Embed Size (px)
Citation preview

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 7 1 , N O . 2 1 , 2 0 1 8
ª 2 0 1 8 T H E A U T H O R S . P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E AM E R I C A N
C O L L E G E O F C A R D I O L O G Y F O U N DA T I O N . T H I S I S A N O P E N A C C E S S A R T I C L E U N D E R
T H E C C B Y - N C - N D L I C E N S E ( h t t p : / / c r e a t i v e c o mm o n s . o r g / l i c e n s e s / b y - n c - n d / 4 . 0 / ) .
JACC STATE-OF-THE-ART REVIEW
Chronic ThromboembolicPulmonary Hypertension
Evolving Therapeutic Approaches for Operable andInoperable DiseaseEhtisham Mahmud, MD,a Michael M. Madani, MD,b Nick H. Kim, MD,c David Poch, MD,c Lawrence Ang, MD,a
Omid Behnamfar, MD,a Mitul P. Patel, MD,a William R. Auger, MDc
ABSTRACT
ISS
Fro
Su
Su
Ba
Sp
Pa
rel
Ma
Chronic thromboembolic pulmonary hypertension (CTEPH), a rare consequence of an acute pulmonary embolism, is a disease
that is underdiagnosed, and surgical pulmonary thromboendarterectomy (PTE) remains the preferred therapy. However,
determination of operability is multifactorial and can be challenging. There is growing excitement for the percutaneous
treatment of inoperable CTEPH with data from multiple centers around the world showing the clinical feasibility of balloon
pulmonary angioplasty. Riociguat remains the only approved medical therapy for CTEPH patients deemed inoperable or with
persistent pulmonary hypertension after PTE. We recommend that expert multidisciplinary CTEPH teams be developed at
individual institutions. Additionally, optimal and standardized techniques for balloon pulmonary angioplasty need to be
developed along with dedicated interventional equipment and appropriate training standards. In the meantime, the
percutaneous revascularization option is appropriate for patients deemed inoperable in combination with targeted medical
therapy, or those who have failed to benefit from surgery. (J Am Coll Cardiol 2018;71:2468–86) © 2018 The Authors.
Published by Elsevier on behalf of the American College of Cardiology Foundation. This is an open access article
under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
C hronic thromboembolic pulmonary hyper-tension (CTEPH), a form of pre-capillary pul-monary hypertension, results from
incomplete resolution of pulmonary thromboemboliand formation of a chronic, fibrotic, flow-limitingorganized thrombus within the pulmonary vascularbed. CTEPH is a relatively rare outcome, developingin 0.56% to 3.2% of acute pulmonary embolism survi-vors (1–3), with those patients exhibiting recurrent orunprovoked pulmonary embolism at a greater risk forexperiencing this outcome (4–9). However, the his-tory of “acute pulmonary embolism” in this patientpopulation is debatable because many patients
N 0735-1097
m the aDivision of Cardiovascular Medicine, University of California San D
rgery, University of California San Diego, La Jolla, California; and the c
lpizio Cardiovascular Center, University of California San Diego, La Jolla, C
yer, and Merck; and has served on the Speakers Bureau for Bayer. Dr. P
eakers Bureau for Bayer. Dr. Auger has served as an advisory board memb
nel; and has received research funding from Bayer for the CTEPH registry
ationships relevant to the contents of this paper to disclose.
nuscript received December 3, 2017; revised manuscript received March
present with signs of chronic disease at the time ofinitial diagnosis.
Because the majority of patients with acute pul-monary embolism do not develop CTEPH, severaladditional factors are felt to be contributory (Table 1).Certain hypercoagulable states including the pres-ence of antiphospholipid antibodies and elevatedfactor VIII levels are more common among patientswith CTEPH, with a prevalence of 20% and 41%,respectively (10,11). By contrast, levels of anti-thrombin III, protein C, protein S, or Factor V Leidenare not different among the general populationand patients with CTEPH (12,13). Alternative
https://doi.org/10.1016/j.jacc.2018.04.009
iego, La Jolla, California; bDivision of Cardiothoracic
Division of Pulmonary and Critical Care Medicine,
alifornia. Dr. Kim has been a consultant for Actelion,
och has been a consultant; and has served on the
er (uncompensated) for Bayer’s CTEPH Image Expert
. All other authors have reported that they have no
19, 2018, accepted April 3, 2018.

AB BR E V I A T I O N S
AND ACRONYM S
BPA = balloon pulmonary
angioplasty
CBCT = cone beam computed
tomography
CT = computed tomography
CTED = chronic
thromboembolic disease
CTEPH = chronic
thromboembolic pulmonary
hypertension
LAO = left anterior oblique
mPAP = mean pulmonary
artery pressure
PAH = pulmonary arterial
hypertension
Pd/Pa = mean distal to
proximal arterial pressure ratio
PTE = pulmonary
thromboendarterectomy
PVR = pulmonary vascular
resistance
RPE = reperfusion pulmonary
edema
UC = University of California
= ventilation/perfusion
J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8 Mahmud et al.M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6 Chronic Thromboembolic Pulmonary Hypertension
2469
pathophysiological hypotheses include ineffectiveendogenous fibrinolysis, fibrin variants resistant tointrinsic fibrinolysis, and in situ thrombosis due topulmonary arteriopathy rather than a thromboem-bolic basis for disease (14–16). Deficient angiogenesisand inflammation have similarly been suggested asplaying a role in disease evolution (17). Inflammatorymarkers such as C-reactive protein and tumor necro-sis factor alpha are elevated in CTEPH, and the pres-ence of inflammatory cytokines also suggests thatfailure in endogenous fibrinolysis and thrombusbreakdown could be a consequence of an inflamma-tory process (18–20). Other infrequent conditions andclinical disorders associated with the development ofCTEPH include ventriculoatrial shunt, pacemakerpresence, previous splenectomy, a myeloproliferativedisorder, and the presence of chronic inflammatorydisorders such as inflammatory bowel disease andosteomyelitis (21–23).
CLINICAL PRESENTATION
Patients with CTEPH often present with progressivedyspnea, exercise intolerance, and nonspecific ab-normalities on physical examination. As the diseaseprogresses, there is a high risk of developing pulmo-nary hypertension and right heart failure. Patientsfrequently have New York Heart Association func-tional class III to IV symptoms (7) and may exhibitsigns and symptoms of right ventricular hypertrophyor failure, such as jugular venous distension, rightventricular lift, fixed splitting of the S2 heart sound,right ventricular S3, exertional angina, syncope,hepatomegaly, ascites, and peripheral edema (10,24).
The natural history of acute pulmonary embolism isresolution of emboli within 3 to 6 months in patientsreceiving antithrombotic therapy. Therefore, persis-tent signs and symptoms after this period of anti-coagulation therapy might signal the presence ofchronic thromboembolic disease (CTED), and an eval-uation for such is warranted (25). However, CTEPH isoften diagnosed at an advanced stage due to nonspe-cific symptoms and late appearance of more specificsigns (26). In the European CTEPH registry, it wasobserved that over a year (median 14.1 months) passedfrom the time of clinical presentation to diagnosis (27).Data from the same registry revealed that 74.8% ofpatients with CTEPH reported a previous history ofacute pulmonary embolism, whereas only 56.1% had ahistory of deep venous thromboembolism (27).
DIAGNOSIS
The diagnosis of CTEPH solely based on history andphysical examination findings is challenging, and
more common cardiopulmonary conditionssuch as cardiomyopathy, ischemic heart dis-ease, and obstructive or restrictive pulmonarydisease, are typically suspected (24,27). Chestradiography and pulmonary function testsare helpful in excluding possible airway orparenchymal lung diseases; electrocardiog-raphy may demonstrate findings associatedwith pulmonary hypertension or other cardiacdisorders (28–30). For those patients withsuspected pulmonary vascular disease asdescribed in the preceding text, additionalevaluative studies need to be considered.To screen for pulmonary hypertension andright heart dysfunction, transthoracic echo-cardiography should be obtained (31). Dopplerestimate of right ventricular systolic pressure,right ventricular and atrial chamber size andfunction, and interventricular septal motionare features discernible with this noninvasiveimaging modality. An echocardiogram pos-sesses the additional value in assessingwhether there is valvular or left heart disease,either as a comorbid condition or as thepossible alternative etiology of pulmonaryhypertension. Diagnostic algorithms (25,32)
recommend ventilation/perfusion (V/Q) lung imagingas a pivotal screening test in the evaluation of CTEPHpatients (Table 2, Figure 1).LUNG VENTILATION-PERFUSION SCINTIGRAPHY.
V/Q lung imaging is the initial screening test forevaluating patients with pulmonary hypertensionsuspected of CTEPH (3,10,24). V/Q scanning ishighly sensitive (96% to 97.4%) in detectingperfusion abnormalities and therefore suggestingthe possibility of CTED. Furthermore, with itsnegative predictive value of nearly 100%, a normalV/Q scan excludes the diagnosis of CTEPH (33).Nonetheless, despite the value of lung scintig-raphy, V/Q scan is under-utilized and data fromthe PAH-QuERI (Pulmonary Arterial HypertensionQuality Enhancement Research Initiative) registrydemonstrate that only 57% of pulmonary arterialhypertension (PAH) patients undergo V/Q imagingto exclude CTEPH during their evaluation (34).However, the nonspecificity of this modality limitsits utility for the diagnosis of CTEPH, and anyabnormal perfusion scan requires additional diag-nostic imaging. Computed tomographic pulmonaryangiography, magnetic resonance imaging, and/orcatheter-based pulmonary angiography are ulti-mately required to establish the diagnosis ofCTED.
V/Q

TABLE 1 Risk Factors for the Development of CTEPH
Acute pulmonary embolism
Recurrent pulmonary embolic events
Large perfusion defect
Higher pulmonary artery pressure at time of initial PE diagnosis
Idiopathic (unprovoked) pulmonary embolus
Hemostatic risk factors
Elevated factor VIII, von Willebrand factor, type 1 plasminogenactivator inhibitor
Abnormal fibrinogen structure
Antiphospholipid antibodies and lupus anticoagulant
Non–type-O blood groups
Elevated lipoprotein(a)
Associated medical conditions
Splenectomy
Ventriculoatrial shunt
Infected intravenous catheters/devices
Chronic inflammatory disorders
Hypothyroidism
Malignancy
CTEPH ¼ chronic thromboembolic pulmonary hypertension; PE ¼ pulmonaryembolism.
TABLE 2 Diagnostic Tests Used for CTEPH
Diagnostic Technique Features and Supportive Findings
Chest radiography � Chronic pulmonary embolism: avascular lung areas;asymmetric central pulmonary artery enlargement;evidence of pleural disease
� Pulmonary hypertension: dilatation of main pulmonaryarteries, right atrial or right ventricular enlargement inadvanced disease
Electrocardiography � Right ventricular hypertrophy with right axis deviation
Pulmonary functiontests
� Reduction in DLCO� Mild restrictive defect due to parenchymal scarring
Echocardiography � Pulmonary hypertension� Right atrial enlargement� Right ventricular hypertrophy� Increased tricuspid regurgitation velocity
V/Q scan � Preferred initial test with high sensitivityto detect CTEPH
� Normal ventilation scan with awedge-shaped perfusion defect
CTPA � Lower sensitivity than V/Q scan� Right ventricular enlargement� Recanalized thromboembolic material associated
with attenuated pulmonary arteries beyondthe obstruction
� Bronchial artery collateral flow� Mosaic perfusion of the pulmonary parenchyma
MRI � Evaluation of pulmonary hemodynamics, and rightventricular size and function
� MRA with contrast enhancement has similarsensitivity to CTPA
Pulmonary angiographyand right heartcatheterization
� “Gold standard” technique to assess the locationand extent of disease; more sensitive at segmentaland subsegmental level than CTPA
� Determine surgical accessibility� Hemodynamic evaluation to confirm the diagnosis
CTEPH ¼ chronic thromboembolic pulmonary hypertension; CTPA ¼ computed tomography pulmonary angi-ography; DLCO ¼ diffusing capacity of the lungs for carbon monoxide; MRA ¼ magnetic resonance angiography;MRI ¼ magnetic resonance imaging; V/Q ¼ ventilation-perfusion.
Mahmud et al. J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8
Chronic Thromboembolic Pulmonary Hypertension M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6
2470
COMPUTED TOMOGRAPHY. Given the near universalinclination for evaluating pulmonary vascular anat-omy with computed tomography (CT) pulmonaryangiography, this imaging modality plays an essentialrole in evaluating patients with suspected CTEPH. CTpulmonary angiography may reveal a variety of ab-normalities suggesting CTEPH such as recanalized ororganized thromboembolic material in the pulmonaryarteries, bronchial artery collateral flow, and a mosaicperfusion pattern of the pulmonary parenchyma(35–38) (Figure 2). Additional benefits of this modalityare the assessment of possible underlying paren-chymal lung and mediastinal disease. It can alsodetect other pulmonary vessel disorders that maypresent with perfusion defects on V/Q lung scanningsuch as pulmonary artery sarcoma, pulmonary veno-occlusive disease, or fibrosing mediastinitis, helpingdifferentiate them from CTEPH. However, potentialdifficulties with this imaging modality relate tothe interpretive expertise required and the lowersensitivity for detecting CTED in segmental and sub-segmental vessels. In a recent report, the ability of320-slice CT imaging to detect thromboembolic find-ings in suspected CTEPH patients was evaluated us-ing digital subtraction pulmonary angiography as thecomparative diagnostic method. Although a sensi-tivity and specificity of 97% and 97.1% for CTE relatedfindings was reported in the main and lobar seg-ments, a sensitivity of only 85.8% and specificity of94.6% was observed in the distal vessels (39).
Another less frequently used diagnostic modality iscone beam CT (CBCT), which, though not widelyavailable, has the advantage of evaluating organizedthrombi in segmental and subsegmental pulmonaryarteries in greater detail (40). In CBCT, the x-rays aredivergent, forming a cone instead of the slices oftraditional CT with the x-ray tube and detector panelrotating around the patient (41). When comparedwith CT pulmonary angiography, all segmentalbranches noted with CBCT were detectable with CTpulmonary angiography, but only 69% of sub-segmental branches seen on CBCT could be observedwith CT pulmonary angiography (40). Distal pulmo-nary artery lesion findings on CBCT in CTEPH arereported to be highly consistent (>90%) with those ofselective angiography.
MAGNETIC RESONANCE IMAGING. This imagingmodality has the advantage of being free of ionizingradiation and has the ability to evaluate pulmonaryarterial and parenchymal abnormalities alongwith pulmonary hemodynamics and right ventriculardisease. It has good agreement with otherimaging techniques in CTEPH (42–44), but remains

FIGURE 1 Diagnostic Work-Up of CTEPH
ECG, echocardiogramEvaluation for pulmonary hypertension and other cardiac disorders
Chest radiography, pulmonary function studiesGeneral studies assessing airway or parenchymal lung disease
Signs & symptoms of pulmonary hypertension with/without priorhistory of venous thromboembolism
Ventilation/Perfusion lung scanSubsegmental or larger unmatched perfusion defects
Catheter-based pulmonary angiography• Confirmation of CTE disease• Assessment of operability
Right heart catheterizationConfirmation and assessment of pulmonary hypertension
(i.e., mPAP ≥ 25 mm Hg, PCWP ≤ 15 mm Hg)
CT pulmonary angiography• Confirmation of CTE disease
• Assessment of lung parenchyma, mediastinum, cardiac structures• Exclusion of alternative possible diagnosis (i.e., pulmonary artery
sarcoma, pulmonary veno-occlusive disease, fibrosing mediastinitis)
Magnetic resonance imaging• Confirmation of CTE disease
Abnormal
NormalCTEPH excluded
Ventilation/perfusion imaging plays a central and key role in the diagnostic work-up of
CTEPH. A normal scan virtually excludes the diagnosis while an abnormal scan requires
additional diagnostic tests including invasive hemodynamic and angiographic evaluation.
CT ¼ computed tomography; CTE ¼ chronic thromboembolism; CTEPH ¼ chronic
thromboembolic pulmonary hypertension; ECG ¼ electrocardiogram; mPAP ¼ mean
pulmonary artery pressure; PCWP ¼ pulmonary capillary wedge pressure.
J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8 Mahmud et al.M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6 Chronic Thromboembolic Pulmonary Hypertension
2471
infrequently used because it is time-consuming,not as readily available, and requires interpretiveexpertise (45).
CATHETER-BASED PULMONARY ANGIOGRAPHY
AND RIGHT HEART CATHETERIZATION. Catheter-based pulmonary angiography is safe and has beenconsidered the “gold standard” for imaging in theevaluation of CTEPH. When combined with rightheart catheterization, it can confirm the presence ofCTE disease to the level of the subsegmental vessels,exclude other possible diagnoses, accurately localizeor “map out” lesions in the determination of surgicalaccessibility, and evaluate pulmonary hemodynamicsand right heart function (46,47). Because diagnosticangiography is crucial for identifying organizedthromboembolic disease warranting surgical resec-tion or interventional treatment, image optimizationis critically important.
Biplane subtraction pulmonary angiography re-quires attention to: 1) patient positioning; 2) flat de-tector angulation; 3) collimation; and 4) imagingsystem settings. When obtaining right pulmonary an-giograms, the frontal and lateral flat detectors are keptin straight anterior-posterior and left lateral (or leftanterior oblique [LAO] 90�) views, respectively.Left pulmonary angiograms can be performed instraight anterior-posterior and left lateral views.Rotation of views 20� leftward (to LAO 20� and LAO110�, respectively) is traditionally performed todecrease overlap of themediastinum and left lung, butis not necessary with digital subtraction angiography.Frontal and lateral angiograms are acquired at4 frames/s during contrast injection, then decreased to1 frame/s during the levophase. Angiographic imagingis often prolonged to record levophase pulmonary veindrainage and exclude pulmonary vein stenosis oranomalies.
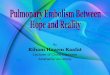
Characteristic pulmonary angiographic findingssuggestive of CTEPH include webs or bands, intimalirregularities, pouch defects, abrupt vascular nar-rowing, and complete obstruction of pulmonaryarteries (48) (Figure 3). Though in the past, selectivepulmonary angiography of individual pulmonaryartery segments was unnecessary for identifyingCTED and determining surgical candidacy, theevolving success of distal vessel thromboendarter-ectomy and the availability of balloon pulmonaryangioplasty has revived the value of this technique.With this, a new classification of lesion morphologybased on the lesion opacity and the blood flow distalto the lesion on pulmonary angiographic images hasbeen described, as follows: type A, ring-like stenosis;
type B, web lesion; type C, subtotal lesion; type D,total occlusion; and type E, tortuous lesion (49)(Figure 4).
MANAGEMENT OF OPERABLE CTED
Both American and European guidelines endorsesurgical therapy in all patients who have accessibledisease and are considered suitable surgical candi-dates (24,25). Surgery by means of a complete bilat-eral pulmonary thromboendarterectomy offers thebest chance of improved long-term outcomes. Atexperienced centers, disease at segmental and evensubsegmental branches can be removed. After theintroduction of the procedure at the University of

FIGURE 2 CT Pulmonary Angiography in CTEPH
(A) Evolution from acute to chronic thromboembolic disease. Left panel showing acute
pulmonary embolism in the right descending pulmonary artery. One year later, vessel
distortion, web and intimal thickening is seen at the same location (middle panel), with
vessel attenuation distally (right panel). (B) CT pulmonary angiographic features of
chronic thromboembolic disease. Left panel showing right middle lobe vessel
narrowing (open red arrow) with lining thrombus versus intimal thickening involving the
right descending pulmonary artery. Recanalized thrombus is seen in the left descending
pulmonary artery (solid red arrow). Right panel showing marked vessel narrowing from
organized clot in the right descending pulmonary artery (solid white arrow) and web in
a proximal left lower lobe segmental vessel (open arrow). (C) “Mosaic perfusion” in
CTEPH. Segmental regions of hyperperfusion and hypoperfusion. CT ¼ computed to-
mography; CTEPH ¼ chronic thromboembolic pulmonary hypertension.
Mahmud et al. J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8
Chronic Thromboembolic Pulmonary Hypertension M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6
2472
California (UC) San Diego in 1970, the technique hasundergone significant iterative modification andimprovement. This has resulted in reduction ofperioperative mortality from almost 20% in the earlyyears to <2% at UC San Diego (50).
The techniques of the operation, known as pul-monary thromboendarterectomy (PTE) or pulmo-nary endarterectomy, are well established, anddetails have been described previously (51,52). Theprocedure is performed via median sternotomy andrequires cardiopulmonary bypass with deep hypo-thermia and total circulatory arrest. Once sternot-omy is performed and the patient is placed oncardiopulmonary bypass, the core temperature isactively cooled to 18�C to 20�C. The head and theheart are wrapped with special cooling jackets andare cooled even further. The process of cooling cantake 30 to 75 min depending on the patient’s bodyhabitus. After appropriate cooling, an aortic cross-clamp is applied, cardioplegia for myocardial pro-tection is administered, and the right pulmonaryartery is explored between the superior vena cavaand aorta. The plane of the dissection is carefullyidentified, which is typically between the intimaland medial layer of the artery, but is often distortedand difficult to establish. The endarterectomy isthen continued into the lobar, segmental, and sub-segmental branches (Online Video 1). Althoughremoval of some thromboembolic material ispossible without circulatory arrest, significantcollateral blood flow occurs through the bronchialarteries, precluding complete endarterectomy.Therefore, circulatory arrest is essential and pro-vides a bloodless field for recognition of the planeof dissection and removal of the thromboembolicmaterial from the pulmonary vasculature (Figure 5)(53). Circulatory arrest times are typically limited to20 min at a time, and complete endarterectomy canusually be performed within this time period. Onceendarterectomy is completed, the circulation isrestarted and the artery closed; the process is thenrepeated for the left side. The patient is thenrewarmed, a process that takes 75 to 120 min. Ifindicated, additional cardiac procedures, such ascoronary artery bypass grafting or valve interven-tion are performed during this rewarming period. Atthe conclusion of the procedure, the patient istaken off cardiopulmonary bypass and the chest isclosed. Generally, these patients require minimalinotropic support and have significantly improvedhemodynamic parameters immediately aftersurgery.
Operating on distal thromboembolic material ischallenging, and patients with lesions located in the

FIGURE 3 Pulmonary Angiographic Findings in CTEPH
(A) Abrupt vascular narrowing with intimal irregularity of the right interlobar artery (white arrow). (B) Early contrast phase showing rounded
vascular irregularity, “pouch defect” consistent with recanalized thrombus. (C) Web defect and vessel narrowing (open arrow) of the left
descending pulmonary artery. (D) Value of lateral angiogram: lateral view (LAT) clearly defining the occlusion of the right descending pul-
monary artery beyond the superior segment take off. CTEPH ¼ chronic thromboembolic pulmonary hypertension; PA ¼ posterior-anterior
view.
J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8 Mahmud et al.M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6 Chronic Thromboembolic Pulmonary Hypertension
2473
distal segmental or subsegmental arteries are morelikely to be deemed technically inoperable than thosewith more proximal disease. In such patients, theplane of dissection is started proximally in the normal
area of the vessel and carefully extended until thediseased areas distally in the segmental and sub-segmental branches are encountered and removed.This can be challenging because the normal intima is

FIGURE 4 Novel Angiographic Classification of CTEPH Lesions
(A) Type A: ring-like stenosis lesion. (B) Type B: web lesion. (C) Type C: subtotal lesion. (D) Type D: total occlusion lesion. (E) Type E: tortuous
lesion. Type A–D lesions (arrows) are located proximal to the subsegmental pulmonary artery, namely, the segmental and subsegmental
arteries. Type E lesions (arrowheads) are located distal to the subsegmental artery. CTEPH ¼ chronic thromboembolic pulmonary hyper-
tension. Reprinted with permission from Kawakami et al. Circ Cardiovasc Interv 2016;9:e003318 (49).
FIGURE 5 Surgical Specimen Resected During PTE Surgery
Bilateral pulmonary endarterectomy with resection of proximal level I disease with associated diagnostic pulmonary angiograms. PTE ¼ pulmonary thromboendar-
terectomy. (Online Video 1) Distal vessel pulmonary thromboendarterectomy. The dissection plane between the intimal and medial layers of the proximal pulmonary
artery is identified and the dissection extended distally to the occluded segment. Following this, the chronic thromboembolic material is removed.
Mahmud et al. J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8
Chronic Thromboembolic Pulmonary Hypertension M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6
2474

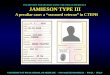
FIGURE 6 Level I to IV Surgical Classification for CTEPH
Surgical resection of proximal to more distal level of disease in CTEPH patients. Technically, level III to IV disease is more challenging to resect
but results in hemodynamic and clinical improvement; however, resection is associated with higher complications. CTEPH ¼ chronic
thromboembolic pulmonary hypertension.
J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8 Mahmud et al.M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6 Chronic Thromboembolic Pulmonary Hypertension
2475
quite fragile and difficult to dissect free. In caseswhere the obstructive material is visible distally, anexperienced surgeon may start the plane of dissectionat the segmental level. The goal is to ensure that allthromboembolic material is removed, and all thebranches have been cleared, before restarting thecirculation.
A recent intraoperative classification of the disease(levels I to IV) (Figure 6) suggested by the UC SanDiego group categorizes pulmonary thromboembo-lism in CTEPH as levels, based on the location of thefibrotic thromboembolic material: level 1, involvingthe main pulmonary arteries; level 2, starting at thelobar branches; level 3, starting at the segmentalbranches; and level 4, where disease is only encoun-tered at the subsegmental branches. In addition,Level 1C indicates complete occlusion of 1 lung withtotal obstruction of the main right or left pulmonaryartery, and level 0 indicates no evidence of CTEPH in
the corresponding lung. It is important to note thatthis is a surgical classification as encountered at thetime of endarterectomy. As imaging modalitiesimprove, the ability to predict the level of diseasepre-operatively has improved; however, invariablymore disease is encountered at the time of surgerythan predicted on routine imaging pre-operatively.Notably, greater technical expertise is required forlevel III to IV disease resection with higher compli-cations, but hemodynamic improvement can still beexpected after successful surgery.
Historically accepted indications for PTE werea mean pulmonary artery pressure (mPAP)>30 mm Hg, pulmonary vascular resistance (PVR)>300 dynes ∙ s ∙ cm�5, and New York Heart Asso-ciation functional classification of III to IV (54,55).However, it is also presently indicated for patientswith symptomatic CTED who are dyspneic ordevelop pulmonary hypertension only with exercise.

TABLE 3 Pulmonary Hypertension Medical Therapy Used for the Treatment of CTEPH
Drug Class Evidence and Effects
Soluble guanylatecyclasestimulants(riociguat)
� CHEST-1 trial (randomized, double-blind,placebo-controlled study) (74);Improved pulmonary vascular resistance and 6-minwalk distance after 16 weeks
� CHEST-2 trial (follow-up extension study) (75);Persistent efficacy for up to 1 yr
Endothelin receptorantagonists(macitentan andbosentan)
Macitentan� MERIT-1 trial (randomized, double-blind,
placebo-controlled study) (76);Improved pulmonary vascular resistance after 16 weeks
Bosentan� BENEFiT trial (randomized, double blind,
placebo-controlled study) (77);Improved pulmonary vascular resistance and cardiacindex after 16 weeks
� Systematic review of BENEFiT and 10observational studies (78);Similar results were reported
Phosphodiesterase 5inhibitors(sildenafil)
� Randomized, double blind, placebo-controlled pilot study (79);Improvement in World Health Organizationfunctional class and pulmonary vascular resistanceafter 12 weeks
Prostanoids(epoprostenoland treprostinil)
Epoprostenol� Retrospective cohort study in severe inoperable CTEPH (80);
Improvement in pulmonary vascular resistance,pulmonary artery pressure, and exercise capacityafter 3 months
Iloporost� AIR study (randomized, double-blind, placebo-controlled
study) (81); Improvement in New York Heart Associationfunctional class and 6-min walk distance at 12 weeks
Treprostinil� Uncontrolled trial in severe inoperable CTEPH (82);
Improved pulmonary vascular resistance after20 months, and higher 5-yr survival rate(53% vs. 16% in historical controls)
AIR ¼ Aerosolized Iloprost Randomized trial; BENEFiT ¼ Bosentan Effects in iNopErable Forms of chronIcThromboembolic pulmonary hypertension trial; CTEPH ¼ chronic thromboembolic pulmonary hypertension;CHEST-1 ¼ Chronic Thromboembolic Pulmonary Hypertension Soluble Guanylate Cyclase–Stimulator Trial 1;CHEST-2 ¼ BAY63-2521 – Long-term Extension Study in Patients With Chronic Thromboembolic PulmonaryHypertension; MERIT-1 ¼ Macitentan for the Treatment of Inoperable Chronic Thromboembolic PulmonaryHypertension trial; PAH ¼ pulmonary arterial hypertension.
Mahmud et al. J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8
Chronic Thromboembolic Pulmonary Hypertension M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6
2476
Surgery results in symptomatic relief and has thetheoretical benefit of preventing disease progressionthat might lead to irreversible small vessel changesand pulmonary hypertension. Operability assess-ment can be complex and requires a multidisci-plinary team of CTEPH experts, which includesrepresentatives from cardiothoracic surgery, pulmo-nary vascular medicine, interventional cardiology,and imaging. This assessment accounts for surgicalaccessibility, presence of hemodynamic or ventila-tory impairments, and evaluation of underlyingcomorbidities prohibiting PTE (56). Perioperativemortality is increased with markedly elevated pre-operative PVR >1,000 dynes ∙ s ∙ cm�5, and to aneven greater extent with residual pulmonary hyper-tension following PTE (22,50,56–58). Nevertheless,the severity of pre-operative PVR and the degree ofpulmonary hypertension should not be considered a
contraindication to surgical intervention as thesepatients may ultimately have the most benefit fromsurgery (50,59). Data from an international registryshow that of 679 newly diagnosed consecutiveCTEPH patients, 427 patients (62.9%) were consid-ered operable (27). Although pre-op PVR >1,500dynes ∙ s ∙ cm�5 and older age were consideredcontraindications to surgery in this registry,currently, these factors do not independentlyconstitute contraindication to surgery at manyexperienced institutions. Furthermore, many ofthose initially considered inoperable went on tohave surgery after a second opinion at an expertcenter.
POST-PULMONARY ENDARTERECTOMY OUTCOMES. Pa-tients undergoing PTE may experience various com-plications similar to other cardiothoracic surgicalprocedures such as arrhythmias, pericardial orpleural effusions, atelectasis, wound infection, anddelirium. Notably, significant reperfusion pulmonaryedema (RPE), a type of noncardiogenic high-permeability pulmonary edema, occurs in 9.6% ofpatients after PTE and can present with mild post-operative hypoxemia to severe hemorrhagic pulmo-nary edema (60,61). The risk of RPE is increasedin patients with high pre-operative and persistentpost-PTE pulmonary hypertension while periopera-tive treatment with methylprednisolone has no effecton the incidence of lung injury in CTEPH patientsundergoing PTE (62).
Cognitive neurological dysfunction is observed inonly a fraction of patients undergoing PTE due toeither deep hypothermia or circulatory arrest (63,64).The benefits of maintaining antegrade cerebralperfusion compared with deep hypothermic circula-tory arrest was evaluated in a randomized controlledtrial, and no difference in cognitive function wasobserved (65). However, there was a significantcrossover to the circulatory arrest group, emphasizingthe need for a bloodless field during completeendarterectomy.
Due to the small number of specialized centers withexperience in PTE and management of patients withCTEPH, there are limited reports on long-term out-comes. The UC San Diego group has reported a 5-yearand 10-year survival of 82% and 75%, respectively,with in-hospital mortality of only 2.2% (51). Other in-stitutions also report 5-year survival rates of 75% to90% (66–70), and 10-year survival rates of 72% (71).Results from an international prospective registry,including 679 newly diagnosed CTEPH patients,showed that patients who underwent PTE surgery had

CENTRAL ILLUSTRATION CTEPH Treatment Algorithm by the Multidisciplinary UC San Diego CTEPH Team
Mahmud, E. et al. J Am Coll Cardiol. 2018;71(21):2468–86.
Once the diagnosis of CTEPH is confirmed, patients are evaluated for PTE surgery. In cases deemed to be to be inoperable, with persistent symptomatic pulmonary
hypertension after PTE surgery, or with an unacceptable risk-benefit ratio, targeted medical therapy and/or BPA is considered. Often patients undergo combined
medical therapy and BPA for optimal hemodynamic and clinical results. BPA ¼ balloon pulmonary angioplasty; CTEPH ¼ chronic thromboembolic pulmonary
hypertension; PTE ¼ pulmonary thromboendarterectomy; UC ¼ University of California.
J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8 Mahmud et al.M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6 Chronic Thromboembolic Pulmonary Hypertension
2477
improved 3-year survival rates compared with thosenot undergoing surgery (27). Other benefits thatare typically observed include improvements in he-modynamic parameters (reduction in PVR and mPAP),
improvement in functional class, remodeling of theright ventricle resulting in reduced wall thickness,increased right and left ventricular ejection fractions,and reduced volumes (51,71,72).

TABLE 4 UC San Diego Approach to BPA
Overall treatment plan
� 4 to 6 separate BPA sessions� Baseline pulmonary angiogram� Baseline and intermittent perfusion scanning� Baseline and intermittent 6-min walk test, BNP, functional assessment� Treatment concluded with 1 BPA procedure in each lung
Individual BPA procedure steps
1. Identify target lung region with largest defect on most recent perfusion scan2. Ultrasound-guided right (or left) femoral vein access, 9-F sheath placement3. Right heart catheterization and hemodynamic measurement within target lung4. 6-F 90-cm sheath advanced over wire into target lung pulmonary artery5. Anticoagulation using IV unfractionated heparin (goal ACT 200 to 250 s)6. 6-F 110-cm Judkins right, multipurpose, hockey stick, or extended back-up guide
catheter advanced over stiff, angled Glidewire into target lung region7. Segmental pulmonary angiography is performed with deep breath holds and injection
of 1:1 diluted contrast at 7.5 to 15 frames/s without digital subtraction8. Atraumatic, workhorse 0.014-inch guidewire, supported by 2.0-mm rapid exchange
balloon catheter used to cross target lesions; avoid polymer-jacketed guidewires9. For complete occlusions, antegrade wire escalation with a microcatheter and increasing
guidewire tip stiffness; avoid polymer-jacketed guidewires10. Pd/Pa measurements during free breathing or deep breath hold using microcatheter-
based pressure measurements for easy and repeated use during BPA11. Serial balloon inflation using 2.0- to 4.0-mm semi- and noncompliant balloons with
serial dilations of undersized balloons to avoid vessel perforation/rupture and injury12. Selective use of sculpting or scoring balloons for fibrotic recalcitrant lesions13. Procedure conclusion when 3 to 5 diseased segments are treated during an initial
session, 400-ml IV contrast is administered, and/or 2-Gy exposure reached14. Overnight admission to a monitored bed/IMU
ACT ¼ activated clotting time; BNP ¼ B-type natriuretic peptide; BPA ¼ balloon pulmonary angioplasty;IMU ¼ intermediate care unit; IV ¼ intravenous; Pd/Pa ¼ mean distal to proximal arterial pressure ratio;UC ¼ University of California.
Mahmud et al. J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8
Chronic Thromboembolic Pulmonary Hypertension M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6
2478
MANAGEMENT OF INOPERABLE CTEPH
PAH-targeted therapies are widely used “off label” inthe treatment of CTEPH (Table 3). Retrospective datafrom a single center suggest that pre-treating patients
FIGURE 7 BPA of the Left Lower Lobe
The baseline and final left lower lobe A8 (lateral), A9 (middle), and A10
treatment session. All 3 segments were occluded and recanalized with 2
with PAH-targeted therapy had no impact on surgicaloutcomes but was associated with a delay in referralfor surgical evaluation (73). Efforts are currently un-derway to prospectively study the impact of “bridgingtherapy” or pre-treating patients with PAH therapiesbefore PTE.
Riociguat, a soluble guanylate cyclase stimulator,is the only therapy approved for inoperable CTEPH orpatients with persistent/recurrent pulmonary hyper-tension after PTE based on the results of the CHEST-1trial (Chronic Thromboembolic Pulmonary Hyper-tension Soluble Guanylate Cyclase–Stimulator Trial 1)(74). This was a 16-week multicenter, randomized,double-blind, placebo-controlled study of 261 pa-tients with either inoperable CTEPH (determined by apanel of expert CTEPH surgeons) or persistent/recurrent pulmonary hypertension following PTE.The riociguat group had significant improvement in6-min walk distance of 39 m versus a decrease of 6 min the placebo group (p < 0.001). The riociguat groupalso had a decrease in PVR, reduction in N-terminalprohormone B-type natriuretic peptide, andimprovement in World Health Organization func-tional class (74). A long-term extension study(CHEST-2 [BAY63-2521–Long-term Extension Study inPatients With Chronic Thromboembolic PulmonaryHypertension]) reported that these favorable resultspersisted to 1 year (75).
More recently, the endothelin receptor antagonist,macitentan, was studied in a Phase II randomized,placebo-controlled trial in 80 patients with
(medial) segment balloon pulmonary angioplasty (BPA) at a single
.0- to 4.0-mm diameter balloons.

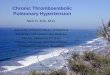
FIGURE 8 Exemplary BPA Procedure With Sequential Hemodynamic Assessment
Serial balloon pulmonary angioplasty (BPA) was performed in a right lower lobe A8 segment. An initial angiogram (top row, left image) showed diminished upper
branch distal perfusion and lower branch subtotal occlusion. Intravascular hemodynamics (bottom row) were notable for elevated baseline pulmonary artery (PA)
pressure (systolic >60 mm Hg, mean 35 to 40 mm Hg), significantly dampened distal pressure waveform (upper branch), and resting Pd/Pa ratio <0.50. BPA using
2.0-mm and 3.0-mm balloons resulted in immediately improved upper vessel perfusion by angiography (top row, right image) and intravascular hemodynamics (distal
pressure waveform and Pd/Pa >0.50). A repeat procedure 2 months later showed improved angiographic appearance of both A8 branches (middle row, left image),
PA pressure (systolic 50 mm Hg, mean <30 mm Hg), distal pressure waveform (systolic 20 to 25 mm Hg), and resting Pd/Pa >0.60. Repeat BPA using a 4.0-mm
balloon in both branches resulted in immediately improved distal pressure (systolic 25 to 30 mm Hg) and Pd/Pa >0.65. Final angiography following kissing balloon
inflation showed improved flow within both branches. Pd/Pa ¼ mean distal to proximal arterial pressure ratio (purple line).
J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8 Mahmud et al.M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6 Chronic Thromboembolic Pulmonary Hypertension
2479
inoperable CTEPH. In the macitentan-treated group,PVR decreased to 73.0% of baseline, whereas PVRdecreased to 87.2% of baseline (p ¼ 0.041) in theplacebo-treated group. At 24 weeks, 6-min walk
distance increased in the macitentan-treated groupby 35 m compared with an increase of only 1 m in theplacebo-treated group. Important distinctions mustbe made between the methods of this study and the

TABLE 5 BPA for CTEPH With Longer-Term (>12 Months) Outcomes
LocationFirst
Author (yrs) NTotal
ProceduresProcedures/
PatientReduction in
mPAP (mm Hg)Long-TermSurvival
Boston,MA
Feinstein (1994–1999) 18 47 2.6/patient 43.0 � 12.1 to33.7 � 10.2 (p ¼ 0.007)
89% at 34.2 months
Oslo,Norway
Andreassen (2003–2011) 20 73 3.7/patient 45 � 11 to33 � 10 (p < 0.001)
85% at 51 months
Okayama,Japan
Mizoguchi (2004–2011) 68 255 3.8/patient 45.4 � 9.6 to24.0 � 6.4 (p < 0.01)
97% at 2.2 � 1.4 yrs
Sendai,Japan
Sugimura (2009–2011) 12 — 5/patient 47.8 � 1.6 to24.8 � 4.9 (p < 0.01)
100% at 12 months
Aoki (2009–2016) 77 424 5.5/patient 38 � 10 to25 � 6 (p < 0.01)
98.4% at 5 yrs
Tokyo,Japan
Yanagisawa (2009–2013) 70 — 4/patient (<65 yrs)3/patient ($65 yrs)
42 to 26.0 (<65 yrs),41 to 23.5 ($65 yrs)(both p < 0.05)
100% (<65 yrs), 96.8%($65 yrs) at 12 months
Shimura (2009–2014) 110 423 3.8/patient 43 to 26 (p < 0.05) 100% at 1.97 yrs
Inami (2009–2016) 170 649 3.8/patient Values not available 98.8% at 1 yr98.0% at 3 yrs95.5% at 5 yrs
Multiple cities,Japan
Ogawa (2004–2016) 308 1,408 4.6/patient 43.2 � 11.0 to 24.3 � 6.4after BPA; 22.5 � 5.4 atfollow-up (p < 0.05)
96.8% at 1 to 2 yrs94.5% at 3 yrs
mPAP ¼ mean pulmonary artery pressure; other abbreviations as in Tables 1 and 4.
Mahmud et al. J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8
Chronic Thromboembolic Pulmonary Hypertension M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6
2480
CHEST-1 study. The MERIT (Macitentan for theTreatment of Inoperable Chronic ThromboembolicPulmonary Hypertension) study was smaller in size,included only patients who were inoperable, andpermitted the use of background PAH therapy (61% ofthe patients also using PDE-5 or oral/inhaled prosta-cyclin) (76).
BENEFIT (Bosentan Effects in iNopErable Forms ofchronIc Thromboembolic pulmonary hypertension), adouble-blind, randomized, placebo-controlled studyof the endothelin receptor antagonist, bosentan, ininoperable or persistent/recurrent pulmonary hyper-tension after PTE demonstrated a reduction in PVR by24% in the bosentan-treated group compared withplacebo (95% confidence interval: �31.5% to �16.0%;p < 0.0001) at 16 weeks (77). However, the trial failedto demonstrate a difference in 6-min walk distance at16 weeks, which was a coprimary endpoint. There isno obvious explanation for the differences observedin the outcomes between the BENEFIT and MERITtrials and could include trial size, design, and prop-erties of the specific endothelin receptor antagoniststudied. Other PAH-targeted therapies, includingprostacyclins and PDE-5 inhibitors, have shown somebenefits in small case-controlled studies or subgroupsof larger PAH randomized controlled trials (78–82).However, the subgroup of PTE patients pre-treatedwith PAH therapies had no significant advantageover those without medical therapy. Instead, themedically treated group had a significant time delayin referral for surgery compared with the rest.
PERCUTANEOUS INTERVENTIONAL THERAPY
Balloon pulmonary angioplasty (BPA), also known aspercutaneous transluminal pulmonary angioplasty,was initially studied as an alternative treatment forselected patients with inoperable CTEPH almost 2decades ago (83,84), but the approach was abandoneddue to the frequency of major complications. Over thepast 5 years, the procedure has undergone refinementwith promising outcomes and safety data fromvarious centers around the world. Contemporary BPAaims to disrupt organized, flow-limiting obstructionsand improve pulmonary vascular blood flow.Unlike coronary artery and peripheral vascular in-terventions, where symptomatic relief can be expe-rienced after revascularization of a single vessel,clinical improvement following BPA is typicallyobserved after revascularization of multiple diseasedsegments and regions. In recognition of the success ofBPA, the 2015 European Society of Cardiology/Euro-pean Respiratory Society guidelines for the diagnosisand treatment of pulmonary hypertension have rec-ommended BPA in CTEPH patients who are techni-cally inoperable or carry an unfavorable risk-benefitratio for PTE (recommendation Class IIb, Level ofEvidence: C) (25).
BPA has been performed in the majority ofpatients for symptomatic, inoperable CTEPH (85–93)or for persistent/recurrent pulmonary hypertensionfollowing PTE (94–96). Rescue BPA has also been re-ported as a transitional or bridging treatment option

J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8 Mahmud et al.M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6 Chronic Thromboembolic Pulmonary Hypertension
2481
in rapidly deteriorating CTEPH patients for stabiliza-tion before PTE (95,96). BPA can also be combinedwith PTE in selected CTEPH patients with surgicallyaccessible disease for one lung and inoperable diseaseaffecting the contralateral lung (97).
PATIENT SELECTION FOR BPA. BPA is still reservedfor patients with inoperable CTEPH. Because opera-bility assessment is complex and multifactorial, amultidisciplinary team approach consisting of pul-monary vascular medicine specialists, interventionalcardiologists, PTE surgical experts, and imaging spe-cialists is recommended for evaluating and identi-fying appropriate patients with CTEPH for BPA(Central Illustration). Surgical inoperability is acontentious issue and highly dependent on localsurgical expertise, patient comorbidities, proximalversus distal pulmonary segmental disease, and pa-tient preference (25). At experienced centers aroundthe world, segmental and subsegmental resection canbe performed to great effect, whereas at less experi-enced centers, resection may be limited to diseaselocated at the level of the main and lobar vessels.Once a patient has been deemed inoperable a sec-ondary assessment is made to determine if the pa-tient is suitable for BPA. Once again, an assessmentmust be made regarding the degree of observedvascular obstruction, hemodynamic impairment andsymptoms. In addition, assessment of the specificlesion types must be made as certain lesion typesconfer greater procedural risk and lower successrates (49).
TECHNIQUE OF BALLOON PULMONARY ANGIOPLASTY.
In the absence of a consistent and agreed upontechnique for the performance of BPA, we describethe approach undertaken at UC San Diego (Table 4). Acomplete treatment course usually involves 4 to 6separate BPA procedures, spaced apart by 3 to 7 days,and concluded by a final treatment in each lung.Target vessels are identified based on noninvasivelung perfusion scans with the goal to revascularizethe areas with the largest perfusion defects. Inter-mittent perfusion scans are repeated to observeoverall changes in lung perfusion from baseline andreprioritize diseased regions. Six-min walk tests areperformed at baseline and repeated at intervals tofollow the clinical response to treatment. Right heartcatheterization and hemodynamic measurementsbefore each BPA procedure monitor the cumulativeeffect of treatment on cardiopulmonary hemody-namics. Any single procedure is limited to no morethan 2 Gy of radiation exposure and/or 400 ml ofadministered contrast.
Target les ion character i zat ion . Characteristicpulmonary angiographic findings suggestive ofCTEPH include webs or bands, intimal irregularities,pouch defects, abrupt vascular narrowing, and com-plete obstruction of pulmonary arteries (48). How-ever, contemporary imaging modalities, includingintravascular ultrasound, optical coherence tomog-raphy, and CBCT have been used in CTEPH foradjunctive lesion characterization and BPA guidance(85,87,98,99). Webs and slit-like lesions in distalsegments are usually the main targets for the BPAprocedure. More severely obstructed lesions may alsobe approached provided antegrade or collateral flowpast the lesion is confirmed (99). At our center, theprimary anatomic imaging modality to identifyoptimal targets for BPA remains segmental pulmo-nary angiography.
To help avoid vascular injury, 0.014-inch work-horse guidewires with soft, atraumatic, spring-coiltips are used. Even when treating occluded vessels,using an atraumatic wire in conjunction with aballoon or microcatheter support and judicious use ofantegrade wire escalation with increased guidewiretip stiffness leads to the safest outcomes. Cautionshould be exercised in the use of polymer-jacketedguidewires because early experience for us andothers suggests increased risk of vascular injury andpulmonary hemorrhage (92). In general, our approachhas been to treat 1 to 2 pulmonary lobes in the samelung during any single BPA procedure.
The majority of distal pulmonary vascular lesionscan be initially treated using 2.0-mm diameter bal-loons, whereas proximal segment angioplasty isperformed with sequential balloon inflations usinglarger-diameter, noncompliant balloons typicallyranging between 2.5 and 4.0 mm (Figure 7). In someinstances, lesion modification using specialty de-vices such as the Chocolate (TriReme, Pleasanton,California) or AngioSculpt (Spectranetics, ColoradoSprings, Colorado) balloon catheters can be attemp-ted with prolonged balloon inflation, whereas moreaggressive approaches using cutting balloons oratherectomy catheters increase the risk of vesselinjury and should be avoided. Deployment ofcovered stents for catastrophic rupture is possible.Although data for long-term pulmonary arterypatency following BPA are limited, restenosis isconsidered uncommon (87), and stenting to preventrestenosis after balloon angioplasty is not recom-mended considering significant pulmonary vascularmobility during the respiratory cycle (85–87). How-ever, significant lesion recoil after balloon angio-plasty is occasionally observed and could potentially

Mahmud et al. J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8
Chronic Thromboembolic Pulmonary Hypertension M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6
2482
be addressed by a thin bioresorbable scaffolddeveloped for this vascular bed.Funct iona l assessment . Prediction of obstructivepulmonary artery disease is difficult by angiographyalone, and relatively normal-appearing vessels withinpulmonary segments underperfused by noninvasiveimaging warrant intravascular functional assessment(Figure 8). Measuring distal pressure using amicrocatheter-based manometer (Navvus Micro-Catheter, Acist, Eden Prairie, Minnesota) that can beadvanced over any guidewire is an effective strategy.There is no standardized protocol or numerical cut-point for pressure measurement or subsequent ther-apy. In 1 study, the BPA procedure was continuedwith the aim of achieving a mean distal to proximalarterial pressure ratio (Pd/Pa) >0.80 unless thebaseline mPAP was >35 mm Hg (100). Investigatorsreported a very low rate of procedure-related adverseevents using this strategy and were able to avoid RPEin the majority of patients. Our strategy has been touse a Pd/Pa ratio for treatment guidance withvalues <0.75 prompting additional balloon dilation(larger balloons, higher pressures, or scoring bal-loons/guidewires). Frequently, the ratio only changesmarginally and improves over time. Interval nonin-vasive perfusion scans between therapy sessions arealso useful to evaluate perfusion within treated seg-ments and support repeat intervention for areas withpersistent hypoperfusion.
COMPLICATIONS OF BPA. In recent series, BPAperiprocedural mortality ranged from 0% to 10% (85–93). The 2 most common complications of BPAinclude RPE and pulmonary vascular injury, with rareepisodes of vessel perforation/rupture. Despite theadvances and improvement of the procedure, RPEremains a frequent complication of BPA with anincidence as high as 53% to 60% as reported in someolder studies (86,87). Several factors associated withRPE following BPA include first procedure, severity ofbaseline pulmonary hypertension, and a high level ofplasma B-type natriuretic peptide (84,86). CTEPHpatients with underdeveloped bronchial arteries aremore likely to develop RPE following the BPA pro-cedure (101). Inami et al. (102), in a study of 150consecutive BPA procedures in CTEPH, proposed thePulmonary Edema Predictive Scoring Index as aproduct of PVR before BPA and the sum of changes inpulmonary flow grades with the procedure, to predictthe risk of RPE following BPA. In their study, thisscoring index was the strongest factor among studyvariables correlating with the occurrence of RPE (p <
0.0001) and was a marker of the risk of RPE (cutoffvalue 35.4, negative predictive value 92.3%).
The combined approach of pressure wire guidanceto measure gradients across stenosis and the Pulmo-nary Edema Predictive Scoring Index might be usefulin reducing the risk of RPE and vascular complica-tions (100). This approach to finishing each BPA ses-sion using the scoring index with the goal ofscores <35.4 and the guidance of pressure wire toachieve a distal mean pulmonary arterialpressure <35 mm Hg in each target lesion resulted insimilar hemodynamic improvements as BPA withoutthis guidance, but was associated with fewer numbersof BPA procedures and treated target lesions, andabsence of RPE. However, no definitive data exist tosupport this approach.
Pulmonary artery perforation/rupture is a seriouscomplication of BPA and is reported in 0% to 7% ofprocedures (86–88,103). Some measures suggestedto decrease the risk of pulmonary artery perforationinclude proper wire positioning, knuckle-wire tech-nique, appropriate balloon sizing, and avoidance ofoccluded segments without distal flow (99). Nonin-vasive positive-pressure ventilation with supple-mental oxygen, and in more severe situationsmechanical ventilation and extracorporeal mem-brane oxygenation, should be considered as the firsttherapeutic strategy for severe lung injury orvascular rupture following BPA to maintainoxygenation and preserve blood pressure (104).Immediate balloon tamponade of the perforated/ruptured vessel, cessation/reversal of anti-coagulation, covered stent implantation, Gelfoaminjection, and transcatheter coil embolization aresuggested bailout techniques in these situations(87,104).
CLINICAL OUTCOMES OF BPA. In the short term, theprocedure is associated with improvements in car-diopulmonary hemodynamics, pulmonary perfusion,exercise tolerance, World Health Organization func-tional class, and 6-min walk distance (85,87–90,105).Hemodynamic improvements, such as decrease inmPAP and PVR, are proportional to the number oftreated vessels (86–90). Pulmonary hypertensiondoes not resolve immediately during or following aBPA session, and it can take a few weeks to observethe positive impacts of the procedure (87–106).Studies have shown improvement in the quality oflife and symptom resolution disproportionate to thedegree of reduction in pulmonary hypertension (107).Although the available data on long-term outcomes ofBPA in CTEPH are limited (Table 5), persistence ofhemodynamic benefit (reduction in PVR and pulmo-nary artery pressure) of the BPA procedure at a me-dian of 2.8 years after procedural completion (91) has

J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8 Mahmud et al.M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6 Chronic Thromboembolic Pulmonary Hypertension
2483
been observed. Recently, cumulative data from 7centers in Japan for outcomes of over 308 inoperableCTEPH patients treated with BPA (from 2004 to 2016;1,408 procedures) was reported with 3-year survivalof 94.5%, and a 44% reduction in mPAP (43.2 �11.0 mm Hg to 24.3 � 6.4 mm Hg after final BPA) (93).Complications including pulmonary injury (17.8%),hemoptysis (14.0%), and pulmonary artery perfora-tion (2.9%) were not infrequent.
The initial experience at UC San Diego confirms theefficacy and safety of the procedure. Using the tech-nique described in this paper, we have treated 38patients (183 procedures) without any major compli-cations (0%) but procedure-related minor hemoptysisof 6.6%. In the 20 patients who have completed 1-yearfollow-up, we have observed improvement in func-tional class, a 26% reduction in mPAP (39.1 �8.9 mm Hg to 28.8 � 6.0 mm Hg) and 90% survival,with both deaths being unrelated to the BPA proced-ure. Although difference in patient selection andtechnique could be contributing to the differences inoutcomes between the various centers, it is clear thatthe technique is effective with short-term efficacyand long-term durability.
Improvement in right ventricular function hasbeen observed after BPA (103,108,109). Improvedhemodynamics after BPA may lead to right ventricu-lar reverse remodeling, improved systolic function,and reduced subclinical myocardial injury withreduced high-sensitivity troponin T level (110). Sec-ondary positive effects of BPA on renal function havealso been reported (111,112). A study of 9 CTEPH pa-tients with gradually deteriorated PVR at 4.1 (2.7 to7.9) years after PTE reported significant improvementin PVR of 4.2 (2.8 to 4.8) Wood units (p < 0.05) at 1.9(1.3 to 3.3) years after subsequent BPA procedure(s)(92). Safety and efficacy of the procedure has alsobeen demonstrated in elderly patients (age $65 years)compared with younger patients, with similar changeof hemodynamics, rate of periprocedural complica-tions, length of intensive care unit and in-hospitalstay, and all-cause mortality (113).
CONTEMPORARY TREATMENT STRATEGIES
FOR CTEPH
CTEPH is a disease that is underdiagnosed, and sur-gical PTE remains the preferred therapy. However,determination of operability can be challenging, re-quires an expert team, and availability of surgicalexpertise is limited. There is growing excitement forthe percutaneous treatment of inoperable CTEPHwith data from multiple centers around the world
showing the clinical feasibility of BPA for the treat-ment of CTEPH. Riociguat remains the only approvedmedical therapy and is an important adjunct fortreatment in patients deemed inoperable or withpersistent pulmonary hypertension after PTE.
In order for this disease to be appropriatelytreated, we recommend that expert CTEPH teamsincluding surgical specialists be developed at indi-vidual institutions. It is our opinion that BPA beoffered at CTEPH centers as a part of a multidisci-plinary approach to treatment decisions. Addition-ally, optimal and standardized techniques for BPAneed to be developed along with dedicated inter-ventional equipment and appropriate training stan-dards. The majority of interventional outcomes datahave been self-reported without adjudication, withheterogeneous techniques and paucity of long-termoutcomes. In order to adequately evaluate the suc-cess of this procedure as compared with surgicalendarterectomy, more rigorous and standardizeddata collection are required. The cumulative benefitand adverse effect of multiple procedures, especiallyon patient radiation exposure and renal contrasteffects, must be determined. A multicenter evalua-tion with objective adjudication for short-term suc-cess along with evaluation of long-term outcomes ofBPA are required before true equipoise can beestablished for randomized comparisons of BPAversus PTE for patients with segmental/sub-segmental CTEPH. In the meantime, the percuta-neous revascularization option is appropriate forpatients deemed inoperable in combination withtargeted medical therapy, or those who have failedto benefit from surgery. Whether BPA could poten-tially allow for discontinuation of targeted medicaltherapy is unknown and should be carefully studied.The ongoing RACE trial (Riociguat Versus BalloonPulmonary Angioplasty in Non-operable ChronicthromboEmbolic Pulmonary Hypertension;NCT02634203) is addressing the question of thecomparative benefit of riociguat versus BPA forinoperable CTEPH, and its results are eagerlyawaited.
CONCLUSIONS
There have been remarkable improvements in treat-ment options for CTEPH patients over the pastdecade. PTE remains the only definitive and poten-tially curative therapy. Recent advancements in sur-gical techniques and instruments now allow distalendarterectomy, making surgery the treatment ofchoice even in patients with segmental or distal

Mahmud et al. J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8
Chronic Thromboembolic Pulmonary Hypertension M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6
2484
disease. On the basis of positive randomized clinicaltrial data, we also have targeted medical therapy tofill an unmet need for those deemed inoperable.Furthermore, BPA with the introduction of newtechniques and technologies now offers an alterna-tive interventional treatment to PTE for select CTEPHpatients not amenable to surgery. However, despitethe recent advances with BPA, there is no standardtechnique for global adoption, and patient selectionremains a significant challenge. We still lack adequateprospective long-term data after BPA, which high-lights the need for future registries and carefullyconducted studies to determine the safety, efficacy,and durability of the procedure.
Due to these uncertainties, and with the evolvingmanagement approaches, CTEPH patients should bereferred to an advanced center experienced in theevaluation and care of this unique patient population.The optimal treatment for any CTEPH patient re-quires a comprehensive review by a multidisciplinaryteam capable of providing all current treatmentmodalities.
ADDRESS FOR CORRESPONDENCE: Dr. EhtishamMahmud, University of California San Diego, SulpizioCardiovascular Center, 9434 Medical Center Drive, LaJolla, California 92037. E-mail: [email protected]: @UCSDHealth.
RE F E RENCE S
1. Lang IM, Pesavento R, Bonderman D, Yuan JX.Risk factors and basic mechanisms of chronicthromboembolic pulmonary hypertension: a cur-rent understanding. Eur Respir J 2013;41:462–8.
2. Ende-Verhaar YM, Cannegieter SC, VonkNoordegraaf A, et al. Incidence of chronic throm-boembolic pulmonary hypertension after pulmo-nary embolism: a contemporary view of thepublished literature. Eur Respir J 2017;49:1601792.
3. Galie N, Hoeper MM, Humbert M, et al. Guide-lines for the diagnosis and treatment of pulmonaryhypertension: the Task Force for the Diagnosis andTreatment of Pulmonary Hypertension of the Eu-ropean Society of Cardiology (ESC) and the Euro-pean Respiratory Society (ERS). Eur Heart J 2009;30:2493–537.
4. Pengo V, Lensing AW, Prins MH, et al. Incidenceof chronic thromboembolic pulmonary hyperten-sion after pulmonary embolism. N Engl J Med2004;350:2257–64.
5. Becattini C, Agnelli G, Pesavento R, et al. Inci-dence of chronic thromboembolic pulmonary hy-pertension after a first episode of pulmonaryembolism. Chest 2006;130:172–5.
6. Dentali F, Donadini M, Gianni M, et al. Incidenceof chronic pulmonary hypertension in patientswith previous pulmonary embolism. Thromb Res2009;124:256–8.
7. Gall H, Hoeper MM, Richter MJ, et al. Anepidemiological analysis of the burden of chronicthromboembolic pulmonary hypertension in theUSA, Europe and Japan. Eur Respir Rev 2017;26:160121.
8. Korkmaz A, Ozlu T, Ozsu S, Kazaz Z, Bulbul Y.Long-term outcomes in acute pulmonary throm-boembolism: the incidence of chronic thrombo-embolic pulmonary hypertension and associatedrisk factors. Clin Appl Thromb Hemost 2012;18:281–8.
9. Guerin L, Couturaud F, Parent F, et al. Preva-lence of chronic thromboembolic pulmonary hy-pertension after acute pulmonary embolism.Prevalence of CTEPH after pulmonary embolism.Thromb Haemost 2014;112:598–605.
10. Fedullo PF, Auger WR, Kerr KM, Rubin LJ.Chronic thromboembolic pulmonary hypertension.N Engl J Med 2001;345:1465–72.
11. Bonderman D, Turecek PL, Jakowitsch J, et al.High prevalence of elevated clotting factor VIII inchronic thromboembolic pulmonary hypertension.Thromb Haemost 2003;90:372–6.
12. Auger WR, Permpikul P, Moser KM. Lupusanticoagulant, heparin use, and thrombocytopeniain patients with chronic thromboembolic pulmo-nary hypertension: a preliminary report. Am J Med1995;99:392–6.
13. Wolf M, Boyer-Neumann C, Parent F, et al.Thrombotic risk factors in pulmonary hyperten-sion. Eur Respir J 2000;15:395–9.
14. Morris TA, Marsh JJ, Chiles PG, Auger WR,Fedullo PF, Woods VL Jr. Fibrin derived from pa-tients with chronic thromboembolic pulmonaryhypertension is resistant to lysis. Am J Respir CritCare Med 2006;173:1270–5.
15. Egermayer P, Peacock AJ. Is pulmonary em-bolism a common cause of chronic pulmonaryhypertension? Limitations of the embolic hypoth-esis. Eur Respir J 2000;15:440–8.
16. Fedullo PF, Rubin LJ, Kerr KM, Auger WR,Channick RN. The natural history of acute andchronic thromboembolic disease: the search forthe missing link. Eur Respir J 2000;15:435–7.
17. Quarck R, Wynants M, Verbeken E, Meyns B,Delcroix M. Contribution of inflammation andimpaired angiogenesis to the pathobiology ofchronic thromboembolic pulmonary hypertension.Eur Respir J 2015;46:431–43.
18. Zabini D, Heinemann A, Foris V, et al.Comprehensive analysis of inflammatory markersin chronic thromboembolic pulmonary hyperten-sion patients. Eur Respir J 2014;44:951–62.
19. Quarck R, Nawrot T, Meyns B, Delcroix M.C-reactive protein: a new predictor of adverseoutcome in pulmonary arterial hypertension. J AmColl Cardiol 2009;53:1211–8.
20. Langer F, Schramm R, Bauer M, Tscholl D,Kunihara T, Schafers HJ. Cytokine response topulmonary thromboendarterectomy. Chest 2004;126:135–41.
21. Jais X, Ioos V, Jardim C, et al. Splenectomy andchronic thromboembolic pulmonary hypertension.Thorax 2005;60:1031–4.
22. Bonderman D, Skoro-Sajer N, Jakowitsch J,et al. Predictors of outcome in chronic thrombo-embolic pulmonary hypertension. Circulation2007;115:2153–8.
23. Bonderman D, Wilkens H, Wakounig S, et al.Risk factors for chronic thromboembolic pulmo-nary hypertension. Eur Respir J 2009;33:325–31.
24. Kim NH, Delcroix M, Jenkins DP, et al. Chronicthromboembolic pulmonary hypertension. J AmColl Cardiol 2013;62:D92–9.
25. Galiè N, Humbert M, Vachiery JL, et al. 2015ESC/ERS guidelines for the diagnosis and treat-ment of pulmonary hypertension: the Joint TaskForce for the Diagnosis and Treatment of Pulmo-nary Hypertension of the European Society ofCardiology (ESC) and the European RespiratorySociety (ERS). Eur Heart J 2016;37:67–119.
26. Lang IM, Madani M. Update on chronicthromboembolic pulmonary hypertension. Circu-lation 2014;130:508–18.
27. Pepke-Zaba J, Delcroix M, Lang I, et al. Chronicthromboembolic pulmonary hypertension(CTEPH): results from an international prospectiveregistry. Circulation 2011;124:1973–81.
28. Morris TA, Auger WR, Ysrael MZ, et al.Parenchymal scarring is associated with restrictivespirometric defects in patients with chronicthromboembolic pulmonary hypertension. Chest1996;110:399–403.
29. Wakamatsu K, Inoue H, Aizawa H,Mitsuyama T, Tsuda H, Hara N. Recurrent chestopacities in a patient with thromboembolic pul-monary hypertension. Respiration 1998;65:492–4.
30. Steenhuis LH, Groen HJ, Koeter GH, van derMark TW. Diffusion capacity and haemodynamicsin primary and chronic thromboembolic pulmonaryhypertension. Eur Respir J 2000;16:276–81.
31. Raisinghani A, Ben-Yehuda O. Echocardiogra-phy in chronic thromboembolic pulmonary hy-pertension. Semin Thorac Cardiovasc Surg 2006;18:230–5.

J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8 Mahmud et al.M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6 Chronic Thromboembolic Pulmonary Hypertension
2485
32. Gopalan D, Blanchard D, Auger WR. Diagnosticevaluation of chronic thromboembolic pulmonaryhypertension. Ann Am Thorac Soc 2016;13 Suppl 3:S222–39.
33. Tunariu N, Gibbs SJ, Win Z, et al. Ventilation-perfusion scintigraphy is more sensitive thanmultidetector CTPA in detecting chronic throm-boembolic pulmonary disease as a treatable causeof pulmonary hypertension. J Nucl Med 2007;48:680–4.
34. McLaughlin VV, Langer A, Tan M, et al.Contemporary trends in the diagnosis and man-agement of pulmonary arterial hypertension: aninitiative to close the care gap. Chest 2013;143:324–32.
35. Hasegawa I, Boiselle PM, Hatabu H. Bronchialartery dilatation on MDCT scans of patients withacute pulmonary embolism: comparison withchronic or recurrent pulmonary embolism. AJR AmJ Roentgenol 2004;182:67–72.
36. King MA, Ysrael M, Bergin CJ. Chronic throm-boembolic pulmonary hypertension: CT findings.AJR Am J Roentgenol 1998;170:955–60.
37. Giannouli E, Maycher B. Imaging techniques inchronic thromboembolic pulmonary hypertension.Curr Opin Pulm Med 2013;19:562–74.
38. Pena E, Dennie C. Acute and chronic pulmo-nary embolism: an in-depth review for radiologiststhrough the use of frequently asked questions.Semin Ultrasound CT MR 2012;33:500–21.
39. Sugiura T, Tanabe N, Matsuura Y, et al. Role of320-slice CT imaging in the diagnostic workup ofpatients with chronic thromboembolic pulmonaryhypertension. Chest 2013;143:1070–7.
40. Sugiyama M, Fukuda T, Sanda Y, et al. Orga-nized thrombus in pulmonary arteries in patientswith chronic thromboembolic pulmonary hyper-tension; imaging with cone beam computed to-mography. Jpn J Radiol 2014;32:375–82.
41. Scarfe WC, Farman AG, Sukovic P. Clinical ap-plications of cone-beam computed tomography indental practice. J Can Dent Assoc 2006;72:75–80.
42. Kreitner KF, Kunz RP, Ley S, et al. Chronicthromboembolic pulmonary hypertension -assessment by magnetic resonance imaging. EurRadiol 2007;17:11–21.
43. Abolmaali N, Seitz U, Esmaeili A, et al. Evalu-ation of a resistance-based model for the quanti-fication of pulmonary arterial hypertension usingMR flow measurements. J Magn Reson Imaging2007;26:646–53.
44. Roeleveld RJ, Marcus JT, Faes TJ, et al.Interventricular septal configuration at MR imag-ing and pulmonary arterial pressure in pulmonaryhypertension. Radiology 2005;234:710–7.
45. Ley S, Ley-Zaporozhan J, Pitton MB, et al.Diagnostic performance of state-of-the-art imag-ing techniques for morphological assessment ofvascular abnormalities in patients with chronicthromboembolic pulmonary hypertension(CTEPH). Eur Radiol 2012;22:607–16.
46. Nicod P, Peterson K, Levine M, et al. Pulmo-nary angiography in severe chronic pulmonaryhypertension. Ann Intern Med 1987;107:565–8.
47. Kovacs G, Berghold A, Scheidl S, Olschewski H.Pulmonary arterial pressure during rest and
exercise in healthy subjects: a systematic review.Eur Respir J 2009;34:888–94.
48. Auger WR, Fedullo PF, Moser KM,Buchbinder M, Peterson KL. Chronic major-vesselthromboembolic pulmonary artery obstruction:appearance at angiography. Radiology 1992;182:393–8.
49. Kawakami T, Ogawa A, Miyaji K, et al. Novelangiographic classification of each vascular lesionin chronic thromboembolic pulmonary hyperten-sion based on selective angiogram and results ofballoon pulmonary angioplasty. Circ CardiovascInterv 2016;9:e003318.
50. Madani MM, Auger WR, Pretorius V, et al.Pulmonary endarterectomy: recent changes in asingle institution’s experience of more than 2,700patients. Ann Thorac Surg 2012;94:97–103.
51. Jamieson SW, Kapelanski DP. Pulmonary end-arterectomy. Curr Probl Surg 2000;37:165–252.
52. Madani MM, Jamieson SW. Pulmonary endar-terectomy for chronic thromboembolic disease.Oper Tech Thorac Cardiovasc Surg 2006;11:264–74.
53. Jenkins DP, Madani M, Mayer E, et al. Surgicaltreatment of chronic thromboembolic pulmonaryhypertension. Eur Respir J 2013;41:735–42.
54. Jamieson SW, Auger WR, Fedullo PF, et al.Experience and results with 150 pulmonarythromboendarterectomy operations over a 29-month period. J Thorac Cardiovasc Surg 1993;106:116–26.
55. Thistlethwaite PA, Kaneko K, Madani MM,Jamieson SW. Technique and outcomes of pul-monary endarterectomy surgery. Ann Thorac Car-diovasc Surg 2008;14:274–82.
56. Fedullo P, Kerr KM, Kim NH, Auger WR.Chronic thromboembolic pulmonary hypertension.Am J Respir Crit Care Med 2011;183:1605–13.
57. Mayer E, Jenkins D, Lindner J, et al. Surgicalmanagement and outcome of patients withchronic thromboembolic pulmonary hypertension:results from an international prospective registry.J Thorac Cardiovasc Surg 2011;141:702–10.
58. Dartevelle P, Fadel E, Mussot S, et al. Chronicthromboembolic pulmonary hypertension. EurRespir J 2004;23:637–48.
59. Thistlethwaite PA, Kemp A, Du L, Madani MM,Jamieson SW. Outcomes of pulmonary endarter-ectomy for treatment of extreme thromboembolicpulmonary hypertension. J Thorac Cardiovasc Surg2006;131:307–13.
60. Levinson RM, Shure D, Moser KM. Reperfusionpulmonary edema after pulmonary artery throm-boendarterectomy. Am Rev Respir Dis 1986;134:1241–5.
61. Lee KC, Cho YL, Lee SY. Reperfusion pulmo-nary edema after pulmonary endarterectomy. ActaAnaesthesiol Sin 2001;39:97–101.
62. Kerr KM, Auger WR, Marsh JJ, et al. Efficacy ofmethylprednisolone in preventing lung injuryfollowing pulmonary thromboendarterectomy.Chest 2012;141:27–35.
63. Macchiarini P, Kamiya H, Hagl C, et al. Pul-monary endarterectomy for chronic thromboem-bolic pulmonary hypertension: is deep
hypothermia required? Eur J Cardiothorac Surg2006;30:237–41.
64. Mikus PM, Mikus E, Martin-Suarez S, et al.Pulmonary endarterectomy: an alternative to cir-culatory arrest and deep hypothermia: mid-termresults. Eur J Cardiothorac Surg 2008;34:159–63.
65. Vuylsteke A, Sharples L, Charman G, et al.Circulatory arrest versus cerebral perfusion duringpulmonary endarterectomy surgery (PEACOG): arandomised controlled trial. Lancet 2011;378:1379–87.
66. Ogino H, Ando M, Matsuda H, et al. Japanesesingle-center experience of surgery for chronicthromboembolic pulmonary hypertension. AnnThorac Surg 2006;82:630–6.
67. Corsico AG, D’Armini AM, Cerveri I, et al. Long-term outcome after pulmonary endarterectomy.Am J Respir Crit Care Med 2008;178:419–24.
68. Freed DH, Thomson BM, Berman M, et al.Survival after pulmonary thromboendarterectomy:effect of residual pulmonary hypertension.J Thorac Cardiovasc Surg 2011;141:383–7.
69. Ishida K, Masuda M, Tanabe N, Matsumiya G,Tatsumi K, Nakajima N. Long-term outcome afterpulmonary endarterectomy for chronic thrombo-embolic pulmonary hypertension. J Thorac Car-diovasc Surg 2012;144:321–6.
70. Saouti N, Morshuis WJ, Heijmen RH,Snijder RJ. Long-term outcome after pulmonaryendarterectomy for chronic thromboembolic pul-monary hypertension: a single institution experi-ence. Eur J Cardiothorac Surg 2009;35:947–52.
71. Cannon JE, Su L, Kiely DG, et al. Dynamic riskstratification of patient long-term outcome afterpulmonary endarterectomy: results from theUnited Kingdom national cohort. Circulation 2016;133:1761–71.
72. D’Armini AM, Zanotti G, Ghio S, et al. Reverseright ventricular remodeling after pulmonaryendarterectomy. J Thorac Cardiovasc Surg 2007;133:162–8.
73. Jensen KW, Kerr KM, Fedullo PF, et al. Pul-monary hypertensive medical therapy in chronicthromboembolic pulmonary hypertension beforepulmonary thromboendarterectomy. Circulation2009;120:1248–54.
74. Ghofrani HA, D’Armini AM, Grimminger F,et al. Riociguat for the treatment of chronicthromboembolic pulmonary hypertension. N EnglJ Med 2013;369:319–29.
75. Simonneau G, D’Armini AM, Ghofrani HA, et al.Riociguat for the treatment of chronic thrombo-embolic pulmonary hypertension: a long-termextension study (CHEST-2). Eur Respir J 2014;45:1293–302.
76. Ghofrani HA, Simonneau G, D’Armini AM, et al.Macitentan for the treatment of inoperablechronic thromboembolic pulmonary hypertension(MERIT-1): results from the multicentre, phase 2,randomised, double-blind, placebo-controlledstudy. Lancet Respir Med 2017;5:785–94.
77. Jais X, D’Armini AM, Jansa P, et al. Bosentanfor treatment of inoperable chronic thromboem-bolic pulmonary hypertension: BENEFiT (BosentanEffects in iNopErable Forms of chronIc Thrombo-embolic pulmonary hypertension), a randomized,

Mahmud et al. J A C C V O L . 7 1 , N O . 2 1 , 2 0 1 8
Chronic Thromboembolic Pulmonary Hypertension M A Y 2 9 , 2 0 1 8 : 2 4 6 8 – 8 6
2486
placebo-controlled trial. J Am Coll Cardiol 2008;52:2127–34.
78. Becattini C, Manina G, Busti C, Gennarini S,Agnelli G. Bosentan for chronic thromboembolicpulmonary hypertension: findings from a system-atic review and meta-analysis. Thromb Res 2010;126:e51–6.
79. Suntharalingam J, Treacy CM, Doughty NJ,et al. Long-term use of sildenafil in inoperablechronic thromboembolic pulmonary hypertension.Chest 2008;134:229–36.
80. Cabrol S, Souza R, Jais X, et al. Intravenousepoprostenol in inoperable chronic thromboem-bolic pulmonary hypertension. J Heart LungTransplant 2007;26:357–62.
81. Olschewski H, Simonneau G, Galiè N, et al.Inhaled iloprost for severe pulmonary hyperten-sion. N Engl J Med 2002;347:322–9.
82. Skoro-Sajer N, Bonderman D, Wiesbauer F,et al. Treprostinil for severe inoperable chronicthromboembolic pulmonary hypertension.J Thromb Haemost 2007;5:483–9.
83. Voorburg JA, Cats VM, Buis B, Bruschke AV.Balloon angioplasty in the treatment of pulmonaryhypertension caused by pulmonary embolism.Chest 1988;94:1249–53.
84. Feinstein JA, Goldhaber SZ, Lock JE,Ferndandes SM, Landzberg MJ. Balloon pulmonaryangioplasty for treatment of chronic thromboem-bolic pulmonary hypertension. Circulation 2001;103:10–3.
85. Sugimura K, Fukumoto Y, Satoh K, et al.Percutaneous transluminal pulmonary angioplastymarkedly improves pulmonary hemodynamics andlong-term prognosis in patients with chronicthromboembolic pulmonary hypertension. Circ J2012;76:485–8.
86. Kataoka M, Inami T, Hayashida K, et al.Percutaneous transluminal pulmonary angioplastyfor the treatment of chronic thromboembolicpulmonary hypertension. Circ Cardiovasc Interv2012;5:756–62.
87. Mizoguchi H, Ogawa A, Munemasa M,Mikouchi H, Ito H, Matsubara H. Refined balloonpulmonary angioplasty for inoperable patientswith chronic thromboembolic pulmonary hyper-tension. Circ Cardiovasc Interv 2012;5:748–55.
88. Andreassen AK, Ragnarsson A, Gude E,Geiran O, Andersen R. Balloon pulmonary angio-plasty in patients with inoperable chronic throm-boembolic pulmonary hypertension. Heart 2013;99:1415–20.
89. Inami T, Kataoka M, Ando M, Fukuda K,Yoshino H, Satoh T. A new era of therapeuticstrategies for chronic thromboembolic pulmonaryhypertension by two different interventionaltherapies; pulmonary endarterectomy and percu-taneous transluminal pulmonary angioplasty. PLoSOne 2014;9:e94587.
90. Taniguchi Y, Miyagawa K, Nakayama K, et al.Balloon pulmonary angioplasty: an additionaltreatment option to improve the prognosis ofpatients with chronic thromboembolic pulmonaryhypertension. EuroIntervention 2014;10:518–25.
91. Inami T, Kataoka M, Yanagisawa R, et al. Long-term outcomes after percutaneous transluminalpulmonary angioplasty for chronic thromboem-bolic pulmonary hypertension. Circulation 2016;134:2030–2.
92. Olsson KM, Wiedenroth CB, Kamp JC, et al.Balloon pulmonary angioplasty for inoperablepatients with chronic thromboembolic pulmonaryhypertension: the initial German experience. EurRespir J 2017;49:1602409.
93. Ogawa A, Satoh T, Fukuda T, et al. Balloonpulmonary angioplasty for chronic thromboem-bolic pulmonary hypertension: results of a multi-center registry. Circ Cardiovasc Qual Outcomes2017;10:e004029.
94. Shimura N, Kataoka M, Inami T, et al. Addi-tional percutaneous transluminal pulmonary an-gioplasty for residual or recurrent pulmonaryhypertension after pulmonary endarterectomy. IntJ Cardiol 2015;183:138–42.
95. Tsuji A, Ogo T, Demachi J, et al. Rescueballoon pulmonary angioplasty in a rapidlydeteriorating chronic thromboembolic pulmonaryhypertension patient with liver failure andrefractory infection. Pulm Circ 2014;4:142–7.
96. Nakamura M, Sunagawa O, Tsuchiya H, et al.Rescue balloon pulmonary angioplasty underveno-arterial extracorporeal membrane oxygena-tion in a patient with acute exacerbation of chronicthromboembolic pulmonary hypertension. IntHeart J 2015;56:116–20.
97. Wiedenroth CB, Liebetrau C, Breithecker A,et al. Combined pulmonary endarterectomy andballoon pulmonary angioplasty in patients withchronic thromboembolic pulmonary hypertension.J Heart Lung Transplant 2016;35:591–6.
98. Tatebe S, Fukumoto Y, Sugimura K, et al.Optical coherence tomography as a novel diag-nostic tool for distal type chronic thromboembolicpulmonary hypertension. Circ J 2010;74:1742–4.
99. Ogo T. Balloon pulmonary angioplasty forinoperable chronic thromboembolic pulmonaryhypertension. Curr Opin Pulm Med 2015;21:425–31.
100. Inami T, Kataoka M, Shimura N, et al. Pres-sure-wire-guided percutaneous transluminalpulmonary angioplasty: a breakthrough incatheter-interventional therapy for chronicthromboembolic pulmonary hypertension. J AmColl Cardiol Intv 2014;7:1297–306.
101. Takei M, Kataoka M, Kawakami T, Yamada Y,Yamada M, Fukuda K. Under-developed bronchialarteries as a risk factor for complications inballoon pulmonary angioplasty. Int J Cardiol 2016;203:1016–7.
102. Inami T, Kataoka M, Shimura N, et al. Pul-monary edema predictive scoring index (PEPSI), anew index to predict risk of reperfusion pulmonaryedema and improvement of hemodynamics inpercutaneous transluminal pulmonary angio-plasty. J Am Coll Cardiol Intv 2013;6:725–36.
103. Fukui S, Ogo T, Morita Y, et al. Right ven-tricular reverse remodeling after balloon pulmo-nary angioplasty. Eur Respir J 2014;43:1394–402.
104. Hosokawa K, Abe K, Oi K, Mukai Y, Hirooka Y,Sunagawa K. Balloon pulmonary angioplasty-related complications and therapeutic strategy inpatients with chronic thromboembolic pulmonaryhypertension. Int J Cardiol 2015;197:224–6.
105. Fukui S, Ogo T, Goto Y, et al. Exerciseintolerance and ventilatory inefficiency improveearly after balloon pulmonary angioplasty inpatients with inoperable chronic thromboembolicpulmonary hypertension. Int J Cardiol 2015;180:66–8.
106. Hosokawa K, Abe K, Oi K, Mukai Y, Hirooka Y,Sunagawa K. Negative acute hemodynamicresponse to balloon pulmonary angioplasty doesnot predicate the long-term outcome in patientswith chronic thromboembolic pulmonary hyper-tension. Int J Cardiol 2015;188:81–3.
107. Darocha S, Pietura R, Pietrasik A, et al.Improvement in quality of life andhemodynamics inchronic thromboembolic pulmonary hypertensiontreated with balloon pulmonary angioplasty. Circ J2017;81:552–7.
108. Tsugu T, Murata M, Kawakami T, et al. Sig-nificance of echocardiographic assessment forright ventricular function after balloon pulmonaryangioplasty in patients with chronic thromboem-bolic induced pulmonary hypertension. Am J Car-diol 2015;115:256–61.
109. Broch K, Murbraech K, Ragnarsson A, et al.Echocardiographic evidence of right ventricularfunctional improvement after balloon pulmonaryangioplasty in chronic thromboembolic pulmonaryhypertension. J Heart Lung Transplant 2016;35:80–6.
110. Kimura M, Kohno T, Kawakami T, et al.Balloon pulmonary angioplasty attenuatesongoing myocardial damage in patients withchronic thromboembolic pulmonary hypertension.Int J Cardiol 2016;207:387–9.
111. Kimura M, Kataoka M, Kawakami T, Inohara T,Takei M, Fukuda K. Balloon pulmonary angioplastyusing contrast agents improves impaired renalfunction in patients with chronic thromboembolicpulmonary hypertension. Int J Cardiol 2015;188:41–2.
112. Inami T, Kataoka M, Ishiguro H, et al. Percu-taneous transluminal pulmonary angioplasty forchronic thromboembolic pulmonary hypertensionwith severe right heart failure. Am J Respir CritCare Med 2014;189:1437–9.
113. Yanagisawa R, Kataoka M, Inami T, et al.Safety and efficacy of percutaneous transluminalpulmonary angioplasty in elderly patients. Int JCardiol 2014;175:285–9.
KEY WORDS balloon pulmonaryangioplasty, BPA, chronic thromboembolicpulmonary hypertension, CTEPH, PTE,pulmonary thromboendarterectomy
APPENDIX For a supplemental video andits legend, please see the online version of thispaper.