Embed Size (px)
Citation preview

Maria J. Eriksson, Erik Jørgensen, Jan Peder Amlie, Fredrik Gadler and Henning BundgaardHavndrup, Svend Aakhus, Bertil Svane, Thomas Fritz Hansen, Lars Køber, Knut Endresen, Morten Kvistholm Jensen, Vibeke Marie Almaas, Linda Jacobsson, Peter Riis Hansen, Ole
Hypertrophic Obstructive Cardiomyopathy: A Scandinavian Multicenter StudyLong-Term Outcome of Percutaneous Transluminal Septal Myocardial Ablation in
Print ISSN: 1941-7640. Online ISSN: 1941-7632 Copyright © 2011 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleCirculation: Cardiovascular Interventions
doi: 10.1161/CIRCINTERVENTIONS.110.9597182011;4:256-265; originally published online May 3, 2011;Circ Cardiovasc Interv.
http://circinterventions.ahajournals.org/content/4/3/256World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circinterventions.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Interventions Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Answer
Permissions and Rights Question andunder Services. Further information about this process is available in thepermission is being requested is located, click Request Permissions in the middle column of the Web pageClearance Center, not the Editorial Office. Once the online version of the published article for which
can be obtained via RightsLink, a service of the CopyrightCirculation: Cardiovascular Interventionsin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from by guest on November 3, 2013http://circinterventions.ahajournals.org/Downloaded from

Long-Term Outcome of Percutaneous Transluminal SeptalMyocardial Ablation in Hypertrophic
Obstructive CardiomyopathyA Scandinavian Multicenter Study
Morten Kvistholm Jensen, MD; Vibeke Marie Almaas, MD; Linda Jacobsson, MD;Peter Riis Hansen, MD, PhD; Ole Havndrup, MD, PhD; Svend Aakhus, MD, PhD;Bertil Svane, MD, PhD; Thomas Fritz Hansen, MD, PhD; Lars Køber, MD, PhD;
Knut Endresen, MD, PhD; Maria J. Eriksson, MD, PhD; Erik Jørgensen, MD;Jan Peder Amlie, MD, PhD; Fredrik Gadler, MD, PhD; Henning Bundgaard, MD, PhD
Background—Single-center reports on percutaneous transluminal septal myocardial ablation (PTSMA) in patients withhypertrophic obstructive cardiomyopathy have shown considerable differences in outcome.
Methods and Results—We report the long-term outcome of 313 PTSMA procedures performed in 279 patients withhypertrophic obstructive cardiomyopathy aged 59�14 years from 1999 to 2010 in 4 Scandinavian centers. Sixty-ninepercent of patients had �1 comorbidity at baseline. The median (interquartile range) of left ventricular outflow tractgradient at rest was reduced from 58 mm Hg (34 to 89 mm Hg) at baseline to 12 mm Hg (8 to 24 mm Hg) at 1-year(P�0.001) and during Valsalva maneuver from 93 mm Hg (70 to 140 mm Hg) to 21 mm Hg (11 to 42 mm Hg)(P�0.001). The proportion of patients with syncope was reduced from 18% to 2% (P�0.001), and the proportion inNew York Heart Association class III/IV was reduced from 94% to 21% (P�0.001). All treatment effects remainedstable during the follow-up. New York Heart Association class III/IV at the most recent follow-up (2.9�2.6 years) wasassociated with diabetes mellitus (P�0.03), chronic obstructive pulmonary disease (P�0.02), and valve diseaseunrelated to hypertrophic cardiomyopathy (P�0.01). In-hospital mortality was 0.3%. The 1-, 5- and 10-year survivalrates were 97%, 87%, and 67%, respectively (P�0.06 versus an age- and sex-matched background population) in allpatients and 99%, 94%, and 88%, respectively (P�0.12) in patients aged �60 years (48�9 years, n�141). Age (hazardratio, 1.07; 95% CI, 1.03 to 1.1) was the only predictor of survival.
Conclusions—In this multicenter study, the in-hospital mortality after PTSMA was low despite considerable comorbidi-ties. The hemodynamic and symptomatic effects were sustained long term. The long-term symptomatic outcome wasassociated with baseline comorbidities. The 10-year survival rate was comparable to that in an age- and sex-matchedbackground population, and age was the only predictor of survival. (Circ Cardiovasc Interv. 2011;4:256-265.)
Key Words: percutaneous transluminal septal myocardial ablation � cardiomyopathy hypertrophic� left ventricular outflow obstruction � survival � treatment outcome � multicenter study
Left ventricular outflow tract obstruction (LVOTO) ispresent in up to two thirds of patients with hypertrophic
cardiomyopathy (HCM).1 The obstructive form of HCM(HOCM) is associated with increased morbidity and mortal-ity.2 The long-term symptomatic effectiveness of myectomyhas been proven in patients with HOCM with severe drugrefractory symptoms and possibly improves survival.3–7 Per-cutaneous transluminal septal myocardial ablation (PTSMA)was introduced in 1995 as an alternative to myectomy and has
been shown to reduce the LVOTO and associated symp-toms.8–10 Myectomy has been the gold standard for septalreduction therapy because of solid long-term results (eg,survival comparable to the background population).11 Thefavorable outcome of myectomy reported from high-volumecenters has been matched by a few high-volume PTSMAcenters.12,13 However, single-center reports on annual mortal-ity rates after PTSMA ranges considerably,14 with highmortality rates in some reports contributing to keep myec-
Received September 24, 2010; accepted April 7, 2011.From the Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark (M.K.J., O.H., L.K., E.J., H.B.); Oslo University Hospital,
Rikshospitalet, Oslo, Norway (V.M.A., S.A., K.E., J.P.A.); Karolinska University Hospital, Stockholm, Sweden (L.J., B.S., M.J.E., F.G.); andCopenhagen University Hospital, Gentofte Hospital, Gentofte, Denmark (P.R.H., T.F.H.).
Correspondence to Morten Kvistholm Jensen, MD, Department of Cardiology, 2142, The Heart Centre, Rigshospitalet, Blegdamsvej 9, 2100Copenhagen, Denmark. E-mail [email protected]
© 2011 American Heart Association, Inc.
Circ Cardiovasc Interv is available at http://circinterventions.ahajournals.org DOI: 10.1161/CIRCINTERVENTIONS.110.959718
256

tomy the gold standard. Direct comparisons between suchstudies may be misleading. Multicenter studies may add toour knowledge of PTSMA outcome. Therefore, in the presentmulticenter study, we analyzed the short- and long-termoutcome of PTSMA performed in 4 Scandinavian heartcenters.
Clinical Perspective on p 265
MethodsThe Scandinavian HOCM Database (www.scand-hocm.org) wasestablished in collaboration among heart centers at Oslo UniversityHospital, Rikshospitalet, Oslo, Norway; Copenhagen UniversityHospital, Gentofte Hospital, Gentofte, Denmark; Karolinska Univer-sity Hospital, Stockholm, Sweden; and Copenhagen UniversityHospital, Rigshospitalet, Copenhagen, Denmark. PTSMA was intro-duced independently in these centers from 1999 to 2001. The aim ofthe collaboration is to evaluate the long-term outcome of PTSMA ina clinical multicenter setting. The database complies with dataregistry regulations within the European Union and Norway and wasapproved by relevant data authorities and committees for ethicsin medicine.
The participating heart centers are based in public universityhospitals. All PTSMA operators had a record of �1000 percutaneouscoronary interventions before their first PTSMA. Patients withHOCM were followed by subspecialized HCM cardiologists andexamined by experts in echocardiography.
PatientsAll patients treated with PTSMA in the 4 centers from 1999 to 2010were included. The patients were referred from a geographicallydefined background population of approximately 10 million citizens,which is �50% of the Scandinavian population. Retrospective datafor this study were merged in the database in 2007. Since 2007, newpatients and follow-up data have been included prospectively. Datawere retrieved from patient files, echocardiography reports, andsurvival registries and registered at baseline and annually duringfollow-up. Data were withdrawn from the Scandinavian HOCMDatabase on April 4, 2010.
HCM/HOCM was diagnosed in accordance with the AmericanCollege of Cardiology/European Society of Cardiology consensusdocument,11 and arterial hypertension, to an extent, that could notexplain the degree of myocardial hypertrophy was not considered anobstacle for establishing the diagnosis. The indication for PTSMAwas HOCM with severe drug refractory, New York Heart Asso-ciation (NYHA) class III/IV symptoms and a resting LVOTgradient of �30 mm Hg (1 center), �50 mm Hg (3 centers), or�100 mm Hg during provocation. Since its introduction in the 4centers, PTSMA has been the primary treatment of choice.Myectomy was considered in patients with midventricular ob-struction or in patients needing valve, coronary artery bypassgraft, or other kinds of cardiac surgery. A high perioperative riskwas considered in favor of PTSMA, and multivessel coronaryartery disease was considered in favor of myectomy. Finally,patient preferences were taken into account. The ratio betweenPTSMA procedures and myectomies was �7:1.
The PTSMA procedures were guided by transthoracic ortransesophageal echocardiography. In all cases, intracoronaryechocardiography contrast was used according to previous de-scriptions.8,15,16 The alcohol was injected slowly during a periodof 5 to 10 minutes, and then the balloon was kept inflated for 10minutes. The volume of injected alcohol was reduced during thefirst years after implementation of PTSMA and, subsequently, 0.1mL alcohol per millimeter septum thickness per septal branch hasbeen used as guidance.
According to our protocols, patients were monitored (includingtelemetry) in coronary care units for 7 days after the PTSMAprocedure. After 48 hours, the temporary pacemaker was removed if
the patient seemed to have normal cardiac conduction. If high-gradeatrioventricular (AV) conduction disturbances were seen during thefollowing days, a permanent pacemaker (PPM) implantation wasoffered. Patients were discharged to follow-up in our outpatientclinics.
Treatment EffectsThe hemodynamic effects of PTSMA were evaluated by changes inechocardiographically obtained LVOT gradients.17 The symptomaticeffects were evaluated by changes in NYHA class and CanadianCardiovascular Society class scores. The proportion of patients with�1 syncope (abrupt transient loss of consciousness and spontaneousawakening not explained by emotional, neurological, environmental,or other noncardiac causes) within 1 year of assessment wasregistered. Palpitations were registered similarly.
ComplicationsComplications during PTSMA procedures and in-hospital monitor-ing were registered. Events were acute heart failure and death, andarrhythmic events were bradycardia, asystole, and sustained andnonsustained ventricular tachycardia and ventricular fibrillation(VF). Coronary artery complications were coronary dissection,coronary perforation, acute pericardial effusion, pericardial tampon-ade, and alcohol displacement. Bundle branch block and AV block,including advanced heart block, leading to PPM implantation wereregistered. Advanced heart block was defined as bifascicular block,second- or third-degree AV block. Asystole due to third-degree AVblock was classified as third-degree AV block (ie, advancedheart block).
Background PopulationThe expected age- and sex-matched survival rates were calculatedfor each patient on the basis of survival in the Danish population (5.4million citizens).18 On the basis of these survival rates, survival of afictive age- and sex-matched background population of averageDanes in a 20:1 ratio to the PTSMA cohort was constructed. We usedthe Danish background population (2001 to 2005) for these calcu-lations, ignoring possible minor differences in life expectancy amongScandinavian populations.19
Statistical AnalysisData were analyzed using the SAS version 9.1 statistical software.Baseline refers to pre-PTSMA data, and most recent follow-uprefers to the most recently available data after PTSMA. Data arepresented as mean�SD when normally distributed or median(interquartile range [IQR]) when nonnormally distributed. Pro-portions are presented as percentages (%). Student t test was usedfor paired comparisons of continuous variables. Unpaired com-parisons were performed with the Student t test or Wilcoxon ranksum test, depending on the data distribution. Proportions werecompared with �2 test or Fisher exact test when unpaired andMcNemar test when paired.
All patients treated with PTSMA (alcohol injection performed)entered the survival analysis at the date of their first PTSMA.Patients were censored if they were still alive when survival statuswas obtained from the survival registries. Death of all causes wasconsidered an event. No patients were censored for other cardiovas-cular events or interventions such as myocardial infarction, valvularsurgery, and coronary bypass because such patients were stillconsidered to be at risk of developing adverse events related toPTSMA. Kaplan-Meier estimates of survival were calculated, andtime-to-event curves were compared using the log-rank test. Predic-tors of death were analyzed in a univariable Cox regression model,and continuous variables (excluding age) were log transformed asappropriate. The assumption of proportional hazards, linearity ofcontinuous variables, and lack of interactions were found to be validwithout transformation. Results are presented as hazard ratio (HR)
Jensen et al Long-Term Outcome of PTSMA in Scandinavia 257

and 95% CI. A 2-sided P�0.05 was considered significant.Repeated-measures ANOVA and generalized estimating equationanalyses were used to account for multiple observations per patientduring follow-up as appropriate.
ResultsFrom 1999 to 2010, 313 PTSMA procedures were performedin 279 patients (age, 59�14 years) (Table 1). Symptoms andfunctional class were assessed at 1033 time points (1 to 8follow-up assessments per patient), and 594 echocardiogra-phy examinations were performed at baseline and during2.9�2.6 years of follow-up. The prevalences of comorbiditiesare listed in Table 1. The proportions of patients with 0, 1, 2,3, and 4 comorbidities were 31%, 35%, 27%, 7%, and 0.4%,respectively. Forty-four percent of patients (range, 37% to48% between centers) had a history of some degree of arterialhypertension. In 95% of the procedures, 1 septal branch wasablated, and in the rest, 2 septal branches were ablated.
Within 2 years after the first PTSMA, 14% of patients weretreated with another septal reduction therapy (6 myectomy,26 PTSMA) (Figure 1).
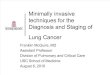
Hemodynamic and Symptomatic EffectsThere were no differences in baseline LVOT gradients at restbetween the center using a resting LVOT gradient�30 mm Hg as a criterion for performing PTSMA (median,55 mm Hg; IQR, 38 to 70 mm Hg) and the centers using the�50 mm Hg as a criterion (median, 59 mm Hg; IQR, 33 to90 mm Hg; P�0.5). The LVOT gradients at rest werereduced from 58 mm Hg (IQR, 34 to 89 mm Hg) at baselineto 12 mm Hg (IQR, 8 to 24 mm Hg) at 1-year follow-up(P�0.001) and with a small further decrease (0.9 mm Hg peryear) during the follow-up period (P�0.03) (Figure 2). TheLVOT gradients during Valsalva maneuver were reducedfrom 93 mm Hg (IQR, 70 to 140 mm Hg) at baseline to21 mm Hg (IQR, 11 to 42 mm Hg) at 1-year follow-up(P�0.001) and remained stable during the follow-up period(P�0.14) (Figure 2).
The proportion of patients in NYHA class III/IV wasreduced from 94% at baseline to 21% at 1-year follow-up(P�0.001) and remained stable during the follow-up period(P�0.99) (Figure 3). The proportion of patients in CanadianCardiovascular Society class III/IV was reduced from 16% atbaseline to 3% at 1-year follow-up (P�0.001) and remainedstable during the follow-up period (P�0.5) (Figure 3). Theproportion of patients with syncope or palpitations were 18%and 34%, respectively, at baseline compared to 2%(P�0.001) and 13% (P�0.001) at 1-year follow-up andremained stable during the follow-up period (P�0.35 andP�0.45, respectively) (Figure 3). Left ventricle ejectionfraction was 59�7% at baseline and 58�9% at 1-yearfollow-up (P�0.08) and remained stable during the follow-upperiod (P�0.2).
In patients in NYHA class III/IV at most recent follow-up(21%), LVOT gradients at rest (median, 13 mm Hg; IQR, 10to 30 mm Hg) and during Valsalva-maneuver (median,21 mm Hg; IQR, 14 to 47 mm Hg) were not significantlydifferent from LVOT gradients in patients in NYHA class I/IIat rest (median, 11 mm Hg; IQR, 7 to 17 mm Hg; P�0.06)and during Valsalva maneuver (median, 20 mm Hg; IQR, 10to 41 mm Hg; P�0.3). Patients in NYHA class III/IV at themost recent follow-up had more baseline comorbidities (0, 1,2, 3, and 4 years, 12%, 44%, 29%, 15%, and 0%, respec-tively) than patients in NYHA class I/II (36%, 31%, 25%,6%, and 1%, respectively; P�0.03) and tended to be older(61�15 years versus 57�13 years, respectively, P�0.17).NYHA class III/IV at most recent follow-up was associatedwith diabetes mellitus (P�0.03), chronic obstructive pulmo-nary disease (P�0.02), and valve disease not related to HCM(P�0.01). Ninety-one percent of patients without comorbidi-ties at baseline were in NYHA class I/II at most recentfollow-up compared to 72% (P�0.01) of the patients with �1comorbidity. Symptomatic improvement defined as de-creased NYHA or Canadian Cardiovascular Society class ordisappearance of syncope was evident in 88% of patients atmost recent follow-up.
Table 1. Baseline Characteristics of 279 Patients TreatedWith PTSMA
Characteristic Value
Demographic
Age at first PTSMA, y 59�14
Female sex, % 46
Clinical follow-up, y 2.9�2.5
Comorbidity
Obesity (BMI �30 kg/m2) 80 (32)
COPD 18 (6)
Diabetes mellitus 19 (7)
History of arterial hypertension 123 (44)
Cerebrovascular events 15 (5)
Heart valve disease (not related to HCM) 22 (8)
Previous invasive treatment
PCI 19 (7)
Pacemaker (total) 45 (16)
Pacemaker (LVOT gradient) 40 (14)
Pacemaker (other) 5 (1.8)
ICD 4 (1.4)
Myectomy 4 (1.4)
Heart surgery (other) 3 (1.1)
Echocardiography
IVSd, mm 19�4
LVEDd, mm 43�6
LVPWd, mm 13�3
Maximal wall thickness, mm 20�4
Left atrial dimension, mm 45�7
LVEF, % 59�7
Data are presented as mean�SD or n (%), unless otherwise indicated. BMIindicates body mass index; COPD, chronic obstructive pulmonary disease;HCM, hypertrophic cardiomyopathy; ICD, implantable cardioverter-defibrillator;IVSd, interventricular septum diastolic dimension; LVEDd, left ventriculardiastolic dimension; LVEF, left ventricular ejection fraction; LVOT, left ventric-ular outflow tract; LVPWD, left ventricular posterior wall diastolic dimension;PCI, percutaneous coronary intervention; PTSMA, percutaneous transluminalseptal myocardial ablation.
258 Circ Cardiovasc Interv June 2011

ComplicationsThe in-hospital mortality was 0.3% (n�1), and the 30-daymortality was 0.6%. The patient who died in the hospital wasa 72-year-old woman with left bundle branch block. ThePTSMA procedure was performed without complications, but8 hours later, she developed acute heart failure with advancedheart block (treated with pacing) and refractory hypotension.In the autopsy report, myocardial changes typically seen inHCM were described, but no evidence of unintentionalcoronary lesions, ischemic heart disease, or any other expla-nation for the fatal outcome was disclosed.
In-hospital VF occurred in 9 (2.8%) patients during thePTSMA procedure (n�4) or during the in-hospital monitor-ing (n�5) (Table 2). All patients with VF were defibrillatedusing external defibrillators and had immediate completerecovery. The volume of alcohol injected during procedurescomplicated by in-hospital VF tended to be lower (1.7�0.3mL) than the volume injected during procedures not compli-cated by VF (2.2�0.7 mL, P�0.08). In 2 patients, VF wasrelated to injection of contrast (ie, before alcohol injection).Implantable cardioverter-defibrillators were not used in case
of per- or periprocedural VF, and there was no associationbetween VF and long-term survival (Table 3).
Episodes of third-degree heart block were seen in 36% ofpatients during the PTSMA procedures and in 23% during thepostprocedural observation (Table 2). Sixteen percent (45/279) of patients had a PPM before the first PTSMA, and 20%(45/230) without a PPM or an implantable cardioverter-defibrillator (n�4) before PTSMA had a PPM implantedwithin 30 days after PTSMA (ie, in total, 32% [90/279] hada PPM 30 days after the first PTSMA). The indication forPPM implantation after PTSMA was advanced heart block in98% of cases. In patients requiring PPM implantation, theinjected alcohol volume was 2.3�0.7 mL compared to2.2�1.0 mL (P�0.006) in the remaining patients. Thepacemaker implantation rate of 30% from 1999 to 2004 wasreduced to 17% (P�0.01) in the following period. Thisreduction may be related to a reduction in the volume ofinjected alcohol from 2.6�0.9 mL until 2004 to 2.0�0.6 mLin the following period (P�0.001).
Bradycardia or asystole occurred during in-hospital moni-toring after 12 (3.9%) PTSMA procedures and were related to
Figure 1. Freedom from reintervention(percutaneous transluminal septal myo-cardial ablation or myectomy) after per-cutaneous transluminal septal myocar-dial ablation in 279 patients in 4Scandinavian heart centers (1999 to2010).
Figure 2. LVOT gradients at baseline and after percutaneous transluminal septal myocardial ablation in 279 patients in 4 Scandinavianheart centers (1999 to 2010). A, At rest. B, During Valsalva maneuver. LVOT indicates left ventricular outflow tract.
Jensen et al Long-Term Outcome of PTSMA in Scandinavia 259

failure of temporary pacemakers or late-occurring (�48hours after PTSMA) advanced heart blocks. In 2 patients,pericardial effusions causing tamponade were evacuated byacute sternotomy. In 1 patient, a pericardial effusion wasevacuated by pericardiocentesis, and in 1 patient, an effusion(9 mm) was treated conservatively (Table 2). No othercomplications led to acute surgery. Two cases of thrombosisin the left anterior descending artery during the PTSMAprocedure were observed (1 in-stent). Both cases were suc-cessfully treated, and coronary flows were normalized.
SurvivalThe median observational time (April 4, 2010) used in thesurvival analysis was 3.7 years (IQR, 1.4 to 6.3 years).Thirty-four deaths occurred during 1142 patient-years (ie, anoverall mortality rate of 3% per year). The 1-, 5-, and 10-yearsurvival rates after PTSMA were 97% (95% CI, 95% to99%), 87% (95% CI, 81% to 92%), and 67% (95% CI, 53%to 80%), respectively, compared to 98%, 90%, and 78% inthe age- and sex-matched background population (HR, 1.4;95% CI, 0.99 to 2.0; log-rank P�0.06) (Figure 4). Patientsaged �60 years (48�9 years, n�141) had 1-, 5-, and 10-yearsurvival rates of 99% (95% CI, 98% to 100%), 94% (95% CI,
88% to 99%), and 88% (95% CI, 78% to 98%) compared to100%, 97%, and 93% (HR, 1.8; 95% CI, 0.85 to 3.9; log-rankP�0.12) in the age- and sex-matched background population(Figure 5). In patients aged �60 years (70�7 years, n�138)the 1-, 5- and 10-year survival rates were 95% (95% CI, 93%to 97%), 79% (95% CI, 70% to 88%), and 46% (95% CI, 35%to 57%) compared to 97%, 83%, and 63% (HR, 1.4; 95% CI,0.96 to 2.1; log-rank P�0.09) in the age- and sex-matchedbackground population (Figure 5). Eleven percent of patientshad an implantable cardioverter-defibrillator at most recentfollow-up. There were no differences in survival among the 4heart centers (log-rank P�0.9).
Age at baseline, sex, chronic obstructive pulmonary dis-ease, and sum of arrhythmic events during in-hospital mon-itoring were univariably associated (P�0.1) with reducedsurvival. These parameters were analyzed in a multivariableCox regression model (Table 3). There were no interactionsamong these 4 variables. Age at baseline showed significantassociation to survival (HR, 1.07; 95% CI, 1.03 to 1.1;P�0.001), and there was a nonsignificant association be-tween chronic obstructive pulmonary disease (HR, 2.4; 95%CI, 0.9 to 5.7; P�0.06) and survival, whereas female sex(HR, 1.09; 95% CI, 0.5 to 2.3; P�0.9) and the sum of
Figure 3. Symptomatic state at baseline and after percutaneous transluminal septal myocardial ablation in 4 Scandinavian heart cen-ters (1999 to 2010). A, Dyspnea. B, Chest pain. C, Syncope. D, Palpitations. Where no bar is shown, the prevalence was 0%. Errorbars represent SE of the proportion. CCS indicates Canadian Cardiovascular Society; NYHA, New York Heart Association.
260 Circ Cardiovasc Interv June 2011

arrhythmic events during in-hospital monitoring (HR, 1.2;95% CI, 0.8 to 1.7; P�0.5) were not associated with survival.Adding postprocedural advanced heart block (univariablyassociated with increased survival) to the multivariable Coxanalysis did not disclose any association to survival (HR, 1.4;95% CI, 0.7 to 2.8; P�0.4).
DiscussionConsidering the observational time of 1142 patient-years, thisfirst multicenter study reporting long-term outcome ofPTSMA is among the largest studies of PTSMA.14 The mainfindings included a low in-hospital mortality and a lowcomplication rate. Survival after PTSMA was only predictedby age and was comparable to the survival in an age- andsex-matched background population. Additionally, the hemo-dynamic and symptomatic benefits were sustained, but in21% of the patients, dyspnea (NYHA class III/IV) persisteddespite successful reduction of the LVOTO. Persistence ofNYHA class III/IV at follow-up was associated with noncar-diac or cardiac comorbidities.
Our in-hospital mortality was 0.3% compared to 1.0%(n�611) reported by Fernandes et al.12 Comorbidities tend toincrease the surgical mortality,20 but in the present cohortwith considerable comorbidity, the 30-day mortality was0.6% compared to 0.8% (n�289) after myectomy reported byOmmen et al.4 The survival in the present PTSMA-treatedcohort (87% at 5 years) was not significantly reducedcompared to survival in an age- and sex-matched backgroundpopulation (90% at 5 years, P�0.06). Five-year survivalreported from other PTSMA centers have been higher thanthe survival in our background population (97% [n�100]13
and 92% [n�611]12). In contrast, Sorajja et al21 reported a4-year survival rate of 88% (n�138) after PTSMA, whichseems to be lower than the 4-year survival rate in the presentstudy (92%). Kuhn et al10 reported a mortality rate of 4.3%per year after PTSMA (n�644) compared to 3.0% per year inthe present study. Thus, the survival in this study seems to bein the midrange of reported survival rates after PTSMA.
In addition to the value of increased total number ofpatients in a multicenter study, the effects of differences inlocal routines (eg, referral routines, case selection [age, sex,HCM phenotype, methods for gradient measurements, pres-ence of comorbidities, previous treatment], operator skills,minor differences in procedures, differences in postprocedurecare, medication and recommendations for PPM or implant-able cardioverter-defibrillator, follow-up routines) may havebeen leveled out and had a reduced effect on the overallresults. Thus, the results of our multicenter study may bemore generalizable than those from single-center studies.
The size of our cohort and the death rate limit the analysisof differences in survival between patients and the age- andsex-matched background population, but it should be notedthat there was a trend toward a reduced survival in thePTSMA-treated patients with HCM. However, this trendmight be explained to some extent by a generally highermortality caused by the presence of HCM per se.
We found age to be the sole predictor of survival in thepresent study. Generally, reported myectomy cohorts havebeen younger (mean age, 45 to 50 years)4,6,7,22 than PTSMAcohorts (mean age, 54 to 64 years).9,10,12,14,21,23 In a recentmeta-analysis of outcome after PTSMA versus myectomy,Leonardi et al14 reported that odds ratios for treatment effecton all-cause mortality as well as sudden cardiac death were infavor of PTSMA after adjustment for available baselinecharacteristics, including age. Our finding of an 88% survival10 years after PTSMA in patients aged �60 years, comparedto the 10-year survival rate of 83% reported by Ommen et al4
in a slightly younger myectomy population (age, 45�20years; n�289) seems to confirm the more favorable survivalafter PTSMA compared to myectomy as reported by Leon-ardi et al.14 However, such comparisons of survival estimatesbetween studies have statistical limitations and are affectedby a number of confounding factors. Taken together, it islikely that age to a considerable extent explains the reporteddifferences in survival between PTSMA- and myectomy-treated patients.
Several reports have documented the hemodynamic andsymptomatic effects of PTSMA in the short and interme-diate term.9,10,21,24 –27 In the present study, the resting
Table 2. Complications After 313 PTSMA Procedures in279 Patients
During PTSMAIn-HospitalMonitoring
Injected volume of alcohol, mL 2.2�0.8
CKMB max, �g/L . . . 152�104
TNT max, �g/L . . . 3.26�1.76
TNI max, �g/L . . . 22�16
Complications (n�313)
Coronary artery perforation 3 (1.0) . . .
Coronary artery spasm 4 (1.3) . . .
Wire/balloon failure 3 (0.9) . . .
Alcohol displacement 5 (1.6) . . .
Thrombosis 2 (0.6) . . .
Hemopericardium/tamponade/effusion
0 (0) 4 (1.3)
Femoral hematoma 0 (0) 19 (6)
Cerebrovascular events 0 (0) 0 (0)
Death 0 (0) 1 (0.3)
Arrhythmia (n�313)
Bradycardia 5 (1.6) 5 (1.6)*
Asystole 4 (1.3) 9 (2.9)*
Sustained ventricular tachycardia 0 (0) 0 (0)
Ventricular fibrillation 4 (1.3) 5 (1.6)
Conduction disturbances (n�230)†
First-degree AVB 6 (2.6) 9 (3.9)
Second-degree AVB 2 (0.9) 3 (1.3)
Third-degree AVB 82 (36) 54 (23)
Data are presented as mean�SD or n (%). AVB indicates atrioventricularblock; CKMB, creatinine kinase MB; PTSMA, percutaneous transluminal septalmyocardial ablation; TNI, troponin I; TNT, troponin T.
*Two (0.6%) patients experienced both asystole and bradycardia.†Conduction disturbances only evaluated in patients without permanent
pacemakers and implantable cardioverter-defibrillators at baseline.
Jensen et al Long-Term Outcome of PTSMA in Scandinavia 261

LVOT gradient was 12 mm Hg (IQR, 8–24 mm Hg) at 1-yearfollow-up. This finding matches that of resting LVOT gradientsof 22 mm Hg (IQR, 15–23 mm Hg) after PTSMA in a meta-analysis by Leonardi et al14 (n�2207). Furthermore, this hemo-dynamic effect and the symptomatic improvements afterPTSMA were sustained in the long term (Figures 2 and 3).
At most recent follow-up, 21% of the patients in the presentstudy were in NYHA class III/IV. This subgroup had noincreased LVOT gradients at rest or during Valsalva maneuvercompared to patients in NYHA class I/II. Olivotto et al28
reported an increasing proportion of patients in NYHA classIII/IV (n�237) from 10% to 23% during 12�7 years follow-up
Table 3. Univariable and Multivariable Cox Regression Analyses of Baseline Variables andProcedure-Related Variables as Predictors for Death After PTSMA
Cox Regression Analysis
Univariable Multivariable
HR (95% CI) P HR (95% CI) P
Baseline
Age, y 1.07 (1.04–1.10) �0.001 1.07 (1.03–1.1) �0.001
Female sex 1.8 (0.9–3.5) 0.10 1.09 (0.5–2.3) 0.92
Hospital . . . 0.90 . . . . . .
PTSMA procedure
Date of first PTSMA, d 1.0 (0.99–1.00) 0.32 . . . . . .
Injected volume of alcohol, mL 1.1 (0.8–1.6) 0.47 . . . . . .
Maximal CKMB, �g/L 1.0 (1.0–1.0) 0.45 . . . . . .
Comorbidity
Obesity (BMI �30 kg/m2) 0.9 (0.4–2.0) 0.80 . . . . . .
Diabetes mellitus 0.7 (0.1–4.9) 0.69 . . . . . .
COPD 2.6 (1.1–6.4) 0.03 2.4 (0.97–5.7) 0.06
History of arterial hypertension 0.9 (0.4–1.7) 0.55 . . . . . .
Hypercholesterolemia 0.7 (0.3–1.7) 0.45 . . . . . .
Ischemic heart disease (previous PCI) 1.8 (0.9–3.8) 0.31 . . . . . .
History of apoplexia 1.5 (0.5–4.9) 0.51 . . . . . .
Valve disease not related to HCM 2.0 (0.9–4.7) 0.10* . . . . . .
Procedural arrhythmia
Advanced heart block 1.5 (0.8–2.9) 0.25 . . . . . .
AF 1.6 (0.2–11) 0.66 . . . . . .
Nonsustained VT . . . 0.98 . . . . . .
Sustained VT . . . . . . . . . . . .
VF . . . 0.99 . . . . . .
Bradycardia 2.6 (0.6–11) 0.20 . . . . . .
Asystoli . . . 0.99 . . . . . .
Sum of procedural arrhythmias 1.4 (0.8–2.4) 0.26 . . . . . .
Postprocedural arrhythmia
Advanced heart block 2.0 (1.0–3.9) 0.05† . . . . . .
AF 1.1 (0.4–3.1) 0.86 . . . . . .
Nonsustained VT 1.2 (0.5–2.8) 0.63 . . . . . .
Sustained VT . . . . . . . . . . . .
VF . . . 0.99 . . . . . .
Bradycardia 3.0 (0.7–13) 0.13 . . . . . .
Asystoli 2.5 (0.8–8.3) 0.13 . . . . . .
No. of postprocedural arrhythmias 1.4 (0.99–2.1) 0.06 1.2 (0.8–1.7) 0.55
AF indicates atrial fibrillation; CKMB, creatinine kinase MB; COPD, chronic obstructive pulmonary disease; HCM,hypertrophic cardiomyopathy; HR, hazard ratio; PCI, percutaneous coronary intervention; PTSMA, percutaneoustransluminal septal myocardial ablation; VF, ventricular fibrillation; VT, ventricular tachycardia.
*P�0.1.†HR �1.0.
262 Circ Cardiovasc Interv June 2011

(age, 56�23 years at follow-up), although only 3% had signif-icant LVOTO. Thus, persistent dyspnea after PTSMA is notnecessarily due to a failure of the procedure but may be causedby other HCM-related pathophysiologic factors, such as diastol-ic dysfunction, atrial fibrillation, or reduced stroke volume. Wedid, however, also find that cardiac and noncardiac comorbidi-ties were associated with persistent NYHA class III/IV symp-toms. Functional impairment due to concomitant comorbiditycan only partly be differentiated from impairment caused byintrinsic HCM.
We found a high prevalence of a history of arterialhypertension. Our cohort had mainly asymmetrical hypertro-phy (septum, 19�4 mm; posterior wall, 13�3 mm), andprevious mild to moderate hypertension was not consideredto be the etiology of the observed degree of hypertrophy. Wehave no data allowing us to dissect the time relationshipbetween the development of hypertension and the develop-
ment of LVOTO. However, as in patients with hypertensionin general, it is likely that arterial hypertension also is atrigger for development of more severe hypertrophy inpatients with HCM, which may increase the likelihood fordeveloping LVOTO and need for PTSMA when hypertensionand HCM coexist.
Advanced heart block occurred during 34% of procedures(Table 2). This finding was comparable to incidences of46%29 and 38%30 reported from other PTSMA centers.Twenty percent of the patients in the present study had a PPMimplanted as a complication to PTSMA compared to 5%29
and 18%30 in the other centers. The reduction of the volumeof injected alcohol seemed to be associated with a reductionin the need for PPM implantations in the present study.However, the high rate of PPM implantations we sawemphasizes the need to look carefully into our routines tolower the PPM implantation rate to the 5% to 10% reported
Figure 4. Survival after PTSMA in 279patients in 4 Scandinavian heart centers(1999 to 2010). Background indicatesage- and sex-matched background pop-ulation; PTSMA, percutaneous translumi-nal septal myocardial ablation.
Figure 5. Survival after percutaneoustransluminal septal myocardial ablationstratified by age in 4 Scandinavian heartcenters (1999 to 2010). Solid line indi-cates age �60 years (mean, 48�9years); thin solid line, age- and sex-matched background population;dashed line, age �60 years (mean,70�7 years); and thin dashed line, age-and sex-matched background popula-tion. P values represent comparisonsbetween each group and its age- andsex-matched background population.
Jensen et al Long-Term Outcome of PTSMA in Scandinavia 263

from some PTSMA centers.23,29,31 Conduction disturbancesalso are seen after myectomy, necessitating PPM implanta-tion in up to 8% of patients.7
Reports of in-hospital VF in relation to PTSMA haveattracted considerable attention.23,31 We found 9 (2.8%) casesof in-hospital VF (4 procedural and 5 postprocedural). Othercenters have reported an in-hospital incidence of ventriculartachycardia, VF, or sudden death of 2% to 3% during or afterPTSMA.21,23 According to our experience, in-hospital ven-tricular arrhythmia can be handled safely but warrants carefulmonitoring.
In the present study, 14% of the patients had a reinterven-tion (myectomy or PTSMA) within 2 years, which is com-parable to an 83% success rate (no reintervention) afterPTSMA reported by Sorajja et al21 but seems higher thanreintervention rates of 5% to 10% reported by others.23,31,32
However, our low in-hospital mortality during PTSMA andre-PTSMA indicates that a careful PTSMA strategy, whichmay necessitate re-PTSMA in selected cases, can be consid-ered safe. The majority of reinterventions were performedwithin 2 years after PTSMA. At 2- to 3-year follow-up, theLVOT gradients at rest and during Valsalva maneuver werelow and remained stable during the rest of the follow-upperiod (Figure 2). Thus, if the gradients remained low for 1 to2 years after PTSMA, LVOTO did not seem to reoccur.
ConclusionsIn this long-term multicenter study, PTSMA-treated patientshad sustained hemodynamic and symptomatic effects, and thesurvival was comparable to that in the background popula-tion, with age as the only predictor of survival. The in-hospital mortality was low despite significant comorbidity.The long-term symptomatic outcome was significantly af-fected by baseline comorbidities.
AcknowledgmentsWe thank Christian Hassager, MD, PhD, from The Heart Center,Rigshospitalet, University of Copenhagen, Copenhagen, Denmark,for valuable contributions to the study.
Sources of FundingThis study was supported by the Lundbeck Foundation, Denmark;The Danish Medical Research Fund, Axel Muusfeldts Fond, Den-mark; The Heart Centre Research Council, Rigshospitalet, Copen-hagen University Hospital, Denmark; and Inger and John Fredrik-sens Heart Foundation, Oslo, Norway.
DisclosuresNone.
References1. Shah JS, Esteban MT, Thaman R, Sharma R, Mist B, Pantazis A, Ward
D, Kohli SK, Page SP, Demetrescu C, Sevdalis E, Keren A, Pellerin D,McKenna WJ, Elliott PM. Prevalence of exercise-induced left ventricularoutflow tract obstruction in symptomatic patients with non-obstructivehypertrophic cardiomyopathy. Heart. 2008;94:1288–1294.
2. Elliott PM, Gimeno JR, Tome MT, Shah J, Ward D, Thaman R,Mogensen J, McKenna WJ. Left ventricular outflow tract obstruction andsudden death risk in patients with hypertrophic cardiomyopathy. EurHeart J. 2006;27:1933–1941.
3. Schulte HD, Borisov K, Gams E, Gramsch-Zabel H, Losse B,Schwartzkopff B. Management of symptomatic hypertrophic
obstructive cardiomyopathy—long-term results after surgical therapy.Thorac Cardiovasc Surg. 1999;47:213–218.
4. Ommen SR, Maron BJ, Olivotto I, Maron MS, Cecchi F, Betocchi S,Gersh BJ, Ackerman MJ, McCully RB, Dearani JA, Schaff HV, Dan-ielson GK, Tajik AJ, Nishimura RA. Long-term effects of surgical septalmyectomy on survival in patients with obstructive hypertrophic cardio-myopathy. J Am Coll Cardiol. 2005;46:470–476.
5. Dearani JA, Ommen SR, Gersh BJ, Schaff HV, Danielson GK. Surgeryinsight: septal myectomy for obstructive hypertrophic cardiomyopa-thy—the Mayo Clinic experience. Nat Clin Pract Cardiovasc Med. 2007;4:503–512.
6. Woo A, Williams WG, Choi R, Wigle ED, Rozenblyum E, Fedwick K,Siu S, Ralph-Edwards A, Rakowski H. Clinical and echocardiographicdeterminants of long-term survival after surgical myectomy in obstructivehypertrophic cardiomyopathy. Circulation. 2005;111:2033–2041.
7. Smedira NG, Lytle BW, Lever HM, Rajeswaran J, Krishnaswamy G,Kaple RK, Dolney DO, Blackstone EH. Current effectiveness and risks ofisolated septal myectomy for hypertrophic obstructive cardiomyopathy.Ann Thorac Surg. 2008;85:127–133.
8. Sigwart U. Non-surgical myocardial reduction for hypertrophicobstructive cardiomyopathy. Lancet. 1995;346:211–214.
9. Faber L, Welge D, Fassbender D, Schmidt HK, Horstkotte D, SeggewissH. One-year follow-up of percutaneous septal ablation for symptomatichypertrophic obstructive cardiomyopathy in 312 patients: predictors ofhemodynamic and clinical response. Clin Res Cardiol. 2007;96:864–873.
10. Kuhn H, Lawrenz T, Lieder F, Leuner C, Strunk-Mueller C, ObergasselL, Bartelsmeier M, Stellbrink C. Survival after transcoronary ablation ofseptal hypertrophy in hypertrophic obstructive cardiomyopathy (TASH):a 10 year experience. Clin Res Cardiol. 2008;97:234–243.
11. Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ,Seidman CE, Shah PM, Spencer WH, III, Spirito P, Ten Cate FJ, WigleED. American College of Cardiology/European Society of Cardiologyclinical expert consensus document on hypertrophic cardiomyopathy. Areport of the American College of cardiology Foundation Task Force onClinical Expert Consensus Documents and the European Society of Car-diology Committee for Practice Guidelines. J Am Coll Cardiol. 2003;42:1687–1713.
12. Fernandes VL, Nielsen C, Nagueh SF, Herrin AE, Slifka C, Franklin J,Spencer WH III. Follow-up of alcohol septal ablation for symptomatichypertrophic obstructive cardiomyopathy the Baylor and Medical Uni-versity of South Carolina experience 1996 to 2007. J Am Coll CardiolCardiovasc Interv. 2008;1:561–570.
13. Seggewiss H, Rigopoulos A, Welge D, Ziemssen P, Faber L. Long-termfollow-up after percutaneous septal ablation in hypertrophic obstructivecardiomyopathy. Clin Res Cardiol. 2007;96:856–863.
14. Leonardi RA, Kransdorf EP, Simel DL, Wang A. Meta-analyses of septalreduction therapies for obstructive hypertrophic cardiomyopathy: com-parative rates of overall mortality and sudden cardiac death aftertreatment. Circ Cardiovasc Interv. 2010;3:97–104.
15. Faber L, Seggewiss H, Fassbender D, Bogunovic N, Strick S, SchmidtHK, Gleichmann U. [Percutaneous transluminal septal myocardialablation in hypertrophic obstructive cardiomyopathy: acute results in 66patients with reference to myocardial contrast echocardiography]. ZKardiol. 1998;87:191–201.
16. Seggewiss H, Gleichmann U, Faber L, Fassbender D, Schmidt HK, StrickS. Percutaneous transluminal septal myocardial ablation in hypertrophicobstructive cardiomyopathy: acute results and 3-month follow-up in 25patients. J Am Coll Cardiol. 1998;31:252–258.
17. Jensen MK, Havndrup O, Pecini R, Dalsgaard M, Hassager C, Helqvist S,Kelbaek H, Jorgensen E, Kober L, Bundgaard H. Comparison of Valsalvamanoeuvre and exercise in echocardiographic evaluation of left ventric-ular outflow tract obstruction in hypertrophic cardiomyopathy. Eur JEchocardiogr. 2010;11:763–769.
18. Statistics Denmark. www.statbank.dk. Accessed May 15, 2009.19. Statistisk Årbog 2010. http://www.dst.dk/pukora/epub/upload/15197/
headword/dk/431.pdf. Accessed June 9, 2010.20. Roques F, Nashef SA, Michel P, Gauducheau E, de Vincentiis C, Baudet
E, Cortina J, David M, Faichney A, Gabrielle F, Gams E, Harjula A,Jones MT, Pintor PP, Salamon R, Thulin L. Risk factors and outcome inEuropean cardiac surgery: analysis of the EuroSCORE MultinationalDatabase of 19030 patients. Eur J Cardiothorac Surg. 1999;15:816–822;discussion 822–813.
21. Sorajja P, Valeti U, Nishimura RA, Ommen SR, Rihal CS, Gersh BJ,Hodge DO, Schaff HV, Holmes DR Jr. Outcome of alcohol septal
264 Circ Cardiovasc Interv June 2011

ablation for obstructive hypertrophic cardiomyopathy. Circulation. 2008;118:131–139.
22. Brown ML, Schaff HV, Dearani JA, Li Z, Nishimura RA, Ommen SR.Relationship between left ventricular mass, wall thickness, and survivalafter subaortic septal myectomy for hypertrophic obstructive cardiomy-opathy. J Thorac Cardiovasc Surg. 2011;141:439–443.
23. van der LC, Scholzel B, ten Berg JM, Geleijnse ML, Idzerda HH, vanDomburg RT, Vletter WB, Serruys PW, Ten Cate FJ. Usefulness ofclinical, echocardiographic, and procedural characteristics to predictoutcome after percutaneous transluminal septal myocardial ablation. AmJ Cardiol. 2008;101:1315–1320.
24. Veselka J, Duchonova R, Palenickova J, Zemanek D, Tiserova M, Lin-hartova K, Cervinka P. Impact of ethanol dosing on the long-termoutcome of alcohol septal ablation for obstructive hypertrophic cardio-myopathy: a single-center prospective, and randomized study. Circ J.2006;70:1550–1552.
25. Bhagwandeen R, Woo A, Ross J, Wigle ED, Rakowski H, Kwinter J,Eriksson MJ, Schwartz L. Septal ethanol ablation for hypertrophicobstructive cardiomyopathy: early and intermediate results of a Canadianreferral centre. Can J Cardiol. 2003;19:912–917.
26. Gietzen FH, Leuner CJ, Obergassel L, Strunk-Mueller C, Kuhn H.Transcoronary ablation of septal hypertrophy for hypertrophic obstructive
cardiomyopathy: feasibility, clinical benefit, and short term results inelderly patients. Heart. 2004;90:638–644.
27. Kim JJ, Lee CW, Park SW, Hong MK, Lim HY, Song JK, Jin YS, ParkSJ. Improvement in exercise capacity and exercise blood pressureresponse after transcoronary alcohol ablation therapy of septal hypertro-phy in hypertrophic cardiomyopathy. Am J Cardiol. 1999;83:1220–1223.
28. Olivotto I, Gistri R, Petrone P, Pedemonte E, Vargiu D, Cecchi F.Maximum left ventricular thickness and risk of sudden death in patientswith hypertrophic cardiomyopathy. J Am Coll Cardiol. 2003;41:315–321.
29. Faber L, Welge D, Fassbender D, Schmidt HK, Horstkotte D, SeggewissH. Percutaneous septal ablation for symptomatic hypertrophic obstructivecardiomyopathy: managing the risk of procedure-related AV conductiondisturbances. Int J Cardiol. 2007;119:163–167.
30. El-Jack SS, Nasif M, Blake JW, Dixon SR, Grines CL, O’Neill WW.Predictors of complete heart block after alcohol septal ablation for hyper-trophic cardiomyopathy and the timing of pacemaker implantation.J Interv Cardiol. 2007;20:73–76.
31. Veselka J, Zemanek D, Tomasov P, Duchonova R, Linhartova K. Alcoholseptal ablation for obstructive hypertrophic cardiomyopathy: ultra-lowdose of alcohol (1 ml) is still effective. Heart Vessels. 2009;24:27–31.
32. Alam M, Dokainish H, Lakkis N. Alcohol septal ablation for hypertrophicobstructive cardiomyopathy: a systematic review of published studies.J Interv Cardiol. 2006;19:319–327.
CLINICAL PERSPECTIVELeft ventricular outflow tract obstruction in patients with hypertrophic obstructive cardiomyopathy can be reduced by analcohol-induced septal infarct, that is, by selective injection of alcohol in a proximal septal perforator (percutaneoustransluminal septal myocardial ablation [PTSMA]). Single-center reports on outcome of PTSMA treatment have shownmarked differences, and there have been considerable theoretical concerns of potentially malignant arrhythmia in the borderzone of the alcohol-induced infarct. Therefore, surgical myectomy has remained the gold standard. The Scandinavianhypertrophic obstructive cardiomyopathy database was established to evaluate the long-term outcome of PTSMA in aninternational clinical multicenter setting. In 279 patients treated with PTSMA between 1999 and 2010, the left ventricularoutflow tract gradients were reduced to a median (interquartile range) of 12 mm Hg (8 to 24 mm Hg) at rest and 21 mm Hg(11 to 42 mm Hg) during Valsalva maneuver at 1-year follow-up, and these effects remained stable during long-termfollow-up (2.9�2.6 years). The proportion of patients with syncope was reduced from 18% to 2%, and the proportion inNew York Hearth Association class III/IV was reduced from 94% to 21%. Persistent New York Hearth Association classIII/IV was associated with diabetes mellitus, chronic obstructive pulmonary disease, and valve disease unrelated tohypertrophic cardiomyopathy. Ninety-one percent of patients without comorbidities at baseline were in New York HearthAssociation class I/II at follow-up. The in-hospital mortality was 0.3% despite considerable comorbidities, and thelong-term survival was comparable to that in an age- and sex-matched background population. However, a small tendencytoward a reduced survival in the PTSMA-treated patients may have been related the presence of hypertrophiccardiomyopathy per se. PTSMA may become the treatment of choice in hypertrophic obstructive cardiomyopathy in thenear future.
Jensen et al Long-Term Outcome of PTSMA in Scandinavia 265