Embed Size (px)
Citation preview

Challenging Melanocytic Lesions
Carlos N. Prieto-Granada M.D.Assistant Professor
University of Alabama at Birmingham (UAB) Department of Pathology
2018 AAD Annual Meeting2/17/18 – San Diego, CA
Conflicts of InterestNone

Objectives• Case-based review of salient features
from related melanocytic lesions• Quick review of molecular methods used
in diagnosis of melanocytic lesions

Acknowledgments• Jane Messina M.D. and Vernon Sondak
M.D. – Moffitt Cancer Center• Maria Auxiliadora Deschaine M.D. –
University of Oklahoma• Julie V. Schaffer M.D. - Hackensack
University

Case #1

Case #1- Clinical Features10 y/o female, rapidly growing lesions
Pictures courtesy of Dr. Jane Messina and Dr. Vernon Sondak

Case #1- Histopathology

Case #1- Histopathology

Case #1 - DiagnosisA. Juvenile XanthogranulomaB. Dysplastic NevusC. Spitz NevusD. Melanoma E. Benign Epithelioid Histiocytoma

Case #1 - DiagnosisA. Juvenile XanthogranulomaB. Dysplastic NevusC. Spitz NevusD. MelanomaE. Benign Epithelioid Histiocytoma

Classic Spitz Nevus• AKA “Spindle and Epithelioid Cell
Nevus”• First known description from Darier
and Civatte as early as1910 • Characterized by Dr. Sophie Spitz in
1948 as “Melanomas of Childhood” in a series of 13 cases from patients aged 18 months to 12 years old
• Only 1 patient died of widely metastatic disease from a primary lesion consisting of an acral spindle cell tumor associated to the fascia (Clear Cell Sarcoma?)
Spitz S. Am J Pathol. 1948;24:591-609.Barnhill RL. Mod Pathol. 2006;19 Suppl 2:S21-33. Picture courtesy of Dr. Martin C. Mihm

PhotoscourtesyofDr.JulieSchaffer
JXG-like PG-like
Pigmented

Architecture• Usually compound -
predominantly junctional (Reed), dermal (desmoplastic) variants
• Junctional component:– Well-circumscribed large nests
of cells in a “raining down” pattern
– Epidermal hyperplasia – Kamino bodies
• Dermal component: • Symmetrical, imparting a
dome shape to the lesion • Inverted triangle shape with
evident maturation (“zonation”)
Cytology• Epithelioid and spindle cells
with: – Pink/“hyalinized” cytoplasm– Large, often pleomorphic
nuclei with vesicular chromatin and prominent nucleoli
– Bizarre forms and giant cells can be seen
• Pagetoid spread is common (Pagetoid variant)
• Mitoses are commonly seen (rapid growth) (less than 6 per mm2)
Busam KJ, Barnhill RL. Am J Surg Pathol. 1995 Sep;19(9):1061-7 Barnhill RL. Mod Pathol. 2006;19 Suppl 2:S21-33.



Case #1 –Which of these stains will be helpful in problematic cases?
A. S100 and Sox10B. Tyrosinase and Mart-1C. HMB45 and p16D. Trichrome and PAS
Case #1 –Which of these stains will be helpful in problematic cases?
A. S100 and Sox10B. Tyrosinase and Mart-1C. HMB45 and p16D. Trichrome and PAS

p16: product of the CDKN2A gene (9p21.3) HBM45: Melanosome associated antigen
Ki-67 and Mart-1 cocktail

Case #2

Case #2 – Clinical/Dermoscopic Features
Pedrosa AF et al Dermatol Pract Concept. 2016 Apr 30;6(2):37-41 PhotocourtesyofDr.JulieSchaffer
20 y/o female, lower leg pigmented lesion

Case #2 – Histopathology

Case #2 - DiagnosisA. Common Acquired NevusB. Dysplastic NevusC. Spindle Cell MelanomaD. Pigmented Spindle Cell Nevus of Reed E. Atypical Spitz Tumor

Case #2 - DiagnosisA. Common Acquired NevusB. Dysplastic NevusC. Spindle Cell MelanomaD. Pigmented Spindle Cell Nevus of Reed E. Atypical Spitz Tumor

Pigmented Spindle Cell Nevus of Reed• AKA “Pigmented Spindle Cell
Tumor of Reed”• First described by Dr. Richard
J. Reed in 1975• “Dark brown-black macular or
papular dome-shaped lesion appearing in the lower limbs of females in the first 4 decades of life”
Reed RJ et al. Semin Oncol. 1975 Jun;2(2):119-47

Picture courtesy of Dr. Martin C. Mihm
Pigmented Spindle Cell Nevus of Reed
PhotocourtesyofDr.JulieSchaffer

Pictures courtesy of Dr. Martin C. Mihm
Pigmented Spindle Cell Nevus of Reed

Case #2 – How would you treat these lesions (Classic Spitz and PSCN) (2 might be correct)
A. Observe and re-excise upon recurrenceB. Conservative (narrow margin) re-excisionC. Wide local excision with 5-10 mm margin D. Wide local excision with 10 mm margin
and sentinel lymph node biopsyE. Cryotherapy

Case #2 – How would you treat these lesions (Classic Spitz and PSCN) (2 might be correct)
A. Observe and re-excise upon recurrenceB. Conservative (narrow margin) re-excisionC. Wide local excision with 5-10 mm margin D. Wide local excision with 10 mm margin and
sentinel lymph node biopsyE. Cryotherapy

Case #3

Case #3 – Clinical Features
Pictures courtesy of Dr. Ma. Auxiliadora Deschaine and Dr. Jane Messina
14 y/o female, right arm lesion

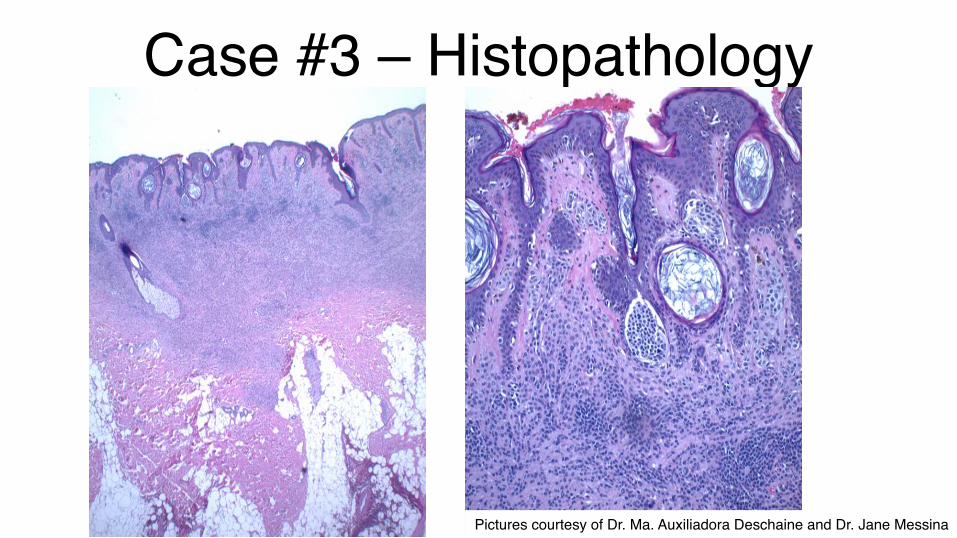
Case #3 – Histopathology
Pictures courtesy of Dr. Ma. Auxiliadora Deschaine and Dr. Jane Messina

Case #3 – Histopathology
Pictures courtesy of Dr. Ma. Auxiliadora Deschaine and Dr. Jane Messina

Case #3 - DiagnosisA. Intradermal melanocytic nevus B. Classic Spitz NevusC. Spitzoid MelanomaD. Desmoplastic Spitz NevusE. Benign Epithelioid Histiocytoma

Case #3 - DiagnosisA. Intradermal melanocytic nevus B. Classic Spitz NevusC. Spitzoid MelanomaD. Desmoplastic Spitz NevusE. Benign Epithelioid Histiocytoma

Desmoplastic Spitz Nevus• Uncommon Spitz variant,
usually presents in the extremities as scaly, erythematous, flesh-colored or occasionally pigmented papulonodule
• Affected patients are usually in the third decade of life
• The lesions usually show variable amount of fibrosis/hyalinization and are often dermal-based
Moscarella E et al Br J Dermatol. 2015 Apr;172(4):1045-51Bastian BC et al Am J Pathol. 2000 Sep;157(3):967-72.

Mart -1 negativeCD68 positiveCD163 positiveMart -1 positive
McKee PH, Calonje E, Granter SR. Pathology of the skin with clinical correlations Philadelphia Elsevier Mosby; 2005Glusac, Earl; McNiff, Jennifer American Journal of Dermatopathology. 21(1):1-7, February 1999.Cangelosi JJ Am J Dermatopathol. 2008 Aug;30(4):373-6.
Desmoplastic Spitz Nevus Benign Epithelioid Histiocytoma
Benign Epithelioid Histiocytoma

Case #3 – Clinical Features
Pictures courtesy of Dr. Ma. Auxiliadora Deschaine and Dr. Jane Messina
Case #3 – Histopathology
Pictures courtesy of Dr. Ma. Auxiliadora Deschaine and Dr. Jane Messina

Case #3 – Histopathology
Pictures courtesy of Dr. Ma. Auxiliadora Deschaine and Dr. Jane Messina
Case #3 – Diagnosis of Background Lesion
A. Lentigo maligna melanomaB. EphelidesC. Nevus spilus (Agminated Nevus)
(segmental variant)D. Nevoid MelanomaE. Nevus spilus (Agminated Nevus)

Case #3 – Diagnosis of Background Lesion
A. Lentigo maligna melanomaB. EphelidesC. Nevus spilus (Agminated Nevus)
(segmental variant)D. Nevoid MelanomaE. Nevus spilus (Agminated Nevus)

Haenssle HA et al J Am Acad Dermatol. 2009 Aug;61(2):337-41
Common Nevus Spilus
Nevus Spilus
Segmental Nevus Spilus

Case #3
Pictures courtesy of Dr. Ma. Auxiliadora Deschaine and Dr. Jane Messina

Case #3 – Which genetic aberration characterizes this type of Spitz nevus (desmoplastic)?
A. BAP1 lossB. BRAF V600EC. HRAS amplificationsD. BRAF fusionsE. ALK1 fusions

Case #3 – Which genetic aberration characterizes this type of Spitz nevus (desmoplastic)?
A. BAP1 lossB. BRAF V600EC. HRAS amplificationsD. BRAF fusionsE. ALK1 fusions

Desmoplastic Spitz NevusThe majority of Spitz lesions with desmoplastic features will show an activation of HRAS (11p15.5), through either:
- Increased copy number of 11p (amplification) - Activating mutations of HRAS
Bastian BC et al Am J Pathol. 2000 Sep;157(3):967-72.

HRASp.G13R,p.A11Sandamplification
HRASp.G13R,p.A11Sandamplification
Porubsky C et al J Cutan Pathol. 2018 Feb;45(2):180-183.
Proline for Arginine in position 13Alanine for Serine in position 11

Sarin KY et al JAMA Dermatol. 2013 Sep;149(9):1077-81

Molecular Taxonomy of Melanocytic Lesions
Wiesner T et al Pathology. 2016 Feb;48(2):113-31.
BAP1 LossALK1

Case #3 – How would you treat/manage this patient (2 might be correct)
A. Observe and excise new lesionsB. Wide local excision with 5-10 mm margin C. Wide local excision with 10 mm margin
and sentinel lymph node biopsyD. If amenable, re-excision with narrow
margins and plastic reconstruction
Case #3 – How would you treat/manage this patient (2 might be correct)
A. Observe and excise new lesionsB. Wide local excision with 5-10 mm margin C. Wide local excision with 10 mm margin
and sentinel lymph node biopsyD. If amenable, re-excision with narrow
margins and plastic reconstruction

Case #4

Case #4 – Clinical/Dermoscopic Features
Yoradjian A et al An Bras Dermatol. 2012 May-Jun;87(3):349-57
11 y/o male, chest lesion

Case #4 – Histopathology

Case #4 – Histopathology
Case #4 - DiagnosisA. Spitzoid MelanomaB. Spitz NevusC. Atypical Spitz Tumor/NevusD. Superficial Spreading MelanomaE. Granular Cell Tumor

Case #4 - DiagnosisA. Spitzoid MelanomaB. Spitz NevusC. Atypical Spitz Tumor/NevusD. Superficial Spreading MelanomaE. Granular Cell Tumor

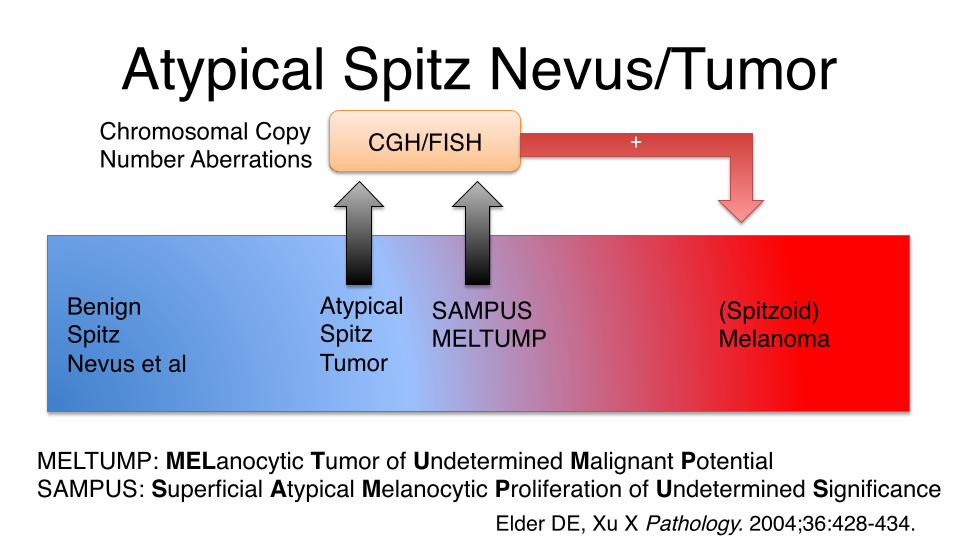
Atypical Spitz Nevus/Tumor

Atypical Spitz Nevus/Tumor

Atypical Spitz Nevus/Tumor
Atypical Spitz Nevus/Tumor
Benign Spitz Nevus et al
Atypical Spitz Tumor
SAMPUSMELTUMP
(Spitzoid) Melanoma
MELTUMP: MELanocytic Tumor of Undetermined Malignant PotentialSAMPUS: Superficial Atypical Melanocytic Proliferation of Undetermined Significance
CGH/FISH +Chromosomal Copy Number Aberrations
Elder DE, Xu X Pathology. 2004;36:428-434.

1. 6p25: RREB1 (Ras-responsive binding protein) > 2 copies
2. 6q23: MYB (myeloblastosis viral oncogene) loss*
3. 11q13: CCDN1 (cyclin-D1 protein) > 2 copies
4. CEP6: centromere of 6 5. 8q24: MYC > 2 copies6. 9p21: CDKN2A (p16 protein) loss*7. CEP9: centromere of 9 Pros: No limit in terms of cellularity, relatively easy to do, quick turnaround timeCons: Technical difficulties, required thresholds/ratios, narrow view of the potential aberrations, might be hampered by poly/aneuploidy or senescent changes
FISH Vs. CGHFISH CGH
Analysis of genomic material of tumor versus normal Pros: Panoramic, comprehensive view of the genomeCons: Special equipment is required, limit in thickness 0.4 mm., certain findings are still of undetermined significance
Modified from Dr. Timothy McCalmont’s ASDP board review lecture

FISH findings and prognosis in Atypical Spitzoid Lesions
• 9p21: CDKN2A (codes for p16Ink4A) homozygous deletion – associated with “high risk lesions”
• 6q23: MYB (codes for MYB protein) isolated loss – associated with “low risk lesions”
Tetzlaff MT et al , Clin Lab Med. 2017;37(3):431-448.

Case #4 – How would you treat these lesions (Atypical Spitz nevus/tumor) (2 might be correct)
A. Observe and re-excise upon recurrenceB. Conservative (narrow margin) re-excisionC. Wide local excision with 5-10 mm margin D. Wide local excision with 10 mm margin and
clinical follow up of lymph node basin(s)E. Cryotherapy

Case #4 – How would you treat these lesions (Atypical Spitz nevus/tumor) (2 might be correct)
A. Observe and re-excise upon recurrenceB. Conservative (narrow margin) re-excisionC. Wide local excision with 5-10 mm margin D. Wide local excision with 10 mm margin
and clinical follow up of lymph node basin(s)
E. Cryotherapy

The End! Questions?Thank you very much for your
attention/endurance

References1. Barnhill RL. The Spitzoid lesion: rethinking Spitz tumors, atypical variants, 'Spitzoid melanoma' and risk assessment. Mod Pathol. 2006;19 Suppl
2:S21-33.2. Busam KJ, Barnhill RL. Pagetoid Spitz nevus. Intraepidermal Spitz tumor with prominent pagetoid spread. Am J Surg Pathol. 1995 Sep;19(9):1061-7.3. McKee PH, Calonje E, Granter SR. Pathology of the skin : with clinical correlations / [edited by] Phillip H. McKee, Eduardo Calonje, Scott R. Granter.
Edinburgh: Philadelphia Elsevier Mosby; 2005.4. Pedrosa AF, Lopes JM, Azevedo F, Mota A. Spitz/Reed nevi: a review of clinical-dermatoscopic and histological correlation. Dermatol Pract Concept.
2016 Apr 30;6(2):37-41.5. Reed RJ, Ichinose H, Clark WH Jr, Mihm MC Jr. Common and uncommon melanocytic nevi and borderline melanomas. Semin Oncol. 1975 Jun;2(2):
119-47.6. Wiesner T, Kutzner H, Cerroni L, et al. Genomic aberrations in spitzoid melanocytic tumours and their implications for diagnosis, prognosis and
therapy. Pathology. 2016;48:113-131.7. Moscarella E, Al Jalbout S, Piana S, Argenziano G, Lallas A, Longo C, Hofmann-Wellenhof R, Zalaudek I. The stars within the melanocytic garden:
unusual variants of Spitz naevi. Br J Dermatol. 2015 Apr;172(4):1045-51.8. Porubsky C(1), Teer JK(2)(3), Zhang Y(2), Deschaine M(3), Sondak VK(4), Messina JL(3)(4)Genomic analysis of a case of agminated Spitz nevi and
congenital-pattern nevi arising in extensive nevus spilus. J Cutan Pathol. 2018 Feb;45(2):180-183. 9. Bastian BC, LeBoit PE, Pinkel D. Mutations and copy number increase of HRAS in Spitz nevi with distinctive histopathological features. Am J Pathol.
2000;157:967-972.10. Sarin KY, Sun BK, Bangs CD, Cherry A, Swetter SM, Kim J, Khavari PA. Activating HRAS mutation in agminated Spitz nevi arising in a nevus spilus.
JAMA Dermatol. 2013 Sep;149(9):1077-81.11. Luo S, Tsao H. Epidermal, sebaceous, and melanocytic nevoid proliferations are spectrums of mosaic RASopathies. J Invest Dermatol. 2014 Oct;
134(10):2493-6.12. Glusac EJ(1), McNiff JM. Epithelioid cell histiocytoma: a simulant of vascular and melanocytic neoplasms. Am J Dermatopathol. 1999 Feb;21(1):1-7.13. Cangelosi JJ(1), Prieto VG, Baker GF, Moore BA, Diwan AH. Unusual presentation of multiple epithelioid cell histiocytomas. Am J Dermatopathol.
2008 Aug;30(4):373-6.14. Haenssle HA, Kaune KM, Buhl T, Thoms KM, Padeken M, Emmert S, Schön MP. Melanoma arising in segmental nevus spilus: detection by
sequential digital dermatoscopy. J Am Acad Dermatol. 2009 Aug;61(2):337-41.15. Yoradjian A, Enokihara MM, Paschoal FM. Spitz nevus and Reed nevus. An Bras Dermatol. 2012 May-Jun;87(3):349-5716. Elder DE, Xu X. The approach to the patient with a difficult melanocytic lesion. Pathology. 2004;36:428-434.17. Tetzlaff MT, Reuben A, Billings SD, Prieto VG, Curry JL. Toward a Molecular-Genetic Classification of Spitzoid Neoplasms. Clin Lab Med. 2017;37(3):
431-448.18. Theisen, A. (2008) Microarray-based Comparative Genomic Hybridization (aCGH). Nature Education 1(1):4519. Gerami P, Cooper C, Bajaj S, et al. Outcomes of atypical spitz tumors with chromosomal copy number aberrations and conventional melanomas in
children. Am J Surg Pathol. 2013;37:1387-1394.20. Gerami P, Busam K, Cochran A, et al. Histomorphologic assessment and interobserver diagnostic reproducibility of atypical spitzoid melanocytic
neoplasms with long-term follow-up. Am J Surg Pathol. 2014;38:934-940.