Embed Size (px)
Citation preview
Copyright (C) by the Congress of Neurological Surgeons
Volume 44(5) May 1999 pp 1005-1017
Chiari I Malformation Redefined: Clinical and Radiographic Findings for 364 Symptomatic Patients
[Clinical Studies]
Milhorat, Thomas H. M.D.; Chou, Mike W. M.D.; Trinidad, Elizabeth M. M.D.; Kula, Roger W. M.D.; Mandell, Menachem M.D.; Wolpert, Chantelle M.B.A., P.A.-C.; Speer, Marcy C. Ph.D.
Departments of Neurosurgery (THM, MWC, EMT), Neurology (RWK), and Radiology (MM), State University of New York Health Science Center at Brooklyn, Brooklyn, New York; The Long Island College Hospital (THM, MWC, EMT, RWK), Brooklyn, New York; and the Department of Medicine (CW, MCS), Section of Medical Genetics, Duke University Medical Center, Durham, North Carolina
Received, June 26, 1998. Accepted, January 6, 1999. Reprint requests: Thomas H. Milhorat, M.D., Department of Neurosurgery, SUNY-Health Science Center at Brooklyn,
450 Clarkson Avenue, Box 1189, Brooklyn, NY 11203-2098.
Outline
l Abstract l PATIENTS AND METHODS
l Patients l Baseline assessments l Morphological features of the PCF l Volume of the PCF l Pedigree development and assessment of familial aggregation l Statistical analyses
l RESULTS l Clinical presentation l Clinical syndrome l MRI findings l Quantitative measurements of the PCF l Clinicoradiological correlations l Familial incidence and inheritance patterns
l DISCUSSION l CONCLUSIONS l ACKNOWLEDGMENTS l REFERENCES
Graphics
Page 1 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
l Table 1 l Figure 1 l Table 2 l Table 3 l Table 4 l Table 5 l Table 6 l Figure 2 l Table 7 l Figure 3
Abstract
OBJECTIVE: Chiari malformations are regarded as a pathological continuum of hindbrain maldevelopments characterized by downward herniation of the cerebellar tonsils. The Chiari I malformation (CMI) is defined as tonsillar herniation of at least 3 to 5 mm below the foramen magnum. Increased detection of CMI has emphasized the need for more information regarding the clinical features of the disorder.
METHODS: We examined a prospective cohort of 364 symptomatic patients. All patients underwent magnetic resonance imaging of the head and spine, and some were evaluated using CINE-magnetic resonance imaging and other neurodiagnostic tests. For 50 patients and 50 age- and gender-matched control subjects, the volume of the posterior cranial fossa was calculated by the Cavalieri method. The families of 21 patients participated in a study of familial aggregation.
RESULTS: There were 275 female and 89 male patients. The age of onset was 24.9 +/- 15.8 years (mean +/- standard deviation), and 89 patients (24%) cited trauma as the precipitating event. Common associated problems included syringomyelia (65%), scoliosis (42%), and basilar invagination (12%). Forty-three patients (12%) reported positive family histories of CMI or syringomyelia. Pedigrees for 21 families showed patterns consistent with autosomal dominant or recessive inheritance. The clinical syndrome of CMI was found to consist of the following: 1) headaches, 2) pseudotumor-like episodes, 3) a Meniere's disease-like syndrome, 4) lower cranial nerve signs, and 5) spinal cord disturbances in the absence of syringomyelia. The most consistent magnetic resonance imaging findings were obliteration of the retrocerebellar cerebrospinal fluid spaces (364 patients), tonsillar herniation of at least 5 mm (332 patients), and varying degrees of cranial base dysplasia. Volumetric calculations for the posterior cranial fossa revealed a significant reduction of total volume (mean, 13.4 ml) and a 40% reduction of cerebrospinal fluid volume (mean, 10.8 ml), with normal brain volume.
CONCLUSION: These data support accumulating evidence that CMI is a disorder of the para-axial mesoderm that is characterized by underdevelopment of the posterior cranial fossa and overcrowding of the normally developed hindbrain. Tonsillar herniation of less than 5 mm does not exclude the diagnosis. Clinical manifestations of CMI seem to be related to cerebrospinal fluid disturbances (which are responsible for headaches, pseudotumor-like episodes, endolymphatic hydrops, syringomyelia, and hydrocephalus) and direct compression of nervous tissue. The demonstration of familial aggregation suggests a genetic component of transmission.
Page 2 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
The Chiari I malformation (CMI) is a disorder of uncertain origin that has been traditionally defined as downward herniation of the cerebellar tonsils through the foramen magnum (12,26,32,35,71,78). The anomaly is a leading cause of syringomyelia (12,32,61,65,78) and occurs in association with osseus abnormalities at the craniovertebral junction. In contrast to other Chiari malformations, CMI tends to present in the second or third decade of life and is sometimes referred to as the "adult-type" Chiari malformation. CMI is distinguished from the more familiar Chiari II malformation, which is present at birth and consists of downward herniation of the lower cerebellum and medulla into the spinal canal, in association with myelodysplasia and complex anomalies of the brain such as aqueductal forking and polymicrogyria (14,60). The comparatively rare Chiari III malformation is also present at birth and is defined as cerebellar herniation into a cervical encephalocele (26,60). From a developmental standpoint, Chiari malformations have been classified as neuroectodermal defects (14,59), although there is accumulating evidence that tonsillar herniation in CMI is attributable to overcrowding of the hindbrain by an underdeveloped posterior cranial fossa (PCF) (10,35,54,55,71,72,86,96,102).
Current interest in CMI can be attributed to magnetic resonance imaging (MRI), which has revolutionized diagnosis and has led to the detection of cases that either were not recognized or were erroneously identified as other conditions. The resulting increase in the number of reported cases has emphasized the need for greater understanding of the pathogenesis and clinical manifestations of CMI. Growing concerns regarding the risk of inheritance cannot be answered on the basis of case reports of familial aggregation (9,23,39,92).
To investigate the syndrome of CMI, we studied a prospective cohort of 364 symptomatic patients, including those with ambiguous or unfamiliar symptoms. The study provides a comprehensive review of the symptoms, neurodiagnostic findings, and inheritance patterns for this group of patients.
PATIENTS AND METHODS Patients
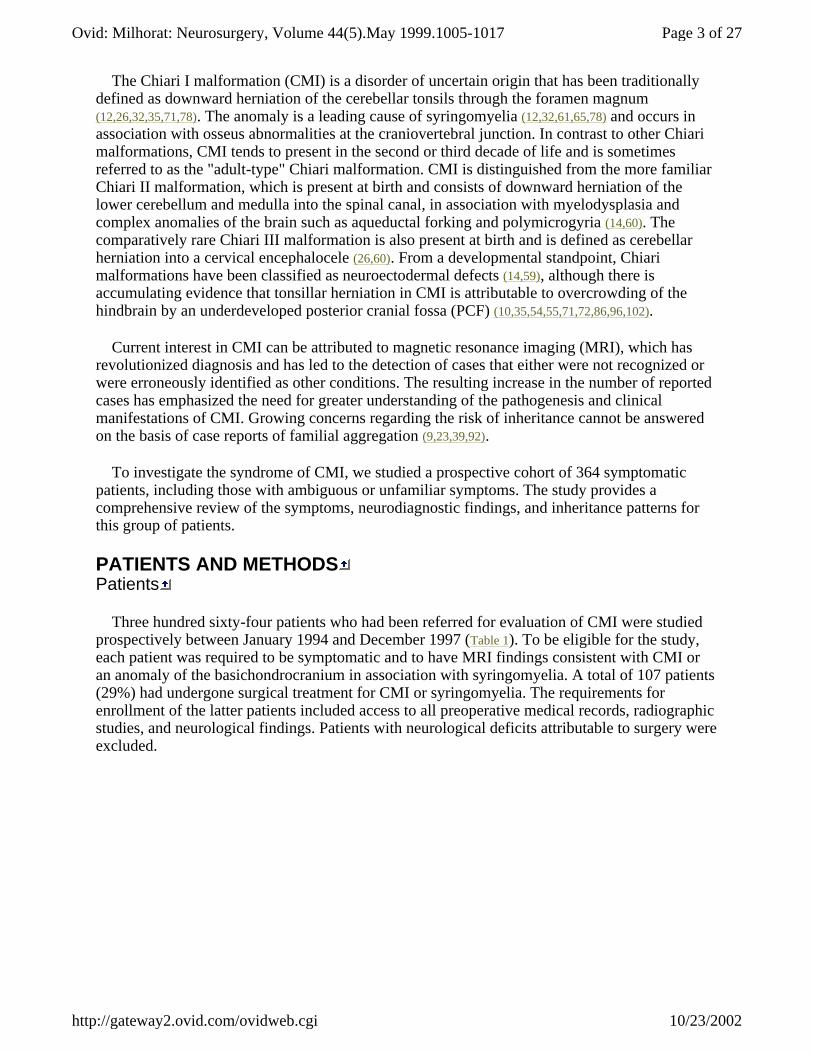
Three hundred sixty-four patients who had been referred for evaluation of CMI were studied prospectively between January 1994 and December 1997 (Table 1). To be eligible for the study, each patient was required to be symptomatic and to have MRI findings consistent with CMI or an anomaly of the basichondrocranium in association with syringomyelia. A total of 107 patients (29%) had undergone surgical treatment for CMI or syringomyelia. The requirements for enrollment of the latter patients included access to all preoperative medical records, radiographic studies, and neurological findings. Patients with neurological deficits attributable to surgery were excluded.
Page 3 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
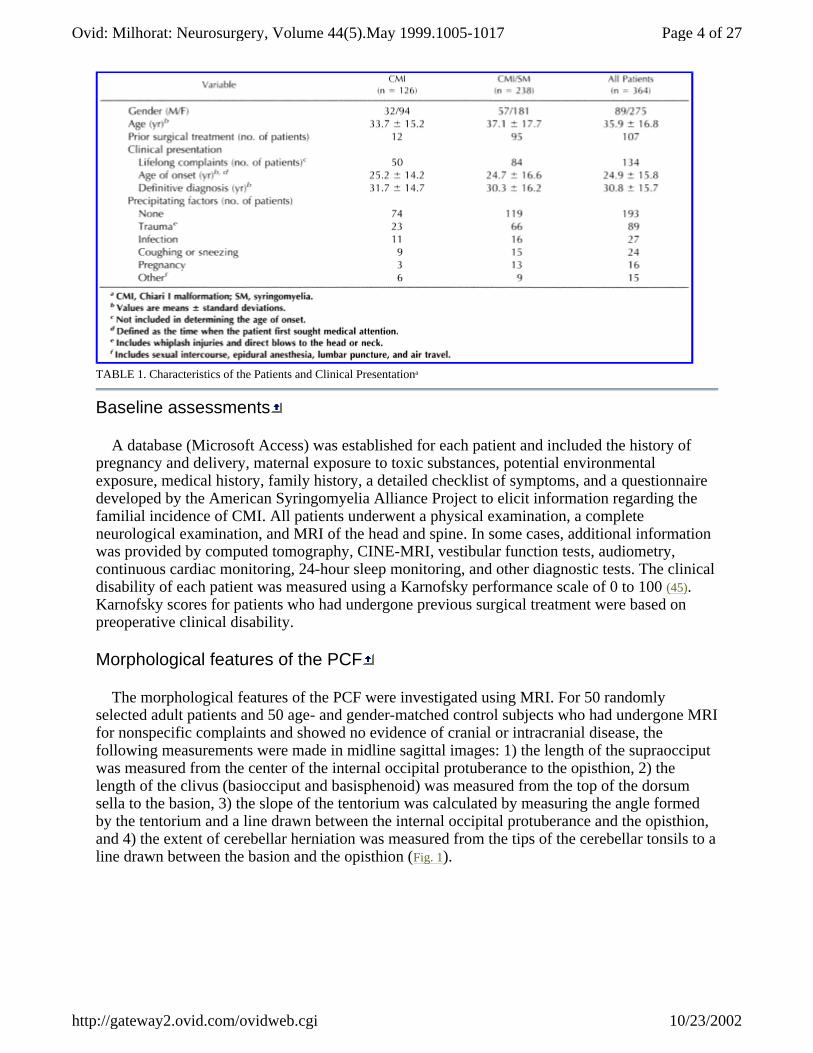
TABLE 1. Characteristics of the Patients and Clinical Presentationa
Baseline assessments
A database (Microsoft Access) was established for each patient and included the history of pregnancy and delivery, maternal exposure to toxic substances, potential environmental exposure, medical history, family history, a detailed checklist of symptoms, and a questionnaire developed by the American Syringomyelia Alliance Project to elicit information regarding the familial incidence of CMI. All patients underwent a physical examination, a complete neurological examination, and MRI of the head and spine. In some cases, additional information was provided by computed tomography, CINE-MRI, vestibular function tests, audiometry, continuous cardiac monitoring, 24-hour sleep monitoring, and other diagnostic tests. The clinical disability of each patient was measured using a Karnofsky performance scale of 0 to 100 (45). Karnofsky scores for patients who had undergone previous surgical treatment were based on preoperative clinical disability.
Morphological features of the PCF
The morphological features of the PCF were investigated using MRI. For 50 randomly selected adult patients and 50 age- and gender-matched control subjects who had undergone MRI for nonspecific complaints and showed no evidence of cranial or intracranial disease, the following measurements were made in midline sagittal images: 1) the length of the supraocciput was measured from the center of the internal occipital protuberance to the opisthion, 2) the length of the clivus (basiocciput and basisphenoid) was measured from the top of the dorsum sella to the basion, 3) the slope of the tentorium was calculated by measuring the angle formed by the tentorium and a line drawn between the internal occipital protuberance and the opisthion, and 4) the extent of cerebellar herniation was measured from the tips of the cerebellar tonsils to a line drawn between the basion and the opisthion (Fig. 1).
Page 4 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
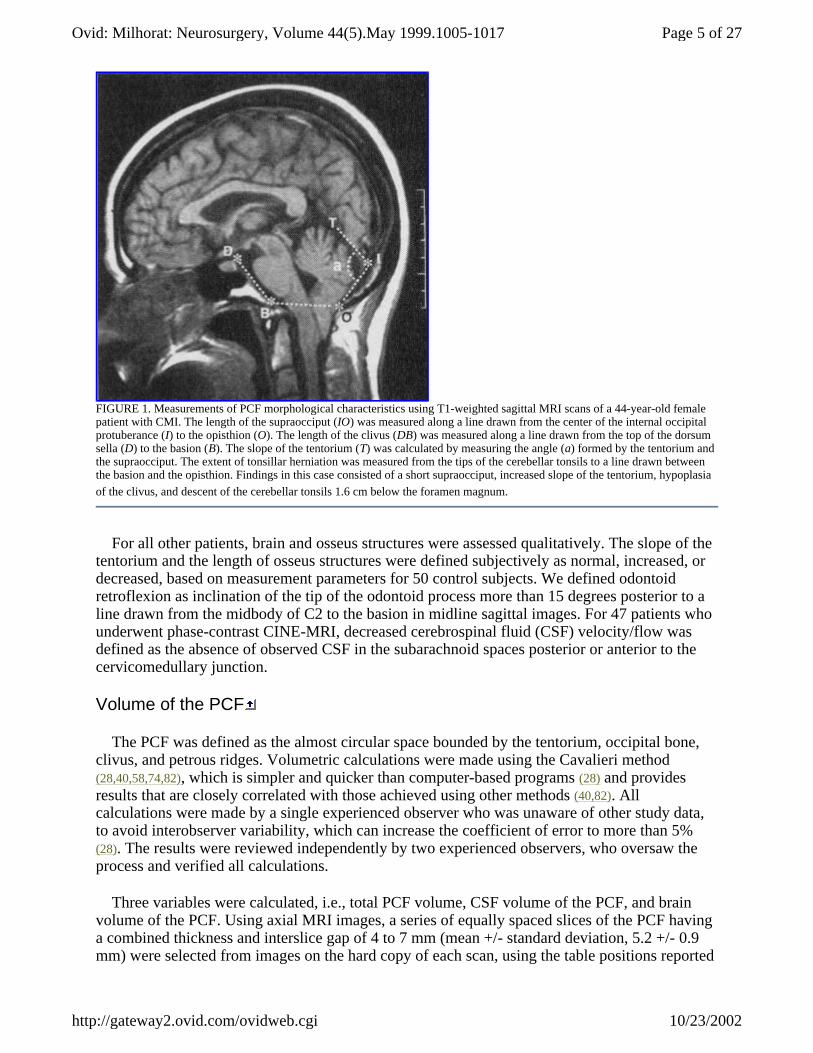
FIGURE 1. Measurements of PCF morphological characteristics using T1-weighted sagittal MRI scans of a 44-year-old female patient with CMI. The length of the supraocciput (IO) was measured along a line drawn from the center of the internal occipital protuberance (I) to the opisthion (O). The length of the clivus (DB) was measured along a line drawn from the top of the dorsum sella (D) to the basion (B). The slope of the tentorium (T) was calculated by measuring the angle (a) formed by the tentorium and the supraocciput. The extent of tonsillar herniation was measured from the tips of the cerebellar tonsils to a line drawn between the basion and the opisthion. Findings in this case consisted of a short supraocciput, increased slope of the tentorium, hypoplasia of the clivus, and descent of the cerebellar tonsils 1.6 cm below the foramen magnum.
For all other patients, brain and osseus structures were assessed qualitatively. The slope of the tentorium and the length of osseus structures were defined subjectively as normal, increased, or decreased, based on measurement parameters for 50 control subjects. We defined odontoid retroflexion as inclination of the tip of the odontoid process more than 15 degrees posterior to a line drawn from the midbody of C2 to the basion in midline sagittal images. For 47 patients who underwent phase-contrast CINE-MRI, decreased cerebrospinal fluid (CSF) velocity/flow was defined as the absence of observed CSF in the subarachnoid spaces posterior or anterior to the cervicomedullary junction.
Volume of the PCF
The PCF was defined as the almost circular space bounded by the tentorium, occipital bone, clivus, and petrous ridges. Volumetric calculations were made using the Cavalieri method (28,40,58,74,82), which is simpler and quicker than computer-based programs (28) and provides results that are closely correlated with those achieved using other methods (40,82). All calculations were made by a single experienced observer who was unaware of other study data, to avoid interobserver variability, which can increase the coefficient of error to more than 5% (28). The results were reviewed independently by two experienced observers, who oversaw the process and verified all calculations.
Three variables were calculated, i.e., total PCF volume, CSF volume of the PCF, and brain volume of the PCF. Using axial MRI images, a series of equally spaced slices of the PCF having a combined thickness and interslice gap of 4 to 7 mm (mean +/- standard deviation, 5.2 +/- 0.9 mm) were selected from images on the hard copy of each scan, using the table positions reported
Page 5 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
on the scan. A clear plastic sheet with an imprinted grid of 4-mm, regularly spaced points was placed over 7 to 12 (mean +/- standard deviation, 8.5 +/- 1.2) consecutive axial images, and the number of points falling within the PCF on each slice (Pi) was counted. The minimal number of points for each scan was 117 (mean +/- standard deviation, 141 +/- 10.5), which produces a coefficient of error of less than 5% (28). The true anatomic distance between two consecutive points on the grid was established by counting the number of points along a line placed over the centimeter ruler of the scan, thereby correlating the grid with the field of view of the scan. When necessary, the centimeter ruler was extended to establish an integer number of points and a whole number of centimeters. To calculate the area associated with each point (Ap), the anatomic distance between two consecutive points was squared. The sum of the points that fell within the PCF ([SIGMA]Pi) was multiplied by Ap and the distance between slices (T) to calculate volume (V), using the following equation: V = T [middle dot] Ap [middle dot] [SIGMA]Pi. Calculations of CSF and brain volumes were made separately on each scan. Measurements of the PCF, including the extent of tonsillar herniation, were compared with previously published data (1,10,13,71,72,94,96,102).
Pedigree development and assessment of familial aggregation
Twenty-one families participated in a study of familial aggregation. The protocol for the study was reviewed and approved by the Institutional Review Board of Duke University Medical Center. Written informed consent was received from each family. Photographs of all prospective probands were reviewed by a dysmorphologist to exclude individuals with a known genetic syndrome. The medical records and MRI scans of prospective affected relatives were examined to confirm the diagnosis of CMI. The database was expanded to include each affected family member. After the inclusion criteria of the study had been met, a pedigree was established for each family.
Statistical analyses
The statistical analyses were performed with SPSS for Windows (version 7.5; SPSS, Inc., Chicago, IL). Mean values are presented with their standard deviations. We assessed mean differences in the linear measurements and volume of the PCF for 50 patients and 50 control subjects using independent-sample Student's t tests. Significance was indicated by a two-tailed P value of less than 0.05. For 50 patients, morphometric features of the PCF were compared with clinical disability (as measured by Karnofsky scores) using univariate correlations and a stepwise multiple logistic regression model, to identify potential radiographic variables affecting outcomes. In the study population, the extent of tonsillar descent was compared with Karnofsky scores and the incidence of syringomyelia using univariate logistic regression analysis.
RESULTS Clinical presentation
Table 1 shows variations in the clinical presentation of CMI. There were 275 female and 89 male patients, with a mean age of 35.9 +/- 16.8 years (range, 1-76 yr). The age of onset was defined as the time when the patient first sought medical attention. One hundred thirty-four patients (37%) reported histories of lifelong complaints such as headaches and clumsiness. Patients with syringomyelia presented at a slightly younger age (24.7 +/- 16.6 yr) and received diagnoses earlier (30.3 +/- 16.2 yr) than did patients without syringomyelia (25.2 +/- 14.2 and 31.7 +/- 14.7 yr, respectively). Although the majority of patients described a spontaneous onset of symptoms, 89 (24%) cited trauma as the precipitating event. Common misdiagnoses included
Page 6 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
migraine, fibromyalgia, and multiple sclerosis. By the time of definitive diagnosis, 215 patients (59%) had been told by at least one physician that they suffered from a psychogenic disorder.
Clinical syndrome
The most common symptom of CMI was suboccipital headache. This was experienced by 296 patients (81%) and was described as a heavy, crushing, or pressure-like sensation at the back of the head that radiated to the vertex and behind the eyes and inferiorly to the neck and shoulders. The headaches had a pounding quality when severe but were otherwise nonthrobbing. A distinctive feature of the headaches was their tendency to be accentuated by physical exertion, Valsalva maneuvers, head dependency, and sudden changes in posture. Female patients of menstrual age tended to experience an accentuation of symptoms during the week preceding menses. With few exceptions, Chiari-related headaches could be clearly distinguished from cervicogenic and other headache syndromes.
Ocular disturbances were reported by 283 patients (78%) (Table 2). Affected individuals were defined as those with two or more of the following intermittent symptoms: retro-orbital pressure or pain, visual phenomena such as floaters or flashing lights, blurred vision, photophobia, diplopia, and visual field cuts. Most of these symptoms were accentuated by the same factors that affected suboccipital headaches. Neuroophthalmological examinations revealed few objective findings. Ocular disturbances among young women were the leading cause of erroneous diagnoses of multiple sclerosis.
Page 7 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
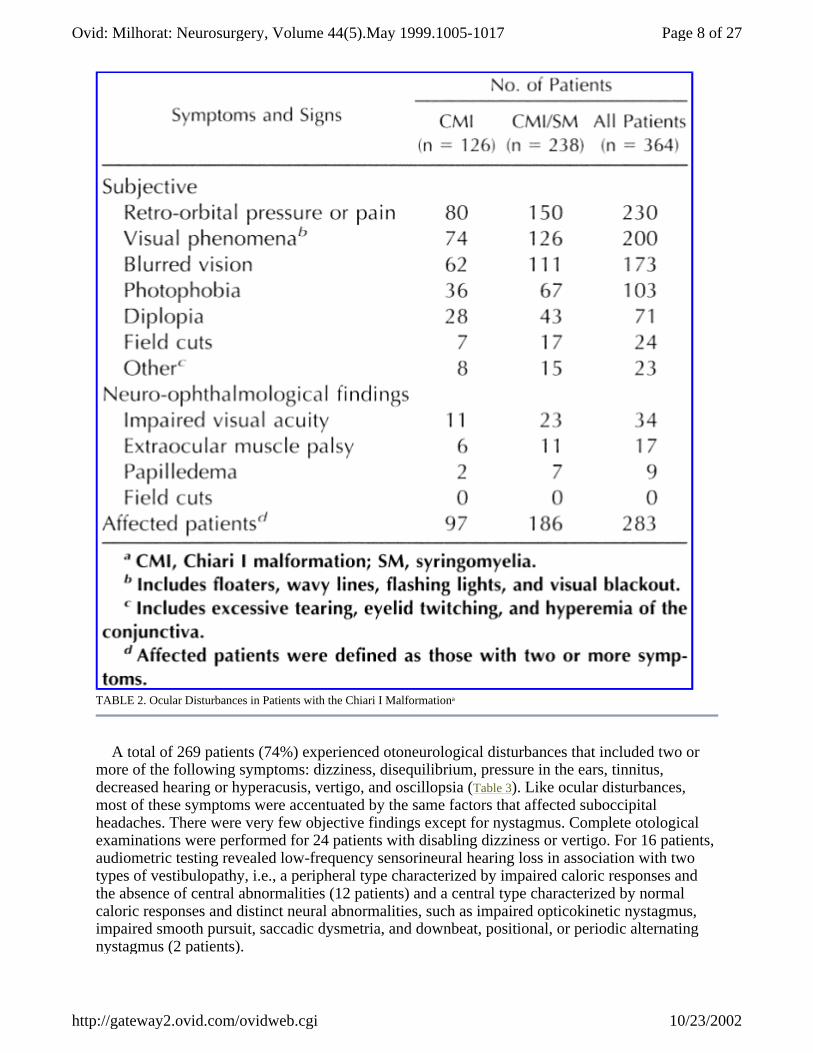
TABLE 2. Ocular Disturbances in Patients with the Chiari I Malformationa
A total of 269 patients (74%) experienced otoneurological disturbances that included two or more of the following symptoms: dizziness, disequilibrium, pressure in the ears, tinnitus, decreased hearing or hyperacusis, vertigo, and oscillopsia (Table 3). Like ocular disturbances, most of these symptoms were accentuated by the same factors that affected suboccipital headaches. There were very few objective findings except for nystagmus. Complete otological examinations were performed for 24 patients with disabling dizziness or vertigo. For 16 patients, audiometric testing revealed low-frequency sensorineural hearing loss in association with two types of vestibulopathy, i.e., a peripheral type characterized by impaired caloric responses and the absence of central abnormalities (12 patients) and a central type characterized by normal caloric responses and distinct neural abnormalities, such as impaired opticokinetic nystagmus, impaired smooth pursuit, saccadic dysmetria, and downbeat, positional, or periodic alternating nystagmus (2 patients).
Page 8 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
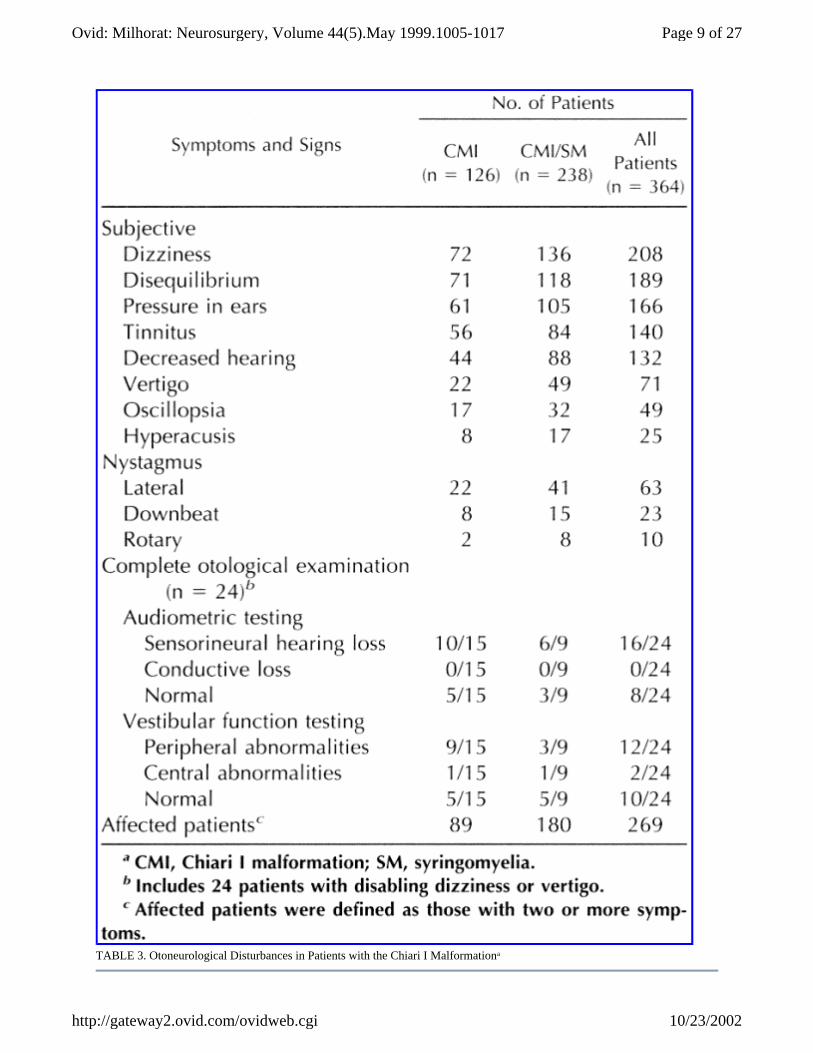
TABLE 3. Otoneurological Disturbances in Patients with the Chiari I Malformationa
Page 9 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi

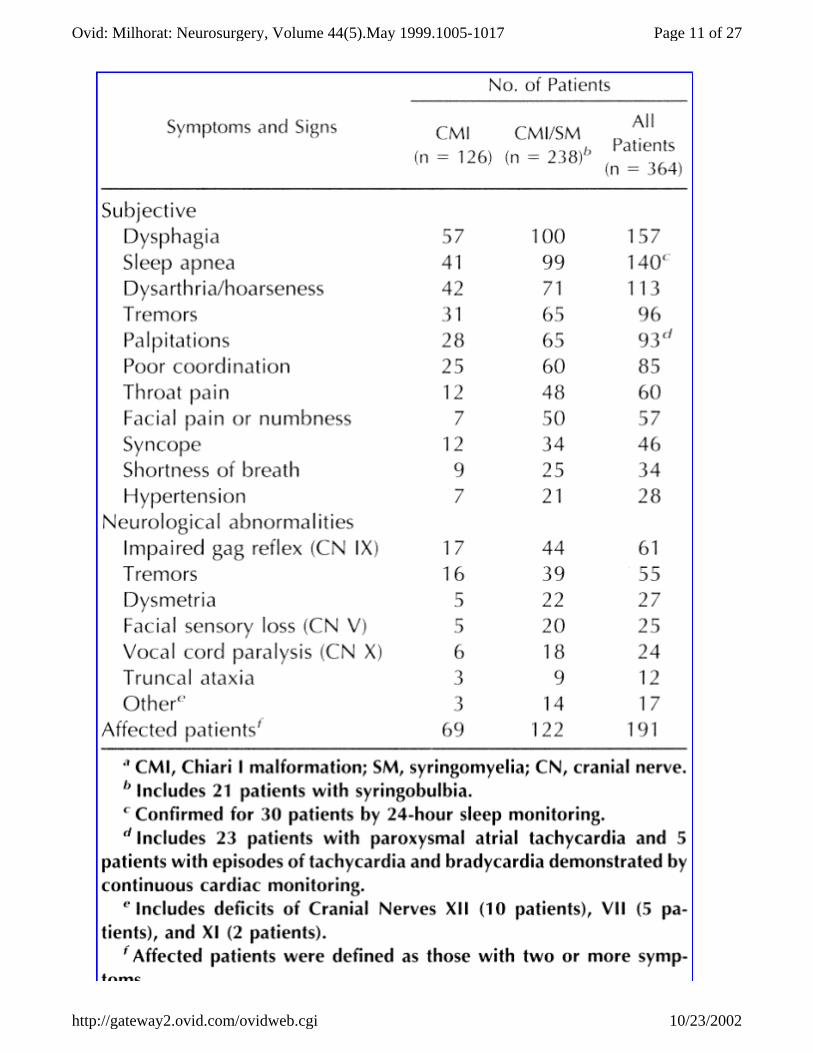
Table 4 summarizes lower cranial nerve, brain stem, and cerebellar disturbances for 191 patients (52%). The most common symptoms were dysphagia, sleep apnea, dysarthria, tremors, palpitations, and poor coordination. Objective findings consisted of cranial nerve deficits and cerebellar signs in a minority of the patients. The diagnosis of sleep apnea was confirmed for 30 patients by 24-hour sleep monitoring. For 28 of 42 patients with histories of palpitations or evidence of bradycardia in physical examinations, continuous cardiac monitoring demonstrated either paroxysmal atrial tachycardia (23 patients) or episodes of tachycardia and bradycardia (5 patients).
Page 10 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
Page 11 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi

TABLE 4. Lower Cranial Nerve, Brain Stem, and Cerebellar Disturbances in Patients with the Chiari I Malformationa
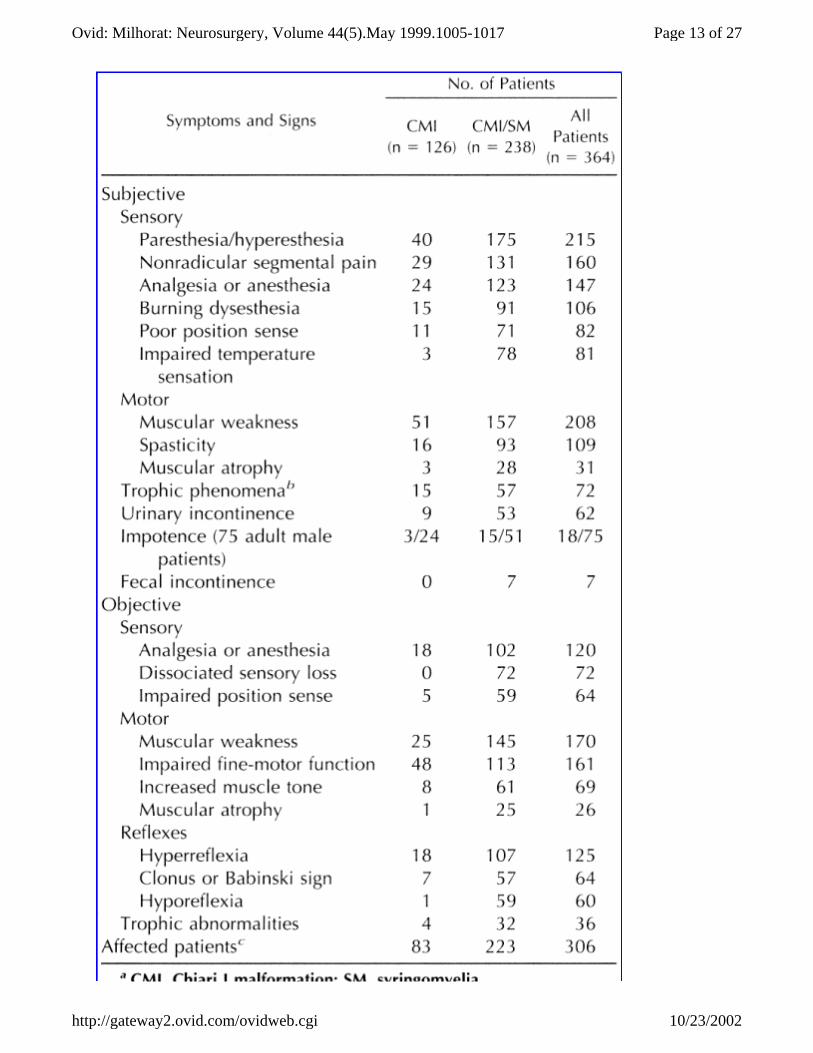
Disturbances of spinal cord function were present in 223 of 238 patients (94%) with syringomyelia (Table 5). The incidence, type, and severity of symptoms were typical for syringomyelia (12,18,32,36,50,63,64,78). An unexpected finding was the presence of similar but less severe disturbances in 83 of 126 patients (66%) without syringomyelia. In this group, the most common symptoms were muscular weakness, paresthesia or hyperesthesia, nonradicular segmental pain, analgesia or anesthesia, spasticity, trophic phenomena, burning dysesthesia, and poor position sense. Objective findings included impaired fine-motor function of the hands (48 patients), muscular weakness (25 patients), analgesia or anesthesia (18 patients), and hyperreflexia (18 patients). Nonspecific disturbances in the study population included chronic fatigue (210 patients), impaired recent memory (142 patients), cervicogenic pain (125 patients), low back pain (87 patients), and episodic nausea or vomiting (65 patients).
Page 12 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
Page 13 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
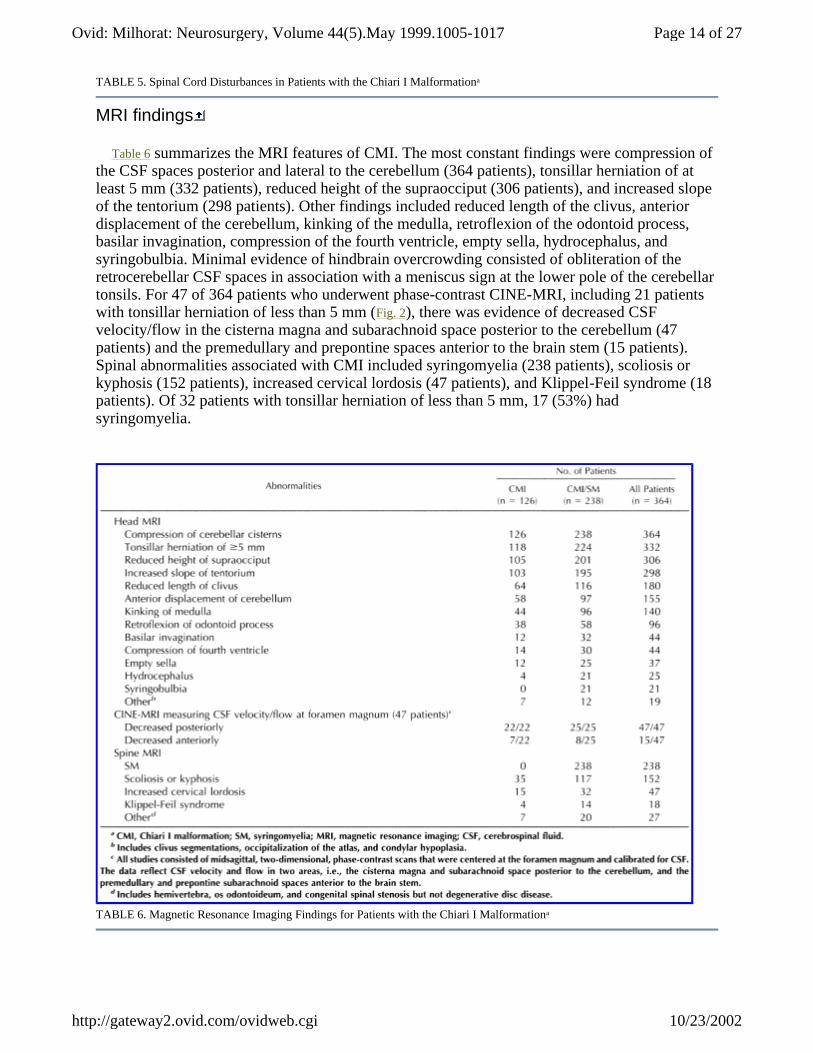
TABLE 5. Spinal Cord Disturbances in Patients with the Chiari I Malformationa
MRI findings
Table 6 summarizes the MRI features of CMI. The most constant findings were compression of the CSF spaces posterior and lateral to the cerebellum (364 patients), tonsillar herniation of at least 5 mm (332 patients), reduced height of the supraocciput (306 patients), and increased slope of the tentorium (298 patients). Other findings included reduced length of the clivus, anterior displacement of the cerebellum, kinking of the medulla, retroflexion of the odontoid process, basilar invagination, compression of the fourth ventricle, empty sella, hydrocephalus, and syringobulbia. Minimal evidence of hindbrain overcrowding consisted of obliteration of the retrocerebellar CSF spaces in association with a meniscus sign at the lower pole of the cerebellar tonsils. For 47 of 364 patients who underwent phase-contrast CINE-MRI, including 21 patients with tonsillar herniation of less than 5 mm (Fig. 2), there was evidence of decreased CSF velocity/flow in the cisterna magna and subarachnoid space posterior to the cerebellum (47 patients) and the premedullary and prepontine spaces anterior to the brain stem (15 patients). Spinal abnormalities associated with CMI included syringomyelia (238 patients), scoliosis or kyphosis (152 patients), increased cervical lordosis (47 patients), and Klippel-Feil syndrome (18 patients). Of 32 patients with tonsillar herniation of less than 5 mm, 17 (53%) had syringomyelia.
TABLE 6. Magnetic Resonance Imaging Findings for Patients with the Chiari I Malformationa
Page 14 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
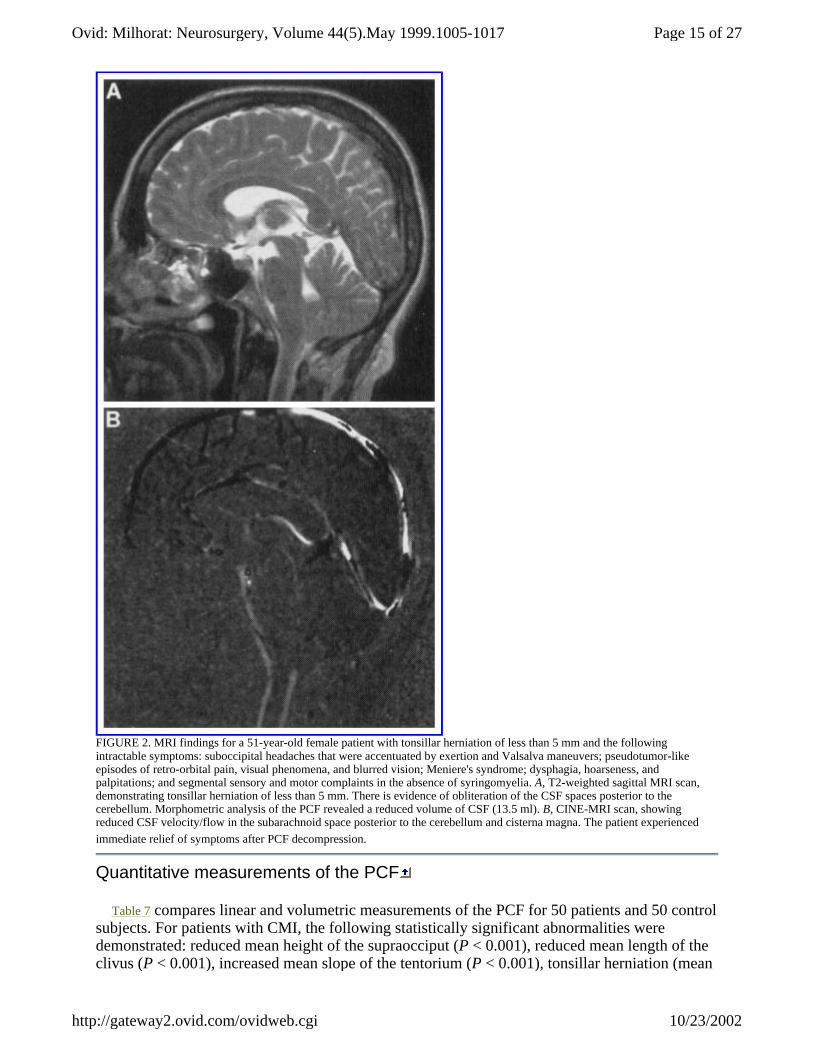
FIGURE 2. MRI findings for a 51-year-old female patient with tonsillar herniation of less than 5 mm and the following intractable symptoms: suboccipital headaches that were accentuated by exertion and Valsalva maneuvers; pseudotumor-like episodes of retro-orbital pain, visual phenomena, and blurred vision; Meniere's syndrome; dysphagia, hoarseness, and palpitations; and segmental sensory and motor complaints in the absence of syringomyelia. A, T2-weighted sagittal MRI scan, demonstrating tonsillar herniation of less than 5 mm. There is evidence of obliteration of the CSF spaces posterior to the cerebellum. Morphometric analysis of the PCF revealed a reduced volume of CSF (13.5 ml). B, CINE-MRI scan, showing reduced CSF velocity/flow in the subarachnoid space posterior to the cerebellum and cisterna magna. The patient experienced immediate relief of symptoms after PCF decompression.
Quantitative measurements of the PCF
Table 7 compares linear and volumetric measurements of the PCF for 50 patients and 50 control subjects. For patients with CMI, the following statistically significant abnormalities were demonstrated: reduced mean height of the supraocciput (P < 0.001), reduced mean length of the clivus (P < 0.001), increased mean slope of the tentorium (P < 0.001), tonsillar herniation (mean
Page 15 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
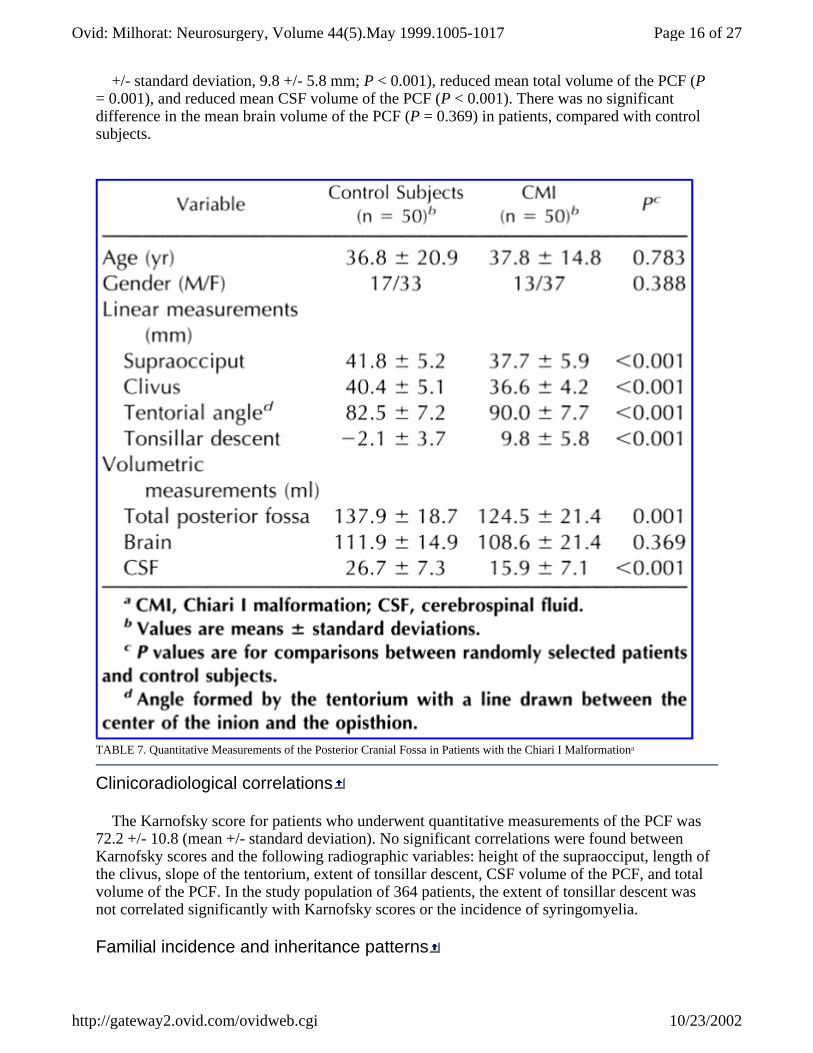
+/- standard deviation, 9.8 +/- 5.8 mm; P < 0.001), reduced mean total volume of the PCF (P = 0.001), and reduced mean CSF volume of the PCF (P < 0.001). There was no significant difference in the mean brain volume of the PCF (P = 0.369) in patients, compared with control subjects.
TABLE 7. Quantitative Measurements of the Posterior Cranial Fossa in Patients with the Chiari I Malformationa
Clinicoradiological correlations
The Karnofsky score for patients who underwent quantitative measurements of the PCF was 72.2 +/- 10.8 (mean +/- standard deviation). No significant correlations were found between Karnofsky scores and the following radiographic variables: height of the supraocciput, length of the clivus, slope of the tentorium, extent of tonsillar descent, CSF volume of the PCF, and total volume of the PCF. In the study population of 364 patients, the extent of tonsillar descent was not correlated significantly with Karnofsky scores or the incidence of syringomyelia.
Familial incidence and inheritance patterns
Page 16 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
Forty-three patients (12%) had at least one close relative with one of the following diagnoses: CMI and syringomyelia (19 families), CMI in the absence of syringomyelia (17 families), or syringomyelia of unknown origin (7 families). An additional 72 patients reported that at least one close relative exhibited symptoms similar to their own but had not been evaluated by neuroimaging. The only neural defect encountered among more than 4000 close relatives was meningomyelocele (two families), which is consistent with the incidence of this anomaly in the general population (24).
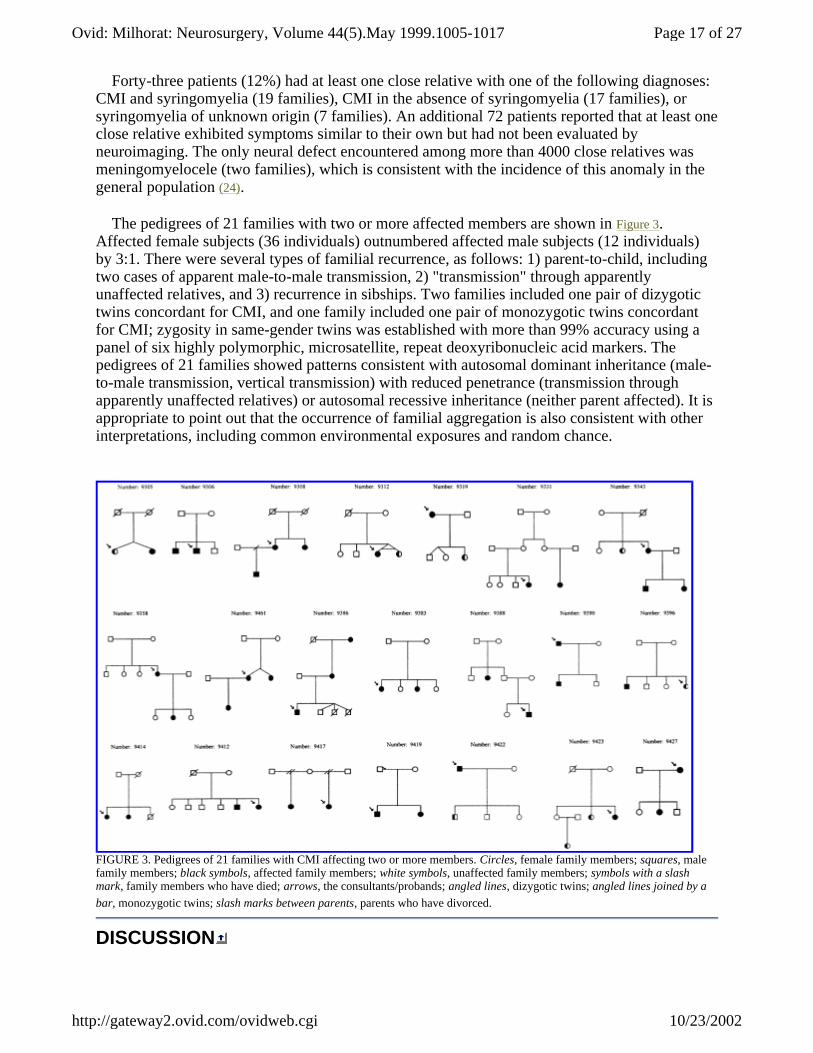
The pedigrees of 21 families with two or more affected members are shown in Figure 3. Affected female subjects (36 individuals) outnumbered affected male subjects (12 individuals) by 3:1. There were several types of familial recurrence, as follows: 1) parent-to-child, including two cases of apparent male-to-male transmission, 2) "transmission" through apparently unaffected relatives, and 3) recurrence in sibships. Two families included one pair of dizygotic twins concordant for CMI, and one family included one pair of monozygotic twins concordant for CMI; zygosity in same-gender twins was established with more than 99% accuracy using a panel of six highly polymorphic, microsatellite, repeat deoxyribonucleic acid markers. The pedigrees of 21 families showed patterns consistent with autosomal dominant inheritance (male-to-male transmission, vertical transmission) with reduced penetrance (transmission through apparently unaffected relatives) or autosomal recessive inheritance (neither parent affected). It is appropriate to point out that the occurrence of familial aggregation is also consistent with other interpretations, including common environmental exposures and random chance.
FIGURE 3. Pedigrees of 21 families with CMI affecting two or more members. Circles, female family members; squares, male family members; black symbols, affected family members; white symbols, unaffected family members; symbols with a slash mark, family members who have died; arrows, the consultants/probands; angled lines, dizygotic twins; angled lines joined by a bar, monozygotic twins; slash marks between parents, parents who have divorced.
DISCUSSION
Page 17 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
Chiari malformations are generally regarded as a pathological continuum of increasingly severe hindbrain maldevelopments (12,32,78). The association of Chiari II and Chiari III malformations with embryological defects of the brain and spinal cord has established these lesions as primary neural anomalies (14,26,59). However, there is clinical and experimental evidence that chronic tonsillar herniation in CMI could be attributable to underdevelopment of the occipital bone and overcrowding of the cerebellum within a too-small PCF (10,35,54,55,71,72,86,96,102). Recent morphometric studies are consistent with this view (10,71,86,96,102), and Nishikawa et al. (71) suggested that the fundamental defect may involve underdevelopment of the occipital somites originating from the para-axial mesoderm.
The proposition that CMI is a disorder of mesodermal origin was supported by the following findings in this study: 1) neurological examinations and MRI scans of the brain and spinal cord of 364 patients failed to provide any evidence of neuroectodermal defects; 2) the neural abnormalities that were present (e.g., syringomyelia and hydrocephalus) were attributable to the secondary effects of chronic tonsillar herniation; 3) the incidence of neural anomalies among close relatives of affected individuals was similar to that in the general population; and 4) the MRI findings of reduced height of the supraocciput, increased slope of the tentorium, hypoplasia of the clivus, and osseus abnormalities at the craniovertebral junction were consistent with a defect of the para-axial mesoderm.
Other MRI findings provided substantial evidence of hindbrain overcrowding. The most constant abnormality was compression of the CSF spaces posterior and lateral to the cerebellum (364 patients, 100%). Tonsillar herniation of at least 5 mm below the foramen magnum was present in 332 patients (91%). Less constant findings of hindbrain overcrowding included anterior displacement of the cerebellum, kinking of the medulla occurring with retroflexion of the odontoid process or basilar invagination, and compression of the fourth ventricle. Quantitative measurements of the PCF demonstrated significant reductions in CSF volume (P < 0.001) and total PCF volume (P = 0.001) but no differences in brain volume (P = 0.369) for 50 randomly selected patients, compared with control subjects. Taken together, these findings support and extend accumulating evidence that the fundamental problem in CMI is a volumetrically small PCF (10,71,86,96,102), which results in varying degrees of hindbrain overcrowding. Similar abnormalities probably underlie the development of "acquired CMI" in some cases of craniosynostosis (27), hypophosphatemic rickets (22), achondroplasia (69), and Paget's disease (80).
There is limited information regarding the epidemiological features of CMI. The anomaly is defined as a rare disorder (70), and female subjects outnumber male subjects by a wide margin (50,71,78). As shown in Table 1, approximately 25% of patients cited trauma as the precipitating factor. The most common mechanisms were whiplash injuries and direct blows to the head and neck (53), which raises the possibility that certain types of trauma accentuate tonsillar impaction or result in subarachnoid hemorrhage that destabilizes a marginally compensated CSF system.
The likelihood that CMI can be genetically transmitted has been suggested by two lines of evidence, i.e., the association of CMI with known genetic disorders, such as achondroplasia (69), Hadju-Cheney syndrome (99), and Klippel-Feil syndrome (71,101), and case reports of familial aggregation (9,23,39,59), including cases of monozygotic twins (9,92) and triplets (23) concordant for CMI. The incidence of familial syringomyelia is reported as 2% (25), but there are no data, to our knowledge, regarding the risk of inheritance in CMI. In this study, 43 patients (12%) reported positive family histories for CMI or syringomyelia. Analysis of the pedigrees of 21 families revealed patterns of inheritance consistent with autosomal dominant inheritance with reduced penetrance or autosomal recessive inheritance. These modes of transmission have also
Page 18 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi

been reported for patients with familial syringomyelia (16,21,109).
Previous reports have documented the complex symptom patterns for CMI (12,18,20,31,32,35,50,78,89,95,107). Presenting symptoms can include headaches (47,56,75-77,93,98,100) in association with a wide variety of ocular (3,51,56,85,90,97,108), otoneurological (15,38,41,44,48,52,68,84,85,87,103,105), brain stem (2,5-7,19,29,30,34,43,46,49,57,79,83,97,104), and spinal cord (29,36,62,64) disturbances. Although many of the symptoms discussed in this report (Tables 2-5) have been described previously, some are less familiar or have been difficult to relate to the specific effects of tonsillar herniation and syringomyelia. A majority of the patients in the study population complained that their symptoms had been ascribed to psychogenic causes.
There is evidence that some ambiguous or unfamiliar symptoms may be CSF-related. For example, given the significant reduction of CSF volume in the PCF demonstrated in this study (mean, 10.8 ml; 40%), it is evident that newly formed CSF is displaced from the compressed subarachnoid spaces of the PCF into available spaces within the supratentorial and spinal compartments. Such displacements almost certainly affect CSF compliance and would be expected to alter the normal damping effect of an open CSF system, which mitigates changes in venous volume and pressure occurring with respirations, the cardiac pulse, Valsalva maneuvers, and changes in posture (60). Under these conditions, CSF displacements could play a role in the following symptoms: 1) sub-occipital headaches that radiate to the vertex and behind the eyes and inferiorly to the neck and shoulders, 2) pseudotumor-like episodes of retro-orbital pain and visual phenomena, and 3) a Meniere's disease-like syndrome of pressure in the ears, dizziness, disequilibrium, tinnitus, and hearing loss. The exquisite sensitivity of these symptoms to physical activities, including Valsalva maneuvers, is consistent with reduced compliance of the CSF system. For some patients with vestibular dysfunction, otological testing revealed low-frequency sensorineural hearing loss in association with peripheral vestibulopathy (Table 3). These findings fulfill the criteria for endolymphatic hydrops (4,42) and suggest that CSF displacements in CMI contribute to disturbances of CSF-perilymph dynamics.
The most obvious CSF-related symptoms are those attributable to syringomyelia (Table 5). These can occur because of stretching and distention of nervous tissue or dissection of central canal cavities into the parenchymal tissues of the spinal cord (61). Although it was once thought that syringomyelia was caused by the forceful diversion of CSF from the fourth ventricle into the central canal (37,106), it is now known that most syrinxes do not communicate with the fourth ventricle and are separated from it by an occluded or stenotic segment of the canal (61,63,65). Current evidence suggests that syrinx formation is the result of an obstruction of CSF flow at the foramen magnum, which exaggerates the pulsatile systolic pulse wave in the spinal subarachnoid space (73) and drives CSF through anatomically continuous perivascular and interstitial spaces (66,67,91) into the central canal of the spinal cord. More severe obstructions of CSF circulation are occasionally causes of hydrocephalus (Table 6).
An unexpected finding in this study was the presence of spinal cord disturbances in 83 of 126 patients (66%) who did not have syringomyelia. Some of these disturbances are related to mechanical compression of the cervicomedullary junction (12,18,29,32,78), but another explanation could be that the exaggerated systolic pulse wave in the spinal canal is capable of producing symptoms that mimic those of syringomyelia. Compression of the brain stem and lower cranial nerves was the most likely cause of dysphagia, hoarseness, sleep apnea, and palpitations. The incidence of cardiac irregularities in the study population seemed unusually high for a cohort of predominantly young adult female subjects, and an association between sinus arrhythmia and CMI was noted previously (43,88,97). It is acknowledged that many of the symptoms described in this report occur with variable frequencies in the general population and could be unrelated.
Page 19 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
Clinical descriptions of CMI have undergone continuous revision since the original report, by Chiari (26), of tonsillar herniation in patients dying as a result of hydrocephalus. In recent years, the term CMI has been used synonymously with tonsillar ectopia or chronic tonsillar herniation in a wide variety of congenital and acquired disorders. The radiological definition of CMI has been reported as tonsillar herniation of at least 3 mm (13) or at least 5 mm (1) below the foramen magnum. However, this definition is limited to a single criterion and makes no reference to clinical symptoms or the presence or absence of associated findings such as syringomyelia.
The radiological definition of CMI may be too restrictive. In this study, there were 32 of 364 patients (9%) who exhibited tonsillar herniation of less than 5 mm and symptoms that were typical of CMI. Seventeen of those 32 patients (53%) had syringomyelia. All patients showed MRI evidence of hindbrain overcrowding (Fig. 2A), and CINE-MRI demonstrated abnormalities of CSF velocity/flow (Fig. 2B) that were similar to those reported for patients with tonsillar herniation of at least 5 mm (8,17,81). These observations indicate that the extent of tonsillar herniation cannot be used as the sole criterion for the diagnosis of CMI. We could not confirm reports (1,11,33,94) that the severity of symptoms is directly related to the extent of tonsillar herniation. Because tonsillar herniation of at least 5 mm can be encountered as an incidental finding among asymptomatic patients (33), it is likely that the position of the cerebellar tonsils, although providing a general index of hindbrain overcrowding, is only one factor influencing the clinical features of CMI.
CONCLUSIONS
CMI is a disorder of the mesoderm and is thus inherently different from Chiari II and Chiari III malformations. The anomaly occurs sporadically but can be transmitted genetically in some families. The most constant feature of CMI is a volumetrically small PCF, which predisposes patients to hindbrain overcrowding. Displacements of CSF probably contribute to the symptoms. The clinical syndrome of CMI is characterized by headaches, pseudotumor-like episodes, a Meniere's disease-like syndrome, lower cranial nerve signs, and spinal cord disturbances even in the absence of syringomyelia. Diagnosis is established by MRI. Minimal evidence of hindbrain overcrowding consists of obliteration of the retrocerebellar CSF spaces in association with a meniscus sign at the lower pole of the cerebellar tonsils. CINE-MRI can be helpful in demonstrating a disturbance of CSF velocity/flow at the foramen magnum in patients with tonsillar herniation of less than 5 mm.
ACKNOWLEDGMENTS
This work was supported by grants from the National Institutes of Health (Grant NS26630 to MCS) and the Bobby Jones Foundation.
We are indebted to the study patients, the American Syringomyelia Alliance Project, and Peter Homel, Ph.D., Pierre S. Girgis, M.D., Tania Parsa, M.D., Jill R. Gretenstein, Amy Franklin, and Artem Y. Vaynman for valuable assistance.
REFERENCES
1. Aboulezz AO, Sartor K, Geyer CA, Gado MH: Position of cerebellar tonsils in the normal population and in patients with Chiari malformation: A quantitative approach with MR imaging. J Comput Assist Tomogr 9:1033-1036, 1985. [Medline Link] [BIOSIS Previews Link] [Context Link]
Page 20 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
2. Ahmmed AU, Mackenzie I, Das VK, Chatterjee S, Lye RH: Audio-vestibular manifestations of Chiari malformation and outcome of surgical decompression: A case report. J Laryngol Otol 110:1060-1064, 1996. [Medline Link] [BIOSIS Previews Link] [Context Link]
3. Alarcon J, Dobato JL, Mateo D, Benito C, Gimenez-Roldan S: Arnold-Chiari malformation with multiple paroxysmal manifestations induced by coughing. Neurologia 7:25-29, 1992. [Medline Link] [Context Link]
4. Alford B: Meniere's disease: Criteria for diagnosis and evaluation of therapy for reporting-Report of subcommittee on equilibrium and its measurement. Trans Am Acad Opthalmol Otolaryngol 76:1462-1464, 1972. [Context Link]
5. Ali MM, Russell N, Awada A, McLean D: A cranio-cervical malformation presenting as acute respiratory failure. J Emerg Med 14:569-572, 1996. [Medline Link] [BIOSIS Previews Link] [Context Link]
6. Alvarez D, Requena I, Arias M, Valdes L, Pereiro I, De la Torre R: Acute respiratory failure as the first sign of Arnold-Chiari malformation associated with syringomyelia. Eur Respir J 8:661-663, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
7. Arcaya J, Cacho J, Del Campo F, Grande J, Maillo A: Arnold-Chiari malformation associated with sleep apnea and central dysregulation of arterial pressure. Acta Neurol Scand 88:224-226, 1993. [Medline Link] [BIOSIS Previews Link] [Context Link]
8. Armonda RA, Citrin CM, Foley KT, Ellenbogen RG: Quantitative CINE-mode magnetic resonance imaging of Chiari I malformations: An analysis of cerebrospinal fluid dynamics. Neurosurgery 35:214-223, 1994. [Medline Link] [BIOSIS Previews Link] [Context Link]
9. Atkinson JLD, Kokmen E, Miller GM: Evidence of posterior fossa hypoplasia in the familial variant of adult Chiari I malformation: Case report. Neurosurgery 42:401-404, 1998. [Fulltext Link] [Medline Link] [Context Link]
10. Badie B, Mendoza D, Batzdorf U: Posterior fossa volume and response to suboccipital decompression with Chiari I malformation. Neurosurgery 37:214-218, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
11. Ball WS, Crone KR: Chiari I malformation: From Dr. Chiari to MR imaging. Radiology 195:602-604, 1995. [Medline Link] [Context Link]
12. Banerji NK, Millar JHD: Chiari malformation presenting in adult life. Brain 97:157-168, 1974. [Medline Link] [Context Link]
13. Barkovich AJ, Wippold JF, Sherman JL, Citrin CM: Significance of cerebellar tonsillar position on MR. AJNR Am J Neuroradiol 7:795-799, 1986. [Medline Link] [BIOSIS Previews Link] [Context Link]
14. Barry A, Patten BM, Stewart BH: Possible factors in the development of the Arnold-Chiari malformation. J Neurosurg 14:285-301, 1957. [Context Link]
15. Barton JJ, Sharpe JA: Oscillopsia and horizontal nystagmus with accelerating slow phases following lumbar puncture in the Arnold-Chiari malformation. Ann Neurol 33:418-421, 1993. [Medline Link] [BIOSIS Previews Link] [Context Link]
16. Bentley SJ, Campbell MJ, Kaufman P: Familial syringomyelia. J Neurol Neurosurg Psychiatry 38:346-349, 1975. [Medline Link] [Context Link]
17. Bhadelia RA, Bogdan AR, Wolpert SM, Lev S, Appignani BA, Heilman CB: Cerebrospinal fluid flow waveforms: Analysis in patients with Chiari I malformation by means of gated phase-contrast MR imaging velocity measurements. Radiology 196:195-202, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
18. Bindal AK, Dunsker SB, Tew JM Jr: Chiari I malformation: Classification and management. Neurosurgery 37:1069-1074, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
19. Birns JW: An unusual form of laryngeal paralysis associated with Arnold-Chiari malformations. Ann Otol Rhinol Laryngol 93:447-451, 1984. [Medline Link] [BIOSIS Previews Link] [Context Link]
Page 21 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi

20. Brill CB, Gutierrez J, Mishkin MM: Chiari I malformation: Association with seizures and developmental disabilities. J Child Neurol 12:101-106, 1997. [Medline Link] [BIOSIS Previews Link] [Context Link]
21. Busis NA, Hochberg FH: Familial syringomyelia. J Neurol Neurosurg Psychiatry 48:936-938, 1985. [Medline Link] [BIOSIS Previews Link] [Context Link]
22. Caldemeyer KS, Boaz JC, Wappner RS, Moran CC, Smith RR, Quets JP: Chiari I malformation: Association with hypophosphatemic rickets and MR imaging appearance. Radiology 195:733-738, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
23. Cavender RK, Schmidt JH: Tonsillar ectopia and Chiari malformations: Monozygotic triplets-Case report. J Neurosurg 82:497-500, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
24. Centers for Disease Control: Spina bifida incidence at birth: United States, 1983-1990. MMWR 41:497-500, 1992. [Medline Link] [BIOSIS Previews Link] [Context Link]
25. Chatel M, Menault F, Pecker J: Arguments en faveur de l'origine genetique des tableaux malformatifs syringohydromyeliques. Neurochirurgie 25:160-165, 1979. [Medline Link] [BIOSIS Previews Link] [Context Link]
26. Chiari H: Ueber Veranderungen des Kleinhirns in folge von Hydrocephalie des Grosshirns. Dtsch Med Wochenschr 17:1172-1175, 1891. [Context Link]
27. Cinalli G, Renier D, Sebag G, Sainte-Rose C, Arnaud E, Pierre-Kahn A: Chronic tonsillar herniation in Crouzon's and Apert's syndromes: The role of premature synostosis of the lambdoid suture. J Neurosurg 83:575-582, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
28. Clatterbuck RE, Sipos EP: The efficient calculation of neurosurgically relevant volumes from computed tomographic scans using Cavalieri's direct estimator. Neurosurgery 40:339-343, 1997. [Fulltext Link] [Medline Link] [BIOSIS Previews Link] [Context Link]
29. Da Silva JA, Brito JC, Da Nobrega PV: Autonomic nervous system disorders in 230 cases of basilar impression and Arnold-Chiari deformity. Neurochirurgia 35:183-188, 1992. [Medline Link] [Context Link]
30. Doherty JM, Spence DP, Young C, Calverley PM: Obstructive sleep apnoea with Arnold-Chiari malformation. Thorax 50:690-691, 1995. [Fulltext Link] [Medline Link] [BIOSIS Previews Link] [Context Link]
31. Dyste GN, Menezes AH: Presentation and management of Pediatric Chiari malformations without myelodysplasia. Neurosurgery 23:589-597, 1988. [Medline Link] [BIOSIS Previews Link] [Context Link]
32. Dyste GN, Menezes AH, VanGilder JC: Symptomatic Chiari malformations: An analysis of presentation, management, and long-term outcome. J Neurosurg 71:159-168, 1989. [Medline Link] [Context Link]
33. Elster AD, Chen MY: Chiari I malformations: Clinical and radiologic reappraisal. Radiology 183:347-353, 1992. [Medline Link] [BIOSIS Previews Link] [Context Link]
34. Elta GH, Caldwell CA, Nostrant TT: Esophageal dysphagia as the sole symptom in type I Chiari malformation. Dig Dis Sci 41:512-515, 1996. [Fulltext Link] [Medline Link] [BIOSIS Previews Link] [Context Link]
35. Friede RL, Roessmann U: Chronic tonsillar herniation: An attempt at classifying chronic herniations at the foramen magnum. Acta Neuropathol (Berl) 34:219-235, 1976. [Medline Link] [BIOSIS Previews Link] [Context Link]
36. Gamache FW, Ducker TB: Syringomyelia: A neurological and surgical spectrum. J Spinal Disord 3:293-298, 1990. [Medline Link] [Context Link]
37. Gardner WJ, Goodall RJ: The surgical treatment of Arnold-Chiari malformation in adults: An explanation of its mechanism and importance of encephalography in diagnosis. J Neurosurg 7:199-206, 1950. [Context Link]
38. Gingold SI, Winfield JA: Oscillopsia and primary cerebellar ectopia: Case report and review of the literature.
Page 22 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
Neurosurgery 29:932-936, 1992. [BIOSIS Previews Link] [Context Link]
39. Gripp KW, Scott CI Jr, Nicholson L, Magram G, Grissom LE: Chiari malformation and tonsillar ectopia in twin brothers and father with autosomal dominant spondylo-epiphyseal dysplasia tarda. Skeletal Radiol 26:131-133, 1997. [Medline Link] [Context Link]
40. Gundersen HJG, Boysen M, Reith A: Comparison of semiautomatic digitizer-tablet and simple point counting performance in morphometry. Virchows Arch [B] 37:317-325, 1981. [Medline Link] [BIOSIS Previews Link] [Context Link]
41. Hendrix RA, Bacon CK, Sclafani AP: Chiari I malformation associated with asymmetric sensorineural hearing loss. J Otolaryngol 21:102-107, 1992. [Medline Link] [BIOSIS Previews Link] [Context Link]
42. House WF: Meniere's disease: Management and theory. Otolaryngol Clin North Am 8:515-535, 1975. [Medline Link] [BIOSIS Previews Link] [Context Link]
43. Ireland PD, Mickelsen D, Rodenhouse TG, Bakos RS, Goldstein B: Evaluation of the autonomic cardiovascular response in Arnold-Chiari deformities and cough syncope syndrome. Arch Neurol 53:526-531, 1996. [Medline Link] [BIOSIS Previews Link] [Context Link]
44. Johnson GD, Harbaugh RE, Lenz SB: Surgical decompression of Chiari I malformation for isolated progressive sensorineural hearing loss. Am J Otol 15:634-638, 1994. [Medline Link] [BIOSIS Previews Link] [Context Link]
45. Karnofsky DA, Burchenal JH, Armistead GC, Southam CM, Bernstein JL, Craver LF, Rhoads CP: Triethylene melamine in the treatment of neoplastic disease. Arch Intern Med 87:477-516, 1951. [Context Link]
46. Keefover R, Sam M, Bodensteiner J, Nicholson A: Hypersomnolence and pure central sleep apnea associated with the Chiari I malformation. J Child Neurol 10:65-67, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
47. Khurana RK: Headache spectrum in Arnold-Chiari malformation. Headache 31:151-155, 1991. [Medline Link] [Context Link]
48. Kumar A, Pieri A, Krol G: Rebound caloric nystagmus. Laryngoscope 103:1205-1213, 1993. [Medline Link] [Context Link]
49. Levitt P, Cohn MA: Sleep apnea and the Chiari I malformation: Case report. Neurosurgery 23:508-510, 1988. [Medline Link] [BIOSIS Previews Link] [Context Link]
50. Levy WJ, Mason L, Hahn JF: Chiari malformation presenting in adults: A surgical experience in 127 cases. Neurosurgery 12:377-390, 1983. [Medline Link] [Context Link]
51. Lewis AR, Kline LB, Sharpe JA: Acquired esotropia due to Arnold-Chiari I malformation. J Neuroophthalmol 16:49-54, 1996. [Medline Link] [Context Link]
52. Malis LI, Cohen IRA, Gross SW: Arnold-Chiari malformation. Arch Surg 63:783-798, 1951. [Context Link]
53. Mampalam TJ, Andrews BT, Gelb D, Ferriero D, Pitts LH: Presentation of type I Chiari malformation after head trauma. Neurosurgery 23:760-762, 1988. [Medline Link] [BIOSIS Previews Link] [Context Link]
54. Marin-Padilla M: Notochordal-basichondrocranium relationships: Abnormalities in experimental axial skeletal (dysraphic) disorders. J Embryol Exp Morphol 53:15-38, 1979. [Medline Link] [Context Link]
55. Marin-Padilla M, Marin-Padilla TM: Morphogenesis of experimentally induced Arnold-Chiari malformation. J Neurol Sci 50:29-55, 1981. [Medline Link] [BIOSIS Previews Link] [Context Link]
56. Maroun FB, Jacob JC, Mangan M: The Chiari malformation in adults. Can J Neurol Sci 2:115-120, 1975. [Medline Link] [Context Link]
57. Martinot A, Hue V, Leclerc F, Valee L, Closset M, Pruvo JP: Sudden death revealing Chiari type I malformation in
Page 23 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi

two children. Intensive Care Med 19:73-74, 1993. [Medline Link] [Context Link]
58. Mayhew TM, Olsen DR: Magnetic resonance imaging (MRI) and model-free estimates of brain volume determined using the Cavalieri principle. J Anat 178:133-144, 1991. [Medline Link] [BIOSIS Previews Link] [Context Link]
59. McLone DG, Knepper PA: The cause of Chiari II malformation: A unified theory. Pediatr Neurosci 15:1-12, 1989. [Medline Link] [BIOSIS Previews Link] [Context Link]
60. Milhorat TH: Cerebrospinal fluid physiology, in Milhorat TH: Hydrocephalus and the Cerebrospinal Fluid. Baltimore, Williams & Wilkins, 1972, pp 1-41. [Context Link]
61. Milhorat TH, Capocelli AL Jr, Anzil AP, Kotzen RM, Milhorat RH: Pathological basis of spinal cord cavitation in syringomyelia: Analysis of 105 autopsy cases. J Neurosurg 82:802-812, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
62. Milhorat TH, Johnson RW, Milhorat RH, Capocelli AL Jr, Pevsner PH: Clinicopathologic correlations in syringomyelia using axial magnetic resonance imaging. Neurosurgery 37:206-213, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
63. Milhorat TH, Kotzen RM, Anzil AP: Stenosis of central canal of spinal cord in man: Incidence and pathological findings in 232 autopsy cases. J Neurosurg 80:716-722, 1994. [Medline Link] [BIOSIS Previews Link] [Context Link]
64. Milhorat TH, Kotzen RM, Mu HTM, Capocelli AL Jr, Milhorat RH: Dysesthetic pain in patients with syringomyelia. Neurosurgery 38:940-947, 1996. [Fulltext Link] [Medline Link] [BIOSIS Previews Link] [Context Link]
65. Milhorat TH, Miller JI, Johnson WD, Adler DE, Heger IM: Anatomical basis of syringomyelia occurring with hindbrain lesions. Neurosurgery 32:748-754, 1993. [Medline Link] [BIOSIS Previews Link] [Context Link]
66. Milhorat TH, Nakamura S, Heger I, Nobandegani F, Murray S: Ultrastructural evidence of sink function of central canal of spinal cord as demonstrated by clearance of horseradish peroxidase. Electron Microsc Soc Am Proc 50:700-701, 1992. [Context Link]
67. Milhorat TH, Nobandegani F, Miller JI, Rao C: Noncommunicating syringomyelia following occlusion of the central canal in rats: Experimental model and histological findings. J Neurosurg 78:274-279, 1993. [Medline Link] [BIOSIS Previews Link] [Context Link]
68. Mossman SS, Bronstein AM, Gresty MA, Kendall B, Rudge P: Convergence nystagmus associated with Arnold-Chiari malformation. Arch Neurol 47:357-359, 1990. [Medline Link] [BIOSIS Previews Link] [Context Link]
69. Nakai T, Asato R, Miki Y, Tanaka F, Matsumoto S, Konishi J: A case of achondroplasia with downward displacement of the brain stem. Neuroradiology 37:293-294, 1995. [Medline Link] [Context Link]
70. National Organization of Rare Disease: Directory. New Fairfield, CT, National Organization of Rare Diseases, 1997. [Context Link]
71. Nishikawa M, Sakamoto H, Hakuba A, Nakanishi N, Inoue Y: Pathogenesis of Chiari malformation: A morphometric study of the posterior cranial fossa. J Neurosurg 86:40-47, 1997. [Medline Link] [BIOSIS Previews Link] [Context Link]
72. Nylan H, Krogness KG: Size of posterior fossa in Chiari type I malformation in adults. Acta Neurochir (Wien) 40:233-242, 1978. [Medline Link] [BIOSIS Previews Link] [Context Link]
73. Oldfield EH, Muraszko K, Shawker TH, Patronas NJ: Pathophysiology of syringomyelia associated with Chiari I malformation of the cerebellar tonsils: Implications for diagnosis and treatment. J Neurosurg 80:3-15, 1994. [Medline Link] [BIOSIS Previews Link] [Context Link]
74. Pakkenberg B, Boesen J, Albeck M, Gjerris F: Unbiased and efficient estimation of total ventricular volume of the brain obtained from CT scans by a stereological method. Neuroradiology 31:413-417, 1989. [Medline Link] [BIOSIS Previews Link] [Context Link]
Page 24 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi

75. Palma V, Sinisi L, Andreone V, Fazio N, Serra LL, Ambrosio G, DeMichele G: Hind-brain hernia headache and syncope in type I Arnold-Chiari malformation. Acta Neurol (Napoli) 15:457-461, 1993. [Medline Link] [Context Link]
76. Pascual J, Iglesias F, Oterino A, Vazquez-Barquero A, Berciano J: Cough, exertional, and sexual headaches: An analysis of 72 benign and symptomatic cases. Neurology 46:1520-1524, 1996. [Fulltext Link] [Medline Link] [PsycINFO Link] [BIOSIS Previews Link] [Context Link]
77. Pascual J, Oterino A, Berciano J: Headache in type I Chiari malformation. Neurology 42:1519-1521, 1992. [Medline Link] [BIOSIS Previews Link] [Context Link]
78. Pillay PK, Awad IA, Little JR, Hahn JF: Symptomatic Chiari malformation in adults: A new classification based on magnetic resonance imaging with clinical and prognostic significance. Neurosurgery 28:639-645, 1991. [Medline Link] [BIOSIS Previews Link] [Context Link]
79. Pollack IF, Pang D, Kocoshis S, Putnam P: Neurogenic dysphagia resulting from Chiari malformations. Neurosurgery 30:709-719, 1992. [Medline Link] [BIOSIS Previews Link] [Context Link]
80. Pryce AP, Wiener SN: Syringomyelia associated with Paget's disease of the skull. AJR Am J Roentgenol 155:881-882, 1990. [Medline Link] [BIOSIS Previews Link] [Context Link]
81. Pujol J, Roig C, Capdevilla A, Pou A, Marti-Vilalta JL, Kulisevsky J, Escartin A, Zannoli G: Motion of the cerebellar tonsils in Chiari type I malformation studied by CINE phase-contrast MRI. Neurology 45:1746-1753, 1995. [Fulltext Link] [Medline Link] [BIOSIS Previews Link] [Context Link]
82. Regeur L, Pakkenberg B: Optimizing sampling designs for volume measurements of components of human brain using a stereological method. J Microsc 155:113-121, 1989. [Medline Link] [BIOSIS Previews Link] [Context Link]
83. Ruff ME, Oakes WJ, Fisher SR, Spock A: Sleep apnea and vocal cord paralysis secondary to type I Chiari malformation. Pediatrics 80:231-234, 1987. [Medline Link] [BIOSIS Previews Link] [Context Link]
84. Rydell RE, Pulec JL: Arnold-Chiari malformation. Arch Otolaryngol 94:8-12, 1971. [Medline Link] [BIOSIS Previews Link] [Context Link]
85. Saez RJ, Onofrio BM, Yanagihara T: Experience with Arnold-Chiari malformation: 1960-1970. J Neurosurg 45:416-422, 1976. [Medline Link] [BIOSIS Previews Link] [Context Link]
86. Schady W, Metcalfe RA, Butler P: The incidence of craniocervical bony anomalies in the adult Chiari malformation. J Neurol Sci 82:193-203, 1987. [Medline Link] [BIOSIS Previews Link] [Context Link]
87. Sclafani AP, DeDio RM, Hendrix RA: The Chiari malformation. Ear Nose Throat J 70:208-212, 1991. [Medline Link] [BIOSIS Previews Link] [Context Link]
88. Selmi F, Davies KG, Weeks RD: Type I Chiari deformity presenting with profound sinus bradycardia: Case report and literature review. Br J Neurosurg 9:543-545, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
89. Semple DA, McClure JH: Arnold-Chiari malformation in pregnancy. Anaesthesia 51:580-582, 1996. [Fulltext Link] [Medline Link] [Context Link]
90. Spooner JW, Baloh RW: Arnold-Chiari malformation: Improvement in eye movements after surgical treatment. Brain 104:51-60, 1981. [Medline Link] [Context Link]
91. Stoodley MA, Brown SA, Brown CJ, Jones NR: Arterial pulsation-dependent perivascular cerebrospinal fluid flow into the central canal in the sheep spinal cord. J Neurosurg 86:686-693, 1997. [Medline Link] [BIOSIS Previews Link] [Context Link]
92. Stovner LJ: Headaches and Chiari type I malformation: Occurrence in female monozygotic twins and first-degree relatives. Cephalalgia 12:304-307, 1992. [Medline Link] [BIOSIS Previews Link] [Context Link]
Page 25 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
93. Stovner LJ: Headache associated with the Chiari type I malformation. Headache 33:175-181, 1993. [Medline Link] [BIOSIS Previews Link] [Context Link]
94. Stovner LJ, Rinck P: Syringomyelia in Chiari malformation: Relation to extent of cerebellar tissue herniation. Neurosurgery 31:913-917, 1992. [Medline Link] [BIOSIS Previews Link] [Context Link]
95. Stovner LJ, Sjaastad O: Segmental hyperhidrosis in two siblings with Chiari type I malformation. Eur Neurol 35:149-155, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
96. Stovner LJ, Bergan U, Nilsen G, Sjaastad O: Posterior cranial fossa dimensions in the Chiari I malformation: Relation to pathogenesis and clinical presentation. Neuroradiology 35:113-118, 1993. [Medline Link] [Context Link]
97. Stovner LJ, Kruszewski P, Shen JM: Sinus arrhythmia and pupil size in Chiari I malformation: Evidence of autonomic dysfunction. Funct Neurol 8:251-257, 1993. [Medline Link] [Context Link]
98. Sullivan LP, Stears JC, Ringel SP: Resolution of syringomyelia and Chiari I malformation by ventriculoatrial shunting in patient with pseudotumor cerebri and a lumboperitoneal shunt. Neurosurgery 22:744-747, 1988. [Medline Link] [BIOSIS Previews Link] [Context Link]
99. Tanimoto A, Tamaki N, Nagashima T, Nakamura M: Syringomyelia associated with Hadju-Cheney syndrome: Case report. Neurosurgery 39:400-403, 1996. [Fulltext Link] [Medline Link] [BIOSIS Previews Link] [Context Link]
100. Tortosa A, Arbizu T, Ferran E, Peres J: Trigeminal neuralgia as the first manifestation in Arnold-Chiari deformity. Neurologia 6:148-150, 1991. [Medline Link] [Context Link]
101. Ulmer JL, Elster AD, Ginsberg LE, Williams DW: Klippel-Feil syndrome: CT and MR of acquired and congenital abnormalities of cervical spine and cord. J Comput Assist Tomogr 17:215-224, 1993. [Medline Link] [Context Link]
102. Vega A, Quintana F, Berciano J: Basichondrocranium anomalies in adult Chiari type I malformation: A morphometric study. J Neurol Sci 99:137-145, 1990. [Medline Link] [BIOSIS Previews Link] [Context Link]
103. Weber PC, Cass SP: Neurotologic manifestations of Chiari I malformation. Otol Head Neck 109:853-860, 1993. [Context Link]
104. Weig SG, Buckthal PE, Choi SK, Zellem RT: Recurrent syncope as the presenting symptom of Arnold-Chiari malformation. Neurology 41:1673-1674, 1991. [Medline Link] [BIOSIS Previews Link] [Context Link]
105. Wiggs WJ Jr, Sismanis A, Laine FJ: Pulsatile tinnitus associated with congenital central nervous system malformations. Am J Otol 17:241-244, 1996. [Medline Link] [BIOSIS Previews Link] [Context Link]
106. Williams B: On the pathogenesis of syringomyelia: A review. J R Soc Med 73:798-806, 1980. [Medline Link] [Context Link]
107. Wurm G, Pogady P, Markut H, Fischer J: Three cases of hindbrain herniation in adults with comments on some diagnostic difficulties. Br J Neurosurg 10:137-142, 1996. [Medline Link] [BIOSIS Previews Link] [Context Link]
108. Yamanochi H, Iwasaki Y, Sugai K, Mukuno K: Duane retraction syndrome associated with Chiari I malformation. Pediatr Neurol 9:327-329, 1993. [Medline Link] [Context Link]
109. Zakeri A, Glasauer FE, Egnatchik JG: Familial syringomyelia: Case report and review of the literature. Surg Neurol 44:48-53, 1995. [Medline Link] [BIOSIS Previews Link] [Context Link]
Key words: Basilar invagination; Cerebellar ectopia; Chiari malformation; Cranial base dysplasia; Genetic transmission; Hydrocephalus; Meniere's syndrome; Pseudotumor cerebri; Scoliosis; Syringomyelia
Page 26 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi
Accession Number: 00006123-199905000-00042
Copyright (c) 2000-2002 Ovid Technologies, Inc. Version: rel5.1.0, SourceID 1.6412.1.59
Page 27 of 27Ovid: Milhorat: Neurosurgery, Volume 44(5).May 1999.1005-1017
10/23/2002http://gateway2.ovid.com/ovidweb.cgi