Embed Size (px)
Citation preview

Brit. J. Ophthal. (1976) 6o, 419
Cilio-retinal infarction after retinal vein occlusion
D. McLEOD AND C. P. RING*From Moorfields Eye Hospital, London
Cilio-retinal arterioles are branches of the posteriorciliary arteries which supply areas of inner retinacontiguous with the optic disc in about 20 per centof individuals (Hayreh, I963a). The cilio-retinalterritory is spared from ischaemic necrosis afterocclusion of the central retinal artery, whileinfarction of retina supplied by cilio-retinalarterioles may accompany ischaemic swelling ofthe disc when the posterior ciliary arteries areoccluded in temporal arteritis (Hayreh, i969).Only two cases of retinal infarction in the cilio-
retinal distribution have so far been described inassociation with occlusion of the central retinalvein (Oosterhuis, I968; Hayreh, 197I), althoughsuch cases are not rare. The purpose of this paperis to present a series of Io further cases togetherwith a case of cilio-retinal infarction associatedwith a hemisphere branch retinal vein occlusion.The interrelationships between retinal vein occlu-sion and impaired posterior ciliary perfusion arediscussed in the light of our findings.
*Supported by the Prevention of Blindness Research Fund
Address for reprints: D. McLeod, FRCS, Moorfields Eye Hospital,City Road, London ECIV 2PD
Patients and methodsThe i I patients were drawn from the ophthalmicpractice in Moorfields Eye Hospital (MEH), StThomas's Hospital (STH), the Edinburgh RoyalInfirmary (ERI), and the National Hospital, QueenSquare (NHQS) (Table). Six patients were observedpersonally by one or other of us, while in the remainingcases we referred to case records and photographs.Fluorescein angiography was performed by the routinetechnique of the department concemed, in whichio or 20 per cent fluorescein solution was injected intoan antecubital vein. Photographs were generally takenat intervals of one second during the initial dye transit,using a Zeiss (Oberkochen) fundus camera. In all casesthe initial photographic assessment was carried outwithin two weeks of the onset of symptoms and in sevencases within three days of visual loss. A medical exami-nation and systemic investigation were carried out inmost patients but were not standardized. Similarly,visual fields were tested by a variety of routine clinicaltechniques.
ResultsCENTRAL RETINAL VEIN OCCLUSION (Cases i-io)
The patients noticed sudden visual deterioration inone eye, and several complained specifically of a
Table Particulars of i I cases of cilio-retinal infarction
Source
STHMEH
MEHMEHSTHERIMEHMEHMEH
Age(years)
3579
4'695052753269
Sex
MaleFemale
FemaleMaleMaleFemaleFemaleMaleFemale
No. ofcilio-retinalarterioles
3I
2
42
4
2
2
2
NHQS 69 Female 3
5 MEH 39 Female 2
Eye
LeftRight
RightLeftRightRightRightLeftRight
Visual acuity
At onset At one year
6/6o 6/4CF PL
6/24CF6/6o6/i86/246/i8CF
6/6CF6/I2
6/4PL6/9CF
Right 6/6o 6/i8Left 6/I8 6/12
Systemicdisease
Cerebrovascularinsufficiency
Migraine
Angina pectoris
Hypertension(on treatment)
Arteriosclerosis
* Fig. 4 in McLeod (1g97b); t Fig. I in McLeod (1975a); t Fig. 6 in McLeod (I976)CF = counting fingers; PL = perception of light
Fig.no.
2
Case10.
2
3
45
6789
I0
I I
34
t
I:
Bloodpressure(mmHg)
120/90190/100
140/80120/70I I/070110/70I 60/go110/90170/I00
I30/80150/90
on January 8, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.60.6.419 on 1 June 1976. Dow
nloaded from

420 British Jouirnal of Ophthalmology
(Ia) eIhb)_ r- _~~~5
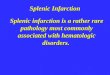
(IC) (Od)FIG. I Case i. (a) Fundus photograph i o days after visual loss: retinal infarction in cilio-retinal territories.(b) Fluorescein angiogram (same study as (a)): early arterio-venous phase, larger cilio-retinal arteriole (arrow) hasfilled. (c) Fluorescein angiogram (same study as (a)): late phase, dye leakage from disc and veins. (d) Fluoresceinangiogram seven months later: early arterio-venous phase, delayed peripapillary choroidal filling
localized scotoma in the central field of vision.Pre-existing ocular lesions had been discovered inonly one patient (case 2), who was known to havehad bilateral preretinal macular fibrosis for six years.
matory signs in the aqueous or anterior vitreous.Apart from a single patient with mild chronicglaucoma (case 9), the intraocular pressure wasnormal in each eye, though the pressure in theaffected eye was generally 2-4 mmHg less than that
Anterior segment in its teiiuw.
On presentation there was no significant abnor-mality in the anterior segment or ocular media of Presenting fundus signsany patient; in particular, there were no inflam- Funduscopy showed widespread retinal haemorr-
on January 8, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.60.6.419 on 1 June 1976. Dow
nloaded from

Cilio-retinal infarction 42I
hages (including blot haemorrhages anterior to theequator) together with distension and tortuosity ofall tributaries of the central retinal vein (Fig. i).Some patients showed occasional perivenous cotton-wool spots or retinal oedema, especially at themacula.
In addition to signs of central vein occlusion,retinal pallor was seen contiguous with the opticdisc, and parts of the periphery of these areasshowed an intense whiteness. The clinical appear-ance was that of ischaemic cloudy swelling of theinner retina. The infarcts comprised the territoriesof supply of cilio-retinal arterioles, and in theeight patients with multiple cilio-retinal vesselseach cilio-retinal territory was infarcted. Haemorr-hages were present within the infarcts but weregenerally few in number, except in case 2 (Fig. 2).There was variable swelling of the optic nerve
head on presentation (Figs I, 3), and marked discpallor was observed in case 7 and in the lower halfof the disc in case 4 (Fig. 4). Papillary haemorrhageswere conspicuous in some cases, but absent in others(Figs I, 3).
Fluorescein angiographyThe intraretinal circulation time (from dye appear-ance in the central artery to filling of the majorveins at the optic disc) exceeded eight seconds inall cases. The central retinal capillary bed wasengorged and fluorescein often leaked from venulesor larger veins in the late phases (Figs I, 2).
Fluorescein perfusion through the cilio-retinalcirculation was consistently impaired relative tocentral arterial perfusion, and the arrival offluorescein in cilio-retinal arterioles was neverobserved to precede the arrival of dye in thecentral artery. The cilio-retinal vessels containeddye in the first available frame of the centralarterial transit in seven cases, while cilio-retinalarteriolar filling was delayed in cases 6, 9, and io.In four patients (cases I, 5, 6, and 8) an intact,engorged cilio-retinal microcirculation was demon-strated with occasional knob-like capillary dilata-tions resembling microaneurysms. In the remainingsix cases the advancement of dye along the cilio-retinal arterioles was very slow, and reversal offlow (Fig. 3c) was seen in cases 2, 3, 7, and 9.The lack of capillary pattern and dye leakageclearly distinguished the cilio-retinal territoryfrom the central retinal supply (Fig. 2) and venulescrossing the infarct filled with dye from the adjacentcirculation. Retrograde entry of dye into the cilio-retinal capillary bed was sometimes seen in thesecases (Fig. 3c).
Angiographic assessment of the posterior ciliarycirculation to the optic disc was often difficultbecause of haemorrhage, but delayed filling of the
(2fz)
(2b)FIG. 2 Case 2. (a) Fundus photograph three daysafter visual loss: haemorrhagic cilio-retinal infarct.(b) Fluorescein angiogram: late phase, dye leakagefrom venules in central arterial territory
disc microcirculation was sometimes demonstrable(Fig. 3). There was variable late leakage of dyefrom the optic disc (Figs I, 3).
Visual functionThe presenting visual acuities in the affected eyesare shown in the Table. Although cloudy retinalswelling involved the papillo-macular bundle in allcases, central fixation was preserved except in case 2,
on January 8, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.60.6.419 on 1 June 1976. Dow
nloaded from

422 British Journal of Ophthalmology
(3a7) (3b)
(3c) (3d)FIG. 3 Case 3. (a) Fundus photograph one day after visual loss: mild ischaemic disc swelling, cilio-retinal infarcts andvenous distension. (b) Fluorescein angiogram: retinal arterial phase, truncated dye front in cilio-retinal arterioles.(c) Fluorescein angiogram: early arterio-venous phase, reversal offlow in cilio-retinal arterioles, optic disc not filled.(d) Fluorescein angiogram: late phase, minimal disc-leakage
in which a large cilio-retinal arteriole suppliedmost of the posterior retina (Fig. 2).
Visual field examination revealed absolute scoto-mata which extended from the blind spot andcorresponded with the distribution of retinalinfarction. The scotoma split fixation in casesI, 3, 4, 5, and 7 because the cilio-retinal supplycontributed to the perifoveal capillary arcade. Inaddition to these absolute defects, field loss in theremaining visual field reflected retinal oedema and
haemorrhage or optic nerve head ischaemia. Anextensive upper field defect in case 4, for example,resulted from infarction of the lower half of theoptic disc.
General medical examinationSystemic disorders found in the patients andpossibly significant in the aetiology of their ocularvascular occlusions are shown in the Table. Therewas no evidence of temporal arteritis in any patient.
on January 8, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.60.6.419 on 1 June 1976. Dow
nloaded from

Cilio-retinal infarction 423
(4b)
FIG. 4 Case 4. (a) Fundus photograph three daysafter visual loss: accumulations of axoplasmic debris inretina (two cotton-wool spots) and inferonasally on disc.(b) Fundus photograph five months later: optic atrophyexcept superonasally. (c) Fluorescein angiogram (samestudy as (b)): retinal arterial phase, delayed filling of discvessels, peripapillary choroid, and cilio-retinal arteriole
Course
Rubeotic glaucoma developed within three monthsof presentation in two patients (cases 2 and 7). Inthe remaining eight cases venous distensionsubsided within a few weeks, with absorption ofretinal haemorrhages and oedema. Visible retino-ciliary venous bypass channels developed in fivepatients (cases I, 3, 5, 6, and Io) and six patientsshowed some improvement in central vision (Table).The optic disc swelling subsided and localizedsectors of pallor of the disc reflected ascendingoptic atrophy secondary to cilio-retinal infarction;atrophy and cupping of the lower half of the discwas seen in case 4 (Fig. 4).Although no unequivocal angiographic evidence
of impaired choroidal perfusion had been found on
presentation, retinal haemorrhages and oedemamade the initial assessment difficult and delayedperipapillary choroidal filling was demonstrated incases I, 4, 5, and 6 on follow-up (Figs I, 4).
HEMISPHERE BRANCH RETINAL VEIN OCCLUSION
(Case i i)A 39-year-old woman noticed sudden blurring ofvision in her left eye the day before presentation.
(4c)
Funduscopy showed distension and tortuosity ofthe veins draining the superior retinal hemisphere.The upper rim of the optic disc was swollen andcloudy retinal swelling was seen in the superiormacular area. The retinal infarct consisted of thatpart of the cilio-retinal circulation which drainedinto the obstructed vein (Fig. 5). Fluoresceinangiography revealed extremely slow perfusion ofa dilated capillary bed within the ischaemic area.
However, the cilio-retinal territories drained by theinferotemporal branch vein filled satisfactorily withdye and showed no cloudy swelling or related fielddefect.
Signs of venous obstruction subsided within a
* -.(4a1)
on January 8, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.60.6.419 on 1 June 1976. Dow
nloaded from

424 British Journal of Ophthalmology
(5ja),- ...
(ic)
few weeks without treatment and left no sequelaeapart from a permanent scotoma below fixation,localized retinal atrophy, and slight sectoral discpallor.
DiscussionCLINICAL PICTURE
The patients in this series presented a variedclinical picture typical of acute retinal vein occlu-sion. Several cases conformed to the descriptionof venous obstruction in youth and middle age
designated 'retinal vasculitis' by Lyle and Wybar(I96I), 'papillophlebitis' by Lonn and Hoyt(I966), and 'optic disc vasculitis' by Hayreh (1972).
(5hb)
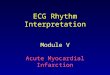
FIG. 5 Case iI. Fluorescein angiograms one day aftervisual loss. (a) Preretinal arterial phase, masking ofchoroidal fluorescence by retinal oedema, lower branchof upper cilio-retinal arteriole has filled. (b) Retinalarterial phase in drainage area of superior hemispherevein, retinal venous phase in drainage area of inferiorhemisphere vein. (c) Late phase, dilated capillaries inischaemic area, slight disc leakage.
These patients illustrated the characteristic toler-ance of a young microcirculation to raised intra-luminal pressure and showed a tendency for spon-taneous recovery without treatment, which hasbeen attributed to the facility for developingretino-ciliary bypass channels (Hart, Sanders, andMiller, 197 I). However, rubeotic glaucoma, afrequent complication of central vein occlusion,developed in two elderly patients in the series.
Retinal pallor, corresponding absolute visualfield defects, and grossly retarded perfusion byfluorescein provided unequivocal clinical proof ofischaemic cloudy swelling in the cilio-retinalterritories. This was also suggested by the signs ofaccumulated axoplasmic debris at the periphery ofthe infarcts (McLeod, I975a) and the subsequentlocalized inner retinal atrophy with loss of super-ficial reflexes from nerve-fibre bundles. However,the ischaemic retina in these cases differed incertain respects from infarcts due to 'pure' arteriolarocclusion. Haemorrhages, for example, were presentwithin the cilio-retinal territories and were extensivein a patient who had pre-existing disease of themacular capillary bed (case 2, Fig. 2). In additionthe cilio-retinal circulation was demonstrably en-
on January 8, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.60.6.419 on 1 June 1976. Dow
nloaded from

Cilio-retinal infarction 425
gorged in some cases and capillary dilatationsresembling microaneurysms were also seen.
In no case of central vein occlusion have we
observed retinal infarction localized to the territoryof a branch of the central retinal artery, so thiscomplication appears to be a development peculiarto the cilio-retinal circulation. This must reflectthe independent origin of cilio-retinal arteriolesfrom the posterior ciliary vessels. However, rela-tively few patients with cilio-retinal arterioles whosuffer a central vein obstruction develop retinalinfarction in the cilio-retinal territories (McLeod,I975b). The two groups of patients (that is, thosewith and those without cilio-retinal infarction)cannot be distinguished either by the severity ofvenous obstruction or by the size of their cilio-retinal vessels.
CIRCULATORY PHYSIOLOGY
The intraluminal pressure in the major ocularveins (Pv) normally approximates to the intraocularpressure (Pio), probably owing to changes in cross-
sectional diameter of these vessels as they leave theglobe-a vascular waterfall (Permutt and Riley,I963). The perfusion pressure (PP) driving bloodthrough the capillary circulations of the retina,choroid, and optic nerve head is therefore definedas the mean arterial blood pressure (Pa) minusthe intraocular pressure (Pio)-that is, PP=Pa-Pio.A reduction in blood flow thus follows obstruc-
tion of the central retinal or posterior ciliaryarteries, though the effects on perfusion may becounteracted by autoregulatory changes in thecalibre of precapillary resistance vessels whichtend to maintain blood flow despite changes inperfusion pressure (Alm and Bill, I972). Ischaemicchanges occur in the inner retina, outer retina, or
optic nerve head when, despite autoregulatoryvasodilatation and collateral flow, capillary perfu-sion is insufficient to meet the individual metabolicrequirements of the various ocular tissues.
Obstruction of the vortex or retinal veins alsocauses a reduction in blood flow (PP==Pa-Pv),while the increase in transmural pressure across
small vessels is an important determinant of transu-dation and haemorrhage formation. Passive dilata-tion of capillaries and venules may reduce theirflow-resistance after venous obstruction (Phillips,Brind, and Levy, I955; Folkow, I962), but theautoregulatory responses of precapillary arteriolesafter retinal vein occlusion have not been estab-lished. Increased transmural pressure gradientsmight be expected to result in arteriolar constrictiondue to a local myogenic reflex (Bayliss, I902);alternatively, vasodilatation might be expected inresponse to retinal hypoxia and accumulation of
metabolites after severe venous occlusion-'meta-bolic autoregulation'.The increase in intraluminal pressure in the
major retinal veins after central vein occlusiondepends upon the change in venous outflowresistance and also upon the arterial blood pressure(since this determines the maximum venouspressure attainable). Total obstruction to retinalvenous outflow has been achieved experimentallyby neoprene latex occlusion of the central vein andpotential retino-ciliary bypass channels (Fujino,Curtin, and Norton, I969). The central venouspressure presumably approached the systolic arterialpressure in these animals and a haemorrhagicretinal infarct resulted. Central vein obstructionsare seldom associated clinically with a completefailure of retinal perfusion. Hart and others(1971) have suggested that the central venouspressure approaches the diastolic arterial pressure,but Duke-Elder and Gloster (I968) emphasizedthat ophthalmodynamometry is unsuitable forassessing either arterial or venous pressures withinthe eye.
PATHOGENESIS OF CILIO-RETINAL INFARCTION
Symptoms and signs of venous obstruction andretinal ischaemia were recent in all our cases,suggesting that these events occurred simul-taneously and probably interdependently. Further-more, in case i i retinal infarction developed onlyin that part of the cilio-retinal territory which wasdrained by the obstructed branch vein, indicatingthat retinal ischaemia was precipitated by venousocclusion.We have assumed that the metabolic require-
ments of the inner retina were the same in thecentral retinal and cilio-retinal territories and thatidentical blood flowed through similar capillarybeds. Furthermore, impaired cilio-retinal perfusionwas considered the cause and not the result ofretinal infarction. Given that the central retinaland cilio-retinal supplies both drain into the centralretinal vein, the localized severe reduction in cilio-retinal perfusion must reflect either an increasedresistance to blood flow along the cilio-retinalarterioles (compared with the central retinalarterioles) or a relatively low driving pressure inthe posterior ciliary supply.
(a) Increased resistance to flowPrecapillary arterioles in the central retinal andcilio-retinal circulations may differ in theirautoregulatory responses to venous occlusion.However, it is unlikely that retinal infarctionresulted from a localized failure of metabolic
on January 8, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.60.6.419 on 1 June 1976. Dow
nloaded from

426 British Journal of Ophthalmology
autoregulation in the cilio-retinal circulation, andan exaggerated reflex constriction of cilio-retinalarterioles (Bayliss effect) is not in keeping withknown autoregulatory responses in branches of theposterior ciliary vessels (Alm and Bill, 1972).
Alternatively, the selective severe impairment ofcilio-retinal perfusion in these cases might reflect a
relatively high 'vasomotor tone' in the posteriorciliary and cilio-retinal arteries, as postulated byBlumenthal, Best, Galin, and Gitter (I97 I).
However, any conclusions drawn from ophthal-modynamoangiographic studies are open to question(Archer, Ernest, and Krill, I972).
(b) Reduction in input arterial pressure
A loiver driving pressure in the posterior ciliaryarteries relative to that in the central artery couldresult in a localized failure of cilio-retinal perfusionafter central vein occlusion. The cilio-retinalarterial pressure might approximate to a raisedvenous pressure sustained by the input pressure
in the larger central arterial supply; the arterio-venous perfusion pressure gradient in the cilio-retinal circulation would thus be effectively elimi-nated.
Unfortunately, there is no satisfactory clinicalmethod of quantifying or comparing input arterialpressures in the various ocular circulations (Duke-Elder and Gloster, I968) and therefore no goodevidence of whether the pressure in the posteriorciliary supply differs appreciably from that in thecentral retinal artery in normal individuals. Thefailure of cilio-retinal perfusion in our cases mightreflect some anatomical variation-for example, an
unusually distal origin of the ciliary supply fromthe ophthalmic artery, or an exceptionally longextraocular course or peculiar pattern of branchingof the posterior ciliary vessels.
Alternatively, this clinical picture may resultfrom central vein occlusion in patients who have a
pre-existing asymptomatic obstruction to flow inthe posterior ciliary circulation which is insufficientin itself to produce ischaemic changes in the outerretina, optic nerve head, or cilio-retinal territory.Such a partial arterial obstruction might reflect thepresence of generalized vascular disease in patientswho develop retinal vein occlusions. Simultaneousinfarction of all cilio-retinal territories in patientswith multiple cilio-retinal arterioles indicates thatany localized obstruction to flow must have beensituated proximal to the emergence of thesevessels from the optic disc, and the peripapillarychoroidal filling defects could be interpreted as
indicating an associated reduction in choroidalblood flow. However, although the central retinalvein is the major efferent channel from the opticdisc (Hayreh, I963b; Anderson, 1970), symptoms of
ischaemic disc-swelling were lacking in several ofour cases, presumably owing to the utilization ofalternative drainage pathways from the disc intochoroidal or pial veins; dilatation of these channelsis part of the process of retino-ciliary collateralformation (Hayreh, I969). In this way isolatedinfarction of the cilio-retinal territories reflectedthe fact that the cilio-retinal circulation is the onlypart of the posterior ciliary supply that dependsentirely on the central vein for drainage.
ConclusionsCentral vein occlusion in patients with partialobstruction of their posterior ciliary arteries maybe the explanation for at least some of our cases,though the relative contribution of reduced ciliaryarterial pressure and raised venous pressure tocilio-retinal ischaemia probably varied from patientto patient. In some cases a critical reduction incilio-retinal perfusion resulted from a degree ofcentral vein obstruction that caused few exudativeor haemorrhagic sequelae in the central retinalterritory. Indeed, some patients might not havepresented had they not possessed a cilio-retinalarterial supply, since central vein occlusion oftenproduces minimal symptoms in the absence ofmacular oedema (Hart and others, 1971).Although experimental central vein occlusion is
known to cause severe retinal ischaemia (Fujinoand others, I969) the relationship between retinalinfarction and venous occlusion is less clearlydefined clinically. These cases show that undercertain conditions venous occlusion may resultin acute retinal infarction in the absence of signifi-cant haemorrhage or extracellular oedema.
This series may represent a spectrum of ocularvascular lesions intermediate between acute centralretinal vein occlusion and acute ischaemic opticneuropathy (which is commonly associated withperipapillary haemorrhages and venous dilatation).
Summary
Retinal ischaemia in the territory supplied bycilio-retinal arterioles is described in io patientswith signs of central retinal vein occlusion and inanother patient with a hemisphere branch veinocclusion. The venous occlusion was transitory innine of the Ii cases, but two elderly patientsdeveloped rubeotic glaucoma.
We thank Mr A. C. Bird, Mr R. K. Blach, Dr J. F.Cullen, Mr L. G. Fison, Dr Eva Kohner, and Mr M. D.Sanders for allowing us to report details of their cases.We are indebted to Mr K. Sehmi and Mr G. Gosai, ofthe Retinal Diagnostic Unit, Moorfields Eye Hospital,for the illustrations, and to Miss L. Martin and MissI. F. Miller for secretarial assistance.
on January 8, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.60.6.419 on 1 June 1976. Dow
nloaded from

Cilio-retinal infarction 427
References
ALM, A., and BILL, A. (1972) Acta physiol. scand., 84, 306ANDERSON, D. R. (I970) Amer. Y. Ophthal., 70, 341ARCHER, D., ERNEST, J. T., and KRILL, A. E. (1972) Ibid., 73, 834BAYLISS, W. M. (1902) J. Physiol. (Lond.), 28, 220BLUMENTHAL, M., BEST, M., GALIN, M. A., and GITTER, K. A. (I97I) Amer. J. Ophthal., 71, 8I9DUKE-ELDER, S., and GLOSTER, j. (I968) In 'System of Ophthalmology', vol. IV. Kimpton, LondonFOLKOW, B. (I962) Arch. int. Pharmacodyn., 139, 455FUJINO, T., CURTIN, V. T., and NORTON, E. W. (I969) Arch. Ophthal. (Chic.), 8I, 395HART, C. D., SANDERS, M. D., and MILLER, S. J. H. (1971) Brit. J. Ophthal., 55, 721HAYREH, S. S. (I963a) Ibid., 47, 71
(I963b) Ann. Inst. Barraquer, 4, 7(I969) Brit. J. Ophthal., 53, 721(I971) Amer. J. Ophthal., 72, 998(1972) Brit. J. Ophthal., 56, 652
LONN, L. I., and HOYT, W. F. (I966) Eye, Ear, Nose, Thr. Monthly, 45, 62LYLE, T. K., and WYBAR, K. (I96I) Brit. Y. Ophthal., 45, 778MCLEOD, D. (I975a) Lancet, 2, 954
(0975b) Brit. Y. Ophthal., 59, 486(1976) Ibid., 6o, in press
OOSTERHUIS, J. A. (I968) In 'Perspectives in Ophthalmology', p. 29, ed. H. E. Henkes. Excerpta MedicaFoundation, Amsterdam
PERMUTT, S., and RILEY, R. L. (I963) Y. appl. Physiol., I8, 924PHILLIPS, F. A., BRIND, S. H., and LEVY, M. H. (1955) Circulat. Res., 3, 357
on January 8, 2020 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.60.6.419 on 1 June 1976. Dow
nloaded from