Embed Size (px)
Citation preview

Chondrodysplasia Punctata Stemming FromMaternal Lupus Erythematosus
Thaddeus E. Kelly,1* Bennett A. Alford,2 and Kenneth M. Greer3
1Division of Medical Genetics, University of Virginia School of Medicine, Charlottesville, Virginia2Division of Pediatric Radiology, University of Virginia School of Medicine, Charlottesville, Virginia3Department of Dermatology, University of Virginia School of Medicine, Charlottesville, Virginia
The finding of stippled epiphyses on a neo-natal radiograph generates a wide differen-tial diagnosis, including genetic and terato-genic causes. We report the case of a maleinfant with stippled epiphyses evident onneonatal radiographs in whom a typicalrash of lupus erythematosus developed. Theskin abnormalities in the infant resulted ina diagnosis of systemic lupus erythematosusin his mother. Over a 3-year follow-up pe-riod, the child has demonstrated strikinglyshort stature, midface hypoplasia, anoma-lous digital development, slow resolution ofthe stippled epiphyses, and near normalcognitive development. The differential di-agnosis of chondrodysplasia punctata andthe literature supporting maternal lupus asone cause are reviewed. Am. J. Med. Genet.83:397–401, 1999. © 1999 Wiley-Liss, Inc.
KEY WORDS: chondrodysplasia punctata;stippled epiphyses; lupuserythematosus
INTRODUCTION
The finding of stippled epiphyses on a neonatal ra-diograph generates a broad differential diagnosis. Avariety of genetic disorders, including skeletal dyspla-sias and metabolic disorders, are included with the fullarray of modes of inheritance. Maternal use of couma-din during pregnancy is a well-recognized cause of neo-natal stippled epiphyses, which is associated with mid-face hypoplasia. This condition carries a good prognosisfor growth and development [Shaul et al., 1972]. Sev-eral recent reports suggest that maternal systemic lu-pus erythematosus (SLE) is a newly recognized causeof neonatal stippled epiphyses [Elcioglu and Hall,1998; Austin-Ward et al., 1998]. We report the case of
a male infant with neonatal lupus erythematosus(NLE) and chondrodysplasia punctata with midfacehypoplasia who, over a 3-year follow-up period hasdemonstrated strikingly short stature and anomalousdigital development, but near normal cognitive devel-opment.
CLINICAL REPORT
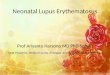
This African-American male infant was born at 335⁄7weeks’ gestation to a 30-year-old primigravida. Shehad had a long history of irregular menses, and herpregnancy followed the use of clomid. She received noprenatal care before 30 weeks’ gestation. Her prenatallaboratory test values at that time were all normal.Delivery was assisted by low forceps; Apgar scoreswere 8 and 9 at one and five min, respectively. Thebaby’s birth weight was 1,890 g, and he was 42 cm inlength with a head circumference (OFC) of 30.5 cm.The Dubowitz score was consistent with 34 weeks’ ges-tation. His neonatal examination was noteworthy forsmall ears, upward-slanting palpebral fissures, mid-face hypoplasia, and a short columella. His hands andfeet were small for his size, and his second fingers bi-laterally were particularly short. His karyotype was anormal male 46,XY. Posterior–anterior and lateralchest radiographs were initially considered normal;however, subsequent review demonstrated a stippledsecondary ossification center the right proximal hu-merus and calcific stippling of the sacrum. At the age of1 month, the baby was brought to the outpatient clinicwith a 2-day history of a rash. The rash consisted of3-mm to 1.5-cm raised erythematous macules with cen-tral clearing over his neck, wrists, ankles, and anteriorthorax totaling about 15 lesions (Fig. 1).
One week later the rash had worsened slightly, anda skin biopsy sample was taken of one of the lesions.The biopsy sample demonstrated a moderate lymphoidinfiltrate in the dermis, with edema of the papillarydermis but an absence of necrobiosis. This rash wasinterpreted as mild interface dermatitis, as seen in er-ythema multiforme or lupus. Immunofluorescent stud-ies showed positive granular IgG and C3 along the der-mal–epidermal junction; test results were also positivefor IgA, C3, and fibrin in the dermal vessels. The his-tologic findings were interpreted as being suggestive of
*Correspondence to: Thaddeus E. Kelly, M.D., Ph.D., Box 386,University Hospital, Charlottesville, VA 22908. E-mail:[email protected]
Received 10 November 1998; Accepted 18 December 1998
American Journal of Medical Genetics 83:397–401 (1999)
© 1999 Wiley-Liss, Inc.

a diagnosis of NLE. When the baby was 6 weeks old, atest for antinuclear antibody gave positive results, witha speckled pattern on immunofluorescence. Furthertesting showed that the patient had antibody to ribo-nucleoprotein (RNP), but tests for antibody to Sm, Ro,La, and double-stranded DNA gave negative results.
The baby’s mother had been followed at the Univer-sity Hospital intermittently since her birth. Other thanher problem with infertility, she enjoyed good health.When questioned, she reported a 2-year history of mildstiffness and soreness of her wrists and knees. A testfor antinuclear antibody showed positive results, witha speckled pattern on immunofluorescence. Furthertesting found antibody to RNP at a high titer (1:12,800). Tests for antibody to Sm, Ro, La, and double-stranded DNA gave negative results. She was referredto the rheumatology clinic, where a diagnosis of SLEwith associated thrombocytopenia was confirmed. Shehad a dramatic response to short-term steroid therapy,and two years later she remains asymptomatic withoutfurther steroid therapy.
At 4 months of age, the infant was 60 cm long andweighed 6.7 kg. Apart from his continuing rash, hismother reported that he had no other problems. In ad-dition to his growth retardation, his examination was
notable for the facial and digital anomalies as well asshort arms and legs. He had striking laxity of the jointsof his legs. A series of skeletal radiographs demon-strated stippled epiphyses at many sites and abnor-malities of his digits (Fig. 2).
Plasma very long chain fatty acid (VLCFA) levelswere normal, as were those of calcium, phosphorus,and alkaline phosphatase, but the acid phosphataselevel was 23.38 U/L (normal: 0.40–4.5). While the boy’sgeneral health remained good, his growth rate slowedover the next 30 months. He fell further behind in hislinear growth such that at age 35 months, his lengthwas 86.5 cm (less than the fifth centile), his weight was11.8 kg (less than the fifth centile), and his OFC was49.3 cm (10th centile).
Skeletal radiographs made at ages 4 and 34 monthsshowed mild stippling of the secondary ossification cen-ter of the right proximal humerus. He had generalizedbrachydactyly of the hands. The first and second proxi-mal phalanges bilaterally were particularly shortened,as was the fourth metacarpal. There was stippled os-sification at the bases of the phalanges. In the feet,there were stippled ossification centers for the hindfoot, and stippled ossifications were present at thebases of the first, second, and third distal phalanges.
Fig. 1. At age 6 weeks, midface hypoplasia and erythematosus rash (A) and annular chest lesions of NLE (B) are evident.
398 Kelly et al.

There were numerous stippled ossifications in the re-gion of the sacrum. Follow-up radiographs at 34months of age showed decreased stippling of secondaryossification centers with residual brachydactyly (Fig. 3).
DISCUSSION
In 1954, McCuistion and Schoch postulated the ex-istence of neonatal lupus skin disease in infants ofmothers with SLE. This theory was supported in 1981by the demonstration of autoantibodies (Ro) in the se-rum samples of mothers with SLE and their neonateswith NLE [Franco et al., 1981, Kephart et al., 1981]. Ina 1995 review, McCauliffe described the clinical mani-festations of NLE as involving four organ systems. Thecutaneous manifestations are erythematous annularplaques that appear weeks after delivery and resolve
by about age 6 months, with residual dyspigmentationand mild atrophy of the skin. The cardiac manifesta-tions include complete heart block, myocarditis, andcongestive heart failure. Hematologic abnormalities in-clude neonatal, self-limited depression of all cellularblood components. Finally, hepatic manifestations in-clude neonatal self-limited hepatomegaly, hepatitis,and cholestasis.
Most infants with NLE have anti-Ro (SS-A) and anti-La (SS-B) autoantibodies. These antibodies, transpla-centally acquired, are associated with all the clinicalforms of NLE. Sheth et al. [1995] reported the cases oftwo infants and reviewed reports of five others withNLE who were anti-Ro and anti-La negative but anti-RNP positive. These infants demonstrated only cuta-neous manifestations of NLE. Unfortunately, radio-graphic findings were not described in any of these re-
Fig. 2. A: At age 4 months, an anterior–posterior radiograph of the left hand shows brachydactyly, with stippled ossification of secondary ossificationcenters for the distal phalanges, and significant deformity of the proximal phalanges of the first and second digits. B: An anterior–posterior radiographof the of the foot shows stippled ossification of the tarsal centers and stippled ossification of the distal phalanges, with significant deformity of theproximal phalanx of the great toe.
Chondrodysplasia Punctata From Maternal Lupus 399

ports. The infant reported herein was anti-Ro and anti-La negative while being anti-RNP positive. He had thetypical cutaneous findings of NLE and striking skeletalabnormalities, but no cardiac, hepatic, or hematologicfindings.
Elcioglu and Hall [1998] reported on siblings whodied in utero at 36 and 24 weeks’ gestation, respec-tively. Their mother had SLE and was treated withsteroids during both pregnancies. Autopsy of the infant
who died at 36 weeks showed growth retardation(weight, length, and OFC less than the fifth centile),short limbs, midface hypoplasia, short digits, and hy-poplastic nails. Radiographs demonstrated stippledepiphyses, most notably of the sacrum, proximalfemora, hands, and feet. The infant who died at 24weeks showed stippling of the laryngeal cartilage, tar-sal bones, proximal femora, and distal humeri. Therewas growth retardation, evidenced by short limbs anddigits. Both fetuses were male; the first had a normal46,XY karyotype, but no studies of VLCFAs were done.Austin-Ward et al. [1998] reported on a female infantborn to a mother with SLE treated with prednisone andaspirin throughout her pregnancy. The infant showedIUGR, midface hypoplasia, and stippling of the sacrumand tarsal bones. Cutaneous manifestations of NLE de-veloped, but no other abnormalities. No follow-up wasprovided beyond 39 days of age.
In 1994, Mansour et al. reported chondrodysplasiapunctata in an extremely premature male infant bornto a mother with SLE. A female co-twin was normal.The male infant had growth retardation, short limbs,short digits, and midface hypoplasia; radiographsshowed stippling of the lumbosacral spine and the car-pal bones. In 1993, Costa et al. reported on two unre-lated infants with chondrodysplasia punctata whosemothers had SLE. The first was a female infant born at29 weeks’ gestation who had tarsal and sacral stip-pling. The cutaneous findings of NLE later developedand then resolved, and the infant was said to be devel-opmentally normal at 1 year of age. The second was amale infant born at 36 weeks’ gestation, with humeraland femoral stippling. The karyotype was normal, aswere VLCFAs. This infant died at 6 months of compli-cations of severe static encephalopathy.
The differential diagnosis of stippled epiphyses in anewborn infant is broad. Typical signs are rhizomelicshortness of the limbs combined with cataracts, mid-face hypoplasia, and poor growth and developmentalong with various peroxisomal defects, including defi-ciencies of four distinct peroxisomal enzymes. This con-stellation is also seen in Zellweger and Refsum syn-dromes. In these disorders there is defective metabo-lism of VLCFAs; elevated levels of phytanic acid andplasmalogens are diagnostic [Barr et al. 1993; Motleyet al., 1997; Purdue et al., 1997; Ofman et al., 1998].Stippled epiphyses are seen in a mild autosomal dom-inant form of a skeletal dysplasia known as Conradi-Hunermann disease [Sheffield et al., 1976]. This ep-onym has also been applied to an X-linked dominantdisorder that is lethal in the male fetus and an X-linkedrecessive disorder with arylsulfatase E deficiency [Kal-ter et al., 1989; Daniele et al., 1998]. It also occurs as anonspecific finding in some malformation syndromes,such as trisomy 18.
A variety of abnormalities involving vitamin K giverise to chondrodysplasia punctata. Maternal vitamin Kdeficiency stemming from various maternal gastroin-testinal disorders is an example. An autosomal reces-sive defect in vitamin K epoxide reductase gives rise tomultiple clotting factor deficiencies, including deficien-cies of factors II, VIII, and XI and protein S and C[Pauli et al., 1987]. Affected infants have stippled
Fig. 3. A: At age 34 months, a follow-up radiograph of the hand showsresidual digital deformities, especially involving the first and second digits,with decreased stippled ossification of secondary ossification centers. B: Alateral radiograph of the foot shows nearly complete resolution of the stip-pling of the tarsal centers.
400 Kelly et al.

epiphyses at birth. Best known among the latter groupis warfarin embryopathy as a result of maternal use ofcoumadin during pregnancy [Shaul et al., 1975]. In dis-orders with vitamin K abnormalities, the stippledepiphyses disappear later in childhood, while midfacehypoplasia persists beyond infancy. The similarity inthe manifestations of chondrodysplasia punctata stem-ming from vitamin K abnormalities and those seenwith NLE suggests that one of the many autoantibod-ies in SLE has an effect on vitamin K activity or resultsin a bleeding disorder within the developing epiphyses.
SLE is an autoimmune disease in which a variety ofautoantibodies is produced. Anti-Ro and anti-La arecommonly noted in infants with NLE. The few cases ofNLE reported to date to be associated with chondro-dysplasia punctata, and for which autoantibody assayswere done, suggest that there may be an associationwith the presence of anti-U1 RNP antibodies and skel-etal abnormalities. It appears that chondrodysplasiapunctata should be added to the list of teratogenic con-sequences of maternal SLE [Toriello, 1998]. Radio-graphic evaluation of newborns exposed to maternalSLE combined with further antibody studies will berequired to define the entity more accurately [Solomonet al.. 1995]. More reports that follow the course of suchchildren will be required, to better appreciate the long-term prognosis for these infants.
REFERENCESAustin-Ward E, Castillo S, Cuchacovich M, Espinoza A, Cofre-Beca J,
Gonzalez S, Solivelles X, Bloomfield J. 1998. Neonatal lupus syndrome:a case with chondrodysplasia punctata and other unusual manifesta-tions. J Med Genet 35:695–697.
Barr DGD, Kirk JM, Al Howasi M, Wanders RJA, Schutgens RBH. 1993.Rhizomelic chondrodysplasia punctata with isolated DHAP-AT defi-ciency. Arch Dis Child 68:415–417.
Costa T, Tiller G, Chitayat D, Silverman E. Maternal systemic lupus ery-thematosus (SLE) and chondrodysplasia punctata in two infants: coin-cidence or association? First Meeting of Bone Dysplasia Society, Chi-cago, June 1993.
Daniele A, Parenti G, d’Addio M, Andria G, Ballabio A, Meroni G. 1998.Biochemical characterization of arylsulfatase E and functional analysisof mutations found in patients with X-linked chondrodysplasia punc-tata. Am J Hum Genet 62:562–572.
Elcioglu N, Hall CM. 1998. Maternal systemic lupus erythematosus andchondrodysplasia punctata in two sibs: phenocopy or coincidence? JMed Genet 35:690–694.
Franco HL, Weston WL, Peebles C, Forstot SL, Phanuphak P. 1981. Au-toantibodies directed against sicca syndrome antigens in the neonatallupus syndrome. J Am Acad Dermatol 4:67–72.
Kalter DC, Atherton DJ, Clayton PT. 1989. X-linked dominant Conradi-Hunermann syndrome presenting as a congenital erythroderma. J AmAcad Dermatol 21:248–256.
Kephart DC, Hood AF, Provost TT. 1981. Neonatal lupus erythematosus:new serologic findings. J Invest Dermatol 77:331–333.
Mansour S, Liberman D, Young I. 1994. Brachytelephalangic chondrodys-plasia punctata in an extremely premature infant. Am J Med Genet53:81–82.
McCauliffe DP. 1995. Neonatal lupus erythematosus: a transplacentallyacquired autoimmune disorder. Semin Dermatol 14:47–53.
McCuiston CH, Schoch EP. 1954. Possible discoid lupus erythematosus ina newborn infant: report of a case with subsequent development ofsystemic lupus erythematosus in mother. Arch Dermatol 70:782–785.
Motley AM, Hettema EH, Hogenhout EM, Brites P, ten Asbroek ALMA,Wijburg FA, Baas F, Heijmans HS, Tabak HF, Wanders RJA, Distel B.1997. Rhizomelic chondrodysplasia punctata is a peroxisomal proteintargeting disease caused by a non-functional PTS2 receptor. NatureGenet 15:377–380.
Ofman R, Hettema EH, Hogenhout EM, Caruso U, Muijsers AO, WandersRJA.1998. Acyl-CoA: dihydroxyacetonephosphate acyltransferase:cloning of the human cDNA and resolution of the molecular basis inrhizomelic chondrodysplasia punctata type 2. Hum Mol Genet 7:847–853.
Pauli RM, Lian JB, Mosher DF, Suttie JW. 1987. Association of congenitaldeficiency of multiple vitamin K–dependent coagulation factors and thephenotype of the warfarin embryopathy: clues to the teratogenicity ofcoumadin derivatives. Am J Hum Genet 41:566–583.
Purdue PE, Zhang JW, Skoneczny M, Lararow PB. 1997. Rhizomelic chon-drodysplasia punctata is caused by deficiency of human PEX7, a ho-mologue of the yeast PTS2 receptor: Nature Genet 15:381–384.
Shaul W, Emery H, Hall JG. 1975. Chondrodysplasia punctata and mater-nal warfarin use during pregnancy. Am J Dis Child 129:360–362.
Sheffield LJ, Danks EM, Mayne V, Hutchinson LA. 1976. Chondrodyspla-sia punctata: 23 cases of a mild and relatively common variety. J Pe-diatr 89:916–923.
Sheth AP, Esterly NB, Ratoosh SL, Smith JP, Hebert AA, Silverman E.1995. U1 RNP positive neonatal lupus erythematosus: association withanti-La antibodies? Br J Dermatol 1995;132:520–526.
Solomon BA, Laude TA, Shalita AR. 1995. Neonatal lupus erythematosus:discordant disease expression of U RNP positive antibodies in fraternaltwins. Is this a subset of neonatal lupus erythematosus or a new syn-drome? J Am Acad Dermatol 32:858–862.
Toriello HV. 1998. Chondrodysplasia punctata and maternal systemic lu-pus erythematosus. J Med Genet 35:698–699.
Chondrodysplasia Punctata From Maternal Lupus 401