Embed Size (px)
Citation preview

Chromogranin B in Heart FailureA Putative Cardiac Biomarker Expressed in the Failing Myocardium
Helge Røsjø, MD; Cathrine Husberg, MSc, PhD; Mai Britt Dahl, MSc; Mats Stridsberg, MD, PhD;Ivar Sjaastad, MD, PhD; Alexandra Vanessa Finsen, MD, PhD; Cathrine Rein Carlson, MSc, PhD;
Erik Øie, MD, PhD; Torbjørn Omland, MD, PhD, MPH; Geir Christensen, MD, PhD, MHA
Background—Chromogranin B (CgB) is a member of the granin protein family. Because CgB is often colocalized withchromogranin A (CgA), a recently discovered cardiac biomarker, we hypothesized that CgB is regulated during heartfailure (HF) development.
Methods and Results—CgB regulation was investigated in patients with chronic HF and in a post–myocardial infarction HFmouse model. Animals were phenotypically characterized by echocardiography and euthanized 1 week after myocardialinfarction. CgB mRNA levels were 5.2-fold increased in the noninfarcted part of the left ventricle of HF animals comparedwith sham-operated animals (P�0.001). CgB mRNA level in HF animals correlated closely with animal lung weight (r�0.74,P�0.04) but not with CgA mRNA levels (r�0.20, P�0.61). CgB protein levels were markedly increased in both thenoninfarcted (110%) and the infarcted part of the left ventricle (70%) but unaltered in other tissues investigated. MyocardialCgB immunoreactivity was confined to cardiomyocytes. Norepinephrine, angiotensin II, and transforming growth factor-�increased CgB gene expression in cardiomyocytes. Circulating CgB levels were increased in HF animals (median levels inHF animals versus sham, 1.23 [interquartile range, 1.03 to 1.93] versus 0.98 [0.90 to 1.04] nmol/L; P�0.003) and in HFpatients (HF patients versus control, 1.66 [1.48 to 1.85] versus 1.47 [1.39 to 1.58] nmol/L; P�0.007), with levels increasingin proportion to New York Heart Association functional class (P�0.03 for trend). Circulating CgB levels were only modestlycorrelated with CgA (r�0.31, P�0.009) and B-type natriuretic peptide levels (r�0.27, P�0.014).
Conclusions—CgB production is increased and regulated in proportion to disease severity in the left ventricle andcirculation during HF development. (Circ Heart Fail. 2010;3:503-511.)
Key Words: heart failure � molecular biology � biological markers � chromogranin B
Advances in treatment of acute coronary syndromes havereduced short-term mortality following acute myocardial
infarction (MI), but at the cost of a higher incidence of post-MIheart failure (HF).1 Improved pathophysiological understandingof HF and better tools for risk prediction and diagnostic purposesare therefore needed.2 The cardiac biomarkers used routinely inclinical practice today are proteins specific to the diseasedmyocardium, either released during cell necrosis (cardiac spe-cific troponins)3 or secreted secondary to cardiomyocyte strain(B-type natriuretic peptide, BNP).4 However, there is still a needfor markers reflecting other pathophysiological processes inheart disease.5 Thus, identifying new proteins regulated in thefailing myocardium may potentially improve both the under-standing of HF development and lead to the discovery of novelcardiac biomarkers.
Clinical Perspective on p 511
Chromogranin B (CgB) is a 50-kDa protein belonging to agroup of acidic proteins called the granin protein family.6 Themost extensively studied and well-known member of thegranin family is chromogranin A (CgA), a protein currentlyused clinically as a biomarker in patients with neuroendocrinetumors.7 Recently, CgA has been shown to increase with theseverity of HF8 and to be an independent predictor ofmortality in patients with acute coronary syndrome.9–11
Moreover, increased CgA production has been demonstratedin cardiomyocytes of the failing myocardium.12 However, aconfounding factor possibly reducing CgA’s merit as acardiac biomarker is the increase in CgA levels seen with theuse of proton pump inhibitors (PPIs).13 In contrast, CgB
Received March 24, 2009; accepted May 24, 2010.From the Medical Division (H.R., M.B.D., T.O.) and EpiGen, Institute of Clinical Epidemiology and Molecular Biology (M.B.D.), Akershus University
Hospital, Lørenskog, Norway; the Institute of Clinical Medicine (H.R., T.O.), University of Oslo, Oslo, Norway; the Institute for Experimental MedicalResearch (C.H., I.S., C.R.C., G.C.), Oslo University Hospital, Ullevål, Oslo, Norway; the Department of Medical Sciences (M.S.), Uppsala University,Uppsala, Sweden; the Department of Cardiology (I.S.), Oslo University Hospital, Ullevål, Oslo, Norway; Research Institute for Internal Medicine (A.V.F.,E.Ø.) and the Department of Cardiology (A.V.F., E.Ø.), Oslo University Hospital, Rikshospitalet, Oslo, Norway; and the Center for Heart FailureResearch, University of Oslo, Oslo, Norway (H.R., C.H., M.B.D., I.S., A.V.F., C.R.C., E.Ø., T.O., G.C.).
The online-only Data Supplement is available at http://circheartfailure.ahajournals.org/cgi/content/full/CIRCHEARTFAILURE.109.867747/DC1.Correspondence to Helge Røsjø, MD, Medical Division, Akershus University Hospital, Sykehusveien 27, 1478 Lørenskog, Norway. E-mail
[email protected]© 2010 American Heart Association, Inc.
Circ Heart Fail is available at http://circheartfailure.ahajournals.org DOI: 10.1161/CIRCHEARTFAILURE.109.867747
503
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

levels appear to be unaffected by PPI use and may provideadditional diagnostic information to CgA in patients withneuroendocrine tumors.14 Additionally, colocalization ofCgA and CgB in atrial tissue has been documented,15 linkingCgB to the myocardium and possibly also cardiovascularpathophysiology. Accordingly, we hypothesized that CgBlevels in the myocardium and the circulation are increasedand closely regulated during HF development.
MethodsMouse Model of HFA permanent ligation of the left main coronary artery were per-formed in mice in the HF group, whereas sham-operated (sham)animals underwent the same procedure except ligation of thecoronary artery.16 Echocardiographic examination was performed 1week after the primary operation. The criteria for including animalsin the HF group have previously been validated.17
Patients With HF and Healthy Control SubjectsEighty patients with echocardiographically documented impairedsystolic function (left ventricular ejection fraction �50%) wereincluded in the clinical part of this study: 70 patients from theAkershus University Hospital outpatient HF clinic and 10 patientshospitalized at Akershus University Hospital for worsening HF withdyspnea as the most prominent symptom. All patients were classifiedaccording to the New York Heart Association (NYHA) functionalclass system by a single investigator (H.R.). Patients with noncurablemalignancy and life expectancy �1 year, acute MI, cardiac surgery,or percutaneous coronary intervention during the last 3 months werenot eligible for participation in the study. Accordingly, none of thehospitalized patients were diagnosed with an acute MI.
Twenty control subjects with similar age and sex distribution asthe patients were also recruited. These individuals had no history ofcardiovascular disease or other concurrent disease, no current symp-toms of cardiovascular disease as evaluated by 1 investigator (H.R.),and they did not use medication regularly.
The study protocol was approved by the Regional Ethics Com-mittee before the initiation of the study. All participants gave theirwritten informed consent prior to study commencement.
Quantitative Real-Time PCRGene expression was measured with premade TaqMan GeneExpression assays from Applied Biosystems (Foster City,Calif): mouse model: CgB (Mm00483287_m1), CgA(Mm00514341_m1), BNP (Mm00435304_g1), ribosomal proteinL4 (RPL4) (Mm00834993_g1); and rat cardiomyocytes: CgB(Rn01514853_m1), CgA (Rn00572200_m1), BNP (Rn00580641_m1),RPL4 (Rn00821091_g1).
Immunoblotting and ImmunhistochemistryA purified polyclonal goat antihuman CgB was used for immuno-blotting (1:100 dilution) and immunhistochemistry (Sc-1489, SantaCruz Biotechnology, Santa Cruz, Calif). This antibody showedstrong and specific binding to the C-terminal region of CgB (seeOnline-only Data Supplement, Figure S1). A secondary antibody(diluted 1:2500) against goat (6160–05) was used for immunoblot-ting (Southern Biotech, Birmingham, Ala). CgA immunoreactivity inmouse myocardial sections was detected by a purified polyclonalrabbit antihuman CgA antibody (Sc-13090, Santa Cruz).
RadioimmunoassayPlasma CgB levels were measured by an in-house made region-specific radioimmunoassay (RIA) detecting CgB439–451,18 plasmaCgA levels by a commercial RIA identifying CgA116–439 (Euro-Diagnostica, Malmo, Sweden), and left ventricular (LV) tissue CgAlevels with an in-house made region-specific RIA detectingCgA361–372.19
Cell Culture ExperimentsAfter 24-hour starvation of the cells, neonatal rat cardiomyocyteswere stimulated as previously reported20 for 24 hours with thefollowing agents: forskolin (FSK) [10 �mol/L], norepinephrine (NE)[100 �mol/L], endothelin-1 (ET-1) [250 ng/mL], angiotensin II(AngII) [1 �mol/L] (all Sigma-Aldrich, St Louis, Mo), tumornecrosis factor-� (TNF-�) [10 ng/mL] (BioSource International,Camarillo, Calif), and transforming growth factor-� (TGF-�) [10ng/mL] (R&D Systems, Minneapolis, Minn).
Statistical AnalysisContinuous data are presented as mean (�SEM) or median andinterquartile range (IQR) and categorical values as counts (percent-age). Continuous variables were compared by the Student t testexcept circulating biomarker values that were compared by theMann–Whitney U test due to a right-skewed distribution. Categoricalvariables were compared by the �2 test or Fisher exact test asappropriate. Correlations and trends were calculated using Spearmanrank correlation. Probability values �0.05 were considered signifi-cant for all analyses. Statistical analyses were performed with SPSSfor Windows version 14.0 (SPSS, Chicago, Ill).
Details regarding methods can be found in the online-only DataSupplement. The authors (H.R., T.O., and G.C.) had full access tothe data and take responsibility for its integrity. All authors have readand agreed to the manuscript as written.
Results
Characteristics of AnimalsWe used a post-MI mouse HF model to study CgB production invarious tissues during HF development. As shown in Table 1,the animals included in the post-MI group had clear evidence ofHF and compensatory myocardial hypertrophy.
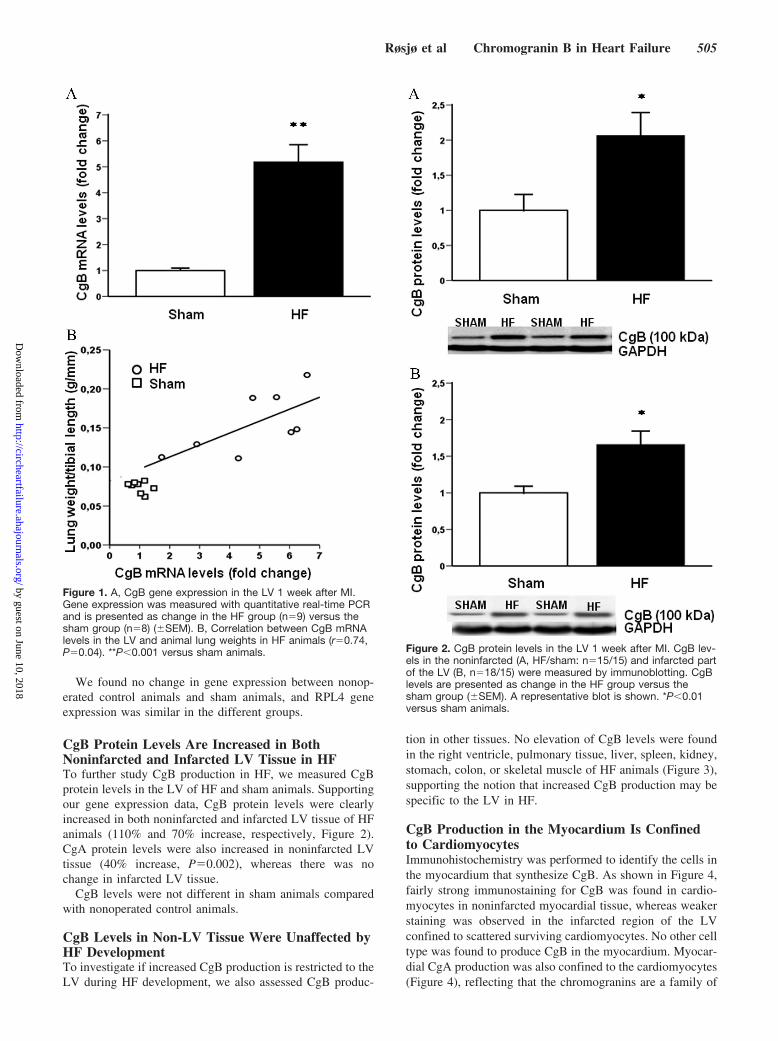
LV CgB Gene Expression Is Increased and CloselyRegulated in HFTo investigate regulation of CgB gene expression in the LVduring HF development, CgB mRNA levels in noninfarctedtissue of HF animals were compared with levels in shamanimals. CgB mRNA levels were 5.2 times upregulated in HFanimals (Figure 1A). Moreover, because CgB mRNA levelsin HF animals correlated with animal lung weights (r�0.74,P�0.04, Figure 1B), LV CgB gene expression appears to beclosely regulated in proportion to disease severity during HFdevelopment. CgA mRNA levels were also increased in HFanimals (4.8-fold increase, P�0.025), but there was nosignificant correlation between LV CgA and CgB mRNAlevels in HF (r�0.20, P�0.61) or sham animals (r�0.57,P�0.14).
Table 1. Descriptive Statistics of Animals
HF (n�35) Sham (n�29) P
Animal weight, day 0, g 24.2�0.3 24.3�0.4 0.83
Lung weight/tibial length, g/mm 0.161�0.007 0.079�0.001 �0.001
LV mass/tibial length, g/mm 0.057�0.001 0.045�0.001 �0.001
RV mass/tibial length, g/mm 0.013�0.001 0.011�0.001 0.004
LV BNP mRNA levels 5.8�0.7 1.0�0.1 �0.001
RV indicates right ventricle. BNP mRNA levels were analyzed in a subset ofanimals and are presented as mean change in the HF group (n�9) versus thesham group (n�8) (�SEM).
504 Circ Heart Fail July 2010
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
We found no change in gene expression between nonop-erated control animals and sham animals, and RPL4 geneexpression was similar in the different groups.
CgB Protein Levels Are Increased in BothNoninfarcted and Infarcted LV Tissue in HFTo further study CgB production in HF, we measured CgBprotein levels in the LV of HF and sham animals. Supportingour gene expression data, CgB protein levels were clearlyincreased in both noninfarcted and infarcted LV tissue of HFanimals (110% and 70% increase, respectively, Figure 2).CgA protein levels were also increased in noninfarcted LVtissue (40% increase, P�0.002), whereas there was nochange in infarcted LV tissue.
CgB levels were not different in sham animals comparedwith nonoperated control animals.
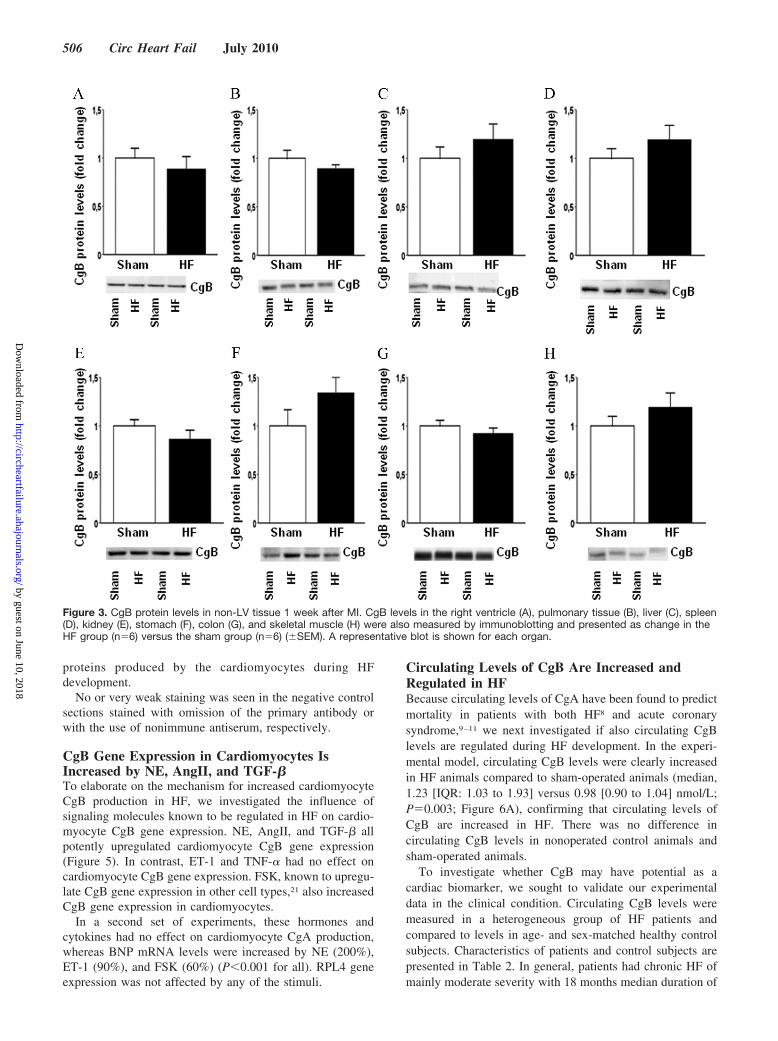
CgB Levels in Non-LV Tissue Were Unaffected byHF DevelopmentTo investigate if increased CgB production is restricted to theLV during HF development, we also assessed CgB produc-
tion in other tissues. No elevation of CgB levels were foundin the right ventricle, pulmonary tissue, liver, spleen, kidney,stomach, colon, or skeletal muscle of HF animals (Figure 3),supporting the notion that increased CgB production may bespecific to the LV in HF.
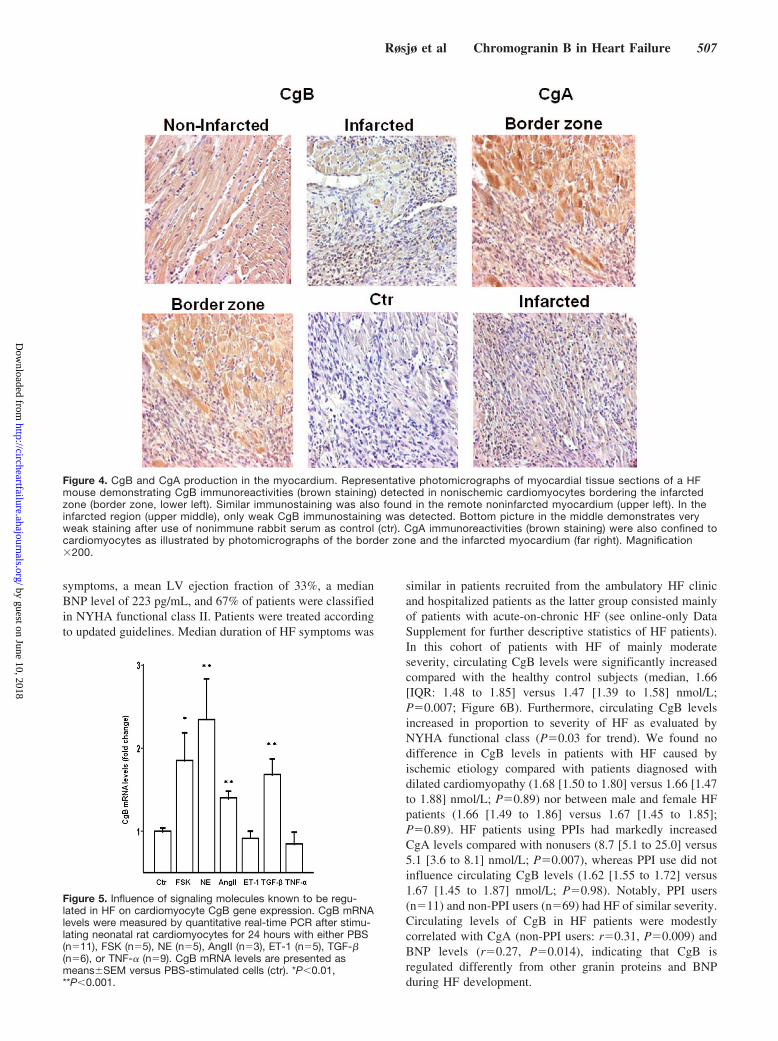
CgB Production in the Myocardium Is Confinedto CardiomyocytesImmunohistochemistry was performed to identify the cells inthe myocardium that synthesize CgB. As shown in Figure 4,fairly strong immunostaining for CgB was found in cardio-myocytes in noninfarcted myocardial tissue, whereas weakerstaining was observed in the infarcted region of the LVconfined to scattered surviving cardiomyocytes. No other celltype was found to produce CgB in the myocardium. Myocar-dial CgA production was also confined to the cardiomyocytes(Figure 4), reflecting that the chromogranins are a family of
Figure 1. A, CgB gene expression in the LV 1 week after MI.Gene expression was measured with quantitative real-time PCRand is presented as change in the HF group (n�9) versus thesham group (n�8) (�SEM). B, Correlation between CgB mRNAlevels in the LV and animal lung weights in HF animals (r�0.74,P�0.04). **P�0.001 versus sham animals. Figure 2. CgB protein levels in the LV 1 week after MI. CgB lev-
els in the noninfarcted (A, HF/sham: n�15/15) and infarcted partof the LV (B, n�18/15) were measured by immunoblotting. CgBlevels are presented as change in the HF group versus thesham group (�SEM). A representative blot is shown. *P�0.01versus sham animals.
Røsjø et al Chromogranin B in Heart Failure 505
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
proteins produced by the cardiomyocytes during HFdevelopment.
No or very weak staining was seen in the negative controlsections stained with omission of the primary antibody orwith the use of nonimmune antiserum, respectively.
CgB Gene Expression in Cardiomyocytes IsIncreased by NE, AngII, and TGF-�To elaborate on the mechanism for increased cardiomyocyteCgB production in HF, we investigated the influence ofsignaling molecules known to be regulated in HF on cardio-myocyte CgB gene expression. NE, AngII, and TGF-� allpotently upregulated cardiomyocyte CgB gene expression(Figure 5). In contrast, ET-1 and TNF-� had no effect oncardiomyocyte CgB gene expression. FSK, known to upregu-late CgB gene expression in other cell types,21 also increasedCgB gene expression in cardiomyocytes.
In a second set of experiments, these hormones andcytokines had no effect on cardiomyocyte CgA production,whereas BNP mRNA levels were increased by NE (200%),ET-1 (90%), and FSK (60%) (P�0.001 for all). RPL4 geneexpression was not affected by any of the stimuli.
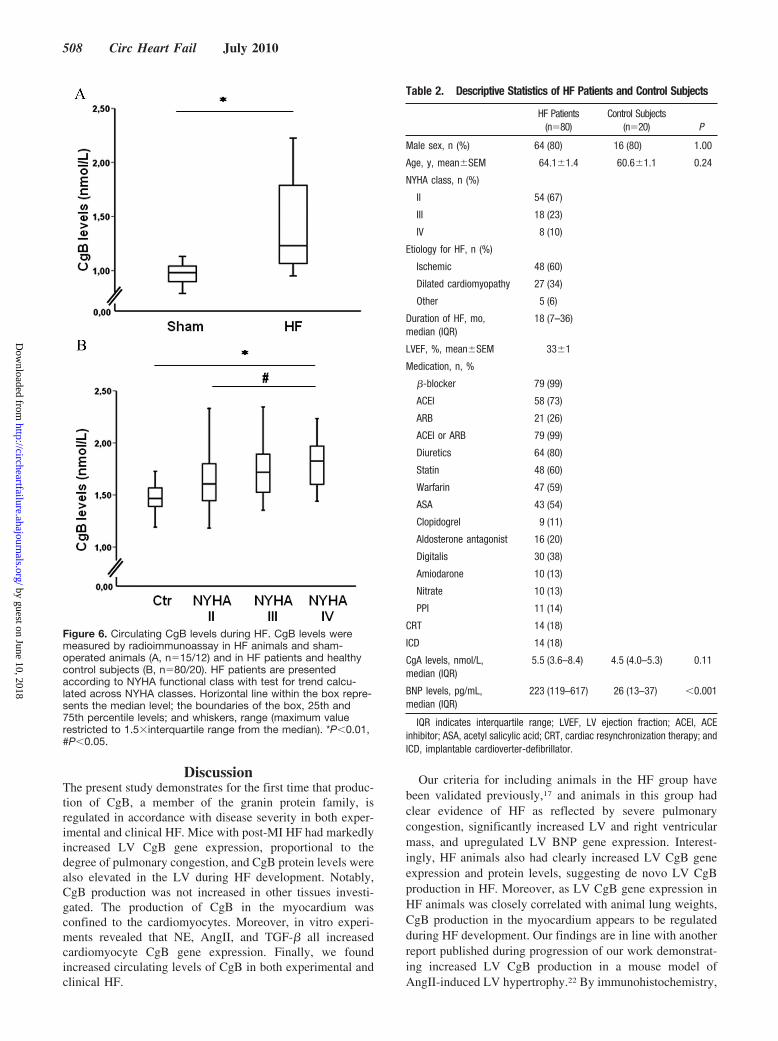
Circulating Levels of CgB Are Increased andRegulated in HFBecause circulating levels of CgA have been found to predictmortality in patients with both HF8 and acute coronarysyndrome,9–11 we next investigated if also circulating CgBlevels are regulated during HF development. In the experi-mental model, circulating CgB levels were clearly increasedin HF animals compared to sham-operated animals (median,1.23 [IQR: 1.03 to 1.93] versus 0.98 [0.90 to 1.04] nmol/L;P�0.003; Figure 6A), confirming that circulating levels ofCgB are increased in HF. There was no difference incirculating CgB levels in nonoperated control animals andsham-operated animals.
To investigate whether CgB may have potential as acardiac biomarker, we sought to validate our experimentaldata in the clinical condition. Circulating CgB levels weremeasured in a heterogeneous group of HF patients andcompared to levels in age- and sex-matched healthy controlsubjects. Characteristics of patients and control subjects arepresented in Table 2. In general, patients had chronic HF ofmainly moderate severity with 18 months median duration of
Figure 3. CgB protein levels in non-LV tissue 1 week after MI. CgB levels in the right ventricle (A), pulmonary tissue (B), liver (C), spleen(D), kidney (E), stomach (F), colon (G), and skeletal muscle (H) were also measured by immunoblotting and presented as change in theHF group (n�6) versus the sham group (n�6) (�SEM). A representative blot is shown for each organ.
506 Circ Heart Fail July 2010
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
symptoms, a mean LV ejection fraction of 33%, a medianBNP level of 223 pg/mL, and 67% of patients were classifiedin NYHA functional class II. Patients were treated accordingto updated guidelines. Median duration of HF symptoms was
similar in patients recruited from the ambulatory HF clinicand hospitalized patients as the latter group consisted mainlyof patients with acute-on-chronic HF (see online-only DataSupplement for further descriptive statistics of HF patients).In this cohort of patients with HF of mainly moderateseverity, circulating CgB levels were significantly increasedcompared with the healthy control subjects (median, 1.66[IQR: 1.48 to 1.85] versus 1.47 [1.39 to 1.58] nmol/L;P�0.007; Figure 6B). Furthermore, circulating CgB levelsincreased in proportion to severity of HF as evaluated byNYHA functional class (P�0.03 for trend). We found nodifference in CgB levels in patients with HF caused byischemic etiology compared with patients diagnosed withdilated cardiomyopathy (1.68 [1.50 to 1.80] versus 1.66 [1.47to 1.88] nmol/L; P�0.89) nor between male and female HFpatients (1.66 [1.49 to 1.86] versus 1.67 [1.45 to 1.85];P�0.89). HF patients using PPIs had markedly increasedCgA levels compared with nonusers (8.7 [5.1 to 25.0] versus5.1 [3.6 to 8.1] nmol/L; P�0.007), whereas PPI use did notinfluence circulating CgB levels (1.62 [1.55 to 1.72] versus1.67 [1.45 to 1.87] nmol/L; P�0.98). Notably, PPI users(n�11) and non-PPI users (n�69) had HF of similar severity.Circulating levels of CgB in HF patients were modestlycorrelated with CgA (non-PPI users: r�0.31, P�0.009) andBNP levels (r�0.27, P�0.014), indicating that CgB isregulated differently from other granin proteins and BNPduring HF development.
Figure 4. CgB and CgA production in the myocardium. Representative photomicrographs of myocardial tissue sections of a HFmouse demonstrating CgB immunoreactivities (brown staining) detected in nonischemic cardiomyocytes bordering the infarctedzone (border zone, lower left). Similar immunostaining was also found in the remote noninfarcted myocardium (upper left). In theinfarcted region (upper middle), only weak CgB immunostaining was detected. Bottom picture in the middle demonstrates veryweak staining after use of nonimmune rabbit serum as control (ctr). CgA immunoreactivities (brown staining) were also confined tocardiomyocytes as illustrated by photomicrographs of the border zone and the infarcted myocardium (far right). Magnification�200.
Figure 5. Influence of signaling molecules known to be regu-lated in HF on cardiomyocyte CgB gene expression. CgB mRNAlevels were measured by quantitative real-time PCR after stimu-lating neonatal rat cardiomyocytes for 24 hours with either PBS(n�11), FSK (n�5), NE (n�5), AngII (n�3), ET-1 (n�5), TGF-�(n�6), or TNF-� (n�9). CgB mRNA levels are presented asmeans�SEM versus PBS-stimulated cells (ctr). *P�0.01,**P�0.001.
Røsjø et al Chromogranin B in Heart Failure 507
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
DiscussionThe present study demonstrates for the first time that produc-tion of CgB, a member of the granin protein family, isregulated in accordance with disease severity in both exper-imental and clinical HF. Mice with post-MI HF had markedlyincreased LV CgB gene expression, proportional to thedegree of pulmonary congestion, and CgB protein levels werealso elevated in the LV during HF development. Notably,CgB production was not increased in other tissues investi-gated. The production of CgB in the myocardium wasconfined to the cardiomyocytes. Moreover, in vitro experi-ments revealed that NE, AngII, and TGF-� all increasedcardiomyocyte CgB gene expression. Finally, we foundincreased circulating levels of CgB in both experimental andclinical HF.
Our criteria for including animals in the HF group havebeen validated previously,17 and animals in this group hadclear evidence of HF as reflected by severe pulmonarycongestion, significantly increased LV and right ventricularmass, and upregulated LV BNP gene expression. Interest-ingly, HF animals also had clearly increased LV CgB geneexpression and protein levels, suggesting de novo LV CgBproduction in HF. Moreover, as LV CgB gene expression inHF animals was closely correlated with animal lung weights,CgB production in the myocardium appears to be regulatedduring HF development. Our findings are in line with anotherreport published during progression of our work demonstrat-ing increased LV CgB production in a mouse model ofAngII-induced LV hypertrophy.22 By immunohistochemistry,
Figure 6. Circulating CgB levels during HF. CgB levels weremeasured by radioimmunoassay in HF animals and sham-operated animals (A, n�15/12) and in HF patients and healthycontrol subjects (B, n�80/20). HF patients are presentedaccording to NYHA functional class with test for trend calcu-lated across NYHA classes. Horizontal line within the box repre-sents the median level; the boundaries of the box, 25th and75th percentile levels; and whiskers, range (maximum valuerestricted to 1.5�interquartile range from the median). *P�0.01,#P�0.05.
Table 2. Descriptive Statistics of HF Patients and Control Subjects
HF Patients(n�80)
Control Subjects(n�20) P
Male sex, n (%) 64 (80) 16 (80) 1.00
Age, y, mean�SEM 64.1�1.4 60.6�1.1 0.24
NYHA class, n (%)
II 54 (67)
III 18 (23)
IV 8 (10)
Etiology for HF, n (%)
Ischemic 48 (60)
Dilated cardiomyopathy 27 (34)
Other 5 (6)
Duration of HF, mo,median (IQR)
18 (7–36)
LVEF, %, mean�SEM 33�1
Medication, n, %
�-blocker 79 (99)
ACEI 58 (73)
ARB 21 (26)
ACEI or ARB 79 (99)
Diuretics 64 (80)
Statin 48 (60)
Warfarin 47 (59)
ASA 43 (54)
Clopidogrel 9 (11)
Aldosterone antagonist 16 (20)
Digitalis 30 (38)
Amiodarone 10 (13)
Nitrate 10 (13)
PPI 11 (14)
CRT 14 (18)
ICD 14 (18)
CgA levels, nmol/L,median (IQR)
5.5 (3.6–8.4) 4.5 (4.0–5.3) 0.11
BNP levels, pg/mL,median (IQR)
223 (119–617) 26 (13–37) �0.001
IQR indicates interquartile range; LVEF, LV ejection fraction; ACEI, ACEinhibitor; ASA, acetyl salicylic acid; CRT, cardiac resynchronization therapy; andICD, implantable cardioverter-defibrillator.
508 Circ Heart Fail July 2010
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

we demonstrated that CgB production is confined to thecardiomyocytes in the myocardium. We postulate that themyocardium may be an important source of increase incirculating CgB levels found in HF because (1) CgB produc-tion was increased in a closely regulated manner in the LVduring HF development, (2) no regulation of CgB productionwas found in any other organ investigated, and (3) CgB andthe chromogranins are considered marker-proteins for exocy-tosis in numerous cell types.23
The mechanism for increased CgB production in cardio-myocytes was investigated in vitro. We used FSK as apositive control as the CgB promoter contains a cAMPresponse element.24 NE has been found to activate cAMPresponse element transcription sites through both �1- and�-adrenergic receptor signaling,25,26 and NE-induced increasein CgB gene expression may reflect CgB stimulus-transcription-secretion coupling in the myocardium duringHF, a mechanism known to be important for CgB productionand secretion in nonmyocardial tissue.21 Because circulatingNE levels in HF are increased in proportion to patient NYHAfunctional class,27 the effect of NE on cardiomyocyte CgBproduction, and possibly also secretion, may explain the closeassociation found between CgB levels in the myocardium andplasma and indices of severity of HF. However, additionalstudies are needed to precisely characterize the effect of NEon cardiomyocyte CgB exocytosis and the relative impor-tance of NE versus the effect by AngII and TGF-� on CgBproduction and secretion.
To our knowledge, no previous study has examined CgBproduction or circulating CgB levels during HF development.Increased CgB production has been found in neuroendocrinetumors,28 and circulating CgB levels have been proposed as apotential biomarker in patients with neuroendocrine tu-mors.14,29 The demonstration of increased circulating CgBlevels during HF development suggests that CgB may poten-tially represent a novel cardiac biomarker. This notion issupported by regulation of circulating CgB levels in propor-tion to NYHA functional class. However, the relative in-crease in circulating CgB levels in HF individuals was largerin the animal model than in the clinical study, indicating thatCgB production may be more potently induced in the earlyphase of HF development compared with the stable, chronicphase. A trend for higher CgB levels in hospitalized than inambulatory patients (Supplemental Table S1 and Figure S2)is also compatible with the theory that acute decompensationmay lead to higher CgB levels than observed in the chronicstate. Furthermore, contemporary HF therapy may havecontributed to lower CgB levels in stable ambulatory patients.
CgB has been reported to be robust and stable in vitro, withonly 3.7% degradation found in plasma samples stored atroom temperature for 24 hours.29 In addition, circulating CgBlevels were unaffected by PPI use, a medication currentlyrecommended as a prophylactic measure in many patientswith heart disease,30 and with well-known stimulatory effectson CgA production.13 Moreover, few other conditions areknown to be associated with increased circulating CgB levels.In fact, except for the rare neuroendocrine tumors,14,29,31,32
confounding by other diseases does not seem to represent amajor problem for use of CgB as a marker of cardiac status.
Even in prostate cancer patients with metastatic disease andtumors with widespread neuroendocrine differentiation, only14% of patients had increased circulating CgB levels,whereas 59% of patients had increased CgA levels.33 Takentogether, this information suggests that the collection andhandling of blood samples is relatively simple for CgB.
Reports on circulating CgB levels in association withcardiovascular disease are scarce, but 1 study investigated theassociation between presurgery CgB levels and postsurgeryatrial fibrillation in patients undergoing coronary by-passgrafting.34 The authors found no difference in CgB levelsbetween patients developing arrhythmias and patients instable sinus rhythm after surgery, opposing the hypothesisthat CgB levels could reflect autonomous imbalance. Incontrast, a polymorphism in the CgB gene was reported to bethe strongest predictor of enhanced vasoconstriction in astudy assessing association between single nucleotide poly-morphisms in the adrenergic pathway and venous vasocon-striction.35 The net effect of increased circulating CgB levelsin HF patients with regard to autonomic nervous system toneis not clear and will require additional investigations. In-creased CgB levels may also have direct effects on thecardiomyocytes and the myocardium. CgB, in contrast toCgA, translocates to the nucleus and has been found toregulate gene transcription, including increasing myocyteenhancer factor 2 (MEF2) production,36 a well-known pro-hypertrophic factor in the myocardium.37 CgB is also consid-ered an important modulator of the inositol 1,4,5-triphosphatereceptor (IP3R),38 and recently, CgB was shown to regulateAngII-induced myocardial hypertrophy in vitro by modifyingCa2� release from the sarcoplasmic reticulum through theIP3R.22 The augmentation of IP3R-mediated Ca2� release byCgB may also be of importance for the generation ofventricular arrhythmias in HF because the IP3R recently wasshown to regulate ryanodine receptor stability during myo-cardial remodeling.39 Because both CgB and the IP3R40 areupregulated in the failing myocardium, this CgB-IP3R-complex may be responsible for altered Ca2� homeostasisresulting in increased susceptibility to arrhythmias. Addition-ally, as CgB production in cardiomyocytes is closely regu-lated by NE, CgB levels in the myocardium, and potentiallyalso in the circulation, may integrate information on cardio-myocyte NE stimulation and IP3R activity, both risk factorsfor development of ventricular arrhythmias. Still, similar tothe situation of other recently proposed markers, more workis needed to establish CgB as a clinically useful HF biomar-ker (Table 3). Of note, CgA also binds to the IP3R but seemsto be inferior to CgB for regulation of IP3R activity.38 Incontrast, fragments of CgA have been found to affect severalimportant processes in HF such as myocardial contractility,endothelial function, and arterial tone,41 whereas such effectshave not been recognized for CgB fragments. A comparisonof CgA and CgB is provided in Table 4; however, the relativemerit of circulating CgA and CgB as cardiac biomarkers mustbe further characterized.
The main limitation of this study is lack of data relatingCgB to outcome in patients with HF. The HF patient cohortis of modest size and consists of patients with both ischemicand nonischemic HF, and acute and chronic HF. Our data for
Røsjø et al Chromogranin B in Heart Failure 509
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
CgB as a cardiac biomarker clearly needs to be validated inlarger HF cohorts, both regarding diagnostic and prognosticutility. Consequently, the current study should be considereda phase one/proof of concept investigation of CgB as acardiac biomarker.42
In conclusion, we have found increased CgB production inLV cardiomyocytes from post-MI HF animals proportional toHF severity. Because cardiomyocyte CgB gene expressionwas increased by NE, AngII, and TGF-�, myocardial CgBlevels may reflect alterations in important hormonal andparacrine mediators in HF. Furthermore, circulating CgBlevels were increased in both HF animals and in patients withHF of mainly moderate severity, again proportionate to HFseverity. Moreover, as CgB production was not altered inother organs investigated, the increased circulating levels
may at least partly reflect enhanced CgB production in theLV. Finally, because circulating CgB levels were not affectedby PPI use and increased in HF patients, CgB may representa potential new HF biomarker, but this must be validated inlarger clinical studies.
AcknowledgmentsWe thank Camilla Skjæret for skilful technical assistance with thequantitative real-time PCR analysis, Bjørg Austbø, Geir Florholmen,and Anett Hellebø Ottesen for assistance with the cell cultureexperiments; Vigdis Bakkelund and Anne Grethe Hokstad forcollecting blood samples; Inger Olsson for help with the RIA-anal-ysis; and the Section for Comparative Medicine at Oslo UniversityHospital, Ullevål for animal care.
Sources of FundingThis study was supported by the South-Eastern Norway RegionalHealth Authority; the Norwegian Heart and Lung Foundation;Akershus University Hospital; the University of Oslo; the RaagholtFoundation; the Anders Jahre Fund for Promotion of Science; andOslo University Hospital, Ullevål. Dr Røsjø is recipient of a researchfellowship from the South-Eastern Norway Regional Health Author-ity to study chromogranins in cardiovascular disease. The sponsorshad no role in any of the following: design and conduct of the study,collection, management, analysis and interpretation of the data, orpreparation, review, and approval of the article.
DisclosuresDrs Røsjø, Stridsberg, Omland, and Christensen are partners in apatent application filed by the University of Oslo regarding the useof CgB as a cardiac biomarker. Dr Stridsberg has a contract withEuro-Diagnostica AB (Malmo, Sweden) for developing a commer-cially available method for measuring CgB.
References1. Velagaleti RS, Pencina MJ, Murabito JM, Wang TJ, Parikh NI,
D’Agostino RB, Levy D, Kannel WB, Vasan RS. Long-term trends in theincidence of heart failure after myocardial infarction. Circulation. 2008;118:2057–2062.
2. Vasan RS. Biomarkers of cardiovascular disease: molecular basis andpractical considerations. Circulation. 2006;113:2335–2362.
3. Antman EM. Decision making with cardiac troponin tests. N Engl J Med.2002;346:2079–2082.
4. Hama N, Itoh H, Shirakami G, Nakagawa O, Suga S, Ogawa Y, MasudaI, Nakanishi K, Yoshimasa T, Hashimoto Y. Rapid ventricular inductionof brain natriuretic peptide gene expression in experimental acute myo-cardial infarction. Circulation. 1995;92:1558–1564.
5. Braunwald E. Biomarkers in heart failure. N Engl J Med. 2008;358:2148–2159.
6. Taupenot L, Harper KL, O’Connor DT. The chromogranin-secretograninfamily. N Engl J Med. 2003;348:1134–1149.
7. O’Connor DT, Deftos LJ. Secretion of chromogranin A by peptide-producing endocrine neoplasms. N Engl J Med. 1986;314:1145–1151.
8. Ceconi C, Ferrari R, Bachetti T, Opasich C, Volterrani M, Colombo B,Parrinello G, Corti A. Chromogranin A in heart failure; a novel neuro-humoral factor and a predictor for mortality. Eur Heart J. 2002;23:967–974.
9. Omland T, Dickstein K, Syversen U. Association between plasma chro-mogranin A concentration and long-term mortality after myocardialinfarction. Am J Med. 2003;114:25–30.
10. Estensen ME, Hognestad A, Syversen U, Squire I, Ng L, Kjekshus J,Dickstein K, Omland T. Prognostic value of plasma chromogranin Alevels in patients with complicated myocardial infarction. Am Heart J.2006;152:927.e1–e6.
11. Jansson AM, Røsjø H, Omland T, Karlsson T, Hartford M, Flyvbjerg A,Caidahl K. Prognostic value of circulating chromogranin A levels in acutecoronary syndromes. Eur Heart J. 2009;30:25–32.
12. Pieroni M, Corti A, Tota B, Curnis F, Angelone T, Colombo B, CerraMC, Bellocci F, Crea F, Maseri A. Myocardial production of chromo-
Table 3. Established and Novel HF Biomarkers ReleasedFrom Cardiomyocytes
Inflammation
TNF-�
Fas (APO-1)
Interleukins 1, 6, and 18
Cardiomyocyte injury
Cardiac-specific troponins I and T
Myosin light-chain kinase I
Heart-type fatty-acid protein
Creatine kinase-MB fraction
Cardiomyocyte stress
BNP
N-terminal pro-BNP
Midregional fragment of proadrenomedullin
ST2
New biomarkers
CgA
CgB
Osteoprotegerin
Growth-differentiation factor-15
Modified from Braunwald.5
Table 4. Comparison of Functional Properties of Interest in HFfor CgA and CgB
CgA CgB
Produced by cardiomyocytes Yes Yes
Increased in the LV in HF Yes Yes
Production in cardiomyocytes increased byNE, AngII, and TGF-�
No Yes
Circulating levels influenced by use of PPI Yes No
Binding to the inositol 1,4,5-triphosphatereceptor38
Weak Strong
Associated with development ofcardiomyocyte hypertrophy22
Unknown Yes
Effect on myocardial contractility41 Attenuated Unknown
Effect on vascular contractility41 Attenuated Unknown
Effect on endothelial integrity41 Enhance Unknown
510 Circ Heart Fail July 2010
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

granin A in human heart: a new regulatory peptide of cardiac function.Eur Heart J. 2007;28:1117–1127.
13. Waldum HL, Arnestad JS, Brenna E, Eide I, Syversen U, Sandvik AK.Marked increase in gastric acid secretory capacity after omeprazoletreatment. Gut. 1996;39:649–653.
14. Stridsberg M, Eriksson B, Fellstrom B, Kristiansson G, Tiensuu JE.Measurements of chromogranin B can serve as a complement to chro-mogranin A. Regul Pept. 2007;139:80–83.
15. Steiner HJ, Weiler R, Ludescher C, Schmid KW, Winkler H. Chromo-granins A and B are co-localized with atrial natriuretic peptides insecretory granules of rat heart. J Histochem Cytochem. 1990;38:845–850.
16. Iversen PO, Woldbæk PR, Tønnessen T, Christensen G. Decreased hema-topoiesis in bone marrow of mice with congestive heart failure. Am JPhysiol Regul Integr Comp Physiol. 2002;282:R166–R172.
17. Finsen AV, Christensen G, Sjaastad I. Echocardiographic parametersdiscriminating myocardial infarction with pulmonary congestion frommyocardial infarction without congestion in the mouse. J Appl Physiol.2005;98:680–689.
18. Stridsberg M, Eriksson B, Oberg K, Janson ET. A panel of 13 region-specific radioimmunoassays for measurements of human chromograninB. Regul Pept. 2005;125:193–199.
19. Stridsberg M, Eriksson B, Oberg K, Janson ET. A panel of 11 region-specific radioimmunoassays for measurements of human chromograninA. Regul Pept. 2004;117:219–227.
20. Florholmen G, Andersson KB, Yndestad A, Austbø B, Henriksen UL,Christensen G. Leukaemia inhibitory factor alters expression of genesinvolved in rat cardiomyocyte energy metabolism. Acta Physiol Scand.2004;180:133–142.
21. Mahata SK, Mahapatra NR, Mahata M, O’Connor DT. Neuroendocrinecell type-specific and inducible expression of chromogranin/secre-togranin genes: crucial promoter motifs. Ann N Y Acad Sci. 2002;971:27–38.
22. Heidrich FM, Zhang K, Estrada M, Huang Y, Giordano FJ, Ehrlich BE.Chromogranin B regulates calcium signaling, nuclear factor kappaBactivity, and brain natriuretic peptide production in cardiomyocytes. CircRes. 2008;102:1230–1238.
23. Huh YH, Jeon SH, Yoo SH. Chromogranin B-induced secretory granulebiogenesis: comparison with the similar role of chromogranin A. J BiolChem. 2003;278:40581–40589.
24. Pohl TM, Phillips E, Song KY, Gerdes HH, Huttner WB, Ruther U. Theorganisation of the mouse chromogranin B (secretogranin I) gene. FEBSLett. 1990;262:219–224.
25. Minneman KP, Lee D, Zhong H, Berts A, Abbott KL, Murphy TJ.Transcriptional responses to growth factor and G protein-coupledreceptors in PC12 cells: comparison of alpha(1)-adrenergic receptorsubtypes. J Neurochem. 2000;74:2392–2400.
26. Muller FU, Neumann J, Schmitz W. Transcriptional regulation by cAMPin the heart. Mol Cell Biochem. 2000;212:11–17.
27. Cohn JN, Levine TB, Olivari MT, Garberg V, Lura D, Francis GS, SimonAB, Rector T. Plasma norepinephrine as a guide to prognosis in patientswith chronic congestive heart failure. N Engl J Med. 1984;311:819–823.
28. Lloyd RV, Cano M, Rosa P, Hille A, Huttner WB. Distribution ofchromogranin A and secretogranin I (chromogranin B) in neuroendocrinecells and tumors. Am J Pathol. 1988;130:296–304.
29. Sekiya K, Ghatei MA, Salahuddin MJ, Bishop AE, Hamid QA, IbayashiH, Polak JM, Bloom SR. Production of GAWK (chromogranin-B420–493)-like immunoreactivity by endocrine tumors and its possiblediagnostic value. J Clin Invest. 1989;83:1834–1842.
30. Saini SD, Schoenfeld P, Fendrick AM, Scheiman J. Cost-effectiveness ofproton pump inhibitor cotherapy in patients taking long-term, low-doseaspirin for secondary cardiovascular prevention. Arch Intern Med. 2008;168:1684–1690.
31. Stridsberg M, Oberg K, Li Q, Engstrom U, Lundqvist G. Measurementsof chromogranin A, chromogranin B (secretogranin I), chromogranin C(secretogranin II) and pancreastatin in plasma and urine from patientswith carcinoid tumours and endocrine pancreatic tumours. J Endocrinol.1995;144:49–59.
32. Stridsberg M, Husebye ES. Chromogranin A and chromogranin B aresensitive circulating markers for phaeochromocytoma. Eur J Endocrinol.1997;136:67–73.
33. Angelsen A, Syversen U, Haugen OA, Stridsberg M, Mjølnerød OK,Waldum HL. Neuroendocrine differentiation in carcinomas of theprostate: do neuroendocrine serum markers reflect immunohistochemicalfindings? Prostate. 1997;30:1–6.
34. Jideus L, Ericson M, Stridsberg M, Nilsson L, Blomstrom P, Blomstrom-Lundqvist C. Diminished circadian variation in heart rate variabilitybefore surgery in patients developing postoperative atrial fibrillation.Scand Cardiovasc J. 2001;35:238–244.
35. Fung MM, Nguyen C, Mehtani P, Salem RM, Perez B, Thomas B, Das M,Schork NJ, Mahata SK, Ziegler MG, O’Connor DT. Genetic variationwithin adrenergic pathways determines in vivo effects of presynapticstimulation in humans. Circulation. 2008;117:517–525.
36. Yoo SH, You SH, Kang MK, Huh YH, Lee CS, Shim CS. Localizationof the secretory granule marker protein chromogranin B in the nucleus:potential role in transcription control. J Biol Chem. 2002;277:16011–16021.
37. Kolodziejczyk SM, Wang L, Balazsi K, DeRepentigny Y, Kothary R,Megeney LA. MEF2 is upregulated during cardiac hypertrophy and isrequired for normal post-natal growth of the myocardium. Curr Biol.1999;9:1203–1206.
38. Choe CU, Ehrlich BE. The inositol 1,4,5-trisphosphate receptor (IP3R)and its regulators: sometimes good and sometimes bad teamwork. SciSTKE. 2006;2006:re15.
39. Harzheim D, Movassagh M, Foo RSY, Ritter O, Tashfeen A, Conway SJ,Bootman MD, Roderick HL. Increased InsP3Rs in the junctionalsarcoplasmic reticulum augment Ca2� transients and arrhythmiasassociated with cardiac hypertrophy. Proc Natl Acad Sci U S A. 2009;106:11406–11411.
40. Go LO, Moschella MC, Watras J, Handa KK, Fyfe BS, Marks AR.Differential regulation of two types of intracellular calcium releasechannels during end-stage heart failure. J Clin Invest. 1995;95:888–894.
41. Helle KB. The chromogranin A-derived peptides vasostatin-I and cat-estatin as regulatory peptides for cardiovascular functions. CardiovascRes. 2010;85:9–16.
42. Hlatky MA, Greenland P, Arnett DK, Ballantyne CM, Criqui MH, ElkindMS, Go AS, Harrell FE Jr, Howard BV, Howard VJ, Hsue PY, KramerCM, McConnell JP, Normand SL, O’Donnell CJ, Smith SC Jr, WilsonPW. Criteria for Evaluation of Novel Markers of Cardiovascular Risk: aScientific Statement from the American Heart Association. Circulation.2009;119:2408–2416.
CLINICAL PERSPECTIVEThe cardiac biomarkers used routinely in clinical practice today are proteins specific to the diseased myocardium, either releasedduring cell necrosis (cardiac-specific troponins) or secreted secondary to cardiomyocyte strain (B-type natriuretic peptide).However, there is still a need for markers reflecting other pathophysiological processes in heart disease. We have identifiedchromogranin B (CgB) as a protein that is closely regulated in the left ventricle in heart failure (HF), while production wasunaltered in other tissues investigated. Circulating levels of CgB were also elevated in patients with HF compared with healthycontrol subjects, and levels increased in proportion to severity of HF as evaluated by NYHA functional class. Plasma CgB levelscorrelated only modestly with B-type natriuretic peptide and chromogranin A (CgA) levels, another granin protein and novel HFbiomarker, indicating that CgB is regulated by other mechanism than B-type natriuretic peptide and CgA in HF. As CgB isclosely associated with Ca2�signaling, CgB could potentially be a marker providing information on processes currently notreflected by established HF biomarkers. However, the role of CgB in HF development and as a cardiac biomarker still requiresadditional experimental and clinical studies before clinical utility may be established.
Røsjø et al Chromogranin B in Heart Failure 511
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
Vanessa Finsen, Cathrine Rein Carlson, Erik Øie, Torbjørn Omland and Geir ChristensenHelge Røsjø, Cathrine Husberg, Mai Britt Dahl, Mats Stridsberg, Ivar Sjaastad, Alexandra
Failing MyocardiumChromogranin B in Heart Failure: A Putative Cardiac Biomarker Expressed in the
Print ISSN: 1941-3289. Online ISSN: 1941-3297 Copyright © 2010 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation: Heart Failure
doi: 10.1161/CIRCHEARTFAILURE.109.8677472010;3:503-511; originally published online June 2, 2010;Circ Heart Fail.
http://circheartfailure.ahajournals.org/content/3/4/503World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circheartfailure.ahajournals.org/content/suppl/2010/06/02/CIRCHEARTFAILURE.109.867747.DC1Data Supplement (unedited) at:
http://circheartfailure.ahajournals.org//subscriptions/
is online at: Circulation: Heart Failure Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further information isthe Editorial Office. Once the online version of the published article for which permission is being requested
can be obtained via RightsLink, a service of the Copyright Clearance Center, notCirculation: Heart Failurein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 10, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
S1
SUPPLEMENTAL MATERIAL
S2
SUPPLEMENTAL MATERIAL
to
Chromogranin B in Heart Failure: a Putative Cardiac Biomarker Expressed in the
Failing Myocardium
Helge Røsjø MD1,2,3
; Cathrine Husberg MSc, PhD2,4
; Mai Britt Dahl MSc1,2,5
; Mats
Stridsberg MD, PhD6; Ivar Sjaastad MD, PhD
2,4,7; Alexandra Vanessa Finsen MD,
PhD2,8,9
; Cathrine Rein Carlson MSc, PhD2,4
; Erik Øie MD, PhD2,8,9
; Torbjørn Omland
MD, PhD, MPH1,2,3
; Geir Christensen MD, PhD, MHA2,4
1) Medical Division, Akershus University Hospital, Lørenskog, Norway
2) Center for Heart Failure Research, University of Oslo, Oslo, Norway
3) Institute of Clinical Medicine, University of Oslo, Oslo, Norway
4) Institute for Experimental Medical Research, Oslo University Hospital, Ullevål,
Oslo, Norway
5) EpiGen, Institute of Clinical Epidemiology and Molecular Biology, Akershus
University Hospital, Lørenskog, Norway
6) Department of Medical Sciences, Uppsala University, Uppsala, Sweden
7) Department of Cardiology, Oslo University Hospital, Ullevål, Oslo, Norway
8) Research Institute for Internal Medicine, Oslo University Hospital, Rikshospitalet,
Oslo, Norway
9) Department of Cardiology, Oslo University Hospital, Rikshospitalet, Oslo,
Norway
S3
Supplemental Methods
Mouse Model of HF
Six week old C56BL/6 mice (Taconic, Skensved, Denmark) were anesthetized with 0.2 mg
propofol in the tail vein before being trachetomized, connected to an animal ventilator, and
ventilated with a mixture of 98% oxygen and 2% isoflurane. Via a left-sided thoracotomy,
pericardectomy was performed followed by ligation of the left main coronary artery in the HF
group. Sham-operated (sham) animals underwent the same procedure except ligation of the
coronary artery. One week after the primary operation, a full echocardiographic examination
was performed while animals were anesthetized breathing a gas mixture of oxygen and
isoflurane supplied via a facemask. Criteria used for including animals in the HF group were:
1) MI >40 % of the circumference of the LV, 2) left atrial diameter >2.0 mm, 3) >35 %
increase in lung weight compared to the sham group (e.g. lung weight >0.2 g).
After sacrificing the animals one week post-surgery, hearts were removed, blotted dry and
dissected into the right and LV. The LV was further divided into the infarcted and non-
infarcted part in HF animals. Lung tissue and tissue samples from liver, spleen, kidney,
stomach, part of the colon and the anterior tibial muscle were also collected. Tissue intended
for qRT-PCR or immunoblotting were immediately frozen in liquid nitrogen and stored at
70°C until use, while hearts collected for immunohistological analysis were fixed overnight in
4% formalin, washed in 30% ethanol and stored in 70% ethanol at 4°C before use.
To evaluate the effect on gene expression and protein levels by anesthesia and surgery per se
sham animals were compared to age-matched non-operated animals for all experiments.
S4
The study was performed according to the recommendations given by the European Council
for Laboratory Animal Science and approved by the Norwegian Council for Animal Research.
HF Patients
All patients were included at a single center, Akershus University Hospital, a secondary
referral and teaching hospital in metropolitan Oslo, Norway, with a catchment area of
approximately 320.000 people. The seventy patients recruited from the ambulatory HF clinic
were at the time of study inclusion managed solely by scheduled 30 minutes visits to specially
trained nurses in the outpatient clinic. Of these seventy patients, twelve had been hospitalized
for worsening HF during the last three months. We also included ten patients with a previous
diagnosis of HF that were hospitalized at the time of patient recruitment: for all of these ten
patients the index hospitalization was HF related as classified by the treating physician
(International Classifications of Diseases, 10th
revision, World Health Organization: code
I50.1 or I50.9).
Troponin T (TnT) values were measured in all hospitalized, but not in ambulatory patients.
No patient had evidence of acute myocardial infarction as defined by the recent universal
definition of myocardial infarction: Rise and/or fall of TnT values exceeding the 99th
percentile of the upper reference limit.1
A transthoracic echocardiogram had been obtained within the last 18 months in all but 3
patients (4%) who had been clinically stable during this period, i.e. no change in severity of
HF symptoms or NYHA functional class during the last 12 months and no hospitalization for
worsening HF during the last 24 months. One of these patients had been evaluated by
myocardial single photon emission computed tomography (SPECT) during the last 12 months
S5
and had a LVEF of 20% and no evidence of reversible myocardial ischemia. Patients with HF
and preserved LV function (>50%) were not included in the clinical cohort. Seventy-three
patients (91%) had undergone coronary angiography for diagnostic purposes.
Blood Samples
Blood samples from humans were drawn from an antecubital vein, while blood samples from
animals were collected from the vena cava inferior after a laparotomy of anesthetized animals
breathing a combination of oxygen and isoflurane. Blood samples were immediately put on
ice, centrifuged within 30 minutes, and the plasma stored at –70°C. Plasma B-type natriuretic
peptide (BNP) levels were measured by a two-step sandwich immunoassay (Architect® BNP
assay, Abbott Diagnostics, Abbott Park, IL).
qRT-PCR
Tissue (20-35 mg) from the non-infarcted region of the LV from 9 HF mice and 8 sham mice
was used for RNA extraction. Homogenization was performed with the Mixer Mill MM 300
system (RETSCH, Haan, Germany) after adding 175 μl lyses buffer and a 5 mm stainless
steel bead (Qiagen, Hilden, Germany) to the samples. Total RNA was extracted by the use of
the SV Total RNA Isolation System (Promega Corporation, Madison, WI). RNA
concentration was measured with the NanoDrop system (NanoDrop Technologies,
Wilmington, DE) and RNA quality evaluated with the Agilent BioAnalyzer 2100 (Agilent
Technologies Inc., Santa Clara, CA). cDNA was produced from 5 μg RNA with the High-
Capacity cDNA Archive kit (Applied Biosystems, Foster City, CA); the GeneAmp PCR
system 9700 thermal cycler (Applied Biosystems) was used for the reverse transcription. The
results were detected on a 7900 HT Real-Time PCR System (Applied Biosystems), and the
relative gene expression was determined by using the standard curve method.2 The standard
S6
curve for CgB was plotted from neonatal mouse brain tissue, while myocardial tissue was
used for plotting BNP and RPL4 standard curves. All samples were run in triplicate and RPL4
served as an internal control. Levels are presented as change from the mean in the sham group
(fold change).
1-D Gel Electrophoresis and Immunoblotting
Frozen myocardial tissue samples were homogenized in a cold lysis buffer containing 210
mM sucrose, 40 mM NaCl, 30 mM Hepes, 5 mM EDTA, 1% Tween-20, and different
protease inhibitors (Complete EDTA-free protease inhibitor cocktail, Roche Diagnostics,
Basel, Switzerland). Mechanical homogenization was performed with the Mixer Mill MM
300 system with insoluble material removed after centrifugation at 14000 x g. The lysates
were added 1% SDS as a final concentration. Total protein content was measured with the
micro BCA protein assay kit (Pierce Biotechnology, Rockford, IL) according to the
manufactures protocol. Prior to gel loading, lysates were denaturated for 5 minutes at 100°C
after mixing 20-30 ug protein with SDS gel-loading buffer (50% sucrose, 7.5% SDS,
0.0625M Tris-HCl, pH 6.8, 2mM EDTA, pH 7.5, 3.1% DTT, and 0.01% bromophenolblue).
After protein loading, polyacrylamide gels (10-12 %) were run approximately for 75 minutes
at 200 V, however, with some variation as electrophoresis length was chosen according to the
protein of interest. Precision Plus Protein Dual Color Standard (161-0374) was used as the
molecular marker (Bio-Rad Laboratories Inc., Hercules, CA) and included in all gels. Proteins
separated on gels were transferred to Hybond-P PVDF membranes (RPN303F, Amersham
Biosciences Europe, Freiburg, Germany) using a Mini Trans-Blot Cell system (Bio-Rad
Laboratories Inc.), incubated at room temperature (RT) with 5% skimmed dry milk diluted in
Tris-buffered saline containing 0.1% Tween (TBS-t) for 2 hours to avoid unspecific antibody
binding. Primary antibodies were diluted in 5% skimmed dry milk in TBS-t before incubation
S7
overnight at 4°C. The next day secondary antibodies diluted in 5% skimmed dry milk in TBS-
t were incubated to the membranes for 1 hour at RT. Membranes were washed three times for
5-15 minutes in TBS-t in between and after all incubation steps. The roller mixer (444-1607,
VWR International) was used for incubations.
For visualizing immunostained proteins the ECL Plus Western Detection System (Amersham
Biosciences Europe, Freiburg, Germany) and an ImageReader LAS 3000-mini digital detector
(Fujifilm, Tokyo, Japan) were used with densitometry of immunostained bands measured with
MultiGauge (Fujifilm). Equal protein loading on gels was controlled by using anti-
glyceraldehyde-3-dehydrogenase (GAPDH) as an internal control (2118, Cell Signaling
Technology, Beverly, MA). We used a secondary anti-goat antibody for GADPH analysis
(4030-05, Southern Biotech, Birmingham, AL).
In general, protein lysates from HF and sham animals were loaded in every second well in the
acrylamide gels to avoid differences due to technical difficulties, six individuals per group
were maximum per gel. For myocardial tissue with n>6 in HF and sham groups; blots were
compared by normalizing bands against three individuals whom had samples run on all gels.
CgB levels are presented as change from the mean in the sham group. As CgB has a highly
acidic charge, CgB migrates slower in the SDS-PAGE system than predicted from its
calculated molecular weight. By immunoblotting, strong protein bands were found for the
positive controls with molecular weights corresponding to what has earlier been reported as
the full length CgB molecule in the SDS-PAGE system (100-120 kDa).3 Total protein extracts
from neonatal mouse brain or a rat pheochromocytoma cell line (PC12 cell line, sc-2250,
Santa Cruz Biotechnology, Santa Cruz, CA) were included in the gels as positive controls.
S8
Radioimmunoassay on Tissue Homogenate
Frozen LV tissue samples were homogenized as described in the previous section. CgA
protein levels were measured with an in-house made region-specific RIA detecting CgA361-
3724 from 50 µg of total protein homogenate. All samples were measured in duplicate and no
sample had CgA levels below the detection limit (<2 fmol/tube). LV tissue samples were
homogenized as described in the previous section.
Immunohistochemistry
The CgB (sc-1489, Santa Cruz) and CgA (Sc-13090, Santa Cruz) antibodies were followed by
anti-goat IgG (Vector Laboratories, Burlingame, CA). The CgA antibody was a purified
polyclonal rabbit anti-human CgA raised against the C-terminal part of CgA. The
immunoreactivities were further amplified using avidin-biotin-peroxidase complexes
(Vectastain Elite kit, Vector Laboratories). Diaminobenzidine was used as the chromogen in a
commercial metal enhanced system (Pierce Biotechnology). The sections were counter-
stained with hematoxylin. Omission of the primary antibody or use of non-immune rabbit
serum served as negative controls.
Cell Culture Experiments
Neonatal rat cardiomyocytes were isolated from neonatal (1-3 days) Wistar rats (Taconic).
Mechanical disruption of cells and evaluation of RNA concentrations and quality were
performed as described under section qRT-PCR, except that total RNA was isolated from the
neonatal rat cardiomyocytes by the use of the RNeasy mini kit (Qiagen, Valencia, CA).
Reverse transcription reactions were performed with iScript Select cDNA Synthesis Kit (Bio-
Rad Laboratories Inc.).
S9
Gene expression in stimulated cells is presented as change vs. gene expression in PBS
stimulated cells (fold change). Samples were run in duplicate or triplicate and RPL4 gene
expression was used as an internal control.
Mapping of Binding Site for CgB Antibody Used in Immunoblotting and
Immunohistochemistry
Peptide Synthesis
Mouse CgB (NP_031720) was synthesized as 20-mer peptides with five amino acids offsets
on cellulose membranes using a Multipep automated peptide synthesizer (INTAVIS
Bioanalytical Instruments AG, Cologne, Germany) as described.
5
Immunoblot Analysis
The membranes were blocked in 5% non-fat dry milk for 60 minutes at room temperature,
incubated overnight at 4°C with primary antibody in TBS-t, washed five times 5 minutes
in
TBS-t and incubated with a horseradish-peroxidase-conjugated secondary antibody in 5%
non-fat dry milk for 60 minutes at room temperature. Blots were developed by using ECL
Plus (GE HealthCare, RPN2132). The chemiluminescence signals were detected by Las-4000
(Fujifilm).
Antibodies
Immunoblotting was carried out using goat anti-CgB (1:100 dilution, sc-1489, Santa Cruz).
Donkey anti-goat IgG HRP affinity purified polyclonal antibody (1:2500 dilution, HAF109,
R&D Systems, Minneapolis, MN) was used as secondary antibody.
S10
Evaluation of CgB Antibody Used for Immunoblotting and Immunohistochemistry by
Blocking Peptide
1-D gel electrophoresis and immunoblotting were performed as earlier described except that a
blocking peptide (sc-1489 P, Santa Cruz) specific for our CgB antibody was preadded in
excess to the primary antibody solution aimed to one half of the Hybond-P PVDF membrane
prior to transferring proteins from the gel.
Supplemental Results
Characteristics of Patients Included From the Ambulatory HF Clinic and the
Hospitalized HF Patients
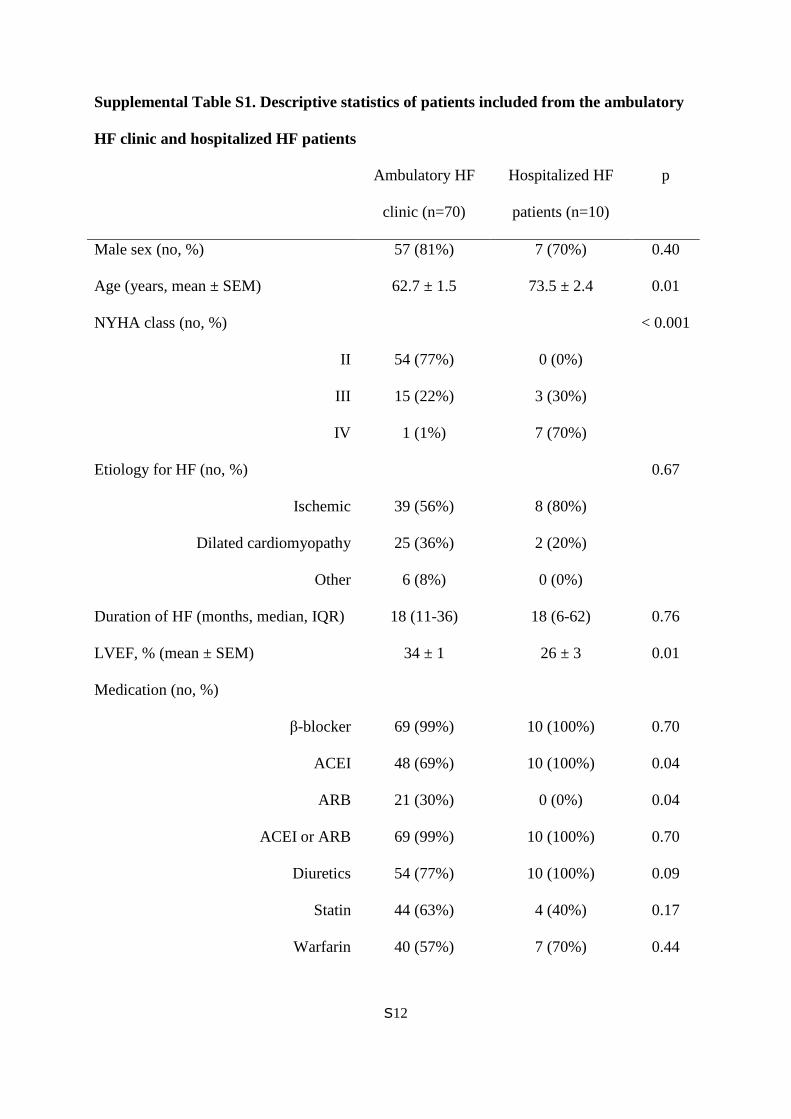
The hospitalized HF patients included in the study were older and had more severe HF as
evaluated by LVEF, BNP levels, and NYHA functional class compared to the other HF
patients (Table S1). A higher proportion of these patients were also treated with cardiac
resynchronization therapy, digitalis, and ACE-inhibitors (ACEI). However, there were no
difference in combined ACEI/AngII receptor blocker medication between patients admitted
from the ambulatory HF clinic and the hospitalized HF patients (Table S1). Diuretic and
nitrate use, and circulating CgA levels were of borderline difference. There was also a trend
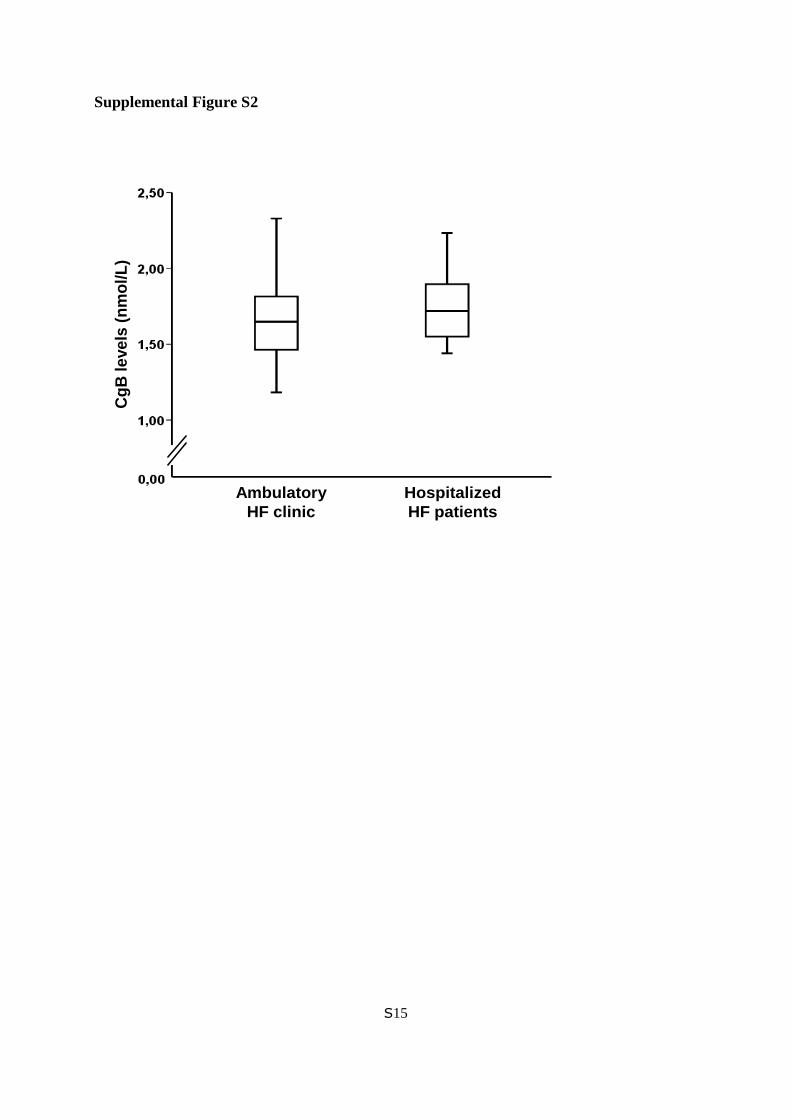
towards higher levels of circulating CgB in the hospitalized HF patients compared to the other
HF patients, but the difference did not reach statistical significance (median 1.72 [interquartile
range: 1.54-1.93] vs. 1.65 [1.46-1.82] nmol/L, p=0.27, Table S1 and Figure S2).
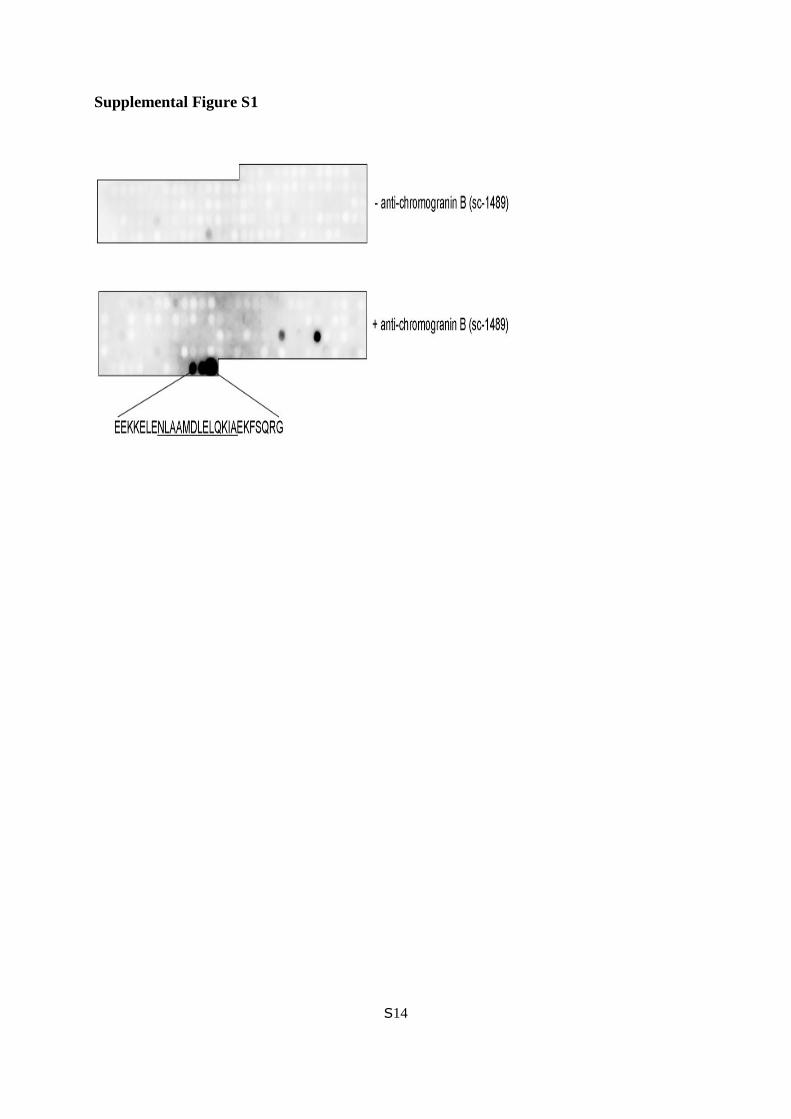
Epitope Mapping of Anti-CgB Antibody (sc-1489)
Strong and specific binding was observed to the amino acid sequence
EEKKELENLAAMDLELQKIAEKFSQRG (Figure S1, lower panel) where underlined amino
acids indicate the core epitope. The identified residues are located to the extreme C-terminus

S11
in CgB and are consistent with the source information from the manufacturer (Santa Cruz).
Immunoblotting without incubation with primary antibody was used as a negative control
(Figure S1, upper panel).
Evaluation of CgB Antibody by Blocking Peptide
No bands were detected on the part of the membrane pretreated with the blocking peptide
(Figure S3), indicating that our CgB antibody is sensitive and specific for CgB. Strong bands
corresponding to what has earlier been reported as the full length CgB molecule in the SDS-
PAGE system (100-120 kDa)3 were found on the non-pretreated half of the membrane.
S12
Supplemental Table S1. Descriptive statistics of patients included from the ambulatory
HF clinic and hospitalized HF patients
Ambulatory HF
clinic (n=70)
Hospitalized HF
patients (n=10)
p
Male sex (no, %) 57 (81%) 7 (70%) 0.40
Age (years, mean ± SEM) 62.7 ± 1.5 73.5 ± 2.4 0.01
NYHA class (no, %)
II
III
IV
54 (77%)
15 (22%)
1 (1%)
0 (0%)
3 (30%)
7 (70%)
< 0.001
Etiology for HF (no, %)
Ischemic
Dilated cardiomyopathy
Other
39 (56%)
25 (36%)
6 (8%)
8 (80%)
2 (20%)
0 (0%)
0.67
Duration of HF (months, median, IQR) 18 (11-36) 18 (6-62) 0.76
LVEF, % (mean ± SEM) 34 ± 1 26 ± 3 0.01
Medication (no, %)
β-blocker
ACEI
ARB
ACEI or ARB
Diuretics
Statin
Warfarin
69 (99%)
48 (69%)
21 (30%)
69 (99%)
54 (77%)
44 (63%)
40 (57%)
10 (100%)
10 (100%)
0 (0%)
10 (100%)
10 (100%)
4 (40%)
7 (70%)
0.70
0.04
0.04
0.70
0.09
0.17
0.44
S13
ASA
Clopidogrel
Aldosterone antagonist
Digitalis
Amiodarone
Nitrate
PPI
38 (54%)
8 (11%)
14 (20%)
22 (31%)
8 (11%)
7 (10%)
9 (13%)
5 (50%)
1 (10%)
2 (20%)
8 (80%)
2 (20%)
3 (30%)
2 (20%)
0.80
0.89
1.00
0.003
0.44
0.07
0.54
CRT 10 (14%) 4 (40%) 0.05
ICD 12 (17%) 2 (20%) 0.82
CgB levels, nmol/L (median, IQR) 1.65 (1.46-1.82) 1.72 (1.54-1.93) 0.27
CgA levels, nmol/L (median, IQR) 5.1 (3.6-8.3) 7.9 (6.2-12.2) 0.08
BNP levels, pg/mL (median, IQR) 210 (107-368) 1470 (874-2515) <0.001
NYHA indicates New York Heart Association functional class; IQR, interquartile range;
LVEF, left ventricular ejection fraction; ACEI, ACE-inhibitor; ARB, AngII receptor blocker;
ASA, acetyl salicylic acid; PPI: proton pump inhibitor; CRT, cardiac resynchronization
therapy; ICD, implantable cardioverter-defibrillator; CgB, chromogranin B; CgA,
chromogranin A; and BNP, B-type natriuretic peptide.
.
S14
Supplemental Figure S1
S15
Supplemental Figure S2
Ambulatory
HF clinic
Hospitalized
HF patients
Cg
B le
ve
ls (
nm
ol/
L)

S16
Supplemental Figure S3
Sh
am
Sh
am
HF
HF
Sh
am
Sh
am
HF
HF
Blocking peptide +/- + + + + - - - -
CgB (100 kDa)
S17
Supplemental Figure legends
Supplemental Figure S1. Epitope mapping of anti-CgB, sc-1489. CgB residues important for
antibody binding were identified by overlaying an array of immobilized CgB 20-mer peptides
with anti-CgB, sc-1487 (lower panel). Strong and specific binding was observed to the amino
acid sequence EEKKELENLAAMDLELQKIAEKFSQRG which is located to the C-terminal
end of CgB and is consistent with the source information of the manufacturer. The given
amino acids are relevant for binding and underlined amino acids indicate the core epitope.
Immunoblotting without incubation with primary antibody was used as a negative control
(upper panel).
Supplemental Figure S2. Circulating CgB levels in patients admitted from the ambulatory
HF clinic and hospitalized HF patients. The horizontal line within the box represents the
median level, the boundaries of the box the 25th and 75th percentile levels, and the whiskers
range (maximum value restricted to 1.5 x interquartile range from the median).
Supplemental Figure S3. CgB antibody evaluated by use of a blocking peptide. No bands
were detected on the part of the membrane pretreated with the blocking peptide (left side)
while strong bands corresponding to what has earlier been reported as the full length CgB
molecule in the SDS-PAGE system (100 kDa) were found on the non-pretreated part (right
side).
S18
Supplemental References
(1) Thygesen K, Alpert JS, White HD, Jaffe AS, Apple FS, Galvani M, Katus HA, Newby
LK, Ravkilde J, Chaitman B, Clemmensen PM, Dellborg M, Hod H, Porela P,
Underwood R, Bax JJ, Beller GA, Bonow R, van der Wall EE, Bassand JP, Wijns W,
Ferguson TB, Steg PG, Uretsky BF, Williams DO, Armstrong PW, Antman EM, Fox
KA, Hamm CW, Ohman EM, Simoons ML, Poole-Wilson PA, Gurfinkel EP, Lopez-
Sendon JL, Pais P, Mendis S, Zhu JR, Wallentin LC, Fernandez-Aviles F, Fox KM,
Parkhomenko AN, Priori SG, Tendera M, Voipio-Pulkki LM, Vahanian A, Camm AJ,
De CR, Dean V, Dickstein K, Filippatos G, Funck-Brentano C, Hellemans I, Kristensen
SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL, Morais
J, Brener S, Harrington R, Morrow D, Lim M, Martinez-Rios MA, Steinhubl S, Levine
GN, Gibler WB, Goff D, Tubaro M, Dudek D, Al-Attar N. Universal definition of
myocardial infarction. Circulation. 2007;116:2634-2653.
(2) Yuan JS, Reed A, Chen F, Stewart CN, Jr. Statistical analysis of real-time PCR data.
BMC Bioinformatics. 2006;7:85.
(3) Taupenot L, Harper KL, O'Connor DT. The chromogranin-secretogranin family. N Engl
J Med. 2003;348:1134-1149.
(4) Stridsberg M, Eriksson B, Oberg K, Janson ET. A panel of 11 region-specific
radioimmunoassays for measurements of human chromogranin A. Regul Pept.
2004;117:219-227.

S19
(5) Frank R. The SPOT-synthesis technique. Synthetic peptide arrays on membrane
supports--principles and applications. J Immunol Methods. 2002;267:13-26.





























