Embed Size (px)
Citation preview
CHAPTER 4 Management of MS-related symptoms 1
Chapter 4 Management of MS-related symptoms
CONTENTS
4.1 Introduction ----------------------------------------------------------------------------------------5
4.2 Fatigue -------------------------------------------------------------------------------------------------6 4.2.1 Learning objectives ---------------------------------------------------------------------------------------------------------------------- 6
4.2.2 Desired patient outcomes ---------------------------------------------------------------------------------------------------------- 6
4.2.3 Introduction ------------------------------------------------------------------------------------------------------------------------------------ 6
4.2.4 Nursing assessment ---------------------------------------------------------------------------------------------------------------------- 7
4.2.5 Interventions ---------------------------------------------------------------------------------------------------------------------------------- 7
4.2.6 Conclusion --------------------------------------------------------------------------------------------------------------------------------------- 8
4.2.7 References ----------------------------------------------------------------------------------------------------------------------------------------8
4.3 Bladder dysfunction -------------------------------------------------------------------------9 4.3.1 Learning objectives -----------------------------------------------------------------------------------------------------------------------9
4.3.2 Desired patient outcomes -----------------------------------------------------------------------------------------------------------9
4.3.3 Introduction ----------------------------------------------------------------------------------------------------------------------------------10
4.3.4 Nursing assessment ---------------------------------------------------------------------------------------------------------------------11
4.3.5 Pharmacological interventions for bladder dysfunction in MS ---------------------------------13
4.3.6 Conclusion -------------------------------------------------------------------------------------------------------------------------------------14
4.3.7 References -------------------------------------------------------------------------------------------------------------------------------------15
4.3.8 Suggested reading ----------------------------------------------------------------------------------------------------------------------15
4.4 Bowel dysfunction ---------------------------------------------------------------------------17 4.4.1 Learning objectives --------------------------------------------------------------------------------------------------------------------17
4.4.2 Desired patient outcomes --------------------------------------------------------------------------------------------------------17
4.4.3 Introduction ----------------------------------------------------------------------------------------------------------------------------------17
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND2
4.4.4 Nursing assessment --------------------------------------------------------------------------------------------------------------------18
4.4.5 Interventions --------------------------------------------------------------------------------------------------------------------------------19
4.4.6 References -------------------------------------------------------------------------------------------------------------------------------------22
4.4.7 Suggested reading ----------------------------------------------------------------------------------------------------------------------23
4.5 Pain ----------------------------------------------------------------------------------------------------24 4.5.1 Learning objectives --------------------------------------------------------------------------------------------------------------------24
4.5.2 Desired patient outcomes --------------------------------------------------------------------------------------------------------24
4.5.3 Introduction ----------------------------------------------------------------------------------------------------------------------------------24
4.5.4 Cause of pain in MS ---------------------------------------------------------------------------------------------------------------------25
4.5.5 Nursing assessment --------------------------------------------------------------------------------------------------------------------25
4.5.6 Interventions --------------------------------------------------------------------------------------------------------------------------------26
4.5.7 References -------------------------------------------------------------------------------------------------------------------------------------29
4.5.8 Suggested reading ----------------------------------------------------------------------------------------------------------------------30
4.6 Spasticity -------------------------------------------------------------------------------------------31 4.6.1 Learning objectives --------------------------------------------------------------------------------------------------------------------31
4.6.2 Desired patient outcomes --------------------------------------------------------------------------------------------------------31
4.6.3 Introduction ----------------------------------------------------------------------------------------------------------------------------------31
4.6.4 Nursing assessment --------------------------------------------------------------------------------------------------------------------32
4.6.5 Interventions --------------------------------------------------------------------------------------------------------------------------------32
4.6.6 References -------------------------------------------------------------------------------------------------------------------------------------33
4.6.7 Suggested reading ----------------------------------------------------------------------------------------------------------------------33
4.7 Tremor ------------------------------------------------------------------------------------------------35 4.7.1 Preface ---------------------------------------------------------------------------------------------------------------------------------------------35
4.7.2 Learning objectives --------------------------------------------------------------------------------------------------------------------35
4.7.3 Desired patient outcomes --------------------------------------------------------------------------------------------------------35
4.7.4 Introduction ----------------------------------------------------------------------------------------------------------------------------------35
4.7.5 Nursing assessment --------------------------------------------------------------------------------------------------------------------36
4.7.6 Interventions --------------------------------------------------------------------------------------------------------------------------------38
4.7.7 References -------------------------------------------------------------------------------------------------------------------------------------38
4.7.8 Suggested reading ----------------------------------------------------------------------------------------------------------------------39
CHAPTER 4 Management of MS-related symptoms 3
4.8 Altered mobility -------------------------------------------------------------------------------40 4.8.1 Learning objectives --------------------------------------------------------------------------------------------------------------------40
4.8.2 Desired patient outcomes --------------------------------------------------------------------------------------------------------40
4.8.3 Introduction ----------------------------------------------------------------------------------------------------------------------------------40
4.8.4 Nursing assessment --------------------------------------------------------------------------------------------------------------------40
4.8.5 Interventions --------------------------------------------------------------------------------------------------------------------------------42
4.8.6 References -------------------------------------------------------------------------------------------------------------------------------------42
4.8.7 Suggested reading ----------------------------------------------------------------------------------------------------------------------43
4.9 Speechandswallowingdifficulties ---------------------------------------------44 4.9.1 Learning objectives --------------------------------------------------------------------------------------------------------------------44
4.9.2 Desired patient outcomes --------------------------------------------------------------------------------------------------------44
4.9.3 Introduction ----------------------------------------------------------------------------------------------------------------------------------44
4.9.4 Nursing assessment --------------------------------------------------------------------------------------------------------------------45
4.9.5 Interventions --------------------------------------------------------------------------------------------------------------------------------45
4.9.6 References -------------------------------------------------------------------------------------------------------------------------------------46
4.9.7 Suggested reading ----------------------------------------------------------------------------------------------------------------------46
4.10 Visual problems in MS -------------------------------------------------------------------47 4.10.1 Learning objectives --------------------------------------------------------------------------------------------------------------------47
4.10.2 Desired patient outcomes --------------------------------------------------------------------------------------------------------47
4.10.3 Introduction ----------------------------------------------------------------------------------------------------------------------------------47
4.10.4 Nursing assessment --------------------------------------------------------------------------------------------------------------------48
4.10.5 Interventions --------------------------------------------------------------------------------------------------------------------------------49
4.10.6 Impact of visual problems for person with MS -----------------------------------------------------------------49
4.10.7 Role of the MS nurse -------------------------------------------------------------------------------------------------------------------49
4.10.8 Conclusion -------------------------------------------------------------------------------------------------------------------------------------50
4.10.9 References -------------------------------------------------------------------------------------------------------------------------------------50
4.10.10 Suggested reading ----------------------------------------------------------------------------------------------------------------------50
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND4
4.11 Depression -----------------------------------------------------------------------------------------51 4.11.1 Learning objectives --------------------------------------------------------------------------------------------------------------------51
4.11.2 Desired patient outcomes --------------------------------------------------------------------------------------------------------51
4.11.3 Introduction ----------------------------------------------------------------------------------------------------------------------------------51
4.11.4 Nursing assessment --------------------------------------------------------------------------------------------------------------------52
4.11.5 Interventions --------------------------------------------------------------------------------------------------------------------------------53
4.11.6 References -------------------------------------------------------------------------------------------------------------------------------------55
4.12 Cognitive impairment --------------------------------------------------------------------56 4.12.1 Learning objectives --------------------------------------------------------------------------------------------------------------------56
4.12.2 Desired patient outcomes --------------------------------------------------------------------------------------------------------56
4.12.3 Introduction ----------------------------------------------------------------------------------------------------------------------------------56
4.12.4 Nursing assessment --------------------------------------------------------------------------------------------------------------------57
4.12.5 Nursing care plan ------------------------------------------------------------------------------------------------------------------------58
4.12.6 References -------------------------------------------------------------------------------------------------------------------------------------59
4.13 Progress check ---------------------------------------------------------------------------------60
4.14 Progress check answers-----------------------------------------------------------------65
4.15 Glossary ---------------------------------------------------------------------------------------------70
CHAPTER 4 Management of MS-related symptoms 5
4.1 INTRODUCTIONSymptomatic therapies are highly important in patient management.
The complaints and symptoms most commonly associated with multiple sclerosis (MS) are:
· Fatigue
· Bladder and bowel dysfunctions
· Pain
· Spasticity
· Tremor and alterations in mobility
· Speech and swallowing difficulties
· Visual disturbances
· Depression
· Cognitive impairment.
In all aspects of the management the process of patient care the Clinical Nurse Specialist (CNSp) should use the core competencies of the MS nurse competency framework as a guide for his/her role. The MS nurse must undertake a complete holistic assessment of the patient incorporating a full physical, psychological and social assessment, and then use this assessment to appropriately plan care. The assessment and care plan should be based on a recognised theoretical framework and incorporate a plan for the evaluation of patient care.
This chapter provides specific guidance to support the nursing assessment and management of MS-related symptoms. The desired outcomes of treatment for these symptoms are also presented. In the process of assessing, planning, implementing and evaluating all aspects of patient care the CNSp must be aware of the limitations to his/her own scope of practice and refer the patient on to the relevant multidisciplinary team member at the appropriate time.
At the end of the chapter, please find a section entitled Progress check; this section tests your knowledge of the information presented in the chapter.
Management of MS-related symptoms
CHAPTER 4
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND6
4.2 FATIGUEFatigue is recognised as the most common symptom of MS (Schapiro & Schneider; cited in Halper & Holland, 2011). Surveys and case control studies indicate that 75–95 % of individuals experience fatigue, and 50–60% report fatigue as their most disabling symptom (Fisk et al, 1994; Freal et al, 1984). ‘The term MS fatigue refers to a lassitude or overwhelming fatigue that comes on suddenly’ (Schapiro & Schneider; cited in Halper & Holland, 2011).
4.2.1 Learning objectivesAfter completing this section, the reader will be able to:
· Describe the desired outcomes of fatigue interventions
· Describe and apply strategies for the assessment of fatigue
· Implement interventions for the management of fatigue.
4.2.2 Desired patient outcomesThe patient will be able to discuss and outline the problems they are experiencing with fatigue. The patient will learn how to manage and cope with their fatigue. The patient will gain a further understanding on fatigue as a symptom in MS and the treatments used.
The patient will demonstrate improved performance on daily activities in the home and at work, as determined by patient self-report and fatigue measurement scales (see Appendix 2).
4.2.3 IntroductionFatigue not only exacerbates impairment and disability, it is also directly related to the individual’s sense of control over the illness and overall mental health. It is suggested that fatigue is one of the major reasons for unemployment among people with multiple sclerosis (PWMS) (Edgley et al, 1991). The pathophysiological basis of MS-related fatigue remains obscure despite intensive investigation.
The MS Trust describes a variety of different types of fatigue, which affect MS patients including primary fatigue, short-circuiting fatigue, lassitude, heat sensitive fatigue, secondary fatigue, medication side effect fatigue, post-exertion, infection triggered fatigue or environmental (MS Trust, 2011).
Patients with MS rank fatigue as one of the MS-related symptoms that most impairs their quality of life. Fatigue is considered a chronic condition that can be accompanied by neurological exacerbations or no change in neurological symptoms.
Fatigue in MS is often characterised as either focal-muscle fatigability or a generalised sense of lassitude. The aetiology of MS-related fatigue is not well understood; however, default conduction of the demyelinated fibres and the presence of circulating cytokines in serum and cerebrospinal fluid may be contributing factors. Furthermore, many MS-related symptoms may contribute to fatigue, including depression, pain, insomnia, or mobility impairment. Therefore, before appropriate treatment can be administered, the origin of fatigue should be determined. (Coulthard-
CHAPTER 4 Management of MS-related symptoms 7
Morris & Vollmer 1995; Fisk et al, 1994; Krupp et al, 1989; Multiple Sclerosis Council for Clinical Practice Guidelines 1998; Schapiro & Schneider cited in Halper & Holland, 2011; Van den Noort & Holland 1999; Vercoulen et al, 1996).
In this section guidelines assessing fatigue are presented. Interventions for managing fatigue and desired treatment outcomes are also discussed.
4.2.4 Nursing assessmentThe nursing assessment of fatigue begins with obtaining a full patient report on the history of the fatigue, determining whether it is a new symptom and if the fatigue is continuous or intermittent. The nurse, in conjunction with the patient will identify possible contributing factors, such as relapse, medications, sleep disturbances, concurrent illness (e.g. infection), level of activity (e.g. deconditioning), heat, lifestyle patterns, diet, exercise, psychosocial issues, pain, depression and spasticity.
Assessing the severity of the fatigue involves, administering a fatigue measurement scale (see appendix 2 Modified Fatigue Impact Scale [MFIS] in The Multiple Sclerosis Quality of Life Inventory [MSQLI]); determining the fatigue’s effect on the patient’s daily activities; and asking the patient to complete a fatigue-management diary.
The nurse will determine the impact of fatigue on other MS-related symptoms, as listed above other MS symptoms can exacerbate each other (e.g. depression and fatigue or spasticity and fatigue).
The nurse and patient together will identify existing management strategies and coping behaviours used by the patient and determine the effectiveness of same.
4.2.5 InterventionsIn 2011 the MS Trust (UK) recommended coping with fatigue through a fatigue management plan comprising advice on frequent rests, prioritising activities, planning ahead, organising living and work space and leading a healthy lifestyle (MS Trust, 2011).
The MS nurse will encourage appropriate lifestyle modifications.
4.2.5.1 Frequent rest and prioritising activities
The nurse and patient together, will plan the patient’s day in accordance with his or her daily activities, allowing for rest breaks and adequate sleeping patterns to suit each patient individually. The side effects of a variety of medications, which the patient may be receiving, can include fatigue. Informing the patient of this may help them to understand aspects of the cause of their fatigue. These medications include; anti-spasticity medications, anticonvulsants/anti-epileptics, and antidepressants.
4.2.5.2 Organising living and work spaces
Environmental issues can impact on fatigue, such as temperature extremes. Adjusting the home/work environment according to the patient’s requirements (e.g. turning on or installing air conditioning) may alleviate their fatigue.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND8
4.2.5.3 Leading a healthy lifestyle
The nurse should involve appropriate members of the multidisciplinary team in order to better assist the patient. For example it may be helpful to refer the patient to a dietician, for detailed advice on appropriate foods to maximise energy levels. Involving an occupational therapist can assist the patient with practical assistive devices for home or the work place e.g. appropriate mobility aides.
Referring to a physiotherapist can provide the patient with a personal fitness programme to increase stamina.
The nurse’s role, regarding fatigue must include ongoing evaluation of the patient’s fatigue management strategies, to ensure they are effective and if not, investigate the reasons in conjunction with the patient.
4.2.6 ConclusionThe MS nurse has a key role in the assessment, education and support of the MS patient with fatigue. As fatigue is the most common symptom of MS (Schapiro & Schneider; cited in Halper & Holland, 2011), the MS nurse will need to develop expert skills in assisting the patient with the management of this symptom.
4.2.7 References
Coulthard-Morris L, Vollmer T. Multiple sclerosis fatigue: classification and treatment options. Mult Sclerosis Clin Issues 1995; 2: 2–6.
Edgley K, Sullivan M, Dehoux E, 1991. A survey of multiple sclerosis: Eleven Determinates of Employment Status.
Fisk JD, Pontefract A, Ritvo PG et al. The impact of fatigue on patients with multiple sclerosis. Can J Neurol Sci 1994; 21: 9–14.
Freal JF, Kraft GH, Congell JK. Symptomatic fatigue in MS. Archives Physical Medical Rehabilitation 1984; 65: 135–138.
Halper & Holland, 2011 Comprehensive Nursing Care in Multiple Sclerosis. 3rd ed; Springer Publishing Company, New York.
Irish Medicines Board (2010, updated 2011) Summary of Product Characterisitics for Modafinil [online] Accessed 15/2/12 at www.imb.ie.
Krupp LB, LaRocca NG, Scheinberg AD. The fatigue severity scale: application to patients with multiple sclerosis and systemic lupus erythematosus. Arch Neurol 1989; 46: 1121–1123.
Multiple Sclerosis Council for Clinical Practice Guidelines. Fatigue and multiple sclerosis: evidence-based management strategies for fatigue in multiple sclerosis. Paralyzed Veterans of America; 1998.
MS Trust 2011 Multiple Sclerosis Information for Health and Social Care Professionals, 4th ed. Hertfordshire.
Van den Noort S, Holland NJ. Multiple sclerosis in clinical practice. 2nd ed. New York: Demos Medical Publishing Co. Inc.; 1999.
Vercoulen JH, Hommes OR, Swanink CM et al. The measurement of fatigue in patients with multiple sclerosis: a multidimensional comparison of patients with chronic fatigue syndrome and healthy subjects. Arch Neurol 1996; 53: 642–649.
CHAPTER 4 Management of MS-related symptoms 9
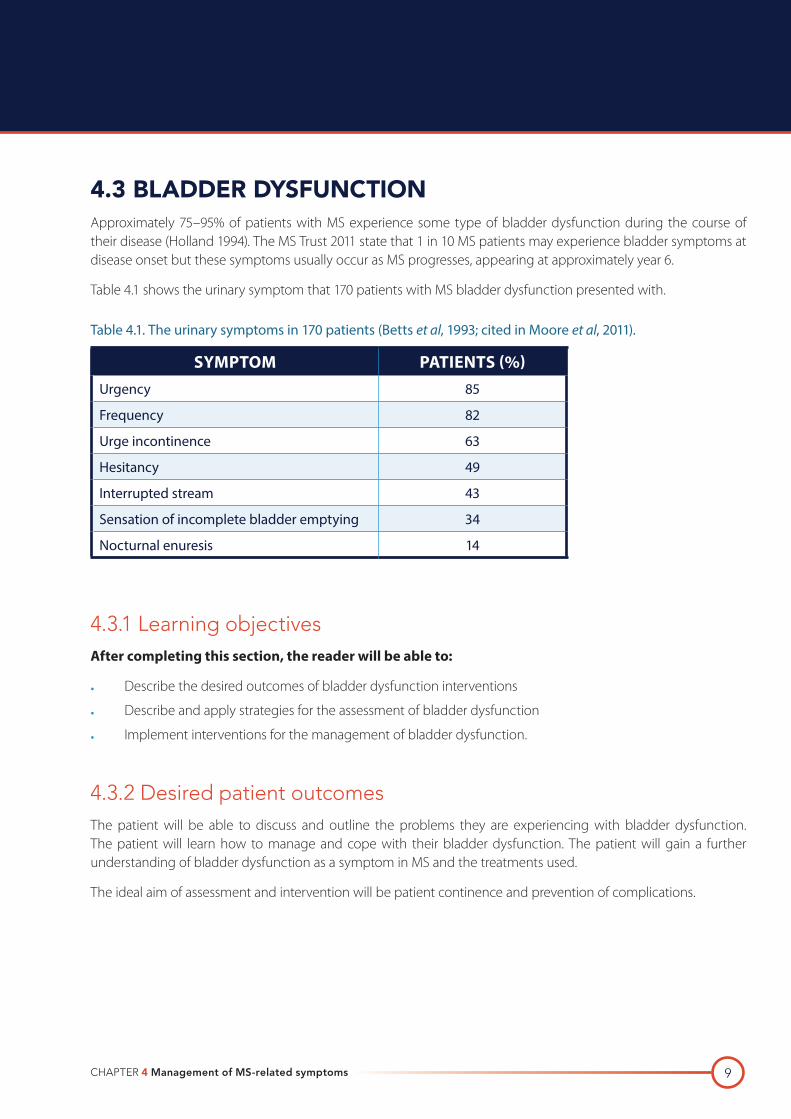
4.3 BLADDER DYSFUNCTIONApproximately 75–95% of patients with MS experience some type of bladder dysfunction during the course of their disease (Holland 1994). The MS Trust 2011 state that 1 in 10 MS patients may experience bladder symptoms at disease onset but these symptoms usually occur as MS progresses, appearing at approximately year 6.
Table 4.1 shows the urinary symptom that 170 patients with MS bladder dysfunction presented with.
Table 4.1. The urinary symptoms in 170 patients (Betts et al, 1993; cited in Moore et al, 2011).
SYMPTOM PATIENTS (%)Urgency 85
Frequency 82
Urge incontinence 63
Hesitancy 49
Interrupted stream 43
Sensation of incomplete bladder emptying 34
Nocturnal enuresis 14
4.3.1 Learning objectivesAfter completing this section, the reader will be able to:
· Describe the desired outcomes of bladder dysfunction interventions
· Describe and apply strategies for the assessment of bladder dysfunction
· Implement interventions for the management of bladder dysfunction.
4.3.2 Desired patient outcomesThe patient will be able to discuss and outline the problems they are experiencing with bladder dysfunction. The patient will learn how to manage and cope with their bladder dysfunction. The patient will gain a further understanding of bladder dysfunction as a symptom in MS and the treatments used.
The ideal aim of assessment and intervention will be patient continence and prevention of complications.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND10
4.3.3 IntroductionTwo neural circuits are thought to control bladder function: the sacral spinal cord for storage and the pontine micturation centre for emptying. Any disruption in the pathways between these circuits may result in a dysfunction (Blaivas, 1980). ‘Interruption of the spinal cord pathways may result in excessive detrusor contractions, involuntary sphincter relaxation or contraction, or detrusor areflexia with urinary retention’ (Namey cited in Halper & Holland, 2011).
According to Kurtze (1983; cited in Moore et al, 2011), the severity of bladder problems correlates with the degree of spinal cord involvement.
The types of bladder dysfunction most commonly associated with MS are (Andrews & Husmann, 1997; Giannantoni et al, 1998; Holland, 1994; van den Noort & Holland, 1999):
· Failure to store
· Failure to empty
· Combination of failure to store and failure to empty.
These types of bladder dysfunction are referred to as ‘neurogenic bladder’ (Namey cited in Halper & Holland, 2011)
Failure to store (detrusor hyperreflexia) is the most common type of bladder dysfunction in MS, with reported incidences ranging from 26–50%. Failure to store occurs when the bladder is unable to accommodate increasing urine volumes, causing spontaneous contractions within the bladder. Symptoms of this dysfunction include urgency, frequency and urge incontinence.
Failure to empty is less common (i.e. incidence is 19–40%) but can result in more serious complications than failure to store. It may be caused by one or more of the following:
· An atonic bladder
· Detrusor hyperreflexia with poorly sustained contractions
· Detrusor-sphincter dyssynergia.
Symptoms of failure to empty include retention, overflow incontinence, and urinary tract infections. Patients will characteristically have a post residual volume of urine of 100 ml or more.
Combination failure to store and failure to empty occurs in 24–46% of patients with bladder dysfunction and MS. This condition is often associated with detrusor-sphincter dyssynergia and the only real way to diagnose it is by using urodynamics. The post residual volume of urine is variable. Symptoms of this type of bladder dysfunction include those associated with both failure to store and failure to empty.
CHAPTER 4 Management of MS-related symptoms 11
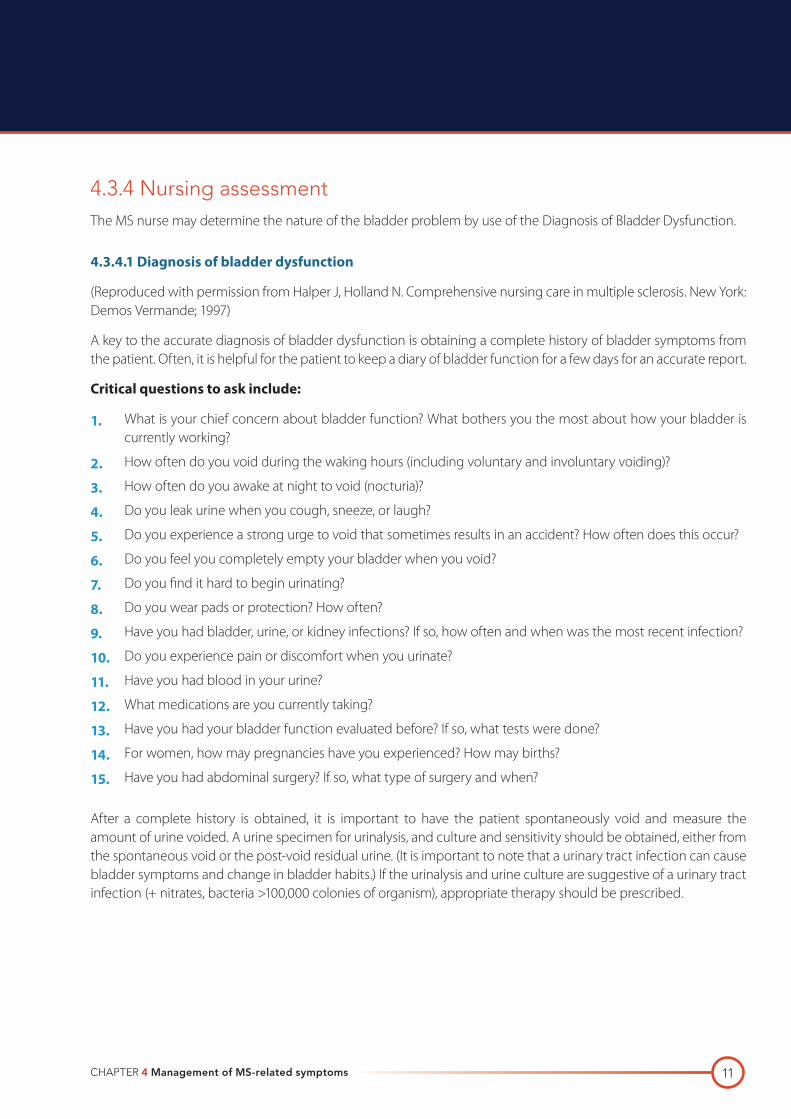
4.3.4 Nursing assessmentThe MS nurse may determine the nature of the bladder problem by use of the Diagnosis of Bladder Dysfunction.
4.3.4.1 Diagnosis of bladder dysfunction
(Reproduced with permission from Halper J, Holland N. Comprehensive nursing care in multiple sclerosis. New York: Demos Vermande; 1997)
A key to the accurate diagnosis of bladder dysfunction is obtaining a complete history of bladder symptoms from the patient. Often, it is helpful for the patient to keep a diary of bladder function for a few days for an accurate report.
Critical questions to ask include:
1. What is your chief concern about bladder function? What bothers you the most about how your bladder is currently working?
2. How often do you void during the waking hours (including voluntary and involuntary voiding)?
3. How often do you awake at night to void (nocturia)?
4. Do you leak urine when you cough, sneeze, or laugh?
5. Do you experience a strong urge to void that sometimes results in an accident? How often does this occur?
6. Do you feel you completely empty your bladder when you void?
7. Do you find it hard to begin urinating?
8. Do you wear pads or protection? How often?
9. Have you had bladder, urine, or kidney infections? If so, how often and when was the most recent infection?
10. Do you experience pain or discomfort when you urinate?
11. Have you had blood in your urine?
12. What medications are you currently taking?
13. Have you had your bladder function evaluated before? If so, what tests were done?
14. For women, how may pregnancies have you experienced? How may births?
15. Have you had abdominal surgery? If so, what type of surgery and when?
After a complete history is obtained, it is important to have the patient spontaneously void and measure the amount of urine voided. A urine specimen for urinalysis, and culture and sensitivity should be obtained, either from the spontaneous void or the post-void residual urine. (It is important to note that a urinary tract infection can cause bladder symptoms and change in bladder habits.) If the urinalysis and urine culture are suggestive of a urinary tract infection (+ nitrates, bacteria >100,000 colonies of organism), appropriate therapy should be prescribed.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND12
The nurse will perform a bladder ultrasound (if appropriately trained and competent to do so and if equipment available at clinic). This will allow the obtainment of a post-void residual. The significance of results depend on local hospital policy, although van den Noort et al (1999) suggests 100 ml to be a clinically significant finding some hospitals require higher post-void residual prior to intervention, please refer to local hospital policy in your area. NICE guidelines recommend the use of bladder scans in the assessment of post void residuals (NICE, 2006).
In conjunction with the patient, the nurse will be able to describe the problematic patient symptoms in terms of frequency, urgency, hesitancy, burning and discomfort, incontinence, incidence of urinary tract infections, retention, nocturia and to determine onset and duration of symptoms.
Following these investigations the nurse will be in a position to categorise bladder dysfunction into one of the following categories according to presenting symptoms:
· Failure to store (i.e. presenting symptoms include frequency, urgency, and incontinence)
· Failure to empty (i.e. presenting symptoms include hesitancy, dribbling and leaking, retention, and sensations of incomplete emptying)
· Combination of failure to store and failure to empty (i.e. presenting symptoms include a combination of the above-mentioned symptoms).
The nurse can identify possible contributing factors to the bladder dysfunction by taking a thorough patient history and being alert to; concurrent medical conditions (e.g. urinary tract infection, other infections), reduced mobility, poor cognition, reduced dexterity, spasticity, ataxia and/or tremor, nutrition and fluid intake (especially if the patient has a high caffeine intake).
Bladder dysfunction can impact on many aspects of the patient’s life. The nurse and patient may discuss the impact of bladder dysfunction on the patient’s sexual activity, recreation/social activities, employment, quality of life and impact to carer, if applicable.
Secondary complications including infection (urinary tract infections) and skin breakdown should also be assessed.
The nurse will also be in a position to determine the impact of bladder dysfunction on other MS-related symptoms, e.g. bladder dysfunction and depression and will assess the severity of the dysfunction by administering a quality of life scale, e.g. the Bladder Control Scale in: The MSQLI.
The nurse and patient together will identify existing management strategies and coping behaviours used by the patient, and determine the effectiveness of same.
CHAPTER 4 Management of MS-related symptoms 13
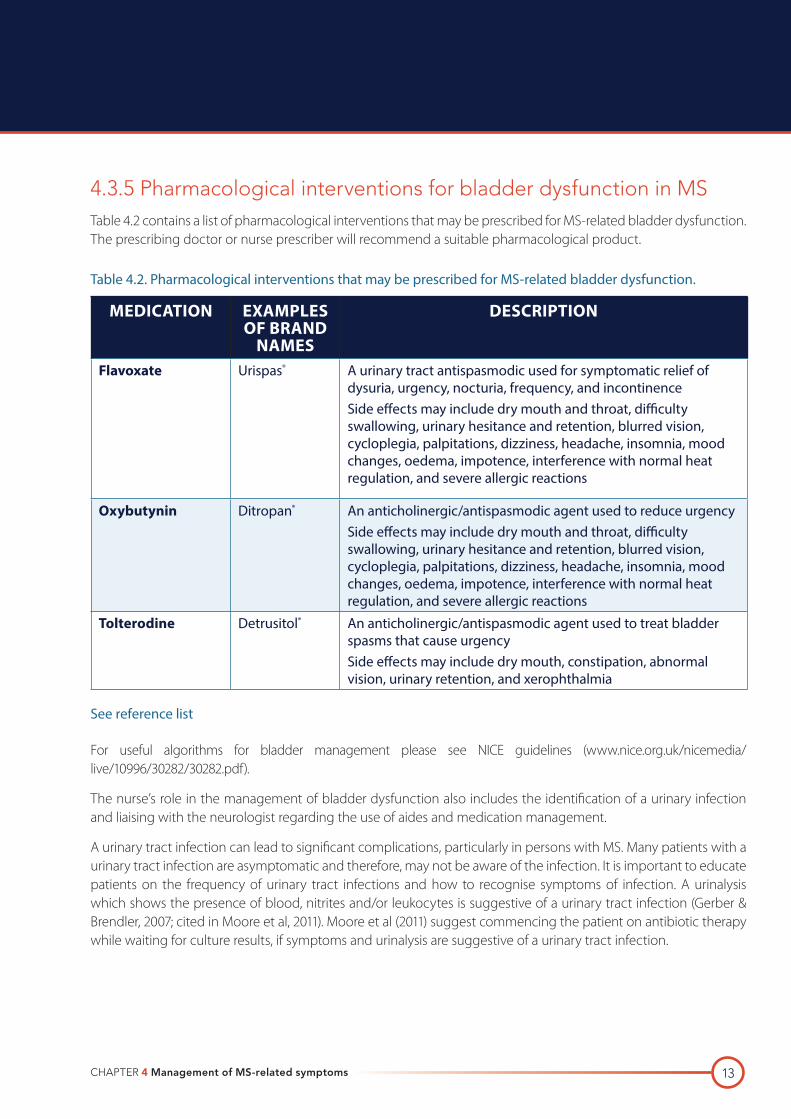
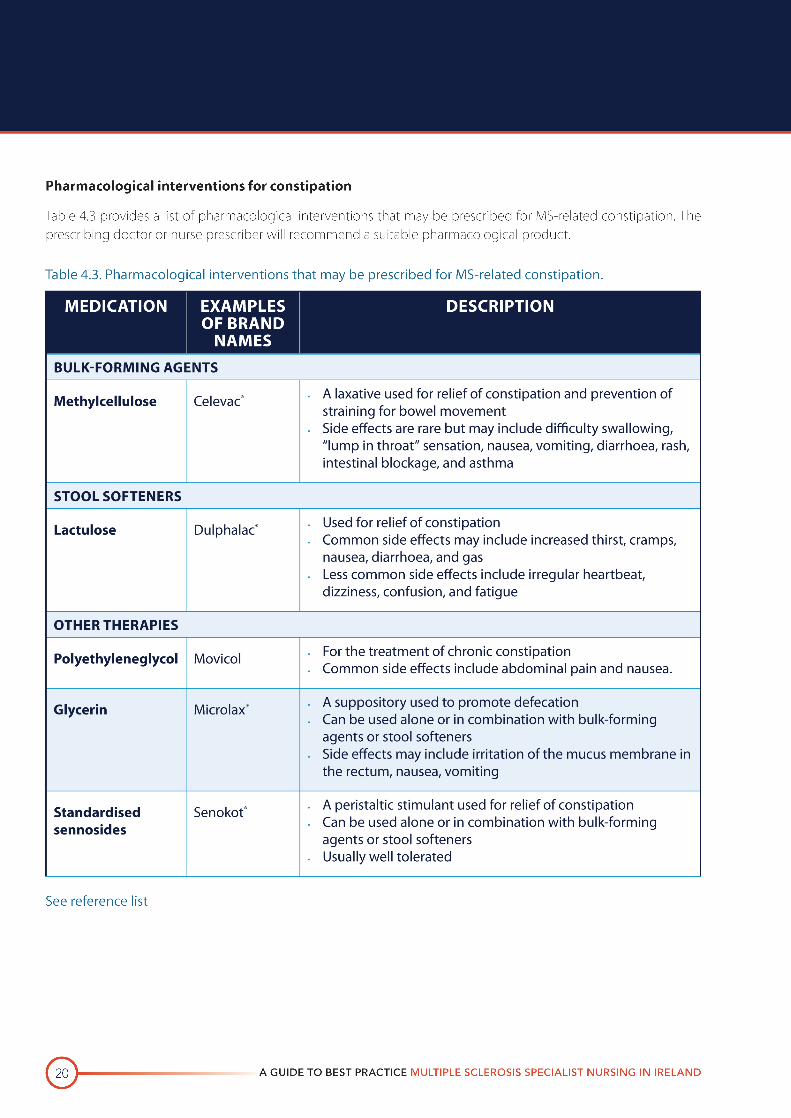
4.3.5 Pharmacological interventions for bladder dysfunction in MSTable 4.2 contains a list of pharmacological interventions that may be prescribed for MS-related bladder dysfunction. The prescribing doctor or nurse prescriber will recommend a suitable pharmacological product.
Table 4.2. Pharmacological interventions that may be prescribed for MS-related bladder dysfunction.
MEDICATION EXAMPLES OF BRAND
NAMES
DESCRIPTION
Flavoxate Urispas® A urinary tract antispasmodic used for symptomatic relief of dysuria, urgency, nocturia, frequency, and incontinenceSide effects may include dry mouth and throat, difficulty swallowing, urinary hesitance and retention, blurred vision, cycloplegia, palpitations, dizziness, headache, insomnia, mood changes, oedema, impotence, interference with normal heat regulation, and severe allergic reactions
Oxybutynin Ditropan® An anticholinergic/antispasmodic agent used to reduce urgencySide effects may include dry mouth and throat, difficulty swallowing, urinary hesitance and retention, blurred vision, cycloplegia, palpitations, dizziness, headache, insomnia, mood changes, oedema, impotence, interference with normal heat regulation, and severe allergic reactions
Tolterodine Detrusitol® An anticholinergic/antispasmodic agent used to treat bladder spasms that cause urgency Side effects may include dry mouth, constipation, abnormal vision, urinary retention, and xerophthalmia
See reference list
For useful algorithms for bladder management please see NICE guidelines (www.nice.org.uk/nicemedia/live/10996/30282/30282.pdf).
The nurse’s role in the management of bladder dysfunction also includes the identification of a urinary infection and liaising with the neurologist regarding the use of aides and medication management.
A urinary tract infection can lead to significant complications, particularly in persons with MS. Many patients with a urinary tract infection are asymptomatic and therefore, may not be aware of the infection. It is important to educate patients on the frequency of urinary tract infections and how to recognise symptoms of infection. A urinalysis which shows the presence of blood, nitrites and/or leukocytes is suggestive of a urinary tract infection (Gerber & Brendler, 2007; cited in Moore et al, 2011). Moore et al (2011) suggest commencing the patient on antibiotic therapy while waiting for culture results, if symptoms and urinalysis are suggestive of a urinary tract infection.

A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND14
Educate the patient on intermittent self-catheterisation if required. Ensure they can perform this task safely and effectively; this may require ongoing education, support and demonstration. The MS nurse may involve continence advisors, who work within the community, to assess and make appropriate recommendations in conjunction with the nurse and patient.
Patient and family education regarding catheter care is a key aspect in preventing complications associated with indwelling catheters. The MS nurse may provide information and support to the patient and family/carers on drainage and emptying, risk of infection and risk of blockage.
The MS nurse in consultation with the neurologist or urologist, may feel the use of a bladder stimulator will benefit the patient. A trial carried out on 36 patients, 29 of which had MS, found that the bladder stimulator device was effective at emptying the neurogenic bladder (Dasgupta et al, 1997); however after performing two systematic reviews of randomised controlled trials using Cochrane library NICE guidelines (2006) state that the adverse effects of bladder stimulation include vaginal irritation, tenderness, bleeding and faecal incontinence (NICE, 2006).
Patient education on issues that may exacerbate their bladder dysfunction is necessary to allow the patient to modify their lifestyle accordingly. Exacerbating influences include, but are not limited to, caffeine and alcohol consumption, dehydration and constipation.
A urology consultation may be required if symptoms remain unmanageable. Fowler & O’Malley (2003) suggest that the following symptoms require a referral to urology specialist: recurrent urinary tract infections, evidence of impaired renal function, pain thought to be arising from the upper or lower urinary tract and haematuria. These recommendations are similar to NICE guidelines although also included is urgent referral for suspected malignant mass arising from the urinary tract, microscopic haematuria in the over 50s.
The need for invasive treatments such as supra-pubic catheterisation or Botox (Botulinum toxin) injections will also require a urology consultation. A study carried out by Kalsi et al (2007) cited in Moore et al (2011), on 43 MS patients receiving Botulinum toxin A injections for detrusor over-activity, 42 of these patients had to undertake intermittent self-catheterisation as a direct result of the injections. NICE guidelines (2006) state that the availability of Botulinum toxin A for detrusor over-activity has led to its uptake in practice, however there is limited high-quality safety data available.
The nurse’s role, regarding bladder dysfunction must include ongoing evaluation of the patient’s management strategies, to ensure they are effective and if not, investigate the reasons in conjunction with the patient.
4.3.6 ConclusionThe MS nurse has a key role in the assessment, education and support of the MS patient with bladder dysfunction. The MS nurse will need to develop expert skills in assisting the patient with the management of this symptom.
CHAPTER 4 Management of MS-related symptoms 15
4.3.7 References Andrews KL, Husmann DA. Bladder dysfunction and management in multiple sclerosis. Mayo Clin Proc 1997; 72: 1176–1183.
Avorn J, Monane M, Gurwitz JH et al. Reduction of bacteriuria and pyuria after ingestion of cranberry juice. JAMA 1994; 271: 751–754.
Blaivas JG. Management of bladder dysfunction in multiple sclerosis. Neurology 1980; 30: 12–18.
Giannantoni A, Scivoletto G, Di Stasi SM et al. Urological dysfunction and upper urinary tract involvement in multiple sclerosis patients. Neurourol Urodyn 1998; 17: 89–98.
Halper & Holland, 2011 Comprehensive Nursing Care in Multiple Sclerosis 3rd ed, Springer Publishing Company, New York.
Holland N. Bladder management in multiple sclerosis. MS Management 1994; 1: 7–11.
Irish Medicines Board (1990, revised 2011) summary product characteristics for Urispas http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PA1404-001-001_23022011134024.pdf
Irish Medicines Board (1995, revised 2012) summary product characteristics for Ditropan http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PA0540-146-002_25042012134558.pdf
Irish Medicines Board (2001, revised 2011) summary product characteristics for Detrusitol http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PPA0465-080-001A_27062011113942.pdf
Lee YL, Owens J, Thrupp L, Cesario TC. Does cranberry juice have antibacterial activity? JAMA 2000; 283: 1691.
Moore et al. Multiple sclerosis and bladder dysfunction. British Journal of Neuroscience Nursing 2011; 7(5): 645–654.
MS Trust 2011 Multiple Sclerosis Information for Health and Social Care Professionals, 4th ed. Hertfordshire.
National Institute for Health and Clinical Excellence (NICE) 2006 Urinary Incontinence the management of urinary incontinence in women RCOG Press. Available Online at www.nice.org.uk/nicemedia/live/10996/30281/30281.pdf. Accessed 15th June 2012.
Van den Noort S, Holland NJ. Multiple sclerosis in clinical practice. 2nd edition. New York: Demos Medical Publishing Co. Inc.; 1999.
Walker EB, Barney DP, Mickelsen JN et al. Cranberry concentrate: UTI prophylaxis. J Fam Pract 1997; 45: 167–168.
Zafriri D, Ofek I, Adar R et al. Inhibitory activity of cranberry juice on adherence of type 1 and type P fimbriated Escherichia coli to eucaryotic cells. Antimicrob Agents Chemother 1989; 33: 92–98.
4.3.8 Suggested readingBetts CD, D’Mellow MT, Fowler CJ. Urinary symptoms and the neurological features of bladder dysfunction in multiple sclerosis. J Neurol Neurosurg Psych 1993; 56: 245–250.
Catanzaro M, O’Shaughnessy EJ, Clowers DC, Brooks G. Urinary bladder dysfunction as a remedial disability in multiple sclerosis: a sociologic perspective. Arch Phys Med Rehab 1982; 63: 472–474.
Fowler CJ. Bladder dysfunction in multiple sclerosis: causes and treatments. Int Mult Sclerosis J 1994; 1: 99–107.
Fowler CJ, van Korrebroeck PE, Nordenbo A, Van Poppel H. Treatment of lower urinary tract dysfunction in patients with multiple sclerosis: Committee of the European Study Group of SUDIMS. J Neurol Neurosurg Psych 1992; 55: 986–989.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND16
Halper J, Holland N. Comprehensive nursing care in multiple sclerosis. New York: Demos Vermande; 1997.
Holland NJ. Clinical bulletin: bladder dysfunction in multiple sclerosis. National Multiple Sclerosis Society; 1998.
Kotkin L, Milam DF. Evaluation and management of the urologic consequences of neurologic disease. Tech Urol 1996; 2: 210–219.
Multiple Sclerosis Council for Clinical Practice Guidelines. Urinary dysfunction and multiple sclerosis: evidence-based management strategies for fatigue in multiple sclerosis. Paralyzed Veterans of America; 1998.
Perkash I. Long-term urologic management of the patient with spinal cord injury. Urol Clin North Am 1993; 20: 423–434.
Thompson IM, Lauvetz R. Oxybutynin in bladder spasm, neurogenic bladder and enuresis. Urology 1976; 8: 452–454.
Valiquette G, Herbert J, Meade-D’Alisara P. Desmopressin in the management of nocturia in patients with multiple sclerosis: a double-blind, crossover trial. Arch Neurol 1996; 53: 1270–1275.
Warren JW. Catheter-associated urinary tract infections. Infect Dis Clin North Am 1997; 11: 609–622.
CHAPTER 4 Management of MS-related symptoms 17
4.4 BOWEL DYSFUNCTIONLike bladder dysfunction, bowel dysfunction is common among MS patients (i.e. prevalence approximately 68%). DasGupta et al (2003) cited in MS trust 2011, suggest that bowel problems are under reported and neglected in MS patients.
4.4.1 Learning objectivesAfter completing this section, the reader will be able to:
· Describe the desired outcomes of treatment interventions for bowel dysfunction
· Describe and apply strategies for the assessment of bowel dysfunction
· Implement interventions for the management of constipation and faecal incontinence.
4.4.2 Desired patient outcomesThe patient will be able to discuss and outline the problems they are experiencing with bowel dysfunction. The patient will learn how to manage and cope with their bowel dysfunction. The patient will gain a further understanding of bowel dysfunction as a symptom in MS and the treatments used.
The ideal aim of assessment and intervention will be patient continence, prevention of complications and establishment of a regular bowel pattern.
4.4.3 IntroductionIt should be noted that many individuals with bladder symptoms do not experience bowel problems. Furthermore, bowel dysfunction does not appear to be associated with the degree of disability. However, it is associated with the duration of MS (Chia et al, 1995; Clanet, 1994; Fowler et al, 1996; Hinds et al, 1990).
Neural control of defecation is not as well understood as that of micturition. However, it has been suggested that the pons controls defecation along with influence from spinal cord neural centres and other cortical centres (Hinds et al, 1990).
Neurological control of continent defecation involves sensory messages to the sacral spinal cord and brain; as a result motor impulses reach the anorectum to co-ordinate reflex activity and voluntary relaxation of the anal canal for evacuation. The pathological changes in MS can result in autonomic nerve pathway damage in the spinal cord. This leads to altered colonic motility due to impaired parasympathetic and sympathetic input (MS Trust, 2011).
The two main types of bowel dysfunction in MS are constipation and faecal incontinence.
Constipation is defined as two or fewer bowel movements per week and/or the use of suppositories, laxatives, or enemas more than once per week to promote bowel movements. Constipation occurs in approximately 36–53% of MS patients. Factors that contribute to constipation include certain medications, weakened abdominal muscles, pubococcygeal spasticity, diet, and immobility (Chia et al, 1995; Hinds et al, 1990; MS Trust, 2011; Namey cited in Halper & Holland, 2011; van den Noort 1999).
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND18
Faecal incontinence is defined as the involuntary passage of stool. It occurs in about 25% of patients with MS once per week and 51% of patients less than once a month. Factors contributing to faecal incontinence include constipation that causes rectal distension and overflow, diminished rectal sensation, sphincter dysfunction, certain medications, and diet (Hinds et al, 1990; van den Noort, 1999).
Because of the private nature of issues surrounding bowel function, patients may be embarrassed to share their concerns in this area. However, MS management should always include an assessment of patients’ bowel functioning from initial diagnosis onward.
4.4.4 Nursing assessmentThe MS nurse must first assess the nature of the bowel problem. Due to the private and sensitive nature of bowel function the nurse must strive to provide an open, non-judgemental environment for discussion, which ensures privacy, reassurance and permission from the patient to broach the subject.
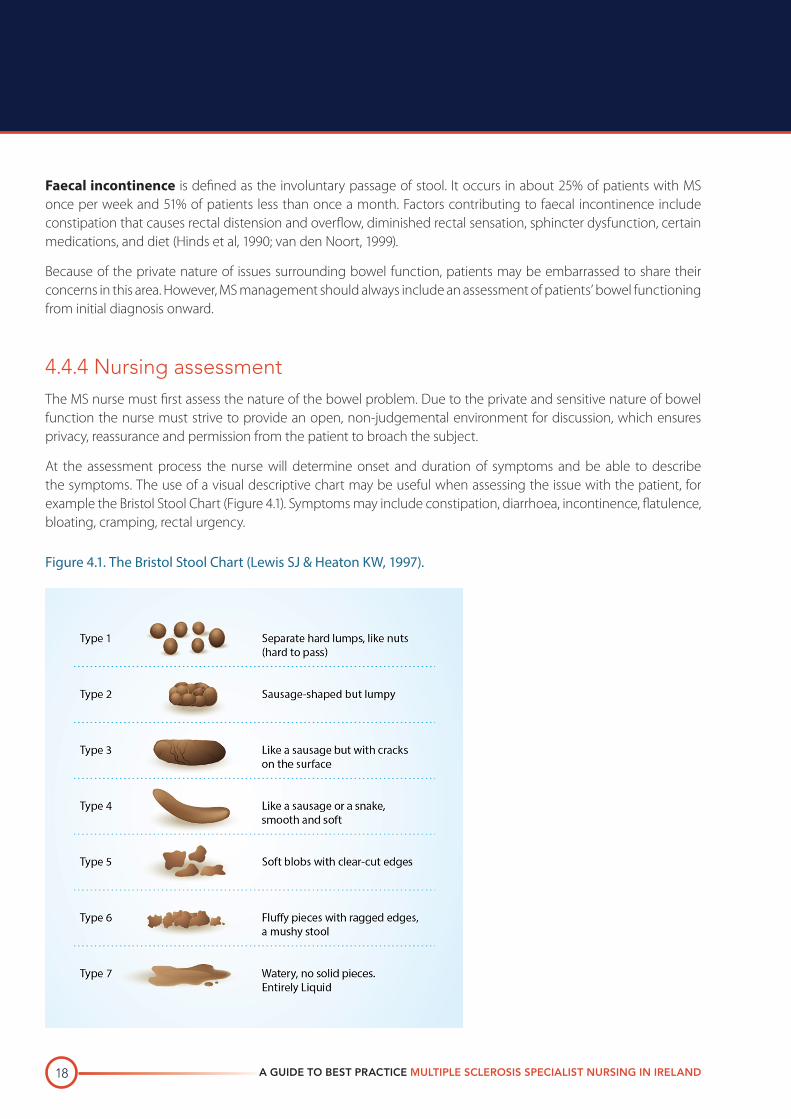
At the assessment process the nurse will determine onset and duration of symptoms and be able to describe the symptoms. The use of a visual descriptive chart may be useful when assessing the issue with the patient, for example the Bristol Stool Chart (Figure 4.1). Symptoms may include constipation, diarrhoea, incontinence, flatulence, bloating, cramping, rectal urgency.
Figure 4.1. The Bristol Stool Chart (Lewis SJ & Heaton KW, 1997).
CHAPTER 4 Management of MS-related symptoms 19
The nurse will identify possible contributing factors to the bowel dysfunction by taking a thorough patient history and being alert to: concurrent medical conditions, medications, reduced mobility, altered nutrition and/or fluid intake.
Similarly to bladder problems, bowel dysfunction can impact several aspects of daily living. The nurse and patient together will investigate the impact of bowel dysfunction on sexual activity, recreational/social activities and employment, quality of life and impact to carer, if applicable.
Secondary complications including haemorrhoids, impaction or bowel obstruction and/or infection should also be assessed.
The nurse will assess the severity of the dysfunction by administering a quality of life scale, e.g. the Bowel Control Scale in: The MSQLI.
The nurse and patient together will identify existing management strategies and coping behaviours used by the patient, and determine the effectiveness of the same.
4.4.5 InterventionsThe nurse will assist the patient to develop a regular bowel routine based on their usual daily activities and plan a regular timeframe for defecation.
Instructing the patient to take advantage of the urge to defecate to ensure regular emptying of the bowels. Making use, for example, of the gastro-colic reflex, which occurs approximately 20 minutes after a meal.
The MS nurse may refer the patient to members of the multidisciplinary team for appropriate assistance.
The dietician: for appropriate advice regarding high fibre diet and adequate fluid intake which both have impact on healthy bowel function.
The physiotherapist: for an activity plan to include regular physical activity to promote bowel function.
The nurse, in consultation with the neurologist, may adjust medication regimes that may be contributing to the bowel dysfunction. The BNF (2011) cite gastro-intestinal disturbances as the primary side effect of Baclofen (anti-spasicity), and constipation is one of the primary side effects of Lyrica (neuropathic pain).
4.4.5.1 Interventions specific to constipation
If the patient’s specific issue is constipation the nurse should, in conjunction with the above, instruct the patient on correct positioning for adequate defecation – the patient should bend forward and elevate knees so that they are higher than hips (a footstool may be required).
In cases of constipation, the physiotherapist can provide biofeedback training. Biofeedback therapy involves retraining muscles to defecate (Bywater & While, 2006) this therapy includes ‘postural re-education and pelvic floor re-education regarding the proper pattern of defecation’ (Leung et al, 2008).
CHAPTER 4 Management of MS-related symptoms 21
4.4.5.2 Interventions specific to faecal incontinence
Faecal incontinence can be difficult for the patient to accept due to the psychosocial implications and burden to the patient and carer.
The nurse will encourage the patient to regularly evacuate the bowels, as part of a bowel management plan that fits around the patient’s daily activities.
The nurse will rule out bowel infection as the cause of the incontinence by performing stool cultures.
Patient education should include; avoiding bowel irritants including alcohol, caffeine, spicy foods and the unnecessary use of antibiotics.
In severe cases the use of anal plugs may be required. A small scale study carried out by Norton & Kamm (2001) found that anal plugs were useful for intractable faecal incontinence, but should be used as a last resort and some patients were unable to tolerate the plugs (Bywater & While, 2006).
For the NICE guideline algorithm on faecal incontinence please see www.nice.org.uk/nicemedia/live/11012/30548/30548.pdf.
Pharmacological interventions for faecal incontinence
NOTE: Nurses should always consult the neurologist before recommending any of the treatments listed in Table 4.4.
Table 4.4. Pharmacological interventions for faecal incontinence.
MEDICATION EXAMPLES OF BRAND
NAMES
DESCRIPTION
Loperamide Imodium® · An antidiarrhoeal agent used as an adjunct in the management of acute diarrhoea, together with appropriate fluid and electrolyte replacement
· Side effects may include skin rash, urticaria, nausea, altered taste, headache, chills, dry mouth, cough, and constipation
See reference list
The nurse’s role, regarding bowel dysfunction must include recognition of any stress and anxiety that may be exacerbating the issue. It also involves the ongoing evaluation of the patient’s management strategies in order to determine their effectiveness, and in conjunction with the patient determine why some strategies may no longer be effective. A new management plan should then be agreed.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND22
4.4.6 References BNF (2011). Available at www.medicinescomplete.com/mc/bnf/current/5336.htm?q=baclofen&t=search&ss=text&p=1#_5336. Accessed on 23/1/12.
Bywater A, While A. Management of bowel dysfunction in people with multiple sclerosis. British Journal of Community Nursing 2006; 11(8): 333–341.
Chia YW, Fowler CJ, Kamm MA et al. Prevalence of bowel dysfunction in patients with multiple sclerosis and bladder dysfunction. J Neurol 1995; 242: 105–108.
Clanet M (chair). The symptoms of multiple sclerosis and their management. In: Proceedings of the MS Forum Modern Management Workshop; April 1992; Paris, France. Worthing UK: Professional Postgraduate Services Europe Ltd.; 1994.
Fowler CJ, Henry MM. Gastrointestinal dysfunction in patients with multiple sclerosis. Semin Neurol 1996; 16: 277–279.
Halper & Holland, 2011 Comprehensive Nursing Care in Multiple Sclerosis. 3rd edition. Springer Publishing Company, New York.
Hinds JP, Eidelman BH, Wald A. Prevalence of bowel dysfunction in multiple sclerosis: a population survey. Gastroenterol 1990; 98: 1538–1542.
Irish Medicines Board (1996, updated 2011) Summary of Product Characterisitics for Movicol [online]. Accessed 15/2/12 at www.imb.ie.
Irish Medicines Board (1977, updated 2009) Summary of Product Characterisitics for Imodium [online]. Accessed 15/2/12 at www.imb.ie.
Irish Medicines Board (1998, revised 2008) summary product characteristics for Celevac http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PA1142-010-001_09122008221639.pdf
Irish Medicines Board (2011, revised 2009) summary product characteristics for Lactulose resolution http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PA1569-001-001_12042011094022.pdf
Irish Medicines Board (1998, revised 2008) summary product characteristics for Microlax http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PA0823-046-001_30052011143019.pdf
Irish Medicines Board (2009) summary product characteristics for Senokot http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PPA1151-113-001_04092009224349.pdf
Leung RWC et al. The efficacy of a multidisciplinary approach to the management of constipation: a case series. J Assoc Charter Physiother Womens Health 2008; 102: 36–44.
Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol 1997; 32(9): 920–924.
MS Trust 2011 Multiple Sclerosis Information for Health and Social Care Professionals, 4th edition. Hertfordshire.
van den Noort S, Holland NJ. Multiple sclerosis in clinical practice. 2nd edition. New York: Demos Medical Publishing Co. Inc.;1999.
CHAPTER 4 Management of MS-related symptoms 23
4.4.7 Suggested reading
Caruana BJ, Wald A, Hinds JP, Eidelman BH. Anorectal sensory and motor function in neurogenic faecal incontinence: comparison between multiple sclerosis and diabetes mellitus. Gastroenterol 1991; 100: 465–470.
Chia YW, Gill KP, Jameson JS et al. Paradoxical puborectalis contraction is a feature of constipation in patients with multiple sclerosis. J Neurol Neurosurg Psych 1996; 60: 31–35.
Hinds JP, Wald A. Colonic and anorectal dysfunction associated with multiple sclerosis. Am J Gastroenterol 1989; 84: 587–595.
Nordenbo AM, Andersen JR, Andersen JT. Disturbances of anorectal function in multiple sclerosis. J Neurol 1996; 243: 445–451.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND24
4.5 PAIN‘Pain is common in people with MS’ (MS Trust, 2011). Pain is defined as an unpleasant sensory and emotional response to a condition caused by actual or potential tissue damage. Estimates of the prevalence of pain in MS vary from 10% to 80% (30– 90% MS Trust 2011), depending on the type of pain experienced.
4.5.1 Learning objectivesAfter completing this section, the reader will be able to:
· Describe the desired outcomes of treatment interventions for acute, subacute, and chronic pain
· Describe and apply strategies for the assessment of pain
· Implement interventions for the management of:
– Acute pain
– Subacute pain
– Chronic neuropathic pain
– Chronic musculoskeletal pain.
4.5.2 Desired patient outcomesThe patient will be able to discuss and outline the problems they are experiencing with pain. The patient will learn how to manage and cope with their pain. The patient will gain a further understanding of pain as a symptom in MS and the treatments used.
The ideal aim of assessment and intervention will be that the patient exhibits improved performance of daily activities as determined by patient self-report and by pain measurement scale, e.g. short form McGill pain questionnaire.
4.5.3 IntroductionMost patients with MS experience chronic pain; acute pain syndromes occur in approximately 10% of patients (Archibald et al, 1994; Clanet, 1994; Moulin, 1996; Moulin, 1988; Moulin et al, 1996; van den Noort & Holland 1999).
Objective assessments of pain are difficult to obtain since pain is a subjective experience that is not always directly related to the degree of injury experienced by the patient. Furthermore, emotional, cognitive, and behavioural responses, as well as psychosocial factors such as expectations, previous pain experiences, and secondary pain, all influence the pain experience (Harden, 1998; Vaney 1996).
CHAPTER 4 Management of MS-related symptoms 25
4.5.4 Cause of pain in MSThe cause of pain in MS depends on whether the pain syndrome is acute, subacute, or chronic.
Acute pain is often characterised by paroxysmal attacks that are brief in duration (i.e. lasting seconds) and occur repeatedly. It results from abnormal axon conduction or a “short circuit” in axon conduction. That is, axonal changes from demyelination cause spontaneous electrical discharges that spread or jump to adjacent fibres (ephaptic transmission). If this impulse spreads to a sensory pathway, it may result in a painful sensation, such as trigeminal neuralgia. Paroxysmal sensations can be provoked by touch, movement, or hyperventilation.
Subacute pain may last days or even weeks. It is caused by demyelination (optic neuritis is the most common) or a secondary source, such as painful bladder spasms associated with a neurogenic bladder and infection or vertebral compression fractures resulting from frequent corticosteroid treatment or prolonged immobility.
Chronic neuropathic or dysaesthetic pain occurs in about one-third of patients with MS; it is believed to be directly related to the demyelination of sensory pathways, particularly those pathways involving the spinothalamic tracts and posterior columns. Chronic musculoskeletal pain, such as backaches and painful leg spasms, usually results from MS-related symptoms rather than the disease itself.
4.5.5 Nursing assessmentThe nurse will assess the nature of the patient’s pain by thorough history taking. To determine the onset, duration, location, severity and patient descriptors, such as burning, stabbing, squeezing, throbbing, etc.
Assess the severity of pain using scales, such as the numerical rating scale (0–10), Short-Form McGill Pain Questionnaire (see Appendix 3) and visual analogue scale.
While taking the patient history the nurse will be alert to possible contributing factors, including relapse, immobility, concurrent illness (e.g. osteoporosis, migraine, disk hernia) and psychosocial issues.
In order to allow adequate and appropriate treatment, the nurse will categorise the pain as acute, subacute or chronic. These categories of pain are sub-divided as follows:
· Acute
– Trigeminal neuralgia
– Tonic seizures
· Subacute
– Optic neuritis
– Steroid-induced compression fractures
– Neural palsies secondary to immobility
· Chronic
– Central neuropathic
– Musculoskeletal (i.e. back and joint pain, painful spasms).
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND26
Pain can greatly impact on many aspects of patient life. During the assessment process the nurse will note the impact of the patient’s pain on daily activities, other MS-related symptoms and psychosocial well-being.
The nurse and patient together will identify existing management strategies and coping behaviours used by the patient, and determine the effectiveness of same.
4.5.6 InterventionsThe nurse must acknowledge and validate the patient’s pain experience and provide ongoing evaluation of pain management strategies for the specific pain category.
4.5.6.1 Specific interventions for acute pain
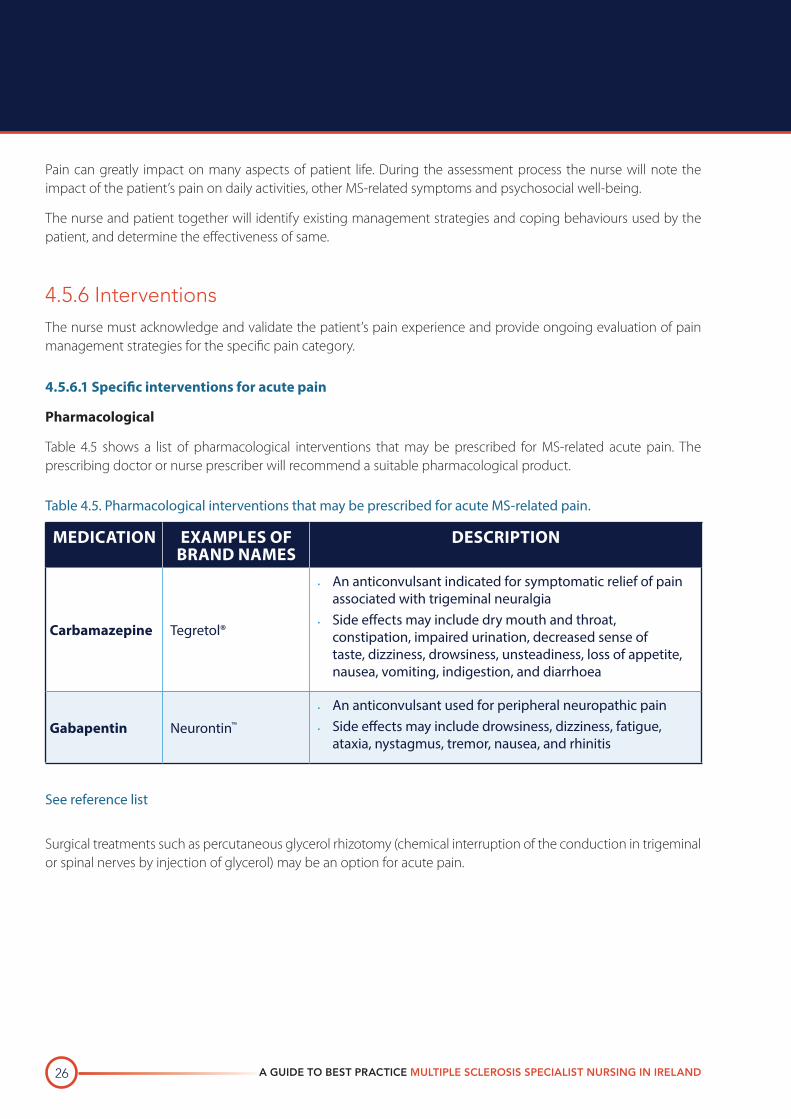
Pharmacological
Table 4.5 shows a list of pharmacological interventions that may be prescribed for MS-related acute pain. The prescribing doctor or nurse prescriber will recommend a suitable pharmacological product.
Table 4.5. Pharmacological interventions that may be prescribed for acute MS-related pain.
MEDICATION EXAMPLES OF BRAND NAMES
DESCRIPTION
Carbamazepine Tegretol®
· An anticonvulsant indicated for symptomatic relief of pain associated with trigeminal neuralgia
· Side effects may include dry mouth and throat, constipation, impaired urination, decreased sense of taste, dizziness, drowsiness, unsteadiness, loss of appetite, nausea, vomiting, indigestion, and diarrhoea
Gabapentin Neurontin™
· An anticonvulsant used for peripheral neuropathic pain
· Side effects may include drowsiness, dizziness, fatigue, ataxia, nystagmus, tremor, nausea, and rhinitis
See reference list
Surgical treatments such as percutaneous glycerol rhizotomy (chemical interruption of the conduction in trigeminal or spinal nerves by injection of glycerol) may be an option for acute pain.
CHAPTER 4 Management of MS-related symptoms 27
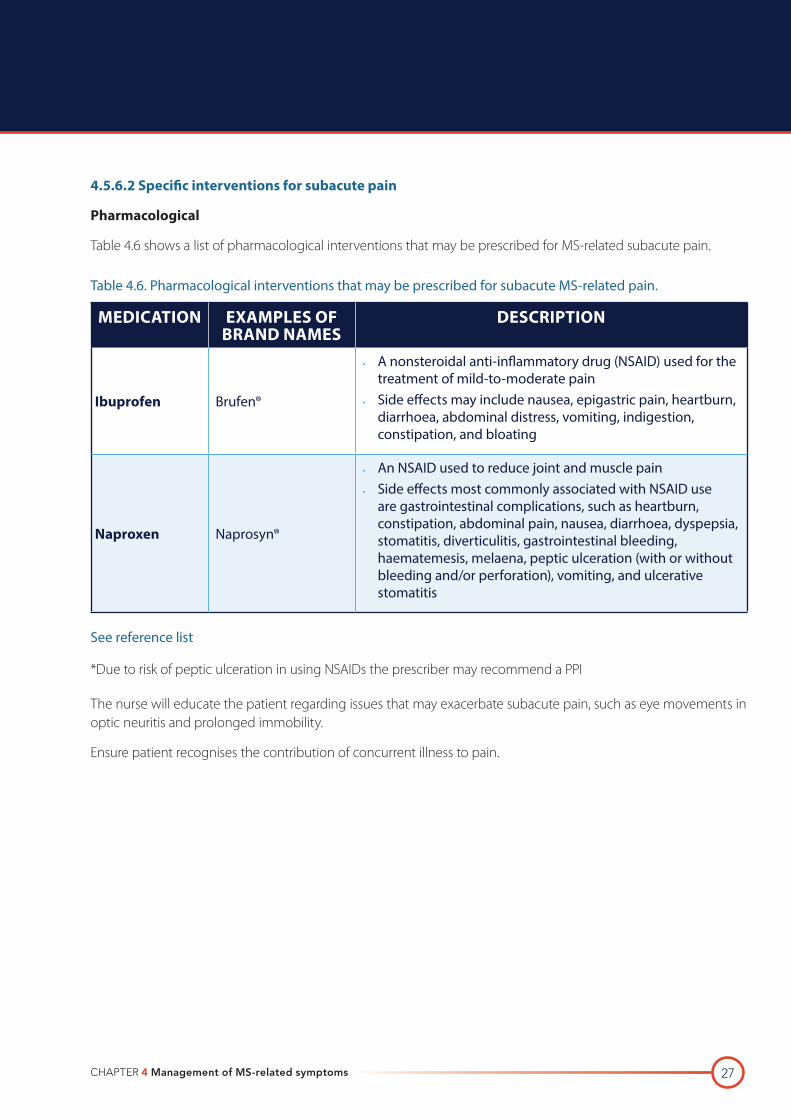
4.5.6.2 Specific interventions for subacute pain
Pharmacological
Table 4.6 shows a list of pharmacological interventions that may be prescribed for MS-related subacute pain.
Table 4.6. Pharmacological interventions that may be prescribed for subacute MS-related pain.
MEDICATION EXAMPLES OF BRAND NAMES
DESCRIPTION
Ibuprofen Brufen®
· A nonsteroidal anti-inflammatory drug (NSAID) used for the treatment of mild-to-moderate pain
· Side effects may include nausea, epigastric pain, heartburn, diarrhoea, abdominal distress, vomiting, indigestion, constipation, and bloating
Naproxen Naprosyn®
· An NSAID used to reduce joint and muscle pain
· Side effects most commonly associated with NSAID use are gastrointestinal complications, such as heartburn, constipation, abdominal pain, nausea, diarrhoea, dyspepsia, stomatitis, diverticulitis, gastrointestinal bleeding, haematemesis, melaena, peptic ulceration (with or without bleeding and/or perforation), vomiting, and ulcerative stomatitis
See reference list
*Due to risk of peptic ulceration in using NSAIDs the prescriber may recommend a PPI
The nurse will educate the patient regarding issues that may exacerbate subacute pain, such as eye movements in optic neuritis and prolonged immobility.
Ensure patient recognises the contribution of concurrent illness to pain.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND28
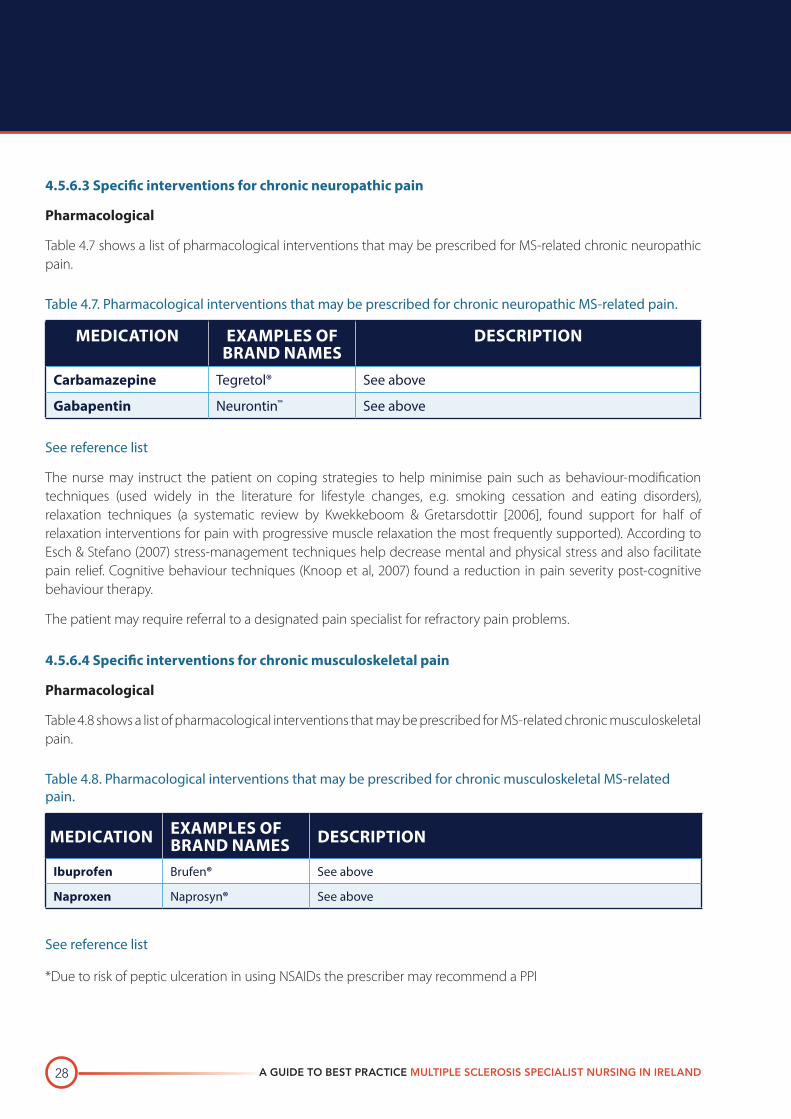
4.5.6.3 Specific interventions for chronic neuropathic pain
Pharmacological
Table 4.7 shows a list of pharmacological interventions that may be prescribed for MS-related chronic neuropathic pain.
Table 4.7. Pharmacological interventions that may be prescribed for chronic neuropathic MS-related pain.
MEDICATION EXAMPLES OF BRAND NAMES
DESCRIPTION
Carbamazepine Tegretol® See above
Gabapentin Neurontin™ See above
See reference list
The nurse may instruct the patient on coping strategies to help minimise pain such as behaviour-modification techniques (used widely in the literature for lifestyle changes, e.g. smoking cessation and eating disorders), relaxation techniques (a systematic review by Kwekkeboom & Gretarsdottir [2006], found support for half of relaxation interventions for pain with progressive muscle relaxation the most frequently supported). According to Esch & Stefano (2007) stress-management techniques help decrease mental and physical stress and also facilitate pain relief. Cognitive behaviour techniques (Knoop et al, 2007) found a reduction in pain severity post-cognitive behaviour therapy.
The patient may require referral to a designated pain specialist for refractory pain problems.
4.5.6.4 Specific interventions for chronic musculoskeletal pain
Pharmacological
Table 4.8 shows a list of pharmacological interventions that may be prescribed for MS-related chronic musculoskeletal pain.
Table 4.8. Pharmacological interventions that may be prescribed for chronic musculoskeletal MS-related pain.
MEDICATION EXAMPLES OF BRAND NAMES DESCRIPTION
Ibuprofen Brufen® See above
Naproxen Naprosyn® See above
See reference list
*Due to risk of peptic ulceration in using NSAIDs the prescriber may recommend a PPI

CHAPTER 4 Management of MS-related symptoms 29
The nurse may refer the patient to a physiotherapist and/or occupational therapist for assessment and rehabilitation interventions, such as exercise programmes. Smith & Grimmer-Somers (2010) highlight benefits from exercise programmes for chronic back pain.
The nurse should be aware of complimentary therapies that may assist the patient in the management of their pain. Gunnarsdottir & Peden-McAlpine (2010) found that reflexology had the potential to decrease the pain experience of women with fibromyalgia. Fox et al (2011) state that meditation improves outcomes in several types of pain.
The nurse’s role, regarding pain must include ongoing evaluation of the patient’s management strategies, to ensure they are effective and if not, investigate the reasons in conjunction with the patient and develop an alternative plan.
4.5.7 References
Archibald CJ, McGrath PJ, Ritvo PG et al. Pain prevalence, severity, and impact in a clinic sample of multiple sclerosis patients. Pain 1994; 58: 89–93.
Clanet M (chair). The symptoms of multiple sclerosis and their management. In: Proceedings of the MS Forum Modern Management Workshop; April 1992; Paris, France. Worthing UK: Professional Postgraduate Services Europe Ltd.; 1994.
Esch T, Stefano GB. A bio-psycho-social-molecular approach to pain and stress management. Forsch Komplementmed 2007; 14(4): 224–234.
Fox et al. Mindfulness meditation for women with chronic pelvic pain: a pilot study. Journal of Reproductive Medicine 2011. 56(3–4): 158–162.
Gunnarsdottir T J, Peden-McAlpine C. Effects of reflexology on fibromyalgia symptoms: a multiple case study. Complementary Therapies in Clinical Practice 2010.
Harden RN, Cole PA. New developments in rehabilitation of neuropathic pain syndromes: interdisciplinary team approach. Neurol Clin 1998; 16: 937–950.
Irish Medicines Board (2006, updated 2011) Summary of Product Characterisitics for Neurontin [online] Accessed 15/2/12 at www.imb.ie.
Irish Medicines Board (1979, revised 2012) summary product characteristics for Tegretol http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PA0013-081-002_14052012134307.pdf
Irish Medicines Board (1975, revised 2011) summary product characteristics for Brufen http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PA0038-080-002_03042012105128.pdf
Irish Medicines Board (1990, revised 2011) summary product characteristics for Naprosyn http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PA0050-128-006_13052011142116.pdf
Knoop H et al. Is cognitive behaviour therapy for chronic fatigue syndrome also effective for pain symptoms? Behaviour Research and Therapy 2007; 45: 2034–2043.
Kwekkeboom KL, Gretarsdottir E. Systematic review of relaxation interventions for pain. Journal of Nursing Scholarship 2006; 38(3)L 269–277.
Moulin DE, Foley KM, Ebers GC. Pain syndromes in multiple sclerosis. Neurology 1988; 38: 1830–1834.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND30
Moulin DE. Pain assessment and management in multiple sclerosis. Int Mult Sclerosis J 1996; 3: 59–63.
Moulin DE, Iezzi A, Amireh R et al. Randomised trial of oral morphine for chronic non-cancer pain. Lancet 1996; 347: 143–147.
MS Trust 2011. Multiple Sclerosis Information for Health and Social Care Professionals, 4th ed. Hertfordshire.
Smith C, Grimmer-Somers K. The treatment effect of exercise programmes for chronic low back pain. Journal of Evaluation in Clinical Practice 2010; 16: 484–491.
Van den Noort S, Holland NJ. Multiple sclerosis in clinical practice. 2nd edition. New York: Demos Medical Publishing Co. Inc.;1999.
Vaney C. Understanding pain mechanisms in multiple sclerosis. MS Management 1996; 3: 11–18.
4.5.8 Suggested reading
Beckonja MM, Galer BS. Pain assessment and evaluation of patients who have neuropathic pain. Neurol Clin 1998; 16: 775–790.
Beric A. Central pain and dysesthesia syndrome. Neurol Clin 1998; 16: 899–918.
Dellemijn P. Are opioids effective in relieving neuropathic pain? Pain 1999; 80: 453–462.
Halper J, Holland N. Comprehensive nursing care in multiple sclerosis. New York: Demos Vermande; 1997.
Khan OA. Gabapentin relieves trigeminal neuralgia in multiple sclerosis patients. Neurology 1998; 51: 611–614.
Krames ES. Interventional pain management: appropriate when less invasive therapies fail to provide adequate analgesia. Med Clin North Am 1999; 83: 787–808.
MacQuay HJ, Tramer M, Nye BA et al. A systematic review of antidepressants in neuropathic pain. Pain 1996; 68: 217–227.
Melzack R. The short-form McGill Pain Questionnaire. Pain 1987; 30: 191–197.
Moulin DE. Pain in central and peripheral demyelinating disorders. Neurol Clin 1998; 16: 889–898.
Samkoff LM, Daras M, Tuchman AJ, Koppel BS. Amelioration of refractory dysesthetic limb pain in multiple sclerosis by gabapentin. Neurology 1997; 49: 304–305.
Warnell P. The pain experience of a multiple sclerosis population: a descriptive study. Axon 1991; 13: 26–28.
CHAPTER 4 Management of MS-related symptoms 31
4.6 SPASTICITY‘Spasticity or muscle hypertonia occurs as a result of abnormal spinal and brain stem reflexes’ (Harris cited in Halper & Holland, 2011). Spasticity is a common MS-related symptom. The EU-SPASM group’s definition of spasticity is ‘disordered sensorimotor control, resulting from an upper motor neurone lesion, presenting as intermittent or sustained involuntary activation of muscles’ (Stevenson & Jarrett [ed], 2006).
4.6.1 Learning objectivesAfter completing this section, the reader will be able to:
· Describe the desired outcomes of treatment interventions for spasticity
· Describe and apply strategies for the assessment of spasticity
· Implement interventions for the management of spasticity.
4.6.2 Desired patient outcomesThat the patient will be able to discuss and outline the problems they are experiencing with spasticity. The patient will learn management and safety strategies to deal with their spasticity. The patient will experience a reduction in spasms as demonstrated by patient self-report, improvements in Ashworth scale scores and improvements in Spasm frequency scale score.
4.6.3 IntroductionSpasticity can be both phasic (spasms) and tonic (constant stiffness). O’Connor (2009; cited in Halper & Holland, 2011) states that spasticity is more likely to occur in larger stronger muscles, those involved in upright posture and/or moving against gravity.
The muscle groups that are most likely to develop spasticity are the quadriceps, adductors of hips, hamstrings, and gastrocnemius muscles (van den Noort & Holland, 1999).
Mild spasticity is generally treated through passive stretching of the affected limb. Severe spasticity may require medication and surgical interventions, such as motor-point blocks, botulinum toxin injections, insertion of an intrathecal baclofen pump, and in extreme circumstances further surgical management (e.g. tendon release), in addition to stretching exercises. Severe spasticity, which is most often noted in individuals with restricted mobility, can lead to skin breakdown, seating problems, contractures, and pain (Shapiro, 1998).
There are two principles of management for spasticity: 1) optimizing individual’s posture and movement 2) Preventing or managing factors that may increase spasticity and spasms (MS Trust, 2011). Nurses, physiotherapists and occupational therapists play a key role in the treatment and management of spasticity (MS Trust, 2011).
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND32
4.6.4 Nursing assessmentThe MS nurse will determine the location, onset and duration of the spasticity and describe the symptoms, which may include stiffness, weakness, flexor or extensor spasms, clonus and pain.
The nurse will, in conjunction with the patient, identify possible contributing factors to spasticity, such as relapse, infection, strs, anxiety, constipation, bladder dysfunction, altered skin integrity and medications.
The nurse will assess the impact of spasticity on various aspects of daily living, such as seating, gait, comfort, energy level, sexual activity, hygiene and sleep.
The severity of the spasticity must be assessed by a competent practitioner, by use of the Modified Ashworth Scale, which measures tone intensity, although Stevenson & Jarrett (ed) 2006 suggest that its reliability may be problematic, the Spasm frequency Scale is used to measure spasm frequency and the Clonus and spasms score, used to measure frequency and provocation of both spasm and clonus (Stevenson & Jarrett [ed), 2006).
Spasticity can greatly impact on many aspects of patient life. During the assessment process the nurse will note the impact of the patient’s spasticity on daily activities, other MS-related symptoms and psychosocial well-being.
The nurse and patient together will identify existing management strategies and coping behaviours used by the patient, and determine the effectiveness of same. Alternative strategies will be collaboratively developed as the need arises.
4.6.5 Interventions
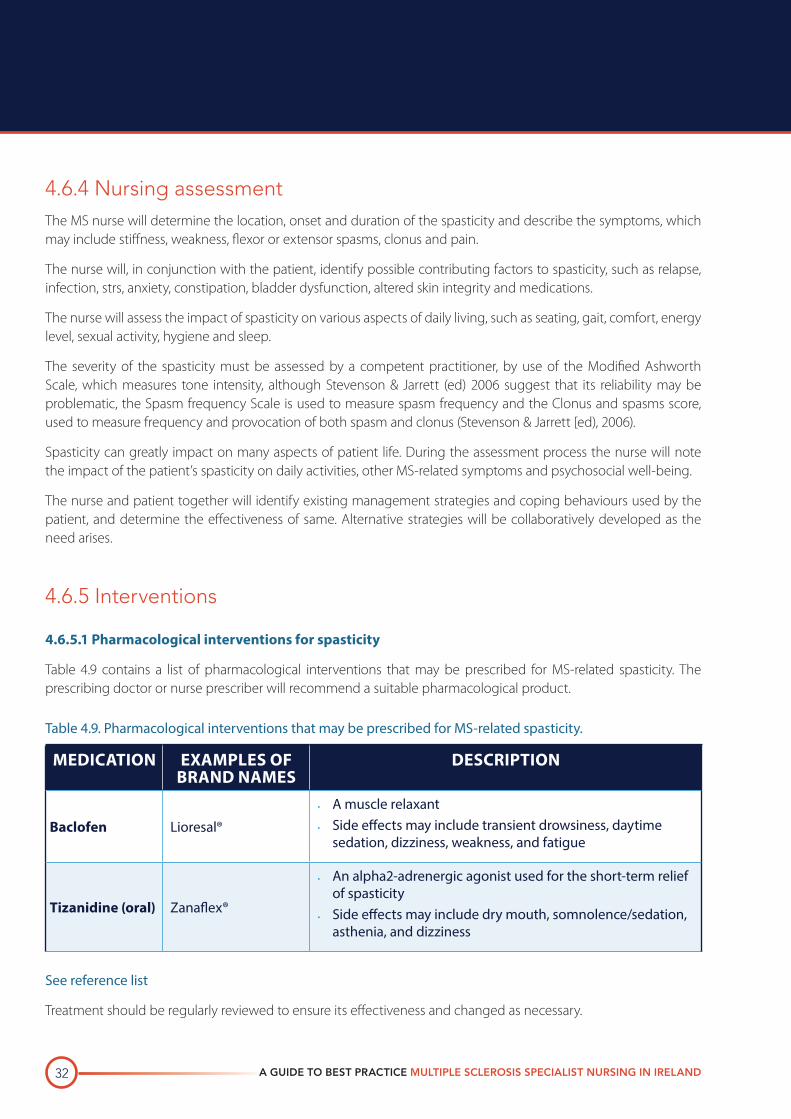
4.6.5.1 Pharmacological interventions for spasticity
Table 4.9 contains a list of pharmacological interventions that may be prescribed for MS-related spasticity. The prescribing doctor or nurse prescriber will recommend a suitable pharmacological product.
Table 4.9. Pharmacological interventions that may be prescribed for MS-related spasticity.
MEDICATION EXAMPLES OF BRAND NAMES
DESCRIPTION
Baclofen Lioresal®· A muscle relaxant
· Side effects may include transient drowsiness, daytime sedation, dizziness, weakness, and fatigue
Tizanidine (oral) Zanaflex®
· An alpha2-adrenergic agonist used for the short-term relief of spasticity
· Side effects may include dry mouth, somnolence/sedation, asthenia, and dizziness
See reference list
Treatment should be regularly reviewed to ensure its effectiveness and changed as necessary.
CHAPTER 4 Management of MS-related symptoms 33
4.6.5.2 Non-pharmacological interventions
The nurse may refer the patient to a physiotherapist and/or occupational therapist for exercise programmes, assistive devices and seating modification to aid with the management of spasticity. For useful algorithms in spasticity please see: Walton: A practical approach to spasticity management in people with multiple sclerosis (British Journal of Neuroscience Nursing 2011; 7[4], p. 589).
A variety of other treatment options may be required depending on the severity of spasticity and response to previous treatments. Injection of botulinum toxin (Botox®), injection of phenol, and intrathecal baclofen pump, all of which are recommended by NICE guidelines, however botulinum should not be used routinely but in the case of localised hypertonia or spasticity, which is not responding to other treatments (NICE, 2003).
The nurse’s role, regarding spasticity must include ongoing evaluation of the patient’s management strategies, to ensure they are effective and if not, investigate the reasons in conjunction with the patient.
4.6.6 References
Halper & Holland, 2011 Comprehensive Nursing Care in Multiple Sclerosis 3rd ed, Springer Publishing Company, New York.
Irish Medicines Board (1994, revised 2011) summary product characteristics for Lioresal http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PPA0465-054-001A_22122011134040.pdf
Irish Medicines Board (2006, revised 2012) summary product characteristics for Zanaflex http://www.imb.ie/images/uploaded/swedocuments/LicenseSPC_PPA0465-168-001_13042012143059.pdf
MS Trust 2011 Multiple Sclerosis Information for Health and Social Care Professionals, 4th ed. Hertfordshire.
National Institute for Health and Clinical Excellence (NICE) 2003. Multiple sclerosis: management of multiple sclerosis in primary and secondary care. Accessed online at http://publications.nice.org.uk/multiple-sclerosis-cg8/guidance#managing-specific-impairments. Available 14 June 2012.
Shapiro RT. Symptom management in multiple sclerosis. 3rd edition. New York: Demos Medical Publishing Co. Inc.; 1998.
Stevenson V & Jarrett L (ed) (2006) Spasticity Management. Informa Healthcare, Oxon, UK.
Van den Noort S, Holland NJ. Multiple sclerosis in clinical practice. 2nd edition. New York: Demos Medical Publishing Co. Inc.;1999.
4.6.7 Suggested reading
Currie R. Spasticity: a common symptom of multiple sclerosis. Nursing Standard 2001; 15(33): 47–52.
Dunevsky A, Perel AB. Gabapentin for relief of spasticity associated with multiple sclerosis. Am J Phys Med Rehab 1998; 77: 451–454.
Jarrett L, Leary SM, Porter B et al. Managing spasticity in people with multiple sclerosis: a goal orientated approach to intrathecal baclofen therapy. Int J MS Care 2001; 3(4): 10–21.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND34
Jarrett L, Nandi P, Thompson A. Managing lower limb spasticity in multiple sclerosis: does intrathecal baclofen have a role? Journal of Neurology, Neurosurgery and Neuropsychiatry 2002; 73(6): 705–709.
Khan OA, Olek MJ. Clonidine in the treatment of spasticity in patients with multiple sclerosis [letter]. J Neurol 1995; 242: 712–713.
Leary S, Jarrett L, Porter B et al. A multidisciplinary, goal-orientated approach to intrathecal baclofen therapy in progressive neurological disease. Journal of Neurology, Neurosurgery and Psychiatry 2000; 69: 412–413.
Porter B. A review of intrathecal baclofen in the management of spasticity. Br J Nursing 1997; 6(5): 253–260.
Smith C, Birnbaum G, Carter JL et al. Tizanidine treatment of spasticity caused by multiple sclerosis: results of a double-blind, placebo-controlled trial. US Tizanidine Study Group. Neurology 1994; 44(suppl 9): S34–S43.
Smith PF, Darlington CL. Recent developments in drug therapy for multiple sclerosis. Mult Scler 1999; 5: 110–120.
United Kingdom Tizanidine Trial Group. A double-blind, placebo-controlled trial of tizanidine in the treatment of spasticity caused by multiple sclerosis. Neurology 1994; 44(suppl 9): S70–S78.
Ward N. Spasticity in multiple sclerosis. J Community Nursing 1999; 13(7): 4–10.
CHAPTER 4 Management of MS-related symptoms 35
4.7 TREMOR
4.7.1 Preface‘Tremor is a complex movement disorder characterized by involuntary uncontrolled movements’ (MS Trust, 2011). Tremor in MS can affect the limbs, trunk, or speech. It is often the most disabling symptom because it is frustrating for patients and difficult to treat. Even a mild tremor can make simple tasks difficult to perform.
4.7.2 Learning objectivesAfter completing this section, the reader will be able to:
· Describe the desired outcomes of treatment interventions for tremor
· Describe and apply strategies for the assessment of tremor
· Implement interventions for the management of tremor.
4.7.3 Desired patient outcomesThe patient will be able discuss and outline the problems they are experiencing with their tremor. The patient will learn to manage their tremor effectively by adhering to rehabilitative and pharmacologic treatments regimes to reduce and compensate for tremors. The patient will experience a reduction in the tremor as demonstrated by improvement in spiral test scores, nine-hole peg test scores and improvement in daily activities.
4.7.4 IntroductionTremor is generally classified as either postural, intention, or rest tremor (Van den Noort 1999; Clanet 1994; Shapiro 1998).
Intention tremor (also known as action, goal-directed, or hyperkinetic tremor) is associated with voluntary movement. ‘Approximately 25% of people with MS experience upper-limb intention tremor, which limits their ability to participate in daily activities’ (Hawes et al 2010) The amplitude of the tremor increases as the patient reaches nearer to the target (e.g., when reaching for a cup). It can also increase the more the patient tries to be accurate. This tremor may range from mild to severe in nature and is the most common type of tremor seen in MS.
Postural (or attitudinal) tremor occurs whilst voluntarily maintaining a position against gravity (Feyes et al 2004). It can occur during a sustained position, such as with outstretched arms or when legs are crossed. This type of tremor is common in patients with MS and may include titubation of the head and neck that requires support.
Rest tremor occurs when the patient is relaxed or at rest. Most often seen in Parkinson’s disease, rest tremor may occasionally be seen in individuals with MS who have a demyelinating lesion within or near the substantia nigra or nigrostriatal tract. In general, however, rest tremor is rare in MS.
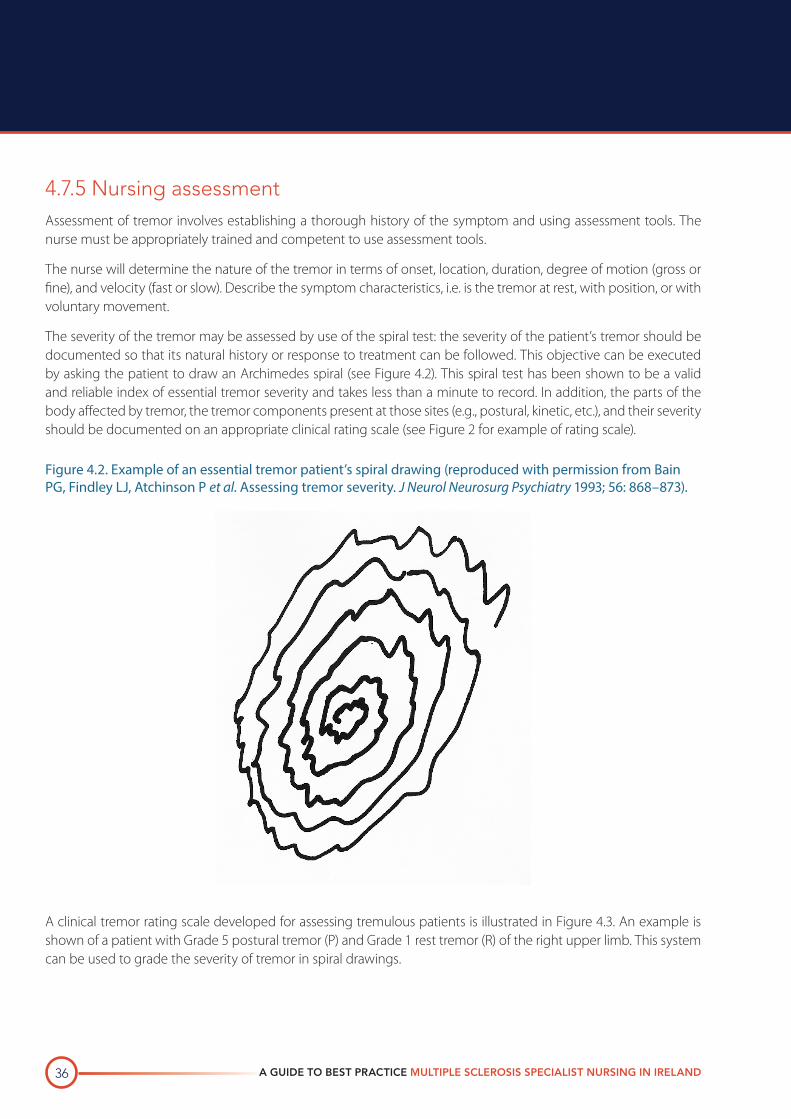
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND36
4.7.5 Nursing assessmentAssessment of tremor involves establishing a thorough history of the symptom and using assessment tools. The nurse must be appropriately trained and competent to use assessment tools.
The nurse will determine the nature of the tremor in terms of onset, location, duration, degree of motion (gross or fine), and velocity (fast or slow). Describe the symptom characteristics, i.e. is the tremor at rest, with position, or with voluntary movement.
The severity of the tremor may be assessed by use of the spiral test: the severity of the patient’s tremor should be documented so that its natural history or response to treatment can be followed. This objective can be executed by asking the patient to draw an Archimedes spiral (see Figure 4.2). This spiral test has been shown to be a valid and reliable index of essential tremor severity and takes less than a minute to record. In addition, the parts of the body affected by tremor, the tremor components present at those sites (e.g., postural, kinetic, etc.), and their severity should be documented on an appropriate clinical rating scale (see Figure 2 for example of rating scale).
Figure 4.2. Example of an essential tremor patient’s spiral drawing (reproduced with permission from Bain PG, Findley LJ, Atchinson P et al. Assessing tremor severity. J Neurol Neurosurg Psychiatry 1993; 56: 868–873).
A clinical tremor rating scale developed for assessing tremulous patients is illustrated in Figure 4.3. An example is shown of a patient with Grade 5 postural tremor (P) and Grade 1 rest tremor (R) of the right upper limb. This system can be used to grade the severity of tremor in spiral drawings.
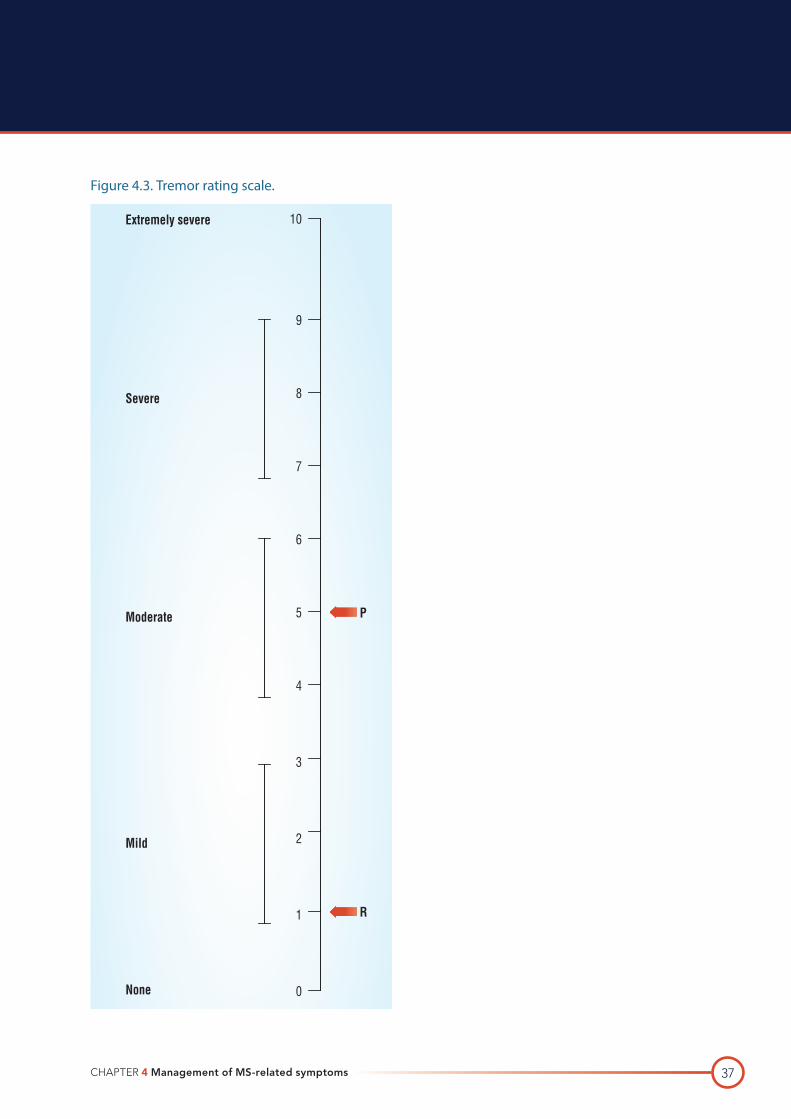
CHAPTER 4 Management of MS-related symptoms 37
Figure 4.3. Tremor rating scale.
10
9
8
7
6
5
4
3
2
1
0
Extremely severe
Severe
Moderate P
R
None
Mild
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND38
Other scales include the Nine-hole peg test and 0–10 Tremor Severity Scale (MS Trust, 2011). Hooper et al (1998) state that the utility and reliability of the The Fahn Tremor Rating is evidently high.
The nurse will identify possible contributing factors to tremor, in conjunction with the patient, such as lifestyle issues (e.g. alcoholism, caffeine) and categorise the tremor. The three categories include intention tremor (tremor with voluntary movement), postural tremor (tremor with certain positioning) and rest tremor (tremor without voluntary movement).
Tremor can greatly impact on many aspects of patient life. During the assessment process the nurse will note the impact of the patient’s tremor on daily activities, and other MS-related symptoms and psychosocial well-being.
The nurse and patient together will identify existing management strategies and coping behaviours used by the patient, and determine the effectiveness of same.
4.7.6 InterventionsSurgical treatments (for severe cases) include stereotactic thalamotomy and unilateral thalamotomy. According to Zirh et al (1999) unilateral thalamotomy is an effective, safe procedure for the treatment of essential tremor. Similarly Thevathasan et al (2011) state that tremor often permanently improves during thalamic stimulation.
The nurse may need to approach the issue of possible loss of the adult role. Patients with tremor may no longer be able to perform normal adult activities, such as feeding or grooming themselves. In fact, patients often rate the inability to feed themselves as the worst consequence of tremor (women also rate the inability to groom themselves as one of the worst consequences).
Referral to a physiotherapist and/or occupational therapist may be useful for instruction on activities to help manage tremor such as patterning (i.e. tracing and repeating basic movement patterns until they become automatic), weighting, robotic aids, e.g., Handy 1 Robotic Aid.
The nurse’s role, regarding tremor must include ongoing evaluation of the patient’s management strategies, to ensure they are effective and if not, investigate the reasons in conjunction with the patient.
4.7.7 References
Bain PG, Findley LJ, Atchinson P et al. Assessing tremor severity. J Neurol Neurosurg Psychiatry 1993; 56: 868–873.
Bain PG, Findley LJ. Assessing tremor severity. London: Smith-Gordon, 1993.
Clanet M (chair). The symptoms of multiple sclerosis and their management. In: Proceedings of the MS Forum Modern Management Workshop; April 1992; Paris, France. Worthing UK: Professional Postgraduate Services Europe Ltd.; 1994.
Feys et al. Effects of vision and arm position on amplitude of arm postural tremor in patients with multiple sclerosis. Physical Medicine and Rehabilitation 2004; 85: 1031–1033.
Hawes et al. Interventions for upper limb intention tremor in multiple sclerosis International Journal of MS Care 2010; 12(3): 122–132.
CHAPTER 4 Management of MS-related symptoms 39
Hooper et al. Rater reliabiltity of Fahn’s tremor rating scale in patients with multiple sclerosis. Physical Medicine and Rehabilitation 1998; 79: 1076–1079.
MS Trust 2011 Multiple Sclerosis Information for Health and Social Care Professionals. 4th edition. Hertfordshire.
Shapiro RT. Symptom management in multiple sclerosis. 3rd ed. New York: Demos Medical Publishing Co. Inc.; 1998.
Thevathasan W et al. Permanent tremor reduction during thalamic stimulation in multiple sclerosis. Journal of Neurology, Neurosurgery and Psychiatry 2011; 82: 419–422. van den Noort S, Holland NJ. Multiple sclerosis in clinical practice. 2nd edition. New York: Demos Medical Publishing Co. Inc.;1999. Zirh A et al. Stereotactic thalamotomy in the treatment of essential tremor of the upper extremity: reassessment including a blinded measure of outcome. Journal of Neurology, Neurosurgery and Psychiatry 1999; 66: 772–775.
4.7.8 Suggested reading
Alushi SH, Worthington J, Glickman S, Bain PG. A study of tremor in multiple sclerosis. Brain 2001; 124: 720–730.
Cooper IS. Relief of intention tremor of multiple sclerosis by thalamic surgery. JAMA 1967; 199: 689–694.
Critchley GR, Richardson PL. Vim thalamotomy for the relief of intention tremor of multiple sclerosis. British Journal of Neurology 1998; 12(6): 559–562.
Duquette P, Pleines J, du Souich P. Isoniazid for tremor in multiple sclerosis [letter]. J Neurol Neurosurg Psych 1985; 48: 957.
Duquette P, Pleines J, du Souich P. Isoniazid for tremor in multiple sclerosis: a controlled trial. Neurology 1985; 35: 1772–1775.
Freeman R, Miyawaki E. The treatment of autonomic dysfunction. J Clin Neurophysiol 1993; 10: 61–82.
Hallett M. Isoniazid and action tremor in multiple sclerosis [letter]. J Neurol Neurosurg Psych 1985; 48: 957.
Hallett M, Lindsey JW, Adelstein BD, Riley PO. Controlled trial of isoniazid therapy for severe postural cerebellar tremor in multiple sclerosis. Neurology 1985; 35: 1374–1377.
Paty DW, Ebers GC. Multiple sclerosis. Philadelphia: F.A. Davis Company; 1998.
Sabra AF, Hallett M, Sudarsky L, Mullally W. Treatment of action tremor in multiple sclerosis with isoniazid. Neurology 1982; 32: 912–913.]
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND40
4.8 ALTERED MOBILITYMobility is defined as the ability to change and control body position. From a basic functional aspect this includes getting in and out of bed, transferring from a bed to a chair and walking to and from the toilet. Symptoms that contribute to altered mobility in MS include spasticity, tremor, ataxia, weakness, loss of balance, pain, fatigue, dizziness, and vertigo. ‘Within 10 to 15 years of disease onset, 80 percent of per sons with MS experience gait problems due to muscle weakness or spasticity, fatigue, and balance impairments’ (Souza et al, 2010).
4.8.1 Learning objectivesAfter completing this section, the reader will be able to:
· Describe the desired outcomes of treatment interventions for altered mobility
· Describe and apply strategies for the assessment of mobility
· Implement interventions for the management of altered mobility.
4.8.2 Desired patient outcomesThe patient will be able to discuss their altered mobility in terms of causes and risks.
The patient will maintain a safe level of activity, as demonstrated by a reduction in the number of falls and complications. The patient will demonstrate improved mobility by becoming increasingly involved in activities requiring mobility.
4.8.3 IntroductionThe factors contributing to altered mobility vary from patient to patient. Proper diagnosis of these factors is therefore necessary before appropriate treatment interventions can be initiated. The main objective of interventions for altered mobility is to ensure that the patient remains as independent as possible in a safe and appropriate manner.
4.8.4 Nursing assessmentThe nurse will determine the nature of the mobility alteration in terms of onset, duration and describe the symptom characteristics of altered mobility such as loss of balance, tripping, falling, inability to transfer, inability to walk. Decreased mobility can led to an increase risk of the development of pressure areas and so, if appropriate the CNSp may include the assessment of the patients pressure area by use of the Waterlow scale (see Appendix 4).
The severity of altered mobility can be assessed by use of the Timed walk for 100 m and the Kurtzke Expanded Disability Status Scale (EDSS) for ambulation (see Table 4.11).
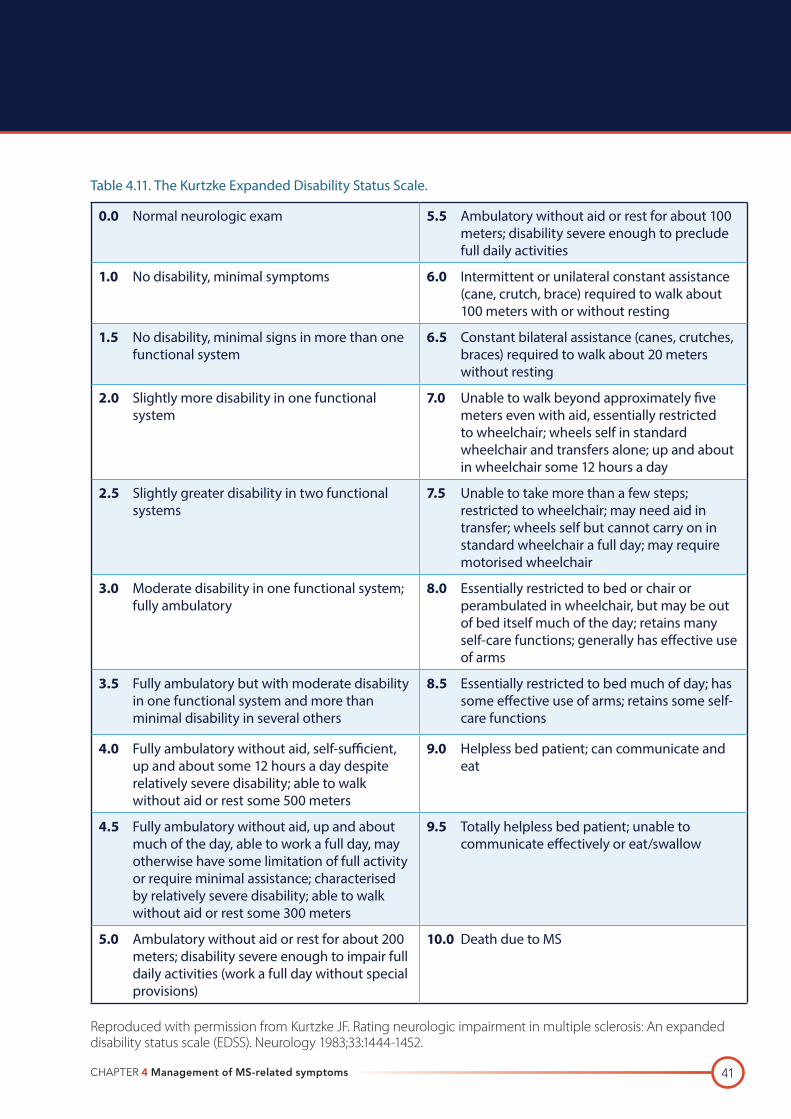
CHAPTER 4 Management of MS-related symptoms 41
Table 4.11. The Kurtzke Expanded Disability Status Scale.
0.0 Normal neurologic exam 5.5 Ambulatory without aid or rest for about 100 meters; disability severe enough to preclude full daily activities
1.0 No disability, minimal symptoms 6.0 Intermittent or unilateral constant assistance (cane, crutch, brace) required to walk about 100 meters with or without resting
1.5 No disability, minimal signs in more than one functional system
6.5 Constant bilateral assistance (canes, crutches, braces) required to walk about 20 meters without resting
2.0 Slightly more disability in one functional system
7.0 Unable to walk beyond approximately five meters even with aid, essentially restricted to wheelchair; wheels self in standard wheelchair and transfers alone; up and about in wheelchair some 12 hours a day
2.5 Slightly greater disability in two functional systems
7.5 Unable to take more than a few steps; restricted to wheelchair; may need aid in transfer; wheels self but cannot carry on in standard wheelchair a full day; may require motorised wheelchair
3.0 Moderate disability in one functional system; fully ambulatory
8.0 Essentially restricted to bed or chair or perambulated in wheelchair, but may be out of bed itself much of the day; retains many self-care functions; generally has effective use of arms
3.5 Fully ambulatory but with moderate disability in one functional system and more than minimal disability in several others
8.5 Essentially restricted to bed much of day; has some effective use of arms; retains some self-care functions
4.0 Fully ambulatory without aid, self-sufficient, up and about some 12 hours a day despite relatively severe disability; able to walk without aid or rest some 500 meters
9.0 Helpless bed patient; can communicate and eat
4.5 Fully ambulatory without aid, up and about much of the day, able to work a full day, may otherwise have some limitation of full activity or require minimal assistance; characterised by relatively severe disability; able to walk without aid or rest some 300 meters
9.5 Totally helpless bed patient; unable to communicate effectively or eat/swallow
5.0 Ambulatory without aid or rest for about 200 meters; disability severe enough to impair full daily activities (work a full day without special provisions)
10.0 Death due to MS
Reproduced with permission from Kurtzke JF. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983;33:1444-1452.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND42
The nurse, in conjunction with the patient will identify contributing factors to altered mobility. These may include; weakness, fatigue, pain, spasticity, lack of coordination, tremor, loss of balance, sensory loss and/or visual impairment, and environmental barriers.
Altered mobility may impact on a variety of daily activities, which should be determined during the assessment. These include employment, social activities, sexual activity, household activities other leisure activities.
The nurse and patient together will identify existing management strategies and coping behaviours used by the patient, and determine the effectiveness of same.
4.8.5 InterventionsThe role of the nurse includes patient education, referral to other members of the multidisciplinary team, providing information on community resources and ongoing evaluation of the patient’s management strategies.
Patient education is a key intervention with regard to altered mobility. The nurse will inform the patient regarding the causes of altered mobility such as spasticity, weakness, loss of balance, sensory changes. The potential risks associated with altered mobility include falls, fractures, and reduced capacity for safe driving. The potential complications of altered mobility include contractures, skin breakdown, compression neuropathies and pain.
It may be appropriate for the nurse to refer the patient to the physiotherapist and/or occupational therapist for assistance in the management of altered mobility including gait retraining, mobility aides, stretching and strengthening programmes, balance training, energy conservation training and environmental accessibility and adaptive equipment.
The nurse will provide the patient with information on community resources that assist with mobility (social worker, community worker, MS Society, community OT, physiotherapist) and refer to same.
The nurse’s role, regarding altered mobility must include ongoing evaluation of the patient’s management strategies, to ensure they are effective and if not, investigate the reasons in conjunction with the patient and where possible implement an alternative strategy.
4.8.6 References
Souza et al. Multiple sclerosis and mobility –related assistive technology: systematic review of literature. Journal of Rehabilitation Research and Development 2010; 47(3): 213–224. van den Noort S, Holland NJ. Multiple sclerosis in clinical practice. 2nd edition. New York: Demos Medical Publishing Co. Inc.;1999.
CHAPTER 4 Management of MS-related symptoms 43
4.8.7 Suggested reading
Baum HM, Rothschild BB. Multiple sclerosis and mobility restriction. Arch Phys Med Rehab 1983; 64: 591–596.
Di Fabio RP, Choi T, Soderberg J, Hansen CR. Health-related quality of life for people with primary progressive multiple sclerosis: influence of rehabilitation. Phys Ther 1997; 77(12): 1716.
Freeman JA, Landdon DW, Hobart JC, Thompson AJ. The impact of Inpatient rehabiliation on primary progressive multiple sclerosis. Annals of Neurology 1997; 42: 236–244.
Freeman JA, Landdon DW, Hobart JC, Thompson AJ. Inpatient rehabilitation in multiple sclerosis: do benefits carry over into the community? Neurology 1999; 52: 50–56.
Thompson AJ. Progress in neurorehabilitation in multiple sclerosis. Current Opinion in Neurology 2002; 15: 267–270.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND44
4.9 SPEECH AND SWALLOWING DIFFICULTIES In MS, speech and voice disturbances are usually present as spastic-ataxic dysarthrias that involve disorders of voice intensity, voice quality, articulation, and intonation. ‘Dysarthria may occur in up to 40% of people with MS’ (Hartelius & Svensson, 1994; Yorkston et al, 2003).
4.9.1 Learning objectivesAfter completing this section, the reader will be able to:
· Describe the desired outcomes of treatment interventions for speech and swallowing difficulties
· Describe and apply strategies for the assessment of speech and swallowing
· Implement interventions for the management of speech and swallowing difficulties.
4.9.2 Desired patient outcomesThe patient will be able to describe the cause of speech and swallowing difficulties. The patient will demonstrate knowledge of safe eating habits and report reductions in choking and coughing at mealtimes. The patient will maintain nutritional status as demonstrated by body mass index (BMI) and serum albumin levels.
The patient will exhibit improved communication.
4.9.3 IntroductionAs the disease progresses the severity of the speech symptoms tend to increase, and generally correspond with the presentation of other MS symptoms involving mobility, vision changes, fatigue and depression (Yorkston et al, 2003 cited in Baylor et al, 2010).
The treatment of dysarthria and dysphagia is effective in improving patient function in daily activities (Merson & Rolnick, 1998).
Although language disturbances, such as aphasia, auditory agnosia, anomia, dysgraphia, and dyslexia are very rare in MS, swallowing disorders are common in patients with advanced disease, particularly if demyelination occurs in the brain stem’s sensorimotor pathways (i.e. cranial nerves VII, IX, X or XII) (Merson & Rolnick, 1998). Self-reports of chewing and swallowing problems generally increase as the disease progresses (i.e. incidence of these problems is 51% in late stages of MS compared to 19% in early stages of the disease) (Hartlelius & Svensson, 1994). Dysphagia affects 30% of MS patients (Hartelius et al, 1994; Poorjavad et al, 2010). And up to 60% of advanced MS experience dysphagia (De Pauw et al, 2002 cited in MS Trust, 2011). Depending on the location and extent of demyelination, swallowing disorders can relapse and remit along with MS exacerbations (Merson & Rolnick, 1998).
CHAPTER 4 Management of MS-related symptoms 45
4.9.4 Nursing assessmentAssessment involves determining the nature of speech and swallow difficulties, identifying possible contributing factors, determining how other activities are impacted upon, identifying the patient’s management strategies and in collaboration with the patient suggesting strategies that can improve the symptoms.
The speech and swallowing difficulties are assessed in terms of onset, duration, severity and describe the symptom characteristics in terms of dysarthia, dysphonia and asphasia (for speech problems) and choking, coughing, delayed swallowing and chewing issues (for swallowing problems).
Possible contributing factors can be identified by questioning the patient regarding same. Factors may include fatigue, cognitive changes and other MS-related symptoms. The nurse will also determine whether the speech and swallowing problems are affecting weight loss, dehydration, respiratory compromise, and changes in social and recreational activities.
Speech and swallowing difficulties may impact on a variety of daily activities, which can be determined, such as employment and social activities.
The nurse and patient together will identify existing management strategies and coping behaviours used by the patient, and determine the effectiveness of same.
4.9.5 InterventionsThe nurse may refer the patient to a Speech and Language therapist for assessment which may include videofluroscopy (for swallow assessment).
Interventions for the management of speech problems can then be planned, such as: oral motor exercises, appropriate timing and rate of speech, new strategies to help patient communicate, signing, hand and facial gestures, use of assistive devices, such as computers and/or letterboards.
Interventions for swallow problems include correct positioning, dietary modifications, such as changes in texture and consistency of foods, alertness at mealtimes, supervision at meals, management of secretions.
The nurse may refer to a dietician for guidance on appropriate nutrition and maintenance of BMI.
Calculation of BMI
BMI is calculated by dividing weight in kilograms (kg) by the square of the patient’s height in metres (m).
Example: Weight: 75 kg, height: 180 cm = 1.8 m. BMI = 75/(1.8)2 = 23
Generally, a BMI between 19 and 30 is considered ideal. If the patient’s BMI falls below 19 or exceeds 30, the patient is at risk for serious health complications and should consult a physician.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND46
Educating the patient’s family is an integral part of the management of safe swallowing practices. Families may need to have appropriate suctioning skills, be proficient in performing the Heimlich manoeuvre and be aware of the signs and symptoms of chest infections. A long term feeding tube may be required for patients who experience severe swallowing difficulties. Both the patient and family will need adequate information and training on the use of the feeding tube and associated complications. The nurse will need to inform the patient about changes to their body image.
The nurse and speech and language therapist must include ongoing evaluation of the patient’s management strategies, to ensure they are effective and if not, investigate the reasons in conjunction with the patient, and where necessary agree a new plan of care.
4.9.6 References
Baylor et al. Variables associated with communicative participation in people with multiple sclerosis: a regression analysis. American Journal of Speech-Language Pathology 2010; 19: 143–153.
Hartlelius L, Svensson P. Speech and swallowing symptoms associated with Parkinson’s disease and multiple sclerosis: a survey. Folia Phoniatr Logop 1994; 46: 9–17.
Merson RM, Rolnick MI. Speech-language pathology and dysphagia in multiple sclerosis. Phys Med Rehab Clin N Am 1998; 9: 631–641.
MS Trust 2011 Multiple Sclerosis Information for Health and Social Care Professionals, 4th edition. Hertfordshire.
4.9.7 Suggested reading
Merson RM, Rolnick MI. Speech-language pathology and dysphagia in multiple sclerosis. Phys Med Rehab Clin North Am 1998; 9: 631–641.
CHAPTER 4 Management of MS-related symptoms 47
4.10 VISUAL PROBLEMS IN MSPrior to starting this module the reader should have an understanding of the anatomy and physiology of the eye, review the cranial nerves associated with eyesight and eye movement and the process of demyelination.
4.10.1 Learning objectivesAfter completing this module the reader should be able to:
· Describe the desired outcomes of treatment interventions for visual problems
· Describe visual problems in MS
· Describe nursing assessment in relation to visual problems
· Describe management and treatment of visual problems in MS
· Describe impact of visual problems on the person with MS
· Outline the role of MS nurse in regard to visual problems in MS.
4.10.2 Desired patient outcomesThe patient will be able to discuss and outline the visual problems they are experiencing. The Patient will learn management and safety strategies to deal with their visual problems. The patient will gain a further understanding of visual problems and the treatments used.
4.10.3 IntroductionThe visual system is composed of the eyes, the optic tract and the visual cortex (Burgess, 2002). Over half the human sensory receptors are located in the eyes (Tortora & Grabowski, 2000). In many cases visual problems are the first symptom that people present with prior to a diagnosis of MS. Visual problems in MS include optic neuritis and eye movement problems, such as diplopia (double vision) and nystagmus (uncontrolled eye movements)(MS Essentials, 2004). Visual problems can impact on activities of daily living. The MS nurse has a role to play in educating and supporting PWMS who experience visual problems.
4.10.3.1 Optic neuritis
The optic nerve is the nerve pathway along which messages travel from the eye to the brain. Inflammation of the optic nerve is described as optic neuritis. In MS, retrobulbar neuritis is the most common (Kanski, 2006). Optic neuritis can develop over hours to days which may affect one (usually unilateral) or occasionally both eyes and take 4–12 weeks to recover.
Most people recover but some may experience more long-term problems. The effect on vision is variable. It may result in blurring of vision, shading, central visual field loss, diminished colour perception and pain in or around the eyes. Temporary blindness in one eye may be the result of optic neuritis.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND48
Response of one pupil to light when compared to the second eye and examination of the optic disc may indicate demyelinating disease. Retinal nerve fibre thickness reduction is significant in the eyes of PWMS who have optic neuritis. The nerve fibre is measured using Optic Coherence Tomography (OCT) (Fisher et al, 2006). Diagnosis of MS may be confirmed with Visual Evoked Potentials, which measure the time it takes for the brain to receive and interpret messages from the eye. Electrodes are placed on the person’s head. The person watches moving images on the screen. The brain wave is analysed to detect abnormalities.
The treatment for optic neuritis is the administration of corticosteroids, which have immunosuppressive and immunomodulatory properties. Treatment is 500 mg -1g/day methylprednisolone IV over 3–7 days often followed by a tapering dose of oral prednisolone over 2–4 weeks (National Multiple Sclerosis Clinical Bulletin, 1999).
4.10.3.2 Eye movement problems
In MS, there can be damage to nerve pathways that control eye movement. Eye movement problems include diplopia (double vision) and nystagmus. Double vision happens when muscles that control a particular eye movement are not coordinated due to weakness of the muscle. This can resolve without treatment. Treatment of double vision may include wearing a cover over one eye. An optician may prescribe prism glasses. Steroids are often used to treat an acute relapse causing diplopia and can speed the rate of recovery.
Nystagmus is uncontrolled horizontal or vertical eye movements. The patient may describe it as a flickering or jumping of the eye. It can be mild or it may be severe enough to affect vision. Fatigue and heat (Uhthoff’s symptom) can make it worse. It may resolve without treatment but it may be difficult to treat. Internuclear Ophthalmologia (INO) is a common presentation in PWMS. It is a horizontal nystagmus (Pavan-Langston, 1996) and includes diplopia and blurred vision.
Oscillopsia is a shaking field of vision due to ocular instability where the eye may turn upwards (Pavan-Langston, 1996; Riordan & Whitcher, 2004). Treatment for oscillopsia may include Gabapentin, Baclofen and Clonazepam (Warlow, 2006).
4.10.4 Nursing assessmentNursing assessment of visual problems involves obtaining a patient history of visual problems. Description of when the symptom started and the features of the visual problem including characteristics, e.g. blurred, double, pain, loss of vision. Assess if symptom is acute or chronic. Determine possible factors that contribute to the problem including fatigue, stress, infection, other MS symptoms, relapse, medications (e.g. tricyclic antidepressants) and temperature (Wells Courtney, 2003). Determine impact of visual problems on other symptoms. Identify how the person with MS manages current visual problems.
CHAPTER 4 Management of MS-related symptoms 49
4.10.5 InterventionsInform the patient about possible causes of visual problems in MS. Refer to the multidisciplinary team, including Neuro-Ophthalmologist and Occupational Therapist. Educate patient on treatments including intravenous steroid administration. Provide information on resources in the community to assist the person with visual problems. Evaluate the impact of visual problems on the person with MS, including safety (e.g. risks of falls, bumping into furniture), changes in lifestyle and communication. Assist patient in implementing strategies to manage visual problems as recommended by the multidisciplinary team. Provide ongoing support as needed (The United Kingdom MS Management Manual, 2006).
4.10.6 Impact of visual problems for person with MSVisual problems in MS can be common. For the person with MS it can be very frightening to experience changes in vision. A common fear is that vision will be lost and not return to normal. Most (90%) of patients will experience good recovery from an acute optic neuritis. Change of vision can impact on other activities of daily living. Education and information on common visual problems in MS and treatment options can help reduce associated anxiety and help the person with MS to cope with changes in vision. The person with MS may need to make some adjustments in order to manage their visual problems. The MS nurse has an important role in helping the person with MS manage visual problems.
4.10.7 Role of the MS nurse
The MS nurse:
· Assesses the nature of the visual problem and determines the onset, duration, location and severity
· Identifies possible contributing factors, such as relapse, concurrent illness, psychological issues or other MS related symptoms
· Assesses if the visual problem is acute or chronic
· Determines the impact on activities of daily living, psychological issues and other MS symptoms
· Refers patients to other members of the multidisciplinary team (e.g. Neuro-Ophthalmologist, Occupational Therapist) and external agencies (e.g. MS Society, PHN, National Council for the Blind of Ireland)
· Educates patient on visual problems and treatments
· Helps patient make adjustments and maintain safety as recommended by the multidisciplinary team
· Provides ongoing support and education as needed (Harper, 2001) for both patient and carer.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND50
4.10.8 ConclusionThe visual system is complex. Problems with vision in MS are common but in most cases can be managed. It is important for health professionals who work with PWMS understand the nature of visual problems in MS and treatments. The MS nurse has a role to play in educating and supporting PWMS and their carers.
4.10.9 References
Burgess M. (2002). Multiple Sclerosis theory and practice for nurses, Whurr, London.
Fisher JB, Jacobs DA, Markowitz CE et al. Ophthalmology 2006; 113 (2): 324–332.
Harper J. (2001) Advanced Concepts in Multiple Sclerosis Nursing, Demos, New York.
Kanski J. (2006). Clinical Diagnosis in Ophthalmology, Mobsy, Winsor.
MS Society (2004). MS Essentials 05: Vision and MS.
National Multiple Sclerosis Society clinical Bulletin (2004) Diagnosis and Management of Visual Problems in MS.
Pavan-Langston, D. (1996) Manual of Ocular Diagnosis and Therapy, 4th edition, Little, Brown and Company, London.
Riordan-Eva P and Whitcher (2004) Vaughan & Asbury’s General Ophthalmology, 16th edition, McGraw Hill, New York.
Tortora G and Grabowski S. (2000) Principles of Anatomy and Physiology, 9th edition Wiley, New York.
The United Kingdom MS Clinical Management Manual 2006.
Warlow C. (2006) The Lancet Handbook of Treatment in Neurology.
Wells Courtney, S. (2003) Multiple Sclerosis Managing Symptoms, 3rd Edition, Multiple Sclerosis Association of America, New Jersey.
4.10.10 Suggested reading
Medopedia., Multiple Sclerosis Vision Problems, www.medopedia.com.
The Multiple Sclerosis Resource Centre, Visual disturbance, www.msrc.co.uk.
The Multiple Sclerosis Resource Centre, Optic Neuritis, www.mrsc.co.uk.
WebMD, Multiple Sclerosis: Vision Problems, http://www.webmd.com.
CHAPTER 4 Management of MS-related symptoms 51
4.11 DEPRESSIONDepression is very common among individuals with MS. The lifetime prevalence for major depression in MS is over 50% (Sadovnick et al, 1991 cited in Mohr et al, 2003). Bol et al (2009) suggest that depression is prevalent in MS, affecting 27– 54% of patients. Feinstein (2002) carried out a study on 140 MS patients and found a prevalence rate of 36% for major depression and a prevalence rate of 29% for suicidal intent (Lester et al, 2007). MS patients at greater risk of depression are those with shorter disease duration (newly diagnosed), greater disease severity and less social support (MS Trust, 2011).
4.11.1 Learning objectivesAfter completing this section, the reader will be able to:
· Describe the desired outcomes of treatment interventions for depression
· Describe and apply strategies for the assessment of depression
· Implement interventions for the management of depression.
4.11.2 Desired patient outcomesThe patient will be able to discuss and outline the problems they are experiencing with depression. The patient will learn management and safety strategies to deal with their depressive illness. Patient will gain a further understanding of depression and the treatments used.
4.11.3 IntroductionPatients with MS have been found to have higher depression levels than those with other chronic disorders (Minden et al, 1987; Surridge, 1969 cited in Mohr et al, 2003). The uncertainty of the future, coupled with the perceived loss of a “normal” life, causes most individuals to feel depressed at least occasionally (Halper et al, 1997; Schapiro, 1991; van den Noort et al, 1999). The symptoms of depression include (Halper et al, 1997):
· Feelings of hopelessness, despair, and guilt
· Fatigue
· Insomnia
· Suicidal ideation.
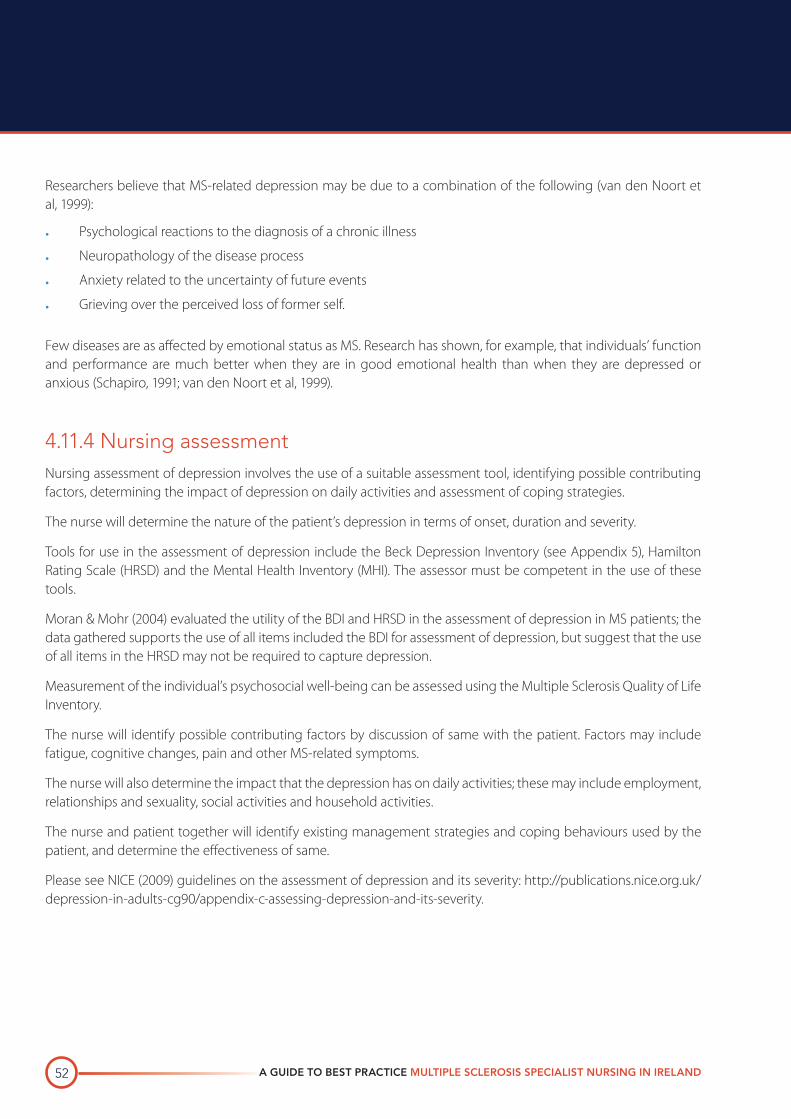
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND52
Researchers believe that MS-related depression may be due to a combination of the following (van den Noort et al, 1999):
· Psychological reactions to the diagnosis of a chronic illness
· Neuropathology of the disease process
· Anxiety related to the uncertainty of future events
· Grieving over the perceived loss of former self.
Few diseases are as affected by emotional status as MS. Research has shown, for example, that individuals’ function and performance are much better when they are in good emotional health than when they are depressed or anxious (Schapiro, 1991; van den Noort et al, 1999).
4.11.4 Nursing assessmentNursing assessment of depression involves the use of a suitable assessment tool, identifying possible contributing factors, determining the impact of depression on daily activities and assessment of coping strategies.
The nurse will determine the nature of the patient’s depression in terms of onset, duration and severity.
Tools for use in the assessment of depression include the Beck Depression Inventory (see Appendix 5), Hamilton Rating Scale (HRSD) and the Mental Health Inventory (MHI). The assessor must be competent in the use of these tools.
Moran & Mohr (2004) evaluated the utility of the BDI and HRSD in the assessment of depression in MS patients; the data gathered supports the use of all items included the BDI for assessment of depression, but suggest that the use of all items in the HRSD may not be required to capture depression.
Measurement of the individual’s psychosocial well-being can be assessed using the Multiple Sclerosis Quality of Life Inventory.
The nurse will identify possible contributing factors by discussion of same with the patient. Factors may include fatigue, cognitive changes, pain and other MS-related symptoms.
The nurse will also determine the impact that the depression has on daily activities; these may include employment, relationships and sexuality, social activities and household activities.
The nurse and patient together will identify existing management strategies and coping behaviours used by the patient, and determine the effectiveness of same.
Please see NICE (2009) guidelines on the assessment of depression and its severity: http://publications.nice.org.uk/depression-in-adults-cg90/appendix-c-assessing-depression-and-its-severity.
CHAPTER 4 Management of MS-related symptoms 53
4.11.5 InterventionsPlease see NICE (2009) guidelines on the treatment and management of depression in adults: www.nice.org.uk/CG90.
4.11.5.1 Nursing care plan
The nursing care plan can be seen in Table 4.12.
Table 4.12. Nursing care plan.
NURSING DIAGNOSIS
INTERVENTION RATIONALE DESIRED INDIVIDUAL OUTCOME(S)
Dep
ress
ion
due
to
diag
nosi
s (r
eact
ive)
· Assess for suicidal ideation
· Educate and reassure individual of appropriateness of response
· Involve partner/carer and/or family in interventions
· Administer depression assessment tools if appropriate
· Inform family physician and psychiatrist of assessment
· Document all assessments and conversations with the individual
· Depression is treatable, regardless of cause
· Involving partner/carer and/or family in interventions helps ensure that the individual adheres to treatment
· Documentation ensures professionalism and provides a record for determining accountability
· Experiences no or fleeting suicidal ideation
· Verbalises understanding that depression is not an unexpected reaction to the diagnosis
· Verbalises that their mood has improved
Dep
ress
ion
rela
ted
to
dis
ease
pro
cess
· Assess for suicidal ideation · Involve partner/carer and/or
family in interventions· Inform General Practitioner of
diagnosis· Document all assessments
and conversations with the individual
· Depression is treatable, regardless of cause
· Involving partner/carer and/or family in interventions helps ensure that the individual adheres to treatment
· Documentation ensures professionalism and provides a record for determining accountability
· Experiences no or fleeting suicidal ideation
· Verbalises acceptance of the unpredictability of the disease course
· Verbalises and acknowledges the symptoms of depression and expresses a willingness to seek treatment
· Verbalises understanding that depression is common in MS
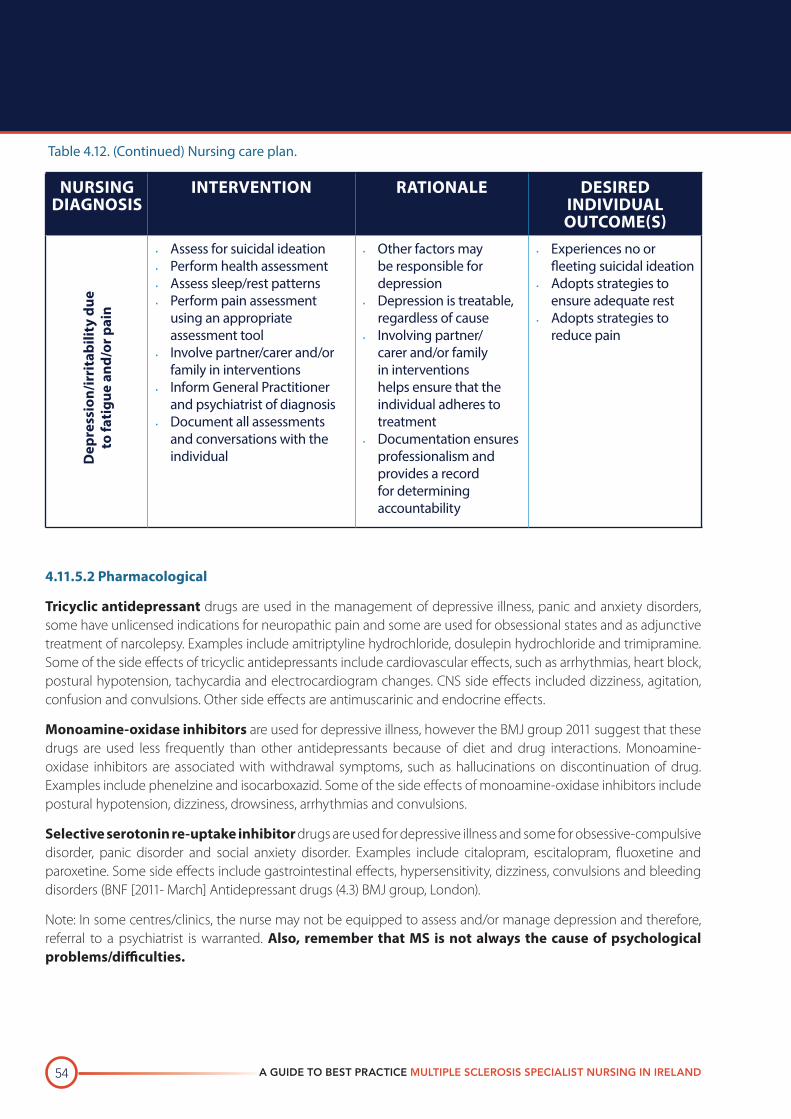
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND54
NURSING DIAGNOSIS
INTERVENTION RATIONALE DESIRED INDIVIDUAL OUTCOME(S)
Dep
ress
ion/
irri
tabi
lity
due
to
fati
gue
and/
or p
ain
· Assess for suicidal ideation· Perform health assessment· Assess sleep/rest patterns· Perform pain assessment
using an appropriate assessment tool
· Involve partner/carer and/or family in interventions
· Inform General Practitioner and psychiatrist of diagnosis
· Document all assessments and conversations with the individual
· Other factors may be responsible for depression
· Depression is treatable, regardless of cause
· Involving partner/carer and/or family in interventions helps ensure that the individual adheres to treatment
· Documentation ensures professionalism and provides a record for determining accountability
· Experiences no or fleeting suicidal ideation
· Adopts strategies to ensure adequate rest
· Adopts strategies to reduce pain
4.11.5.2 Pharmacological
Tricyclic antidepressant drugs are used in the management of depressive illness, panic and anxiety disorders, some have unlicensed indications for neuropathic pain and some are used for obsessional states and as adjunctive treatment of narcolepsy. Examples include amitriptyline hydrochloride, dosulepin hydrochloride and trimipramine. Some of the side effects of tricyclic antidepressants include cardiovascular effects, such as arrhythmias, heart block, postural hypotension, tachycardia and electrocardiogram changes. CNS side effects included dizziness, agitation, confusion and convulsions. Other side effects are antimuscarinic and endocrine effects.
Monoamine-oxidase inhibitors are used for depressive illness, however the BMJ group 2011 suggest that these drugs are used less frequently than other antidepressants because of diet and drug interactions. Monoamine-oxidase inhibitors are associated with withdrawal symptoms, such as hallucinations on discontinuation of drug. Examples include phenelzine and isocarboxazid. Some of the side effects of monoamine-oxidase inhibitors include postural hypotension, dizziness, drowsiness, arrhythmias and convulsions.
Selective serotonin re-uptake inhibitor drugs are used for depressive illness and some for obsessive-compulsive disorder, panic disorder and social anxiety disorder. Examples include citalopram, escitalopram, fluoxetine and paroxetine. Some side effects include gastrointestinal effects, hypersensitivity, dizziness, convulsions and bleeding disorders (BNF [2011- March] Antidepressant drugs (4.3) BMJ group, London).
Note: In some centres/clinics, the nurse may not be equipped to assess and/or manage depression and therefore, referral to a psychiatrist is warranted. Also, remember that MS is not always the cause of psychological problems/difficulties.
Table 4.12. (Continued) Nursing care plan.
CHAPTER 4 Management of MS-related symptoms 55
4.11.6 References
BNF (2011-March) Antidepressant drugs (4.3) BMJ group, London. Feinstein A. The clinical neuropsychiatry of multiple sclerosis. Toronto. Cambridge University Press; 1999. Halper J, Holland N. Comprehensive nursing care in multiple sclerosis. New York: Demos Vermande; 1997. Mohr D. Brain lesion volume and neuropsychological function predict efficacy of treatment for depression in multiple sclerosis. Journal of Consulting and Clinical Psychology 2003; 71(6): 1017–1024. Moran P, Mohr D. The validity of Beck Depression Inventory and Hamilton Rating Scale for Depression items in the assessment of depression among patients with multiple sclerosis. Journal of Behavioural Medicine 2005; 28(1): 35–41. Lester et al. The Association of Illness Severity, Self-reported, Cognitive Impairment, and Perceived Illness Management with Depression and Anxiety in a Multiple Sclerosis Clinic Population. Journal of Behavioural Medicine 2007; 30(2): 177–186. Sadovnick AD, Remick RA et al. Depression and Multiple Sclerosis. Neurology 1996; 46:628–632. Schapiro RT. Multiple sclerosis: a rehabilitation approach to management. New York: Demos Publishing; 1991. The Consortium of Multiple Sclerosis Centres Health Service Research subcommittee (1997) Multiple Sclerosis Quality of Life Inventory. National Multiple Sclerosis Society, New York. van den Noort S, Holland NJ. Multiple sclerosis in clinical practice. 2nd edition. New York: Demos Medical Publishing Co. Inc.; 1999.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND56
4.12 COGNITIVE IMPAIRMENTCognitive changes are common in MS; they occur in approximately 40–70% of individuals with MS. These include short-term memory, reduced attention span, altered concentration, reduced speed of information processing, alteration in visuospatial perception and construction, and in the ability to perform calculations.
4.12.1 Learning objectivesAfter completing this section, the reader will be able to:
· Describe the desired outcomes of treatment interventions for cognitive impairment
· Describe and apply strategies for the assessment of cognitive impairment
· Implement interventions for the management of cognitive impairment.
4.12.2 Desired patient outcomesThe patient will be able to discuss and outline the problems they are experiencing with cognitive impairment. The patient will learn management and safety strategies to deal with their cognitive impairment. Patient will gain a further understanding of cognitive impairment and the treatments used.
4.12.3 IntroductionCognitive changes range from mild to severe in nature and may occur early in the course of the disease and in the absence of physical changes. Even relatively mild deficits can have an impact on individuals’ day-to-day lives. Therefore, nominal assessment of cognitive function should be part of the ongoing neurological and nursing assessment of individuals with MS (Sadovnick, 1996; van den Noort et al, 1999).
The cognitive functions most commonly affected by MS are short-term memory, attention span, concentration, speed of information processing, executive functions, visuospatial perception and construction, and the ability to perform calculations.
In many instances, cognitive difficulties are incorrectly attributed to depression or other emotional disturbances. However, proper identification of cognitive problems is necessary for the development of appropriate management and treatment strategies (Halper et al, 1997).
Mood disorder can have an impact on cognition. Harvey (2011) suggests that cognitive changes are seen in those with mood disorders, where impairments in concentration, attention, learning, memory and executive functioning are highlighted in cognitive tests while a patient is in a depressed mood. Mood disorders are associated with alterations in social cognition, where social cognition is ‘the ability to understand and respond to the thoughts and feelings of others’(Cusi et al, 2012). In a systematic review of the neural basis of social cognition in patients with mood disorders, alterations in social cognition in those with mood disorders was related to patterns of neuronal activation during social encounters (Cusi et al, 2012).
CHAPTER 4 Management of MS-related symptoms 57
4.12.4 Nursing assessmentDuring the nursing assessment, the nurse may become aware of early signs of cognitive impairment. Nursing assessment of cognitive impairment includes assisting with the necessary cognitive testing, providing education to the patient and family regarding the assessment tools, determining the impact of cognitive impairment on daily activities and assessing current coping strategies.
The nurse will determine the nature of the patient’s cognitive impairment in terms of onset, duration and severity and evaluate the individual’s own perspective on his/her cognitive deficits.
An appropriately competent member of the multidisciplinary team will assess cognitive deficits by use of the Mini-Mental Exam, Montreal cognitive assessment (MoCA), Paced auditory serial addition test (PASAT) and the Perceived Deficit Questionnaire (PDQ) from the MS quality of life inventory.
· MoCA is a cognitive screening test designed to detect mild cognitive impairment. It assesses different cognitive domains: attention and concentration, executive functions, memory, language, visuoconstructional skills, conceptual thinking, calculations, and orientation. Administration time is 10 minutes. 30 is the total score, 26 and above is considered a normal result (www.mocatest.org).
· PASAT is a measure of cognitive function that assesses auditory information processing speed and flexibility, as well as calculation ability (www.natioanlmssociety.org). Kisski et al (2011) state that the PASAT is influenced by practice effects, education, anxiety and physical ability. Administration time is 10–15 minutes and scoring is out of 60.
· Self-Reported Cognitive Dysfunction: PDQ. This scale is used to assess perceived cognitive deficits from the patient’s perspective (The Consortium of Multiple Sclerosis Centres Health Service Research subcommittee, 1997).
The nurse should educate the individual about the above-mentioned tests (if necessary), reassure the patient that there is no pass or fail and that these results will assist the neurologist and/or psychologist to determine the cognitive areas the patient may need assistance with.
The nurse will identify possible contributing factors by discussion of same with the patient. Factors may include fatigue, pain, stress and other MS-related symptoms.
The nurse will also determine the impact that the cognitive impairment has on daily activities; these may include employment, relationships and sexuality, social activities and household activities.
The nurse and patient together will identify existing management strategies and coping behaviours used by the patient, and determine the effectiveness of same.
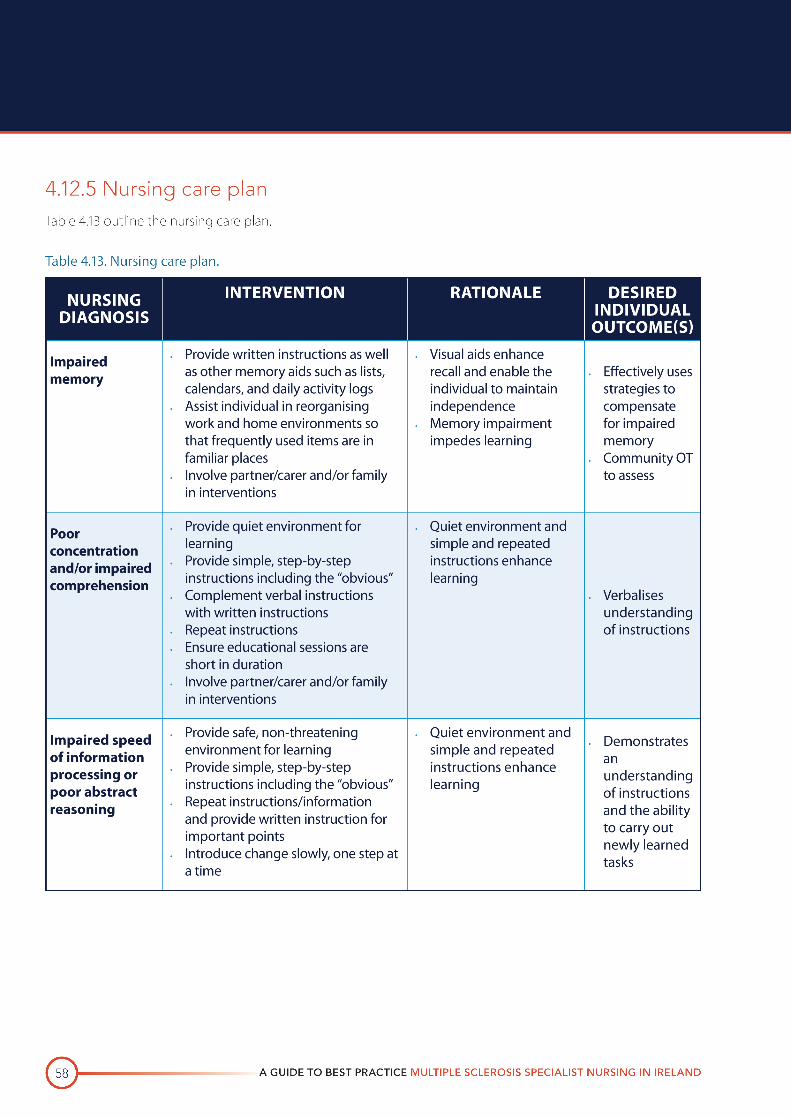
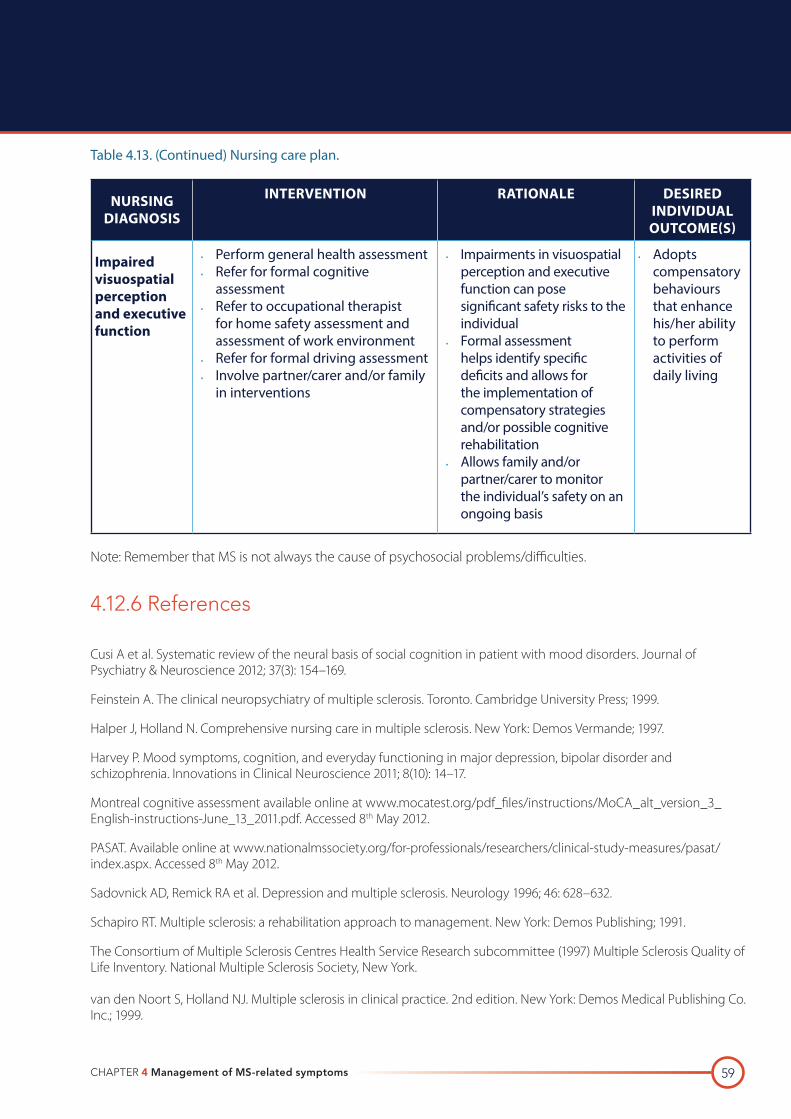
CHAPTER 4 Management of MS-related symptoms 59
NURSING DIAGNOSIS
INTERVENTION RATIONALE DESIRED INDIVIDUAL OUTCOME(S)
Impaired visuospatial perception and executive function
· Perform general health assessment· Refer for formal cognitive
assessment· Refer to occupational therapist
for home safety assessment and assessment of work environment
· Refer for formal driving assessment· Involve partner/carer and/or family
in interventions
· Impairments in visuospatial perception and executive function can pose significant safety risks to the individual
· Formal assessment helps identify specific deficits and allows for the implementation of compensatory strategies and/or possible cognitive rehabilitation
· Allows family and/or partner/carer to monitor the individual’s safety on an ongoing basis
· Adopts compensatory behaviours that enhance his/her ability to perform activities of daily living
Note: Remember that MS is not always the cause of psychosocial problems/difficulties.
4.12.6 References
Cusi A et al. Systematic review of the neural basis of social cognition in patient with mood disorders. Journal of Psychiatry & Neuroscience 2012; 37(3): 154–169.
Feinstein A. The clinical neuropsychiatry of multiple sclerosis. Toronto. Cambridge University Press; 1999.
Halper J, Holland N. Comprehensive nursing care in multiple sclerosis. New York: Demos Vermande; 1997.
Harvey P. Mood symptoms, cognition, and everyday functioning in major depression, bipolar disorder and schizophrenia. Innovations in Clinical Neuroscience 2011; 8(10): 14–17.
Montreal cognitive assessment available online at www.mocatest.org/pdf_files/instructions/MoCA_alt_version_3_English-instructions-June_13_2011.pdf. Accessed 8th May 2012.
PASAT. Available online at www.nationalmssociety.org/for-professionals/researchers/clinical-study-measures/pasat/index.aspx. Accessed 8th May 2012.
Sadovnick AD, Remick RA et al. Depression and multiple sclerosis. Neurology 1996; 46: 628–632.
Schapiro RT. Multiple sclerosis: a rehabilitation approach to management. New York: Demos Publishing; 1991.
The Consortium of Multiple Sclerosis Centres Health Service Research subcommittee (1997) Multiple Sclerosis Quality of Life Inventory. National Multiple Sclerosis Society, New York. van den Noort S, Holland NJ. Multiple sclerosis in clinical practice. 2nd edition. New York: Demos Medical Publishing Co. Inc.; 1999.
Table 4.13. (Continued) Nursing care plan.
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND60
4.13 PROGRESS CHECK1. List five non-pharmacological interventions for fatigue.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
d. _____________________________________________________________________________________________________
e _____________________________________________________________________________________________________
2. List and describe the three types of bladder dysfunction most commonly associated with MS.
a. _____________________________________________________________________________________________________
____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
____________________________________________________________________________________________________
3. List six interventions for faecal incontinence.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
d. _____________________________________________________________________________________________________
e _____________________________________________________________________________________________________
f _____________________________________________________________________________________________________
4. Distinguish between acute, subacute, and chronic pain in MS.
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
CHAPTER 4 Management of MS-related symptoms 61
5. ________________________ and ________________________ are two conditions that may contribute to chronic musculoskeletal pain in MS.
6. List five factors and/or actions that may worsen acute pain, particularly trigeminal neuralgia, in MS.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
d. _____________________________________________________________________________________________________
e _____________________________________________________________________________________________________
7. List five desired patient outcomes of treatment interventions for pain.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
d. _____________________________________________________________________________________________________
e _____________________________________________________________________________________________________
·
8. List nine factors and/or conditions that may contribute to spasticity.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
d. _____________________________________________________________________________________________________
e _____________________________________________________________________________________________________
f. _____________________________________________________________________________________________________
g. _____________________________________________________________________________________________________
h. _____________________________________________________________________________________________________
i. _____________________________________________________________________________________________________
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND62
9. Distinguish between intention, postural, and rest tremors.
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
10. Briefly describe seven interventions for the management of tremor.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
d. _____________________________________________________________________________________________________
e _____________________________________________________________________________________________________
f. _____________________________________________________________________________________________________
g. _____________________________________________________________________________________________________
11. List six strategies that the rehabilitation team may use to manage altered mobility.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
d. _____________________________________________________________________________________________________
e _____________________________________________________________________________________________________
f. _____________________________________________________________________________________________________
CHAPTER 4 Management of MS-related symptoms 63
12. List seven potential risks and/or complications of altered mobility.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
d. _____________________________________________________________________________________________________
e _____________________________________________________________________________________________________
f. _____________________________________________________________________________________________________
g. _____________________________________________________________________________________________________
13. List five desired patient outcomes of interventions for speech and swallowing difficulties.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
d. _____________________________________________________________________________________________________
e _____________________________________________________________________________________________________
14. What is the body mass index (BMI) of a woman who weighs 54 kg and is 175 cm tall? Is this BMI normal? If no, please explain.
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
______________________________________________________________________________________________________
15. List three visual problems associated with MS.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND64
16. List three aspects of the role of the MS nurse and visual disturbances in PWMS.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
17. Name a suitable assessment tool for depression in MS.
______________________________________________________________________________________________________
18. List three symptoms of depression.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
c. _____________________________________________________________________________________________________
19. Cognitive changes are common in MS; they occur in approximately ______________ of individuals with MS.
20. List two nursing diagnoses of cognitive impairment.
a. _____________________________________________________________________________________________________
b. _____________________________________________________________________________________________________
CHAPTER 4 Management of MS-related symptoms 65
4.14 PROGRESS CHECK ANSWERS1. List five non-pharmacological interventions for fatigue.
a. Promote patient understanding of MS-related fatigue
b. Implement energy-conservation strategies through adaptations to home and work environments
c. Encourage appropriate lifestyle modifications (e.g. temperature control, appropriate nutrition and fluid balance, activity/rest patterns, etc.)
d. Inform patient of therapies that may contribute to fatigue (e.g. antispasticity, medications, anticonvulsants, antidepressants, etc.) as well as their side-effect profiles
e. Provide ongoing evaluation of fatigue-management strategies
2. List and describe the three types of bladder dysfunction most commonly associated with MS.
a. Failure to store: occurs when the bladder is unable to accommodate increasing urine volumes, causing spontaneous contractions within the bladder; symptoms include urgency, frequency, and urge incontinence; this is the most common type of bladder dysfunction in MS
b. Failure to empty: is less common, but can result in more serious complications than failure to store; it may be caused by an atonic bladder, detrusor hyperreflexia with poorly sustained contractions, or detrusor-sphincter dyssynergia; symptoms of failure to empty include retention, overflow incontinence, and urinary tract infections.
c. Combination failure to store and failure to empty: occurs in 24–46% of patients with bladder dysfunction and MS; this condition is often associated with detrusor-sphincter dyssynergia; symptoms of this type of bladder dysfunction include those associated with both failure to store and failure to empty
3. List six interventions for faecal incontinence.
a. Ensure adequate evacuation of bowels on a regular basis
b. Rule out bowel infection using stool cultures
c. Avoid unnecessary use of antibiotics
d. Educate patient to use medications for control of this symptom and to avoid bowel irritants (e.g. alcohol, caffeine, and spicy foods)
e. Recognise that anxiety and stress may play a role in this problem
f. Provide ongoing evaluation of bowel dysfunction
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND66
4. Distinguish between acute, subacute, and chronic pain in MS.
Acute pain is often characterised by paroxysmal attacks that are brief in duration (i.e. lasting seconds) and occur repeatedly. It results from abnormal axon conduction or a “short circuit” in axon conduction. Subacute pain may last days or even weeks. It is caused by demyelination (optic neuritis is the most common) or a secondary source. Chronic neuropathic or dysaesthetic pain occurs in about one-third of patients with MS; it is believed to be directly related to the demyelination of sensory pathways. Chronic musculoskeletal pain, such as backaches and painful leg spasms, usually results from MS-related symptoms rather than the disease itself.
5. Osteoporosis and degenerative disk disease are two conditions that may contribute to chronic musculoskeletal pain in MS.
6. List five factors and/or actions that may worsen acute pain, particularly trigeminal neuralgia, in MS.
a. Chewing
b. Speaking
c. Exposure to wind and extreme temperatures
d. Hyperventilation
e. Certain movements/positions
7. List five desired patient outcomes of treatment interventions for pain.
a. Identifies the type of pain experienced
b. Feels that the health-care provider views the pain experience as real
c. Reduces pain symptoms through the use of behavioural strategies, rehabilitation, drugs, and other interventions
d. Successfully adopts coping behaviours
e. Exhibits improved performance on daily activities in the home and at work
8. List nine factors and/or conditions that may contribute to spasticity.
a. Temperature changes
b. Infection
c. Anxiety/stress
d. Constipation
CHAPTER 4 Management of MS-related symptoms 67
e. Pain
f. Immobility
g. Disruption of skin integrity
h. Bladder dysfunction
i. Medications
9. Distinguish between intention, postural, and rest tremors.
Intention tremor is associated with voluntary movement (e.g. when reaching for a cup) and may range from mild to severe in nature. It is the most common type of tremor seen in MS. Postural tremor occurs during a sustained position, such as with outstretched arms or when legs are crossed. Rest tremor occurs when the patient is relaxed or at rest. In general, this type of tremor is rare in MS.
10. Briefly describe seven interventions for the management of tremor.
a. Educate patient about the types and causes of tremor
b. Plan interventions according to the type of tremor
c. Inform patient of the possible treatment options
d. Assist patient in coping with tremor
e. Refer patient to a rehabilitation team for instruction on activities to help manage tremor (e.g. patterning, immobilisation, weighting)
f. Inform patient of factors that may affect tremor (e.g. anxiety, caffeine)
g. Provide ongoing evaluation of tremor management
11. List six strategies that the rehabilitation team may use to manage altered mobility.
a. Gait and assessment retraining
b. Mobility aids
c. Stretching and strengthening programs
d. Balance training
e. Energy-conservation training
f. Environmental accessibility and adaptive equipment
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND68
12. List seven potential risks and/or complications of altered mobility.
a. Falls
b. Fractures
c. Reduced capacity for safe driving
d. Contractures
e. Skin breakdown
f. Compression neuropathies
g. Pain
13. List five desired patient outcomes of interventions for speech and swallowing difficulties.
a. Able to describe the cause of speech and swallowing difficulties
b. Practices safe eating habits through the utilisation of compensatory strategies
c. Reports reductions in choking and coughing at mealtimes
d. Maintains adequate nutritional status
e. Exhibits improved communication
14. What is the body mass index (BMI) of a woman who weighs 54 kg and is 175 cm tall? Is this BMI normal? If no, please explain.
Her BMI is 17.6 (54 ÷1.752). Generally, a BMI between 19 and 30 is considered normal. Since this woman’s BMI falls below 19, she may be at risk for serious health complications and should consult a physician.
15. List three visual problems associated with MS.
f. Optic neuritis
g. Diplopia
h. Nystagmus
CHAPTER 4 Management of MS-related symptoms 69
16. List three aspect of the role of the MS nurse and visual disturbances in PWMS.
Any three of the following:
· Assesses the nature of the visual problem and determines the onset, duration, location and severity
· Identifies possible contributing factors such as relapse, concurrent illness, psychological issues or other MS related symptoms
· Assesses if the visual problem is acute or chronic
· Determines the impact on activities of daily living, psychological issues and other MS symptoms
· Refers patients to other members of the multidisciplinary team (e.g. Neuro-Ophthalmologist, Occupational Therapist) and external agencies (e.g. MS Society, PHN, National Council for the Blind of Ireland)
· Educates the patient on visual problems and treatments
· Helps the patient make adjustments and maintain safety as recommended by the multidisciplinary team
· Provides ongoing support and education as needed for both patient and carer
17. Name a suitable assessment tool for depression in MS.
Multiple Sclerosis Quality of Life Inventory: Mental Health Inventory (MHI)
18. List three symptoms of depression.
Any three of the following:
· Feelings of hopelessness, despair, and guilt
· Fatigue
· Insomnia
· Suicidal ideation
19. Cognitive changes are common in MS; they occur in approximately 40–70% of individuals with MS.
20. List two nursing diagnoses of cognitive impairment.
Any two of the following:
· Impaired memory
· Poor concentration and/or impaired comprehension
· Impaired speed of information processing or poor abstract reasoning
· Impaired visuospatial perception and executive function
A GUIDE TO BEST PRACTICE MULTIPLE SCLEROSIS SPECIALIST NURSING IN IRELAND70
4.15 GLOSSARYBDI Beck Depression Inventory
BMI Body mass index
CNS Central nervous system
CNSp Clinical nurse specialist
HRSI Hamilton Rating Scale
MHI Mental Health Inventory
MoCa Montreal cognitive assessment
MS Multiple sclerosis
PASAT Paced auditory serial addition test
PWMS People with multiple sclerosis