Embed Size (px)
Citation preview
Challenging Symptom Management:
Delirium, Agitation and
Sleeplessness
Shellie Williams, M.D.
University of Chicago Medicine
CE Provider Statements
Rush University Medical Center is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. Rush University Medical Center designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)™. Physicians should claim only credit commensurate with the extent of their participation in the activity.
Rush University is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's Commission on Accreditation. Rush University designates this live/internet enduring material activity for 1.0 Continuing Education credits.
CE Provider Statements & Conflict of Interest Disclosure
This activity is being presented without bias and without commercial support.
Rush University is an approved provider for physical therapy (216.000272), occupational therapy, respiratory therapy, social work (159.001203), nutrition, speech-audiology, and psychology by the Illinois Department of Professional Regulation. Rush University designates this live activity for 1.0 Continuing Education credits.
Disclosure of Conflict of Interest
This presenter has no conflict of interest to disclose.
Objectives
• Identify the common pathophysiology for challenging
symptoms in the palliative care patient.
• Recognize predisposing and precipitating factors for
delirium in the palliative care patient.
• Treat the distressing symptom of agitation associated with
delirium.
• Outline a treatment strategy for sleep disturbance in the
palliative care patient.
Mrs. A
75 yo widow with triple negative stage IV breast cancer (bone, brain mets). Recent xrt brain mets. Daughters note 3 day confusion, lethargy, withdrawn, not
sleeping. HR 110, furrow brow, dry mucosa, abdomen distended,
reaching in air, yelling for her deceased husband with periods of sedation. In ER 0.9 Nacl 125 cc/hr, hydromorphone 1mg iv for pain
and ativan 1mg for agitation. Home Decadron 6 mg bid, Fentanyl patch 50 mcg, Zofran 4 mg q 6 prn. Labs: bun/cr 50/1.4. UA sg 1.030, CXR LLL atelactasis,
KUB diffuse stool pattern. Her daughters tearfully watch her in a confused and
agitated state. “What is happening?” “This is not our mother!”
Challenging Symptoms: Delirium,
Agitation, Sleeplessness
DELIRIUM
AGITATION
INSOMNIA
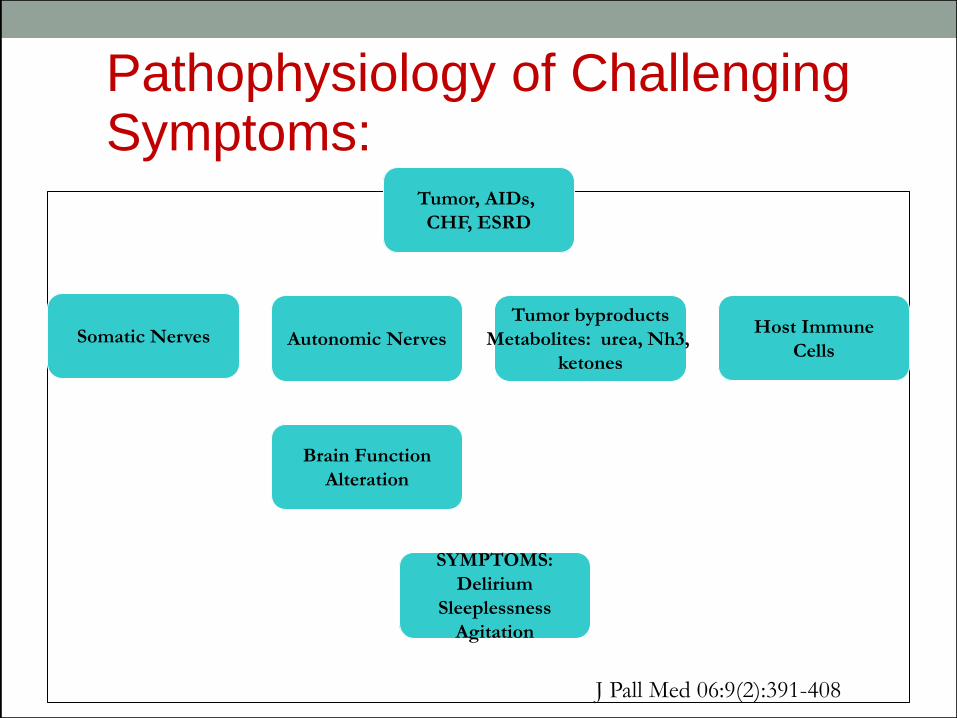
Pathophysiology of Challenging Symptoms:
Tumor, AIDs,
CHF, ESRD
Somatic Nerves Autonomic Nerves
Tumor byproducts
Metabolites: urea, Nh3,
ketones
Brain Function
Alteration
SYMPTOMS:
Delirium
Sleeplessness
Agitation
Host Immune
Cells
J Pall Med 06:9 (2): 391-408 J Pall Med 06:9(2):391-408
Delirium: Defined, DSM-V Disturbance of consciousness (ie, reduced clarity of
awareness of the environment) with reduced ability to focus,
sustain, or shift attention.
Change in cognition (eg, memory deficit, disorientation,
language disturbance, perceptual disturbance) not better
accounted for by a preexisting or established dementia.
The disturbance develops over a short period (usually hours
to days) and tends to fluctuate during the course of the day.
Evidence from the history, physical examination, or lab
findings is present that indicates the disturbance is caused
by a direct physiologic consequence of a general medical
condition, intoxicating substance, medication or other
cause.
Delirium: Prevalence
22%-44% palliative care unit patients at admission
50% advanced cancer patients
68%-90% palliative care patients 30 days prior to death
Reversible in 50% palliative population
1. Leonard M, etal. J Psychosom Res. 2008 Sep;65(3):289-98 2. Morita T, etal. J Pain Sympt Manage 2007;34:579-589
Delirium: Morbidity/Mortality
Life threatening diagnosis
10-26% Higher Mortality
22-76% Increased rate death months post hospitalization
Excess rates Caregiver Stress
Leading cause for Palliative Sedation requests
J Psycho Som Res 2008 J Pain Sym Man 2011; 26 (2) 97-109
Delirium: Pathophysiology
Neurotransmitter Theory:
Cholinergic deficits: benadryl, scopalmine
Norephinephrine excess: antidepressants
Dopamine excess: anti-parkinson meds, anti-psychotics
Cytokines-IL1, IL2, TNF
Cerebral Hypoxia
Stress related hormonal changes
Delirium: Predisposing Factors
Advanced Cancer/Terminal diagnosis
Opioid Therapy
Multiple co-morbidities
Cognitive Impairment
Surgical need
Renal/Hepatic Impairment
Sensory Impairment
Imminent Dying
Advanced Age
Lawlor, P. JAMA, 2000; 284(19): 2427-29
Delirium: Precipitating Factors
Medications
Infection
Metabolic Disturbances
Dehydration
Immobility
Untreated pain
Environment: ICU, changes
Malnutrition
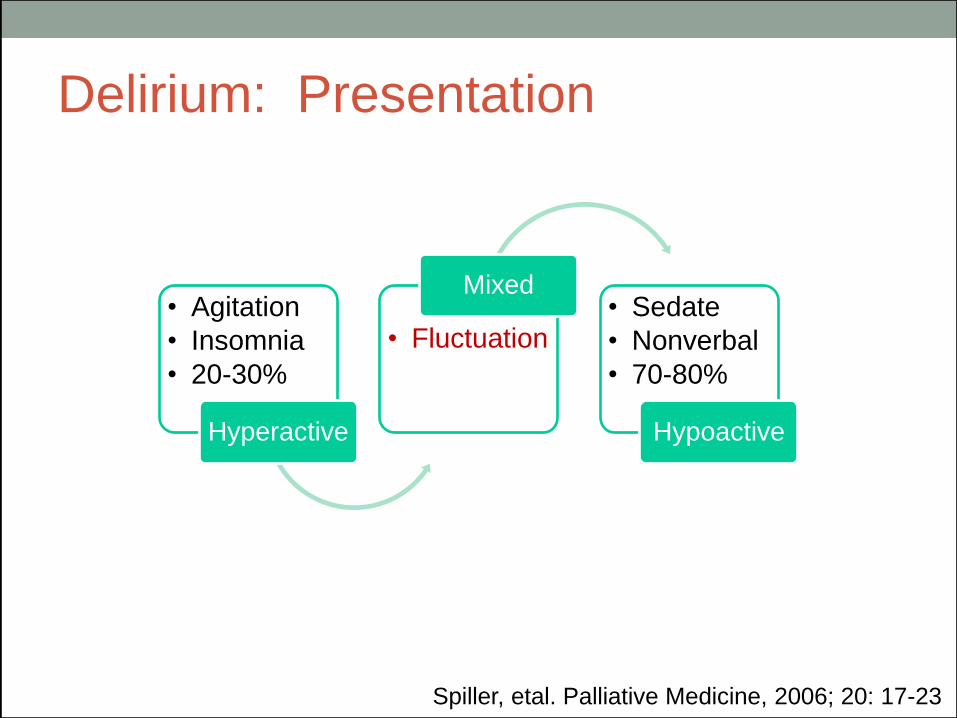
Delirium: Presentation
Spiller, etal. Palliative Medicine, 2006; 20: 17-23
• Agitation
• Insomnia
• 20-30%
Hyperactive
• Fluctuation
Mixed • Sedate
• Nonverbal
• 70-80%
Hypoactive
Delirium: Presentation Terminal
Delirium
Cardinal sign of imminent death (hours-days)
86% Imminently Dying
Hypoactive >80%
Refractory to correction in some cases (50%)
Spiller, etal. Palliative Medicine, 2006; 20: 17-23
Delirium: Agitation Presentation
Hyper-alert
Pacing
Picking Skin
Refusals of care
Vivid hallucinations
Delusions
Homicidal
Suicidal
Spiller, JA. Pall Med 2006; 20: 17-23
Delirium: Family Experience
• Impedes Communication • Limits patient/family precious time
• Creates anxiety & fear
• Overwhelm with care of patient • Feel premature separation • Shift in burden of decision-making
Delirium: Guiding Steps for Family
and Clinician
• Normal in advanced disease • Treatable in most • Patient’s and family’s goals of care direct
evaluation, treatment • Weigh burden of evaluation • Evaluate likelihood a reversible etiology will be
found (50%) • Feasibility of treatment
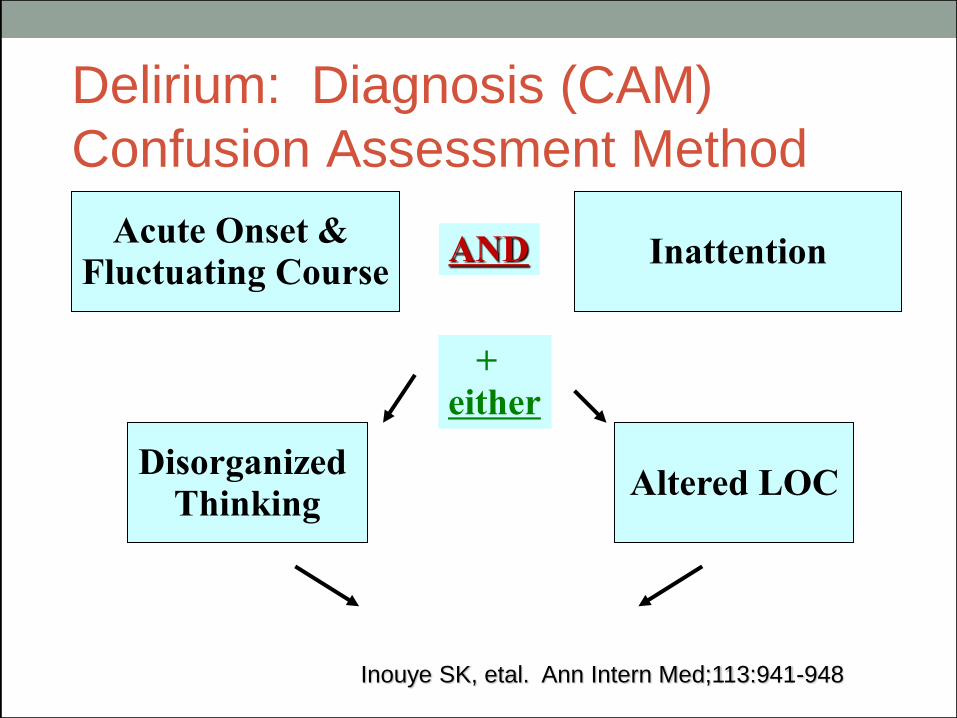
Delirium: Diagnosis (CAM)
Confusion Assessment Method
Inouye SK, etal. Ann Intern Med;113:941-948
Acute Onset & Fluctuating Course
AND Inattention
+ either
Disorganized
Thinking Altered LOC
Delirium: Evaluation
• Caregiver interview: “Is Mrs. X more confused lately?”
• Confusion Assessment Method (CAM)
• Head to toe exam
• Medication, substance use Review (Tox screen)
• Infection (LP, Cultures, CXR)
• Metabolic (CMP, CBC, ABG, TSH, Folate, B12, RPR, HIV)
• Underlying Palliative Dx (MRI, CT, EEG, EKG, ECHO)
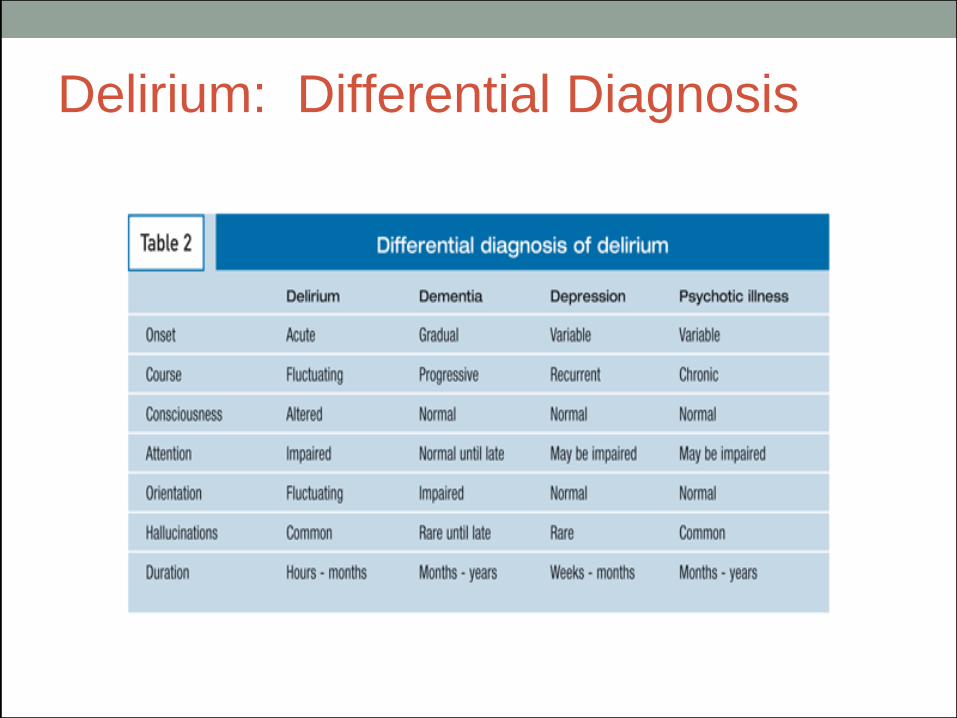
Delirium: Differential Diagnosis
Delirium: 1st Line Prevention
Management
• Frequent Reorientation
• Familiar setting, caregivers
• Oral Rehydration
• Attention to Lighting
• Sensory Aides
• Avoid Restraints/immobilization
• Daily Routine: Limit under/over stimulation
• Sleep Routine
Delirium: 1st Line Management
Treatment of underlying cause…
Multi-factorial, GOC directed
Medications Review
High risk: Steroids, Opioids, Anti-cholinergic, Antibiotics
Rotate opioids
Wean benzodiazepines and anticholinergics
Treat withdrawal, intoxication
Delirium: 1st Line Management
Supportive care:
Nutrition: assistance, supplements, PPN
Pain: schedule analgesics
Skin: oral and body hygiene, change position
Bowels: schedule softner, laxative
Delirium: 1st Line Management
Family/Caregiver Education
Reversible 50-80% cases, 1 week
Longer course severe illness
Representation of active dying
Non-pharmacolgic interventions
Role of medications to treat Agitation:
Neuroleptics, Sedatives
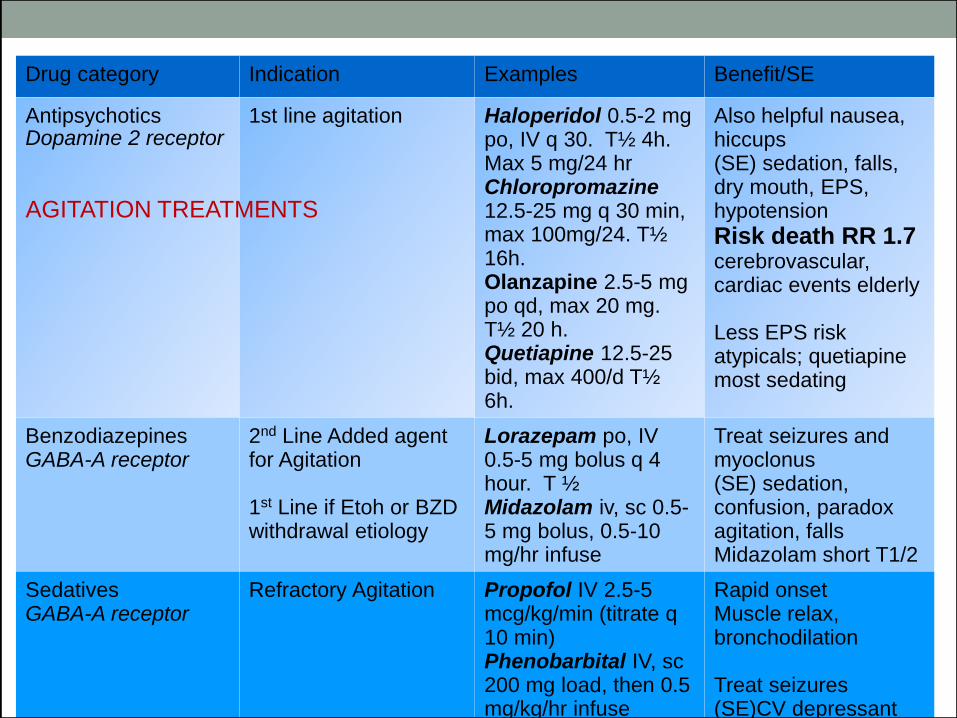
Drug category Indication Examples Benefit/SE
Antipsychotics Dopamine 2 receptor
1st line agitation
Haloperidol 0.5-2 mg po, IV q 30. T½ 4h. Max 5 mg/24 hr Chloropromazine 12.5-25 mg q 30 min, max 100mg/24. T½ 16h. Olanzapine 2.5-5 mg po qd, max 20 mg. T½ 20 h. Quetiapine 12.5-25 bid, max 400/d T½ 6h.
Also helpful nausea, hiccups (SE) sedation, falls, dry mouth, EPS, hypotension
Risk death RR 1.7 cerebrovascular, cardiac events elderly Less EPS risk atypicals; quetiapine most sedating
Benzodiazepines GABA-A receptor
2nd Line Added agent for Agitation 1st Line if Etoh or BZD withdrawal etiology
Lorazepam po, IV 0.5-5 mg bolus q 4 hour. T ½ Midazolam iv, sc 0.5-5 mg bolus, 0.5-10 mg/hr infuse
Treat seizures and myoclonus (SE) sedation, confusion, paradox agitation, falls Midazolam short T1/2
Sedatives GABA-A receptor
Refractory Agitation Propofol IV 2.5-5 mcg/kg/min (titrate q 10 min) Phenobarbital IV, sc 200 mg load, then 0.5 mg/kg/hr infuse
Rapid onset Muscle relax, bronchodilation Treat seizures (SE)CV depressant
AGITATION TREATMENTS
Delirium: Agitation Pharmacology
Anti-psychotics and Benzodiazepines can be doubled every 30 minutes until effective
Once stable add total amount needed for agitation control and give qd-tid (based T1/2)
Drug wean over 5-7 day period, after delirium stable
Death RR 1.7, AR 3.2 during use
Monitoring GOC based:
Anti-psychotic (QTc <450 at start, <25% increase), EPS symptoms, glucose, BMI
Psychosomatics. 1986; 27 (1 suppl): 33-38.
Delirium: Agitation Management
3rd line therapy: Propofol, Midazolam, Phenobarbital
Titration of the drug/(s) of choice to control Agitation
Goal of therapy NOT to hastening death.
Double Effect:
intent to relieve suffering (good), not hasten death (bad intent)
Delirium Overview
Drug Tx:
1st, 2nd, 3rd
Non-Drug
Tx
Treat Causes
Recognize
SLEEPLESSNESS
Sleeplessness: Insomnia Defined
Difficulty initiating sleep, maintaining sleep, or awakening
earlier than desired.
Lack of sleep occurs despite adequate opportunity and
sleep circumstances.
Lack of sleep causes deficits in daytime function.
International Classification of Sleep Disorders, 3rd Edition, American Academy of Sleep Medicine, 2014
Variants of Insomnia
• Short Term
Less than 3 months
Associated with Stressor
Common (Acute pain, hospitalization, grief)
Resolves with resolution of stressor or adaptation to stressor
Chronic
Sleeplessness >/=3 x weekly
Duration > 3 months
International Classification of Sleep Disorders, 3rd Edition, American Academy of Sleep Medicine, 2014
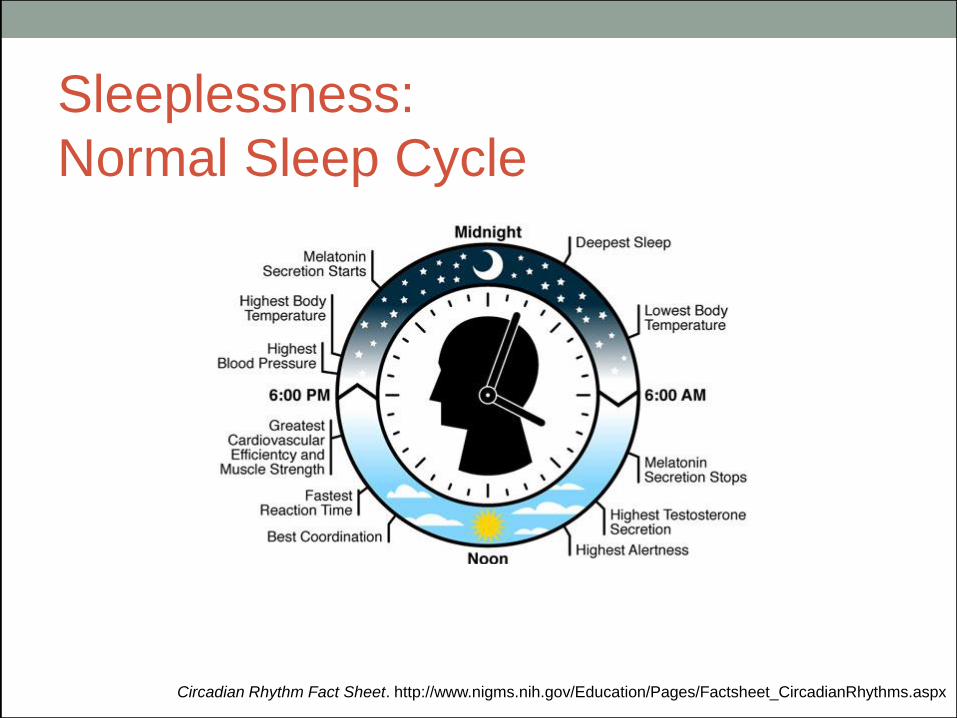
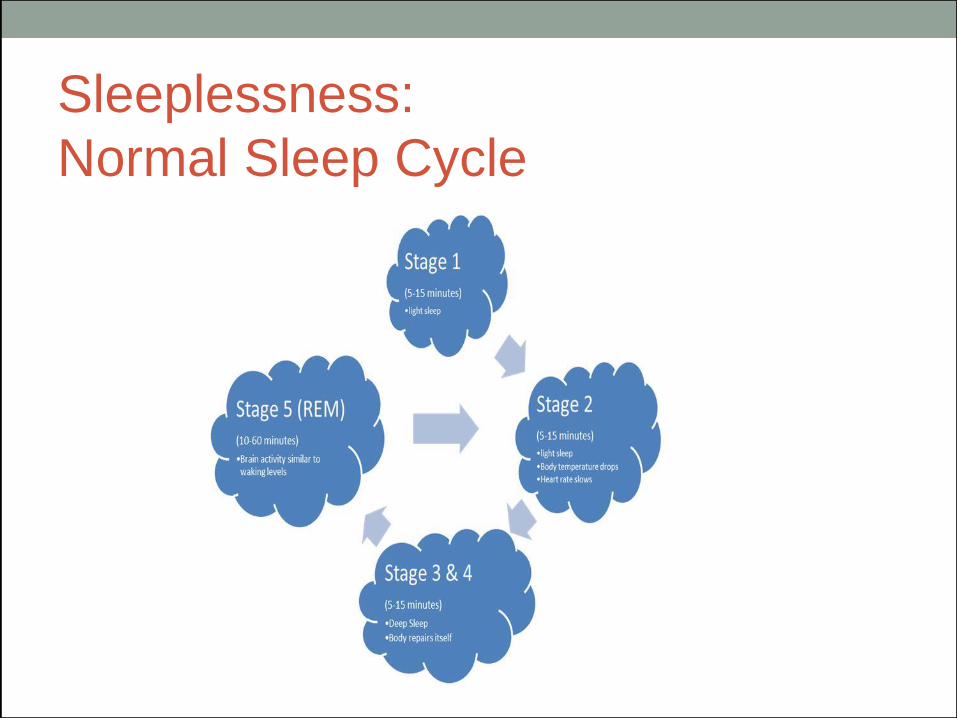
Sleeplessness:
Normal Sleep Cycle
Circadian Rhythm Fact Sheet. http://www.nigms.nih.gov/Education/Pages/Factsheet_CircadianRhythms.aspx
Sleeplessness:
Normal Sleep Cycle
S
Sleeplessness: Presentation
• Sleep Latency >30 minutes to sleep
• Early awakening >30 minutes prior to desired
• Variability of sleep thru the week
• Diminished tolerance to pain
• Increased fatigue
• Diminished Quality of Life
International Classification of Sleep Disorders, 3rd Edition, American Academy of Sleep Medicine, 2014
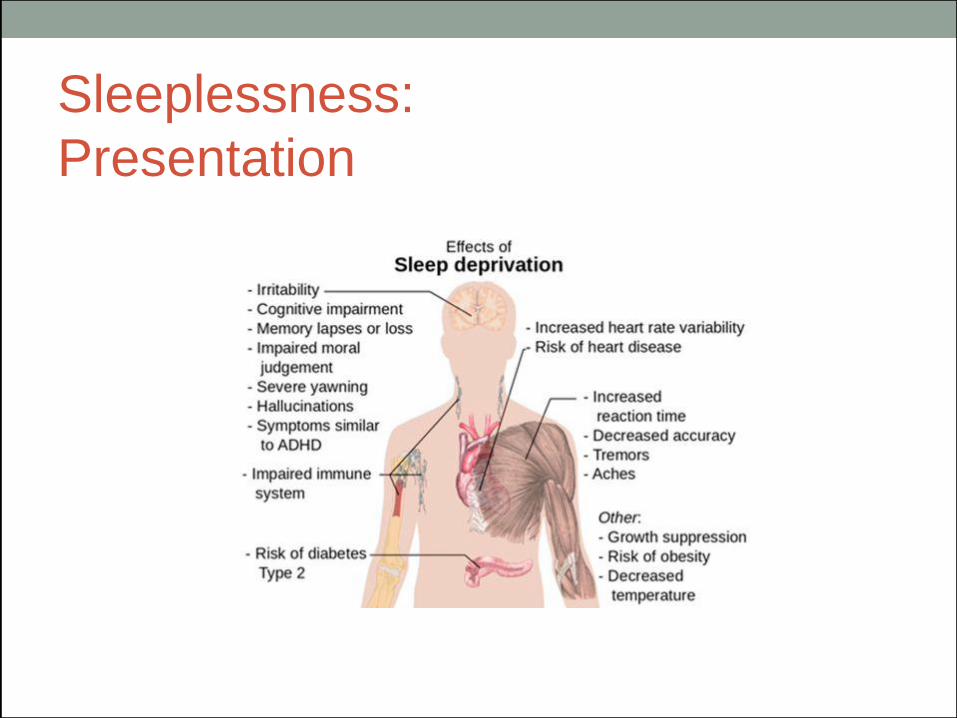
Sleeplessness:
Presentation
Sleeplessness: Epidemiology
30-75% Cancer patients experience insomnia
59% Surgery for malignancy
Survey primary care adults:
69% self reported insomnia
50% occasional
19% chronic
Savard, etal. 2011 Shochat, etal. Sleep 1999; 22 Suppl 2; S359.
Sleeplessness:
Etiology in Palliative Care
CO-MORBIDITY
SYMPTOMS
Untreated
Symptoms
Psychogenic
Spiritual Medication
Comorbidities
TERMINAL ILLNESS
Sleeplessness: Natural History
• 388 adults with insomnia
• 74%, Symptoms > 1 year
• 46%, Symptoms > 3 years
• Resolution insomnia in 54%
• 27% relapse within 5 years
Morin, etal. Arch Int Med 2009; 169: 447.
Sleeplessness: Evaluation
(Sleep History)
• Sleep chronology: Onset, pattern, duration of sleep
• Sleep Hygiene: Change of routine
• Sleep environment: Noise, temperature, odor disrupting
• Physical Symptoms: Cough, sob, pain, hot flashes
• Co-morbidities: CHF, OSA, Restless leg
• Meds: Steroids, Diuretics, ETOH, Caffeine, Stimulants
• Spiritual Concerns: Fears of dying
CAPC Fast Fact # 101: Insomnia Assessment
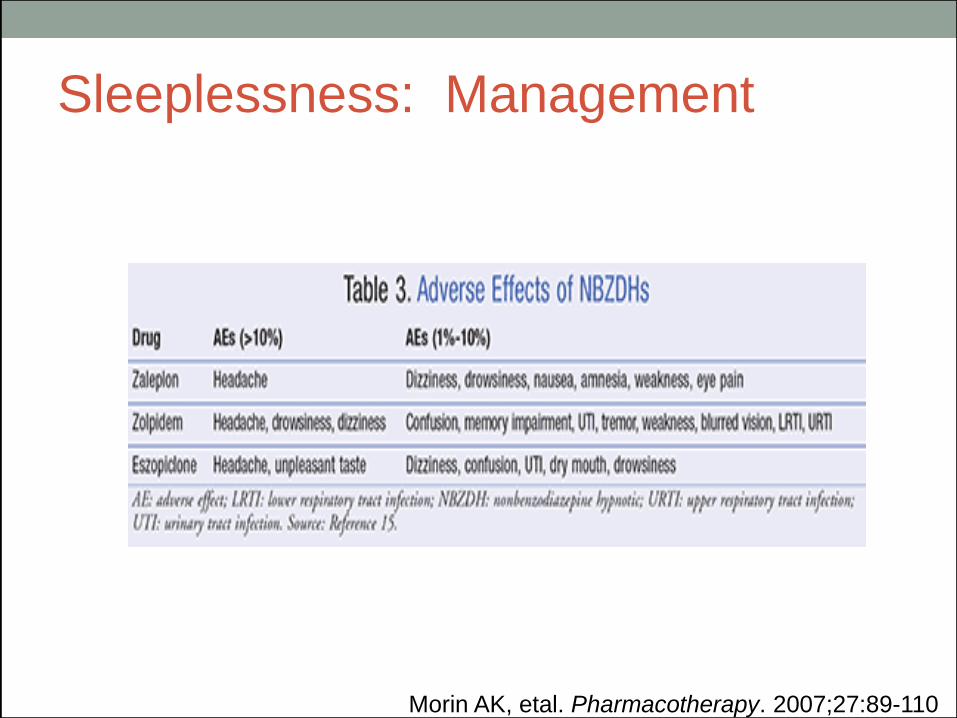
Sleeplessness: Management
(Sleep Hygiene) 1st Line
• Sleep to restful level
• Routine sleep schedule
• Avoid caffeine after lunch
• Avoid Etoh near bedtime
• Adjust bedroom environment
• Avoid light screens prior to bed
• Don't force sleep
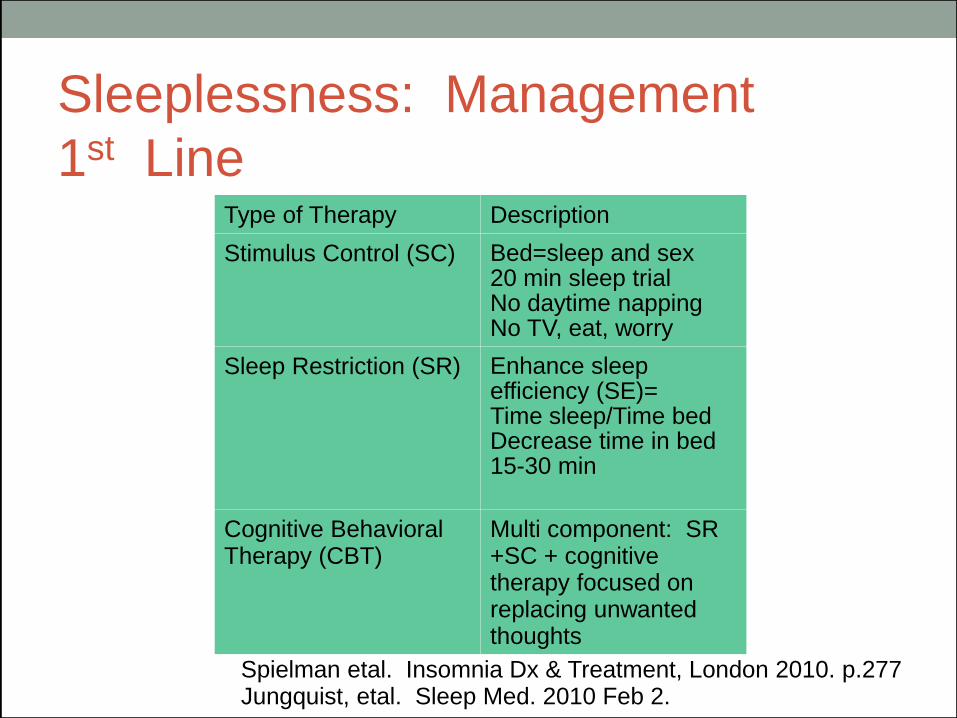
Sleeplessness: Management
1st Line Type of Therapy Description
Stimulus Control (SC) Bed=sleep and sex 20 min sleep trial No daytime napping No TV, eat, worry
Sleep Restriction (SR) Enhance sleep efficiency (SE)= Time sleep/Time bed Decrease time in bed 15-30 min
Cognitive Behavioral Therapy (CBT)
Multi component: SR +SC + cognitive therapy focused on replacing unwanted thoughts
Spielman etal. Insomnia Dx & Treatment, London 2010. p.277 Jungquist, etal. Sleep Med. 2010 Feb 2.
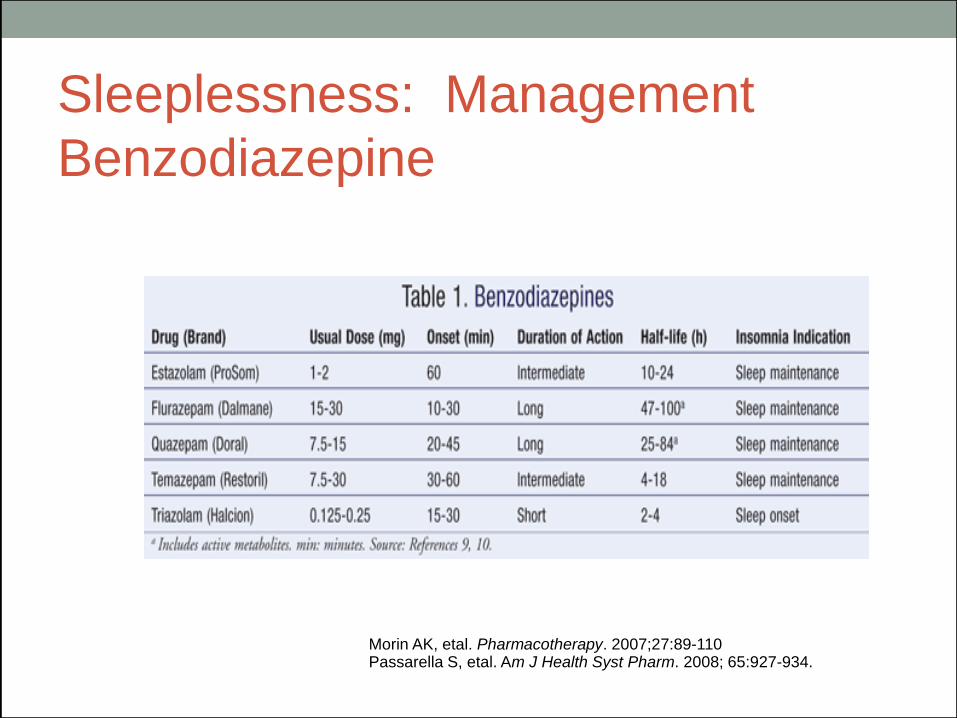
Sleeplessness: Management
Benzodiazepine
Morin AK, etal. Pharmacotherapy. 2007;27:89-110 Passarella S, etal. Am J Health Syst Pharm. 2008; 65:927-934.
Sleeplessness: Management
Benzodiazepine Side Effects:
Amnesia
Paradoxical agitation
Falls
Tolerance
Dependence with
prolonged use
Sleep Architecture:
Increase Sleep time
Decline Sleep latency
Increase Stage 2
Increase delay REM
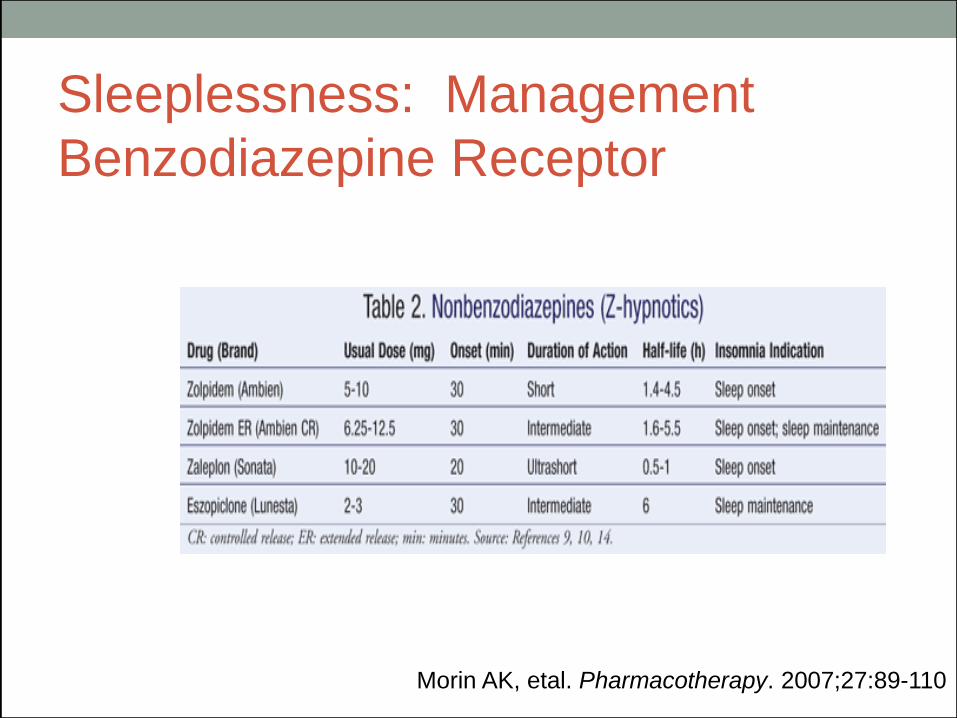
Sleeplessness: Management
Benzodiazepine Receptor
Morin AK, etal. Pharmacotherapy. 2007;27:89-110
Sleeplessness: Management
Morin AK, etal. Pharmacotherapy. 2007;27:89-110
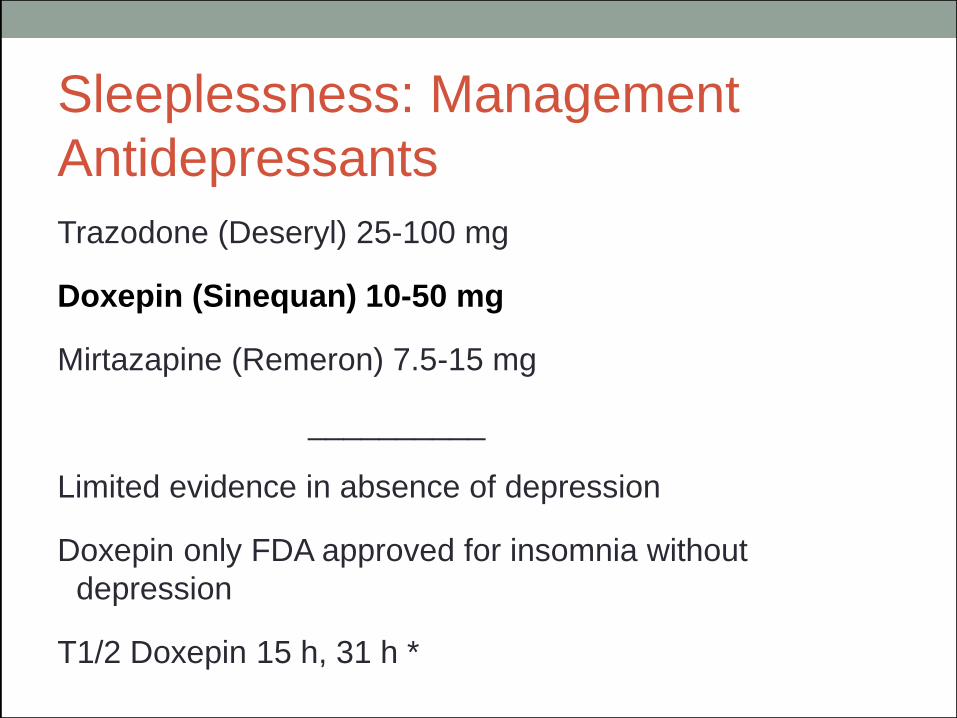
Sleeplessness: Management
Antidepressants
Trazodone (Deseryl) 25-100 mg
Doxepin (Sinequan) 10-50 mg
Mirtazapine (Remeron) 7.5-15 mg
__________
Limited evidence in absence of depression
Doxepin only FDA approved for insomnia without
depression
T1/2 Doxepin 15 h, 31 h *
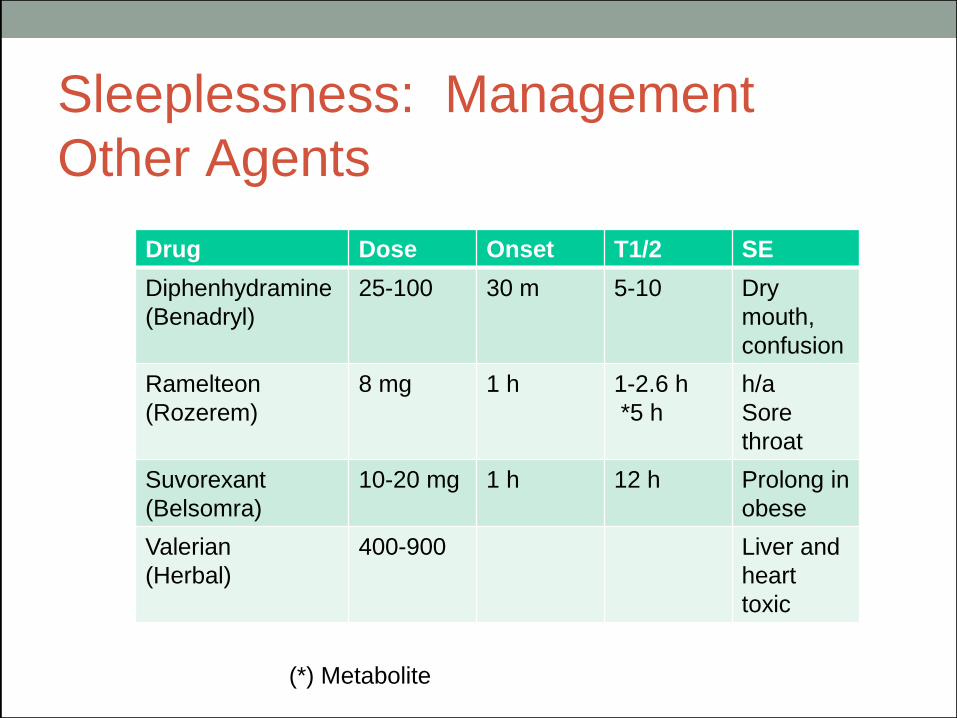
Sleeplessness: Management
Other Agents
Drug Dose Onset T1/2 SE
Diphenhydramine
(Benadryl)
25-100 30 m 5-10 Dry
mouth,
confusion
Ramelteon
(Rozerem)
8 mg 1 h 1-2.6 h
*5 h
h/a
Sore
throat
Suvorexant
(Belsomra)
10-20 mg 1 h 12 h Prolong in
obese
Valerian
(Herbal)
400-900 Liver and
heart
toxic
(*) Metabolite
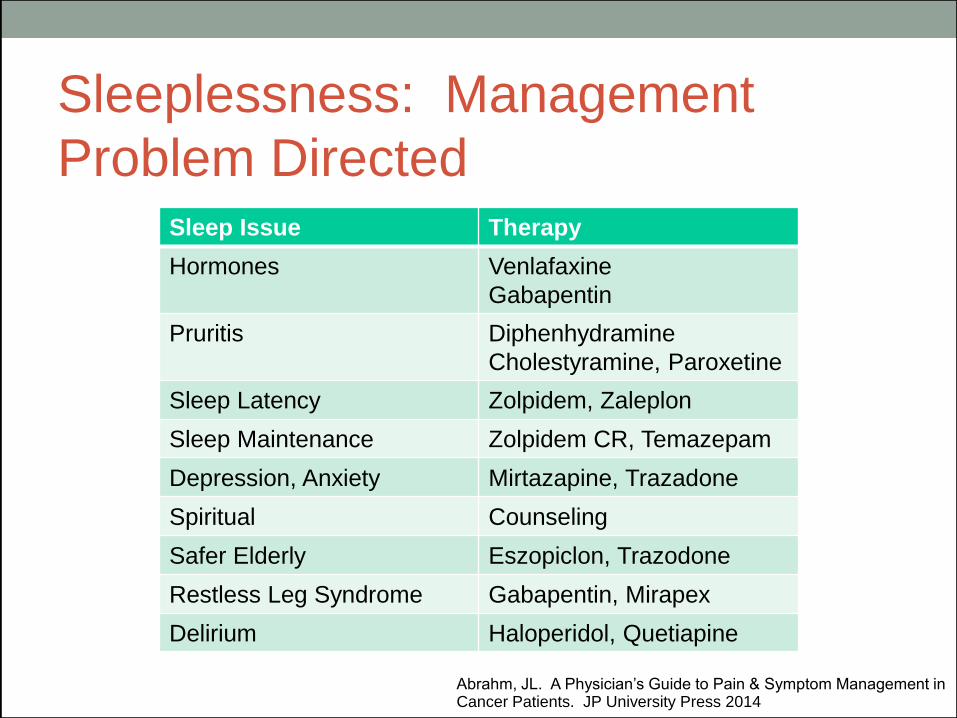
Sleeplessness: Management
Problem Directed
Sleep Issue Therapy
Hormones Venlafaxine
Gabapentin
Pruritis Diphenhydramine
Cholestyramine, Paroxetine
Sleep Latency Zolpidem, Zaleplon
Sleep Maintenance Zolpidem CR, Temazepam
Depression, Anxiety Mirtazapine, Trazadone
Spiritual Counseling
Safer Elderly Eszopiclon, Trazodone
Restless Leg Syndrome Gabapentin, Mirapex
Delirium Haloperidol, Quetiapine
Abrahm, JL. A Physician’s Guide to Pain & Symptom Management in Cancer Patients. JP University Press 2014
Challenging Symptoms:
Treatable
• Establish Disease and Prognosis
• Establish Goals of Care (GOC)
• Assess for symptoms regularly
• Weigh risk: benefit of evaluation and treatment
of symptom
Challenging Symptoms:
Treatable
• Identify symptom cause
• Treat symptom with intent-> Alleviate suffering
• Reassess frequently for symptom control
• Educate family on management and future
needs
J Pall Med 06:9 (2): 391-408 J Pall Med 06:9(2):391-408
…and our life is rounded with a sleep… -William Shakespeare The Tempest, Act IV, Scene 1







![Research Article Delirium during Weaning from Mechanical ... · delirium symptoms, including agitation and combativeness with risk of catheter withdrawal and autoextubation[ ]. It](https://img.pdfslide.net/doc/110x75/60e3043dce5e5d6cd31f3ebb/research-article-delirium-during-weaning-from-mechanical-delirium-symptoms.jpg)