Embed Size (px)
Citation preview

The Oncotype DX® Breast Cancer Assay helps you find an answer
Oncotype DX helps clarify one of the most difficult treatment questions by providing an individualized Recurrence Score® result that assesses the benefit of chemotherapy and the likelihood of breast cancer recurrence.1,2
CHEMO? NO CHEMO?

CHEMO?
2
Landmark NSABP B-20 trial of 651 estrogen receptor–positive (ER-positive), node-negative breast cancer patients found1:
• Theadditionofchemotherapyprovidedonlya4%absolutebenefit,measuredastheproportionofpatientsfreeofdistantrecurrenceat10years
Do all patients have the same magnitude of benefit from chemotherapy?
Prop
ortio
n w
ithou
t dis
tant
recu
rren
ce
0.2
Years0 2 4 6 8 10 12
0.0
0.1
0.3
0.5
0.7
0.9
0.4
0.6
0.8
1.0 92%
88%
n Events
Tam + chemo 424 30Tam 227 26
P=.02
Proportion of all patients free of distant recurrence at 10 years1
4%ABSOLUTE BENEFITFROM TAM + CHEMO
The Oncotype DX® Breast Cancer Assay is the only test that provides patients with an individual score validated to predict chemotherapy benefit and the likelihood of distant recurrence.1-3
NO CHEMO?
3
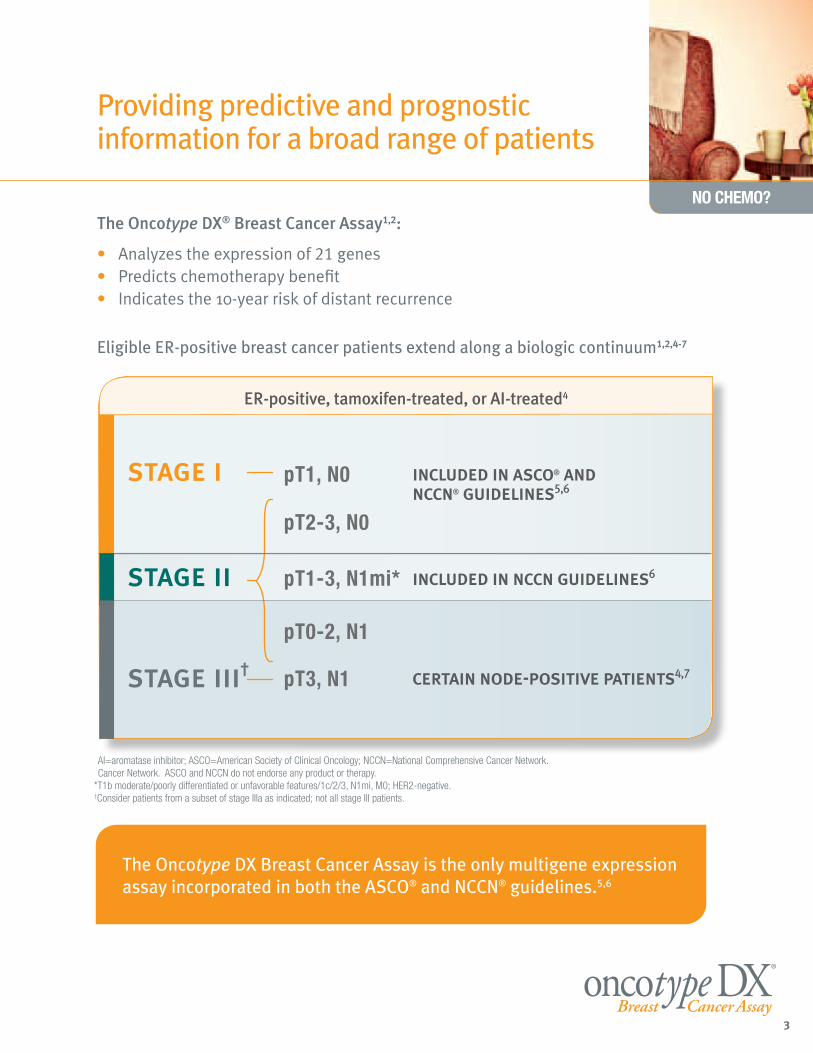
Providing predictive and prognostic information for a broad range of patients
The Oncotype DX® Breast Cancer Assay1,2:
• Analyzestheexpressionof21genes• Predictschemotherapybenefit• Indicatesthe10-yearriskofdistantrecurrence
Eligible ER-positive breast cancer patients extend along a biologic continuum1,2,4-7
included in asco® and nccn® guidelines5,6
stage i
stage ii included in nccn guidelines6
certain node-positive patients4,7 stage iii†
pT1, N0
pT2-3, N0
pT1-3, N1mi*
pT0-2, N1
pT3, N1
ER-positive, tamoxifen-treated, or AI-treated4
AI=aromatase inhibitor; ASCO=American Society of Clinical Oncology; NCCN=National Comprehensive Cancer Network. Cancer Network. ASCO and NCCN do not endorse any product or therapy.
*T1b moderate/poorly differentiated or unfavorable features/1c/2/3, N1mi, M0; HER2-negative.†Consider patients from a subset of stage IIIa as indicated; not all stage III patients.
The Oncotype DX Breast Cancer Assay is the only multigene expression assay incorporated in both the ASCO® and NCCN® guidelines.5,6
CHEMO?
4
Why RT-PCR was chosen for the Oncotype DX® Breast Cancer Assay3:
• Precise,accurate,andhighlyreproducibleoverawidedynamicrange
• Minimizesvariabilitythatmayresultfrom:
—Tissuepreparationmethod,typeoffixative,andfixationtime
—Tumorblockage,storage,andvariabilityinpreparation
—Sampleheterogeneity
• Can be assayed using fixed tissue from core biopsy or surgical excision samples
Genomic Health’s® surgical pathologists take additional steps to ensure accuracy3
• Performmanualmicrodissection
• Clearsamplecontaminants
• Enrichforinvasivetumortissue
With a success rate >97% in generating an accurate result, you can feel confident in the Oncotype DX Breast Cancer Assay.8
Fixedparaffin-embeddedtumorsample.
Accurate, precise, and reproducible
NO CHEMO?
5
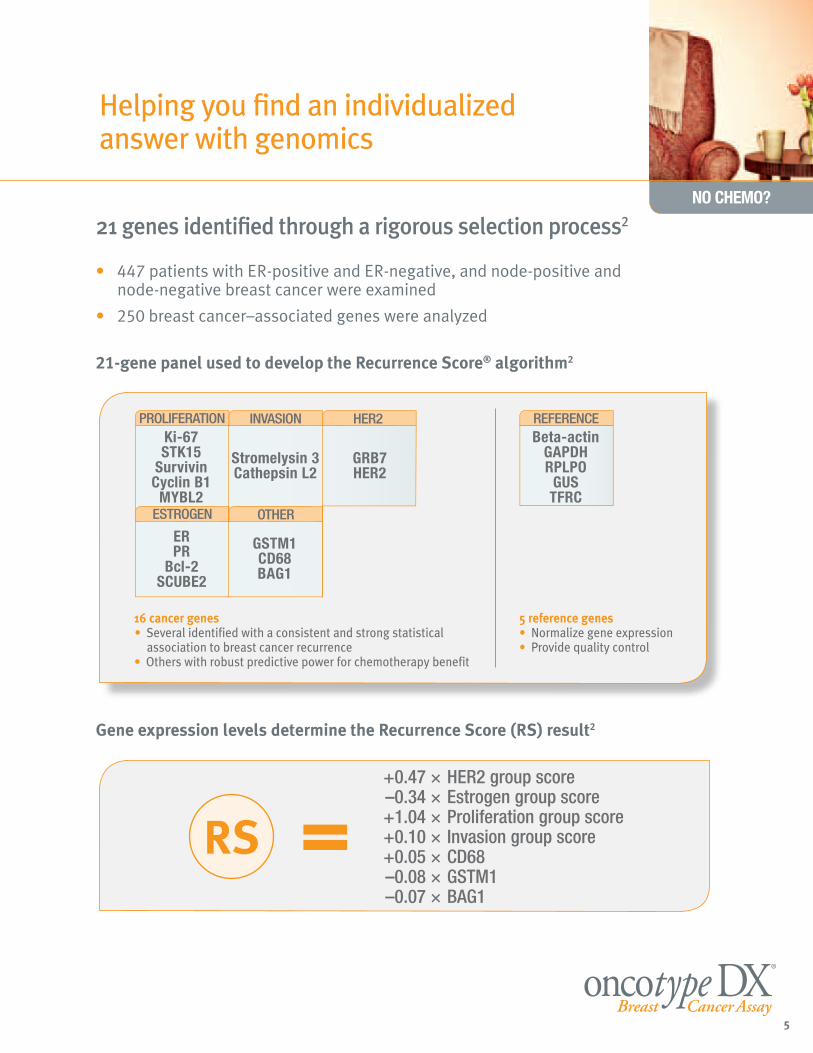
16 cancer genes • Several identified with a consistent and strong statistical
association to breast cancer recurrence• Others with robust predictive power for chemotherapy benefit
5 reference genes• Normalize gene expression • Provide quality control
REFERENCEBeta-actin
GAPDHRPLPO
GUSTFRC
Ki-67STK15
SurvivinCyclin B1
MYBL2
Stromelysin 3Cathepsin L2
GRB7HER2
ERPR
Bcl-2SCUBE2
GSTM1CD68BAG1
PROLIFERATION INVASION HER2
ESTROGEN OTHER
21 genes identified through a rigorous selection process2
• 447patientswithER-positiveandER-negative,andnode-positiveandnode-negativebreastcancerwereexamined
• 250breastcancer–associatedgeneswereanalyzed
21-gene panel used to develop the Recurrence Score® algorithm2
+0.47 × HER2 group score –0.34 × Estrogen group score +1.04 × Proliferation group score +0.10 × Invasion group score +0.05 × CD68 –0.08 × GSTM1 –0.07 × BAG1
RS =
Gene expression levels determine the Recurrence Score (RS) result2
Helping you find an individualized answer with genomics
CHEMO?
6
Rate
of d
ista
nt re
curr
ence
at 1
0 ye
ars
(%)
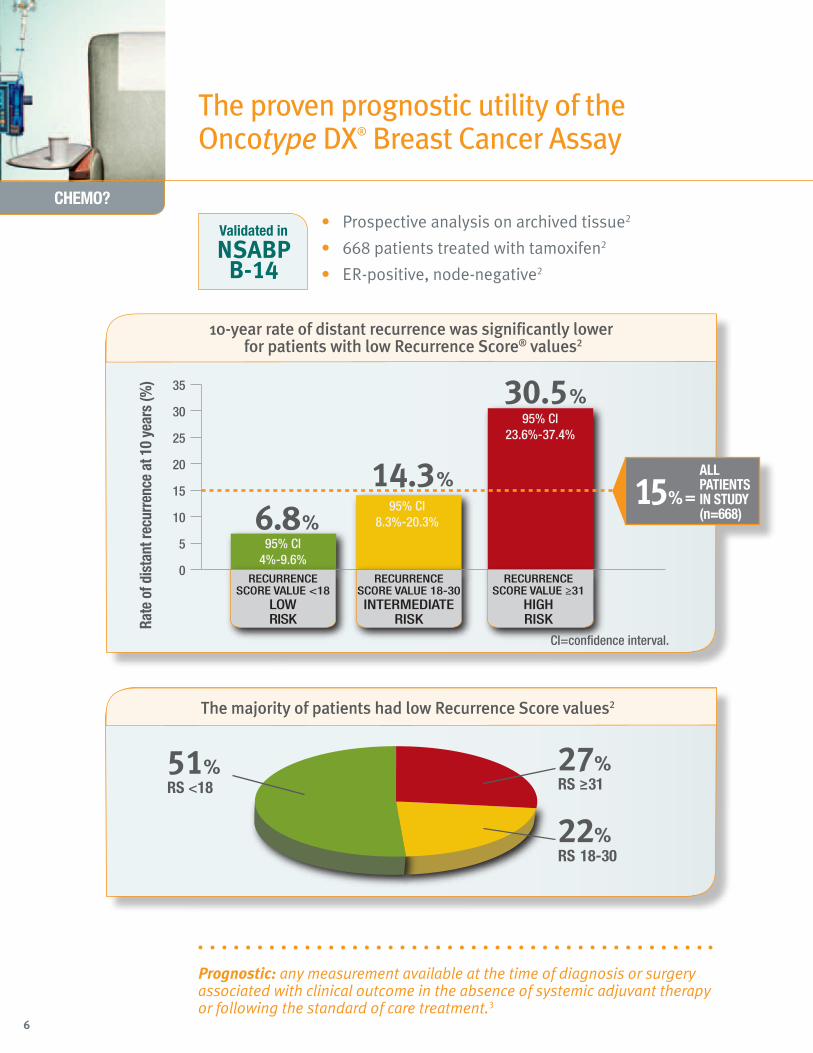
6.8%
0
5
10
15
20
25
30
35
RECURRENCESCORE VALUE <18
LOWRISK
RECURRENCESCORE VALUE 18-30INTERMEDIATE
RISK
RECURRENCESCORE VALUE ≥31
HIGHRISK
14.3%
30.5%
95% Cl4%-9.6%
95% Cl8.3%-20.3%
95% Cl23.6%-37.4%
51%RS <18
27%RS ≥31
22%RS 18-30
CI=confidence interval.
10-year rate of distant recurrence was significantly lower for patients with low Recurrence Score® values2
The majority of patients had low Recurrence Score values2
ALL PATIENTS IN STUDY (n=668)
15%=
• Prospectiveanalysisonarchivedtissue2
• 668patientstreatedwithtamoxifen2
• ER-positive,node-negative2
Prognostic: any measurement available at the time of diagnosis or surgery associated with clinical outcome in the absence of systemic adjuvant therapy or following the standard of care treatment.3
The proven prognostic utility of the Oncotype DX® Breast Cancer Assay
Validated in
NSABP B-14

NO CHEMO?
7
VARIABLE
Age at surgery
Clinical tumor size
Recurrence Score®
HAZARD RATIO
0.71
1.26
3.21*
95% CI
(0.48, 1.05)
(0.86, 1.86)
(2.23, 4.61)
P-VALUE
.08
.23
<.001
Multivariate COX analysis2
*ThehazardratiofortheRecurrenceScoreiscalculatedrelativetoanincrementof50units.
May predict the magnitude of tamoxifen benefit, as shown in a follow-up study to NSABP B-14 (n=645)9†
86%
93%
Years
Prop
ortio
n w
ithou
t dis
tant
recu
rren
ce
0.0
0.2
0.4
0.6
0.8
1.0
2 4 6 8 1610 12 140
n
Placebo 171Tam 142
P=.039
LOW RECURRENCE SCORE VALUE (<18)
Years
Prop
ortio
n w
ithou
t dis
tant
recu
rren
ce
0.0
0.2
0.4
0.6
0.8
1.0
2 4 6 8 1610 12 140
n
Placebo 99Tam 79
P=.82
Years
Prop
ortio
n w
ithou
t dis
tant
recu
rren
ce
0.0
0.2
0.4
0.6
0.8
1.0
2 4 6 8 1610 12 140
n
Placebo 85Tam 69
P=.02
80%
62%
INTERMEDIATE RECURRENCE SCORE VALUE (18-30)
70%
69%
HIGH RECURRENCE SCORE VALUE (≥31)
• Patients with high ER scores (and low Recurrence Score values) saw the largest benefit from treatment with tamoxifen9
Provides significant information about recurrence risk, independent of age and tumor size (P<.001)2
Adding critical information to your treatment decision
†Results should not be used to indicate that tamoxifen should not be given to the high-risk group.3

CHEMO?
8
• Prospectiveanalysisonarchivedtissue1
• 651 patientstreatedwithtamoxifenortamoxifenplusCMF/MF1
• ER-positive,node-negative1
Intermediate Recurrence Score value (18-30); no substantial chemotherapy benefit1*
Years0 2 4 6 8 10 12
Low Recurrence Score® value (<18); little to no chemotherapy benefit1
Prop
ortio
n w
ithou
t dis
tant
recu
rren
ce
Prop
ortio
n w
ithou
t dis
tant
recu
rren
ce
0.1
0.0
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0.1
0.0
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Years0 2 4 6 8 10 12
P=.61 n Events
Tam + chemo 218 8Tam 135 4
P=.39 n Events
Tam + chemo 89 9Tam 45 4
97%
96%
91%
89%
*Clinically important benefit cannot be excluded.
The proven predictive utility of the Oncotype DX® Breast Cancer Assay
Validated in
NSABP B-20

NO CHEMO?
9
Predictive: any measurement associated with benefit or lack of benefit from a particular therapy.3
0.1
0.0
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Years0 2 4 6 8 10 12
28%ABSOLUTE BENEFITFROM TAM + CHEMO
P<.001 n Events
Tam + chemo 117 13Tam 47 18
High Recurrence Score® value (≥31); large chemotherapy benefit1
Abso
lute
incr
ease
in p
ropo
rtio
n fr
eeof
dis
tant
recu
rren
ce (m
ean
± S
E)
0
-10%
10%
20%
30%
40%
RECURRENCESCORE VALUE <18
(n=353)
RECURRENCESCORE VALUE 18-30
(n=134)
RECURRENCESCORE VALUE ≥31
(n=164)
Large reduction in 10-year distant recurrence for high-risk patients treated with chemotherapy1
Prop
ortio
n w
ithou
t dis
tant
recu
rren
ce 88%
60%
Helping you predict the benefit of chemotherapy in node-negative patients

CHEMO?
10
Patient age P=.018
0
20
40
60
80
100
Clinical tumor size P=.001
0
20
40
60
80
100
≤1 cm(n=110)
1.1-2 cm(n=318)
2.1-4 cm(n=196)
>4 cm(n=24)
64% 56% 46% 46%
20% 19% 23% 21%
16% 25% 30% 33%
Recu
rren
ce S
core
val
ueRe
curr
ence
Sco
re v
alue
44%
14%
41%
<40(n=63)
50%
22%
28%
50-59(n=166)
55%
21%
24%
40-49(n=226)
60%
21%
19%
≥60(n=196)
<18 18-30 ≥31
Recurrence Score® value
NSABP B-20 trial (n=651)1
NSABP B-20 trial (n=651)1
• YoungerpatientscanhavelowRecurrenceScorevalues1
• OlderpatientscanhavehighRecurrenceScorevalues1
• PatientswithlargertumorscanhavelowRecurrenceScorevalues1
• PatientswithsmallertumorscanhavehighRecurrenceScorevalues1
Additional insight may help guide your treatment decision

NO CHEMO?
11
0
20
40
60
80
100
Tumor grade (central)
grading by pathologist at central lab
P<.001
WELL(n=119)
MODERATE(n=340)
POOR(n=190)
Recu
rren
ce S
core
val
ue
64%
24%
12%
19%
19%
61%
83%
12%
5%
Tumor grade (site) P<.001
0
20
40
60
80
100grading by pathologist at local hospital
WELL(n=77)
MODERATE(n=339)
Recu
rren
ce S
core
val
ue
56%
22%
22%
36%
22%
42%
POOR(n=163)
73%
16%
12%
<18 18-30 ≥31
Recurrence Score® value
NSABP B-20 trial (n=651)1
• Significantproportionsofhigh-gradetumorshavelowRecurrenceScorevalues1
• Evenlow-gradetumorscanhavehighRecurrenceScorevalues1
Providing independent, significant data beyond traditional measures
Nearly 1 in 3 adjuvant treatment recommendations were changed based on the Recurrence Score results in a decision impact study.10

CHEMO?
12
• Prospectiveanalysisonarchivedtissue4
• 1,231postmenopausalpatientstreatedwithtamoxifenorAl4
• 1,178ER-positive,node-positive,andnode-negative4
Comparative risks were seen in node-negative patients and patients with 1 to 3 nodes who had low Recurrence Score® values3,4
9-ye
ar ri
sk o
f dis
tant
recu
rren
ce (%
)
Recurrence Score value
10
0
20
30
40
50
60
70
80
90
100
4+ POSITIVE NODESn=63
(31 EVENTS)
1-3 POSITIVE NODESn=243
(43 EVENTS)
NODE-NEGATIVE
n=872(72 EVENTS)
0 5 10 15 20 25 40 4530 35 50
Mean95% Cl
Providing independent recurrence risk information across a biologic continuum
Validated in
Trans ATAC
Oncotype DX® is the only multigene expression assay incorporated in the NCCN® guidelines to help guide chemotherapy treatment decisions in patients with micrometastases.6

NO CHEMO?
13
92%
87%
Brea
st c
ance
r−sp
ecifi
c su
rviv
al
0.0
0.25
0.50
0.75
1.00
2 4 6 8 100
n Events
Tam only 55 4CAF-T 91 10
P=.56
LOW RECURRENCE SCORE VALUE (<18)
Years
Brea
st c
ance
r−sp
ecifi
c su
rviv
al
0.0
0.25
0.50
0.75
1.00
2 4 6 8 100
n Events
Tam only 46 11CAF-T 57 10
P=.89
81%
70%
INTERMEDIATE RECURRENCE SCORE VALUE (18-30)
Brea
st c
ance
r−sp
ecifi
c su
rviv
al
Years
Years
0.0
0.25
0.50
0.75
1.00
2 4 6 8 100
n Events
Tam only 47 20CAF-T 71 18
P=.033
73%
54%
HIGH RECURRENCE SCORE VALUE (≥31)
• Prospectiveanalysisonarchivedtissue7
• 367 postmenopausalpatientstreatedwithtamoxifenortamoxifenplusCAF7
• HR-positive,node-positive7
Helping you predict the benefit of chemotherapy in node-positive patients
Half of adjuvant treatment recommendations for node-positive patients were changed based on the Recurrence Score result in a decision impact survey11
• For33.3%ofpatientstestedwithOncotypeDX®,theirtreatmentwaschangedfromchemotherapyplushormonaltherapytohormonaltherapyalone
• For9.4%ofpatientstestedwithOncotypeDX,theirtreatmentwaschangedfromhormonaltherapyalonetochemotherapyplushormonaltherapy
Strong chemotherapy benefit seen only in the high Recurrence Score® value group7
• NosubstantialbenefitinBreastCancerSpecificSurvivalfromanthracyclinebasedchemotherapyfornode-positivepatientswithlowerRecurrenceScorevalues
Validated in
SWOG 8814

CHEMO?
14
PATIENT REPORTPatient/ID: Doe, Jane Sex: FemaleDOB: 01/01/1950Medical Record/Patient #: 556677771Date of Surgery: 9/25/2008Specimen Type/ID: Breast/SURG-0001
Requisition: R00003GOrder Received: 10/15/2008Date Reported: 10/23/2008Client: Community Medical CenterOrdering Physician: Dr. Harry D SmithSubmitting Pathologist: Dr. John P WilliamsSubmitting Pathologist: Dr. Sally M Jones
BREAST CANCER ASSAY DESCRIPTIONOncotype DX Breast Cancer Assay uses RT-PCR to determine the expression of a panel of 21 genes in tumor tissue.The Recurrence Score® is calculated from the gene expression results. The Recurrence Score range is from 0-100.
RESULTS
Breast CancerRecurrence Score = 6
The findings summarized in the Clinical Experience sections of this report areapplicable to the patient populations defined in each section. It is unknownwhether the findings apply to patients outside these criteria.
CLINICAL EXPERIENCE: PROGNOSIS FOR NODE NEGATIVE, ER-POSITIVE PATIENTSThe Clinical Validation study included female patients with Stage I or II, Node Negative, ER-Positivebreast cancer treated with 5 years of tamoxifen. Those patients who had a Recurrence Score of 6
had an Average Rate of Distant Recurrence of 5% (95% CI: 3%-7%)The following results are from a clinical validation study of 668 patients from the NSABP B-14 study. N Engl J Med 2004; 351: 2817-26.
Recurrence Score vs Distant Recurrence in Node Negative, ER-Positive Breast Cancer Prognosis
Page 1 of 3Genomic Health, Inc.301 Penobscot DriveRedwood City, CA 94063 USAToll Free Tel 866-ONCOTYPE (866-662-6897)Worldwide Tel +1 650-569-2080www.oncotypeDX.com
Laboratory Director: Patrick Joseph, MD CLIA Number 05D1018272This test was developed and its performance characteristics determined by Genomic Health, Inc. The laboratory is regulated under the Clinical Laboratory ImprovementAmendments of 1988 (CLIA) as qualified to perform high-complexity clinical testing. This test is used for clinical purposes. It should not be regarded as investigational or forresearch. These results are adjunctive to the ordering physician's workup.
Online Ordering and Reports Available — Please contact Customer Service at [email protected]© 2004-2010 Genomic Health, Inc. All rights reserved. Oncotype DX and Recurrence Score are registered trademarks of Genomic Health, Inc.
GHI004 Rev017
• Thereportalsocontainspredictiveinformationaboutchemotherapybenefit,validatedintheNSABPB-20study1
• Fornode-positivepatients,thereportalsoincludesbothpredictiveandprognosticinformation,asvalidatedintheSWOG8814study7
The first page of the report contains the individualized Recurrence Score®
result between 0 and 100.
Estimate of the likelihood of distant recurrence at 10 years.
The Oncotype DX® Breast Cancer report

NO CHEMO?
15
PATIENT REPORTPatient/ID: Doe, Jane Sex: FemaleDOB: 01/01/1950
Requisition: R00003GOrder Received: 10/15/2008Date Reported: 10/23/2008
QUANTITATIVE SINGLE GENE REPORTThe Oncotype DX assay uses RT-PCR to determine the RNA expression of the genes below. These results may differ from ER, PR, or HER2results reported using other methods or reported by other laboratories.1
The ER, PR, and HER2 Scores are also included in the calculation of the Recurrence Score.
ER Score = Positive
The ER Score positive/negative cut-off of 6.5 units was validated from a study of 761 samples using the 1D5 antibody (immunohistochemistry)and 607 samples using the SP1 antibody (immunohistochemistry). The standard deviation for the ER Score is less than 0.5 units.2
Clinical Experience:For ER positive breast cancer, the magnitude of tamoxifen benefit increases as the ER Score increases from 6.5 to 12.5.3
Please note: The Average Rate of Distant Recurrence reported on Page 1 based on the Recurrence Score was determined in patients whoreceived 5 years of tamoxifen treatment and takes into account the magnitude of tamoxifen benefit indicated by the ER Score.
PR Score = Positive
The PR Score positive/negative cut-off of 5.5 units was validated from a study of 761 samples using the PR636 antibody(immunohistochemistry) and another study of 607 samples using the PR636 antibody (immunohistochemistry). The standard deviation for thePR Score is less than 0.5 units.2
HER2 Score = Negative
The HER2 positive cut-off of 11.5 units, equivocal range from 10.7 to 11.4 units, and negative cut-off of < 10.7 units were validated fromconcordance studies of 755 samples using the HercepTest™ assay (immunohistochemistry) and another study of 568 samples using thePathVysion® assay (FISH). The standard deviation for the HER2 score is less than 0.5 units.4
References:1. ER Score based on quantitative ESR1 expression (estrogen receptor); PR Score based on quantitative PGR expression (progesterone receptor); HER2 Scorebased on quantitative ERBB2 expression.2. ASCO Breast Cancer Symposium 2007 Abstracts #87 by S.S. Badve et al., and #88 by F.L. Baehner et al.3. ASCO Annual Meeting 2005 Abstract #510 by S. Paik et al.4. ASCO Breast Cancer Symposium 2008 Abstracts #13 by F.L. Baehner et al., and #41 by F.L. Baehner et al.
Page 3 of 3Genomic Health, Inc.301 Penobscot DriveRedwood City, CA 94063 USAToll Free Tel 866-ONCOTYPE (866-662-6897)Worldwide Tel +1 650-569-2080www.oncotypeDX.com
Laboratory Director: Patrick Joseph, MD CLIA Number 05D1018272This test was developed and its performance characteristics determined by Genomic Health, Inc. The laboratory is regulated under the Clinical Laboratory ImprovementAmendments of 1988 (CLIA) as qualified to perform high-complexity clinical testing. This test is used for clinical purposes. It should not be regarded as investigational or forresearch. These results are adjunctive to the ordering physician's workup.
Online Ordering and Reports Available — Please contact Customer Service at [email protected]© 2004-2010 Genomic Health, Inc. All rights reserved. Oncotype DX and Recurrence Score are registered trademarks of Genomic Health, Inc.
GHI004 Rev017
Quantitative ER, PR, and HER2 scores,
which are highly concordant with
IHC and FISH3,12,13
Sign up now for the Customer Portal at https://online.genomichealth.com:• Onlineordering• Onlineresults• Importantcustomerinformationpostings
Call Customer Service at 866-ONCOTYPE to open an account.
Helping to make a more informed decision with quantitative data
Genomic Health® accepts all early-stage breast cancer samples
to help confirm or clarify ER status

The Oncotype DX® Breast Cancer Assay helps you find an answer
CHEMO? NO CHEMO?
A personalized approach to breast cancer treatment
• Validatedthroughanextensivesuiteofstudies,acrossacontinuumofmorethan4,000ER-positivepatientsin13clinicalstudies1,2,4,7
• OnlytestincorporatedinboththeASCO®andNCCN®guidelinestohelpguidechemotherapytreatmentdecisions5,6
• Clinicalutilityinnode-negativeandcertainnode-positive,ER-positivebreastcancerpatients1,2,4-7
• Changedadjuvanttreatmentrecommendationsforasignificantproportionofbothnode-negativeandnode-positivepatients10,11
• GenomicHealth®iscommittedtomakingOncotypeDXavailabletoyourpatients3
—Extensivelyreimbursed,withmorethan95%ofprivatelyinsuredlivesandMedicarebeneficiariescoveredforthetest,aswellasexpandingcoverageinnode-positivepatients
—Providesnumerousservicestoeasethereimbursementprocessforyou,yourstaff,andyourpatientsthroughtheGenomicAccessProgram(GAP)
• GenomicHealthisaCLIA-certified,CAP-accreditedreferencelaboratory
For Customer Service, please contact 866-ONCOTYPE (866-662-6897) or e-mail [email protected] within the United States, and +1-650-569-2028 or e-mail [email protected] outside the United States.www.oncotypeDX.com
References:1. PaikS,etal.Geneexpressionandbenefitofchemotherapyinwomenwithnode-negative,estrogenreceptor–positivebreastcancer.J Clin Oncol.2006;24(23):3726-3734.2.PaikS,etal.Amultigeneassaytopredictrecurrenceoftamoxifen-treated,node-negativebreastcancer.N Engl J Med.2004;351(27):2817-2826.3.Dataonfile.GenomicHealth,RedwoodCity,CA.4.DowsettM,etal.RiskofdistantrecurrenceusingOncotypeDXinpostmenopausalprimarybreastcancerpatientstreatedwithanastrozoleortamoxifen:aTransATACstudy.Abstractpresentedat:31stAnnualSanAntonioBreastCancerSymposium;December10-14,2008;SanAntonio,TX.Abstract53.5.HarrisL,etal.AmericanSocietyofClinicalOncology2007updateofrecommendationsfortheuseoftumormarkersinbreastcancer.J Clin Oncol.2007;25(33):5287-5312.6.NationalComprehensiveCancerNetwork®.NCCNClinicalPracticeGuidelinesinOncology™:breastcancer:V.1.2009.http://www.nccn.org.PublishedDecember2,2008.AccessedDecember22,2009.7.AlbainKS,etal;forTheBreastCancerIntergroupofNorthAmerica.Prognosticandpredictivevalueofthe21-geneRecurrenceScoreassayinpostmenopausalwomenwithnode-positive,oestrogen-receptor-positivebreastcanceronchemotherapy:aretrospectiveanalysisofarandomisedtrial.Lancet Oncol.2010;11(1):55-65.8.AndersonJM,etal.MolecularcharacterizationofbreastcancercorebiopsyspecimensbygeneexpressionanalysisusingstandardizedquantitativeRT-PCR.Posterpresentedat:32ndAnnualSanAntonioBreastCancerSymposium;December9-13,2009;SanAntonio,TX.Poster6021.9.PaikS,etal.Expressionofthe21genesintheRecurrenceScoreassayandtamoxifenclinicalbenefitintheNSABPstudyB-14ofnodenegative,estrogenreceptorpositivebreastcancer.J Clin Oncol.2005;23(16S)(suppl).Abstract510.10.LoSS,etal.Prospectivemulticenterstudyoftheimpactofthe21-geneRecurrenceScoreassayonmedicaloncologistandpatientadjuvantbreastcancertreatmentselection[publishedonlineaheadofprintJanuary11,2010].J Clin Oncol.doi:10.1200/JCO.2008.20.2119.11.OratzR,etal.Effectofa21-genereverse-transcriptasepolymerasechainreactionassayontreatmentrecommendationsforpatientswithlymphnode–positiveandestrogenreceptor–positivebreastcancer.Posterpresentedat:32ndAnnualSanAntonioBreastCancerSymposium;December9-13,2009;SanAntonio,TX.Poster2031.12.BadveSS,etal.Estrogen-andprogesterone-receptorstatusinECOG2197:comparisonofimmunohistochemistrybylocalandcentrallaboratoriesandquantitativereversetranscriptionpolymerasechainreactionbycentrallaboratory.J Clin Oncol.2008;26(15):2473-2481.13.BaehnerFL,etal.AKaiser-Permanentepopulation-basedstudyofERandPRexpressionbythestandardmethod,immunohistochemistry(IHC),comparedtoanewmethod,quantitativereversetranscriptionpolymerasechainreaction(RT-PCR).Presentedat:2007AmericanSocietyofClinicalOncologyBreastCancerSymposium;September7-8,2007;SanFrancisco,CA.Abstract88.
© 2010 Genomic Health, Inc. All rights reserved. GHI201 12/10GenomicHealth,OncotypeDX,andRecurrenceScore®areregisteredtrademarksofGenomicHealth,Inc.
Oncotype DX is now available for patients with stage II colon cancer, expanding Genomic Health’s technology to other cancer types.
AmericanSocietyofClinicalOncology(ASCO)andASCOareregisteredtrademarksofASCO;NationalComprehensiveCancerNetwork(NCCN)andNCCNareregisteredtrademarksofNCCN.ASCOandNCCNdonotendorseanyproductortherapy.





























