Embed Size (px)
Citation preview

Chemical composition, radiopacity, and biocompatibility ofPortland cement with bismuth oxideYun-Chan Hwang, DDS, MSD, PhD,a Song-Hee Lee, DDS, MSD,b
In-Nam Hwang, DDS, MSD, PhD,c In-Chol Kang, DDS, MSD, PhD,d
Min-Seok Kim, DDS, MSD, PhD,e Sun-Hun Kim, DDS, MSD, PhD,f
Ho-Hyun Son, DDS, MSD, PhD,g and Won-Mann Oh, DDS, MSD, PhD,h Gwangju, KoreaSCHOOL OF DENTISTRY, DENTAL SCIENCE RESEARCH INSTITUTE, CHONNAM NATIONAL UNIVERSITY
Objective. This study compared the chemical constitution, radiopacity, and biocompatibility of Portland cementcontaining bismuth oxide (experimental cement) with those of Portland cement and mineral trioxide aggregate (MTA).Study design. The chemical constitution of materials was determined by scanning electron miscroscopy and energy-dispersive X-ray analysis. The radiopacity of the materials was determined using the ISO/6876 method. Thebiocompatibility of the materials was tested by MTT assay and tissue reaction.Results. The constitution of all materials was similar. However, the Portland cement and experimental cement weremore irregular and had a larger particle size than MTA. The radiopacity of the experimental cement was similar toMTA. The MTT assay revealed MTA to have slightly higher cell viability than the other materials. However, there wereno statistically significant differences between the materials, with the exception of MTA at 24 h. There was nosignificant difference in the tissue reaction between the experimental groups.Conclusions. These results suggest that the experimental cement may be used as a substitute for MTA. (Oral Surg OralMed Oral Pathol Oral Radiol Endod 2009;107:e96-e102)
Mineral trioxide aggregate (MTA) was developed in1995 at Loma Linda University for use as a root-endfilling material in surgical endodontic treatments.1 Ithas received approval from the U.S. Food and DrugAdministration.2 MTA is commercially available as a
ProRoot MTA (Tulsa Dental Products, Tulsa, OK).Recently, MTA Angelus (Angelus Solucoes Odonto-logicas, Londrina, Brazil) became available on the mar-ket.
MTA has been used for both surgical and nonsurgi-cal applications, such as root-end filling, perforationrepair, resorptive defect repair, direct pulp capping, andapexification.3 Compared with other filling materials,MTA has good sealing ability, superior biocompatibil-ity, and superior antimicrobial activity. Recently, manystudies compared MTA with Portland cement and in-dicated that they had a similar chemical compositionand biocompatiblity.4-7 However, MTA is quite an ex-pensive material. Therefore, Portland cement may be apossible substitute for MTA in endodontics.7
Portland cement is slightly radiopaque but does notmeet the minimum requirements for radiopacity set outin ISO 6876/2001, which is a major disadvantage ofPortland cement if it is to be used clinically.8 MTAconsists of 75 wt% Portland cement, 20 wt% bismuthoxide, and 5 wt% calcium sulfate as a setting modifier.9
Bismuth oxide is a necessary radiopacifier to enable aradiographic assessment of dental materials.10 In thepresent study, an experimental cement containing Port-land cement and bismuth oxide at a ratio of 4:1 wasprepared.
The biocompatibility of a material is also importantfor its clinical use. Recently, it was reported that Port-land cement and MTA are not genotoxins,11,12 and both
The study was financially supported by Chonnam National University.The first 2 authors contributed equally to this work.aAssistant Professor, Department of Conservative Dentistry, Schoolof Dentistry, Dental Science Research Institute, Chonnam NationalUniversity.bGraduate Student, Department of Conservative Dentistry, School ofDentistry, Dental Science Research Institute, Chonnam National Uni-versity.cAssociate Professor, Department of Conservative Dentistry, Schoolof Dentistry, Dental Science Research Institute, Chonnam NationalUniversity.dAssociate Professor, Department of Oral Microbiology, School ofDentistry, Dental Science Research Institute, Chonnam National Uni-versity.eAssociate Professor, Department of Oral Anatomy, School of Dentistry,Dental Science Research Institute, Chonnam National University.fProfessor, Department of Oral Anatomy, School of Dentistry, DentalScience Research Institute, Chonnam National University.gProfessor, Department of Conservative Dentistry, School of Den-tistry, Dental Research Institute, Seoul National University.hProfessor, Department of Conservative Dentistry, School of Dentistry,Dental Science Research Institute, Chonnam National University.Received for publication Jul 15, 2008; returned for revision Nov 13,2008; accepted for publication Nov 15, 2008.1079-2104/$ - see front matter© 2009 All rights reserved.doi:10.1016/j.tripleo.2008.11.015
e96

materials showed similar biocompatibility.13 However,there are few reports on the biocompatibility of Port-land cement mixed with bismuth oxide.
In the present study, it was hypothesized that theradiopacity and biocompatibility of experimental ce-ment made of Portland cement with bismuth oxidewould be similar to MTA. These characteristics wouldpermit its use as a substitute for MTA in clinical situ-ations. To determine the characteristics of the experi-mental cement, the chemical constitution, radiopacity,cytotoxicity, and tissue reactions of the experimentalcement were compared with those of MTA and Port-land cement.
MATERIALS AND METHODSMaterial preparation
The experimental cement used consisted of 75 wt%Portland cement and 25 wt% bismuth oxide and ishereafter referred to as the experimental cement. WhitePortland cement (Union White Cement Industrial Co.,Seoul, Korea) and White MTA (ProRoot MTA, Den-stply Tulsa Dental, Tulsa, OK) were used in this study.
Chemical constitutionThe constitution of MTA, Portland cement, and the
experimental cement was determined by energy-disper-sive X-ray analysis (EDX) attached to a scanning elec-tron microscope (SEM; Hitachi S3000, Wokingham,U.K.). A thin layer of the powder was dispersed over apolymethyl methacrylate slab mounted on an aluminumstub. The samples were carbon coated (K250; Emitech,Ashford, U.K.) for electrical conductivity. The sampleswere then viewed by SEM. EDX was used to determinethe constituent elements of the powders. Three sampleswere made for each material, and the analysis wasperformed 3 times for each sample in different areas.
RadiopacityThe radiopacity of MTA, Portland cement, and the
experimental cement was determined using the methoddescribed by ISO 6876, section 7.7.14 After mixingeach material according to the manufacturer’s instruc-tions, 10 specimens of each material were packed intoa stainless steel ring mold with an internal diameter of10 mm and a depth of 1 mm. The mold was placed ona glass slab before inserting the material. The mold wasthen covered with a glass slide and allowed to set for3 h.
Radiographs were taken with a focus-film distance of!30 cm. The dental X-ray unit was set at 70 kV, 7 mA,and an exposure time of 0.25 s to give a radiographicdensity reading of !2 for the exposed and processedfilm under a 1 mm thick section of the aluminumstepwedge. The radiographs were taken for each sam-
ple. The exposed film was processed in an automaticdeveloping machine.
The photographic densitometer (Model 07-443; Vic-toreen, Cleveland, OH) was used to take readings of theradiographic image of the samples, each step of thestepwedge, and the unexposed part of the film. Threereadings were taken for each film and the mean wascalculated.
The radiographic density values of the materialswere transformed into a radiopacity expressed as theequivalent thickness of aluminum.
Cytotoxicity test: Cell culture and materialextract preparation
Human periodontal ligament (PDL) cells were ob-tained from extracted third molars that were noncariousand had no periodontal disease. The teeth were ex-tracted using an elevator or forceps. Informed consentwas obtained. The PDL cells were primary-cultured inDulbeco’s Modified Eagle Medium (DMEM; Gibco,Grand Island, NY) supplemented with 10% fetal bovineserum (FBS; Gibco) and 1% antibiotics (100 U/mLpenicillin G " 100 #g/mL streptomycin " 0.25 #g/mLamphotericin B; Gibco) at 100% humidity in a 37°CCO2incubator. The cells from the fourth to seventhpassage were used in this study.
The MTA was mixed according to the manufacture’sinstructions. The Portland cement and experimentalcement were sterilized with ethylene oxide and mixedto a consistency similar to MTA in a laminar flow hood.The samples were fabricated in a sterile cylindricalpolyethylene tube, 4 mm in diameter and 6 mm inheight. The material was mixed and placed into thetube. Excess flash was removed and the samples wereexposed to UV light for 30 min for disinfection. Thematerial extracts for the 3-[4,5-dimethyl-thiazol-2-yl]-2,5-diphenyl tetrazolium bromide (MTT) assay wereprepared in a manner similar to the method reportedelsewhere.15 Briefly, 1 sample cylinder was placed intoeach well of a 24-well culture plate and 1 mL DMEMsupplemented with 0.2% FBS and 1% antibiotics wasadded. The sample was kept in a CO2 incubator for72 h. The extract was removed from the well andfiltered for sterilization.
MTT assayThe cells were plated in a 96-well plate at a density of
5.0 $ 103 cells per well and allowed to attach for 24 h.After overnight attachment, each well was treated with100 #L of the material extract. One hundred microliters ofDMEM supplemented with 0.2% fetal bovine serum and1% antibiotics was used as the negative control.
The cell viability was determined from the ability ofthe cells to cleave the MTT to a formazan dye. The
OOOOEVolume 107, Number 3 Hwang et al. e97
medium was removed and 200 #L phosphate-bufferedsaline was added, which was then replaced with 100 #Lcomplete medium and 10 #L of a 5 mg/mL solution ofMTT. The cells were incubated for 4 h at 37°C in a CO2
incubator in the MTT/medium solution. One hundredmicroliters of 6.25% vol/vol 0.1 mol/L NaOH in di-methylsulfoxide solution was added to each well. Theplates were then incubated for 30 min. The opticaldensity was then measured at 490 nm in a multiwellspectrophotometer. The experiment was repeated intriplicate. Two-way analysis of variance was performedto determine the effect of the material and time on thecell viability. Scheffe post hoc analysis was used todetermine the significant differences (P % .05).
Tissue reaction
All experiments using animals were approved by theAnimal Welfare Committee of Chonnam National Uni-
versity. Twenty male Sprague-Dawley rats were used.The MTA, Portland cement, and experimental cementwere investigated. Freshly mixed test materials wereplaced in clean sterile polyethylene tubes, 1 mm indiameter and 10 mm in length, and immediately im-planted subcutaneously in the dorsal region of rats. TheMTA was mixed according to the manufacture’s in-structions. The Portland cement and experimental ce-ment were sterilized with ethylene oxide and mixed toa consistency similar to MTA. An empty tube was usedas control.
After anesthetizing the animals, the dorsal skin wasshaved and disinfected. Four incisions were made throughthe skin using a no. 15 scalpel blade, and 2-cm pocketswere prepared by blunt dissection of the incisions.
The polyethylene tube was carefully implanted in apocket immediately after being loaded with the test ma-terials.
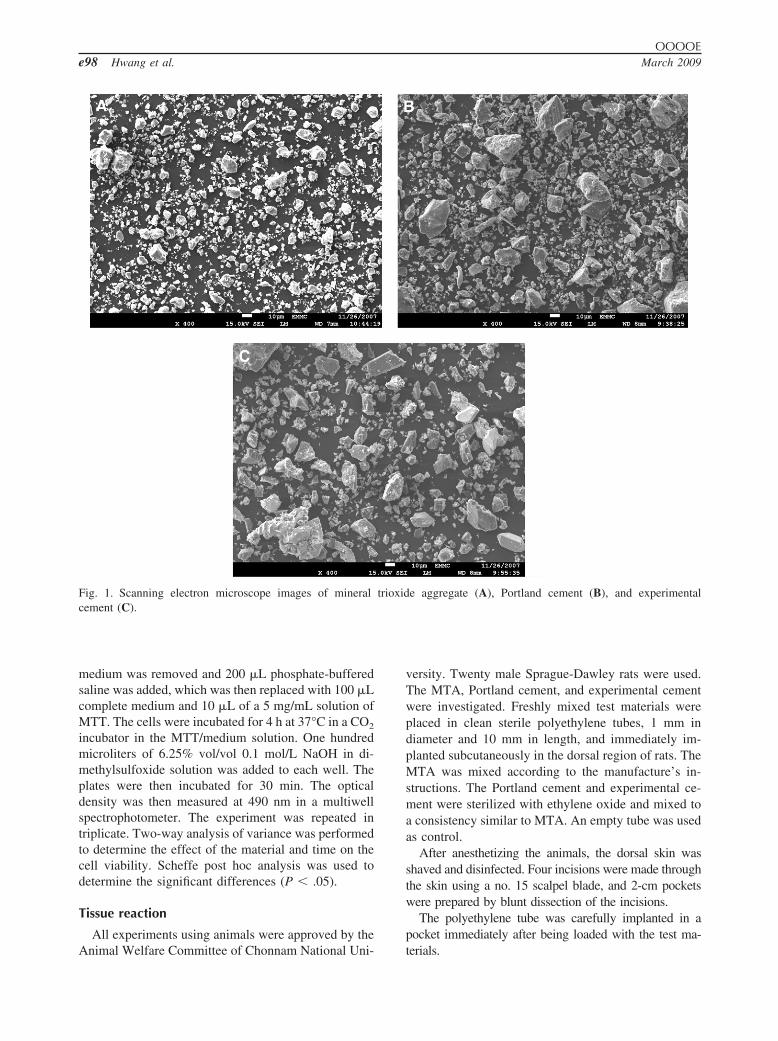
Fig. 1. Scanning electron microscope images of mineral trioxide aggregate (A), Portland cement (B), and experimentalcement (C).
OOOOEe98 Hwang et al. March 2009
The skin was closed with 3/0 silk. The evaluationswere made at 10, 30, and 60 days after surgical implan-tation.
After the experimental periods, all animals wereanesthetized again, the dorsal skin was shaved anddisinfected, and the tubes with the surrounding tissuewere removed in blocks. The animals were killed by anoverdose of anesthesia immediately after removing thetissue samples.
After histology processing, 5-#m-thick serial sec-tions were prepared and stained with hematoxylinand eosin. Tissue sections were made immediately infront of the implanted tube. Histologic evaluationswere made under light microscope. Quantitativeevaluations of the inflammatory cells (lymphocytes,polymorphonuclear leukocytes, macrophages, andgiant cells) were made in 5 separate areas of thesections by observers who were blinded to the pro-cedure. The inflammatory responses were scored andevaluated as: 0, none or few inflammatory cells andno reaction; 1, %25 cells and mild reaction; 2, 25-125 cells and moderate reaction; 3, &125 cells andsevere reaction.16,17 A Kruskal-Wallis test was car-ried out to determine the significant difference forthe inflammatory response of the test materials (P %.05).
RESULTSSEM and EDX
Figure 1 shows SEM images of MTA, Portland ce-ment, and experimental cement. MTA contained smallirregular particles interspersed with some much largerparticles (Fig. 1, A). Portland cement and the experi-mental cement were similar to MTA except for thepresence of coarser and larger particles (Fig. 1,B and C).
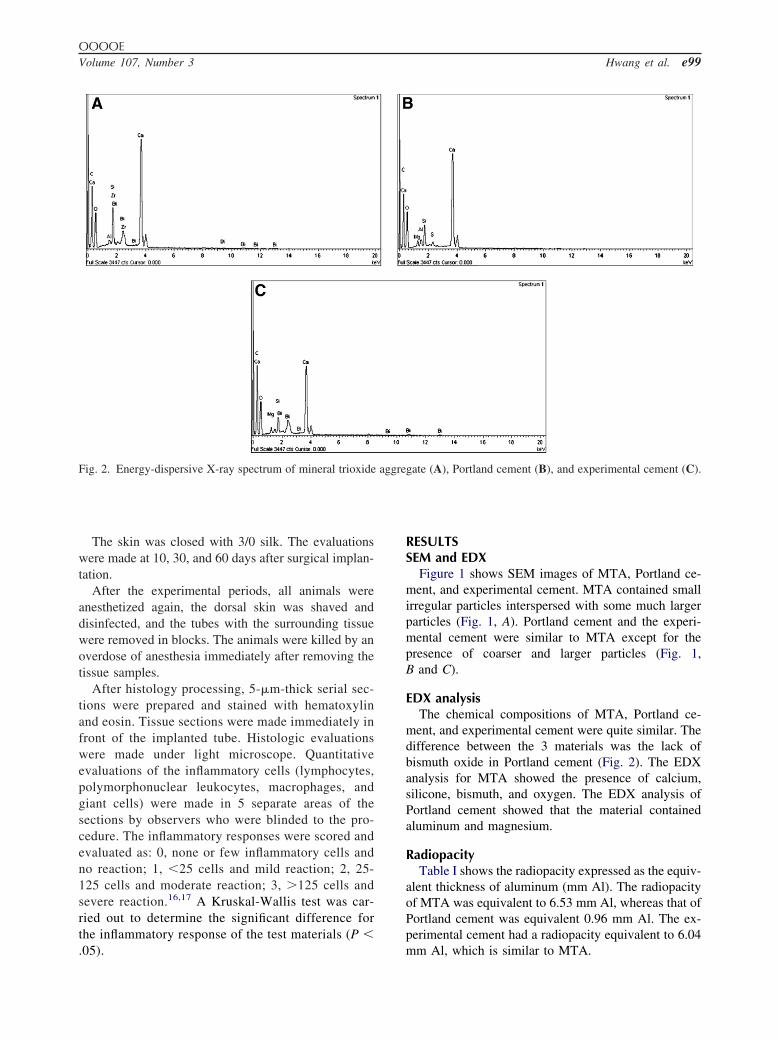
EDX analysisThe chemical compositions of MTA, Portland ce-
ment, and experimental cement were quite similar. Thedifference between the 3 materials was the lack ofbismuth oxide in Portland cement (Fig. 2). The EDXanalysis for MTA showed the presence of calcium,silicone, bismuth, and oxygen. The EDX analysis ofPortland cement showed that the material containedaluminum and magnesium.
RadiopacityTable I shows the radiopacity expressed as the equiv-
alent thickness of aluminum (mm Al). The radiopacityof MTA was equivalent to 6.53 mm Al, whereas that ofPortland cement was equivalent 0.96 mm Al. The ex-perimental cement had a radiopacity equivalent to 6.04mm Al, which is similar to MTA.
Fig. 2. Energy-dispersive X-ray spectrum of mineral trioxide aggregate (A), Portland cement (B), and experimental cement (C).
OOOOEVolume 107, Number 3 Hwang et al. e99
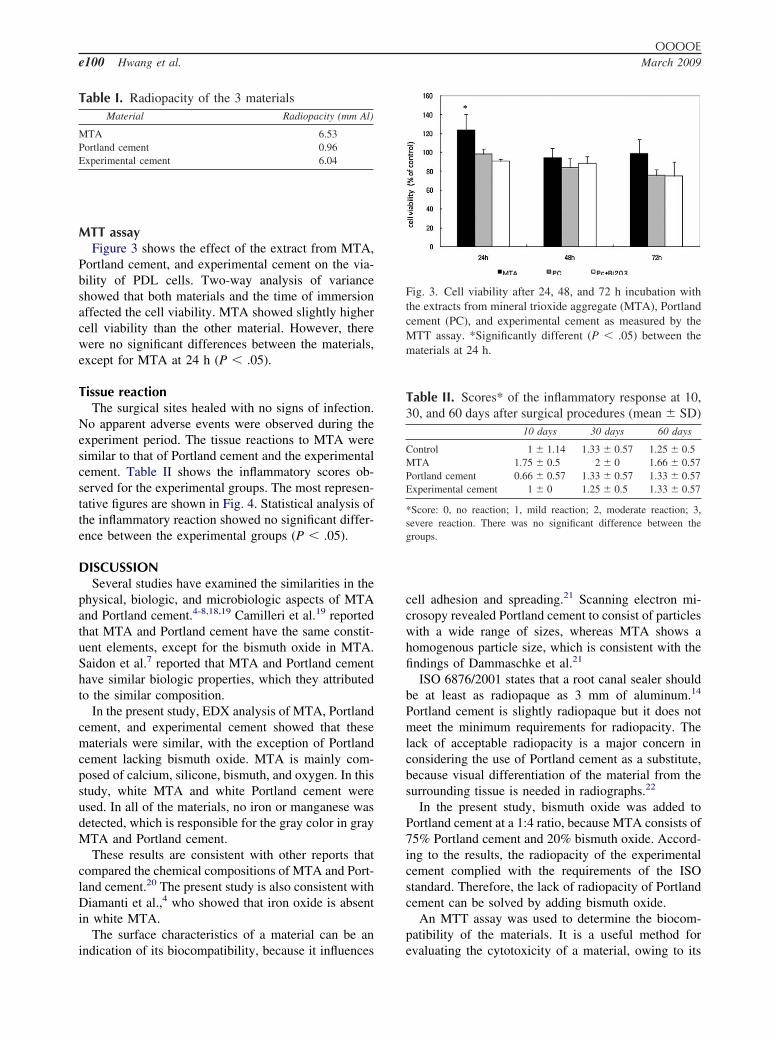
MTT assayFigure 3 shows the effect of the extract from MTA,
Portland cement, and experimental cement on the via-bility of PDL cells. Two-way analysis of varianceshowed that both materials and the time of immersionaffected the cell viability. MTA showed slightly highercell viability than the other material. However, therewere no significant differences between the materials,except for MTA at 24 h (P % .05).
Tissue reactionThe surgical sites healed with no signs of infection.
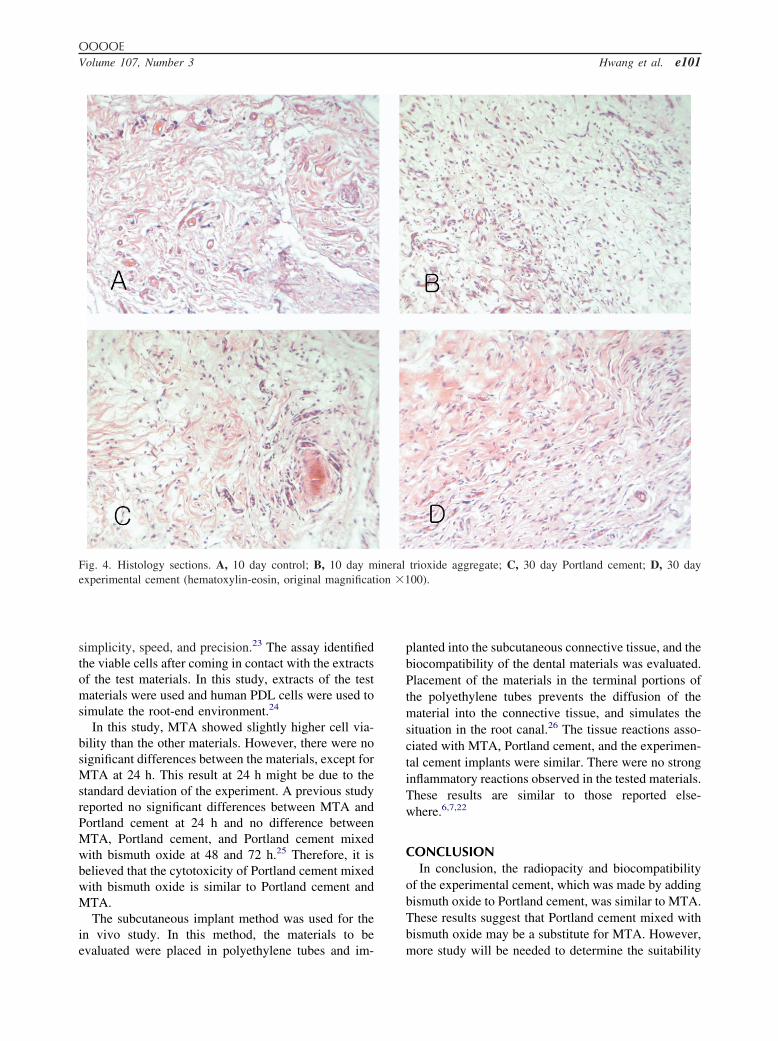
No apparent adverse events were observed during theexperiment period. The tissue reactions to MTA weresimilar to that of Portland cement and the experimentalcement. Table II shows the inflammatory scores ob-served for the experimental groups. The most represen-tative figures are shown in Fig. 4. Statistical analysis ofthe inflammatory reaction showed no significant differ-ence between the experimental groups (P % .05).
DISCUSSIONSeveral studies have examined the similarities in the
physical, biologic, and microbiologic aspects of MTAand Portland cement.4-8,18,19 Camilleri et al.19 reportedthat MTA and Portland cement have the same constit-uent elements, except for the bismuth oxide in MTA.Saidon et al.7 reported that MTA and Portland cementhave similar biologic properties, which they attributedto the similar composition.
In the present study, EDX analysis of MTA, Portlandcement, and experimental cement showed that thesematerials were similar, with the exception of Portlandcement lacking bismuth oxide. MTA is mainly com-posed of calcium, silicone, bismuth, and oxygen. In thisstudy, white MTA and white Portland cement wereused. In all of the materials, no iron or manganese wasdetected, which is responsible for the gray color in grayMTA and Portland cement.
These results are consistent with other reports thatcompared the chemical compositions of MTA and Port-land cement.20 The present study is also consistent withDiamanti et al.,4 who showed that iron oxide is absentin white MTA.
The surface characteristics of a material can be anindication of its biocompatibility, because it influences
cell adhesion and spreading.21 Scanning electron mi-crosopy revealed Portland cement to consist of particleswith a wide range of sizes, whereas MTA shows ahomogenous particle size, which is consistent with thefindings of Dammaschke et al.21
ISO 6876/2001 states that a root canal sealer shouldbe at least as radiopaque as 3 mm of aluminum.14
Portland cement is slightly radiopaque but it does notmeet the minimum requirements for radiopacity. Thelack of acceptable radiopacity is a major concern inconsidering the use of Portland cement as a substitute,because visual differentiation of the material from thesurrounding tissue is needed in radiographs.22
In the present study, bismuth oxide was added toPortland cement at a 1:4 ratio, because MTA consists of75% Portland cement and 20% bismuth oxide. Accord-ing to the results, the radiopacity of the experimentalcement complied with the requirements of the ISOstandard. Therefore, the lack of radiopacity of Portlandcement can be solved by adding bismuth oxide.
An MTT assay was used to determine the biocom-patibility of the materials. It is a useful method forevaluating the cytotoxicity of a material, owing to its
Fig. 3. Cell viability after 24, 48, and 72 h incubation withthe extracts from mineral trioxide aggregate (MTA), Portlandcement (PC), and experimental cement as measured by theMTT assay. *Significantly different (P % .05) between thematerials at 24 h.
Table I. Radiopacity of the 3 materialsMaterial Radiopacity (mm Al)
MTA 6.53Portland cement 0.96Experimental cement 6.04
Table II. Scores* of the inflammatory response at 10,30, and 60 days after surgical procedures (mean ' SD)
10 days 30 days 60 days
Control 1 ' 1.14 1.33 ' 0.57 1.25 ' 0.5MTA 1.75 ' 0.5 2 ' 0 1.66 ' 0.57Portland cement 0.66 ' 0.57 1.33 ' 0.57 1.33 ' 0.57Experimental cement 1 ' 0 1.25 ' 0.5 1.33 ' 0.57
*Score: 0, no reaction; 1, mild reaction; 2, moderate reaction; 3,severe reaction. There was no significant difference between thegroups.
OOOOEe100 Hwang et al. March 2009
simplicity, speed, and precision.23 The assay identifiedthe viable cells after coming in contact with the extractsof the test materials. In this study, extracts of the testmaterials were used and human PDL cells were used tosimulate the root-end environment.24
In this study, MTA showed slightly higher cell via-bility than the other materials. However, there were nosignificant differences between the materials, except forMTA at 24 h. This result at 24 h might be due to thestandard deviation of the experiment. A previous studyreported no significant differences between MTA andPortland cement at 24 h and no difference betweenMTA, Portland cement, and Portland cement mixedwith bismuth oxide at 48 and 72 h.25 Therefore, it isbelieved that the cytotoxicity of Portland cement mixedwith bismuth oxide is similar to Portland cement andMTA.
The subcutaneous implant method was used for thein vivo study. In this method, the materials to beevaluated were placed in polyethylene tubes and im-
planted into the subcutaneous connective tissue, and thebiocompatibility of the dental materials was evaluated.Placement of the materials in the terminal portions ofthe polyethylene tubes prevents the diffusion of thematerial into the connective tissue, and simulates thesituation in the root canal.26 The tissue reactions asso-ciated with MTA, Portland cement, and the experimen-tal cement implants were similar. There were no stronginflammatory reactions observed in the tested materials.These results are similar to those reported else-where.6,7,22
CONCLUSIONIn conclusion, the radiopacity and biocompatibility
of the experimental cement, which was made by addingbismuth oxide to Portland cement, was similar to MTA.These results suggest that Portland cement mixed withbismuth oxide may be a substitute for MTA. However,more study will be needed to determine the suitability
Fig. 4. Histology sections. A, 10 day control; B, 10 day mineral trioxide aggregate; C, 30 day Portland cement; D, 30 dayexperimental cement (hematoxylin-eosin, original magnification $100).
OOOOEVolume 107, Number 3 Hwang et al. e101

of Portland cement mixed with bismuth oxide for clin-ical use.
REFERENCES1. Torabinejad M, Hong CU, McDonald F, Pitt Ford TR. Physical
and chemical properties of a new root-end filling material. JEndod 1995;21:349-53.
2. Torabinejad M, White DJ. Tooth filling material and method ofuse. U.S. Patent No. 5,769,638; June 23, 1998
3. Schwartz RS, Mauger M, Clement DJ, Walker WA III. Mineraltrioxide aggregate: a new material for endodontics. J Am DentAssoc 1999;130:967-75.
4. Diamanti E, Kerezousdis NP, Gakis DB, Tsatsas V. Chemicalcomposition and surface characteristics of grey and new whiteProRoot MTA. J Endod 2003;R81. Abstract.
5. Funteas UR, Wallace JA, Fochtman EW. A comparative analysisof mineral trioxide aggregate and Portland cement. Aus Endod J2003;29:43-4.
6. Holland R, Souza V, Nery MJ, Faraco IM Jr, Bernabe PF,Otoboni Filho JA, Dezan E Jr. Reaction of rat tissue to implanteddentin tube filled with mineral trioxide aggregate, Portland ce-ment or calcium hydroxide. Braz Dent J 2001;12:3-8.
7. Saidon J, He J, Zhu Q, Safavi K, Spangberg LS. Cell and tissuereactions to mineral trioxide aggregate and Portland cement. OralSurg Oral Med Oral Pathol Oral Radiol Endod 2003;95:483-9.
8. Islam I, Chng HK, Yap AU. Comparison of the physical andmechanical properties of MTA and Portland cement. J Endod2006;32:193-7.
9. Torabinejad M, White DJ. Tooth filling material and method ofuse. U.S. Patent No. 5,415,547; May 16, 1995.
10. Coomaraswamy KS, Lumley PJ, Hofmann MP. Effect of bis-muth oxide radioopacifier content on the material properties ofan endodontic Portland cement-based (MTA-like) system. JEndod 2007;33:295-8.
11. Ribeiro DA, Duarte MA, Matsumoto MA, Marques ME, Salva-dori DM. Biocompatibility in vitro tests of mineral trioxideaggregate and regular and white portland cements. J Endod2005;31:605-7.
12. Ribeiro DA, Sugui MM, Matsumoto MK, Duarte MA, MarquesME, Salvadori DM. Genotoxicity and cytotoxicity of mineraltrioxide aggregate and regular and white Portland cements onChinese hamster ovary (CHO) cells in vitro. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2006;101:258-61.
13. De Deus G, Ximenes R, Gurgel-Filho ED, Plotkowski MC,Coutinho-Filho T. Cytotoxicity of MTA and Portland cement onhuman ECV 304 endothelial cells. Int Endod J 2005;38:604-9.
14. International Organization for Standardization. Specification fordental root canal sealing materials. ISO 6876. London: BritishStandards Institution; 1986.
15. Makkawy HA, Koka S, Lavin MT, Ewoldsen NO. Cytotoxicityof root perforation repair materials. J Endod 1998;24:477-9.
16. Federation Dentaire International, Commission on Dental Mate-rials, Equipment, and Therapeutics. Recommended standardpractices for biological evaluation of dental materials. Part 4.11:Subcutaneous implantation test. Int Dent J 1980;30:140-88.
17. Costa CA, Teixeira HM, do Nascimento AB, Hebling J. Bio-compatibility of two current adhesive resins. J Endod2000;26:512-6.
18. Abdullah D, Pitt Ford TR, Papaioannou S, Nicholson J, Mc-Donald F. An evaluation of accelerated Portland cement as arestorative material. Biomaterials 2002;23:401-10.
19. Camilleri J, Montesin FE, Brady K, Sweendy R, Curtis RV, PittFord TR. The constitution of mineral trioxide aggregate. DentMater 2005;21:297-303.
20. Song JS, Mante FK, Romanow WJ, Kim S. Chemical analysis ofpowder and set forms of Portland cement, gray ProRoot MTA,white ProRoot MTA, and gray MTA-Angelus. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2006;102:809-15.
21. Dammaschke T, Gerth HU, Zuchner H, Schafer E. Chemical andphysical surface and bulk material characterization of whiteProRoot MTA and two Portland cements. Dent Mater2005;21:731-8.
22. de Morais CAH, Bernardineli Norberti, Evaluation of tissueresponse to MTA and Portland cement with iodoform. Oral SurgOral Med Oral Pathol Oral Radiol Endod 2006;102:417-21.
23. Vajrabhaya LO, Korsuwannawong S, Jantarat J, Korre S. Bio-compatibility of furcal perforation repair material using cellculture technique: Ketac molar versus ProRoot MTA. Oral SurgOral Med Oral Pathol Oral Radiol Endod 2006;102:48-50.
24. Al-Nazhan S, Spangberg L, Morphological cell changes due tochemical toxicity of a dental material: an electron microscopicstudy on human periodontal ligament fibroblasts and L929 cells.J Endod 1990;16:129-34.
25. Kim EC, Lee BC, Chang HS, Lee W, Hong CU, Min KS.Evaluation of the radiopacity and cytotoxicity of Portland ce-ments containing bismuth oxide. Oral Surg Oral Med Oral PatholOral Radiol Endod 2008;105:54-57.
26. Shahi S, Rahimi S, Lotfi M, Yavari H, Gaderian A. A compar-ative study of the biocompatibility of three root-end filling ma-terials in rat connective tissue. J Endod 2006;32:776-80.
Reprint requests:
Won-Mann Oh, DDS, MSD, PhDDepartment of Conservative DentistrySchool of DentistryChonnam National UniversityHakdong 8, [email protected]
OOOOEe102 Hwang et al. March 2009





























