Embed Size (px)
Citation preview

27-1
Chapter 27
Water, Electrolytes, and
Acid-Base Balance

27-2
27.1 Body Fluids
• Intracellular fluid compartment– All fluids inside cells of body– About 40% of total body weight
• Extracellular fluid compartment– All fluids outside cells– About 20% of total body weight– Subcompartments
• Interstitial fluid and plasma; lymph, CSF, synovial fluid• Primary intracellular ions, interstitial fluid ions, and plasma ions
– Intracellular cation = K+
– Interstitial fluid cation = Na+
– Plasma cation = Na+
– Intracellular anion = Phosphate– Interstitial fluid = Cl-
– Plasma anion = Cl-

27-3
Body Fluid Compartments
Approximate Concentration of major Solutes in Body Fluids*
Intracellular Fluid†
Phosphate (HPO42− plus HPO4
−)
*Expressed as milliequivalents per liter (meq/l).†Data are from skeletal muscle.
Interstitial FluidPlasma
TABLE 27.2
SoluteCations
Sodium (Na+)
Potassium (K+)
Calcium (Ca2+)
Magnesium (Mg2+)
TOTAL
Anions
Chloride (Cl–)
Bicarbonate (HCO3–)
Protein
Other
TOTAL
153.2
4.3
3.8
1.4
145.1
4.1
3.4
1.3
12.0
150.0
4.0
34.0
153.9
118.0
27.0
2.3
0.0
6.6
153.9 200.0
90.0
54.0
40.0
12.0
4.0
200.0
162.7
6.3
17.0
2.2
25.7
111.5
162.7
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

27-4
27.2 Regulation of Body Fluid Concentration and Volume
• Content regulated so total volume of water in body remains constant
• Kidneys are primary regulators of water excretion
• Regulation processes– Osmosis– Osmolality– Baroreceptors– Learned behavior
• Sources of water– Ingestion
– Cellular metabolism
• Routes of water loss– Urine
– Evaporation• Perspiration
• Respiratory passages
– Feces

27-5
Extracellular Fluid Osmolality• Osmolality
– Measure of water vs. solute concentration; the higher the solute concentration, the higher the osmolality
– Adding or removing water from a solution changes osmolality
• Increased osmolality: triggers thirst and ADH secretion
• Decreased osmolality: inhibits thirst and ADH secretion

27-6
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
3
1 Baroreceptorsin heart
2 Juxtaglomerularapparatuses in kidney
1 The baroreceptors in the carotid sinuses and aortic arch detect reduced bloodpressure, which signals the hypothalamic thirst center.
2 Simultaneously, the juxtaglomerular apparatuses detect low blood pressure, whichactivates the renin-angiotensin system to produce angiotensin II. Angiotensin IIstimulates the hypothalamic thirst center.
3 Osmoreceptors in the hypothalamus shrink when blood osmolality goes up,triggering action potentials that stimulate thirst.
4 The combination of these inputs activates thirst and promotes water consumption.
Osmoreceptors inhypothalamus(increased osmolality)
4 Increasedthirst

27-7
Hormonal Regulation of Blood OsmolalityCopyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
ReactionsActions
Actions Reactions
Osmoreceptors in the hypothalamuscontrol center detect the increase in blood osmolality and signal the posteriorpituitary to secrete ADH, whichcauses thirst. ADH also increases thepermeability of the distal convolutedtubule and collecting ducts to water.
Water reabsorption at the distalconvoluted tubule and collectingduct increases; water consumptionincreases .
Blood osmolality increases:Homeostasis Disturbed
Blood osmolality decreases:Homeostasis Restored
Blo
od
osm
ola
lity
(no
rma
l ran
ge)
Blo
od
osm
ola
lity
(no
rma
l ran
ge)
Blood osmolality decreases:Homeostasis Disturbed
Blood osmolality increases:Homeostasis Restored
Osmoreceptors in the hypothalamusdetect the decrease in bloodosmolality and signal the posteriorpituitary to reduce ADH secretion,which decreases thirst.
Water reabsorption at the distalconvoluted tubule and collectingduct decreases; waterconsumption decreases.
Start here
3 4
Control Center
Effectors Activated:
Control CenterEffectors Activated:
2
1
5
6

27-8
Regulation of ECF Volume• ECF can increase or decrease even if osmolality of
extracellular fluid is maintained• Carotid sinus and aortic arch baroreceptors monitor blood
pressure, juxtaglomerular apparatuses monitor pressure changes, receptors in walls of atria and large vessels respond to small changes in BP
• These receptors activate these mechanisms– Neural: increase in BP recognized by baroreceptors. Decreased
sympathetic stimulation of afferent arteriole leads to increased pressure in glomerulus leading to increased filtration and increased urine output.
– Renin-angiotensin-aldosterone– Atrial natriuretic hormone (ANH)– Antidiuretic hormone (ADH)

27-9
Regulation of Blood VolumeCopyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
Actions
Actions
Pituitary:Baroreceptors stimulate posterior pituitary ADH secretionwhen blood volume decreases. Increased ADH alsoincreases the sensation of thirst.
Increased aldosterone and decreased ANH increase
Na+ reabsorption in the distal convoluted tubule and thecollecting duct. Less Na+ and water are excreted in theurine.
Increased ADH increases the permeability of the distal convoluted tubule and the collecting duct to water. Less water is excreted in urine.
Decreased renal blood flow decreases filtrate formation,and less water is excreted in urine.
Decreased aldosterone and increased ANH decrease
Na+ reabsorption into the distal convoluted tubule andcollecting duct. More Na+ in urine, which decreases blood volume
Decreased ADH decreases water reabsorption by thedistal convoluted tubules and collecting ducts. Lesswater returns to the blood, and more water is excreted in the urine.
Blood vessels:Sympathetic division baroreceptors detect increased bloodvolume, which causes vasodilation of renal arteries.
Heart:Atrial cardiac muscle cells secrete ANH when bloodvolume increases.
Kidney:Juxtaglomerular apparatuses inhibit renin release whenblood volume increases, which decreasesaldoster one secretion.
Pituitary:Baroreceptors inhibit posterior pituitary ADH secretionwhen blood volume increases.
Effectors Activated:
Increased renal blood flow increases the rate of filtrateformation, and more water is excreted in the urine.
High blood volume induces elevated bloodpressure: Homeostasis Disturbed
Start here
Blo
od
vo
lum
e(n
orm
al r
ang
e)
Blo
od
vo
lum
e(n
orm
al r
ang
e)
Low blood volume induces lowered bloodpressure: Homeostasis Disturbed
Reduced blood volume due to loss of water
and Na+ in the urine lowers blood pressure:Homeostasis Restored
Increased blood volume due to decreased Na+ and water loss in the urine raises blood pressure:
Homeostasis Restored
Blood vessels:Sympathetic division baroreceptors detect decreasedblood volume, which causes vasoconstriction of renalarteries.
Heart:Atrial cardiac muscle cells do not secrete ANH whenblood volume decreases.
Kidney:Juxtaglomerular apparatuses stimulate renin releasewhen blood volume decreases, which increasesaldosterone secretion.
Reactions
Reactions
Effectors Activated:
3 4
2
1
5
6

27-10
Regulation of ECF VolumeCopyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
DecreasedBP
Kidney
Increased Na+
and waterreabsorptionresults inincreased BP.
Increasedrenin secretion(from kidney)
Angiotensinogen
Angiotensin I
Angiotensin II
Increasedaldosterone secretion
Increased BPin right atrium
ANH
Kidney
Increased ANH Increased Na+
excretion andincreased waterloss result indecreased BP.

27-11
Regulation of ECF Osmolality
• Electrolytes– Molecules or ions with an
electrical charge• Ingestion adds electrolytes to
body• Kidneys, liver, skin, lungs
remove from body– Concentration changes only
when growing, gaining or losing weight
• Na+ Ions– Dominant ECF cations– Responsible for 90-95% of
osmotic pressure
• Regulation of Na+ ions– Kidneys major route of
excretion– Small quantities lost in sweat
{sweat = (in decreasing amounts) water, Na+, urea, Cl-
K+, NH3}. Insensible perspiration is water evaporating from skin. Sensible perspiration is secreted by the sweat glands. Contains solutes
• Terms– Hypernatremia: elevated
plasma Na+ – Hyponatremia: decreased
Na+
27-12
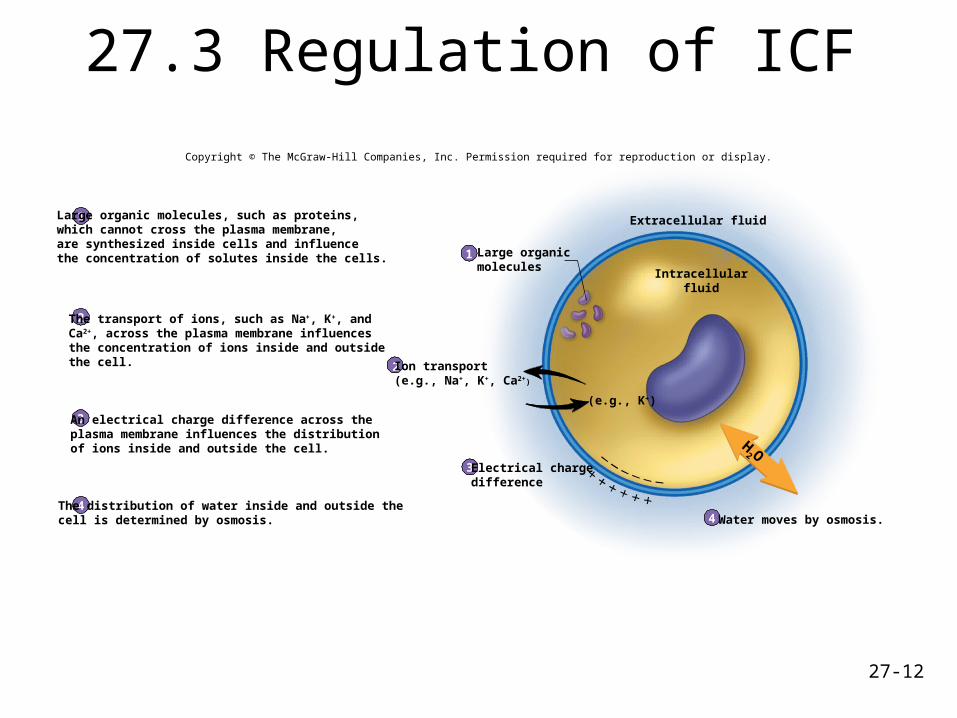
27.3 Regulation of ICF
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
1
2
3
4
1
2
3
4
Large organic molecules, such as proteins,which cannot cross the plasma membrane,are synthesized inside cells and influencethe concentration of solutes inside the cells.
The transport of ions, such as Na+, K+, andCa2+, across the plasma membrane influencesthe concentration of ions inside and outsidethe cell.
An electrical charge difference across theplasma membrane influences the distributionof ions inside and outside the cell.
The distribution of water inside and outside thecell is determined by osmosis.
Large organicmolecules
Extracellular fluid
Intracellularfluid
Water moves by osmosis.
Electrical chargedifference
Ion transport(e.g., Na+, K+, Ca2+)
H2 O
(e.g., K+)

27-13
27.4 Regulation of Specific Electrolytes
• Chloride ions– Predominant anions in ECF
• Magnesium ions– Capacity of kidney to
reabsorb is limited
– Excess lost in urine
– Decreased extracellular magnesium results in greater degree of reabsorption
• Potassium ions– Maintained in narrow range
– Affect resting membrane potentials
– Aldosterone increases amount secreted
• Terms– Hyperkalemia: abnormally
high levels of potassium in extracellular fluid
– Hypokalemia: abnormally low levels of potassium in extracellular fluid.

27-14
Table 27.5 Homeostasis: Mechanisms Regulating Blood Sodium
Response to Changes in Blood Osmolality
Antidiuretic hormone(ADH); the mostimportant regulatorof blood osmolality
Increased bloodosmolality (e.g.,increased Na+
concentration)
Increased ADH secretionfrom the posterior pituitary;mediated through cells inthe hypothalamus
Increased water reabsorptionin the kidney; productionof a small volume ofconcentrated urine
Decreased blood osmolalityas reabsorbed water dilutesthe blood
Decreased bloodosmolality (e.g.,decreased Na+
concentration)
Decreased ADH secretionfrom the posterior pituitary;mediated through cells inthe hypothalamus
Decreased water reabsorptionin the kidney; production of alarge volume of dilute urine
Increased blood osmolalityas water is excreted fromthe blood into the urine
Response to Changes in Blood Pressure
Renin-angiotensinaldosteronehormonemechanism
Decreased bloodpressure in the kidney’safferent arterioles
Increased renin releasefrom the juxtaglomerularapparatuses; renininitiates the conversionof angiotensinogen toangiotensin; angiotensin Iis converted toangiotensin II, which increasesaldosterone secretion fromthe adrenal cortex
Increased Na+ reabsorptionin the kidney (because ofincreased aldosterone);increased water reabsorptionas water follows the Na+;decreased urine volume
Increased blood pressureas blood volume increasesbecause of increased waterreabsorption; bloodosmolality is maintainedbecause both Na+ andwater are reabsorbed*
Increased bloodpressure in the kidney’safferent arterioles
Decreased renin releasefrom the juxtaglomerularapparatuses, resulting inreduced formation ofangiotensin I; reducedangiotensin I leads toreduced angiotensin II,which causes a decreasein aldosterone secretionfrom the adrenal cortex
Decreased Na+ reabsorptionin the kidney (because ofdecreased aldosterone);decreased water reabsorptionas less Na+ is reabsorbed;increased urine volume
Decreased blood pressureas blood volume decreasesbecause water is excreted inthe urine; blood osmolalityis maintained because bothNa+ and water are excretedin the urine*
Atrial natriuretichormone (ANH)
Decreased bloodpressure in theatria of the heart
Decreased ANH releasedfrom the atria
Increased Na+ reabsorptionin the kidney; increasedwater reabsorption as waterfollows the Na+; decreasedurinary volume
Increased blood pressureas blood volume increasesbecause of increased waterreabsorption; bloodosmolality is maintainedbecause both Na+ andwater are reabsorbed*
Increased bloodpressure in theatria of the heart
Increased ANH releasedfrom the atria
Decreased Na+ reabsorptionin the kidney; decreasedwater reabsorption aswater is excreted with Na+
in the urine; increasedurinary volume
Decreased blood osmolalityas blood volume decreasesbecause water is excreted inthe urine; blood osmolalityis maintained because bothNa+ and water are excretedin the urine*
ADH—activated bysignificant decreasesin blood pressure;normally regulates bloodosmolality (see above)
Decreased arterialblood pressure
Increased ADH secretionfrom the posteriorpituitary; mediatedthrough baroreceptors
Increased water reabsorptionin the kidney; productionof a small volume ofconcentrated urine
Increased blood pressureresulting from increasedblood volume; decreasedblood osmolality
Increased arterialblood pressure
Decreased ADH secretionfrom the posteriorpituitary; mediatedthrough baroreceptors
Decreased water reabsorptionin the kidney; production of alarge volume of dilute urine
Decreased blood pressureresulting from decreasedblood volume; increasedblood osmolality
Abbreviation: A DH = antidiuretic hormone.*Assumes normal levels of A DH.
Mechanism Stimulus Response to Stimulus Effect of Response Result
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

27-15
Consequences of AbnormalPlasma Levels of Sodium Ions
Lethargy, confusion, apprehension, seizures, and coma
When accompanied by reduced blood volume:reduced blood pressure, tachycardia, and decreasedurine output
When accompanied by increased blood volume:weight gain, edema, and distension of veins
High dietary sodium (rarely causes symptoms)
Administration of hypertonic saline solutions
Oversecretion of aldosterone
Thirst, fever, dry mucous membranes, and restlessness
Most serious symptoms are convulsions andpulmonary edema
When occurring with increased water volume:weight gain, edema, elevated blood pressure,and bounding pulse
TABLE 27.6
Causes Inadequatedietary intake of sodium
Extrarenal losses
Dilution
Hyperglycemia
Symptoms
HYPERNATREMIA
Causes
Symptoms
Water loss
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
HYPONATREMIA

27-16
Potassium Ion Regulation in ECFCopyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
Blood K+ levels increase:Homeostasis Disturbed
Blood K+ levels decrease:Homeostasis Disturbed
Blood K+ levels decrease:Homeostasis Restored
Blood K+ levels increase:Homeostasis Restored
Decreased blood levels of K+ acton the adrenal cortex to decreasealdosterone secretion
Decreased aldosterone reduces the
rate of K+ secretion from the distalconvoluted tubules and collectingducts of the kidneys into the urine.
Increased blood levels of K+ acton the adrenal cortex to increasealdosterone secretion.
Elevated aldosterone increases the
rate of K+ secretion from the distalconvoluted tubules and collectingducts of the kidney into the urine.
ReactionsActions
ReactionsActions
Start here
Blo
od
k+
(no
rmal
ran
ge)
Blo
od
k+
(no
rmal
ran
ge)
Control Center Effectors Activated:
3 4
2
1
5
6
Control Center Effectors Activated:

27-17
Consequences of AbnormalConcentrations of Potassium Ions
Loss of intracellular K+ due to cell trauma orreduced permeability of plasma membrane
Reduced renal excretion
Increased neuromuscular irritability
Intestinal cramping and diarrhea
Rapid cardiac repolarization
Loss of muscle tone and paralysis
Reduced rate of cardiac action potential conduction
TABLE 27.7
HYPOKALEMIA
Causes
Symptoms
Causes
Symptoms
Mild
Severe Muscle weakness
HYPERKALEMIA
Atrioventricular block
Delayed ventricular depolarization
Bradycardia
Decreased smooth muscle tone
Decreased neuromuscular excitability
Increased renalloss
Reduced K– intake
Alkalosis
Insulin administration
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
27-18
Regulation of Calcium Ions
• Regulated within narrow range– Elevated extracellular
levels prevent membrane depolarization
– Decreased levels lead to spontaneous action potential generation
• Terms– Hypocalcemia– Hypercalcemia
• PTH increases Ca2+ extracellular levels and decreases extracellular phosphate levels
• Vitamin D stimulates Ca2+ uptake in intestines
• Calcitonin decreases extracellular Ca2+ levels

27-19
Consequences of AbnormalConcentrations of Calcium Ions
Nutritional deficiencies
Vitamin D deficiency
Decreased parathyroid hormone secretion
Malabsorption of fats (reduces vitamin D absorption)
Bone tumors that increase Ca2+ deposition
Reduced cardiac ventricular depolarization
TABLE 27.8
HYPOCALCEMIA
Causes
Symptoms Confusion
Muscles pasmsa
Hyperreflexi
Intestinal cramping
Convulsions
Tetany
Inadequate respiratory movements
Prolonged cardiac ventricular depolarization
HYPERCALCEMIA
Excessive parathyroid hormone secretion
Excess vitamin D
Fatigue
Weakness
Causes
Symptoms
Anorexia
Lethargy
Nausea
Constipation
Kidney stones
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

27-20
Regulation of Magnesium IonsCopyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
Decreased blood Mg2+ levelscause the kidneys to reabsorbmost of the Mg2+ from the filtrate.
Less Mg2+ enters the urine, and the
blood Mg2+ level is maintained.
Increased blood Mg2+ levels inthe filtrate exceed the kidney'scapacity to reabsorb Mg2+ fromthe filtrate.
The Mg2+ not reabsorbed from thefiltrate enter the urine.
ReactionsActions
Actions Reactions
Blo
od
Mg
2+
(no
rmal
ran
ge)
Blo
od
Mg
2+
(no
rmal
ran
ge)
Blood Mg2+ levels increase:Homeostasis Disturbed
Start here
Blood Mg2+ levels decrease:Homeostasis Disturbed
Blood Mg2+ levels increase:Homeostasis Restored
Blood Mg2+ levels decrease:Homeostasis Restored
Control Center Effectors Activated:
Control Center Effectors Activated:
3 4
2 5
61

27-21
Consequences of AbnormalConcentrations of Magnesium Ions
Reduced magnesium intestinal absorption
Renal tubular dysfunction
TABLE 27.9
HYPOMAGNESEMIA (rare)
Malnutrition
Alcoholism
Causes
Symptoms
Some diuretics
Irritability
Muscle weakness
Tetany
Convulsions
HYPERMAGNESEMIA (rare)
Renal failure
Magnesium-containingant acids
Nausea
Vomiting
Muscle weakness
Hypotension
Bradycardia
Reduced respiration
Causes
Symptoms
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

27-22
Regulation of Blood Phosphate ionCopyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
Decreased blood PO43– levels
cause the kidneys to reabsorbmost of the PO4
3– from thefiltrate.
Less PO43– enter the urine and the blood
PO43– level is maintained.
Increased blood PO43– levels
cause the PO43– levels in the
filtrate to exceed the kidney’scapacity to reabsorb PO4
3– fromthe filtrate.
The PO43– not reabsorbed from the filtrate
enter the urine.
ReactionsActions
Actions Reactions
B
loo
d P
O43–
(n
orm
al r
ang
e)
B
loo
d P
O43–
(n
orm
al r
ang
e)
Blood PO43– levels increase:
Homeostasis Disturbed
Start here
Blood PO43– levels decrease:
Homeostasis Disturbed
Blood PO43– levels decrease:
Homeostasis DisturbedBlood PO4
3– levels increase:Homeostasis Disturbed
Control Center Effectors Activated:
Control Center Effectors Activated:
3 4
2
1
5
6

27-23
Regulation of Phosphate Ions
• Under normal conditions, reabsorption of phosphate occurs at maximum rate in the nephron
• An increase in plasma phosphate increases amount of phosphate in nephron beyond that which can be reabsorbed; excess is lost in urine
– Hypophosphatemia: reduced absorption from intestine due to vitamin D deficiency or alcohol abuse.
– Hyperphosphatemia: renal failure, chemotherapy, hyperparathyroidism (secondary to elevated plasma calcium levels)

27-24
Reduced intestinal absorption due to vitamin Ddeficiency or alcohol abuse
Hyperparathyroidism (reduced renal PO4− excretion)
Formation of calcium phosphate deposits in tissuesof lungs, kidneys and joints
TABLE 27.10 Consequences of AbnormalConcentrations of Phosphate Ions
HYPOPHOSPHATEMIA
Causes
Symptoms
Causes
Symptoms
Symptoms of reduced Ca2+ related to formationof deposits
Renal failure
Tissue destruction from chemotherapy
Reduced blood clotting
Reduced white blood cell functions
Reduced oxygentransport
Reduced metabolicrate
Hyperparathyroidism (elevatedrenal PO4– excretion)
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
HYPERPHOSPHATEMIA

27-25
Comparison of Strong and Weak Acids
Hydrochloric acidHCI
Hydrogen ionH+
Chloride ionCI–
(complete dissociation)
+
Carbonic acidH2CO3
Hydrogen ion Bicarbonate ion+
Equilibrium
Strong baseNaOH Na+ OH–
Sodium hydroxide Sodium ion Hydroxide ion
+
(partial dissociation)
(complete dissociation)
Strong acid
Weak acidH+ HCO3
–
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

27-26
27.5 Regulation of Acid-Base Balance
• Acids– Release H+ into
solution
• Bases– Remove H+ from
solution
• Acids and bases– Grouped as strong or
weak
• Buffers: Resist changes in pH– When H+ added, buffer
removes it– When H+ removed, buffer
replaces it
• Types of buffer systems– Carbonic acid/bicarbonate– Protein– Phosphate

27-27
Regulation of Acid-Base Balance
Blood pH increases (H+ decreases):Homeostasis Disturbed
Blood pH decreases (H+ increases):Homeostasis Restored
Kidney:The distal convoluted tubules
decrease H+ secretion into the urine
and decrease HCO3– reabsorption into
the blood.
Lungs:The respiratory center in the braindecreases the rate and depth ofbreathing, which increases blood CO2.
Kidney:
Fewer H+ are removed from the blood,
and fewer HCO3– are available to bind
to H+
Lungs:Increased blood CO2 reacts withwater to produce carbonic acid,
which dissociates to increase H+.
H2O + CO2 H2CO3 H+ + HCO3–
Lungs:The respiratory center in the brainincreases the rate and depth ofbreathing, which decreases blood CO2.
Actions
Actions
Buffers:
Buffers release H+.
Reactions
Buffers:
The number of H+ in the blood increases.
H2O + CO2 H2CO3 H+ + HCO3–
Blo
od
pH
(n
orm
al r
ang
e)
Blo
od
pH
(n
orm
al r
ang
e)
Start here
Blood pH decreases (H+ increases):Homeostasis Disturbed
Blood pH decreases (H+ decreases):Homeostasis Disturbed
H2O + CO2 H2CO3 H+ + HCO3–
Buffers:
Buffers bind H.
Kidney:The distal convoluted tubules
increase H+ secretion into the urine
and increase HCO3– reabsorption into
the blood.
Lungs:
Decreased blood CO2 causes H+
react with HCO3– to form carbonic acid,
which decreases H+ in blood.H2O + CO2 H2CO3 H+ + HCO3
–
Buffers:
The number of H+ in the blood decreases.
Reactions
Kidney:
Fewer H+ are removed from the blood,
and fewer HCO3– are available to bind
to H+
Effectors Activated:
Effectors Activated:
3 4
2
1
5
6
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

27-28
Regulation of Acid/Base Balance• Buffers: if pH rises, buffers bind H+; if pH falls,
buffers release H+
– Protein buffer: Intracellular and plasma proteins absorb H+. Provide ¾ of buffering in body. E.g., hemoglobin.
– Bicarbonate buffering system: Important in plasma– Phosphate buffer system: important as an intracellular
buffer• Respiratory center: if pH rises, respiratory rate
decreases; if pH falls, respiratory rate increases• Kidneys: if pH rises, distal tubule decreases H+
secretion into the urine and decreases HCO3-
absorption into the blood (more H2CO3 will dissociate into H+ and HCO3
-); if pH falls, distal tubule increases H+ secretion into the urine and increases HCO3
- absorption into the blood

27-29
Carbonic acid/bicarbonatebuffer system
Components of the carbonic acid/bicarbonate buffer system are not present in high enough concentrations in the extracellularfluid to constitute a powerful buffer system. However, the concentrations of the components of the buffer system are regulated.Therefore, it plays an exceptionally important role in controlling the pH of extracellular fluid.
Intracellular proteins and plasma proteins form a large pool of protein molecules that can act as buffer molecules. Because oftheir high concentration, they provide approximately three-fourths of the body’s buffer capacity. Hemoglobin in red blood cells isan important intracellular protein. Other intracellular molecules, such as histone proteins and nucleic acids, also act as buffers.
Components of the phosphate buffer system are low in the extracellular fluids, compared with the other buffer systems, but it isan important intracellular buffer system.
Protein buffer system
Phosphate buffersystem
Characteristics of Buffer SystemsTABLE 27.11
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

27-30
Respiratory Regulation ofAcid-Base Balance
• Achieved through carbonic acid/bicarbonate buffer system– As carbon dioxide levels increase, pH decreases
– As carbon dioxide levels decrease, pH increases
– Carbon dioxide levels and pH affect respiratory centers
• Hypoventilation increases blood carbon dioxide levels
• Hyperventilation decreases blood carbon dioxide levels

27-31
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
H2O + CO2 H2CO3 H+ + HCO3–
Circulation
Carbonican hydrase
Capillary
11
2
3
2
3
Carbon dioxide reacts with H2O toform H2CO3. An enzyme, carbonicanhydrase, found in red blood cellsand on the surface of blood vesselepithelium, catalyzed the reaction.Carbonic acid dissociates to formH+ and HCO3
–. An equilibrium isquickly established.
Decreased pH in the extracellularfluid stimulates the respiratorycenter and causes an increasedrate and depth of breathing.
Increased rate and depth ofbreathing causes CO2 to beexpelled from the lungs, thusreducing the extracellular CO2
levels. As CO2 levels decrease,theextracellular concentration of H+
decreases, and the extracellularfluid pH increases.
DecreasedpH
Respiratorycenter in
brainstem
Lungs
Increasedrespiratory rate
and depth
Increased CO2
expelled from the lungs

27-32
Renal Regulation of Acid-Base Balance
• Secretion of H+ into filtrate and reabsorption of HCO3
- into ECF cause extracellular pH to increase
• HCO3- in filtrate reabsorbed
• Rate of H+ secretion increases as body fluid pH decreases or as aldosterone levels increase
• Secretion of H+ inhibited when urine pH falls below 4.5

27-33
Renal Regulation ofAcid-Base Balance
CO2Lumen
Na+
4
When the filtrate or blood pH
decreases, H+ combine with HCO3–
to form carbonic acid that is convertedinto CO2 and H2O. The CO2 diffusesinto tubule cells.
In the tubule cells, CO2 combines withH2O to form H2CO3 that dissociates to
form H+ and HCO3.
An antiport mechanism secretes H+ intothe filtrate in exchange for Na+ from thefiltrate. As a result, filtrate pH decreases.
Bicarbonate ions are symported withNa+ into the interstitial fluid. They thendiffuse into capillaries.
In capillaries, HCO3– combine with H+.This decreases the H+ concentrationand increases blood pH.
1
2
5
3
1
2
3
4
5
Peritubularcapillary
Interstitialfluid
Basalmembrane
Tubule cellcytoplasmApicalmembrane
CO2
CO2 + H2O H2CO3
Na+
H+
Symport
Antiport
H+ HCO3–+
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
+ H2O H2CO3 H+ + HCO3
– HCO3– + Na+
27-34
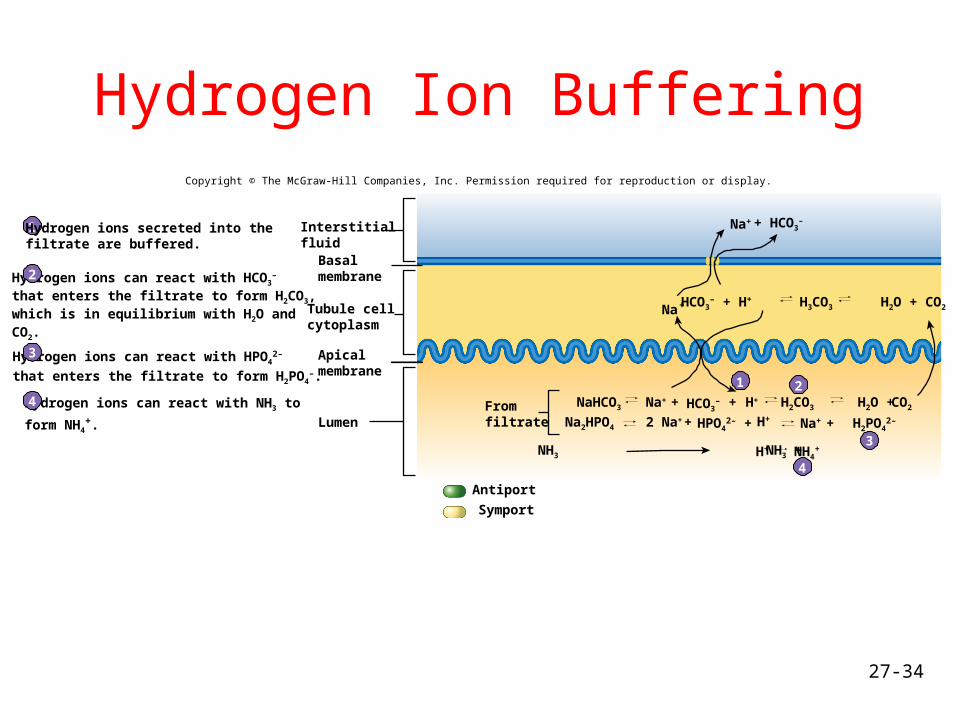
Hydrogen Ion BufferingCopyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
1 2
3
4
Lumen
Na+
Na+
Hydrogen ions can react with HCO3–
that enters the filtrate to form H2CO3,which is in equilibrium with H2O andCO2.
Hydrogen ions can react with HPO42–
that enters the filtrate to form H2PO4–.
Hydrogen ions can react with NH3 to
form NH4+.
1
2
3
4
Hydrogen ions secreted into thefiltrate are buffered.
InterstitialfluidBasalmembrane
Tubule cellcytoplasm
Apicalmembrane
Symport
Antiport
HCO3– + H+ H3CO3 H2O + CO2
NaHCO3Fromfiltrate Na2HPO4
NH3 NH3 +
+ HCO3–
Na+ + HCO3– H2CO3 H2O ++ H+ CO2
2 Na+ + HPO42– + H+ Na+ + H2PO4
2–
H+ NH4+

27-35
Acidosis and Alkalosis• Acidosis: pH body fluids below 7.35
– Respiratory: Caused by inadequate ventilation- reduced elimination of CO2, asthma, damage to respiratory center in brain, emphysema.
– Metabolic: Results from all conditions other than respiratory that decrease pH- diarrhea, vomiting, ingesting overdose of aspirin, untreated diabetes mellitus, anaerobic respiration
• Alkalosis: pH body fluids above 7.45– Respiratory: Caused by hyperventilation, high altitude (reduced
partial pressure of O2
– Metabolic: Results from all conditions other than respiratory that increase pH- severe vomiting, too much aldosterone, ingestion of substances like bicarbonate of soda.
• Compensatory mechanisms

27-36





























