Embed Size (px)
Citation preview

RESEARCH FEATURE
Chronic Illness and Fatigue in Older Individuals: ASystematic ReviewMaral Torossian1, MS, RN & Cynthia S. Jacelon1, PhD, RN-BC, CRRN, FGSA, FAAN
AbstractBackground: Fatigue is a symptom experienced by 40%–74% of older individuals in the United States. Despite its significance, cli-nicians face challenges helping individuals to manage or reduce fatigue levels. Some management issues are attributable to theambiguity around the risk factors, consequences, and the effect of fatigue management strategies.Methods: A literature review was conducted using four databases to identify themes in relation to risk factors, consequences, andmanagement strategies from research studies about fatigue in older individuals with chronic diseases.Results: Findings on fatigue risk factors, such as age, body mass index, and marital status, were contradictory. There was a positiveassociation between fatigue and comorbidities, depression, and anxiety and a negative relationship between fatigue and physicalactivity, sleep, educational status, and socioeconomic status. Fatigue was perceived as a state of “feebleness” and negatively im-pacted individuals’ quality of life. Consequences of fatigue included tiredness, sleepiness, depression, anxiety, worse sense of pur-pose in life, poor self-care, and an increased β-amyloid load. Predictors of worse fatigue consequences included functional health,symptom burden, subjective health, and self-acceptance. Fatigue management strategies included physical activity, rest, sleep,maintaining normal hemoglobin levels, and acetyl-L-carnitine supplementation.Conclusion: This systematic review is of value to older individuals with chronic illnesses, researchers, and clinicians who strive toimprove the quality of life of individuals experiencing fatigue. To prevent undesirable consequences of fatigue, older individualsshould be screened for the discussed modifiable risk factors of fatigue. The inconsistencies in the studies reviewed can guide re-searchers to potential research areas that require further inquiry and exploration to ground future practice on best scientific evidence
Keywords: Chronic disease; chronic illness; fatigue; fatigue consequences; fatigue management; fatigue risk factors;older individuals.
Fatigue is a cardinal symptom experienced by 40%–74%of older individuals living with a chronic disease (Mentinget al., 2018). Fatigue is defined as an overwhelming senseof decreased capacity for activity, physical or mental,due to an imbalance in the availability, utilization, or res-toration of resources (Aaronson et al., 1999), and is attrib-uted to disease-specific, psychological, or cognitive factors(Goedendorp et al., 2014). Fatigue is described as anunpleasant, troublesome, and burdensome symptom, con-tributing to irritability, poormotivation, attention,memory,
Correspondence: Maral Torossian, 294C Green Road, Manchester, CT 06042.E-mail: [email protected]
1 University of Massachusetts Amherst, Amherst, MA, USA
Copyright © 2020 the Author(s). Published by Association of Rehabilitation Nurses.
This is an open access article distributed under the Creative Commons AttributionLicense 4.0 (CCBY), which permits unrestricted use, distribution, and reproductionin any medium, provided the original work is properly cited.
Cite this article as:Torossian,M., & Jacelon, C. S. (2021). : A systematic review. Rehabil-
itation Nursing, 46(3), 125–136. doi: 10.1097/RNJ.0000000000000278
May/June 2021 • Volume 46 • Number 3
and a decline in social and physical function (Menting et al.,2018; Ream & Richardson, 1996).
Although individuals in all age groups experience fa-tigue, this is a concept of particular interest in older individ-uals. First, fatigue is one of the most prevalent symptomsreported in older individuals, whereby 77% of patientsabove the age of 70 years reported fatigue upon hospitaladmission, and had an odds ratio (OR) of 3.20 to retainthis symptom for 3 months following discharge (van Sebenet al., 2019). Second, fatigue can be one of the early signsof aging and a self-reported indicator of frailty (Avlund,2010). Thus, advancing knowledge in fatigue-related factorsand effective fatigue management strategies can help delayfrailty, slow down the aging process, and reduce the oddsof symptom persistence post hospital discharge. Third,fatigue is an independent predictor of mortality in thispopulation, whereby individuals with hematological malig-nancies who experienced more fatigue had significantlyworse prognosis and a shortened overall survival, comparedwith those with lower levels of fatigue (Hofer et al., 2018).In addition, fatigue becomes more debilitating and limitingwhen it coexists with chronic conditions, a phenomenon
www.rehabnursingjournal.com 125

126 Feature Feature
common in older adult. Yet, fatigue is often viewed as anormal part of the aging process, rather than amanifesta-tion of an underlying condition.
Geriatric syndromes are a cluster of multifactorial dis-ease presentations that are nonspecific, common acrossmany diseases, and linked to common risk factors (Inouye,Studenski, Tinetti, & Kuchal, 2007). To date, the classifi-cation of fatigue as a geriatric syndrome is vague. Somestudies have included fatigue when examining the preva-lence or progression of geriatric syndromes (van Seben et al.,2019), whereas others have examined cognitive and func-tional decline,weight loss, incontinence, falls, anddepression,without including fatigue (Bell et al., 2016; Tang, Tang, Hu,& Chen, 2017). This, along with unclear causes of fatigueand treatment strategies, adds to the confusion aboutthe concept of fatigue.
Currently, there is an increased interest in chronic diseasesymptom management, including fatigue. Many researchstudies have addressed fatigue in terms of its triggers, con-sequences, management strategies, older individuals’ per-ceptions of fatigue, and so forth. However, clinicians facechallenges understanding the risk factors of fatigue andeffective treatment strategies. Study findings either pertainto a single chronic disease, a geographic location, or an agegroup, which renders them less useful for application inpractice. Systematic reviews comparing and contrastingfindings of different studies are needed to identify themesacross studies. Literature reviews conducted between 2013and 2018 included supportive care measures in olderindividuals with cancer (Naeim, Aapro, Subbarao, &Balducci, 2014), the contribution of occupational and phys-ical therapy self-management interventions in chronic dis-ease (Richardson et al., 2014), and experiences of olderindividuals with heart disease (Falk, Ekman, Anderson,Fu, & Granger, 2013). However, to date, there has notbeen a review focused on findings across studies thataddress risk factors of fatigue, consequences, and fatiguemanagement strategies.
Understanding risk factors of fatigue that are commonacross multiple chronic diseases may lead to the devel-opment of fatigue management interventions applica-ble to more than one chronic disease—a transdiagnosticapproach—and thus benefit a wider scope of older indi-viduals with various chronic diseases while being awareof disease-specific triggers that require tailored interven-tions. Furthermore, evaluating the effectiveness of currentfatigue management strategies is important to addressgaps and guide future research in this area to improveexisting interventions. More effective fatigue interven-tion, in turn, would improve fatigue levels experiencedby older individuals and enhance their quality of life.Hence, the purpose of this literature review was to answer
the following research questions: (1) What is the currentstate-of-art regarding risk factors and consequences of fa-tigue in older individuals with multiple chronic illnesses?(2) How is fatigue perceived by those experiencing it, andhow does it impact their lives? (3) What are the currentfatigue management interventions in this population?
Methods
To achieve the purpose of the study, a systematic litera-ture reviewwas conducted using the following keywords:“fatigue” (field: title), “older adults or geriatrics or seniorsor elderly” (field: text), and “chronic disease or chroniccondition or chronic illness or long-term condition” (allfields). Four databases (CINAHL, PubMed, PsychInfo,andWeb of Science) were searched with the following re-strictions if the option was provided in the database:peer-reviewed (not an option in PubMed), English lan-guage, and sample age of 65 years or older. No year re-strictions were applied, as the aim of this study was tocapture the evolution of findings across time. Followingthe search process, each abstract was read by both re-searchers. Those saved met the inclusion criteria at thispoint: primary sources, peer-reviewed, English language,title included “fatigue” and its relation to a comorbidity/chronic disease, and had a mean sample age of 65 years orolder (or ran a separate analysis of this age group). Articleswere excluded if theywere secondary sources (literature re-views), had a mean sample age of less than 65 years, orwere irrelevant to the question of interest. That is, if studiesaddressed fatigue in relation to variables other than chronicdiseases, they were excluded from the study. There were nospecific diseases or research methodologies determined apriori for inclusion, as the goal was to gather qualitativeand quantitative data from the widest range of chronic dis-eases in which fatigue was a commonly reported symptomin an older adult.
The researchers then reread, categorized, and groupedthe final number of articles to be included in the reviewbased on the aims/topics addressed. The articles were orga-nized into a matrix (Garrard, 2017). The matrix includedindividual study characteristics, including author, year,study design, type of chronic illness, sample age, samplesize, study aim,measurement of fatigue, risk factors, conse-quences, perceptions, and management of fatigue (Table 1).The categories of thematrix were used to guide the appraisalof each article, which was conducted by the first author andreviewed by the second author. A consensus about the finalnumber of articleswas reached following detailed discussionsabout the characteristics of each of the articles. Articles werealso assessed for biases and limitations, which are presentedthroughout the article.

May/June 2021 • Volume 46 • Number 3 www.rehabnursingjournal.com 127
Results
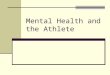
The search strategy yielded 153 articles across all fourdatabases. Of these, 37 studies were excluded for beingduplicates or secondary sources, and 116 articles weresaved. After reexamining the 116 articles, 94 were fur-ther excluded for having a mean sample age of less than65 years or addressing fatigue in relation to variablesother than a chronic disease (sleep, pain, poststroke fa-tigue, fatigue in caregivers, self-reported exhaustion, oridiopathic fatigue). The final number of research studiesthat met the inclusion criteria and were included inthe review was 22. The authors followed the PreferredReporting Items for Systematic Reviews and Meta-Analyses(PRISMA) reporting guideline throughout the article andused the PRISMA flowchart to summarize the steps takenthroughout the search process (Moher et al., 2015; Shamseeret al., 2015; see Figure 1). Narrative synthesis was used tosynthesize the findings (Arai et al., 2007; Rodgers et al.,2009), a commonly used approach in systematic reviewswhen statistical meta-analysis of effectiveness data is notpossible due to heterogeneity of studies.
Sample Characteristics
Research studies included in the review were focused onfatigue in older individuals diagnosed with a broad rangeof chronic diseases, themost common ofwhichwere chronicobstructive pulmonary disease (COPD), congestive heartfailure, and cancer. Sixteen of the 22 studies addressedrisk factors, and nine addressed consequences, individualperceptions, or management as well. One study focusedon consequences, two on subjective perceptions and im-pact on daily life, and two discussed fatigue management.One study addressed both impact of fatigue on daily lifeand management strategies. The research sites of studiesincluded seven from the United States, whereas the re-maining studies were conducted in European countries.
Risk Factors of Fatigue
Sixteen studies in the sample were focused on the firstresearch question: the relationship between fatigue anddifferent variables as risk factors. These studies includedbiophysiological, sociodemographic, psychological, andlifestyle risk factors.
Biophysiological Factors
These included age, body mass index (BMI), comorbidities,gender-related factors, and sleep. Age significantly corre-lated with muscle fatigue (rs = −.26, p < .01) in two studiesincluding men or women exclusively (Lin et al., 2015;Silva et al., 2011). However, two studies recruiting womenwith breast cancer had conflicting findings regarding the
age–fatigue association. In one study, women in the 61–70years age group had the highest fatigue scores com-pared to younger or older women (Muszalik, Kolucka-Pluta, Kedziora-Kornatowska, & Robaczewska, 2016),whereas in another study, women over the age of 75 yearswere nearly 5 times more likely to experience fatigue(OR = 4.81; Jing, Wang, Lin, Lei, &Wang, 2015). A thirdstudy revealed that women between the ages of 40–64years experienced significantly higher emotional distresssecondary to fatigue, in addition to more severe fatigueconsequences, when compared with women 65 years ofage or older (Plach,Heidrich,& Jeske, 2006). Finally, bothin men and women with heart failure, there was no corre-lation between fatigue intensity and age. However, subjec-tive perceptions of age-relatedness of experienced fatiguewas positively associated with fatigue intensity (Stephen,2008).
Findings on the BMI–fatigue association were alsocontradictory. In two studies, individuals with higher BMIhad higher fatigue scores (Lin et al., 2015; Silva et al.,2011), whereas results of another study revealed that onlyunderweightwomen experienced significantlyworse fatiguecompared to other groups (normal, overweight, obese; Jinget al., 2015). It is important to mention that, in the formerstudy, BMI–fatigue correlation was insignificant in a multi-variate linear regression, when accounting for other vari-ables (Silva et al., 2011).
Number of comorbidities was another variable ex-amined in multiple studies; however, findings did notalign either. In two studies, results showed no influenceof comorbidity on fatigue (Galindo-Ciocon & Ciocon,1997; Karakoc & Yurtsever, 2010), whereas findingsin six other studies reflected the opposite. There was asignificant difference in the number of comorbidities betweenfatigued and nonfatigued individuals (Hardy & Studenski,2010; Horne, Johnson, & Crane, 2019; Lin et al., 2015)and a positive correlation between the number of comorbid-ities and perceived fatigue (rs = .18, p < .05; Silva et al., 2011).Interestingly, self-reported comorbidities explained 9%of the variance in fatigue scores in women but was nota significant predictor in men (Horne et al., 2019). Yet, theexperience of concurrent symptoms caused by heart failureor other comorbidities, both inmen andwomen,was signif-icantly correlated with fatigue intensity (Stephen, 2008).Lastly, womenwith breast cancerwhohad one comorbidityhad 1.83 times higher risk of fatigue, and this riskwas three-fold with two or more chronic diseases (Jing et al., 2015).This discrepancy may be due to a number of factors. First,two studies (Galindo-Ciocon & Ciocon, 1997; Karakoc& Yurtsever, 2010) recruited both men and women as op-posed to most of the other studies, in which only men, orwomen,were recruited. Second, the number of comorbidities

Table
1Ch
aracteristicsof
theArticlesInclud
edintheSystem
aticReview
Review
Article
Autho
r(Year),
Locatio
nDesign
Chron
icIllnessof
Sample
SampleAge
(years)
SampleSize
Aim
Fatig
ueMeasurement
Tool
Agn
ihotriet
al.
(2007),IL,USA
Dou
ble-blinded
RCT,crossover
desig
n
Chronicanem
ia,inadditio
nto
HTN
,hypercholesterolemia,
DM
(Type2),CHF,CA
D,gou
t
Meanage:76.1
N=54
Evaluate
theeffectof
epoetin
alfatreatm
enton
hemog
lobin,fatig
ue,qualityoflife,andmob
ilityinelderly
patientswith
chronicanem
ia
FACIT-An
Ekman
&Ehrenb
erg
(2002),Sweden
Descriptive
Chronicheartfailure
Wom
en:83
Men:78
N=158
Describeandcompare
theexperienceof
fatig
ueinagrou
pof
elderly
wom
enandmen
with
severe
chronicheart
failure
Mod
ified
versionof
Fatig
ueInterview
Schedu
le VAS
Galindo
-Ciocon&
Ciocon
(1997),FL,
USA
Cross-sectional
Obesity,cardiac,HTN
,neurolog
ic,lun
gdisease,
sleep
disorders,fibromyalgia,
arthritis,depressio
n
Meanage:72
N=83
Objectivelymeasurechronicfatig
ueandidentifyfactorsthat
contrib
uteto
itsoccurrence
inolderadu
ltsCFS
Hägglun
det
al.
(2008),Sweden
Explorative,
descrip
tive
Chronicheartfailure
73–89
N=10
Illum
inatethelived
experienceof
fatig
ueam
ongelderly
wom
enwith
CHF
N/A
Hardy
&Stud
enski
(2010),PA,U
SACross-sectional
Cardiovascular,neurological,
musculoskeletal,pulmon
ary,
diabetes,cancer,visual,and
general(depressio
n,sle
epprob
lem,chron
icpainetc.)
Meanage:74
N=495
Identifythequ
alities
offatig
ueandassesswhether
they
are
associated
with
distinctchroniccond
ition
sCand
idatequ
estio
nschosen
from
literature
for5
fatig
uequ
alities
Haw
kere
tal.(2010),
Canada
Cross-sectional
OA
Meanage:78
N=613
Evaluate
therelatio
nshipbetweensubjectivesle
epqu
ality
andfatig
ueinindividu
alswith
OA
POMS-F
Hoo
pere
tal.(2017),
France
Cross-sectional
Individu
alswith
mem
ory
complaintsanddifficulty
perfo
rmingADL
Medianage:75
N=269
Explorethecross-sectionalrelationshipbetweenfatig
ueand
cerebralβ-am
yloidin269elderly
individu
als
2Likert-scalequ
estio
ns
Horne
etal.(2019),
NC,USA
Cross-sectional
CVDandothercom
orbidities
Meanage:76
N=98
Exam
inecomorbiditymeasuresthatmay
relate
tothe
symptom
offatig
uepo
stMI
RPFS
-Revise
dPiper
Fatig
ueScale
Jinget
al.(2015),
China
Cross-sectional
Not
mentio
ned
60– 74:390/1,272
≥75:144/
1,272
N=534
TotalN
=1,272
Investigatetheprevalence
offatig
ue,explore
the
relatio
nshipbetweengynecologicalhistoryand
experiences
offatig
ue,and
identifyriskfactorsforfatigue
inmiddle-aged
andelderly
wom
en
CFS
Kapella
etal.(2006),
IL,U
SACross-sectional
COPD
Wom
en:68.7
Men:69.5
N=130
(a)D
escribecharacteristicsof
fatig
ueinpeop
lewith
COPD
and(b)testa
theoreticallyandem
piricallysupp
orted
mod
elof
therelatio
nships
amon
gsubjectivefatig
ue,
dyspnea,functio
nalperform
ance,anxious
anddepressed
moo
ds,and
sleepqu
ality
inpeop
lewith
COPD
Num
ericalRatin
gScale
forfatigue
dimensio
nsFatig
ueAssessm
ent
Instrumentfor
COPD
-related
fatig
ueKarakoc&Yu
rtsever
(2010),Turkey
Descriptive
Cancer
60–64:31/71
≥65:40/71
N=71
Determinetherelatio
nshipbetweenfatig
ueandsocial
supp
ortinelderly
individu
alsreceivingchem
otherapy
VAS-F
128 Feature Feature

Table
1Characteristicsof
theArticlesInclud
edintheSystem
aticReview
,Continued
Review
Article
Autho
r(Year),
Locatio
nDesign
ChronicIllnessof
Sample
SampleAge
(years)
SampleSize
Aim
Fatig
ueMeasurement
Tool
Karakurt&Ünsal
(2013),Turkey
Cross-sectional
COPD
andotherchron
iccond
ition
s(heartdisease,
DM,hyperlipidem
ia,H
TN,
OA,etc.)
Mean:68.87
N=255
Determinethefatig
ue,anxietyanddepressio
nlevels,activities
ofdaily
livingof
patientswith
chronicob
structive
pulmon
arydisease
VAS-F
Kessinget
al.(2016),
theNetherland
sSecond
aryanalysis
ofprospective
datafrom2studies
CHF
Meanage:66.2
N=545
Exam
inewhethergeneraland
exertio
nfatig
uearedistinctively
associated
with
self-care
inpatientswith
chronicHF
Fatigue
AssessmentScale
Dutch
Exertion
Fatigue
Scale
Linet
al.(2015),
China
Cross-sectional
Not
specified
≥65:304/1,158
N=1158
Exploretheprevalence
offatig
ueandidentifytheriskfactors
offatig
ueam
ongmen
aged
45yearsandolderinCh
ina
CFS
Malaguarneraet
al.
(2008),Italy
Dou
ble-blinded
RCT
Not
specified
Wom
en:76.2
Men:78.4
N=96
Evaluatetheeffectofexog
enou
sALC
ontheph
ysicalfunctions
andcogn
itive
status
inelderly
patientswith
fatig
ueWesselyandPowellscore
Fatigue
SeverityScale
Mollaog
luet
al.
(2011),Turkey
Descriptive
COPD
Meanage:72
N=98
Describetheprevalence
andseverityof
fatig
ueandto
investigaterelatio
nships
betweenfatig
ueanddisabilityin
elderly
COPD
patients
VAS-F
Muszalik
etal.
(2016),Poland
Survey
Breastcancer
>61:42/120
N=120
Assessthequ
ality
oflifeinwom
enun
dergoing
radiotherapy
forthe
treatm
entof
breastcancer
FACIT-F
Nicklas
etal.(2016),
NC,USA
Cross-sectionaland
long
itudinal
design
Arthritis,HTN
,CVD
,DM,
osteop
orosis,cancer
Meanage:66.2
N=167
Determinethecross-sectionaland
long
itudinalrelationships
ofob
jectivelymeasuredhabitualPA
tobiom
arkersof
inflammationandself-repo
rted
fatig
ueinmiddle-aged
and
olderadu
lts
SF-36VitalitySubscale
ofMedical
Outcomes
Stud
y
Plachet
al.(2006),
WI,USA
Second
aryanalysis
ofdatafro
mcross-sectional
stud
y
HF
Meanage:69
N=169
Describerepresentatio
nsof
oneHF-relatedsymptom
,fatigue,
andexam
inewhether
representatio
nswererelatedto
physicalhealth
status,health
care
utilizatio
n,and
psycho
logicalw
ell-b
eing
andwhether
they
differedby
age
Symptom
Representatio
nQuestionn
aire
for
Fatig
ueSilvaet
al.(2011),
Brazil
Observatio
nal,
cross-sectional
Not
mentio
ned
Meanage:71.29
N=135
Investigatetheassociationof
clinical,fun
ctional,and
inflammatoryfactorswith
musclefatig
ueandself-perceived
fatig
ueinelderly
wom
en
VAS-F
Step
hen(2008),ID,
USA
Cross-sectional
HF
Meanage:77
N=53
Describetherelatio
nships
betweenfatig
ueintensity
and
symptom
experienceandsymptom
outcom
es(fu
nctio
nal
status,qualityof
life,satisfaction)
Identifythedemog
raph
ic,clinical,and
symptom
outcom
epredictorsof
fatig
ueintensity
inolderadu
ltswith
stableHF
POMS-F
VAS-F
Theand
er&
Uno
sson
(2011),
Sweden
Descriptivecross-
sectional
COPD
N/A
NCOPD
=345
NControl=
245Exam
inegend
erdifferences
inexperiences
offatig
ueand
functio
nallimitatio
nsdu
eto
fatig
ueinpatientswith
chronic
obstructivepu
lmon
arydiseaseandacomparison
grou
p
Structured
questio
nsabou
tfatig
uefrequ
ency,severity,
anddu
ratio
n
Note.RCT=random
izedcontrolledtrial;HTN
=hypertension;DM=diabetesmellitus;CHF=chronicheartfailure;OA=osteoarth
ritis;AD
L=activitiesofdailyliving;CO
PD=chronicobstructivepulmonarydisease;CFS=Ch
alderFatigue
Scale;POMS-F=Profile
ofMoodStatesFatigue
Subscale;PA=physicalactivity;SF-36
=ShortForm-36item;CAD
=coronaryarterydisease;CVD=cardiovasculardisease;HF=heartfailure;NA=notapp
licable;FAC
IT-An=Functional
Assessmento
fChronicIlln
essTherapy-Anemia;VAS
=visualanalog
scale;VA
S-F=VisualAn
alog
Scale-Fatigue;ALC
=Acetyl-L-Carnitine;FACIT-F=FunctionalAssessm
ento
fChronicIlln
essTherapy-Fatigue.
May/June 2021 • Volume 46 • Number 3 www.rehabnursingjournal.com 129

Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart of the articles included in the review.
130 Feature Feature
varied between and within studies, making a significant dif-ference undetectable when two groups were similar in termsof this variable. Lastly, these studies used different fatiguemeasure tools, reflecting different dimensions of fatigue,and measured different aspects of fatigue (risk of fatigue,fatigue intensity, perceived fatigue).
Of the women-specific variables, results of a study onwomen with breast cancer revealed that the number oflive births significantly correlated with fatigue, and theodds of fatigue was 4.17 times higher in women who hadfour or more live births compared to those who only hadone. In addition, postmenopausal women were 1.70 timesmore likely to experience fatigue than premenopausalones (Jing et al., 2015). Although the study had adequatepower, and a reliable, culture-sensitive tool was used tomeasure fatigue (Chalder Fatigue Scale), findings shouldbe interpreted in caution, as the sample consisted of pa-tients with cancer only.
Finally, two studies addressing sleep found a positivecorrelation between sleep and fatigue. In patients withCOPD, researchers found a moderate and a positivecorrelation between sleep (higher scores reflecting worsesleep quality) and fatigue (r = .4, p < .001; Kapella,Larson, Patel, Covey, & Berry, 2006) and worse fatiguelevels in individuals with osteoarthritis who experiencedpoor sleep (Hawker et al., 2010). A study comparingfatigued and nonfatigued individuals found that sleep
disorders were significantly more prevalent in individ-uals in the former group (Galindo-Ciocon & Ciocon,1997). However, a limitation of these studies is that var-iables such as dailymedications, number and type of comor-bidities, and social support that would have influenced ormediated this relationship were not included in either ofthe studies.
Sociodemographic Factors
There was a significant negative correlation between so-cial support (information, security, emotional, and per-ceived) and fatigue (−.78 < r < −.65, p < .001) and asignificant positive correlation between social supportand energy (.71 < r < .82, p < .001) scores (Karakoc &Yurtsever, 2010). Education and economic status werealso correlated with fatigue in all but one study. Five studiesshowed that individuals with higher levels of education hadsignificantly lower fatigue levels (Jing et al., 2015; Karakurt& Ünsal, 2013; Kessing, Denollet, Widdershoven, &Kupper, 2016; Lin et al., 2015; Muszalik et al., 2016);however, that did not hold true in the study by Karakocand Yurtsever (2010). Economic status was positively as-sociated with fatigue scores: Employed individuals orthose in a “very good” economic status had significantlyless fatigue compared with those unemployed (Kessinget al., 2016) or those in “good” or “difficult” economicstanding (Muszalik et al., 2016).

May/June 2021 • Volume 46 • Number 3 www.rehabnursingjournal.com 131
Findings onmarital status varied greatly. Two studiesinvolving men and women showed no significant differ-ence in fatigue scores between married, widowed, single,or divorced individuals (Horne et al., 2019; Karakoc &Yurtsever, 2010). This was contrary to findings of twostudies in which married older individuals experienced sig-nificantly higher fatigue than unmarried ones (Mollaoglu,Fertelli, & Tuncay, 2011; Stephen, 2008). However, twostudies involving either men or women exclusively showedthat single men and single women have higher odds of fa-tigue (OR = 1.94 and OR = 1.42, respectively) comparedwith their married counterparts (Jing et al., 2015; Linet al., 2015). To add up to the inconsistency, widowed in-dividuals in a study experienced worse fatigue comparedto married and unmarried individuals, with no differencesbetween married and unmarried individuals (Karakurt &Ünsal, 2013).
Psychological Factors
Findings across multiple studies were consistent in termsof the relationship between fatigue and psychological var-iables. Depression and anxiety were weakly but signifi-cantly correlated with fatigue scores (r = .36 and r = .32,respectively; Karakurt & Ünsal, 2013). This correlationwas supported, and even stronger, in another study aswell (rfatigue/depression = .45, rfatigue/anxiety = .49, p < .001;Kapella et al., 2006). Similarly, weak but significant cor-relations were found in the study by Silva et al. (2011),where fatigue was positively correlated with depression(rs = .38, p < .01) and negatively correlatedwith perceivedhealth (rs=−.25,p< .01). In otherwords, individualswith fa-tigue had significantly higher depression scores and poorerperceived health (Hardy & Studenski, 2010).
Lifestyle and Fatigue
A number of studies investigated the influence of physicalactivity (PA) or exercise on fatigue. A study examining thecorrelation of inflammation, PA, and fatigue cross-sectionallyand longitudinally found a significant correlation, at baseline,between PA (measured in steps/day) and fatigue (r = .19,p< .05), but not between fatigue and inflammatorymarkerslike C-reactive protein and interleukin-6 (Nicklas et al.,2016). The correlation between fatigue and PA remainedsignificant at the 6-month and 18-month follow-up period,indicating that increasing activity at any point resulted in re-duced fatigue levels. Interestingly, fatigue was significantlycorrelated with C-reactive protein and interleukin-6 at the6-month follow-up (r = −.28 and r = −.29 respectively),but not at the 18-month follow-up (Nicklas et al., 2016).Similarly, other studies supported the correlation betweenPA and muscle fatigue (rs = .29, p < .01), perceived fatigue(rs = −.38, p < .01; Silva et al., 2011), and total fatigue scores
(Galindo-Ciocon & Ciocon, 1997; Lin et al., 2015). An-other study demonstrated that activities of daily living werenegatively correlated with fatigue scores (r = −.45; Karakurt&Ünsal, 2013). Note that the relationship between PA andfatigue is bidirectional. That is, fatigue levels, in their turn,also impact PA. This was supported in a study in which in-dividuals who experienced three or more qualities of fatigueshowed significantlyworse physical performance comparedto those who only reported one fatigue quality (Hardy &Studenski, 2010).
These findings should be interpreted in light of thestudies’ limitations, which included the use of a single fa-tigue scale, one being the Short Form-36 itemVitality sub-scale, which is not specific to older individuals (Nicklaset al., 2016). Another limitation is the lack of a reliablePA measure used in two of these studies (Galindo-Ciocon& Ciocon, 1997; Lin et al., 2015) and no reporting ofthe psychometric properties of fatigue or PA measurementtools in most studies. Finally, none of the study designswere randomized controlled trials (RCTs), meaning thatcausation cannot be implied.
Another lifestyle factor addressed in only one studywas medication use. Diuretics, nitrates, and psychotropicmedications were associated with worse fatigue scores(general and exertional), whereas exertional fatigue scoreswere better (less fatigued) in individuals taking β-blockers.Other medications such as Angiotensin Converting Enzyme(ACE) inhibitors, statins, aspirin, and calcium antagonistsdid not significantly impact fatigue scores (Kessing et al.,2016). Doses of these medications were not mentioned,making inferences for medication management of fatiguereduction impossible.
Consequences of Fatigue
In an attempt to identify qualities of fatigue and examinetheir association with distinct clinical characteristics, Hardyand Studenski (2010) conducted a research study with 495older adults diagnosedwith various chronic diseases. Partic-ipantswere asked to complete surveys related to the numberof chronic conditions, self-rated health, physical function/performance, depression, and presence/absence of fatiguequalities. The researchers identified fatigue qualities basedon the fatigue measure tools in the literature including theCancer Fatigue Scale, the Revised Piper Fatigue Scale, theSchwartz Cancer Fatigue Scale, the MultidimensionalFatigue Inventory, and others. Qualities of fatigue were cate-gorized as mental (consisting of emotional and cognitive do-mains) or physical (relating to weakness, loss of energy, andsleepiness). The most commonly reported fatigue qualitywas tiredness, and the least reported was emotional fatigue,with sleepiness and tiredness being significantly more

132 Feature Feature
prevalent in women than in men. Results showed small tomoderate correlations between fatigue qualities, suggestingthat each represented a distinct underlying pathophysiol-ogy. However, there was overlap between distinct condi-tions and their associated fatigue qualities. For example,pulmonary, musculoskeletal, cardiovascular, and neurolog-ical disorders had higher odds of experiencing sleepinessand tiredness (two qualities of fatigue), despite being linkedto different pathophysiological processes. Hence, researchersconcluded that qualities of fatigue representmanifestations ofa common underlying process like inflammation, commonacross different chronic diseases (Hardy & Studenski,2010). The researchers did not discuss details of the litera-ture review process and how they had determined the finalfive qualities of fatigue. Yet, these findings can still providea basis for clinicians in the management of the differentqualities of fatigue experienced by individuals with chronicdiseases.
A number of predictors were associated with the se-verity of fatigue consequences. For example, functionalhealth, heart failure symptom burden (higher scores indi-cating less symptom burden), subjective health, purposein life, and self-acceptance were negatively associatedwith severity of fatigue consequence (r = −.43, r = −.55,r = −.36, r = −.26, and r = −.27, respectively). Depression,anxiety, symptom burden of other health problems, andnumber of physician visits in the past year positively cor-related with fatigue consequences (r = .42, r = .34, r = .40,and r = .31, respectively). The severity of fatigue conse-quence was a significant predictor of depression, anxiety,and purpose in life (r = .40, r = .20, and r = −.22, respec-tively; Plach et al., 2006). Participants in this study werediagnosed with heart failure. Yet, the fatigue scale used inthe study was originally developed for use among patientswith cancer. The internal consistency of subscale for fatigueconsequence in this sample was .71; however, other sub-scales did not show adequate internal consistency.
A study including individuals aged 70 years or greaterand diagnosed with dementia showed a weak positive asso-ciation between fatigue (measured at the clinical examina-tion that was closest to the positron emission tomographyscan) and β-amyloid load in the hippocampus (β = 0.07,p = .016) in individuals with a clinical dementia rating(CDR) of 0.5 (Hooper et al., 2017). Researchers carriedout a sensitivity analysis on individuals of CDR of 0.5 spe-cifically, as this subgroup had a high risk of progressing toa dementia-related illness like Alzheimer’s disease. This as-sociation was insignificant in the multivariate regressionon data from the whole sample. In addition, there wasno significant association between chronic fatigue and ce-rebral β-amyloid load, although this was not examinedseparately on those with a CDR of 0.5 (Hooper et al.,
2017). Another drawback of the study is the use of a fa-tigue measure tool that was not specifically designed tocapture the physiological aspect of fatigue and consistedof only two items, despite fatigue being a primary variableof interest.
Finally, poor self-care and not consulting a healthcareprovider as neededwere also found to be consequences offatigue, whereby general and exertional fatigue (second-ary to activity) were significant predictors of self-care(β = 0.01, p = .004 and β = 0.06, p = .01, respectively)and consultation with a healthcare provider (β = 0.05,p = .04 and β = 0.05, p = .007, respectively). This associ-ation was significant even after accounting for covariateslike age, gender, and educational level, which are knownto influence these behaviors. In addition, fatigue correlatedpositively with physical and social disability (r = .45,p < .001), with a moderate effect size (Mollaoglu et al.,2011). However, these results relied on participants’ self-reports of self-care and disability, and hence, the risk ofsocial desirability and recall biases may be present (Kessinget al., 2016). Besides, findings pertained to individualswith heart failure only, which is another limitation.
Subjective Perceptions of Fatigue and Its Impact onDaily Life
Researchers in a study interviewed women between theages of 73 and 89 years to illuminate their lived experi-ence of fatigue and how it impacts their life. Accordingto these women, fatigue was a state of loss of energy, dur-ing which optimal rest could not be achieved, regardlessof the number of hours of sleep (Hägglund, Boman, &Lundman, 2008). Individuals also experienced unfamiliarbodily sensations like numbness and breathlessness. Fa-tigue was unpredictable, whereby the physical ability ofthose experiencing it varied tremendously throughoutthe day, making activity planning a challenge, and ren-dered them in need of others’ help. On the social level, fa-tigue presented a networking barrier to these individuals,which led to feelings of loneliness.
In studies involving men and women, both describedfatigue as a state of “feebleness” and “listlessness” with nosignificant difference in fatigue ratings or levels of functionallimitation (Ekman & Ehrenberg, 2002; Karakurt & Ünsal,2013; Theander & Unosson, 2011). However, womencommonly perceived fatigue as “severe,” unlike men whoperceived it as “mild” (Ekman & Ehrenberg, 2002). Thiswas further supported in three studies in individuals withCOPD or heart failure, whereby women experienced morefatigue than men (Kapella et al., 2006; Kessing et al., 2016;Mollaoglu et al., 2011). Both men and women with higherratings of fatigue intensity had a worse health-related

May/June 2021 • Volume 46 • Number 3 www.rehabnursingjournal.com 133
quality of life (r = .53, p < .001), and this associationwas even stronger in individuals who attributed fatigueto age (Stephen, 2008). Individuals coped with fatigue byappreciating the limited yet significant independence andthe fact that they were still able to perform certain tasks.Interviewed women also adjusted the frequency and thetiming of their activities and occasionally accepted helpfrom others. Some were willing to use assistive deviceslike wheelchairs as part of the adaptation, yet others re-fused it for fear of becoming less active. Instead, theyconsciously forced themselves to be as active as possible(Hägglund et al., 2008).
Although these findings provide important insightsof the lived experience of fatigue from older individuals’perspective themselves, it is important to account for thestudies’ limitations. Participants in the first study (Hägglundet al., 2008) were women diagnosed with congestive heartfailure, and hence, the transferability of findings is ques-tionable, especially with the absence of a thorough descrip-tion of the study sample. In addition, steps to ensure rigorand trustworthiness such as keeping an audit trail, memberchecking, or peer debriefing (Lincoln&Guba, 1985) werenot explicitly reported. In regard to the study by Theanderand Unosson (2011), researchers did not report the reli-ability and the validity of the three-item fatigue measureused.
Management of Fatigue
People with chronic illnesses experiencing fatigue adoptedvarious self-management strategies to overcome challengesand reduce fatigue. As discussed earlier, PAwas a signifi-cant predictor of lessened fatigue, and thus, engaging inPA may be an effective way to decrease fatigue levels.Combining exercise and diet in overweight individuals re-sulted in less fatigue, compared to adopting either of thestrategies independently (Nicklas et al., 2016). Partici-pants in different studies also reported that their fatigueresponded to rest and sleep (Ekman & Ehrenberg, 2002;Kapella et al., 2006).
Maintaining normal hemoglobin levels is also a fac-tor in fatigue management. In a RCT, older individualsreceiving epoetin alfa had higher hemoglobin levels bythe end of the study compared to the placebo group. Thisimprovement in hemoglobin levels was associated withlessened fatigue scores (Agnihotri et al., 2007). However,this study was carried out on individuals with anemiaonly, and thus, this interventionmay not be effective in in-dividuals with normal hemoglobin levels.
A study evaluated the impact of acetyl-L-carnitine(ALC; a member of “carnitines” known to have a role in in-termediary metabolism) supplementation on fatigue levels in
individuals aged 70 years or older. In this double-blindedRCT, ALC demonstrated a significant impact on fatigue,where individuals receiving 2 g of ALC twice a day ex-perienced a significant decline in fatigue levels: a 50%decrease in prolonged fatigue after activity, a 7-pointdecrease in physical fatigue scores, a 3.3-point decreasein mental fatigue scores, and a decline of 22.5 points onthe fatigue severity scale. This was also accompanied by a7-point increase in functional status (Malaguarnera et al.,2008). The change in scores was significantly different be-tween the intervention group receiving ALC and the placebogroup.Baseline characteristicswere similar inbothgroups.Re-searchers also reported that there were no adverse drug effectsor abnormal laboratory results in either of the groups.
Discussion
This systematic review aimed to identify risk factors andconsequences of fatigue investigated to date, fatigue man-agement interventions, as well as the perceptions of fatigueby individuals with chronic illnesses and theways inwhichfatigue impacts their lives. Findings demonstrated that fa-tigue can be a result of disease-specific, biophysiological,socioeconomical, and psychological factors, the conse-quences of which include limitations on individuals’ func-tional status, social role, self-care, depression, anxiety,health-related quality of life, and sense of purpose in life.Interventions that could improve fatigue levels includedincreasing PA, getting adequate rest and sleep, maintainingnormal hemoglobin levels, and ALC supplementation. Al-though conditions differ in their pathophysiology, the over-lap between different conditions and their associated fatiguequalities, as well as the correlation between fatigue, inflam-mation, nutrition, and performance, suggests an underlyingcommon pathway (Hardy & Studenski, 2010; Hofer et al.,2018). Hence, besides fatigue management interventionstailored to each individual’s needs, a transdiagnostic ap-proach might be an effective strategy to address fatiguein different chronic conditions using similar interventions.This can help identify additional gaps in the literature andexamine further areas for study.
Future research should be guided toward resolvinginconsistencies in findings of research studies included inthis systematic review. Clarifying the ambiguity regardingthe correlation between fatigue and age, gender, and BMIwould be useful to determine whether clinicians shouldaccount for age and gender in determining baseline fa-tigue levels and whether weight management should bepart of the fatigue-specific interventions or not. A studyof women with cancer found certain gynecological fac-tors to be risk factors for fatigue. Thus, it would be ofvalue to examine whether these findings are generalizable

Key Practice Points• Nurses should carefully screen individuals for identified
risk factors for fatigue, as this provides baselineinformation and guides nurses’ fatigue managementinterventions.
• Nurses should acknowledge older individuals’experiences and perceptions of fatigue and developtailored care plans to meet their needs.
• Nurses can recommend and discuss with otherhealthcare team members the available fatiguemanagement strategies and validate their effectivenessin various chronic conditions.
• Inconsistencies in findings and the lack of ongoingevaluation of fatigue measure scales should guide futureresearch toward areas that need further exploration andvalidation of psychometric properties of the variousfatigue measurement tools.
134 Feature Feature
to women without cancer as well. Besides, there was asignificant association between certain medications andfatigue and between pre-positron emission tomographyscan fatigue scores and β-amyloid load in individualswith a CDR of 0.5. Hence, rigorous RCTs are needed tosupport the preliminary findings from these descriptivestudies and provide the basis for future interventions orpreventive measures.
Different fatigue measures were used in the selectedresearch studies, with the Visual Analogue Scale–Fatiguebeing the most common one (five studies). Given the avail-ability of numerous fatiguemeasurement tools, it would bechallenging to determine which scale to use in different set-tings or with different cultures. Hence, a review focusingon the available fatigue measure tools, their psychometricproperties, and the most convenient setting/culture forthe use of each of them would be helpful in guiding re-searchers to choose the tool that would yield the mostreliable fatigue measures.
Besides the limitations of the individual studies discussedthroughout the text, this systematic review has some limita-tions as well. The limited number of keywords, the searchof only four databases, and the exclusion of the gray liter-ature may have excluded some articles pertaining to thediscussed topic. However, strengths of the review lie inthe detailed presentation of the methods used for study se-lection, maintaining an audit trail to keep track of thedecision-making process, the appraisal of individual stud-ies for robustness, the wide scope of chronic diseases in-cluded with no publication year restrictions, the differentlocations in the U.S. and European countries, and inclu-sion of studies with a mean sample age of 65 years orolder only, so that findings are generalizable and applica-ble to this age group specifically.
Conclusions
This is the first systematic review that integrates findingsrelated to risk factors, consequences, perceptions, andmanagement strategies of fatigue in individuals aged 65 yearsand olderwith various chronic conditions. Findings of thisreview are of value to individuals who share similar char-acteristics (age, chronic diseases) as participants of the in-cluded research studies, to healthcare providers generally,and to rehabilitation nurses specifically, who follow-upolder adults postdischarge and have a major role in man-aging their fatigue. To prevent these undesirable conse-quences, older individuals should be screened for thediscussed modifiable risk factors of fatigue. The inconsis-tencies addressed can guide researchers to potential researchareas to determine the best scientific evidence. Fatigue is aburdensome symptom that affects individuals’ function,psychological well-being, and quality of life. Thus, more at-tention should be paid to unify the approach in care deliveryacross multiple disciplines to reduce fatigue to the furthestextent possible.
Conflict of Interest
The authors declare no conflict of interest.
Funding
The development of this publication was supported by theNational Institute of Nursing Research of the National In-stitutes of Health under Award Number P20NR016599.The content is solely the responsibility of the authors anddoes not necessarily represent the official views of the Na-tional Institutes of Health.
ReferencesAaronson, L. S., Teel, C. S., Cassmeyer, V., Neuberger, G. B.,
Pallikkathayil, L., Pierce, J., … Wingate, A. (1999). Definingand measuring fatigue. Journal of Nursing Scholarship, 31(1),45–50.
Agnihotri, P., Telfer, M., Butt, Z., Jella, A., Cella, D., Kozma, C.M.,… Akamah, J. (2007). Chronic anemia and fatigue in elderlypatients: Results of a randomized, double-blind, placebo-controlled,crossover exploratory study with epoetin alfa. Journal of theAmerican Geriatrics Society, 55(10), 1557–1565. doi:10.1111/j.1532-5415.2007.01357.x
Arai, L., Britten, N., Popay, J., Roberts,H., Petticrew,M., Rodgers,M.,& Sowden, A. (2007). Testing methodological developments in theconduct of narrative synthesis: A demonstration review of researchon the implementation of smoke alarm interventions. Evidence &Policy A Journal of Research Debate and Practice, 3(3), 361–383.doi:10.1332/174426407781738029
Avlund, K. (2010). Fatigue in older adults: An early indicator ofthe aging process? Aging Clinical and Experimental Research,22(2), 100–115. doi:10.1007/BF03324782
Bell, S. P., Vasilevskis, E. E., Saraf, A. A., Jacobsen, J. M. L.,Kripalani, S., Mixon, A. S., … Simmons, S. F. (2016). Geriatricsyndromes in hospitalized older adults discharged to skilled

May/June 2021 • Volume 46 • Number 3 www.rehabnursingjournal.com 135
nursing facilities. Journal of the American Geriatrics Society,64(4), 715–722. doi:10.1111/jgs.14035
Ekman, I., & Ehrenberg, A. (2002). Fatigue in chronic heartfailure – Does gender make a difference? European Journalof Cardiovascular Nursing, 1(1), 77–82. doi:10.1016/S1474-5151(01)00016-0
Falk, H., Ekman, I., Anderson, R., Fu, M., & Granger, B. (2013).Older patients' experiences of heart failure-an integrative literaturereview. Journal of Nursing Scholarship, 45(3), 247–255. doi:10.1111/jnu.12025
Galindo-Ciocon, D., & Ciocon, J. O. (1997). Chronic fatigue in theelderly. Journal of Clinical Geropsychology, 3(4), 291–298.doi:10.1016/S0001-2092(06)63462-5
Garrard, J. (2017).Health sciences literature review made easy: Thematrix method. Burlington, MA: Jones & Bartlett Learning.
Goedendorp, M.M., Tack, C. J., Steggink, E., Bloot, L., Bazelmans,E., & Knoop, H. (2014). Chronic fatigue in Type 1 diabetes:Highly prevalent but not explained by hyperglycemia orglucose variability. Diabetes Care, 37(1), 73–80. doi:10.2337/dc13-0515
Hägglund, L., Boman, K., & Lundman, B. (2008). The experienceof fatigue among elderly women with chronic heart failure.European Journal of Cardiovascular Nursing, 7(4), 290–295.doi:10.1016/j.ejcnurse.2007.12.004
Hardy, S. E., & Studenski, S. A. (2010). Qualities of fatigue andassociated chronic conditions among older adults. Journal ofPain and SymptomManagement, 39(6), 1033–1042. doi:10.1016/j.jpainsymman.2009.09.026
Hawker, G. A., French, M. R., Waugh, E. J., Gignac, M. A. M.,Cheung, C., & Murray, B. J. (2010). The multidimensionalityof sleep quality and its relationship to fatigue in older adultswith painful osteoarthritis. Osteoarthritis and Cartilage, 18(11),1365–1371. doi:10.1016/j.joca.2010.08.002
Hofer, F., Koinig, K. A., Nagl, L., Borjan, B., & Stauder, R. (2018).Fatigue at baseline is associated with geriatric impairments andrepresents an adverse prognostic factor in older patients with ahematological malignancy. Annals of Hematology, 97(11),2235–2243. doi:10.1007/s00277-018-3420-8
Hooper, C., Barreto, P. D. S., Coley, N., Causse, E., Payoux, P.,Salabert, A. S.,… Vellas, B. (2017). Cross-sectional associations oftotal plasma homocysteine with cortical β-amyloid independentlyand as a function of omega 3 polyunsaturated fatty acid statusin older adults at risk of dementia. The Journal of Nutrition,Health & Aging, 21(10), 1075–1080. doi:10.1007/s12603-017-0989-x
Horne, C. E., Johnson, S., & Crane, P. B. (2019). Comparingcomorbidity measures and fatigue post myocardial infarction.Applied Nursing Research, 45, 1–5. doi:10.1016/j.apnr.2018.11.004
Inouye, S. K., Studenski, S., Tinetti, M. E., & Kuchel, G. A. (2007).Geriatric syndromes: Clinical, research, and policy implicationsof a core geriatric concept. Journal of the American GeriatricsSociety, 55(5), 780–791.
Jing,M. J.,Wang, J. J., Lin,W.Q., Lei, Y.X.,&Wang, P. X. (2015). Acommunity-based cross-sectional study of fatigue in middle-agedand elderly women. Journal of Psychosomatic Research, 79(4),288–294. doi:10.1016/j.jpsychores.2015.05.009
Kapella,M. C., Larson, J. L., Patel,M. K., Covey,M.K.,& Berry, J. K.(2006). Subjective fatigue, influencing variables, and consequencesin chronic obstructive pulmonary disease. Nursing Research,55(1), 10–17. doi:10.1097/00006199-200601000-00002
Karakoc, T., & Yurtsever, S. (2010). Relationship between socialsupport and fatigue in geriatric patients receiving outpatientchemotherapy. European Journal of Oncology Nursing, 14(1),61–67. doi:10.1016/j.ejon.2009.07.001
Karakurt, P., & Ünsal, A. (2013). Fatigue, anxiety and depressionlevels, activities of daily living of patients with chronic obstructive
pulmonary disease. International Journal of Nursing Practice,19(2), 221–231. doi:10.1111/ijn.12055
Kessing, D., Denollet, J., Widdershoven, J., & Kupper, N. (2016).Fatigue and self-care in patients with chronic heart failure.European Journal of Cardiovascular Nursing, 15(5), 337–344.doi:10.1177/1474515115575834
Lin, W. Q., Jing, M. J., Tang, J., Wang, J. J., Zhang, H. S., Yuan, L.X.,&Wang, P. X. (2015). Factors associatedwith fatigue amongmen aged 45 and older: A cross-sectional study. InternationalJournal of Environmental Research and Public Health, 12(9),10897–10909. doi:10.3390/ijerph120910897
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. BeverlyHills, CA: SAGE.
Malaguarnera, M., Gargante, M. P., Cristaldi, E., Colonna, V.,Messano, M., Koverech, A., … Motta, M. (2008). AcetylL-carnitine (ALC) treatment in elderly patients with fatigue.Archives of Gerontology and Geriatrics, 46(2), 181–190.doi:10.1016/j.archger.2007.03.012
Menting, J., Tack, C. J., Bleijenberg, G., Donders, R., Fortuyn, H. A.D., Fransen, J.,…Knoop, H. (2018). Is fatigue a disease-specificor generic symptom in chronic medical conditions? HealthPsychology, 37(6), 530–543. doi:10.1037/hea0000598
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A.,Petticrew, M.PRISMA-P Group (2015). Preferred reporting itemsfor systematic review and meta-analysis protocols (PRISMA-P)2015 statement. Systematic Reviews, 4(1), 1. doi:10.1186/2046-4053-4-1
Mollaoglu, M., Fertelli, T. K., & Tuncay, F. O. (2011). Fatigue anddisability in elderly patients with chronic obstructive pulmonarydisease (COPD). Archives of Gerontology and Geriatrics, 53(2),E93–E98. doi:10.1016/j.archger.2010.07.001
Muszalik, M., Kołucka-Pluta, M., Kędziora-Kornatowska, K.,& Robaczewska, J. (2016). Quality of life of women withbreast cancer undergoing radiotherapy using the functionalassessment of chronic illness therapy–fatigue questionnaire.Clinical Interventions in Aging, 11, 1489–1494. doi:10.2147/CIA.S113530
Naeim, A., Aapro, M., Subbarao, R., & Balducci, L. (2014).Supportive care considerations for older adults with cancer.Journal of Clinical Oncology, 32(24), 2627–2634. doi:10.1200/JCO.2014.55.3065
Nicklas, B. J., Beavers, D. P.,Mihalko, S. L.,Miller, G.D., Loeser, R.F., &Messier, S. P. (2016). Relationship of objectively-measuredhabitual physical activity to chronic inflammation and fatigue inmiddle-aged and older adults. The Journals of Gerontology. SeriesA, Biological Sciences and Medical Sciences, 71(11), 1437–1443.doi:10.1093/gerona/glw131
Plach, S. K., Heidrich, S.M., & Jeske, L. (2006). Fatigue representationsin women with heart failure. Research in Nursing & Health, 29(5),452–464. doi:10.1002/nur.20156
Ream, E., & Richardson, A. (1996). Fatigue: A concept analysis.International Journal of Nursing Studies, 33(5), 519–529.doi:10.1016/0020-7489(96)00004-1
Richardson, J., Loyola-Sanchez, A., Sinclair, S., Harris, J., Letts, L.,MacIntyre, N. J., … Ginis, K. M. (2014). Self-managementinterventions for chronic disease: A systematic scoping review.Clinical Rehabilitation, 28(11), 1067–1077. doi:10.1177/0269215514532478
Rodgers, M., Sowden, A., Petticrew, M., Arai, L., Roberts, H.,Britten, N., & Popay, J. (2009). Testing methodological guidance onthe conduct of narrative synthesis in systematic reviews: Effectivenessof interventions to promote smoke alarm ownership and function.Evaluation, 15(1), 49–73. doi:10.1177/1356389008097871
Shamseer, L., Moher, D., Clarke, M., Ghersi, D., Liberati, A.,Petticrew, M.PRISMA-P Group (2015). Preferred reporting itemsfor systematic review and meta-analysis protocols (PRISMA-P)

136 Feature Feature
2015: Elaboration and explanation. BMJ, 350, g7647. doi:10.1136/bmj.g7647
Silva, J. P., Pereira,D. S., Coelho, F.M., Lustosa, L. P., Dias, J.M.D.,&Pereira, L. S. M. (2011). Clinical, functional and inflammatory factorsassociated with muscle fatigue and self-perceived fatigue in elderlycommunity-dwelling women. Brazilian Journal of PhysicalTherapy, 15(3), 241–248. doi:10.1590/S1413-35552011000300011
Stephen, S. A. (2008). Fatigue in older adults with stable heart failure.Heart & Lung: The Journal of Critical Care, 37(2), 122–131.doi:10.1016/j.hrtlng.2007.03.006
Tang,H. J., Tang, H. Y. J., Hu, F.W.,&Chen, C.H. (2017). Changesof geriatric syndromes in older adults survived from intensive care
unit.Geriatric Nursing, 38(3), 219–224. doi:10.1016/j.gerinurse.2016.10.011
Theander, K., & Unosson, M. (2011). No gender differences infatigue and functional limitations due to fatigue among patientswith COPD. Journal of Clinical Nursing, 20(9–10), 1303–1310.doi:10.1111/j.1365-2702.2010.03625.x
van Seben, R., Reichardt, L. A., Aarden, J. J., van der Schaaf,M., vander Esch, M., Engelbert, R. H. H.Hospital-ADL Study Group(2019). The course of geriatric syndromes in acutely hospitalizedolder adults: The hospital-ADL study. Journal of the AmericanMedical Directors Association, 20(2), 152–158e2. doi:10.1016/j.jamda.2018.08.003
For more than 139 additional continuing professional development articles related to Geriatrics topics,go to www.NursingCenter.com/ce.
TEST INSTRUCTIONS• Read the article. The test for this nursing continuing professionaldevelopment (NCPD) activity is to be taken online atwww.nursingcenter.com/CE/RNJ. Tests can no longer be mailed or faxed.•You'll need to create an account (it's free!) and log in to accessMy Plannerbefore taking online tests. Your planner will keep track of all your LippincottProfessional Development online NCPD activities for you.• There's only one correct answer for each question. A passing score forthis test is 7 correct answers. If you pass, you can print your certificateof earned contact hours and access the answer key. If you fail, you havethe option of taking the test again at no additional cost.• For questions, contact Lippincott Professional Development:1-800-787-8985.• Registration deadline is June 2, 2023
PROVIDER ACCREDITATIONLippincott Professional Development will award 3.0 contact hours for thisnursing continuing professional development activity.
Lippincott Professional Development is accredited as a provider ofnursing continuing professional development by the American NursesCredentialing Center's Commission on Accreditation.
This activity is also provider approved by the California Board ofRegistered Nursing, Provider Number CEP 11749 for 3.0 contact hours.Lippincott Professional Development is also an approved provider ofcontinuing nursing education by the District of Columbia, Georgia,and Florida, CE Broker #50-1223. Your certificate is valid in all states.
Payment: The registration fee for this test is $10.00 for members and$12.50 for nonmembers.
1. ARN members can access the discount by logging into the secure“Members Only” area of http://www.rehabnurse.org.2. Select the Education tab on the navigation menu.3. Select Continuing Education.4. Select the Rehabilitation Nursing Journal article of your choice5. You will appear at nursing.CEConnection.com.6. Log in using your Association of Rehabilitation Nursing username andpassword. The first time you log in, youwill have to complete your user profile.7. Confirm the title of the CE activity you would like to purchase.8. Click start to view the article or select take test (if you have previouslyread the article.)9. After passing the posttest, select+Cart to add the CE activity to your cart.10. Select check out and pay for your CE activity. Acopy of the receipt willbe emailed.