Embed Size (px)
DESCRIPTION
Chapter 8 Cholinocelptor Blocking Drugs-jjl.2013.9
Citation preview

Cholinoceptor blocking drugs
Jiang Junlin 江俊麟
Department of Pharmacology,
School of Pharmaceutical Science, Central South University

Cholinoceptor antagonists are divided into M and N subgroups based on their specific receptor affinities.
The N receptor antagonists consist of ganglion-blockers (N1,NN) and neuromuscular junction blockers (N2,NM).

M Receptor-blocking Drugs
are called parasympatholytic because they block the effects of parasympathetic
autonomic discharge.
Naturally occurring compounds with anti-M receptor effects have
been used for millennia as medicines, poisons, and cosmetics.
Atropine is their prototype. Many similar plant alkaloids are known.
Hundred of synthetic anti-M receptor compounds have been
prepared.
daturaAtropena belladonna

Deadly nightshade (Atropena belladonna) is
the natural source of the alkaloid atropine.
The term atropena is derived from Atropos
because of its high toxicity.
Atropine was a popular choice of poison
among professional poisoners during the
Middle Ages because of the slowness of
their effects which allowed the perpetrator
to escape before suspicions. According to
the Scottish legend, the soldiers of
Macbeth slipped atropine into the drinks
of the invading Danes then slaughter them
in their slumber.
In Roman time, ladies in the Court used the
juice from the berry to dilate their pupils
to make them look more sexsual and
attractive and hence the name belladonna
(beautiful lady). Atropena belladonna can
be translated as femme fatale.
Atropine

PharmacokineticsMost of antimuscarinic drugs being tertiary agents
reaches the CNS
Scopolamine is rapidly and fully distributed into the CNS
well absorbed from the gut and widely distributed in the body
where it has greater effects than most others
The quaternary derivatives are poorly taken up by the brain.
They are relatively less effect of CNS
Atropine

Pharmacokinetics
Atropine disappears rapidly from the blood, t ½ of 2-4 h.
The effect declines rapidly in all organs except the eye . Effects on the eye persist for ≥ 3 days.
About 50% of the dose is excreted unchanged in the urine.
The rest appears as hydrolysis and conjugation products.
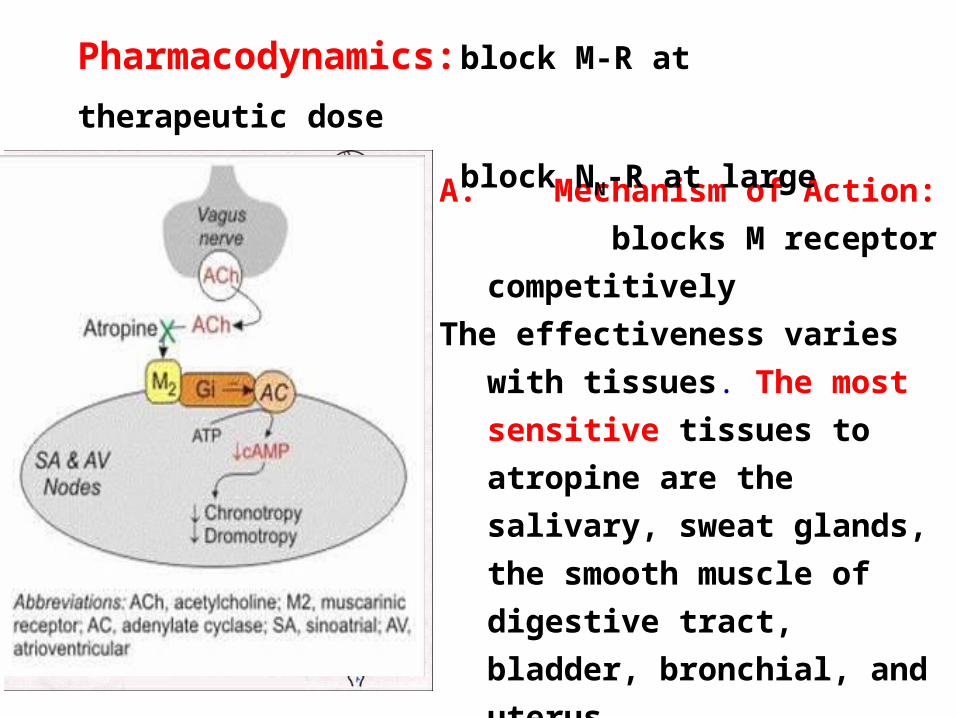
A. Mechanism of Action:
blocks M receptor competitively
The effectiveness varies with tissues.
The most sensitive tissues to
atropine are the salivary, sweat
glands, the smooth muscle of
digestive tract, bladder, bronchial,
and uterus.
The least sensitive is the gastric
parietal cells secreting acid.
Pharmacodynamics: block M-R at therapeutic dose
block NN-R at large dose

The smooth muscles of the iris
The sphincter muscle is innervated by cholinergic fibers to M receptors. Its contraction under the influence of an agonist results in miosis
The radial muscle is innervated by adrenergic fibers to an alpha-1 receptor. Its contraction by an agonist results in mydriasis and its blockade results in miosis
1. Eye— Mydriasis
Atropine and other anti-M drugs block M receptor and results in dilatation of iris and mydriasis.
B. Organ System Effects

1. Eye—
Mydriasis
intraocular pressure↑
Atropine block M receptor, contract the iris, and reduce the angle space of anterior chamber so as to prevent outflow of aqueous humor, increasing the the intraocular pressure.
Atropineblocks M receptor,inhibits the contraction of the iris, and narrow the angle space of anterior chamber
so as to prevent outflow of aqueous humor, increasing the intraocular pressure.

1. Eye—
Mydriasis 扩瞳
intraocular pressure↑ 升眼压
cycloplegia 调节麻痹
Anti-M drugs block M receptor, inhibit the contraction of the ciliary muscle, result in cycloplegia.

Accommodation and pupillary reflexs may not fully recover for 7 to 12 days. Muscarinic antagonist with short duration of actions are preferred as mydriatics in ophthalmological practice.

1. Eye— Mydriasis 扩瞳 intraocular pressure↑ 升眼压 cycloplegia 调节麻痹
Dry eyes
Antimuscarinic drugs reduce lacrimal secretion.

2. Cardioavascular system
Cardiomuscle is controlled by lesser degree of M receptor. Atropine has no clinical significant effect on it.
Sinoatrial nodeis controlled by M receptor.Atropine blocks M receptor and causes tachycardia to next. Lower doses (0.4-0.6 mg) results in initial bradycardia due to block presynaptic M receptor which limit ACh release.
Atropine blocks M receptor on atrioventricular node, increase the conduction, and the PR interval of ECG.
In toxic doses, atropine blocks intraventricular conduction

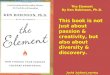
Dose- response curve for the effects of atropine on heart rate
Atropine dose (μg/kg) to back
2 4 6 8 10
60
70
80
●
●●
●●
●
●
●

Almost all vessels contain endothelial M receptors that mediate vasodilation. there is little effect on blood pressure alone.
At toxic doses, and in some individuals at normal doses, atropine cause cutaneous vasodilation. (it is may be a compensatory reaction permitting the radiation of heat to offset the atropin-induced rise in temperature that can accompany inhibition of sweating)
Blood Vessels

3. Respiratory System
Both smooth muscle and secretory glands of the airway receive vagal innervation and contain muscarinic receptors.
Atropine dilates bronchi and inhibits secretion of gland. The effect is more significant in patients with airway disease although the antimuscarinic drugs are not as useful as the β-adrenoceptor stimulants in the treatment of asthma.

4. Gastrointestinal Tract
Prolonged inhibitory effects on the motor activity of the stomach, duodenum, ileum and colon
Reduction in tone and in amplitude and frequency of peristaltic contraction.
Antimuscurinic drugs have marked effect on salivary secretion; Dry mouth occurs frequently.
Atropine inhibits gastric secretion less effectively, reduces the volume and amount of acid, pepsin, and basal secretion in large doses.
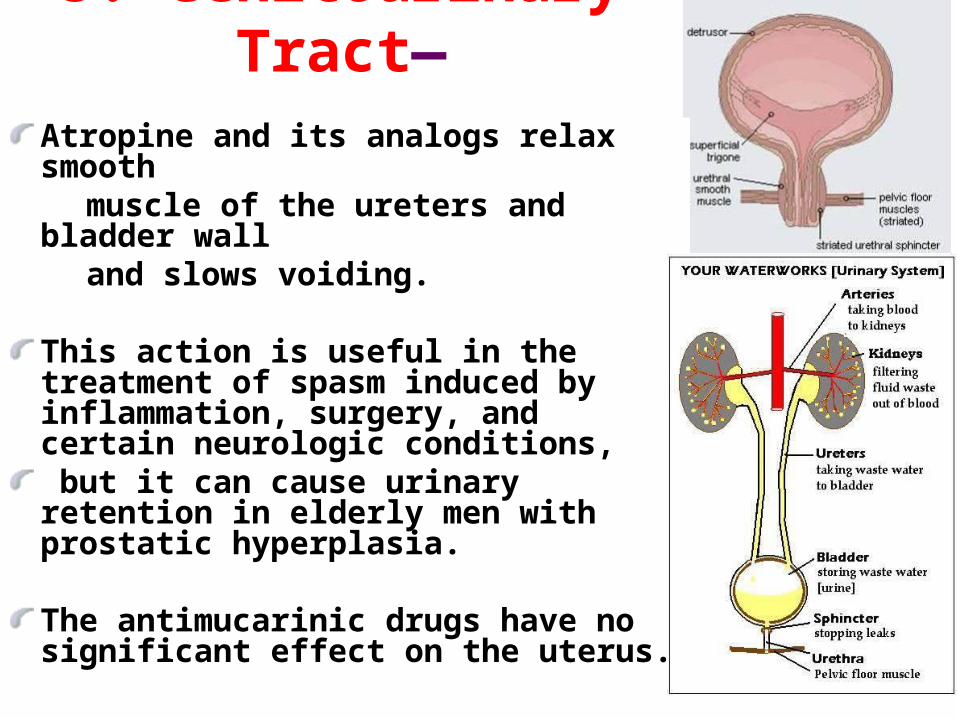
5. Genitourinary Tract—Atropine and its analogs relax smooth
muscle of the ureters and bladder wall and slows voiding.
This action is useful in the treatment of spasm induced by inflammation, surgery, and certain neurologic conditions, but it can cause urinary retention in elderly men with prostatic hyperplasia.
The antimucarinic drugs have no significant effect on the uterus.

6. Sweat Glands—Sympathetic cholinergic fibers innervate
sweat glands.
Atropine suppresses thermoregulatory
sweating.
In adults, body temperature is elevated by
large dose.
In infants and children even ordinary dose
may cause “atropine fever.”
High fever, body temperature is 39-42 , called " atropine fever ℃".

Scopolamine has marked central effects,
producing drowsiness and amnesia.
In toxic doses can cause excitement, agitation, hallucinations, and coma. (larger doses than toxic doses, stimulation is followed by depression, leading to circulatory collapse and respiratory failure
after a period of paralysis and coma)
7. Central Nerve System Atropine has minimal effects on the CNS.

Parkinson's disease occurs when neurons degenerate (lose the ability to function normally) in a part of the brain called the substantia nigra. Many of these neurons that degenerate contain the neurotransmitter called dopamine. As these neurons degenerate, dopamine levels fall, and the balance between dopamine and other neurotransmitters, such as acetylcholine, is thrown off. This neurotransmitter imbalance affects the way muscles work and leads to movement problems.
Therapeutic ApplicationsA. Central Nervous System Disorders
1.Parkinson’s Disease---
It is due to degeneration of dopamine neuron
and relative hyperactive cholinergic
functions.
Centrally acting antimuscarinic preparations
can block M receptor and decrease the
activity of M receptor to remain useful as
adjunctive therapy in some patients.

Accurate measurement of refractive error requires ciliary paralysis
(iridocyclytis and choroditis).
Examining the retina is facilitated by mydriasis. Antimuscarinic agents, administered locally
are extremely helpful in doing the examination.For adults, the shorter acting drugs are
preferred. For children, the greater efficacy
of atropine is necessary, but the possibility of
poisoning is correspondingly increased.
Accommodation and pupillary reflexs may
not fully recover for 7 to 12 days.
Therapeutic Applications- Ophthalmologic Disorders

Respiratory Disorders
Pre-anesthetic administration Irritant anesthetics such as ether markedly increased airway secretion
Atropine or scopolamine could prevent these effects. Scopolamine also block short-term memory (amnesia).

Cardiovascular Disorders
Patients with hyperactive carotid sinus reflexes experience
faintness or syncope as a result of vagal discharge in
response to pressure on the neck, a tight collar.
Antimuscarinic agents may benefit to the disease.
Excessive vagal discharge may
result in depression of sinoatrial or
atrioventricular node.
Atropine or similar antimuscarinic
drugs are appropriate therapy in this
situation.

Gastrointestinal Disorders Anti-M agents can relieve traveler’s
diarrhea and hypermotility. They are
often combined with an opioid
antidiarrhead drug, diphenoxylate.
In this combination, the very low dosage
of the anti-M drugs can decrease
opioid abuse.
Anti M agents are now rarely used for peptic ulcer disease
in the world.

Urinary Disorders
Atropine and other antimuscarinic drugs can relieve the urinary urgency caused by inflammation bladder disorder.
Oxybutynin is often used to relieve bladder
spasm after urologic surgery.
Imipramine, a antidepressant drug with strong antimuscarinic action, has long been used to reduce incontinence in institutionalized elderly patients.

Cholinergic PoisoningAntimusarinic Therapy
Poisoning of cholinesterase inhibitors
can increase the concentration of ACh
in synaptic space and show both the N
and the M effects. Atropine can reverse
the M effects in the CNS as well as the periphery.
Large doses of atropine may be needed to overcome
the M effects of extremely potent agent like
parathion (1605) and warfare nerve gases

Muscarinic stimulantsNausea, vomiting, diarrhea, abdominal pain, salivation, sweating, cutaneous vasodilation, and bronchial constriction.
They are all due to excitement of M receptors. The effects can be blocked by atropine.
Certain mushrooms contain muscarinic alkaloids which can cause typical signs of muscarine.

Adverse Effects Treatment with atropine at one organ almost always induce undesirable effects in other organ systems.
dry mouth, mydriasis, cycloplegia, tachycardia, hot and flushed skin, agitation, delirium, high temperature.
Atropine intoxication is potentially lethal in children (more
sensitive to its effects, particularly to rapid increase in body temperature).
Atropine intoxication is too risky in older individuals (an attack of
glaucoma due to an increase in intraocular pressure).
The poisoning can be treated with cholinesterase inhibitor such as neostigmine.

Scopolamine( 东莨菪碱 )
Characteristics
1.CNS actions: depression (strong)
2.peripheral actions: glands: strong
others: weak
Uses:
1.preanaesthesia medication
2. prevention motion sickness
3. parkinson disease
4. traditional medicine anaesthesia

Motion Sickness -prophylactic Scopolamine is one of the oldest remedies for seasickness.

Parkinson's disease occurs when neurons degenerate (lose the ability to function normally) in a part of the brain called the substantia nigra. Many of these neurons that degenerate contain the neurotransmitter called dopamine. As these neurons degenerate, dopamine levels fall, and the balance between dopamine and other neurotransmitters, such as acetylcholine, is thrown off. This neurotransmitter imbalance affects the way muscles work and leads to movement problems.
Parkinson’s Disease---
It is due to degeneration of dopamine neuron
and relative hyperactive cholinergic
functions.
Centrally acting antimuscarinic preparations
can block M receptor and decrease the
activity of M receptor to remain useful as
adjunctive therapy in some patients.

Anisodamine山莨菪碱Characteristic of actions
1.high selectivity (smooth muscle and vessels)
2.little side effects (not pass through BBB)
Uses visceral colic-antispasmodic agent

Synthetic atropine substitutes
Synthetic Mydriatics:
Homatropine( 后马托品 ), Tropicamide( 托吡卡胺 ), Cyclopentolate( 环喷托酯 ), Eucatropine( 尤卡托品 )
Selective M1 Antagonists-pirenzepine
Synthetic Antispasmatics

Ganglion-Blocking Drugs
These agents block the action of ACh and similar agonists at
the N receptors of autonomic ganglia.
They lack selectivity and have broad side effects so that they
have been rarely used in clinic.
The ganglionblocking drugs are useful in pharmacologic
research because of their
ability to block all
autonomic outflow.

Clinical Applications & Toxicity
Because of the availability of more selective autonomic
blocking agents, the applications of the ganglion
blockers have almost disappeared.
For most patients, the toxicity of the ganglion blocking
drugs are intolerable except for acute use.
Mecamylamine may reduce nicotine craving.
Trimethaphan is occasionally used in hypertensive
emergencies.

Skeletal muscle relaxants act peripherally at neuromuscular junction. According to their action, they are divided into:
•Nondepolarizing (competitive) agents •Depolarizing (hyperdepolarazing) agents
Neuromuscular Blocking Agents

Competitive(curare-like) blockingagents
N+ (14 Å) N+
GI resorptionBBB

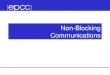
Curare is plant extract from
Chondrodendron tomentosum,Strychnos toxifera etc. It isused by South America tribalsas arrow poison for game hunting. The animals got pa-ralyzed even if not killed bythe arrow. Muscle paralyzingactive principles of curareare alkaloids tubocurarine,toxiferine etc.

Strychnos toxiferaChondrodendrontomentosum
The South Americam lianas

The competitive blockers have affinity for NM receptor at the muscle end-plate, but no intrinsic activity.
The NM-receptor is a macroprotein with5 subunits, which arearranged like a rosettesurrounding the Na+
channel. The two alphasubunits carry two AChbinding sites with nega-tively charged groupswhich combine with thecationic group of AChand open Na+ channel.

Depolarizing agents

Action of succinylcholine(suxamethonium)
Depolarizing agents produce dual mechanism neuro-muscular blockade :Phase I block---persistent depolarization of muscular end-plate which produces transient twitching of the musclePhase II block---membrane repolarize, desensitation of the NM-receptor to Ach which result in paralysis

44