenging bureaucracy34
We would like to thank staff at the followingtrusts for their hard work and support to deliverthis report: Brighton and Sussex UniversityHospital NHS Trust; Central ManchesterUniversity Hospital NHS Foundation Trust;Central and North West London NHSFoundation Trust; Nottingham UniversityHospital NHS Trust; Salford Royal NHSFoundation Trust; South Tees Hospital NHSFoundation Trust; and South West YorkshirePartnership NHS Foundation Trust.
We would like to thank nhsManagers.net fortheir help in completing a survey of NHS staffearlier this year to support our interim report.
We would also like to thank the seniorrepresentatives we interviewed from thefollowing 14 national bodies:• British Orthopaedic Trainees Association• Care Quality Commission• Department of Health• General Medical Council • Health & Social Care Information Centre • Healthcare Quality Improvement Partnership • Monitor• National Cancer Intelligence Network • NHS Blood and Transplant• NHS England • NHS Trust Development Authority • Royal College of Nursing • Royal College of Physicians • Royal College of Radiologists
We would also like to acknowledge theProgramme Advisory Group (PAG) that hasprovided oversight and advice to the review, with representation from the followingorganisations:• Barchester Healthcare• Better Regulation Executive • British Medical Association
Acknowledgements
• Care Quality Commission
• Care UK
• CHKS
• Department of Health
• Environment Agency
• Foundation Trust Network
• General Medical Council
• General Pharmaceutical Council
• Health and Safety Executive
• Foundation Trust Network
• Health and Care Professions Council
• Health & Social Care Information Centre
• Health Education England
• Healthcare Quality Improvement Partnership
• Human Fertilisation and Embryology Authority
• Human Tissue Authority
• Independent Healthcare Advisory Services
• Leeds and York Partnership NHS FoundationTrust
• Monitor
• National Institute for Health & CareExcellence
• NHS Clinical Commissioners
• NHS England
• NHS Litigation Authority
• NHS North Yorkshire and HumberCommissioning Support Unit
• NHS Trust Development Authority
• Nursing and Midwifery Council
• Oxford University Hospitals NHS Trust
• Public Health England
• Royal College of Nursing
• Royal College of Physicians
• King’s College Hospital NHS Foundation Trust
• West Midlands Ambulance Service NHSFoundation Trust
Challenging bureaucracy 35
Department of Health (2013), Fundamentalreview of data returns.
Department of Health (2011), Fundamentalreview of data returns: a consultation on therecommendations of the review.
NHS Confederation (2013), Informationoverload.
NHS Confederation and IndependentHealthcare Advisory Services (2009), What’s it all for? Removing unnecessary bureaucracy in regulation.
NHS England (2013), NHS hospital data anddatasets: a consultation.
Royal College of Nursing (2012), Paperwork andadministration.
Department for Business Innovation and Skills(2013), Better regulation framework manual
Further reading
Royal College of Physicians (2011), Response ofthe Royal College of Physicians to equity andexcellence: Liberating the NHS.
Health & Social Care Information Centre,Academy of Medical Royal Colleges (2013),Standards for the clinical structure and contentof patient records. London.
National Advisory Group on the Safety ofPatients in England (2013), A promise to learn –a commitment to act: improving the safety ofpatients in England.
Professor Sir Bruce Keogh KBE (2013),Review into the quality of care and treatmentprovided by 14 hospital trusts in England:overview report.
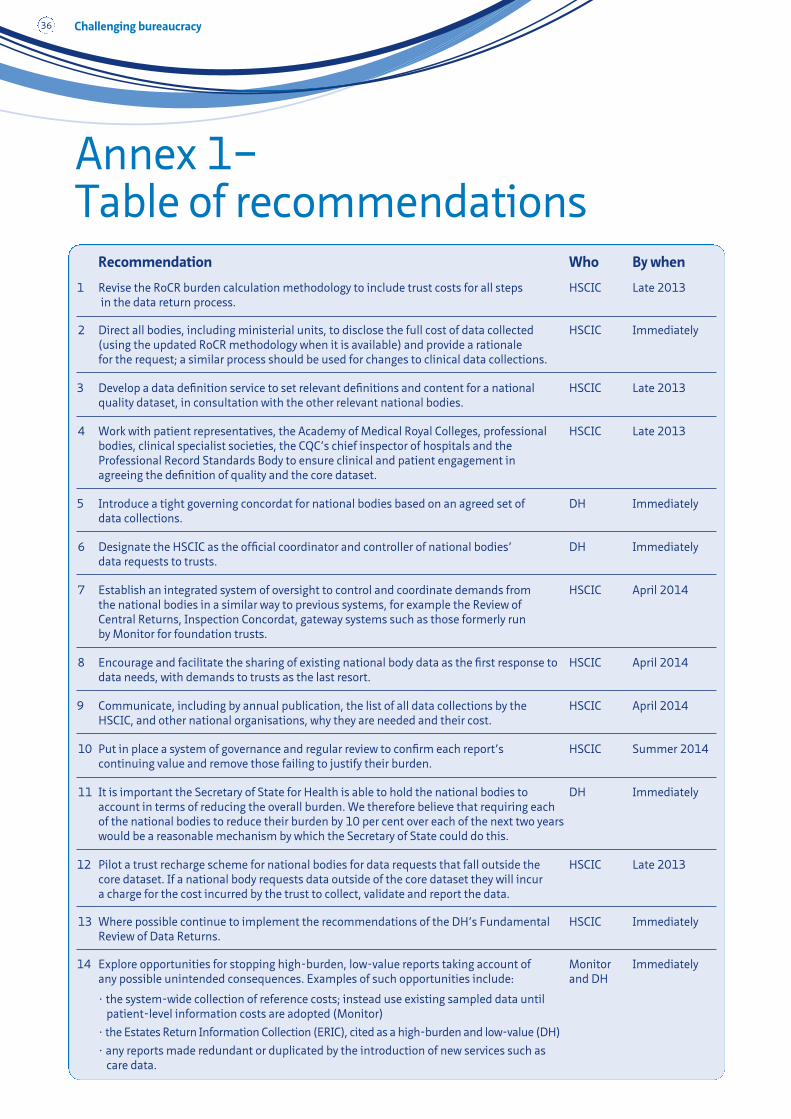
Challenging bureaucracy36
Annex 1– Table of recommendations
Recommendation Who By when
1 Revise the RoCR burden calculation methodology to include trust costs for all steps HSCIC Late 2013in the data return process.
2 Direct all bodies, including ministerial units, to disclose the full cost of data collected HSCIC Immediately(using the updated RoCR methodology when it is available) and provide a rationalefor the request; a similar process should be used for changes to clinical data collections.
3 Develop a data definition service to set relevant definitions and content for a national HSCIC Late 2013quality dataset, in consultation with the other relevant national bodies.
4 Work with patient representatives, the Academy of Medical Royal Colleges, professional HSCIC Late 2013bodies, clinical specialist societies, the CQC’s chief inspector of hospitals and the Professional Record Standards Body to ensure clinical and patient engagement in agreeing the definition of quality and the core dataset.
5 Introduce a tight governing concordat for national bodies based on an agreed set of DH Immediatelydata collections.
6 Designate the HSCIC as the official coordinator and controller of national bodies’ DH Immediatelydata requests to trusts.
7 Establish an integrated system of oversight to control and coordinate demands from HSCIC April 2014the national bodies in a similar way to previous systems, for example the Review of Central Returns, Inspection Concordat, gateway systems such as those formerly run by Monitor for foundation trusts.
8 Encourage and facilitate the sharing of existing national body data as the first response to HSCIC April 2014data needs, with demands to trusts as the last resort.
9 Communicate, including by annual publication, the list of all data collections by the HSCIC April 2014HSCIC, and other national organisations, why they are needed and their cost.
10 Put in place a system of governance and regular review to confirm each report’s HSCIC Summer 2014continuing value and remove those failing to justify their burden.
11 It is important the Secretary of State for Health is able to hold the national bodies to DH Immediatelyaccount in terms of reducing the overall burden. We therefore believe that requiring each of the national bodies to reduce their burden by 10 per cent over each of the next two years would be a reasonable mechanism by which the Secretary of State could do this.
12 Pilot a trust recharge scheme for national bodies for data requests that fall outside the HSCIC Late 2013core dataset. If a national body requests data outside of the core dataset they will incur a charge for the cost incurred by the trust to collect, validate and report the data.
13 Where possible continue to implement the recommendations of the DH’s Fundamental HSCIC ImmediatelyReview of Data Returns.
14 Explore opportunities for stopping high-burden, low-value reports taking account of Monitor Immediatelyany possible unintended consequences. Examples of such opportunities include: and DH
• the system-wide collection of reference costs; instead use existing sampled data until patient-level information costs are adopted (Monitor)
• the Estates Return Information Collection (ERIC), cited as a high-burden and low-value (DH)
• any reports made redundant or duplicated by the introduction of new services such as care data.
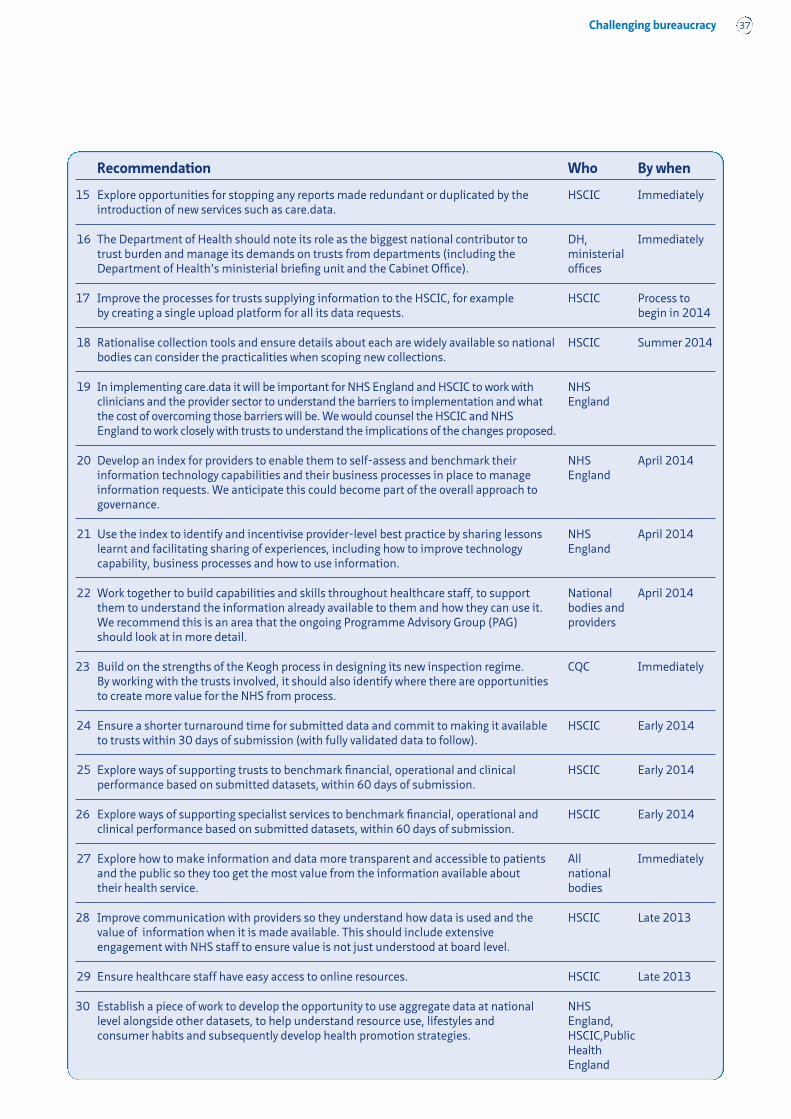
Challenging bureaucracy 37
Recommendation Who By when
15 Explore opportunities for stopping any reports made redundant or duplicated by the HSCIC Immediatelyintroduction of new services such as care.data.
16 The Department of Health should note its role as the biggest national contributor to DH, Immediatelytrust burden and manage its demands on trusts from departments (including the ministerial Department of Health’s ministerial briefing unit and the Cabinet Office). offices
17 Improve the processes for trusts supplying information to the HSCIC, for example HSCIC Process to by creating a single upload platform for all its data requests. begin in 2014
18 Rationalise collection tools and ensure details about each are widely available so national HSCIC Summer 2014bodies can consider the practicalities when scoping new collections.
19 In implementing care.data it will be important for NHS England and HSCIC to work with NHS clinicians and the provider sector to understand the barriers to implementation and what Englandthe cost of overcoming those barriers will be. We would counsel the HSCIC and NHS England to work closely with trusts to understand the implications of the changes proposed.
20 Develop an index for providers to enable them to self-assess and benchmark their NHS April 2014information technology capabilities and their business processes in place to manage Englandinformation requests. We anticipate this could become part of the overall approach to governance.
21 Use the index to identify and incentivise provider-level best practice by sharing lessons NHS April 2014learnt and facilitating sharing of experiences, including how to improve technology Englandcapability, business processes and how to use information.
22 Work together to build capabilities and skills throughout healthcare staff, to support National April 2014them to understand the information already available to them and how they can use it. bodies and We recommend this is an area that the ongoing Programme Advisory Group (PAG) providersshould look at in more detail.
23 Build on the strengths of the Keogh process in designing its new inspection regime. CQC ImmediatelyBy working with the trusts involved, it should also identify where there are opportunities to create more value for the NHS from process.
24 Ensure a shorter turnaround time for submitted data and commit to making it available HSCIC Early 2014to trusts within 30 days of submission (with fully validated data to follow).
25 Explore ways of supporting trusts to benchmark financial, operational and clinical HSCIC Early 2014performance based on submitted datasets, within 60 days of submission.
26 Explore ways of supporting specialist services to benchmark financial, operational and HSCIC Early 2014clinical performance based on submitted datasets, within 60 days of submission.
27 Explore how to make information and data more transparent and accessible to patients All Immediatelyand the public so they too get the most value from the information available about nationaltheir health service. bodies
28 Improve communication with providers so they understand how data is used and the HSCIC Late 2013value of information when it is made available. This should include extensive engagement with NHS staff to ensure value is not just understood at board level.
29 Ensure healthcare staff have easy access to online resources. HSCIC Late 2013
30 Establish a piece of work to develop the opportunity to use aggregate data at national NHS level alongside other datasets, to help understand resource use, lifestyles and England, consumer habits and subsequently develop health promotion strategies. HSCIC,Public
Health England

In February 2013, the Secretary of State for Healthcommissioned the NHS Confederation to complete areview of the bureaucratic burdens on providers of NHScare from national bodies. The request followedpublication of Robert Francis QC’s report into failings incare at Mid Staffordshire NHS Foundation Trust.
Challenging bureaucracyThis report sets out what we found and what actionsshould be taken to free the NHS from unnecessarybureaucracy. We believe our recommendations willhelp ensure that healthcare staff spend as much timeas possible delivering patient care.
Alternative formats can be requested from:Tel 0870 444 5841 Email: [email protected] visit www.nhsconfed.org/publications© The NHS Confederation 2013. You may copy or distribute this work, but you must givethe author credit, you may not use it for commercial purposes, and you may not alter,transform or build upon this work.
Registered Charity no: 1090329
Stock code: BOK60069
The NHS Confederation50 Broadway London SW1H 0DBTel 020 7799 6666Email [email protected]
Follow the NHS Confederation on Twitter@nhsconfed





























