Embed Size (px)
Citation preview
Charles Krasner, M.D.
University of NV, Reno School of Medicine
Sierra NV Veterans Affairs Medical Center
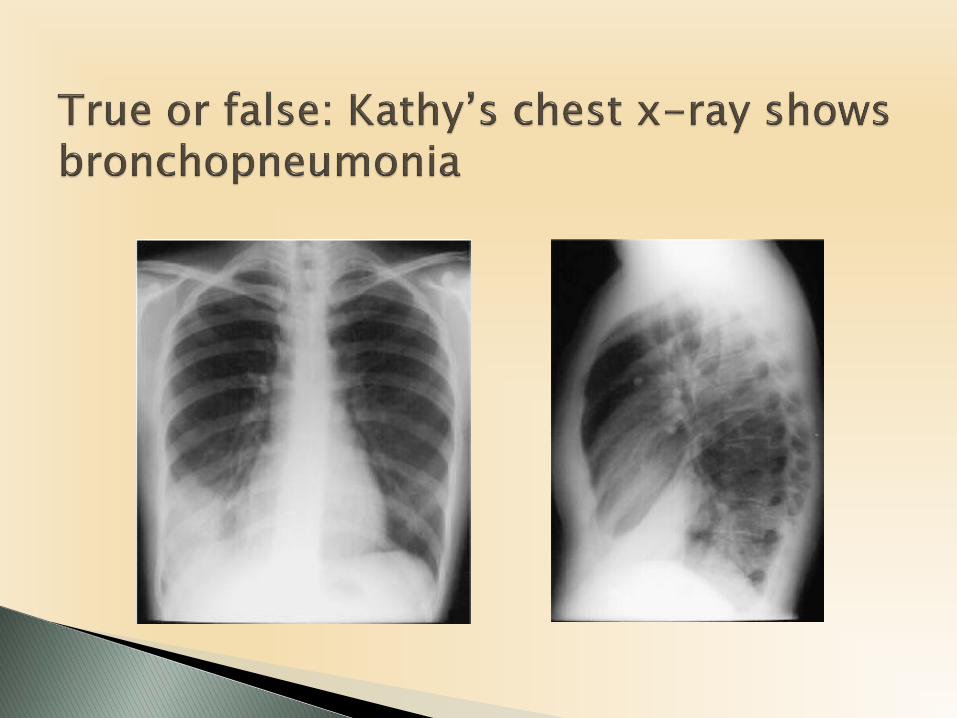
Kathy Peters is a 63 y.o. patient that presents to your urgent care office today with a history of coughing and wheezing for the past 5 days. Originally, she thought she was getting a cold; however, her symptoms have been getting worse, and she states she has never felt this "wiped out" from a cold. She is here to see you today because she feels like she has become more short of breath over the past 24 hours.
She tells you that she started feeling sick approximately 5 days ago. It started with a dry cough; however, over the past couple days she has expectorated some clear, and more recently, thicker rust-colored, mucous. She denies frank blood in her sputum. She notices some wheezing after coughing spells. This morning, Kathy woke up in a "coughing fit" and she said she felt some sharp pain in her chest. She rates the pain a 5/10 when it occurs. Kathy has felt feverish over the past few days; she sometimes gets the "chills." Her highest temperature was 102 degrees
PMH: hypertensionHabits: smoker for 30 years
BP: 110/80, HR: 96, RR: 26, T: 101.6, SpO2: 94% on room air
Physical exam: fatigued appearing, congested cough
Wheezing and rhonchi right lower chest with expiration
As you consider all of her presenting symptoms and history you begin to think that the most likely choice out of your differential diagnosis list is:
a. Asthma
b. Chronic Bronchitis
c. Nosocomial Pneumonia
d. Community-Acquired Pneumonia (CAP)

Candida albicans
Staph aureus
Strep pneumonia (pneumococcus)
Pseudomonas aeruginosa
Mycoplasma pneumonia
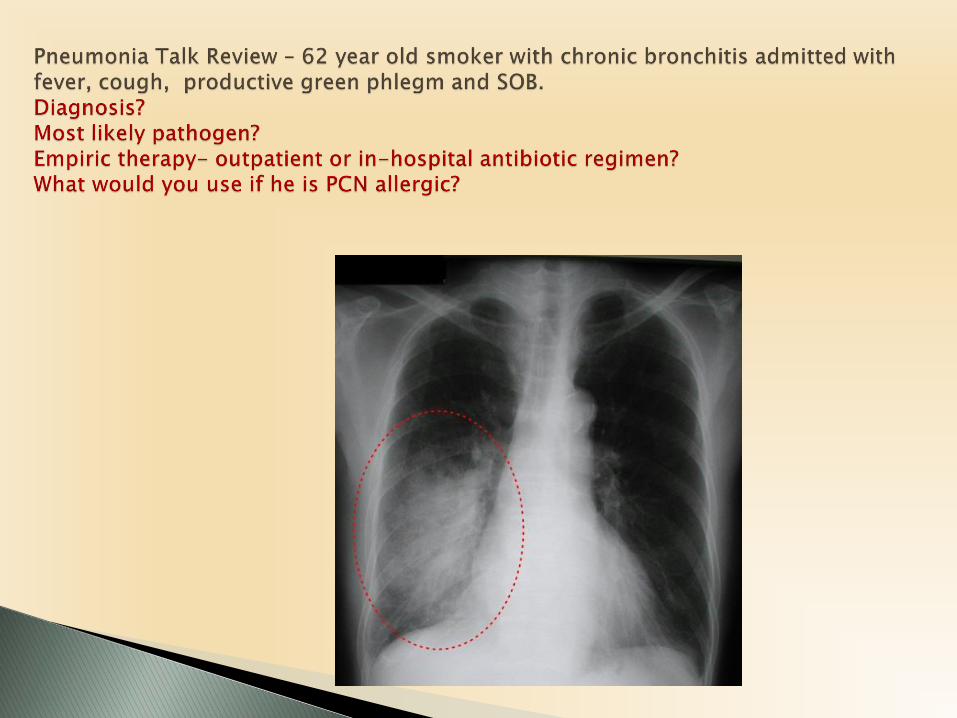
Chest radiography
Blood cultures
Arterial blood gases
Sputum cultures
a. M. pneumoniae
b. S. Pneumoniae
c. C. pneumoniae
d. A virus
e. Legionella
The CURB-65 scale is a simple test to determine pneumonia severity, but it is not a substitute for clinical judgment. Clinicians should assign 1 point for each criteria met by the patient.
•C onfusion •Blood U rea Nitrogen (BUN) >20 mg/dL •R R >/= 30 •B P (systolic <90 mmHg or diastolic </= 60 mmHg) •>/= 65 y.o.
If the individual scores 0-1 points, outpatient treatment is appropriate.
2 points indicates hospitalization and inpatient treatment. Greater than or equal to 3 points warrants inpatient treatment in
the ICU.
The most appropriate antimicrobial for Kathy:
• A macrolide (azithromycin) OR doxycycline• Combination therapy with a macrolide AND doxycycline• Combination therapy with a beta-lactam (high dose amoxicillin,
Augmentin) AND doxycycline• A respiratory fluoroquinolone (levofloxacin, moxifloxacin)
If Kathy had taken antibiotics in the last 3 months, ciprofloxacin would be an appropriate choice.
• True• False
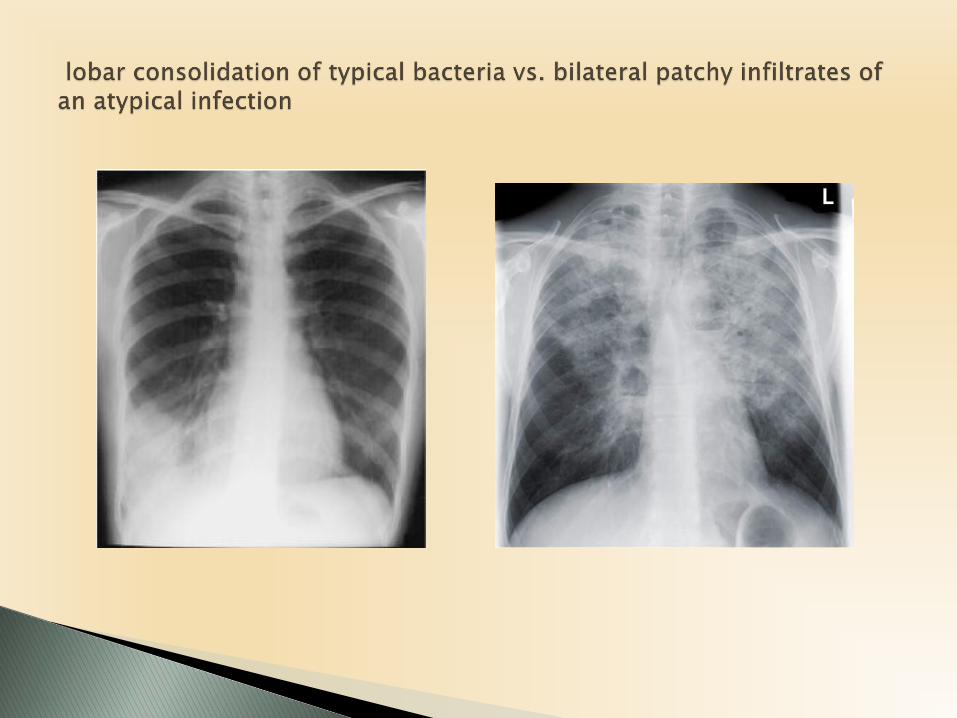
Why classify pneumonia?
Critical difference between these two types as different organisms can be responsible
Pneumonia treatment is almost always initially empiric, therefore knowledge of the likely pathogens is essential in selecting antibiotic regimen
Pneumonia acquired outside the hospital in the immunocompetent host
Often have comorbities that make them susceptible to more severe disease and need for hospitalization - CHF, diabetes, COPD, renal insufficiency, stroke
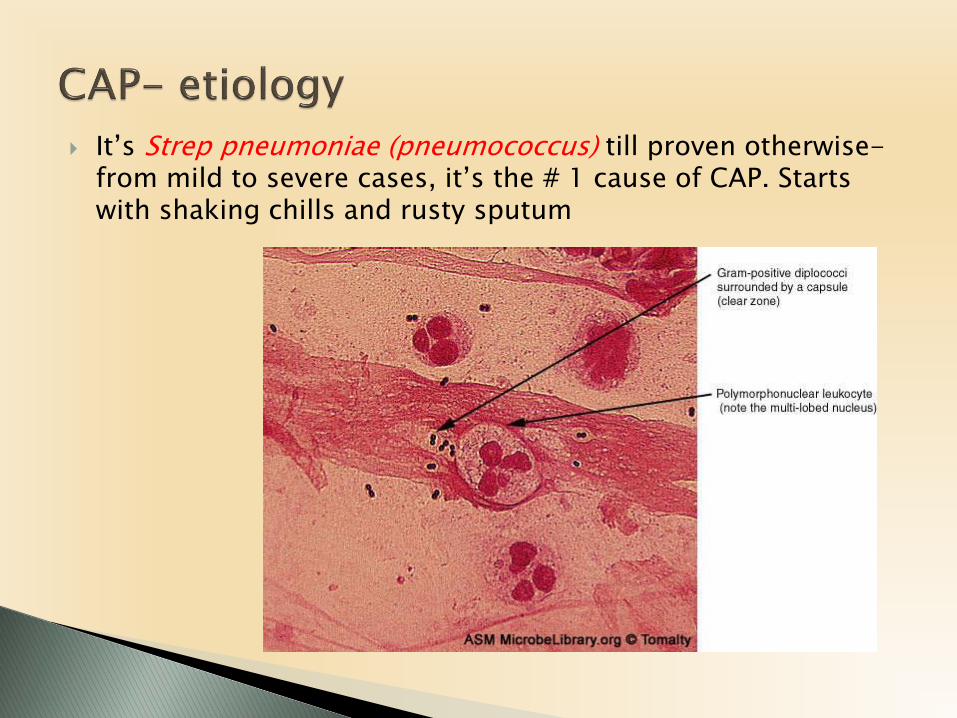
It’s Strep pneumoniae (pneumococcus) till proven otherwise-from mild to severe cases, it’s the # 1 cause of CAP. Starts with shaking chills and rusty sputum
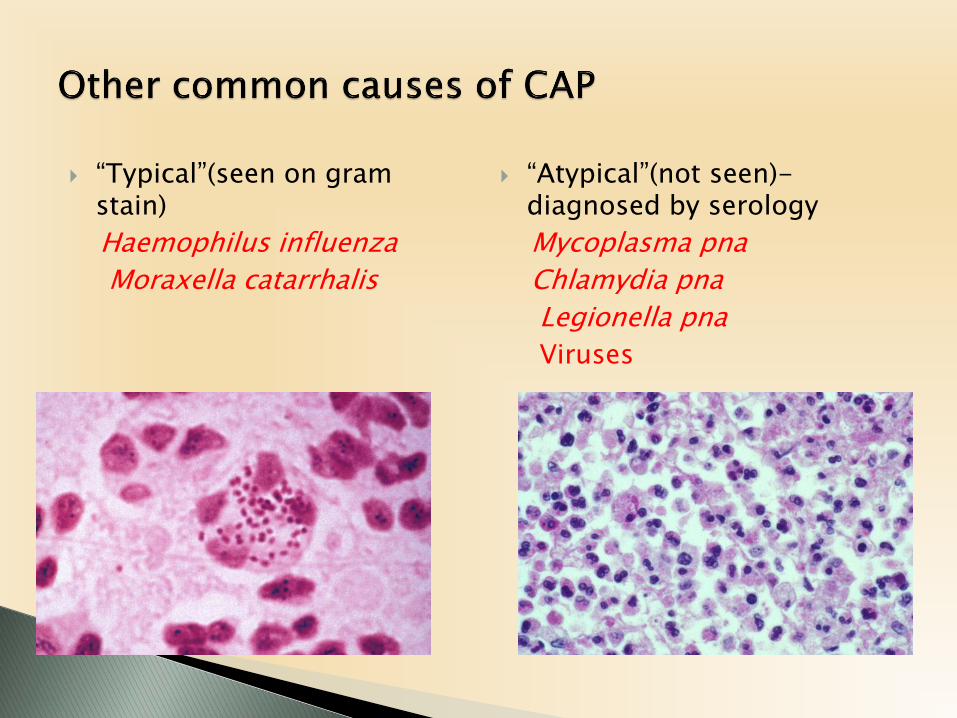
“Typical”(seen on gram stain)
Haemophilus influenza
Moraxella catarrhalis
“Atypical”(not seen)-diagnosed by serology
Mycoplasma pna
Chlamydia pna
Legionella pna
Viruses
Young healthy people, mild disease-
Mycoplasma pneumoniae
Young healthy people with severe disease-
Strep pneumoniae
Smokers-
Strep pneumoniae, Haemophilus influenza, Moraxella catarrhalis
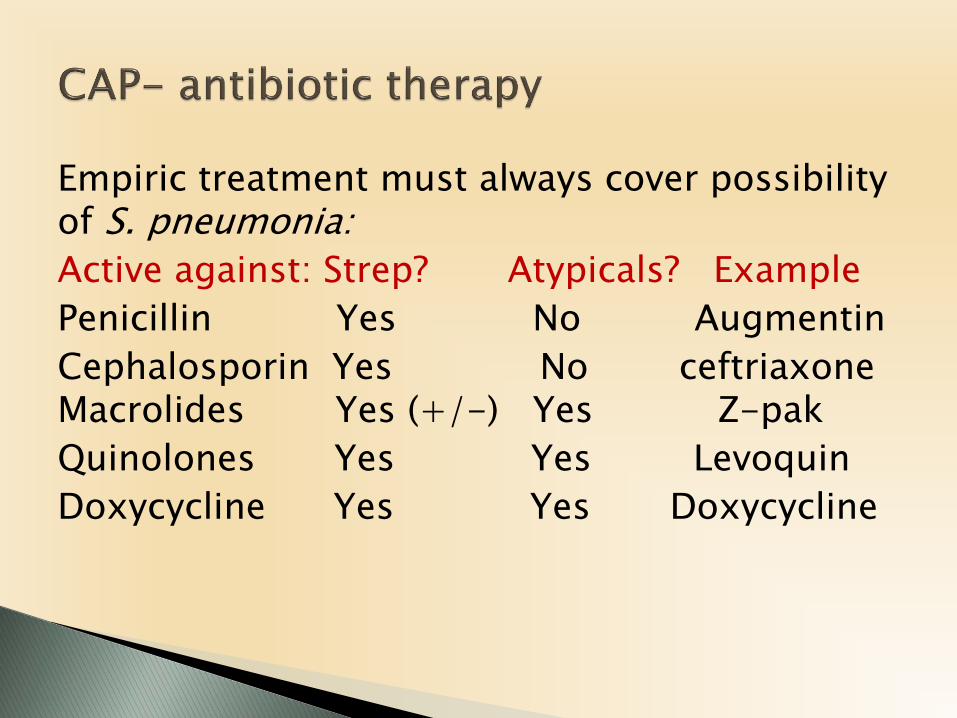
Empiric treatment must always cover possibility of S. pneumonia:
Active against: Strep? Atypicals? Example
Penicillin Yes No Augmentin
Cephalosporin Yes No ceftriaxone Macrolides Yes (+/-) Yes Z-pak
Quinolones Yes Yes Levoquin
Doxycycline Yes Yes Doxycycline
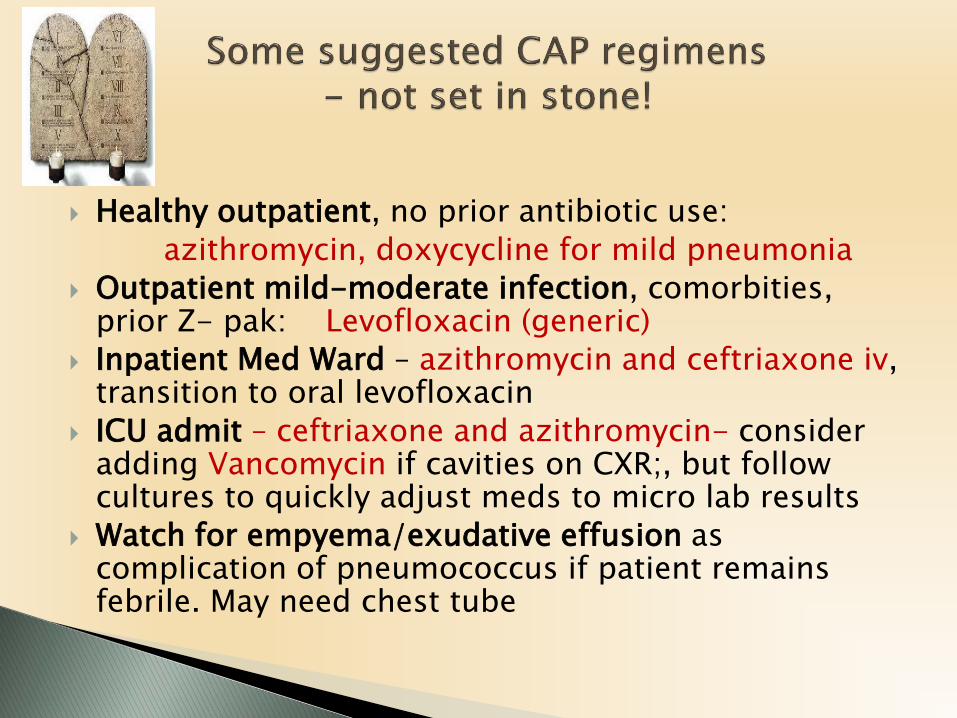
Healthy outpatient, no prior antibiotic use:
azithromycin, doxycycline for mild pneumonia
Outpatient mild-moderate infection, comorbities, prior Z- pak: Levofloxacin (generic)
Inpatient Med Ward – azithromycin and ceftriaxone iv, transition to oral levofloxacin
ICU admit – ceftriaxone and azithromycin- consider adding Vancomycin if cavities on CXR;, but follow cultures to quickly adjust meds to micro lab results
Watch for empyema/exudative effusion as complication of pneumococcus if patient remains febrile. May need chest tube