Embed Size (px)
DESCRIPTION
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master’s Programmes at the University of Pécs and at the University of Debrecen Identification number: TÁMOP-4.1.2-08/1/A-2009-0011. - PowerPoint PPT Presentation
Citation preview

Manifestation of Novel Social Challenges of the European Unionin the Teaching Material ofMedical Biotechnology Master’s Programmesat the University of Pécs and at the University of DebrecenIdentification number: TÁMOP-4.1.2-08/1/A-2009-0011

CHANGES OF RENAL FUNCTIONSIN THE ELDERLY
Miklós Székely and Erika PéterváriMolecular and Clinical Basics of Gerontology – Lecture 11
Manifestation of Novel Social Challenges of the European Unionin the Teaching Material ofMedical Biotechnology Master’s Programmesat the University of Pécs and at the University of DebrecenIdentification number: TÁMOP-4.1.2-08/1/A-2009-0011

TÁMOP-4.1.2-08/1/A-2009-0011
With aging:• Renal mass decreases• Renal blood flow (RBF) decreases• Number of functioning nephrons decreases• GFR decreases, glomerular dysfunctions• Tubular dysfunctions• Excretory capacity decreases• Role in salt/water regulation decreases• Role in pH regulation decreases• Non-excretory renal functions decrease
AGING vs. RENAL FUNCTIONS

TÁMOP-4.1.2-08/1/A-2009-0011
Macula densa
Red blood cells
Podocyte (visceral layer)
Mesangial cell
Basement membrane
Parietal layer ofBowman’s capsule
Afferent arterioleEfferent arteriole
Distal renal tubule
Glomerular structures

TÁMOP-4.1.2-08/1/A-2009-0011
Glomerular structures
Red bloodcell
Podocytes(visceral layer)
Mesangial cell
Basement membrane
Capillary

TÁMOP-4.1.2-08/1/A-2009-0011
Glomerular structures:filter surface
Podocyte(epithelial cell
with foot processes)
Mesangialcell
Red blood cell
Endothelialcell
Capillary lumen
Foot processes
Basement membrane
Red blood cell
Capillary lumen
Bowman’s space
Fenestrations

TÁMOP-4.1.2-08/1/A-2009-0011
filtration of polyanions accumulation of circulating
aggregates in mesangiumfusion of podocyte
foot processes
proteinuria mesangial matrixproduction and
proliferation
focal sclerosis
Anionic charge of glomerular capillaries
Development ofglomerulosclerosis 1

TÁMOP-4.1.2-08/1/A-2009-0011
Glomerular sclerosis
Glomerular sclerosis

TÁMOP-4.1.2-08/1/A-2009-0011
Chronic loss ofrenal tissueProtein intake Diabetes mellitus
hyperglycemia
Hypertrophy and vasodila-tion in remaining nephrons
Glomerular pressure
Altered permselectivity
Arterial pressure
Glomerular hyperfiltration
Direct cellular injury
Cell proliferation and platelet aggregation
Mesangial matrix overproduction
Glomerular sclerosis
Increased protein filtration
Compensatory polyuria
Albuminuria Mesangial cell damage
Development ofglomerulosclerosis 2

TÁMOP-4.1.2-08/1/A-2009-0011Pe
rcen
t of t
otal
nep
hron
s
SNGFR (nl/min)
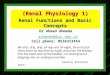
0
10
20
30
0 0 10 20 30 40 50 60 70 80
(37.5)
GFR100%
0
10
20
30
0 0 10 20 30 40 50 60 70 80
(20)
GFR~50%
0
10
20
30
0 0 10 20 30 40 50 60 70 80
(37.5)
40
GFR100%
Aging influences single-nephron-GFR (SNGFR)

TÁMOP-4.1.2-08/1/A-2009-0011
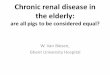
GFR
(ml/m
in)
Years
40
20
60
80
100
120
140
30 40 50 60 70 80
Age vs. GFR

TÁMOP-4.1.2-08/1/A-2009-0011
• In th elderly GFR, tendency for azotemia due to a fall of kidney perfusion (thirst, heat, CO redistribution e.g. heart failure), but no proportional rise in se-creatinine (less muscle lost)
• Tubular reabsorption changes: glucose reabsorbing tubular cells still function, minerals: tendency for K-loss, salt wasting (Na-reabsorption), phosphaturia, poor ADH action (water loss).
• Proteinuria more frequent.• Excretory capacity (drugs!) decreases.• Severe shifts in the osmotic pressure.
Age vs. nephron dysfunctions

TÁMOP-4.1.2-08/1/A-2009-0011
ADH effect decreases with age U/
P in
ulin
(urin
e/pl
asm
a co
nc.
ratio
)
Urine Collection Period0
0
102030405060708090
100110120
1 2 3 4 5 6 7 8 9 10
YoungMiddleOld
ADH

TÁMOP-4.1.2-08/1/A-2009-0011
80
300
400
600
1,000
1,500
Osmoticpressure
Proximal tubuleDistal tubule
Corticomedullary osmotic concentration gradient

TÁMOP-4.1.2-08/1/A-2009-0011
No ADH16 ml
1500
1200
900
600
300
0
Osm
olal
ity (m
Osm
/kg)
100 ml
20 ml
20 ml
2.0 ml
0.3 ml
Lot of ADH
Prox. tub. Loop of Henle Dist. tub +Cort.
collecting duct
Medullary collecting
duct
Concentrating and diluting the urine
NormalHyposthenuria
20 ml
Fluid volume along the nephron

TÁMOP-4.1.2-08/1/A-2009-0011
Spec
ific
grav
ity o
f urin
e
Number of nephrons
1,0002,000,000 1,500,000 1,000,000 500,000 0
1,010
1,020
1,030
1,040
Hyposthenuria
Development of hyposthenuria
Isosthenuria
Specific gravity of plasma

TÁMOP-4.1.2-08/1/A-2009-0011
• Impaired excretion of substances that are excreted through the kidneys the dose of drugs that are eliminated through the kidney has to be decreased!
• Kidney perfusion decreases frequently for a number of reasons, e.g. redistribution in heart failures, exsiccosis – impaired excretory functions – drug doses have to be adjusted.
Kidney and drugs

TÁMOP-4.1.2-08/1/A-2009-0011
• Atrophy of renal parenchyma + sclerotic a. renalis regulation of blood pressure defective, tendency for hypertension, but hypovolemia may cause hypotension.
• Erythropoietin deficiency due to reduced renal parenchyma and gonadal hormon secretion anemia.
• Active D-vitamin formation decreases bone abnormalities (senile osteoporosis).
Aging vs. non-excretory kidney functions

TÁMOP-4.1.2-08/1/A-2009-0011Most common renal diseases and genitourinary conditions in the elderly• Diabetic nephropathy• Glomerulonephritis• Pyelonephritis• Interstitial
nephropathy - analgesic nephropathy- uric acid nephropathy- myeloma kidney
• Urinary retention(The muscles of the bladder and pelvic floor weaken.)
• Urinary incontinence(The capacity of the urinary bladder reduces which leads to frequent urination.)
• Urinary infections • Benign prostatic
hyperplasia, prostate cancer
• Atrophic vaginitis

TÁMOP-4.1.2-08/1/A-2009-0011
Renal failure in the elderly:causesThe incidence of acute renal failure increases following acute tubular necrosis.Risk factors: • age-related decrease
of RBF, GFR, and of ability to concentrate or to dilute urine,
• diabetes mellitus, • hepatic cirrhosis,• congestive heart
failure,
• drugsChronic ischemic renal disease and progressive damage of the renal parenchyma lead to chronic renal failure.Risk factors:• diabetes mellitus• hypertension• hyperlipidemia• obesity

TÁMOP-4.1.2-08/1/A-2009-0011Renal failure in the elderly:dialysis and kidney transplantationThe most common indication of dialysis due to chronic renal failure is diabetic nephropathy (35-40%). There is an increase in the number of renovascular diseases. Among the dialyzed there are less candidates for transplantation due to co-morbidity. The overall survival increases due to the improved efficacy of dialysis. With higher capacity of dialysis, the age-related limits of dialysis have faded away.Age is not a contraindication of kidney transplantation. Both the cadaveric and the living donor can be an option in the elderly. The only limiting factor for kidney transplantation is the presence of multimorbidity (hypertension, DM, significant atherosclerosis).

TÁMOP-4.1.2-08/1/A-2009-0011
Urinary tract infection
Symptoms: fever, dysuria (pain upon urination), urgency, frequency, incontinence, impaired physical and/or mental status. Sepsis can develop quickly and atypically — treatment of urosepsis is extremely difficult. Pathogens: E. Coli, Enterococci, Streptococci, Proteus.Treatment: oral rehydration, frequent urination, selected antibiotics, roboration.

TÁMOP-4.1.2-08/1/A-2009-0011
Incontinence
Definition: Involuntary loss of urine through the urethra.Types: • functional, • stress, • urge, reflex, • overflow.

TÁMOP-4.1.2-08/1/A-2009-0011
Functional incontinence
The patient is not able to control his bladder due to altered circumstances. Causes: • disability, • impaired vision, • dementia, • bigger amount of urine (i.e. diuretics, diabetes
mellitus)Management: • changes in the environment, • timed voiding (scheduled bathroom visits), • urinary indwelling catheter as required,• diapers.

TÁMOP-4.1.2-08/1/A-2009-0011
Stress incontinence Involuntary loss of urine upon elevated intra-abdominal pressure.Causes:• urethral sphincter insufficiency due to weakness of
pelvic floor musculature,• obesity,• prolapsed uterus, atrophic vaginitis, bladder hernia.Management:• weight loss,• Kegel exercises, electro-stimulation,• estrogen, medication (Ditropan, Melipramin), • surgery,• panty liners.

TÁMOP-4.1.2-08/1/A-2009-0011
Urge/reflex incontinence Sudden, unexpected urge to void after certain
stimuli.Causes:• atrophic vaginitis, cystitis,• benign prostatic hyperplasia (BPH),• certain drugs or foods, cold.Management:• casual treatment,• avoiding coffee/tea/alcohol,• estrogen, medication (Ditropan),• electro-stimulation, behavioral training (biofeedback).

TÁMOP-4.1.2-08/1/A-2009-0011
Overflow incontinence Unexpected urine loss from the overfilled
bladder.Causes:• benign prostatic hyperplasia (BPH),• fibrotic stenosis of the urethra,• muscles of the bladder and pelvic floor weak.Management:• casual treatment,• avoiding coffee/tea/alcohol,• estrogen, medication (Ditropan),• behavioral training (biofeedback).